Physiologic Aspects of the Preterm Circulation
|
|
|
- Jemimah Lester
- 5 years ago
- Views:
Transcription





1 Staff Neonatologist, Hospital for Sick Children, Toronto Physiologic Aspects of the Preterm Circulation Patrick McNamara Associate Professor of Pediatrics, University of Toronto

2 The Vulnerable Neonate How will you ensure cardiovascular stability?
3 PROTOCOLS CONFUSION RCTs, metanalysis Art of Medicine Physiology Evidence


4 Myths & Magical numbers & Cook books
5 Case I Case II 26 week (650 g) preterm 3 hours old Vitals BP 30 / 18 (22) Heart rate 160 BP 38 / 26 (32) heart rate 160 Investigations ph 7.19, CO 2 34, Bxs -11 Lactate 5.2 mmol/l ph 7.19, CO 2 34, Bxs -11 Lactate 5.2 mmol/l Likelihood of cardiotrope High Low
6 Myths of the Modern Era Numerical Hypotension (mean blood pressure < GA) is problematic?
7 Must have strong scientific validity Must have strong link to abnormal outcome Must be a reliable surrogate of systemic blood flow

8 Origin of Mean BP > GA
9 Low Blood Pressure leads to adverse neurodevelopmental sequelae? Cerebrovascular autoregulation is compromised in premature infants?
10 Griesen 2005 EHD Is cerebrovascular regulation developed in premature infants? Altered by hypoxaemia x 4-7 hrs (neonatal ovine model) Tweed 1986 Ped Red

11 BP & Cerebral Perfusion Tsuji 2000 Pediatr Tyszcuk 1998 Paediatrics
12 White matter Injury and Hypotension YES NO Weindling (n=86) 1985 De Vries (n=51) 1988 Miall-Allen (n=131) 1987 Trounce (n=200) 1988 Watkins (n=33) 1989 Bejar (n=127) 1992 Low (n=98) 1993 Gronlund (n=42) 1994 D Souza (n=34) 1995 Perlman (n=632) 1996 Wiswell (n=67) 1996 Baud (n=110) 1998 Cunn ham (n=232) 1999 DuPlessis (n=260) 2007
13 N = 211 Higher incidence of IUGR, Postnatal steroids, BPD, Diuretic usage in hypotensive group Martens 2003 Early Human Dev
14 Is Hypotension an Epiphenomenon?
15 A Physiologic Oversimplification Fail to consider systemic blood flow and tissue oxygenation Fail to consider the nature of the problem Fail to consider issues related to maturation Fail to consider response to treatment which may be developmentally regulated
16 Systemic blood flow & MBP LVO SVC flow 1000 r = r = mls/kg/min] mls/kg/min] MBP [mmhg] MBP [mmhg] McNamara et al, 2007

17 Low SVC Flow and Intracranial Injury N = 99 No IVH 18 Late IVH Normal range. Kluckow 2000 ADC
18 Therapeutic Intervention Identifying that there is a cadiovascular problems Deciding on the most appropriate intervention and when?
19

20 One rule (Pressor approach) Preterm PDA Sepsis/NEC does not fit all Fullterm PPHN Sepsis HIE Single ventricle physiology
21 Metabolic Homeostasis Hemoglobin Anemia Hemorrhage Cellular Metabolism Oxygen Saturation Lung disease Shunts Heart Rate arrhythmia Preload Volume status Diastolic function Pericardial effusion Afterload SVR, pericardial P Oxygen Delivery Cardiac Output Contractility Catecholamines, sepsis Cardiomyopathy, acidosis SVR BP Oxygen Consumption Work Breathing, growth, trauma catabolism, fever Basal Metabolism Pain, sedation, anxiety thermogenesis
22 Defining the Nature of the Problem Preload Myocardial Function Afterload Heart Problem Rhythm problem Hypovolaemia Prematurity < 48 hours of life HSDA SVT Overinflation Sepsis / NEC PDA Ligation Coarctation Complete heart block Adrenal suppression Adrenal suppression Pulmonary hypertension HLHS IDM Aortic stenosis

23 Volume, preload & neonates Van Hare 1990 Circ Research
24 Is Preload management important? All sick neonates (e.g. sepsis) need a CVP within normal range [5-8] Identifiable fluid loss e.g. gastroschisis, NEC Poorly compliant right ventricle i.e. Septal hypertrophy / or Hypertrophic cardiomyopathy, TEF/HRV [8-12]
25 Myocardial performance in neonates Systolic Fetal/neonatal myocardium less compliant with 70 % noncontractile tissue (Romero 1983 Ped Res) Less active tension at optimal sarcomere length Friedman 1972 Prog Card Dis Inotrope-responsiveness potentially less Romero 1979 Ped Res Diastolic vulnerability Impaired early filling and low E waves! Riggs 1989 JACC, Reed Circulation 1986
26 Rowland 1995 Am J Card Stress-Velocity Relationship NEONATE CHILD
27 When should Afterload be considered PPHN(Pulmonary Afterload) Ductal Physiology ELBW infants with early LCOS (< 48 hours) Balancing Single ventricle physiology
28 Scenario I 26 week premature infant 760 g (surf x 1) Retrieved by regional transport team Received 2 boluses of crystalloid (20 mls/kg) for mean blood pressure of 20 mmhg BP HR ph Bxs Lac Intervention Admit 45/22 (29) SiMV15/5, FiO hrs 30/16 (20) Observed 45 mins 0.9% saline bolus 35/20 (25) 12 hrs 32/16 (22) Dopamine 7.5µg 38/18 (24) 15 hrs 36/14 (22) Dopamine 10µg 38/16 (23) 20 hrs 41/13 (22) Dobutamine10µg 45/12 (24)


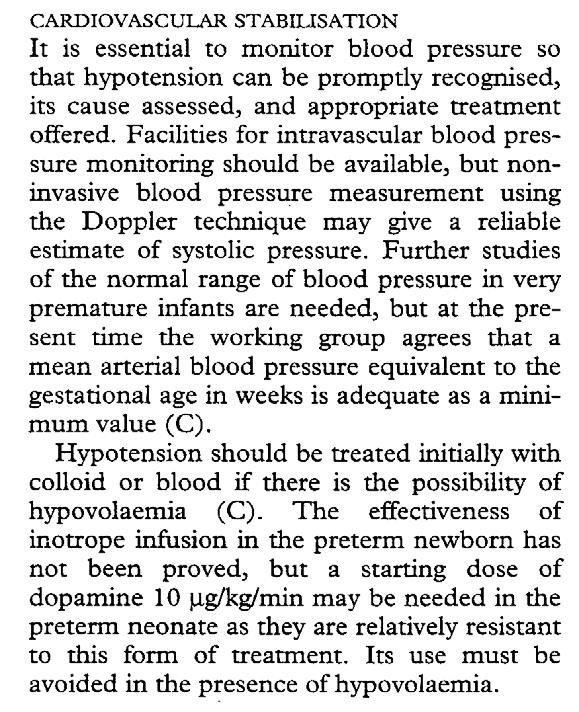
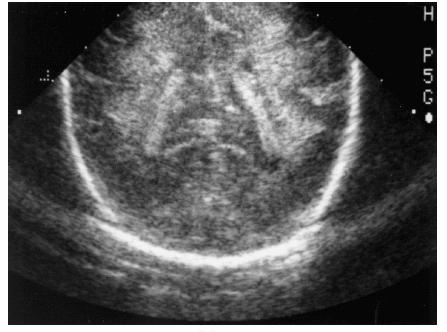
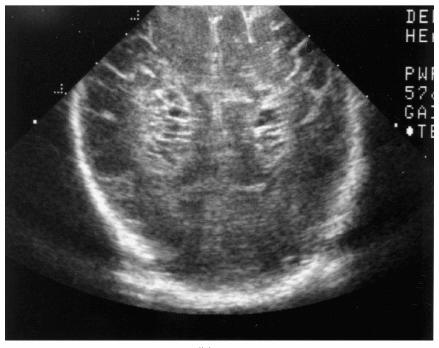
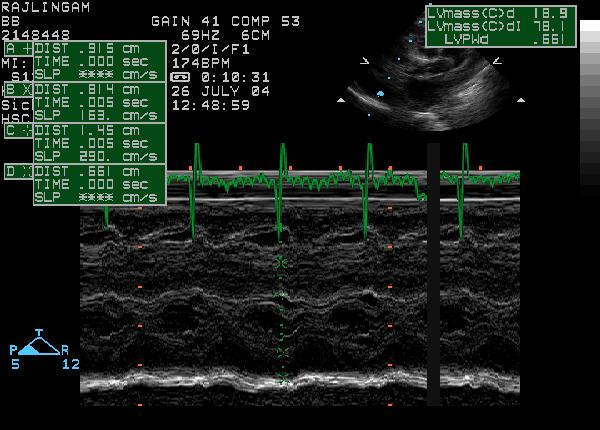
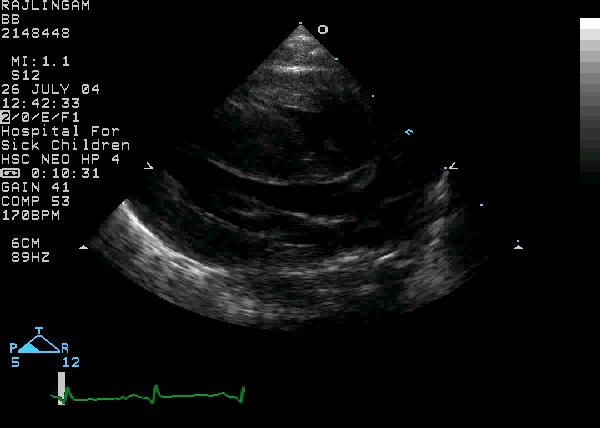
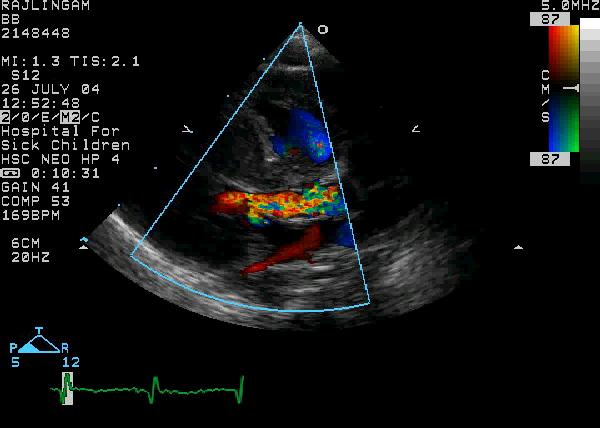
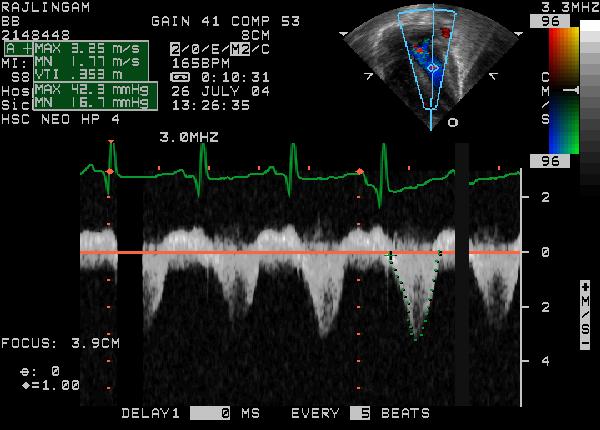
29 Functional USS heart mm HSDA - Left heart volume loading, - SVC flow - absent diastolic flow in superior mesenteric artery & middle cerebral artery

30 Surfactant Hypocapnia Oxygen or Nitric oxide Hypocapnia / Alkalosis Pressors Oxygen Hypothermia PVR +++ PDA Ao SVR Ao Left Ventricle
31 Dopamine Dobutamine Sympathetic amine (Most commonly used agent) Mixed β-1 & α-effects depending on dose Inotropic & afterload increase effects Improved LV performance at low dose (< 2.5 µg/kg/min) Padbury 1986 J Pediatr Synthetic analogue of dopamine Predominant β-1 effect, minimal α-effects Inotropic & afterload reduction effects Theoretical pulmonary vasodilator properties
32 Dopamine and Afterload Group 1 Dopamine 8 µg/kg/min Group 2 Dopamine 6 µg/kg/min Zhang 1999 Arch Dis Child
33 Circulatory instability & PDA Minimize oxygen exposure (SpO2 > 85%) Permissive acidemia ph > 7.25 Permissive hypercapnemia pco mmhg Increase PEEP Avoid excessive fluid restriction compromises end-organ flow Avoid pressor agents to support the myocardium
34 Scenario II Fullterm male, BWgt 4.6 Kg, Low Apgars, Cord ph 6.9, Bxs Mother Glycosuric, Meconium Staining at birth Evaluation at Referral Hospital SpO 2 85%/68% FiO HR 180 / min BP 55/25 (35) Soft ESM 2/6 localized to LLSE Pulses weak Ventilation: 28 / 3, 70 /min ABG: ph7.1, pco2 65, po2 46, BXS Lac 5.6 Cardiovascular Support Crystalloid (20 mls /kg) Cardiotropic Agents (dopamine 15 mcg/kg/min) BP 55/42 (46), HR 192, Anuric ABG: ph 6.8, pco2 65, pao2 45, Bxs -23 Lac 12.4
35 Refractory Hypotension Adrenal insufficiency - steroids Congenital heart disease duct dependant systemic blood flow lesion (e.g. HLHS, coarctation) PGE1 Hypertrophic cardiomyopathy -Preload Tamponade (excessive ventilation, pericardial or pleural effusion, pneumothorax) - Drain
36
37 Progression Inotropes weaned to off PgE1 infusion commenced to support cardiac output Volume resuscitation & Vasopressin ph & Lactates normalized


38 Caution with Cardiotropic agents Tachycardia Increased myocardial oxygen consumption Compliance impaired & diastolic filling Afterload

39 Epinephrine and Outcomes n=91 Campbell 2004 J Perin

40 Catecholamine induced myocardial damage Caspi J Pediatr Res 1994; 36:49-54 Caspi J et al. Circulation 1991; 84:III-394
41 VASOPRESSIN V1 Phospholipid complex mediated Ca ++ release V1 ino release Systemic Vasoconstriction Pulmonary vasodilation AoDP RA preload LA preload Improved Oxygenation CPP LV performance Improved LV output RV performance
42 Is Vasopressin superior to epinephrine in a neonatal model of asphyxial cardiac arrest?
43 Methods: Study Design Model: Neonatal Porcine model of Asphyxial Cardiac arrest Standardized Resuscitation: Single resuscitator performing chest compressions Compression to ventilation rate of 5:1 Intervention: Placebo controlled randomized control trial of single dose Vasopressin vs Epinephrine Block randomization Resuscitation medications prepared in standardized solution to ensure a consistent dose of 0.1 mls/kg administered
44 Interventions Placebo (0.9% saline) Low-dose epinephrine (LDE) mg/kg High-dose epinephrine (HDE) mg/kg Low-dose vasopressin (LDV) U/kg
45 Survival rate (%) 120 # 100 # 80 % Control LDE HDE LDV HDV Improved survival with high-dose Vasopressin, p=0.01 ANOVA
46 SVC Flow SVC flow index SVC flow index p<0.001, 2 rm ANOVA Control LDE HDE p<0.001, 2 rm ANOVA Control HDE LDV HDV mls/min/kg 150 mls/min/kg # # 50 # Time [mins] Time [mins] # p < 0.05 vs baseline p< LDE # p < 0.05 vs HDV Sustained fall in SVC flow greater in HDE animals [vs LDE, Control, and HDV (p< rm ANOVA)]
47 Pulmonary Hemodynamics PAAT:RVETinv RV index 10 8 # Control LDE HDE LDV HDV p<0.001, 2 rm ANOVA 500 Control LDE HDE LDV 400 HDV ratio 6 mls/min/kg # # # # # Time [mins] Time [mins] Decrease in RVI in LDE and HDE groups
48 Summary Improved survival with High-dose Vasopressin when compared to standard dose epinephrine Epinephrine associated with increased need for defibrillation, and greater impairment in myocardial performance or systemic blood flow Vasopressin associated with improved diastolic performance Role of vasopressin and defibrillation in neonatal arrest need prospective evaluation

49 Steroids and the Neonatal Heart The Quick Fix! Fix the BP but MASK a low cardiac output state
50 Seri 2001 Pediatrics
51 Steroids & Cardiovascular status Genomic Effects (hrs) Up-regulation of receptors and signaling pathways Non-Genomic Effects (hrs) Hormone substitution effect Inhibit catecholamine metabolism Release of vasoactive factors Vascular Integrity Increase intracellular calcium bioavailability
52 Myocardial Consequences of Steroids Hypertrophic Cardiomyopathy Hypertension Werner 1992 Ped Res Benediktsson 1993 Lancet Myocardial Dysfunction Dodic 2001 Circ Res Predisposition to arrhythmmias Kauffmann 1994 Ped Res
53 Approach to the Hypotensive Infant Caution when treating numerical hypotension Is there evidence of suboptimal tissue oxygenation and a low-perfusion states Choose your intervention based on the nature of the problem & REASSESS Is the problem preload, afterload or myocardial dysfunction Is their evidence of a HSDA (NSAIDs) Is their evidence of CHD (require Pgs) Early TnECHO may facilitate refinement of the decision making and assessing response
54 Mean BP < GA LCOS? yes no SBP DBP Observe Inodilator e.g. dobutamine Volume MAP Pressors Steroids
55 Mean BP > GA LCOS? yes no Inodilator e.g. dobutamine Observe
56 TnECHO: Hypotensive or LCOS (DA closed, No PPHN) Low LVO < 170 mls/min/kg Normal LVO mls/min/kg High LVO > 350 mls/min/kg Low Preload -Collapsing IVC -LVEDD <3rd -Low E ± A wave V max LV contractility -FS < 25% or -EF < 40% Normal Preload & Normal (FS 25-50%) or (FS>50%) Contractility VOLUME -Fluid bolus VENTILATION --Reduce MAP VASOPRESSIN CARDIOTROPE -Dobutamine or milrinone (Normal DAP or High ESWS) -Epinephrine or Dopamine (Low DAP) VASOPRESSOR -Epinephrine or Dopamine (Low DAP) Re-evaluate
57 Medicine is not only a science; it is also an art. It does not consist of compounding pills and plasters; it deals with the very processes of life, which must be understood before they may be guided. Philipus A. Paracelcus German Physician and Chemist
58 QUESTIONS
59
60
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
MANAGEMENT OF CIRCULATORY FAILURE
 MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
PDA LIGATION Management. Physiology Meets Clinical Care?? Patrick J McNamara Associate Professor of Pediatrics Hospital for Sick Children, Toronto
 PDA LIGATION Management. Physiology Meets Clinical Care?? Patrick J McNamara Associate Professor of Pediatrics Hospital for Sick Children, Toronto Mistaken Beliefs FLAT DISK COSMOGRAPHY and EARTH CENTRALITY-
PDA LIGATION Management. Physiology Meets Clinical Care?? Patrick J McNamara Associate Professor of Pediatrics Hospital for Sick Children, Toronto Mistaken Beliefs FLAT DISK COSMOGRAPHY and EARTH CENTRALITY-
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation?
 can help prevent Postoperative Cardiorespiratory instability following PDA ligation?") Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Enhancing Management of Circulatory Instability in Neonates
 Associate Scientist Enhancing Management of Circulatory Instability in Neonates Patrick McNamara Associate Professor of Pediatrics The Vulnerable Neonate How will you ensure cardiovascular stability? Myths
Associate Scientist Enhancing Management of Circulatory Instability in Neonates Patrick McNamara Associate Professor of Pediatrics The Vulnerable Neonate How will you ensure cardiovascular stability? Myths
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6 Supercedes: N/A 1.0 PURPOSE and INTENT
NEONATAL CLINICAL PRACTICE GUIDELINE Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6 Supercedes: N/A 1.0 PURPOSE and INTENT
Hypotension in the Neonate
 Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
1
 1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
9/16/2012. Progression of Shock. Blood pressure: Pathophysiology & Clinical Management
 Mean BP (mm Hg) 9/16/212 September 2, 14: 6 min Blood pressure: Pathophysiology & Clinical Management Shahab Noori, MD Associate Professor of Pediatrics Division of Neonatology Progression of Shock BP
Mean BP (mm Hg) 9/16/212 September 2, 14: 6 min Blood pressure: Pathophysiology & Clinical Management Shahab Noori, MD Associate Professor of Pediatrics Division of Neonatology Progression of Shock BP
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014
 USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Extracorporeal Membrane Oxygenation (ECMO) Referrals
 Referrals") Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
Neonatal Shock. Imbalance between tissue oxygen delivery and oxygen consumption
 Neonatal Shock Moira Crowley, MD Assistant Professor, Pediatrics Co-director, Neonatal ECMO Program Rainbow Babies and Children s Hospital Case Western Resverve University School of Medicine 1 Objectives
Neonatal Shock Moira Crowley, MD Assistant Professor, Pediatrics Co-director, Neonatal ECMO Program Rainbow Babies and Children s Hospital Case Western Resverve University School of Medicine 1 Objectives
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
I intend to discuss an unapproved/investigative use of a commercial product/device in my presentation
 Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
I have no relevant financial relationships with the manufacturers of any. commercial products and/or provider of commercial services discussed in
 I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this activity I do intend to discuss an unapproved/investigative
I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this activity I do intend to discuss an unapproved/investigative
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H
 HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
PERSISTENT PULMONARY HYPERTENSION OF THE NEWBORN East Bay Newborn Specialists Guideline Prepared by L Truong 12/15/2015
 PERSISTENT PULMONARY HYPERTENSION OF THE NEWBORN East Bay Newborn Specialists Guideline Prepared by L Truong 12/15/2015 Background: Persistent pulmonary hypertension of the newborn occurs in ~2 per 1,000
PERSISTENT PULMONARY HYPERTENSION OF THE NEWBORN East Bay Newborn Specialists Guideline Prepared by L Truong 12/15/2015 Background: Persistent pulmonary hypertension of the newborn occurs in ~2 per 1,000
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Valutazione del neonato con sospetta ipertensione polmonare
 Valutazione del neonato con sospetta ipertensione polmonare Cardiologia Pediatrica Seconda Università degli Studi di Napoli A.O. R.N. dei Colli-Monaldi Napoli Hypoxiemic infant Full or near-term neonate
Valutazione del neonato con sospetta ipertensione polmonare Cardiologia Pediatrica Seconda Università degli Studi di Napoli A.O. R.N. dei Colli-Monaldi Napoli Hypoxiemic infant Full or near-term neonate
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
PPHN (see also ECMO guideline)
") Children s Acute Transport Service Clinical Guidelines PPHN (see also ECMO guideline) Document Control Information Author P Brooke E.Randle Author Position Medical Student Consultant Document Owner E.
Children s Acute Transport Service Clinical Guidelines PPHN (see also ECMO guideline) Document Control Information Author P Brooke E.Randle Author Position Medical Student Consultant Document Owner E.
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato. Win Tin The James Cook University Hospital University of Durham
 Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato Win Tin The James Cook University Hospital University of Durham Introduction Fluid Bolus/es (Intravascular Volume Expansion) - One of the
Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato Win Tin The James Cook University Hospital University of Durham Introduction Fluid Bolus/es (Intravascular Volume Expansion) - One of the
9/13/2015. Laboratory. HPI and PE
 Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Pediatric Septic Shock. Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee
 Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Pharmacology of inotropes and vasopressors
 Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Weeks 1-3:Cardiovascular
 Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Integrated Evaluation of Neonatal Hemodynamics (IENH) and Targeted Echocardiogram Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC &
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Integrated Evaluation of Neonatal Hemodynamics (IENH) and Targeted Echocardiogram Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC &
When Fluids are Not Enough: Inopressor Therapy
 When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
Ventriculo-arterial coupling and diastolic elastance. MasterclassIC Schiermonnikoog 2015
 Ventriculo-arterial coupling and diastolic elastance MasterclassIC Schiermonnikoog 2015 Ventriculo-arterial coupling Dynamic interaction between heart and systemic circulation (modulation of compliance
Ventriculo-arterial coupling and diastolic elastance MasterclassIC Schiermonnikoog 2015 Ventriculo-arterial coupling Dynamic interaction between heart and systemic circulation (modulation of compliance
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
ino in neonates with cardiac disorders
 ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
Haemodynamic Support. (getting the blood to go round and round) philippelefevre.com
 philippelefevre.com") Haemodynamic Support (getting the blood to go round and round) philippelefevre.com Haemodynamic Support Whats wrong with your patient? What can we do about it? Volume expansion Inotropes, Chronotropes
Haemodynamic Support (getting the blood to go round and round) philippelefevre.com Haemodynamic Support Whats wrong with your patient? What can we do about it? Volume expansion Inotropes, Chronotropes
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Shock Management. Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate. PDF created with pdffactory Pro trial version
 Shock Management Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate Definition of Shock The definition of shock does not involve low blood pressure, rapid pulse or cool clammy skin - these
Shock Management Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate Definition of Shock The definition of shock does not involve low blood pressure, rapid pulse or cool clammy skin - these
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS
 Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
 100 100 100 100 100 200 200 200 200 200 300 300 300 300 300 400 400 400 400 400 500 500 500 500 500 Interpret this ECG Include rhythm, STEMI-location, Axis deviation, BBB, hypertrophy. What interventions
100 100 100 100 100 200 200 200 200 200 300 300 300 300 300 400 400 400 400 400 500 500 500 500 500 Interpret this ECG Include rhythm, STEMI-location, Axis deviation, BBB, hypertrophy. What interventions
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Stabilization and Transportation guidelines for Neonates and infants with Heart disease:
 Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations. Eric M. Graham, MD
 Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
SHOCK. May 12, 2011 Body and Disease
 SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University
 Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Perioperative Management of TAPVC
 Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Low Cardiac Output in the Pediatric Patient
 Low Cardiac Output in the Pediatric Patient Jeffrey Burns, M.D., M.P.H. Chief, Division of Critical Care Medicine Children s Hospital Boston Associate Professor of Anesthesia and Pediatrics Harvard Medical
Low Cardiac Output in the Pediatric Patient Jeffrey Burns, M.D., M.P.H. Chief, Division of Critical Care Medicine Children s Hospital Boston Associate Professor of Anesthesia and Pediatrics Harvard Medical
Declaring Brain Death. Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
 Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Agenda เอกราช อร ยะช ยพาณ ชย. - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure 9/6/2016
 6 September 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Agenda - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure http://fullpulse.weebly.com/conversation
6 September 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Agenda - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure http://fullpulse.weebly.com/conversation
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical
 Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical City Children s Hospital, Dallas Hypoxia Shortage of
Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical City Children s Hospital, Dallas Hypoxia Shortage of
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
PHARMACOLOGICAL MANAGEMENT OF CARDIOGENIC SHOCK
 PHARMACOLOGICAL MANAGEMENT OF CARDIOGENIC SHOCK Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion University of the Negev, Beer Sheva,
PHARMACOLOGICAL MANAGEMENT OF CARDIOGENIC SHOCK Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion University of the Negev, Beer Sheva,
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
The ABC of CAB- Circulation, Airway, Breathing: PALS/Resuscitation Update
 The ABC of CAB- Circulation, Airway, Breathing: PALS/Resuscitation Update Jennifer K. Lee, MD Johns Hopkins University Dept. of Anesthesia, Division of Pediatric Anesthesia Disclosures I have research
The ABC of CAB- Circulation, Airway, Breathing: PALS/Resuscitation Update Jennifer K. Lee, MD Johns Hopkins University Dept. of Anesthesia, Division of Pediatric Anesthesia Disclosures I have research
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Useful diagnostic measures: chest x ray to check pulmonary edema, ECG and ECHO to detect cardiac abnormalities (1).
.") Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Impedance Cardiography (ICG) Method, Technology and Validity
 Method, Technology and Validity") Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
NCC Review Cardiac 8/22/12. Intrauterine Blood Flow. Topics
 NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic
NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic