Valvular Heart Disease and auscultation. Jay L. Rubenstone, D.O., F.A.C.C
|
|
|
- Valentine Blair
- 6 years ago
- Views:
Transcription
1 Valvular Heart Disease and auscultation Jay L. Rubenstone, D.O., F.A.C.C
2 2 Normal Structure Mitral Valve Cross sectional Area 4-6cm2 Anterior and Posterior Leaflets Chordae Tendineae Papillary Muscles
3 3 Mitral Stenosis Etiology & Pathology Rheumatic Fever- 99% Other Congenital Carcinoid Lupus Amyloid Infective Endocarditis Mucopolysaccharide Disease
4 4 Pathophysiology Mild MS- orifice <2 cm2 Critical MS- <1 cm2 A-V pressure gradient >20mmHg Increased LA Pressure Increase Pulmonary Venous + Capillary Pressures Increase Pulmonary Artery Systolic Pressure Decrease RV Function (when PAS>30-60mmHg)
5 5 History Exertional Dyspnea Cough/Wheezing Orthopnea/PND/CHF Hemoptysis-Rupture of Pulm Vein-Brochial Vein Shunts
6 6 History Chest Pain-Increase RV Pressures or Unknown Etiology Systemic Emboli (LA clots) Increased LA size, Decreased C.O., Atrial Fib, IE Significantly decreased w/anticoagulation
7 7 Natural History Asymptomatic for 15-20yrs following Rheumatic Fever Additional 5-10 yrs for progression from mild to severe stenosis Stenosis progression approx..09 cm2/yr
8 8 Natural History Presurgical Survival Rates NYHA Class II 80%-10yrs Class III 38%-10yrs, 62% 5yrs Class IV 15%-5yrs
9 9 Management-Medical Endocarditis Prophylaxis Activity Limitation Diruetics- Decrease Na Intake Heart Rate Control for A-fib or Sinus Rhythm Anticoagulation
10 10 Percutaneous Balloon Angioplasty Moderate-Severe MS Mild MS- if Pulmonary Artery Pressures or Wedge Pressure Elevate with Exercise
11 Valve Replacement Indications Combined MS/MR <1.5 cm2-nyha III or IV <1 cm2 Class II if Pulm Artery Pressure >70mmHg Mortality 3-8% Valve Type-Prosthetic or Bioprosthetic, 11
12 12 Mitral Regurgitation Etiology Rheumatic Heart Disease Infective Endocarditis Collagen Vascular Disease Cardiomyopathy Ischemic Heart Disease Mitral Valve Prolapse-most common cause for valve surgery in US
13 13 Pathophysiology Decreased Impedance to Ventricular Emptying Determinants of Regurgitant Flow Instantaneous Size of MV Orifice Dependent on Preload, Afterload, LV Contractility, LV Size LA-LV Pressure Gradient dependent on Systemic Vascular Resistance, LV Pressure, & LV Size
14 14 Pathophysiology LV Compensation Increased End Diastolic Volume Increased Wall Tension Increased Preload Increased LV Emptying Normal Ejection Fraction should be Super Normal >65% to maintain forward cardiac output and B/P
15 15 Pathophysiology LV Decompensation Increase End Systolic Volume Increased End Diastolic Volume Leads to Annulus Dilatation (MR begets MR) Decreased Ejection Fraction and Stroke Volume
16 16 Pathophysiology Ejection Fraction in Mitral Regurgitation >65% normal in compensated MR 50-65% mild impairment 40-50% moderate-severe impairment <35% advanced impairment As ejection fraction decreases operative risk increases.
17 17 History Shortness of Breath Exertional Dyspnea Congestive Heart Failure RHF Significant symptoms in chronic MR usually do not develop until LV decompensation occurs.
18 18 History Medical Treatment Survival 80% 5yr 60% 10yr 30-45% 5yr if MR severe
19 19 Management of Chronic MR Medical Digoxin Diruetics* Afterload Reduction Anticoagulation in A-fib Endocarditis Prophylaxis
20 20 Management of Chronic MR Surgical Indications Asymptomatic Class I EF < 60% or LV Systolic Diameter >45mm Severe MR Class II, III, or IV generally considered for surgery unless EF <30% Valve Repair vs. Replacement
21 21 Mitral Valve Prolapse Systolic Click-Murmur Syndrome Barlow s Syndrome Billowing Mitral Valve Syndrome Floppy Valve Syndrome Myxomatous Valve Syndrome Parachute Valve
22 22 Mitral Valve Prolapse Over diagnosed 2.4% of population Females>Males 2:1 Severe MR- Elderly Male>Young Female
23 23 MVP Etiology Primary Valvular most frequent Connective Tissue Diseases Hyperthyroidism Myotonic Dystrophy Periarteritis Nodosa Von Willebrands
24 24 MVP Pathology Myxomatous Proliferation and Degeneration of Valve Leaflets Increased Quantity of Acid Mucopolysaccharide in Middle Layer of Valve Tissue
25 25 MVP History Most are asymptomatic throughout life Chest pain, fatigue, anxiety Orthostasis-questionable autonomic dysfunction Arrhythmia-SVT, PACs, PVCs Symptoms of MR if present
26 26 Natural History Progressive MR in 15% over yrs Infective Endocarditis Cerebral Emboli-tearing of endothelial covering of myxomatous valve with platelet activation Sudden Cardiac Death-V fib, increased Q-T interval (not well established)
27 27 MVP Management Endocarditis prophylaxis if MR present Holter monitor-beta blocker for ectopy? Aspirin if focal neurological events present MR-treat like any other MR, valves usually amenable to repair *MVP is usually a benign disease*
28 28 Aortic Valve Normal Structure Valve sits at the base of Aortic Root Three Leaflets (cusps)-non coronary, right coronary, left coronary Cusps give rise to ostea of right coronary artery and left main coronary artery Normal cross-sectional area 3-4cm2
29 29 Aortic Stenosis Etiology and Pathology Valvular Supravalvular Subvalvular Hyperthrophic Cardiomyopathy
30 30 Congenital Aortic Stenosis Unicuspid Presents less than one year of age Bicuspid Adult Presentation Chronic turbulent flow Leads to fibrosis, rigidity, calcification Tricuspid Leaflets of unequal size
31 31 Acquired Aortic Stenosis Rheumatic Rare Usually mitral valve also involved Degenerative or Senile Most common cause of adult AS Most common cause of valve replacement Years of normal mechanical stress leads to calcium deposits on leaflets Inflammatory or Infectious component?? >age 65 2% frank AS, 30% Aortic Sclerosis
32 32 Hemodynamics Severe AS Mean systolic pressure gradient 40mmHg in the presence of normal cardiac output Valve area 1.0cm 2 Moderate AS 1-1.5cm 2 Mild AS 1.5-2cm 2 Aortic Sclerosis
33 33 History Long latent period of increasing obstruction Symptoms usually begin in 5 th or 6 th decade Angina in 2/3 of patients Hyperthrophied myocardium Increased ventricular systolic pressure All of which increase myocardial oxygen consumption Oxygen supply-demand imbalance leads to subendocardial ischemia
34 34 History Syncopy Reduced cerebral perfusion Vasodilation in the presence of fixed cardiac output leads to hypotension Baroreceptor-vasodepression due to high LV systolic pressure Dyspnea (CHF) Particularly with exertion due to fixed cardiac output Pulmonary Venous HTN can lead to CHF
35 35 Natural History Asymptomatic latent period With moderate-severe AS valve area can decrease on average 0.12cm2 per year *Angina, synocopy or CHF Average 1-3 year survival 50% Sudden cardiac death rare
36 36 Surgery (Valve Replacement) Indications Symptomatic Patients -valve area 1.0cm 2 Asymptomatic Patients-progressive LV dysfunction (EF <35%) or hypotensive response to mild exercise Delaying surgery in asymptomatic patients with good exercise tolerance is controversial Valve type Prosthetic, Bioprosthetic or TAVR
37 37 Surgery (Valve Replacement) Results Effective prosthetic valve area not normal Surgery replaces Critical AS with Non-critical AS Symptoms can persist if valve-patient mismatch occurs 10 year survival 85%
38 38 Aortic Regurgitation Etiology and Pathology Valvular Rheumatic-Fibrotic Retraction of Leaflets Ankylosing Spondylitis, Behcet s, Psoriatic Arthritis, Giant Cell Arteritis Degenerative AS-75% w/ar Infective Endocarditis-Leaflet Destruction Trauma-ascending aortic tear Bicuspid aortic valve-prolapse or incomplete closure Myxomatous Degeneration-like MVP
39 39 Etiology and Pathology Aortic Root Disease-More common than primary valvular. Root Dilatation leads to noncoaptation of leaflets. Degenerative-Hypertensive Aortic Dilatation Cystic Medial Necrosis-Classic Marfans Syndrome Aortic Dissection Syphilitic Aortitis Rheumatic Disease-same as valvular
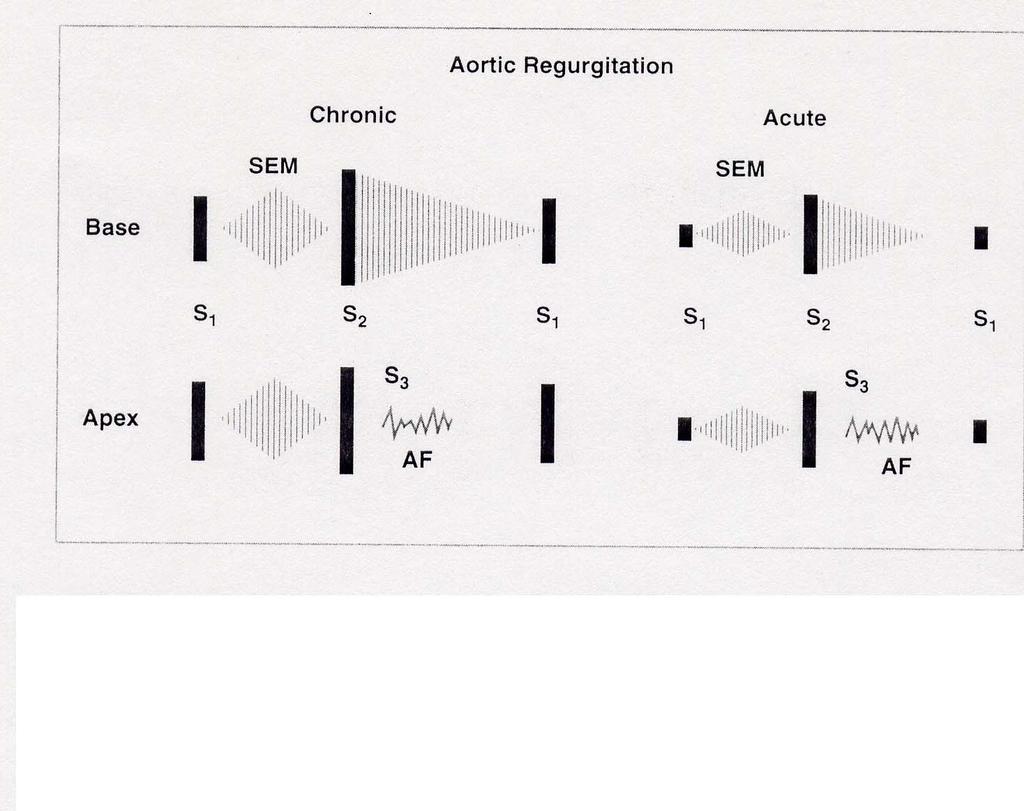
40 40 History Acute AR LV cannot accommodate acute regurgitant volume can lead to cardiovascular collapse Chronic AR Gradual LV enlargement-eccentric hypertrophy Exertional dyspnea, orthopnea, PND, CHF Presents 4 th or 5 th Decade
41 Natural History Acute AR Cardiovascular collapse Inotrophic agents and vasodilators Prompt surgical intervention Chronic AR 75% Five Year Survival 50% Ten Year Survival Progressive downhill course of CHF, Episodic Pulmonary Edema, Sudden Cardiac Death 41
42 42 Medical Treatment Acute AR As above Chronic AR Asymptomatic Mild-Moderate Follow by Echo Yearly Endocarditis Prophalaxis for all AR May not require medical treatment
43 43 Medical Treatment Symptomatic Moderate-Severe AR Limit exertional activity Aggressively treat B/P Diuretics Salt Restriction Digoxin Vasodilators (Nifedipine?)
44 44 Surgical Treatment Indications Defer surgery for chronic severe AR if good exercise tolerance, EF greater than 50%, end systolic diameter < 50 mm, and end diastolic diameter < 70 mm Be aware that progressive decline in LV function or size increases surgical morbidity and mortality
45 45 Surgical Treatment Mortality 3-8% perioperative 5-10% late mortality with significant preop LV dysfunction
46 Cardiac Auscultation Jay L. Rubenstone, D.O., F.A.C.C. October 2012
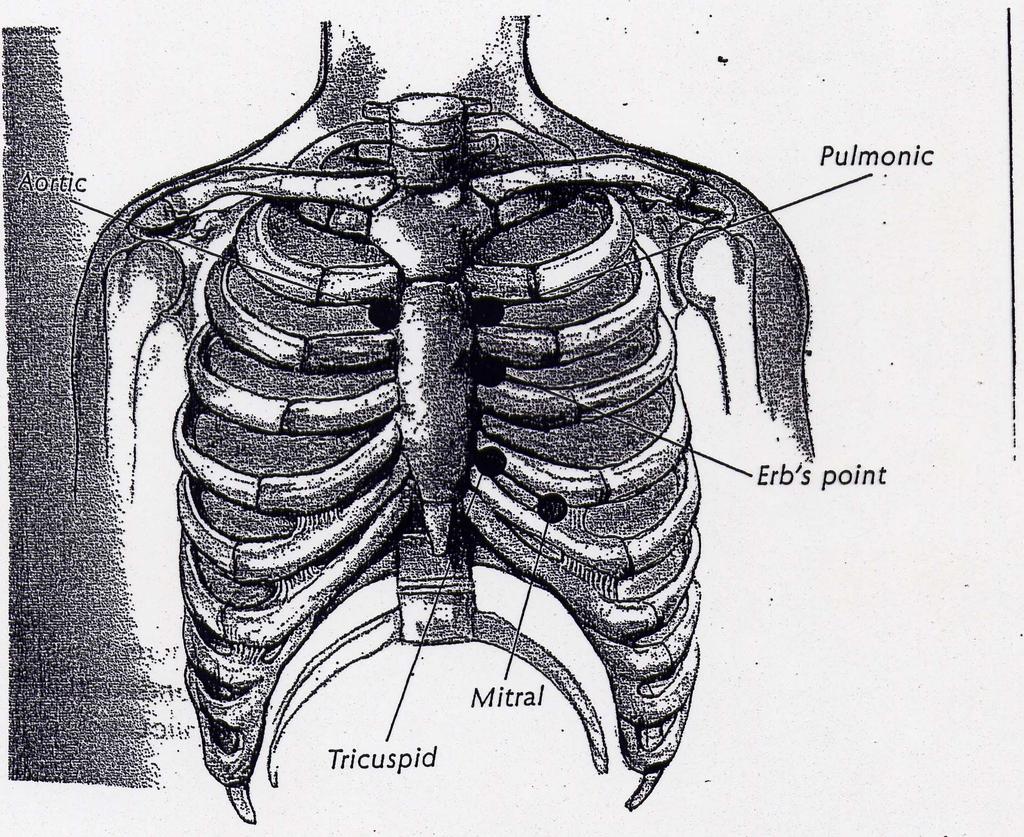
47 Techniques of Examination Order of Exam Aortic Area Pulmonic Area Tricuspid Area Mitral Area
48
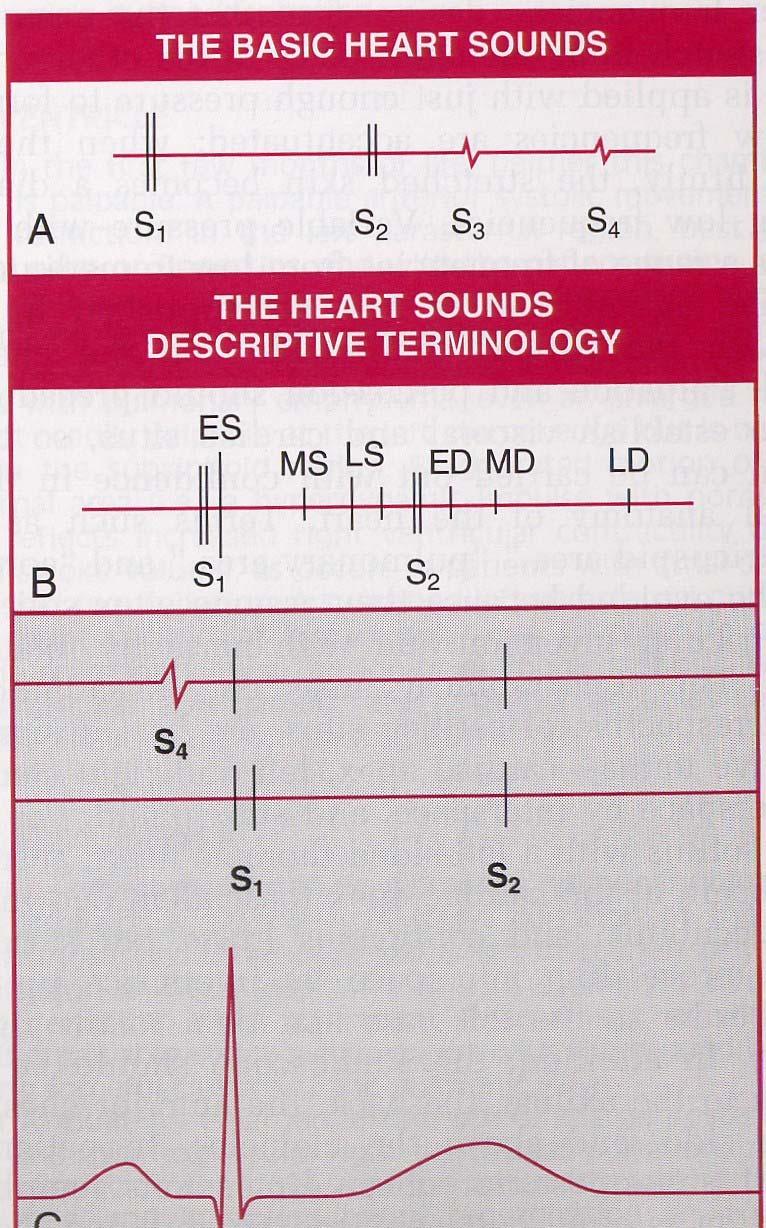
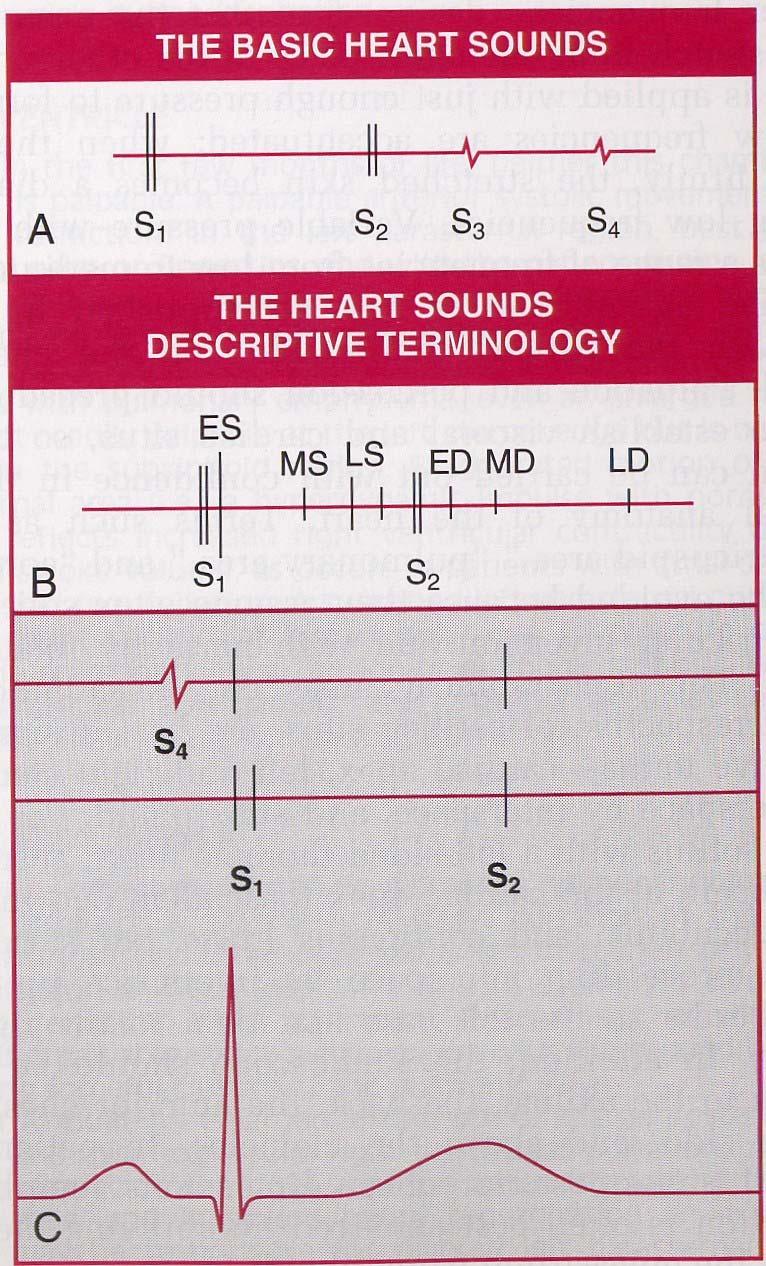
49 Process of Auscultation At each auscultatory area: 1. Concentrate on 1st Heart Sound note Intensity and Splitting 2. Concentrate on 2nd Heart Sound note Intensity and Splitting 3. Listen for Extra Sounds in Systole note Timing, Intensity, Pitch
50 Process of Ascultation 4. Listen for Extra Sounds in Diastole note timing, intensity, pitch 5. Listen for Systolic Murmurs* 6. Listen for Diastolic Murmurs* 7. Other Heart Sounds
51 Process of Ascultation *If Systolic or Diastolic Murmur Present, Note: Location Radiation Intensity Pitch Quality
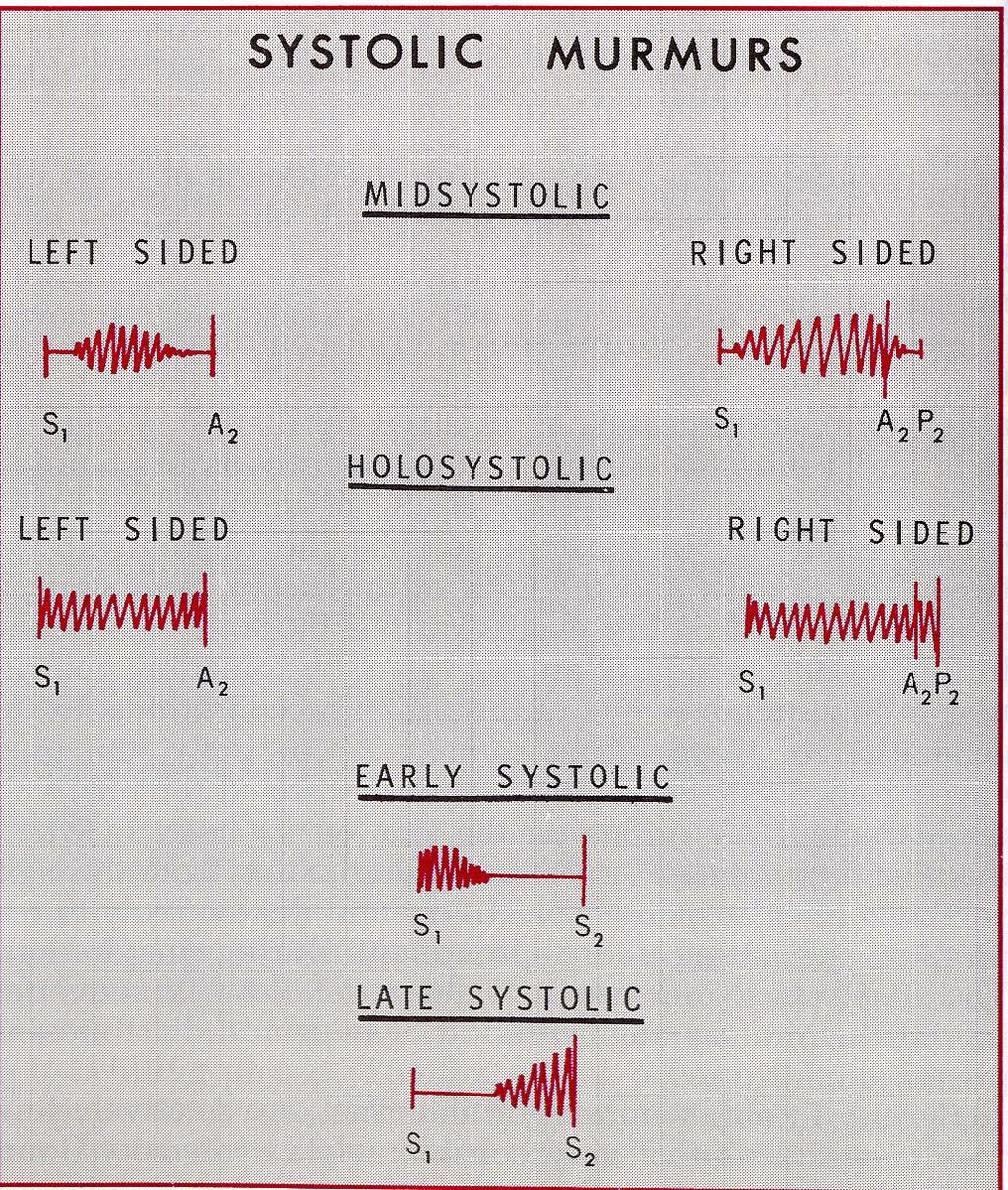
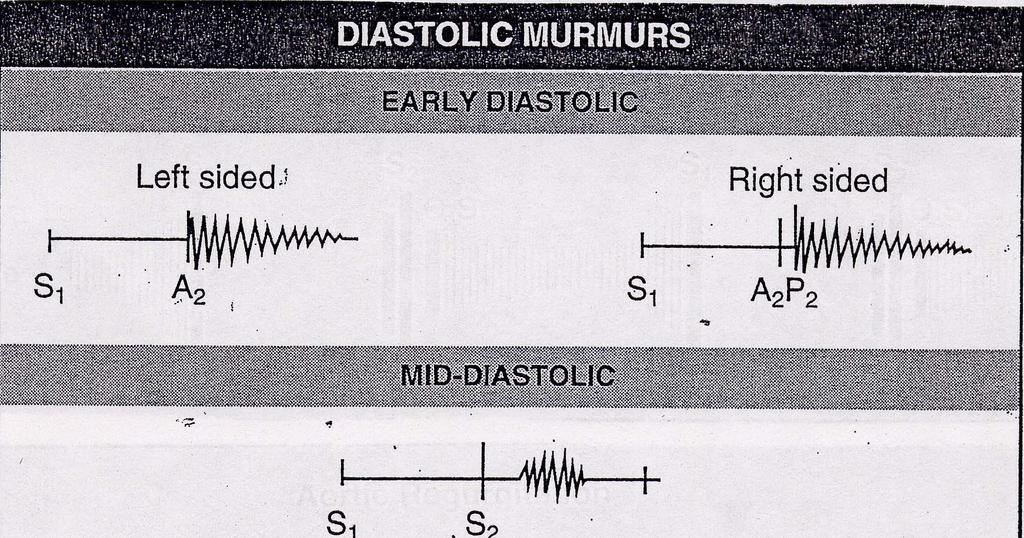
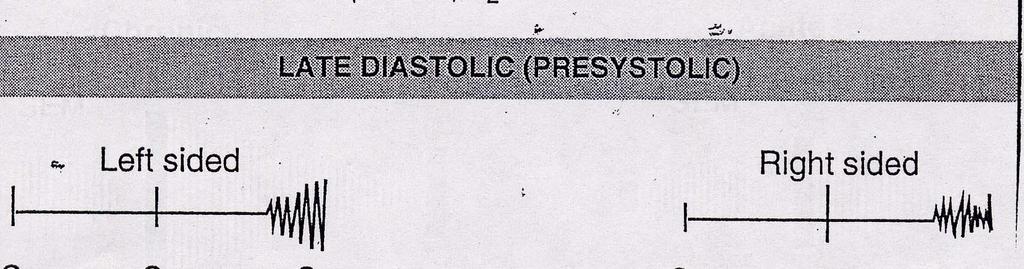
52 Auscultation Timing Systolic Early Mid Late Diastolic Early Mid Late (or Presystolic)
53 Auscultation Location Interspace Centimeters from Midsternal Midclavicular Or Axillary Lines
54 Auscultation Intensity Grade 1 Grade 2 Grade 3 with Grade 4 Grade 5 Grade 6 Very Faint Quiet, but Heard Immediately Moderately Loud, Not Associated a Thrill Loud, May Be Associated with a Thrill Very Loud May be Heard w/stethoscope off chest
55 Auscultation Radiation or Transmission Pitch High, Med, Low Quality Blowing Rumbling Harsh Muscial
56
57 COMPONENTS OF S1 Mitral Valve Closure Best Heard: Apex Tricuspid Valve Closure Best heard: Lower Left Sternal Boarder
58 S1 Wide Splitting RBBB PVC from Left Ventricle Single Sound Normal LBBB PVC from Right Ventricle Paced Beats
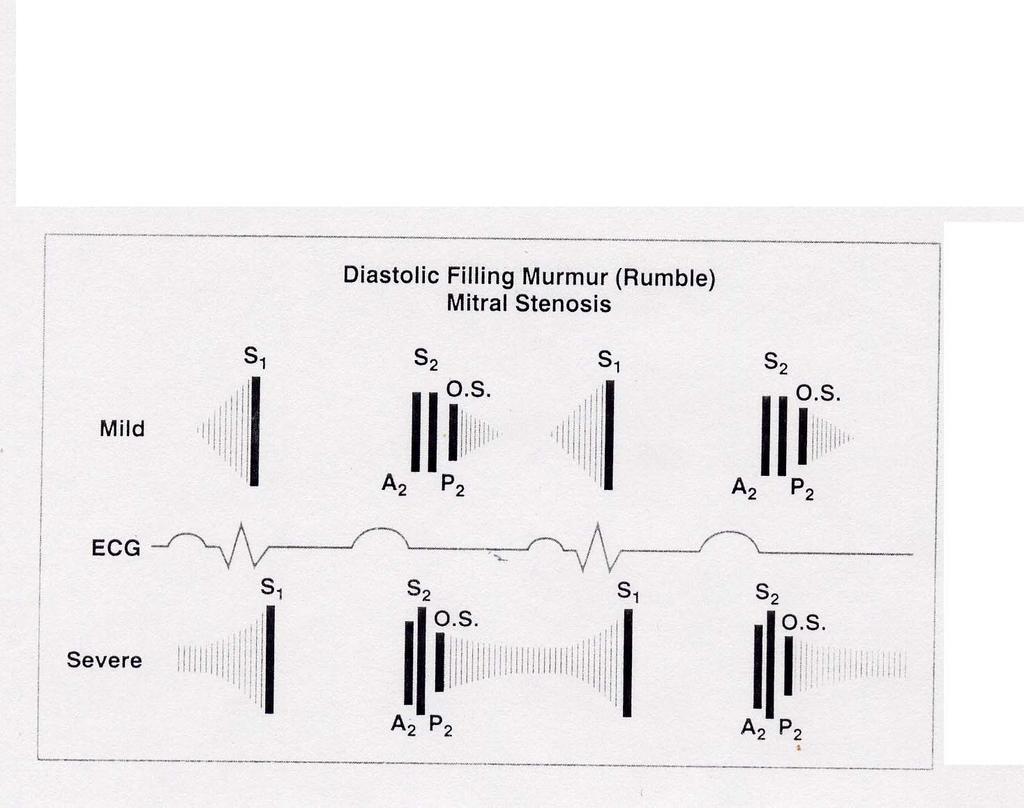
59 S1 Increased Intensity Short PR Rapid HR Atrial Fibrillation Mitral Stenosis
60 S 1 Decreased Intensity Mitral Stenosis (Immobile Leaflets) Opposite of Causes of Increased Intensity
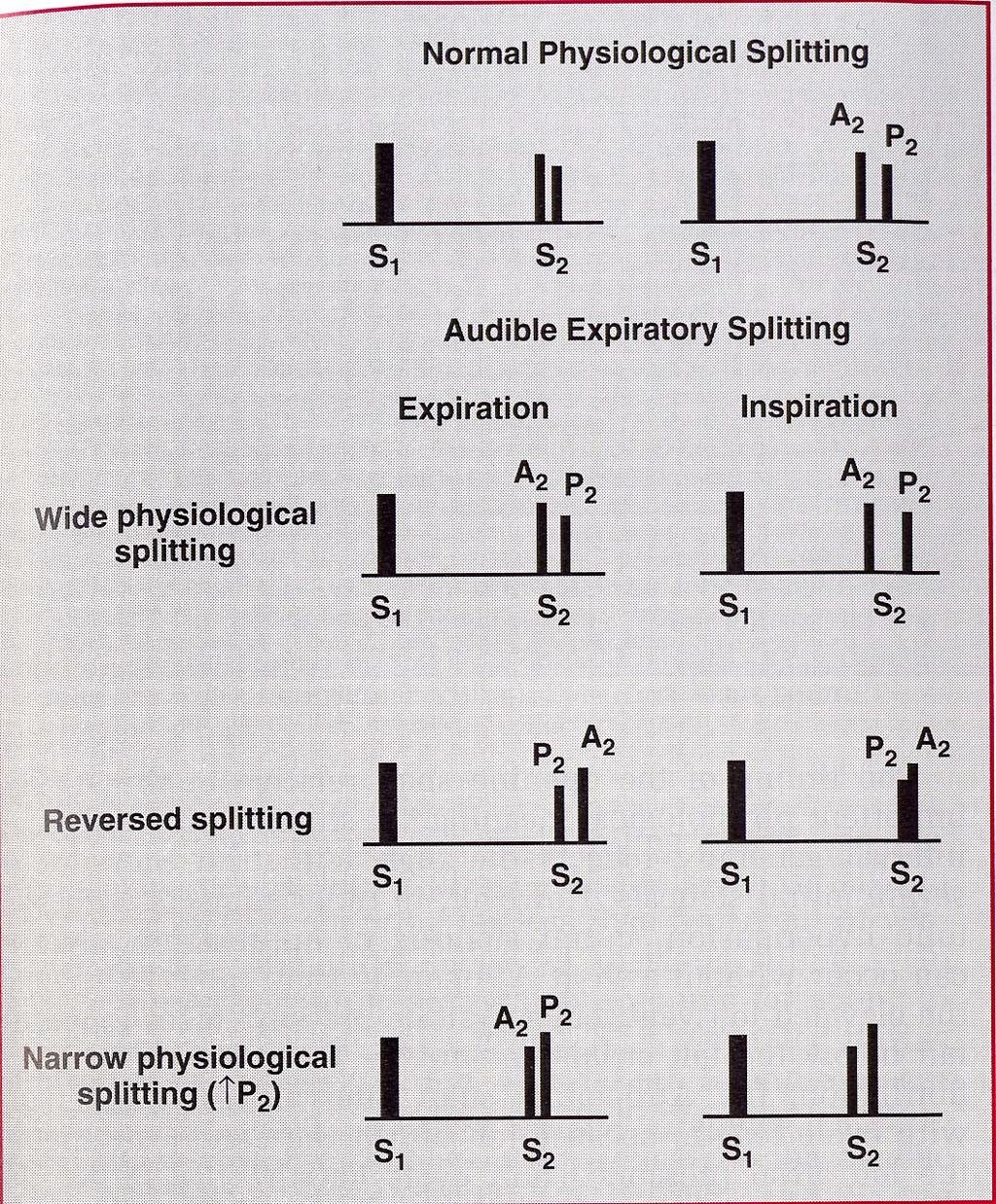
61 S 2 Two Components Aortic Closure A2 Pulmonic Closure P2 Best Heard at the Base
62 S 2 Normal Splitting Best Heard At 2 nd Left Intercostal Space During Inspiration there is Delayed Pulmonic Valve Closure Due to Increased Capacitance of Pulmonary Bed
63 S 2 Loss of Splitting Inaudible P2- Adults with Increased Chest Diameter Congenital (Tetralogy, Pulmonary Atresia Transposition) Increased Pulmonary Valve Resistance-Pulmonary HTN Eisenmenger s Complex-Equal Pulmonary & Systemic Resistances
64 S 2 Persistent Splitting RBBB Pure MR Healthy Adolescents when in Supine Position Fixed Splitting Atrial Septal Defect- Due to Delayed Closure of Pulmonic Valve from Increased Right-Sided Flow
65 S 2 Paradoxical Splitting- P2 before A2 LBBB Paced Beats Increased Intensity A2 Systemic HTN Dilated Aortic Root P2 Pulmonary HTN Dilated Pulmonary Trunk
66 Early Systolic Sounds Ejection Sound- Usually High Frequency Aortic Valve- Aortic Stenosis, Bicuspid Aortic Valve Pulmonary Valve-Pulmonic Stenosis Vary with Respirations Prosthetic Valves- Mechanical, Not Bioprosthetic
67 Mid-Late Systolic Sounds Click High Frequency Sound Found in Mitral Valve Prolapse Occurs Earlier with Valsalva Maneuver or Squatting to Standing
68 Early Diastolic Sounds Opening Snap of Mitral Stenosis (MS) High Frequency-Left Lateral Decubitus Position, Apex Occurs after S2, before S3 MS More Severe with Short A2-OS Interval Precordial Knock Chronic Constrictive Pericarditis Mitral Regurgitation Atrial Myxoma Older Model Prosthetic Mitral Valve
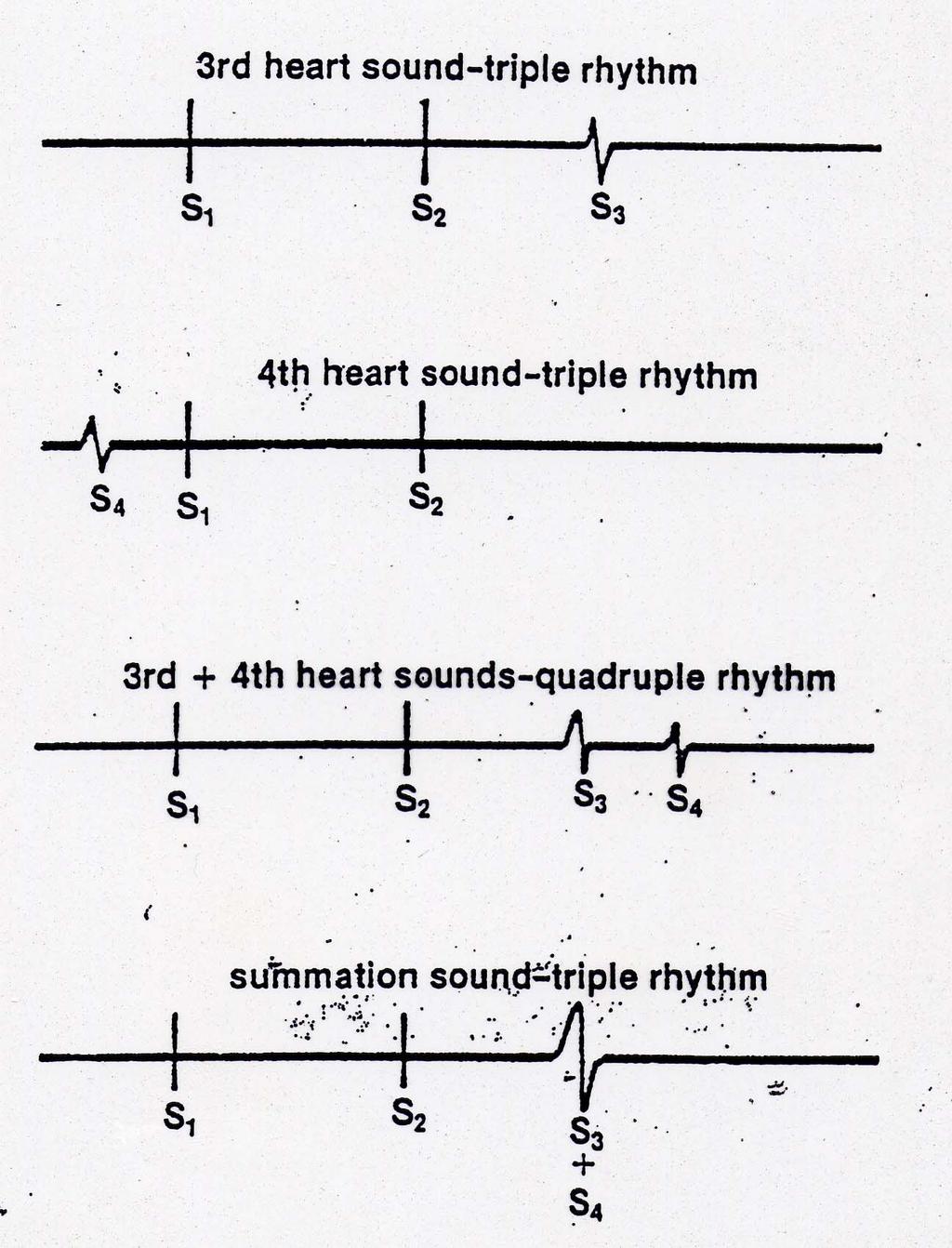
69 MID DIASTOLIC SOUNDS S3 Occurs During Rapid Filling of Left Ventricle (LV) related to LV Volume Low Frequency Best Heard At the Apex w/bell Pt in Left Lateral Decubitus Position Can Be Normal to Age 40??? Can be Pathognomonic for Congestive Heart Failure
70 Late Diastolic Sounds S4 During Atrial Phase of LV Filling Consequence of Ventricular Stiffness Absent in Atrial Fibrillation or Ventricular Pacing Low Frequency Sound Best Heart At the Apex Pt in Left Lateral Decubitus Position HTN, Aortic Stenosis, Ischemic Heart Disease
71 Diastolic Sounds Right Sided S3, S4 Left Lower Sternal Boarder Intensity Varies with Respiration due to Right Heart Filling (Carvallo s Sign) Summation Gallop Occurrence of an Over Lapping S3 and S4 due to Tachycardia
72
73
74
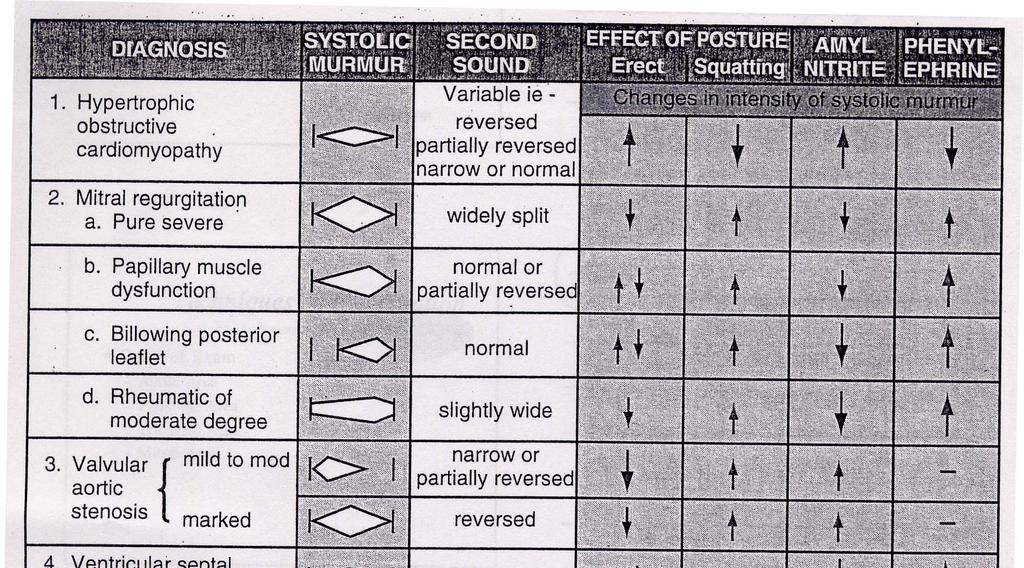
75 Systolic Murmurs Obstruction to Ventricular Outflow Dilatation of Aortic Root or Pulmonary Trunk Accelerated Flow into Aorta or Pulmonary Trunk Innocent Murmurs Some Forms of MR (Papillary Muscle Dysfunction)
76 Systolic Murmurs Acute Mitral Regurgitation (MR) or Tricuspid Regurgitation (TR) Mid Frequency Not Classic Murmur Ventricular-Septal Defect (VSD) High Frequency (diaphram) Atrial-Septal Defect (ASD) Pulmonary Outflow Not Defect Murmur
77 Systolic Murmurs Aortic Valve Stenosis Diamond Shaped, Crescendo-Decrescendo Begins After S1 or with Aortic Ejection Sound Ends Before S2 2 nd Right Intercostal Space, Apex, can radiate to Neck High Frequency, Harsh Can be Musical in Quality at the Apex
78 Systolic Murmurs Pulmonic Stenosis Similar to AS Except Relationship to P2 2 nd Left Intercostal Space
79 Systolic Murmurs Mitral Valve Prolapse High Frequency, Sometimes Honking, Crescendo Murmur Usually Extends to S2 Classic Mid-Late Systolic Click Occurs Earlier with Valsalva & Squatting to Standing
80 Systolic Murmurs Holosystolic Begins with S1, Ends at S2 MR- Radiates to Left Sternal Boarder, Base or Neck, More Commonly Apex to Axilla TR- Carvallo s Sign (Inspiratory Variation) VSD-Across Precordium Patent Ductus Arteriosis (PDA)- Aorto-Pulmonary Connection
81 Normal Systolic Murmurs Still s Murmur Medium Frequency, Vibratory, Originating from Leaflets of Pulmonic Valve Rapid Ejection into Aortic Root or Pulmonary Trunk Pregnancy Anemia Fever Thyrotoxicosis
82 Normal Systolic Murmurs Aortic Sclerosis Most Common Innocent Murmur
83
84 Early Diastolic Murmur Aortic Regurgitation High Pitched, Decrescendo Murmur Best heard at Left Sternal Boarder with the diaphragm w/patient Leaning Forward at End Expiration Acute, Severe AR Murmur Can be Short, Soft and Med Pitched Chronic, Sever AR- Murmur Usually Long, Loud, Blowing Decrescendo, High Frequency
85 Early Diastolic Murmur Graham Steell Murmur of Pulmonic Regurgitation as a Result of Pulmonary HTN High Freq, Decrescendo Blowing Murmur Heard throughout Diastole
86 Mid Diastolic Murmur Mitral Stenosis (MS) Follows Opening Snap Low Pitch Rumble Best Heard Apex over LV Using Bell of Stethoscope Pt in Left Lateral Decubitus Position
87 Mid Diastolic Murmurs Tricuspid Stenosis Similar to MS, except increases with Respiration (Carvallo s Sign) Best Heard at Left Lower Sternal Edge
88 Mid Diastolic Murmurs Pulmonic Regurgitation Crescendo-Decrescendo Murmur when Primary Valvular Abnormality and Not Associated with Pumonary HTN
89 Diastolic Murmurs Late or Presystolic Austin Flint Murmur of Aortic Regurgitation Bubbling Quality, Short Consequence of Aortic Regurgitation impinging on Mitral Valve
90 Diastolic Murmurs Continuous PDA (AortoPulmonary Connection) Rough Thrill A-V Fistulas Hemodialysis Shunt Aortic Valve Sinus to Right Ventricular Fistula Coronary Artery Fistulas
91 Diastolic Murmurs Venous Hum Rough in quality not actually a hum Hepatic Internal Jugular During Anemia, Fever, Pregnancy and Thyrotoxicosis
92
93 Pericardial Friction Rub Three Phases Mid Systolic, Mid Diastolic, Pre Systolic Scratchy, Leathery Best Heard With Diaphragm of Stethoscope Left Sternal Boarder Leaning over at End Expiration Apposition of Abnormal Visceral and Parietal Pericardium Confused with Hamman s Sign in Post Open Heart Surgery (Crunch Sound from Mediastinal Air)
94 Innocent or Normal Murmurs-Systolic Vibratory Systolic Murmur (Still s Murmur) Pulmonic Systolic Murmur (Pulmonary Trunk)* Mammary Soufflé* Peripheral Pulmonic Systolic Murmur (Pulmonary Branches) Supraclavicular or Brachiocephalic Systolic Murmur Aortic Systolic Murmur *common in pregnancy
95 Innocent or Normal Murmurs- Continuous Venous Hum Continuous Mammary Soufflé
96 Conclusions Consistent Approach to Auscultation Knowing What to Look For Follow Through on H&P Confirm or Eliminate Suspicions Knowing How to Find It Proper Utilization of Stethoscope Location and Quality of Heart Sounds & Murmurs

97
98
99
Valvular Heart Disease and Auscultation. Troy L Randle, DO, FACC, FACOI
 Valvular Heart Disease and Auscultation Troy L Randle, DO, FACC, FACOI 2 Normal Structure Mitral Valve Cross-sectional Area 4-6 cm 2 Anterior and Posterior Leaflets Chordae Tendineae Papillary Muscles
Valvular Heart Disease and Auscultation Troy L Randle, DO, FACC, FACOI 2 Normal Structure Mitral Valve Cross-sectional Area 4-6 cm 2 Anterior and Posterior Leaflets Chordae Tendineae Papillary Muscles
Physical Exam Part II
 Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Heart sounds and murmurs. Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct
 Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing. 5. Intensity 2. Shape. 6. Pitch 3. Location of maximum intensity
 Definition Items in description of Timing Shape Location of maximum intensity Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing 5. Intensity 2. Shape 6. Pitch 3. Location of maximum
Definition Items in description of Timing Shape Location of maximum intensity Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing 5. Intensity 2. Shape 6. Pitch 3. Location of maximum
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Cardiac Ausculation in the Elderly
 Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should.
 What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
Cardiac Examination. Pediatrics Clinical Examination
 Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
CARDIAC EXAMINATION MINI-QUIZ
 CARDIAC EXAMINATION MINI-QUIZ 1. Sitting bolt upright, your dyspneic (short of breath) patient has visible jugular venous pulsations to the angle of his jaw, which is 12 cm above his sternal angle. What
CARDIAC EXAMINATION MINI-QUIZ 1. Sitting bolt upright, your dyspneic (short of breath) patient has visible jugular venous pulsations to the angle of his jaw, which is 12 cm above his sternal angle. What
Mitral Valve Disease. Prof. Sirchak Yelizaveta Stepanovna
 Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease. Pregnancy and Cardiovascular Disease MCQ
 Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Clinical significance of cardiac murmurs: Get the sound and rhythm!
 Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
2. The heart sounds are produced by a summed series of mechanical events, as follows:
 Heart Sounds. Phonocardiography 1 Objectives 1. Phonocardiography - Definition 2. What produces the heart sounds 3. Where to listen for the heart sounds 4. How to record a phonocardiogram 5. Normal heart
Heart Sounds. Phonocardiography 1 Objectives 1. Phonocardiography - Definition 2. What produces the heart sounds 3. Where to listen for the heart sounds 4. How to record a phonocardiogram 5. Normal heart
Valvular Heart Disease
 Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
Mitral Valve Disease. Chapter 29
 Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
1. how a careful cardiovascular evaluation can accurately assess pathology and physiology at the bedside, and
 This program will demonstrate: 1. how a careful cardiovascular evaluation can accurately assess pathology and physiology at the bedside, and 2. the importance of integrating this information with selected
This program will demonstrate: 1. how a careful cardiovascular evaluation can accurately assess pathology and physiology at the bedside, and 2. the importance of integrating this information with selected
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Tricuspid and Pulmonic Valve Disease
 Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
By the end of this session, the student should be able to:
 Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
Congestive Heart Failure Patient Profile. Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption
 Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
For more information about how to cite these materials visit
 Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Valvular Stenosis and Regurgitation: Barriers to Flow
 Valvular Stenosis and Regurgitation: Barriers to Flow Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com CNEA 2009 1 Cardiac Valves Prevent Backward Flow Permit Forward Flow 2 www.cardionursing.com
Valvular Stenosis and Regurgitation: Barriers to Flow Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com CNEA 2009 1 Cardiac Valves Prevent Backward Flow Permit Forward Flow 2 www.cardionursing.com
PEDIATRIC HEART MURMURS. Manish Bansal, MD Clinical Assistant Professor Division of Pediatric Cardiology University of Iowa
 PEDIATRIC HEART MURMURS Manish Bansal, MD Clinical Assistant Professor Division of Pediatric Cardiology University of Iowa Murmur murmur. (n.d.). Dictionary.com Unabridged. Retrieved March 9, 2018 from
PEDIATRIC HEART MURMURS Manish Bansal, MD Clinical Assistant Professor Division of Pediatric Cardiology University of Iowa Murmur murmur. (n.d.). Dictionary.com Unabridged. Retrieved March 9, 2018 from
Ethiology of the disease - What may cause it?: One of the following numerous causes can cause aortic regurgitation:
 AORTIC REGURGITATION Aortic regurgitation is one of the aortic valve diseases, the aorta being the artery that brings oxygenated blood to the systemic circulation. The other one is the aortic valve stenosis.
AORTIC REGURGITATION Aortic regurgitation is one of the aortic valve diseases, the aorta being the artery that brings oxygenated blood to the systemic circulation. The other one is the aortic valve stenosis.
Aortic Valve Lesions
 Version 1.0 Valvular Heart Disease 25/03/2012 Aortic Stenosis Aortic Valve Lesions General Most common isolated affected valve, esp elderly 4M:1F Unrecognised can be important cause of anaesthetic & obstetric
Version 1.0 Valvular Heart Disease 25/03/2012 Aortic Stenosis Aortic Valve Lesions General Most common isolated affected valve, esp elderly 4M:1F Unrecognised can be important cause of anaesthetic & obstetric
Valvular Heart Disease: Recognition and Management in the Outpatient Setting
 Valvular Heart Disease: Recognition and Management in the Outpatient Setting Ian S. Harris UCSF Division of Cardiology Case 1: 80 year old man with a history of hypertension, complaining of exertional
Valvular Heart Disease: Recognition and Management in the Outpatient Setting Ian S. Harris UCSF Division of Cardiology Case 1: 80 year old man with a history of hypertension, complaining of exertional
Which one of the following echocardiographic profiles most strongly indicates the need for aortic valve replacement? FS [
 Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Aortic valve disease. Acknowledgement for slides. Heart Valves 4/28/2018. Adopted from
 Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
Cardiology. the Sounds: #7 HCM. LV Outflow Obstruction: Aortic Stenosis. (Coming Soon - HCM)
") A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
High Yield Associations Cardio for Step 1. Amanda Krauss, Adee Elhamdani
 High Yield Associations Cardio for Step 1 Amanda Krauss, Adee Elhamdani EKGs Irregularly irregular with no p waves and inconsistent RR intervals High Yield new onset MC risk factors Regular PP intervals
High Yield Associations Cardio for Step 1 Amanda Krauss, Adee Elhamdani EKGs Irregularly irregular with no p waves and inconsistent RR intervals High Yield new onset MC risk factors Regular PP intervals
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
See below for descriptions of the waveform
 The internal jugular vein (IJV) connects to the right atrium without any intervening valves. The pulsation of the right atrium therefore causes the column of blood in the IJV to rise and fall this is called
The internal jugular vein (IJV) connects to the right atrium without any intervening valves. The pulsation of the right atrium therefore causes the column of blood in the IJV to rise and fall this is called
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Section V VALVULAR HEART T DISEASE. Chapter 27 Aortic Stenosis Chapter 28 Aortic Insufficiency Chapter 29 Mitral Valve Disease...
 Section V VALVULAR HEART T DISEASE Chapter 27 Aortic Stenosis........................... 256 Chapter 28 Aortic Insufficiency....................... 265 Chapter 29 Mitral Valve Disease......................
Section V VALVULAR HEART T DISEASE Chapter 27 Aortic Stenosis........................... 256 Chapter 28 Aortic Insufficiency....................... 265 Chapter 29 Mitral Valve Disease......................
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE. Sampling Rate M-Mode: 1800 / sec 2D: 30 / sec
 M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
Heart and Neck Vessels
 CHAPTER 12 Heart and Neck Vessels ANATOMY The precordium is the area on the anterior chest overlying the heart and great vessels. The heart extends from the second to the fifth intercostal space, and from
CHAPTER 12 Heart and Neck Vessels ANATOMY The precordium is the area on the anterior chest overlying the heart and great vessels. The heart extends from the second to the fifth intercostal space, and from
What s That Sound? Pediatric Murmur Evaluation
 What s That Sound? Pediatric Murmur Evaluation Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director, Pediatric
What s That Sound? Pediatric Murmur Evaluation Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director, Pediatric
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Valvular Heart Disease
 GP Update Refresher 18 th January 2018 Valvular Heart Disease Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President
GP Update Refresher 18 th January 2018 Valvular Heart Disease Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President
Heart Disorders. Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders
 Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders") Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to:
 The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
n S2=Aortic valve closure, pulmonic n S3=Very healthy or very sick LV n Children and young athletes, CHF n S4=Stiff LV, incr LVEDP, HTN, hypertrophy
 Cardiac Physical Exam Valvular Heart Disease Susan Schima MD September 29, 2015 S1=mitral valve closure (can t really hear tricuspid component) S2=Aortic valve closure, pulmonic S3=Very healthy or very
Cardiac Physical Exam Valvular Heart Disease Susan Schima MD September 29, 2015 S1=mitral valve closure (can t really hear tricuspid component) S2=Aortic valve closure, pulmonic S3=Very healthy or very
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
COLIC AND MURMURS: AN OVERVIEW
 COLIC AND MURMURS: AN OVERVIEW Gunther van Loon, DVM, PhD, Department of Large Animal Internal Medicine, Ghent University, Merelbeke, Belgium Introduction Many horses with colic present with a cardiac
COLIC AND MURMURS: AN OVERVIEW Gunther van Loon, DVM, PhD, Department of Large Animal Internal Medicine, Ghent University, Merelbeke, Belgium Introduction Many horses with colic present with a cardiac
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Valvular Heart Disease
 Valvular Heart Disease Objectives: Etiology of valve diseases Pathogenesis Clinical presentation Clinical findings Investigation Management Team Members: Duaa abdulfattah, Basil Almeflh, Jawaher Abanumy,
Valvular Heart Disease Objectives: Etiology of valve diseases Pathogenesis Clinical presentation Clinical findings Investigation Management Team Members: Duaa abdulfattah, Basil Almeflh, Jawaher Abanumy,
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
SESSION D5. The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION D5 Session Description: The Heart of the Matter: Cardiac Disease in Pregnancy Brad M. Dolinsky, MD, MFM
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
CARDIOVASCULAR PHYSICAL EXAMINATION
 CARDIOVASCULAR PHYSICAL EXAMINATION Clarke Atkins, DVM, Diplomate, ACVIM (Internal Medicine and Cardiology) Jane Lewis Seaks Distinguished Professor Emeritus North Carolina State University, College of
CARDIOVASCULAR PHYSICAL EXAMINATION Clarke Atkins, DVM, Diplomate, ACVIM (Internal Medicine and Cardiology) Jane Lewis Seaks Distinguished Professor Emeritus North Carolina State University, College of
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
Valvular Heart Disease: Volume Versus Pressure and the Hemodynamic Compromise
 Valvular Heart Disease: Volume Versus Pressure and the Hemodynamic Compromise Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com NTI 2009 Class Code 112 1 Mastery is not something that strikes in
Valvular Heart Disease: Volume Versus Pressure and the Hemodynamic Compromise Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com NTI 2009 Class Code 112 1 Mastery is not something that strikes in
Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications
 24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Maternal Cardiac Disease In Pregnancy. August 25, 2017 PREGNANCY ECHO CONFERENCE
 Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Physical Exam Of The Cardio- Vascular System. James G. Laws D.O. MACOI
 Physical Exam Of The Cardio- Vascular System James G. Laws D.O. MACOI An Important Part Of The Physical Exam Of The Cardio-Vascular System That Is Commonly Overlooked Is? 20% 20% 20% 20% 20% 1. Palpation
Physical Exam Of The Cardio- Vascular System James G. Laws D.O. MACOI An Important Part Of The Physical Exam Of The Cardio-Vascular System That Is Commonly Overlooked Is? 20% 20% 20% 20% 20% 1. Palpation
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Are you too quick to refer?
 HEART MURMURS IN CHILDREN Are you too quick to refer? Many children with murmurs are unnecessarily referred, say the authors, who describe a thorough cardiovascular exam you can perform in three to five
HEART MURMURS IN CHILDREN Are you too quick to refer? Many children with murmurs are unnecessarily referred, say the authors, who describe a thorough cardiovascular exam you can perform in three to five
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
10/16/2014. CCRN Review - Cardiovascular. CCRN Review - Cardiovascular. CCRN Review - Cardiovascular
 Hypertrophic (IHSS) Diagnosis Chest x ray cardiomegaly Electrocardiography LV hypertrophy, ST segment T was changes, Q waves in inferior & precordial leads Atrial & ventricular dysrhythmias Hypertrophic
Hypertrophic (IHSS) Diagnosis Chest x ray cardiomegaly Electrocardiography LV hypertrophy, ST segment T was changes, Q waves in inferior & precordial leads Atrial & ventricular dysrhythmias Hypertrophic
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
pulmonary valve on, 107 pulmonary valve vegetations on, 113
 INDEX Adriamycin-induced cardiomyopathy, 176 Amyloidosis, 160-161 echocardiographic abnormalities in, 160 intra-mural tumors similar to, 294 myocardial involvement in, 160-161 two-dimensional echocardiography
INDEX Adriamycin-induced cardiomyopathy, 176 Amyloidosis, 160-161 echocardiographic abnormalities in, 160 intra-mural tumors similar to, 294 myocardial involvement in, 160-161 two-dimensional echocardiography
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC
 Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC Overview ACS continued Heart Failure Valvular Disorders and Endocarditis Diagnosis Nuclear stress test- stable angina
Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC Overview ACS continued Heart Failure Valvular Disorders and Endocarditis Diagnosis Nuclear stress test- stable angina
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
ASCeXAM / ReASCE. Practice Board Exam Questions. Tuesday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified