MANAGEMENT OF CIRCULATORY FAILURE
|
|
|
- Annis Hutchinson
- 5 years ago
- Views:
Transcription
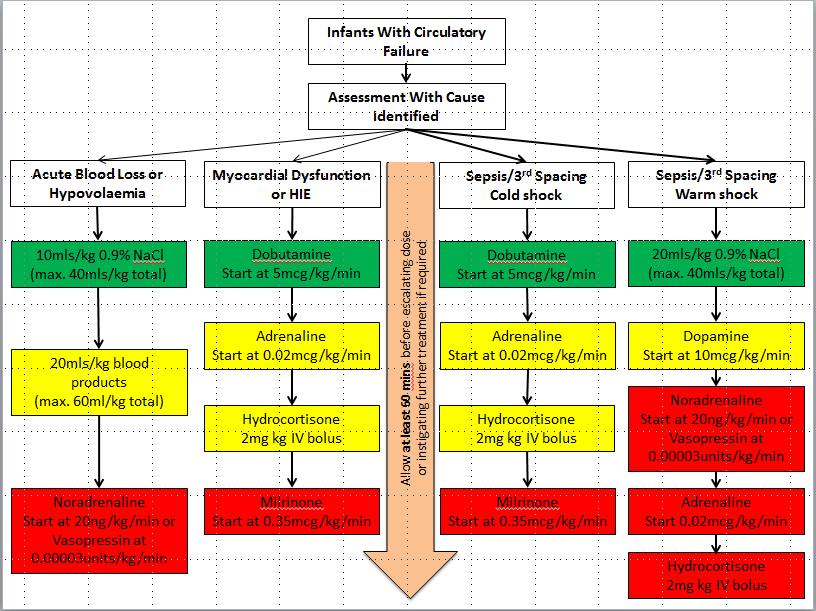
1 MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to an imbalance between systemic oxygen delivery (oxygenation and/or perfusion) and systemic oxygen demand. Its pathology is multifactorial and influenced by internal factors such as poor myocardial contractility and external factors like respiratory failure, PDA, anaemia, sepsis, asphyxia. Treatment for this condition lacks empirical evidence ASSESSMENT Bedside Clinical Parameters: Body temperature o A skin shin gap > 2 C can be associated with poor microcirculation as in significant dehydration or sepsis Blood Pressure o Blood Pressure (BP) = Cardiac Output (CO) x Systemic Vascular Resistance (SVR); Cardiac Output (CO) = Stroke Volume (SV) x Heart Rate (HR); Stroke volume depends on preload, contractility and afterload. o The gold standard measurement of blood pressure is performed via an invasive arterial catheter; alternatives include non-invasive oscillometric methods such as cuff blood pressure measurements. They have a good correlation with the invasive arterial methods. However, this is dependent on the accurate selection of an appropriate blood pressure cuff size and precise application. Heart Rate o A heart rate >160 beats per minute in a can be a sign of hypovolaemia. o Low specificity for predicting cardiovascular compromise. Capillary Refill Time o The vasomotor tone of surface capillaries in premature and low birth weight infants is not established. Capillary refill time is also dependent on the ambient temperature making it less reliable in situations such as total body cooling in HIE in term babies. o Evidence as to whether capillary refill time is reliable in assessing end organ perfusion is therefore conflicting. The sensitivity and specificity of a capillary refill time >3 seconds being predictive of low SVC flow (biomarker associated with intracranial haemorrhage) is 78% and 63% respectively when combined with a mean BP of <30mmHg.. 1
2 Invasive Blood pressure thresholds at 3 th percentile according to gestational age (GA) GA (weeks) Systolic (mmhg) Diastolic (mmhg) Mean (mmhg)
3 Urine Output o An association between low output SVC flow and low urine output in preterm infants has been found, but interpretation is difficult as in the first 24 hours in very premature infants urine output is already very low. o Reduction in urine output is often a late sign of poor perfusion. Biochemical Parameters: Lactate o Levels >4mmol/L in the first 48 hours and >3mmol/L thereafter can indicate significant tissue hypoxia in infants at birth, but up to 4.4mmol/L in the first hours can be normal. o When capillary refill time is >3 seconds and lactate >4mmol/L there is a 97% probability of finding low SVC flow. Base Excess o A base excess at birth of -7.3mmol/L has a sensitivity and specificity of 100% and 71% respectively for death or cerebral injury. o It correlates well to lactate levels in preterm infants. Technological parameters including functional echocardiography: Base Excess Oxygen Extraction Rate and Central Venous Saturation o Tissue oxygenation can be estimated by looking at the oxygen extraction rate (OER=SaO2 - ScvO2)/SaO2; normal=approx. 0.25). For this we have to know what the oxygen delivery (DO2= CO x (Hb x SaO2 x PaO2)) and demand (VO2= CO x Hb x (SaO2 - SvO2)) is. This can be estimated with the knowledge of cardiac output (CO), arterial saturation (SaO2) and central venous saturation (ScvO2 [surrogate for SvO2); normal=approx.65-75%). o A high OER indicates a disturbed balance between DO2 and VO2, which could be caused by an increased VO2 and/or by a decreased DO2. The tissue oxygenation is poor when there is a combination of low CO, low ScvO2, high OER and lactate. There are four fundamental causes for a drop in ScvO2: a drop in CO, a low Hb, low SaO2, increased oxygen consumption without increase in oxygen delivery. 3
4 CVP o Can be used in sick patient as a guide for volume status - normal level 0-6mmHg; beware of high values due to right sided cardiac failure Near-Infrared Spectroscopy (NIRS) o There is good correlation between SVC and cardiac output. o For detailed information on what to measure and how to use the information obtained with NIRS please see separate guidance on Near-Infrared Spectroscopy. Functional Echochardiography (fnecho) o Functional echocardiography (fnecho) is a useful objective method for assessing the systemic and pulmonary blood flow and myocardial performance in different clinical circumstances such as PPHN, PDA, arterial hypotension, acute hypovolaemia or sepsis. It can be used to add information about the haemodynamic status and provide guidance in the choice of inotropic support and treatment options in different clinical scenarios. o For detailed information on what to measure and how to use the information obtained with echocardiography please see separate guidance (Functional Echocardiography). aeeg o aeeg (and Cerebral Fractional Oxygen Extraction) becomes abnormal at MBP <23mmHg in very low birthweight infants suggesting that cerebral perfusion might be compromised. 4
5 MANAGEMENT Prevention: Cord Milking or Delayed Cord Clamping o Lead to less transfusions o Better SVC flow o Less intraventricular haemorrhages o Negligible side-effects Permissive Hypotension (ALL CRITERIA) o Mean BP in mmhg lower than gestational age in weeks o Capillary refill time <4 seconds o Lactate <5 mmol/l o Base excess <-7 mmol/l o Core-shin temperature gap of <2 0 C o Urine output >1ml/kg/hour Treatment: Volume Replacement o There is no simple objective method to assess fluid-responsiveness. However, goal directed therapies indicate that aggressive fluid resuscitation is beneficial in scenarios of acute large volume loss and fluid re-distribution to third spaces. o Current evidence suggests that neither colloids nor crystalloids are superior in terms of successfully treating hypotension, mortality or long-term morbidity except for albumin. o Aliquots of 10-20ml/kg boluses of 0.9% saline are effective and safe for raising blood pressure and cardiac output. o Where circulatory failure is associated with blood loss it is recommended that packed red cell transfusion of 15-20ml/kg be given and fresh frozen plasma is useful in conditions where hypotension is associated with deranged clotting. Inotropic Therapy o Dopamine: Dopamine is an agonist of multiple receptors including α, β, and dopaminergic receptors (in the newborn predominantly affects peripheral and pulmonary vasculature by α adrenergic effect). 25% of infused dopamine is converted into norepinephrine which may contribute to its cardiovascular effects. Dopaminergic effect on kidneys in newborns is not proven. 5
6 o o o o Dopamine is more successful than dobutamine at raising a neonate s blood pressure. There is no difference with regards to short and long term morbidity or mortality. Caution when using in PPHN due to possible increase PVR Dobutamine: Dobutamine has predominantly β1 and β2 adrenergic activity and (-) enantiomer has α1 adrenergic effects. In the peripheral vasculature α1 and β2 adrenergic activity negate each other. In the heart the activitiy is predominantly β1 adrenergic at low doses. There is minimal impact on the SVR and afterload. It has been shown to moderately increase blood pressure and right ventricular output as well as significantly increase superior vena cava and left ventricular output in response to infusions of 10 20mcg/kg/min. It decreases systemic and pulmonary vascular resistance and increase renal and gut perfusion, so may have a role in neonatal surgical pathology. Adrenaline: Adrenaline is believed to act in a similar manner to dopamine in the preterm population; potent non-selective α agonist and also activates both β1 and β2 receptors; activates both β1 and β2 receptors at low doses mcg/kg/min and α1 and β1 receptors at high doses mcg/kg/min. It increases SV, CO, SVR One trial found adrenaline to be as good a dopamine in increasing a neonate s blood pressure. Adrenaline is more likely to cause issues with hyperglycaemia, myocardial oxygen use, raised lactate levels and arrhythmias. Noradrenaline: Norepinephrine is a potent non-selective α agonist with some effect at the β1 receptor. It is released from peripheral nerve endings, it is a potent vasoconstrictor that will also increase myocardial contractility. It has not been studied systematically in the neonatal population. However it is a first line therapy in adult and paediatric vasodilatative shock and has shown less adverse events than Dopamine in the management of adult shock (higher risk of arrhythmias). Milrinone: Milrinone is a selective phosphodiesterase-3 (PDE-3) inhibitor that increases intracellular 3 o 5 o cyclic adenosine-mono-phosphate (camp). Augmentation of 6
7 o o o intracellular camp leads to positive inotropy, lusitropy, reduction in PVR and reduction in systemic afterload. Used predominantly in the maintenance of cardiac output post cardiac surgery and in PPHN; caution when using in PPHN babies with low BP (consider combination with adrenaline or noradrenaline). Vasopressin: Vasopressin is an endogenous neuropeptide which is secreted from the posterior pituitary gland; it increases reabsorption of water (V2 receptors in the collecting duct of the kidney - may cause low Na), vasoconstriction (V1 receptors located in vascular smooth muscle), reduction in heart rate (V1 receptors located in central nervous system), increases adrenal cortisol secretion in presence of ACTH. In severe shock vasopressin has shown to be depleted and the rationale for its use is to increase these depleted levels and promote vasoconstriction (avoid using together with Noradrenaline, if possible). Pentoxifylline: Pentoxifylline, a xanthine derivative, is a phosphodiesterase inhibitor that suppresses TNF-production by adenyl cyclase activation and increased cellular cyclic adenosine 3,5 -monophosphate concentration. Inhibition of TNF-production negates this response and thereby may improve outcome. It also has vasodilative effects and beneficial effects on endothelial cell function, coagulation and immune system. Hydrocortisone: Corticosteroids up-regulate cardiovascular receptors and addresses a preterm neonate s relative adrenocortical insufficiency. It up-regulates and potentiates receptor pathways for both α agonists and angiotensin II, induces the final enzyme in the conversion of stored norepinephrine to epinephrine, increases circulating catecholamine and inhibits local production of vasodilators such as inducible nitric oxide synthase and prostacyclin. Has primarily been used in vasopressor resistant shock and has been shown to increase systemic blood pressure in preterm infants with refractory hypotension within 2 6h without compromising cardiac function, systemic or end-organ blood flow. Helps improve capillary leak syndrome. Concerns about effect on long term development appear to be unfounded, but has been associated with spontaneous intestinal perforation (especially when combined with NSAID). 7
8 Drug Dose Range (IV) SV and CO SVR PVR Dopamine 1 20 mcg/kg/min + HR * Noradrenaline mcg/kg/min - no effect Vasopressin units/kg/min Dobutamine 1 20 mcg/kg/min * - no effect Adrenaline mcg/kg/min mcg/kg/min unknown Milrinone mcg/kg/min Pentoxifylline 5mg/kg/h for 6h from 3-6 days no effect Hydrocortisone 2 mg/kg single dose + 1mg/kg TDS no effect SVR=Systemic Vascular Resistance; PVR= Pulmonary Vascular Resistance; SV=Stroke Volume; CO= Cardiac Output; *=with increasing dose 8
9 9
10 Specific Treatment Considerations: Systolic Hypotension (ABP <3 rd centile), low Cardiac Output o Rule out non cardiovascular factors contributing to low LV filling (preload) such as pneumothorax, chest effusion, pneumopericard, pericardial effusion, high mean airway pressure. o Check heart rate for arrhythmias and if possible cardiac function with fnecho. o Aim for ScvO2 >70% and SVC flow above 40ml/kg/min. o Consider a fluid bolus 10-20ml/kg. o Start Dobutamine (first line), Adrenaline (second line), Milrinone (third line). o Consider ino, Prostaglandin, Tolazoline, Mg-Sulfate, Prostacyclin for PPHN o Beware that during hypothermia CO reduces by 60-70% 10
11 Diastolic Hypotension (ABP <3 rd centile), low Systemic Vascular Resistence o Inotropic agents should be avoided in hypovolaemia as these neonates are typically hypercontractile and tachycardia may impair filling and worsen SBF. o Aim for ScvO2 >70% and SVC flow above 40ml/kg/min. o Treat acute hypovolaemia (absolute/relative) with liberal fluid replacement (total max. 60 ml/kg), either Normal Saline and/or Blood Products as indicated. Avoid Albumin. o Give volume (first line), start Dopamine (second line), Noradrenaline or Vasopressin (third line), Adrenaline (fourth line), consider Phenylephrine. o Consider permissive hypercapnia, shorter IT< 0.35s, higher PEEP >4.5cmH2O, fluid restriction, dobutamine and NSAID in PDA. Consider Pentoxyfilline in NEC on day 3-6. Consider adding Hydrocortisone, if catecholamine resistant shock is present (no response despite using two inotropic agents). 11
12 12
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Hypotension in the Neonate
 Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
When Fluids are Not Enough: Inopressor Therapy
 When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Neonatal Shock. Imbalance between tissue oxygen delivery and oxygen consumption
 Neonatal Shock Moira Crowley, MD Assistant Professor, Pediatrics Co-director, Neonatal ECMO Program Rainbow Babies and Children s Hospital Case Western Resverve University School of Medicine 1 Objectives
Neonatal Shock Moira Crowley, MD Assistant Professor, Pediatrics Co-director, Neonatal ECMO Program Rainbow Babies and Children s Hospital Case Western Resverve University School of Medicine 1 Objectives
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Useful diagnostic measures: chest x ray to check pulmonary edema, ECG and ECHO to detect cardiac abnormalities (1).
.") Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
I intend to discuss an unapproved/investigative use of a commercial product/device in my presentation
 Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Pharmacology of inotropes and vasopressors
 Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
When Fluids are Not Enough: Inopressor Therapy
 When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato. Win Tin The James Cook University Hospital University of Durham
 Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato Win Tin The James Cook University Hospital University of Durham Introduction Fluid Bolus/es (Intravascular Volume Expansion) - One of the
Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato Win Tin The James Cook University Hospital University of Durham Introduction Fluid Bolus/es (Intravascular Volume Expansion) - One of the
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Shock and Vasopressors. Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14
 Shock and Vasopressors Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14 Review Question Unilaterally diminished breath sounds A. Figure 1 B. Figure 2 C. Both D. Neither Related Specialties
Shock and Vasopressors Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14 Review Question Unilaterally diminished breath sounds A. Figure 1 B. Figure 2 C. Both D. Neither Related Specialties
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
How to maintain optimal perfusion during Cardiopulmonary By-pass. Herdono Poernomo, MD
 How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Pediatric Septic Shock. Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee
 Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6
 Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
SHOCK. May 12, 2011 Body and Disease
 SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017
 VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017 CONFLICTS OF INTEREST OVERVIEW Why? When? What? How? WHY? Circulation WHY? - SHOCK!!! Pump (Heart) HYPOVOLAEMIC the pipes have
VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017 CONFLICTS OF INTEREST OVERVIEW Why? When? What? How? WHY? Circulation WHY? - SHOCK!!! Pump (Heart) HYPOVOLAEMIC the pipes have
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
MANAGEMENT OF NEONATAL HYPOTENSION CLINICAL GUIDELINE
 MANAGEMENT OF NEONATAL HYPOTENSION CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1. To provide guidance on the assessment and management of infants with hypotension. All involved will benefit from
MANAGEMENT OF NEONATAL HYPOTENSION CLINICAL GUIDELINE 1. Aim/Purpose of this Guideline 1.1. To provide guidance on the assessment and management of infants with hypotension. All involved will benefit from
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
Haemodynamic Support. (getting the blood to go round and round) philippelefevre.com
 philippelefevre.com") Haemodynamic Support (getting the blood to go round and round) philippelefevre.com Haemodynamic Support Whats wrong with your patient? What can we do about it? Volume expansion Inotropes, Chronotropes
Haemodynamic Support (getting the blood to go round and round) philippelefevre.com Haemodynamic Support Whats wrong with your patient? What can we do about it? Volume expansion Inotropes, Chronotropes
Weeks 1-3:Cardiovascular
 Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Post Resuscitation Care
 Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Anaesthesia. Cardiovascular. Update in. Inotropes and vasopressors in critical care
 Update in Anaesthesia Inotropes and vasopressors in critical care Hannah Dodwell and Bruce McCormick Correspondence Email: hannah.dodwell@doctors.net.uk INTRODUCTION Shock is present in many patients requiring
Update in Anaesthesia Inotropes and vasopressors in critical care Hannah Dodwell and Bruce McCormick Correspondence Email: hannah.dodwell@doctors.net.uk INTRODUCTION Shock is present in many patients requiring
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS
 Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
9/16/2012. Progression of Shock. Blood pressure: Pathophysiology & Clinical Management
 Mean BP (mm Hg) 9/16/212 September 2, 14: 6 min Blood pressure: Pathophysiology & Clinical Management Shahab Noori, MD Associate Professor of Pediatrics Division of Neonatology Progression of Shock BP
Mean BP (mm Hg) 9/16/212 September 2, 14: 6 min Blood pressure: Pathophysiology & Clinical Management Shahab Noori, MD Associate Professor of Pediatrics Division of Neonatology Progression of Shock BP
Dr Richard Pugh Consultant Anaesthetics/ Intensive Care Medicine May 2010
 Dr Richard Pugh Consultant Anaesthetics/ Intensive Care Medicine May 2010 The brainstem: Midbrain, pons, medulla Consciousness Cardiovascular and respiratory regulation Sleep- wake cycle Integration of
Dr Richard Pugh Consultant Anaesthetics/ Intensive Care Medicine May 2010 The brainstem: Midbrain, pons, medulla Consciousness Cardiovascular and respiratory regulation Sleep- wake cycle Integration of
SHOCK in Paediatric Trauma
 SHOCK in Paediatric Trauma Speaker: Tang Sze Kit, (Fellow, Hong Kong College of Paediatric Nursing, MSc, MN, BN) Date: 26/4/2016 Time: 18:30-19:30 Venue: Paediatrics & Adolescent Ambulatory Centre, G/F,
SHOCK in Paediatric Trauma Speaker: Tang Sze Kit, (Fellow, Hong Kong College of Paediatric Nursing, MSc, MN, BN) Date: 26/4/2016 Time: 18:30-19:30 Venue: Paediatrics & Adolescent Ambulatory Centre, G/F,
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Perioperative Management of TAPVC
 Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
Cardiovascular System B L O O D V E S S E L S 2
 Cardiovascular System B L O O D V E S S E L S 2 Blood Pressure Main factors influencing blood pressure: Cardiac output (CO) Peripheral resistance (PR) Blood volume Peripheral resistance is a major factor
Cardiovascular System B L O O D V E S S E L S 2 Blood Pressure Main factors influencing blood pressure: Cardiac output (CO) Peripheral resistance (PR) Blood volume Peripheral resistance is a major factor
Cardiovascular Physiology
 Cardiovascular Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through two vascular systems
Cardiovascular Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through two vascular systems
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
How to resuscitate the patient in early sepsis? A physiological approach. J.G. van der Hoeven, Nijmegen
 How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
Management and treatment of hypotension and hypertension
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Management and treatment of hypotension and hypertension Author : Kit Sturgess Categories : Companion animal, Vets Date :
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Management and treatment of hypotension and hypertension Author : Kit Sturgess Categories : Companion animal, Vets Date :
Physiologic Aspects of the Preterm Circulation
 Staff Neonatologist, Hospital for Sick Children, Toronto Physiologic Aspects of the Preterm Circulation Patrick McNamara Associate Professor of Pediatrics, University of Toronto The Vulnerable Neonate
Staff Neonatologist, Hospital for Sick Children, Toronto Physiologic Aspects of the Preterm Circulation Patrick McNamara Associate Professor of Pediatrics, University of Toronto The Vulnerable Neonate
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
1
 1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the PreSep oximetry catheter for
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the PreSep oximetry catheter for continuous central venous oximetry (ScvO 2 ) 3 The Vigileo
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the PreSep oximetry catheter for continuous central venous oximetry (ScvO 2 ) 3 The Vigileo
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2): Oxford University Press
: Oxford University Press") Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Inventory of paediatric therapeutic needs
 24 April 2013 EMA/PDCO/246339/2013 Human Medicines Development and Evaluation Cardiovascular therapeutic area Agreed by PDCO August 2012 Adopted by PDCO for release for consultation 15-17 August 2012 Start
24 April 2013 EMA/PDCO/246339/2013 Human Medicines Development and Evaluation Cardiovascular therapeutic area Agreed by PDCO August 2012 Adopted by PDCO for release for consultation 15-17 August 2012 Start
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL
 Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
HHS Public Access Author manuscript Crit Care Med. Author manuscript; available in PMC 2015 May 28.
 Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine A full list of authors and affiliations appears
Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine A full list of authors and affiliations appears
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation?
 can help prevent Postoperative Cardiorespiratory instability following PDA ligation?") Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV