Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery s present: Early Repair Era
|
|
|
- Donald Skinner
- 6 years ago
- Views:
Transcription


1 Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery : Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era s: Fetal Interventions Hybrid Surgery Robotics and Nanotechnology Stem Cell Therapy Tissue Engineering 1


2 Highly useful clinical tool Feasible mode of therapy is available Fetus at risk for demise Intervention may alter the evolution of the condition Conditions in which fetus at high risk for prenatal or neonatal death Disease likely to have major lifelong morbidity Modify course of cardiac growth, function, development in utero 2

3 Substantial short term risk to fetus Uncertain long term risk ik to fetus and child Some risk to mother No known medical benefits to the mother McElhinney, Circulation 2010;121 3
4 First reported and most entrenched mode of FCI Fetal arrhythmia or heart block Medication taken orally by mother with transplacental passage to the fetus May be provided directly through umbilical vein, fetal muscular or intravascular injection Fetal SVT most common indication Digoxin mainstay of therapy Sotalol, amiodarone, flecainide Indications depend on fetal age and disease severity In preterm fetus, treat regardless of cardiac dsfnction dysfunction or hydrops Intermittent tachycardia, treatment unnecessary 4


5 Sinus node dysfunction, long QT syndrome, AV block, or fetal distress with acidosis Most common is high grade AV block Association with maternal autoimmune disease, malformation syndromes, cctga Dexamethasone, in association with betait improves overall prognosis Sympathomimetic agents increase heart rate in agonists, fetus, do not restore AV synchrony 5
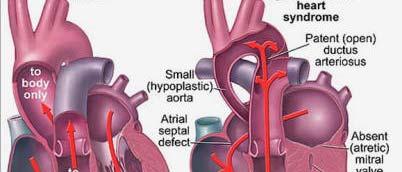
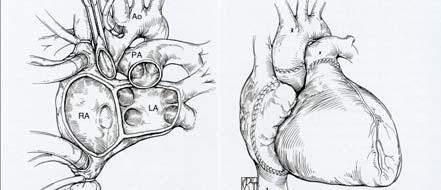
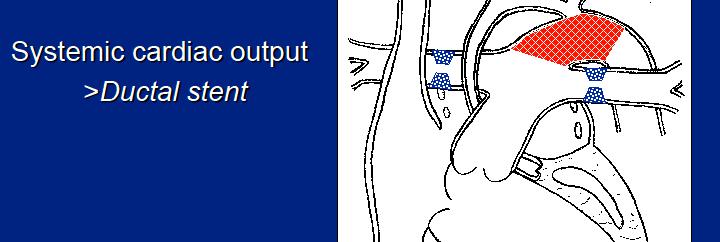
6 Most common closed FCI procedure Alter in utero natural history of midgestation fetal AS with evolving HLHS Physiological features associated with progression to HLHS Retrograde flow in transverse aortic arch Severe LV dysfunction Abnormal mitral valve inflow Left to right flow across foramen ovale Prevent progressive left heart dysfunction and hypoplasia Aortic and mitral valve growth improved No difference in LV growth velocity Clear beneficial changes in left heart physiology Goal to alter left heart physiology and growth to allow biventricular circulation Not a stand alone intervention 6
7 Profound hypoxemia after birth Results in little effective pulmonary blood flow Chronic pulmonary venous hypertension in utero results in pulmonary venous thickening Damage to pulmonary vasculature may contribute to further mortality FCI may improve both major problems posed by restriction of pulmonary venous outflow If left atrium decompressed before birth, perinatal hypoxemia and acidosis prevented If left atrial decompression achieved early in gestation, adverse pulmonary venous remodeling prevented Technical limitations Currently performed in early to mid third trimester 7
8 PA/IVS occurs as a spectrum of hypoplastic right heart disease In newborns, biventricular repair estimated from Z score of tricuspid valve annulus Tricuspid valve Z score in fetuses can also be uses to assess suitability for biventricular outcome Role of FCI is to promote right heart growth and functional development Increase chance of biventricular circulation Identification of potential candidates based on risk of progression to a functionally univentricular circulation Prenatal pulmonary valve perforation and dilation performed in midgestation fetuses Maintenance of valvar patency and improved growth of right heart structures Effects on right heart functional development and postnatal outcome remain to be determined 8


9 Utility of FCI will depend on clinical and technological factors More frequent, earlier diagnosis of CHD Characterization of prognostic features Optimal gestational windows Improved and focused technology Advances in imaging and instrumentation Risk profiles will improve 9
10 Indications Examples Vascular access Very tortuous course of delivery sheaths Better alignment between defect and device Large ASD in patients with small left atrium Bad angle for deployment Avoiding circulatory arrest Stent implantation in a hypoplastic arch Anatomical problem preventing standard d surgical procedure Poor surgical access in apical VSD Interventional procedure during scheduled surgery Stent implantation or balloon angioplasty of pulmonary arteries under direct vision Done surgically, requires right or left ventriculotomy Right ventriculotomy may not be able to see defect Left ventriculotomy can cause LV dysfunction, arrhythmias, and apical aneurysms Perventricular closure avoids transection ti of RV muscle bundles, avoids CPB, not limited by vascular access or patient weight 10


11 -Intraop ballooning and stenting of PAs helpful in select circumstance -Distal branch PA stenosis -Right pulmonary artery runs underneath aorta -Left pulmonary artery near phrenic nerve -Patch material can become calcified leading to stenosis -Stents balloon-expandable -Placed on beating heart -Can develop in-stent stenosis 11

12 Multiple re interventions for right ventricular outflow tract Timing of conduit replacement or pulmonary valve implantation No ideal conduit or valve exists All are susceptible to degeneration and loss of function 12

13 Maximum available size is 22mm Percutaneous approach limited i to patients with RV to PA conduits Can be placed through direct puncture of the RV apex or free wall Will reduce the number of interventions required in children with conduit obstruction or pulmonary insufficiency 13



14 Procedure Norwood Age 1 2 weeks Bidirectional Glenn Shunt 3 4 months Fontan Procedure 3 4 years 14


15 Operative mortality 10 25% Late interstage mortality 8 12% Glenn Procedure 2 5% Developmental delay Neurologic abnormalities Feeding difficulties Ventricular dysfunction Growth delay 15
16 Shock at presentation Birth weight <2.5 kg Prematurity <34 weeks of gestation Age >30 days Aortic atresia Poor RV function Tricuspid regurgitation Intact atrial septum Presence of noncardiac malformations 16


17 17
18 18
19 19


20 Hospital for Sick Children, Toronto, ON 20
21 Despite improved hospital survival, institution reported interstage death has remained constant over past decade at 7 20% Currently neither the STS database nor available administrative databases track patients across admissions Multi center interstage mortality cannot be calculated Dependence on functionally inferior systemic RV to pump to pulmonary and systemic circuits (parallel circulation) Tenuous balance between pulmonary and systemic blood flow Mild desaturation or intravascular volume loss places these infants with minimal myocardial reserve at greater risk for mortality 21


22 Intercurrent Illness Gastroenteritis, fever, respiratory tract infections Concern Hypovolemia Hypoxemia Increased SVR anemia Recurrent/Residual/ Progressive lesions Shunt stenosis/obstruction, neoaortic arch obstruction, restrictive ASD, coronary insufficiency, PA distortion, AVV insufficiency Concern Inadequate pulmonary blood flow Progressive hypoxemia Impaired myocardial performance During late 1990 s, reported anatomic and physiologic variables implicated in interstage death included Diagnosis of aortic atresia Ascending aorta <2.0mm >moderate AV valve insufficiency Post op hemodynamics 22
23 Identify S1P infants at greatest risk Optimize i physiologic i state pre discharge Monitor infants in home for evidence of physiologic variances Keep highest risk S1P infants inpatient until stage 2 Unable to consistently predict which infants most at risk for interstage death Implementation of home monitoring program (HMP) Hypothesis that decreased arterial saturation from baseline, poor weight gain or weight loss may foretell the presence of serious anatomic lesions or intercurrent illness and allow for lifesaving intervention 23


24 Infant scale and pulse oximeters at home Parents asked kd to obtain and record daily weight and oxygen saturation in log book Notification to healthcare provider by parent/caregiver if breach of pre determined criteria occurs Pulse Oximetry Infant probes, continuous monitoring capability, signal verification Weight Digital scale sensitive to 10 grams 24




25 Oxygen sat, weight, and enteral intake recorded on daily log sheet in home monitoring binder Uniform call parameter Infant does not gain grams over 3 days Infant lose >30 grams over 2 3 days O 2 saturations <75% Enteral intake <100cc/kg/24 hours Parents instructed to report any breach Bedside Bdid parent education Rooming In prior to discharge Anticipatory guidance 25


26 Children s Hospital of Wisconsin Potential etiologies contributing to interstage mortality have been identified, however, a lack of proven predictors of interstage demise remains a concern At least one half of interstage infants encounter an at risk physiologic state prior to undergoing S2P A strategy of keeping patients deemed high risk inpatient until S2P can be effective, but costly Interstage mortality can be reduced d via a structured team approach to in home detection of physiological variances Despite diligent interstage care, some infants remain at risk for sudden 26
How Does Imaging Inform Fetal Cardiovascular Treatment?
 How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
Introduction. Study Design. Background. Operative Procedure-I
 Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Hybrid Stage I Palliation / Bilateral PAB
 Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Leitlinien. Hypoplastisches Linksherzsyndrom. Hypoplastic left heart syndrome (HLHS)
") 1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment
 Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Children with Single Ventricle Physiology: The Possibilities
 Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
 Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Atrial Septostomy in HLHS and ECMO: Indications, Technique and Outcome
 Atrial Septostomy in HLHS and ECMO: Indications, Technique and Outcome Dr Damien Kenny, MB, MD Assistant Professor of Pediatrics Director of the Cardiac Catheterization Hybrid Suite Co-Director of the
Atrial Septostomy in HLHS and ECMO: Indications, Technique and Outcome Dr Damien Kenny, MB, MD Assistant Professor of Pediatrics Director of the Cardiac Catheterization Hybrid Suite Co-Director of the
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
FUNCTIONALLY SINGLE VENTRICLE
 MORPHOLOGICAL DETERMINANTS VI TRAN EuroEcho, Budapest, 7 th December 2011 DECLARATION OF CONFLICT OF INTEREST: I have nothing to declare What is the functionally single ventricle? The heart that is incapable
MORPHOLOGICAL DETERMINANTS VI TRAN EuroEcho, Budapest, 7 th December 2011 DECLARATION OF CONFLICT OF INTEREST: I have nothing to declare What is the functionally single ventricle? The heart that is incapable
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin. Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong
 Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
What is the Definition of Small Systemic Ventricle. Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University
 What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
The Double Switch Using Bidirectional Glenn and Hemi-Mustard. Frank Hanley
 The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT
 LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT 10-13 March 2017 Ritz Carlton, Riyadh, Saudi Arabia Zohair AlHalees, MD Consultant, Cardiac Surgery Heart Centre LEFT VENTRICULAR
LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT 10-13 March 2017 Ritz Carlton, Riyadh, Saudi Arabia Zohair AlHalees, MD Consultant, Cardiac Surgery Heart Centre LEFT VENTRICULAR
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Fetal Rhythm and Blues
 Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions
 Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Alagille syndrome, pulmonary artery stenosis in, 143 145, 148 149 Amplatz devices for atrial septal defect closure, 42 46 for coronary
Index Note: Page numbers of article titles are in boldface type. A Alagille syndrome, pulmonary artery stenosis in, 143 145, 148 149 Amplatz devices for atrial septal defect closure, 42 46 for coronary
ULTRASOUND OF THE FETAL HEART
 ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY
 가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of percutaneous fetal balloon valvuloplasty for aortic stenosis 322 Introduction
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of percutaneous fetal balloon valvuloplasty for aortic stenosis 322 Introduction
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of percutaneous fetal balloon valvuloplasty for pulmonary atresia with intact
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of percutaneous fetal balloon valvuloplasty for pulmonary atresia with intact
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
List of Videos. Video 1.1
 Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
PIAF study: Placental insufficiency and aortic isthmus flow Jean-Claude Fouron, MD
 Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE
 Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
The Single Ventricle. Karim Rafaat, M.D.
 The Single Ventricle Karim Rafaat, M.D. The title single ventricle includes those lesions designated as both HLHS HRHS HLHS is far more common, and the strategy for palliation of both lesions similar,
The Single Ventricle Karim Rafaat, M.D. The title single ventricle includes those lesions designated as both HLHS HRHS HLHS is far more common, and the strategy for palliation of both lesions similar,
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Prenatal Predictors of Postnatal Outcome in Pulmonary Atresia with Intact Ventricular Septum: A Multicenter Study
 Fetal Heart Society Concept Research Proposal Date: 10/20/15 Main Study Prenatal Predictors of Postnatal Outcome in Pulmonary Atresia with Intact Ventricular Septum: A Multicenter Study Shaji C. Menon,
Fetal Heart Society Concept Research Proposal Date: 10/20/15 Main Study Prenatal Predictors of Postnatal Outcome in Pulmonary Atresia with Intact Ventricular Septum: A Multicenter Study Shaji C. Menon,
Cardiac Intervention in Fetus. Gyeong-hee Yoo, M.D. Department of Pediatrics Soonchunhyang University Cheonan Hospital
 10 1111 Cardiac Intervention in Fetus Gyeong-hee Yoo, M.D. Department of Pediatrics Soonchunhyang University Cheonan Hospital Fetal echocardiography Serial f/u intrauterine course of disease Cardiac anomaly
10 1111 Cardiac Intervention in Fetus Gyeong-hee Yoo, M.D. Department of Pediatrics Soonchunhyang University Cheonan Hospital Fetal echocardiography Serial f/u intrauterine course of disease Cardiac anomaly
SWISS SOCIETY OF NEONATOLOGY. Prenatal closure of the ductus arteriosus
 SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
How pregnancy impacts adult cyanotic congenital heart disease
 How pregnancy impacts adult cyanotic congenital heart disease Magalie Ladouceur Adult Congenital Heart Disease Unit, Hôpital Européen Georges Pompidou, Centre de reference des Malformations Cardiaques
How pregnancy impacts adult cyanotic congenital heart disease Magalie Ladouceur Adult Congenital Heart Disease Unit, Hôpital Européen Georges Pompidou, Centre de reference des Malformations Cardiaques
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
ISUOG Basic Training. Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA. Basic training. Editable text here
 ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
NEONATAL HYBRID PROCEDURES STRATEGIES TO REDUCE MORBIDITY AND MORTALITY
 NEONATAL HYBRID PROCEDURES STRATEGIES TO REDUCE MORBIDITY AND MORTALITY FOTIOS A. MITROPOULOS, MD, PHD DEPARTMENT OF PEDIATRIC AND ADULT CONGENITAL HEART SURGERY MITERA HYGEIA HOSPITALS, ATHENS, GREECE
NEONATAL HYBRID PROCEDURES STRATEGIES TO REDUCE MORBIDITY AND MORTALITY FOTIOS A. MITROPOULOS, MD, PHD DEPARTMENT OF PEDIATRIC AND ADULT CONGENITAL HEART SURGERY MITERA HYGEIA HOSPITALS, ATHENS, GREECE
Although most patients with Ebstein s anomaly live
 Management of Neonatal Ebstein s Anomaly Christopher J. Knott-Craig, MD, FACS Although most patients with Ebstein s anomaly live through infancy, those who present clinically as neonates are a distinct
Management of Neonatal Ebstein s Anomaly Christopher J. Knott-Craig, MD, FACS Although most patients with Ebstein s anomaly live through infancy, those who present clinically as neonates are a distinct
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING
 PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT
 FOR REPAIRED TETRALOGY OF FALLOT") MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
Adults with Congenital Heart Disease
 Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Most common fetal cardiac anomalies
 Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Failing right ventricle
 Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Fetal Tetralogy of Fallot
 36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
PREGNANCY AND CONGENITAL HEART DISEASE
 PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
Heart Development and Congenital Heart Disease
 Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
Adult Congenital Heart Disease: A Growing Problem. Dr. Gary Webb Cincinnati Children s Hospital Heart Institute
 Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
Surgical Repairs for LVOT Obstructive Lesions. John J. Lamberti MD
 Surgical Repairs for LVOT Obstructive Lesions John J. Lamberti MD Surgical Repairs for LVOT Obstructive Lesions Presented by John J. Lamberti MD Faculty Disclosure Statement: I do not have any relevant
Surgical Repairs for LVOT Obstructive Lesions John J. Lamberti MD Surgical Repairs for LVOT Obstructive Lesions Presented by John J. Lamberti MD Faculty Disclosure Statement: I do not have any relevant
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Anomalous Systemic Venous Connection Systemic venous anomaly
 World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
The Physiology of the Fetal Cardiovascular System
 The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Systematic approach to Fetal Echocardiography. Objectives. Introduction 11/2/2015
 Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
When to implant an ICD in systemic right ventricle?
 When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Complex Congenital Heart Disease in Adults
 Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Critical Heart Disease in the Newborn. What you need to know
 Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan
 PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan Fetal Cardiology Unit, Harris Birthright Research Centre for Fetal Medicine, King's College Hospital, London, UK IMPORTANCE OF PRENATAL
PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan Fetal Cardiology Unit, Harris Birthright Research Centre for Fetal Medicine, King's College Hospital, London, UK IMPORTANCE OF PRENATAL
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Accuracy of the Fetal Echocardiogram in Double-outlet Right Ventricle
 Blackwell Publishing IncMalden, USACHDCongenital Heart Disease 2006 The Authors; Journal compilation 2006 Blackwell Publishing, Inc.? 200723237Original ArticleFetal Echocardiogram in Double-outlet Right
Blackwell Publishing IncMalden, USACHDCongenital Heart Disease 2006 The Authors; Journal compilation 2006 Blackwell Publishing, Inc.? 200723237Original ArticleFetal Echocardiogram in Double-outlet Right
The Fontan circulation. Folkert Meijboom
 The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
cardiac imaging planes planning basic cardiac & aortic views for MR
 cardiac imaging planes planning basic cardiac & aortic views for MR Dianna M. E. Bardo, M. D. Assistant Professor of Radiology & Cardiovascular Medicine Director of Cardiac Imaging cardiac imaging planes
cardiac imaging planes planning basic cardiac & aortic views for MR Dianna M. E. Bardo, M. D. Assistant Professor of Radiology & Cardiovascular Medicine Director of Cardiac Imaging cardiac imaging planes
Assessment of fetal heart function and rhythm
 Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics