AVR with Sutureless Valves State of the Art
|
|
|
- Suzan Warren
- 5 years ago
- Views:
Transcription


1 AVR with Sutureless Valves State of the Art T. Fischlein Department of Cardiac Surgery, Cardiovascular Center Klinikum Nürnberg Paracelsus Medical University Nuremberg, Germany

2 Disclosures Consultant and Proctor for LivaNova Consultant and Proctor for BioStable



3 Features & Benefits Sutureless (Perceval) UNIQUE COLLAPSIBLE DESIGN Thanks to dedicated accessories, the valve diameter can be reduced prior to implantation, increasing visibility. PRECISE POSITIONING Three guiding sutures are used to position the valve in the aortic root. Thanks to this and to the enhanced visibility, precise positioning becomes easier and reproducible. TRULY UNIQUE SUTURELESS VALVE Self-expands in place (no need to knot sutures), reducing operation time and trauma.

 Positioning the valve in a precise, safe,")

4 Perceval advantages thanks to the Collapsibility feature The unique Perceval properties allow to: Reduce the trauma of the operation (smaller incisions, fast and easy positioning, no sutures, reduced ischemic time for the patient, reduced aortic root manipulation) Positioning the valve in a precise, safe, reproducible and controlled way Improving visualization and facilitate even MICS procedures, REDO cases, implantation in small annuli, calcified annuli, obese patients 4


5 Indications & Contraindications (Sutureless) Patients sensitive to cross clamp time Patients with Multiple Risk factors Diabetic patients Patients with low EF AVR + CABGs Old patients WHO CAN BENEFIT THE MOST FROM PERCEVAL? Technically Challenging procedures or at risk of PPM Re-Do Small annuli Calcified aortic roots Obese Patients Patients who need a less traumatic Procedure Patients who need a faster recovery
6 Sutureless Consensus paper key recommendations from an international panel Key recommendations regarding PATIENTS INDICATIONS: Sutureless = alternative to stented valves in patients requiring biological aortic valve replacement Sutureless can be more beneficial in challenging cases redo cases delicate aortic wall conditions as calcified root, prior implantation of aortic homograft or stentless Sutureless valves are the first choice in case of concomitant procedures (including multiple valves) or small annulus to reduce XCT
7 Key Recommendations Sutureless when? Use of sutureless and rapid deployment valves together with minimally invasive approaches in patients requiring biological valve replacement and not serving as candidates for TAVI Use of sutureless and rapid deployment valves are recommend in order to reduce extracorporeal circulation and aortic cross-clamp time Oversizing with sutureless valves is not beneficial and can have negative impact Use of sutureless and rapid deployment valves will lead to a higher adoption rate of minimally invasive approaches in aortic valve replacement Take respect to necessary, brief learning curves for both sutureless and minimally invasive programs 7
8 Indications & Contraindications WHAT ARE THE MAIN CONTRAINDICATIONS - Sutureless Aneurysmal dilation or dissection of the ascending aortic wall Congenital bicuspid aortic valve (Sievers 0) Anatomical characteristics indicating an enlargement of aortic root (e.g. if the ratio of the sinotubular junction Ø and the annulus Ø is larger than 1.3) Endocarditis?
9 Reported PM Implantation Valve Traditional sutured Pacemaker rate (Early) 3.0%-11.8% Mean:7.0%, Author Matthews et al 2011[2] The incidence of PPM implantation following traditional AVR reported in literature can vary from 3.0% to 11.8% (mean 7.0%) [2]. Traditional sutured (Partner II intermediate risk population) 6.9% Leon et al [3] All the risk factors shown in the previous slide may contribute to the variability among centers [3]. Perceval (cavalier trial) 11.8% (Overall) Data on file Perceval (cavalier trial) 9.6% (as a result of AV block III) Fischlein et al 2015 [4] Sutureless, Rapid deployment valves have shown, on average, a slightly higher PM rate compared to traditional valves. Perceval Intuity (Transform) 6 % (as a result of AV block III in patients with no preop cond disorders) 14 % (overall) 11.9% (isolated only) Shrestha et al [5] Barnhart et al 2016 [6] 9


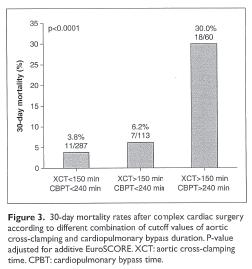
10 Indications (Sutureless) Patients undergoing combined procedures with CABG Published Experience 243 patients with combined procedures Shortening the aortic clamp time and ECC time may help to reduce mortality and morbidity during concomitant procedures Perceval Sutureless proved to be an excellent solution for patients requiring concomitant procedures


11 Indications Patients with small annuli Published Experience



12 Indications Patients with calcified aortic roots Published Experience Elderly Patients: - Lower operative mortality - Lower incidence of sepsis - Lower wound complications - Shorter hospital stay - Faster rehabilitation and discharge

13 Minimal invasive AVR - Right anterior Minithoracotomy (RAT)



14 Redo-OP: after CABG e.g. for AVR Re-op Patients: J Thorac Dis Nov;5(Suppl 6):S669-S672 - Less bleeding - Fewer transfusions Less trauma







15 Perceval is retrievable Stent features and properties PERCEVAL Edwards Intuity Elite Valve retrieval Perceval can be easily retrieved. Perceval retrieval has shown to be feasible and safe for the patient without damaging the aortic root. In case of malpositioning Intuity can be difficult to remove. 15

16 Complications, Management - Repositioning X Movement in a Redo AVR Case
 is the")

17 Sutureless (Perceval) is the MICS enabler Mini-sternotomy Right Anterior Thoracotomy
, 3 rd or 4 th ICS right")
, 2 nd or 3 rd ICS")
18 - Full Sternotomy (Standard) - Mini Sternotomy (Upper Sternotomy), 3 rd or 4 th ICS right (J-Sternotomy) or left or transverse - Right anterior Mini Thoracotomy (RAT), 2 nd or 3 rd ICS Mini Sternotomy RAT
19




20 MIS with conventional aortic valves PROs Reduced Surgical Trauma Decreased Blood Loss Lower Mortality Lower Analgesic Lower ICU Stay Reduced Intubation Time Faster Recovery Less Pain Better Cosmetic Results CONs Technically More Complex Higher Learning Curve Higher X-Clamp Time Higher ECC Time



21 Indications & Contraindications: Published Experience




 Improving clinical outcome AKE")
22 The Sutureless Solution The concept of a sutureless prosthesis has been developed with the aim of: simplifying the surgical technique reducing the implantation time Resektion der AK Taschen, Entkalkung facilitates MICS procedures enables concomitant procedures providing a curative solution, removing the native diseased aortic valve (in contrast to TAVI) Improving clinical outcome Resektion der AK Taschen, Entkalkung AKE
23 Undisputed reduction of XCT in all comparative studies Sutureless (Perceval) vs traditional valves Average XCT saving of 40% (=29 minutes, min 14 max 49) Comparative studies Perceval vs conventional AVR D Onofrio 2013 Dalen 2015 Gilmanov 2014 approach Perceval approach: Full sternotomy, hemisternotomy, RAT vs traditional valve in full sternotomy Perceval in MICS vs Perimount in full sternotomy Isolated/ RAT XCT Perceval XCT trad valves P value Time saving < % < % < % Muneretto 2015 Isolated/all approaches = % Santarpino 2013 Isolated/MICS < % Cross Clamp time savings (%) Shrestha 2013 Perceval in MICS 72% vs conventional in MICS 4.3% < % 23
 2.")


24 Perceval and Stented valves: a propensity-matched score analysis Traditional Sutured Perceval ICU stay (Days) 2.8 Transfusion (Blood units) 2.5 Ventilation (Hours) Source: Better Short-Term Outcome by Using Sutureless Valves: A Propensity-Matched Score Analysis Pollari et al., Ann Thorac. Surgery 2014 Aug;98 (2): 611-6
25


26 Perceval Sutureless Valve Haemodynamic Performance Perceval shows excellent hemodynamic performance with stable gradients over time, which has been reported in various publications The results of the largest cohort can be found in the paper European multicentre experience with the sutureless Perceval valve: clinical and haemodynamic outcomes up to 5 years in over 700 patients Shrestha et al. Eur J Cardiothorac Surg Mar 6. 26
27
.")

28 Perceval vs. TAVI More Cost Effective in Gray Zone Patients The costs associated to the 2 procedures are similar when the cost of the device was excluded (p = 0.217). When included, the sutureless approach resulted a cost saving ( 22,451 vs 33,877, p <0.001). In conclusion, the patients in the gray zone record a satisfying clinical outcome after sutureless surgery and TAVI. Patients in the sutureless group endure more hospital complications, but TAVI entails a higher follow-up mortality. On the costs aspects, TAVI technologies are more expensive, and it reflects on higher overall hospital costs. Clinical Outcome and Cost Analysis of Sutureless Versus Transcatheter Aortic Valve Implantation With Propensity Score Matching Analysis Santarpino et al The American Journal of Cardiology, 2015


29 Perceval vs TAVI Clinical Outcome and Cost Analysis of Sutureless Versus Transcatheter Aortic Valve Implantation With Propensity Score Matching Analysis Santarpino et al The American Journal of Cardiology, 2015




30 Sutureless vs. TAVI Sutureless vs TAVI with para-valvular insufficiency Sutureless vs TAVI without para-valvular insufficiency PVL after TAVI Months Clinical Outcome and Cost Analysis of Sutureless Versus Transcatheter Aortic Valve Implantation With Propensity Score Matching Analysis Santarpino et al; The American Journal of Cardiology, 2015



31 Perceval vs TAVR vs Stented valves a propensity-matched score analysis Propensity matched study: 204 vs 204 vs 204 patients Outcomes: Perceval showed lower rates than TAVR and savr of postop complications at 30 days Perceval showed higher survival rates and freedom from MACCE at 24 months

32 Summary Sutureless allows: Time reduction shorter cross-clamp, CPB and operation time Better outcome shorter intubation time, ICU and hospital stay; less need of transfusions; even in combination with minimal invasive access surgery Cost reduction proven throughout different experiences As a consequence of this positive economic profile and the relevant increased use of the sutureless technology, some insurances have granted additional and more favorable reimbursement levels to sutureless prostheses compared to traditional valves Are we still going to implant traditional tissue valves in the future?



33 PERceval Sutureless Implant Vs STandard - Aortic Valve Replacement First Randomized trial to compare Perceval and standard AVR CT-Scan for surgical planning Low to medium risk patients High number of Mini-sternotomy approach Results will have an impact not only on Perceval but also on standard AVR and could influence future guidelines First large Randomized Trial in Valve Surgery in the last 30 years 33
34 Advantages of Sutureless Prostheses AVR with Sutureless Prostheses Is safe, fast and easy, requiring a short learning curve Shows excellent outcome and patient satisfaction Has the potential to shorten aortic XCT significantly Perceval: Results show advantages for: Small aortic roots Calcified roots Redo and Combined Procedures (AVR+ CABG, septal myectomy, Afib)
35 Conclusions AVR with Sutureless Valves Sutureless aortic valve replacement: A valuable option to reduce trauma of operation in everyday surgery and facilitates fast recovery Is a major step forward for MIC - AVR A cost saving solution, which helps reducing hospital resource consumption (reduced ICU and Hospital stay) Closes the gap between conventional and catheter based (TAVI) aortic valve implantation Sutureless technology = future for AVR


36 Thank you!

37 Cardiac Surgery vs. Cardiology Minimal invasive WHY? David vs. Goliath Small Society AVR Conventional with CPB, Big sternotomy Offer patients: Minimal invasive new technologies; Have to change attitude, Improve results and Increase our power Big Society AVR TAVI Real minimal invasive technique, Beating heart, Offer patients: Small puncture in the groin or full sternotomy Gate Keeper
 transfemorally deployed in a Perceval size S. Durand et al. Canadian Journal of Cardiology, 2015 2. Sapien XT (23 mm) transfemorally deployed in a Perceval size M. Di Eusanio et al.")

38 VIV in Perceval Sutureless Valve The ViV procedure with Perceval is feasible and some published experiences report successful results with SapienXT, CoreValve and Evolut-R: 1. Sapien 3 (23mm) transfemorally deployed in a Perceval size S. Durand et al. Canadian Journal of Cardiology, Sapien XT (23 mm) transfemorally deployed in a Perceval size M. Di Eusanio et al.- Ann Cardiothorac Surg CoreValve transfemorally deployed in a Perceval. Bullesfeld et al. Presented at LondonPCR 2014 as live case 4. Sapien XT (23mm) transapically deployed in a. Fujitaa B. et al.- Interactive CardioVascular and Thoracic Surgery Corevalve and Evolute-R deployed in Perceval. Amabile et al. - The Journal of Thoracic and Cardiovascular Surgery 2016 Perceval Hemodynamics OUS IM A 38
 Cardiac Surgery - Klinikum")
39 Aortic Valve Replacement Sutureless (Perveval) Cardiac Surgery - Klinikum Nürnberg
TAVI Versus Suturless Valve In Intermediate Risk Patients
 TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic,
 Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic, transplantation and Vascular Surgery Hannover Medical School, Germany
Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic, transplantation and Vascular Surgery Hannover Medical School, Germany
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
REDUCING THE IMPACT OF SURGERY AND FACILITATING FASTER RECOVERY
 REDUCING THE IMPACT OF SURGERY AND FACILITATING FASTER RECOVERY AORTIC SOLUTIONS PERCEVAL VALVE PERCEVAL THE BIOLOGICAL VALVE OF CHOICE IN AVR 0914 RE0210195/A AORTIC SOLUTIONS PERCEVAL THE BIOLOGICAL
REDUCING THE IMPACT OF SURGERY AND FACILITATING FASTER RECOVERY AORTIC SOLUTIONS PERCEVAL VALVE PERCEVAL THE BIOLOGICAL VALVE OF CHOICE IN AVR 0914 RE0210195/A AORTIC SOLUTIONS PERCEVAL THE BIOLOGICAL
National Institute for Health and Care Excellence IP865/2 Sutureless Aortic Valve Replacement for aortic stenosis
 National Institute for Health and Care Excellence IP865/2 Sutureless Aortic Valve Replacement for aortic stenosis IPAC 14/06/18: 1 1 NHS professional 2 1 NHS professional ments 1.1 1.1 Current evidence
National Institute for Health and Care Excellence IP865/2 Sutureless Aortic Valve Replacement for aortic stenosis IPAC 14/06/18: 1 1 NHS professional 2 1 NHS professional ments 1.1 1.1 Current evidence
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
MINIMALLY INVASIVE AVR
 MINIMALLY INVASIVE AVR MATTHEW S. PANAGIOTOU MD FETCS CARDIAC SURGEON MEDITERRANEAO HOSPITAL MINIMALLY INVASIVE AVR In cardiac surgery Minimally invasive has been defined as a small chest incision that
MINIMALLY INVASIVE AVR MATTHEW S. PANAGIOTOU MD FETCS CARDIAC SURGEON MEDITERRANEAO HOSPITAL MINIMALLY INVASIVE AVR In cardiac surgery Minimally invasive has been defined as a small chest incision that
Minimally invasive aortic valve surgery: new solutions to old problems.
 SCDU DI CARDIOCHIRURGIA Università degli Studi di Torino Ospedale S. Giovanni Battista Direttore: Prof. Mauro Rinaldi Minimally invasive aortic valve surgery: new solutions to old problems. Prof. Mauro
SCDU DI CARDIOCHIRURGIA Università degli Studi di Torino Ospedale S. Giovanni Battista Direttore: Prof. Mauro Rinaldi Minimally invasive aortic valve surgery: new solutions to old problems. Prof. Mauro
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
TAVR for low-risk patients in 2017: not so fast.
 TAVR for low-risk patients in 2017: not so fast. Enrico Ferrari, MD, FETCS Cardiac Surgery Department Cardiocentro Ticino Foundation Lugano, Switzerland Conflicts of Interest Consultant and proctor for
TAVR for low-risk patients in 2017: not so fast. Enrico Ferrari, MD, FETCS Cardiac Surgery Department Cardiocentro Ticino Foundation Lugano, Switzerland Conflicts of Interest Consultant and proctor for
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital,
 Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
TAVR for Valve-In-Valve. Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology
 TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Β. Κόλλιας, Σ. Ματιάτου, Δ. Αγγουράς.
 Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Οι βιοπροσθετικές αορτικές βαλβίδες ταχείας έκπτυξης στην αντιµετώπιση της σοβαρής αορτικής
Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Οι βιοπροσθετικές αορτικές βαλβίδες ταχείας έκπτυξης στην αντιµετώπιση της σοβαρής αορτικής
Re-do aortic valve replacement after previous homograft aortic root replacement
 Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
Dr Nikolaos Baikoussis
 Dr Nikolaos Baikoussis Cardiac Surgeon Evangelismos General Hospital of Athens, Greece STS database: any procedure not performed with a full sternotomy (FS) and cardiopulmonary bypass (CPB)..(TAVI) Schmitto
Dr Nikolaos Baikoussis Cardiac Surgeon Evangelismos General Hospital of Athens, Greece STS database: any procedure not performed with a full sternotomy (FS) and cardiopulmonary bypass (CPB)..(TAVI) Schmitto
Developments in Valve Surgery
 Developments in Valve Surgery Introduction Will discuss Aortic Valve and Mitral Valve surgery What is a mini valve operation? When do we do traditional valve surgery (SAVR, SMVR) vs. mini valve surgery
Developments in Valve Surgery Introduction Will discuss Aortic Valve and Mitral Valve surgery What is a mini valve operation? When do we do traditional valve surgery (SAVR, SMVR) vs. mini valve surgery
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
When Should We Consider TAVI. (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea
? Pyowon Park Samsung Medical Center Seoul, Korea") When Should We Consider TAVI Procedure in Korea (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea Aortic Stenosis in Korea Rapidly increasing valve disease in Korea Still low incidence
When Should We Consider TAVI Procedure in Korea (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea Aortic Stenosis in Korea Rapidly increasing valve disease in Korea Still low incidence
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Is it a business for the cardiac surgeon?
 TAVI FOR LOW RISK PATIENTS Is it a business for the cardiac surgeon? Augusto D Onofrio Gino Gerosa Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Italy T A V I Cardiac surgery
TAVI FOR LOW RISK PATIENTS Is it a business for the cardiac surgeon? Augusto D Onofrio Gino Gerosa Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Italy T A V I Cardiac surgery
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
CARDIOCHIRURGIA MINI-INVASIVA: INVASIVA: efficacia per il paziente efficienza per la sanita. Dott. Davide Ricci
 CARDIOCHIRURGIA MINI-INVASIVA: INVASIVA: efficacia per il paziente efficienza per la sanita Dott. Davide Ricci SC Cardiochirurgia U Universita degli Studi di Torino Minimally Invasive Surgical approaches
CARDIOCHIRURGIA MINI-INVASIVA: INVASIVA: efficacia per il paziente efficienza per la sanita Dott. Davide Ricci SC Cardiochirurgia U Universita degli Studi di Torino Minimally Invasive Surgical approaches
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update
 Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Minimally invasive aortic valve replacement in high risk patient groups
 Review Article Minimally invasive aortic valve replacement in high risk patient groups Daniel Fudulu, Harriet Lewis, Umberto Benedetto, Massimo Caputo, Gianni Angelini, Hunaid A. Vohra Department of Cardiac
Review Article Minimally invasive aortic valve replacement in high risk patient groups Daniel Fudulu, Harriet Lewis, Umberto Benedetto, Massimo Caputo, Gianni Angelini, Hunaid A. Vohra Department of Cardiac
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison
 Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D.
 Charles T. Klodell, M.D.") Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland
 Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Prof. Dr. Thomas Walther. TAVI in ascending aorta / aortic root dilatation
 Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
Are Heart Valve Referral Centers Feasible in Latin America?
 Are Heart Valve Referral Centers Feasible in Latin America? Vadim Kotowicz, MD Chief of Cardiovascular Surgery Department Italian Hospital of Buenos Aires Disclosure Medtronic inc. Consultanting Johnson
Are Heart Valve Referral Centers Feasible in Latin America? Vadim Kotowicz, MD Chief of Cardiovascular Surgery Department Italian Hospital of Buenos Aires Disclosure Medtronic inc. Consultanting Johnson
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
Thrombocytopenia in Moderate- to High-Risk Sutureless Aortic Valve Replacement
 Korean J Thorac Cardiovasc Surg 2018;51:172-179 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2018.51.3.172 Thrombocytopenia in Moderate- to High-Risk
Korean J Thorac Cardiovasc Surg 2018;51:172-179 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2018.51.3.172 Thrombocytopenia in Moderate- to High-Risk
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Aortic valve implantation using the femoral and apical access: a single center experience.
 Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Le TAVI pour tout le monde?
 Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
Aortic valve replacement with sutureless and rapid deployment aortic valve prostheses
 Symposium: Transcatheter aortic valve implantation Guest Editor: Prof. Khalil Fattouch Journal of Geriatric Cardiology (2016) 13: 504 510 2016 JGC All rights reserved; www.jgc301.com Open Access Aortic
Symposium: Transcatheter aortic valve implantation Guest Editor: Prof. Khalil Fattouch Journal of Geriatric Cardiology (2016) 13: 504 510 2016 JGC All rights reserved; www.jgc301.com Open Access Aortic
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
Less Invasive Aortic Valve Surgery
 Less Invasive Aortic Valve Surgery SCTS Brighton 19th March 2013 Andrew Chukwuemeka MD FRCS Consultant Cardiothoracic Surgeon Hammersmith Hospital Imperial College Healthcare NHS Trust Less Invasive Aortic
Less Invasive Aortic Valve Surgery SCTS Brighton 19th March 2013 Andrew Chukwuemeka MD FRCS Consultant Cardiothoracic Surgeon Hammersmith Hospital Imperial College Healthcare NHS Trust Less Invasive Aortic
The Future of Medicine. Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy
 The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR for Complex Aortic Valvular Conditions
 TAVR for Complex Aortic Valvular Conditions Wilson Y. Szeto, MD Professor of Surgery Chief, Cardiovascular Surgery at Penn Presbyterian Surgical Director, Transcatheter Cardio-Aortic Therapies Associate
TAVR for Complex Aortic Valvular Conditions Wilson Y. Szeto, MD Professor of Surgery Chief, Cardiovascular Surgery at Penn Presbyterian Surgical Director, Transcatheter Cardio-Aortic Therapies Associate
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
TAVI After PARTNER-2 : The Hamilton Approach
 TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
Aortic Stenosis: Background
 Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Aortic valve repair: When and how to employ this novel approach?
 Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR)
") Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
Results of Transapical Valves. A.P. Kappetein Dept Cardio-thoracic surgery
 Results of Transapical Valves A.P. Kappetein Dept Cardio-thoracic surgery Rotterda am, The Netherlands 2002 FIM 2003 2005 2006 2010 THV THV Cribier-Edwards Edwards Edwards Sapien Sapien XT Bovine pericardium
Results of Transapical Valves A.P. Kappetein Dept Cardio-thoracic surgery Rotterda am, The Netherlands 2002 FIM 2003 2005 2006 2010 THV THV Cribier-Edwards Edwards Edwards Sapien Sapien XT Bovine pericardium
TAVR SPRING 2017 The evolution of TAVR
 TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
Sutureless aortic valve replacement
 Keynote Lecture Series Sutureless aortic valve replacement Marco Di Eusanio 1,2, Kevin Phan 2 1 Department of Cardiac Surgery, Sant Orsola-Malpighi Hospital, University of Bologna, Bologna, Italy; 2 The
Keynote Lecture Series Sutureless aortic valve replacement Marco Di Eusanio 1,2, Kevin Phan 2 1 Department of Cardiac Surgery, Sant Orsola-Malpighi Hospital, University of Bologna, Bologna, Italy; 2 The
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
Current Evidence in TAVI patients using ACURATE and LOTUS valves
 Current Evidence in TAVI patients using ACURATE and LOTUS valves Giuseppe Tarantini, MD, PhD, FESC, Professor and Director of Interventional Cardiology University of Padua GISE President Potential conflicts
Current Evidence in TAVI patients using ACURATE and LOTUS valves Giuseppe Tarantini, MD, PhD, FESC, Professor and Director of Interventional Cardiology University of Padua GISE President Potential conflicts
Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel
 TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
Aortic Valve Replacement with a Conventional Stented Bioprosthesis versus Sutureless Bioprosthesis: a Study of 763 Patients
 ORIGINAL ARTICLE Aortic Valve Replacement with a Conventional Stented Bioprosthesis versus Sutureless Bioprosthesis: a Study of 763 Patients Syed Saleem Mujtaba 1, MD; Simon M. Ledingham 1, MD; Asif Raza
ORIGINAL ARTICLE Aortic Valve Replacement with a Conventional Stented Bioprosthesis versus Sutureless Bioprosthesis: a Study of 763 Patients Syed Saleem Mujtaba 1, MD; Simon M. Ledingham 1, MD; Asif Raza
Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques
 Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques Konstadinos A Plestis, MD System Chief of Cardiothoracic and Vascular
Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques Konstadinos A Plestis, MD System Chief of Cardiothoracic and Vascular
7 th Conference of Transcatheter Heart Valve Therapies
 7 th Conference of Transcatheter Heart Valve Therapies May 18-19, 2018, Athens Hilton Athens, Greece Course Directors Stratis Pattakos MD Konstantinos Spargias MD Panos Vardas MD Co-Directors Nick Bouboulis
7 th Conference of Transcatheter Heart Valve Therapies May 18-19, 2018, Athens Hilton Athens, Greece Course Directors Stratis Pattakos MD Konstantinos Spargias MD Panos Vardas MD Co-Directors Nick Bouboulis
2/28/2010. Speakers s name: Paul Chiam. I have the following potential conflicts of interest to report: NONE. Antegrade transvenous transseptal route
 Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Standard AVR. Full Sternotomy CPB
 16.03.2013 by Dr. M. D. Dixit MS (Gen. Surg.), DNB (CVTS), PhD Professor & HOD, CVTS Director, KLES Heart Foundation, KLES Dr. Prabhakar Kore Hospital & MRC, Belgaum Standard AVR Full Sternotomy CPB
16.03.2013 by Dr. M. D. Dixit MS (Gen. Surg.), DNB (CVTS), PhD Professor & HOD, CVTS Director, KLES Heart Foundation, KLES Dr. Prabhakar Kore Hospital & MRC, Belgaum Standard AVR Full Sternotomy CPB
The Cardiac Surgeon of the Future
 The Cardiac Surgeon of the Future Gorav Ailawadi, MD Chief, Section of Adult Cardiac Surgery Professor, Surgery & Biomedical Engineering Director, Minimally Invasive Cardiac Surgery July 19, 2017 Disclosures
The Cardiac Surgeon of the Future Gorav Ailawadi, MD Chief, Section of Adult Cardiac Surgery Professor, Surgery & Biomedical Engineering Director, Minimally Invasive Cardiac Surgery July 19, 2017 Disclosures
What is TAVR? Transcatheter Aortic Valve Replacement
 What is TAVR? Transcatheter Aortic Valve Replacement What Are Your Options for Treating Severe Aortic Stenosis? Treatment for aortic stenosis depends on how far your disease has progressed. If your stenosis
What is TAVR? Transcatheter Aortic Valve Replacement What Are Your Options for Treating Severe Aortic Stenosis? Treatment for aortic stenosis depends on how far your disease has progressed. If your stenosis
8. Nov, 2018 Athens Clossroad 2018, Athens GREEK
 8. Nov, 2018 Athens Clossroad 2018, Athens GREEK Stent Less Bio prosthesis Aortic Valve replacement with Minimally Invasive Approach ~ Indication for the 1 st Surgical Aortic Valve Treatment Considering
8. Nov, 2018 Athens Clossroad 2018, Athens GREEK Stent Less Bio prosthesis Aortic Valve replacement with Minimally Invasive Approach ~ Indication for the 1 st Surgical Aortic Valve Treatment Considering
Update on Percutaneous Therapies for Structural Heart Disease. William Thomas MD Director of Structural Heart Program Tucson Medical Center
 Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S.
 CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
Evolut R in bicuspid valve anatomies
 Evolut R in bicuspid valve anatomies U. Gerckens MD University of Rostock, Germany Potential conflicts of interest Speaker's name: Ulrich Gerckens I have the following potential conflicts of interest to
Evolut R in bicuspid valve anatomies U. Gerckens MD University of Rostock, Germany Potential conflicts of interest Speaker's name: Ulrich Gerckens I have the following potential conflicts of interest to
Transcatheter Valve Replacement: Current State in 2017
 Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Minimally invasive aortic valve surgery: state of the art and future directions
 Keynote Lecture Series Minimally invasive aortic valve surgery: state of the art and future directions Mattia Glauber, Matteo Ferrarini, Antonio Miceli Cardiac Surgery and Great Vessels Department, Istituto
Keynote Lecture Series Minimally invasive aortic valve surgery: state of the art and future directions Mattia Glauber, Matteo Ferrarini, Antonio Miceli Cardiac Surgery and Great Vessels Department, Istituto
Appropriate Use of TAVR - now and in the future. A Surgeon s Perspective. Neil Moat Royal Brompton Hospital, London, UK
 Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative
 Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Echo Assessment Pre-TAVI
 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE
 ESC Congress 2011 27 Aug - 31 Aug 2011, Paris - France CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE N.Russo, L.Compostella, T.Setzu, M.Napodano, L.Testolin,
ESC Congress 2011 27 Aug - 31 Aug 2011, Paris - France CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE N.Russo, L.Compostella, T.Setzu, M.Napodano, L.Testolin,
TAVI limitations for low risk patients
 TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
Transcatheter Aortic Valve Implantation Present Status and Perspectives
 Transcatheter Aortic Valve Implantation Present Status and Perspectives Angioplasty Summit TCTAP 2010 Alain Cribier, MD University of Rouen, France Transcatheter Aortic Valve Implantation has entered the
Transcatheter Aortic Valve Implantation Present Status and Perspectives Angioplasty Summit TCTAP 2010 Alain Cribier, MD University of Rouen, France Transcatheter Aortic Valve Implantation has entered the
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Alternate Vascular Access for TAVR. Gian Paolo Ussia Campus Bio-medico University, Rome Italy
 Alternate Vascular Access for TAVR Gian Paolo Ussia Campus Bio-medico University, Rome Italy g.ussia@unicampus.it REQUIRED Gian Paolo Ussia I have no relevant financial relationships Transcatheter Valves
Alternate Vascular Access for TAVR Gian Paolo Ussia Campus Bio-medico University, Rome Italy g.ussia@unicampus.it REQUIRED Gian Paolo Ussia I have no relevant financial relationships Transcatheter Valves
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Transcatheter procedures of the future; expanding the treatment options for patients with severe aortic stenosis
 Transcatheter procedures of the future; expanding the treatment options for patients with severe aortic stenosis John Webb MD Director interventional cardiology, St Paul s Hospital McLeod Professor of
Transcatheter procedures of the future; expanding the treatment options for patients with severe aortic stenosis John Webb MD Director interventional cardiology, St Paul s Hospital McLeod Professor of
UC Merced UC Merced Undergraduate Research Journal
 UC Merced UC Merced Undergraduate Research Journal Title TAVI: A Safe Alternative for Aortic Stenosis? Permalink https://escholarship.org/uc/item/5d01f0p3 Journal UC Merced Undergraduate Research Journal,
UC Merced UC Merced Undergraduate Research Journal Title TAVI: A Safe Alternative for Aortic Stenosis? Permalink https://escholarship.org/uc/item/5d01f0p3 Journal UC Merced Undergraduate Research Journal,
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients?
 Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS
 Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
TAVR: Intermediate Risk Patients
 TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
Surgical Mininvasive Approach for Mitral Repair Prof. Mauro Rinaldi
 Surgical Mininvasive Approach for Mitral Repair Prof. Mauro Rinaldi SC Cardiochirurgia U Universita degli Studi di Torino PORT-ACCESS TECNIQUE Reduce surgical trauma Minimize disruption of the chest wall
Surgical Mininvasive Approach for Mitral Repair Prof. Mauro Rinaldi SC Cardiochirurgia U Universita degli Studi di Torino PORT-ACCESS TECNIQUE Reduce surgical trauma Minimize disruption of the chest wall
Aortic Stenosis Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan
 Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Fast track surgery: the role of the surgeon Enrico Ferrari, MD University of Lausanne, Switzerland
 June 11 th 2015 Fast track surgery: the role of the surgeon Enrico Ferrari, MD University of Lausanne, Switzerland Fast track Is a process involving rapid progress from preoperative preparation through
June 11 th 2015 Fast track surgery: the role of the surgeon Enrico Ferrari, MD University of Lausanne, Switzerland Fast track Is a process involving rapid progress from preoperative preparation through
Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis
 Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis James Bartholomew McClurken, MD FACC, FCCP, FACS, FESC Professor & Vice-Chair of Surgery, Temple University Hosp.,
Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis James Bartholomew McClurken, MD FACC, FCCP, FACS, FESC Professor & Vice-Chair of Surgery, Temple University Hosp.,
David Dexter MD FACS Sentara Vascular Specialists Assistant Professor of Surgery EVMS. Peripheral Complications of TAVR
 David Dexter MD FACS Sentara Vascular Specialists Assistant Professor of Surgery EVMS Peripheral Complications of TAVR TAVR Complications Reported Complications Rates range from 8% to 15% Predictors of
David Dexter MD FACS Sentara Vascular Specialists Assistant Professor of Surgery EVMS Peripheral Complications of TAVR TAVR Complications Reported Complications Rates range from 8% to 15% Predictors of
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
TAVR Update: Open vs. Closed Future Directions
 TAVR Update: Open vs. Closed Future Directions Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Methodist DeBakey Heart & Vascular Center Disclosures Advisory Board Medtronic Consultant Medtronic
TAVR Update: Open vs. Closed Future Directions Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Methodist DeBakey Heart & Vascular Center Disclosures Advisory Board Medtronic Consultant Medtronic