Early Repolarization: Culprit or Innocent Bystander
|
|
|
- Sybil Hodges
- 6 years ago
- Views:
Transcription
1 EP Morning Conference Early Repolarization: Culprit or Innocent Bystander December 2, 2010 Vic Froelicher, MD
2 Early Repolarization: Culprit or Innocent Bystander Nikhil A. Jain Abhimanyu Uberoi Marco Perez Anthony Weinkopff Euan Ashley Mintu P. Turakhia Shilpy Chowdhury



3 Are these Phenotypes dangerous? PVCs, silent ST depression, early repolarization/ J waves, QRS end slurring/notching

4 ECG Added to Stanford Athletes Annual Preparticipation Exam 2007

5 Global Early Repolarization with J waves Who needs more studies to participate?
6 ST Elevation Lateral Leads (1mm,any) 658 Collegiate Athletes Males>Females, African-Americans>others, no effect resting HR
7 ST Elevation on Resting ECG 1. Acute (Dynamic) 1. Ischemia (localizes, arrhythmogenic) 1. Variant Angina 2. ST Elevation MI 2. Chronic (Stable) 1. Early Repolarization changes with heart rate 2. Pericarditis 3. Over Q waves associated with LV aneurysms 4. Spinal Cord Injury and mental patients 5. Brugada Patterns (V123) but syndrome dynamic
8 ER Benign?
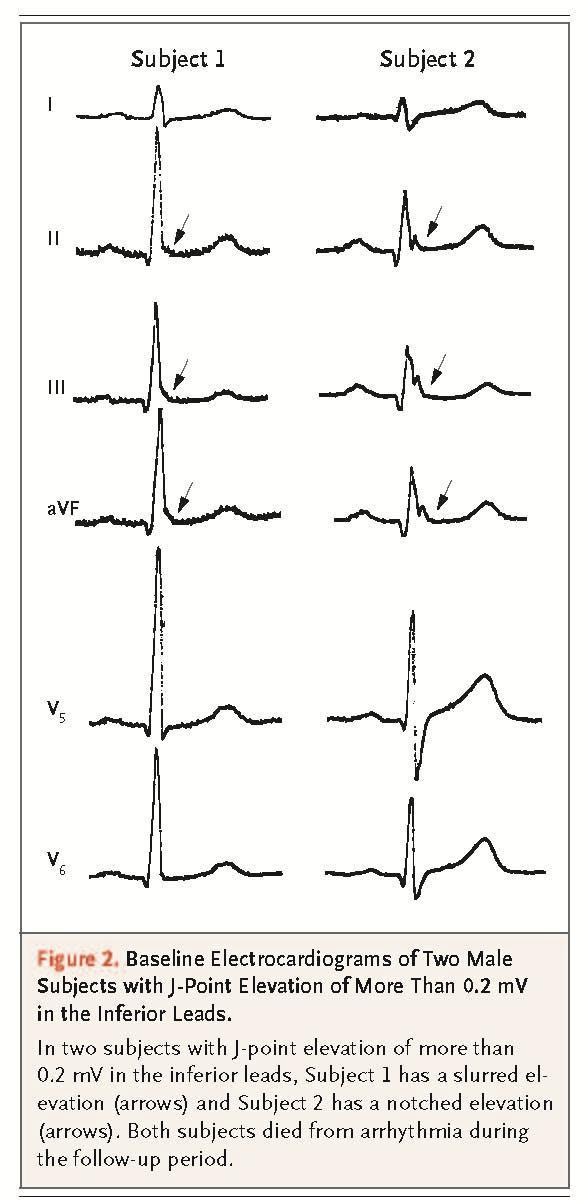
9 Haisseguirre et al, NEJM 2008;358:2016 SCD associated with Early Repolarization Based on a unique population of 202 individuals (mean age 36 yrs) with ventricular tachycardia and no other evidence for heart disease. Two surprising observations were made in this important study: subjects with ECG tracings at the time before VF or VT, dynamic ST elevation similar to that seen with coronary spasm was noted and, 2. Higher prevalence of inferior/lateral notching/slurring on their resting ECGs than in controls (31% vs 5%).
10 Tikkanen et al, NEJM 2009;361:2529 FU ER Community epidemiological study (N=10,864, 44±8 yrs) that considered baseline characteristics and utilized visually interpreted ECGs including manual measurements of ST elevation in the inferior and lateral leads with CV death as the outcome. They found no hazard associated with ER in the lateral leads but roughly an adjusted hazard of 2 for inferior lead ER. The subjects with inferior ER had a higher prevalence of Minnesota Code ECG findings associated with coronary artery disease and the example they provide exhibits ST elevation occurring over inferior Q waves.
11 Methods for Both The amplitude of J-point elevation had to be at least 1 mm (0.1 mv) above the baseline level, either as QRS slurring (a smooth transition from the QRS segment to the ST segment) or notching (a positive J deflection inscribed on the S wave) in the inferior lead (II, III, and avf), lateral lead (I, avl, and V4 to V6 ), or both.
12 Association of Early Repolarization Pattern on ECG with Risk of Cardiac and All-Cause Mortality: A Population- Based Prospective Cohort Study (MONICA/KORA) Sinner et al Methods ERP was assessed manually in all ECGs using paper prints. The criteria for detection of ERP were exactly as recently described by Haıssaguerre and colleagues. Briefly, classification as ERP required a J-point elevation >0.1 mv in 2 adjacent leads with either slurring or notching morphology. Presence or absence of STelevation in addition to J-point elevation was not taken into account and nonspecific intraventricular conduction delay was excluded from analysis.
13 Association of Early Repolarization Pattern on ECG with Risk of Cardiac and All-Cause Mortality: A Population- Based Prospective Cohort Study (MONICA/KORA) Sinner MF, Reinhard W, Muller M, Beckmann B-M, Martens E, et al. (2010) PLoS Med 7(7): e doi: /journal Methods and Findings: Electrocardiograms of 1,945 participants aged y, representing a source population of 6,213 individuals, were analyzed applying a case-cohort design. Mean follow-up was 19 years. Prevalence of ERP was 13.1% in our study. ERP was associated with cardiac and all-cause mortality, most pronounced in those of younger age and male sex; a clear ERP-age interaction was detected (p = 0.005). Age-stratified analyses showed hazard ratios (HRs) for cardiac mortality of 2 for both sexes. An inferior localization of ERP further increased ERP-attributable cardiac mortality to HRs of 3 for both sexes. Conclusions: They found a high prevalence of ERP (13%) in there population-based cohort of middle-aged individuals. ERP was associated with about a 2- to 4-fold increased risk of cardiac mortality in individuals between 35 and 54 y. An inferior localization of ERP was associated with a particularly increased risk.
14
15

16
17 Help from the Literature PubMed search from 1990 onwards yielded the following: Early repolarization : 893 hits J-point wave : 228 hits J-wave : 106 hits J-point elevation : 110 hits J deflection : 87 hits J-point deflection : 16 hits
18 Definition: Early Repolarization ( ) 1. ST Elevation at the J junction of the QRS complex (0.5 mm or more [>0.05 mv]) 2. Distinct notch (J wave) or slur on the down slope of the R wave 3. Concavity of the ST segment 4. Tall, upright T waves 5. V345 more common than II,aVF Most common in the young and Afro-Americans
19 Cellular Physiology Studies (circa 2000) Antzelevitch, Yan, Genning, Boineau JP Action potential studies, mapping suggesting that J wave and R wave slurring are early repolarization and not late depolarization. They co-opt the terms early repolarization and J- point! Do they change the measurement of QRS duration???
20 Definition: Early Repolarization (circa 2008) 1. Distinct notch (J wave) or slur on the down slope of the R wave 2. ST Elevation of 1 mm or more (maybe); Set at onset slur or peak J wave 3. Concavity of the ST segment 4. Tall, upright T waves 5. V345 more common than II,aVF
21 Definition: Early Repolarization (circa 2008) In the current studies, it is difficult to tell or compare what was done methodologically because of inconsistent terminology for ST elevation and how the level was set (J-point, J junction, J wave peak, top of the slur or notch are all possibilities). In the examples provided in the studies, the ST segment often is isoelectric but other times is elevated. No matter how compelling theories based on action potential studies are, the term early repolarization is well established and causes too much confusion if co-opted for another phenomena.
22 Definitions ST Elevation 1 mm (0.1 mv, 100 microv) elevation from isoelectric line at J point (same as QRS end, ST beginning or ST0 [zero]) in lateral and/or inferior leads J-wave distinct positive excursion at the end of the QRS complex. If QRS ends with R wave, J- wave in downslope of R wave; (if ending in S wave, J-wave in upstroke of S wave?) J-wave Syndromes hypothetical merge of Early Repol with Osborn wave, Brugada, ischemia
23 Definition Confusion Contiguous/adjacent versus any lead in an area group (Lateral=I,aVL, V456; Inferior=III,aVF,II) Originally for reproducibility (only 2.5 sec, respiratory variation) Computer analysis based on 10 seconds of average data Wider area of involvement?? J-point = peak of the J wave, beginning of slur or end of the QRS? And what is the end of the QRS? The ECG and Exercise community always called the end of the QRS complex the J-point or QRS end or ST0
24 Definition: Early Repolarization (but with more concave ST segment and positive T wave) ST level set at j-junction (j-point) where the QRS complex meets the ST segment, not at the top of the notch or peak of the J wave

![without [like here] ST](/docs-images/72/67547043/images/25-1.jpg "elevation) On R-wave")
25 Definition: J-waves (can be with or without [like here] ST elevation) On R-wave After S-wave
26
27 Other Pertinent ER Papers ER Normal Variant ECG: Correlate and Consequences. Klatsky et al. (Kaiser Perm Oakland) AJM 2003;115:171. From 73,088 adults (mean age 46) from voluntary Health screen 2,000 ECGs coded: BL 0.5 mm (15%), Definite 1.0 mm (33%); more likely to be male, less than 40 yo, bradycardic, Afro American and physically active. Hypothesis that STE would lead to hospitalizations and diagnoses not supported. J-Point Elevation of Primary VF and matched controls. Rosso et al. (UCSF and Israel) JACC 2008;52: patients with Idiopathic VF, 124 matched controls and 121 athletes. STEL the same in both groups (33% vs 24%) Ability of QRS notching to distinguish malignant vs benign ER. Merchant et al. (Boston) AJC 2009; 104: patients with idiopathic VT/VF, 23% with 1.0 mm STEL J-wave, Slurring and STEL in Athletes with Cardiac arrest. Cappoto et al. Circ AE 2010;3; SCD athletes and 365 healthy athletes, J-wave height/stel= 0.05mV, STEL 10% vs 22%
28 Is Early Repolarization in Idiopathic VT/VF Different? J-Point Elevation of Primary VF and matched controls. Rosso et al. (UCSF and Israel) JACC 2008;52: patients with Idiopathic VF, 124 matched controls and 121 athletes. J point elevation (=J wave) in inferior leads (27 vs 8%), I and AVL (13% vs 1%), V456 7% both, athletes in between. STEL and QRS slurring the same in both groups (33% vs 24%) Ability of QRS notching to distinguish malignant vs benign ER. Merchant et al. (Boston) AJC 2009; 104: patients with idiopathic VT/VF, 23% with 0.10 mv STEL (slurred or notched) 200 normals with STEL, Notching (J-wave) more prevalent in Idiopathic VF (44 vs 5%). J-wave, Slurring and STEL in Athletes with Cardiac arrest. Cappoto et al. Circ AE 2010;3; SCD athletes and 365 healthy athletes, J-wave height/stel= 0.05mV, J-wave/slurring 29% vs 8%, STEL 10% vs 22%
29 Antzelevitch and Yan (J wave Syndromes: [Early Repol, Osborn wave, Brugada, ischemia] in Heart Rhythm 2010;7:549) Three Early Repolarization (ER) subtypes: Type 1 - ER pattern in the lateral precordial leads, prevalent among healthy male athletes and is rarely seen in VF survivors(?) ; Type 2 - ER pattern in the inferior/lateral leads associated with moderate risk; and Type 3 - which displays an ER pattern in the inferior, lateral, and right precordial leads (anterior) and is associated with the highest level of risk for development of malignant arrhythmias and is often associated with ventricular fibrillation storms.
30 Palo Alto VA ECG Data Base 45,829 ECGs obtained from March 1987 to December 1999 at the Palo Alto Veterans Affairs Health Care Center for clinical indications on inpatients and outpatients; death status as of 2002 with cause of death from CPRS. Exclusions: Inpatients (n = 12,319), paced rhythms (n = 290), Wolff Parkinson White syndrome (n = 42), atrial fibrillation/flutter (n = 1,253), acute myocardial infarctions (n = 29), heart rates >100 bpm (n = 2,799), and QRS durations >120 ms (n= 3,141) were excluded from the study leaving a target cohort of 29,281 patients. 25,544 were male (87%, 55 ± 14 years of age) and 3,737 were females (13%, 56 ± 17 years of age); 13% were African American, 6% Hispanic, and 81% Caucasian and other. After 7.6 yrs FU, 6,739 deaths (1,995 CV, 30%)
31 Methods Computer analysis of the ECGs was completed with human confirmation of all computer generated reports. Since J-waves are not recognized by current ECG computer programs, these were coded visually. ST elevation was considered 0.1 mv or more of elevation at the end of the QRS complex J-wave - definite positive excursion at the end of the QRS complex before the J-point or QRS end. If the QRS complex ended with an R wave, the J-wave was noted in the down slope of the R wave; if ending in an S wave, it was noted on the upstroke of the S wave. The criterion requiring two contiguous leads in any area lead group (inferior: II, III and AVF, lateral: I, avl, V4-V6, anterior: V1-V3) was applied. Sub-groups: No ST elevation, inferior lead only, lateral lead only, inferior or lateral lead, inferior and lateral lead, and global elevation (inferior, lateral, and anterior elevation).
32 STEL and J wave Patterns Inferior or lateral ST elevation was present in 664 (2.3%) patients: 185 (0.6%) in inferior leads and 479 (1.6%) in lateral leads, with elevations in both areas in 163 patients (0.6%) patients. Global elevation was present in 0.4% and J waves were present in 11% without and 75% with ST elevation. Patients with lateral ST elevation alone or with any other pattern including lateral ST elevation were significantly younger, had a lower heart rate, a lower prevalence of any ECG abnormality other than LVH and a higher prevalence of African Americans. The inferior lead only elevation group differed from all others with ST elevation by being older, having a higher heart rate, lower prevalence of males and exhibiting more ECG abnormalities, particularly inferior Q waves (13.5%). Those w/o STEL had a lower prevalence of J-waves (11.2%) than any of the STE groups, which ranged from 71% to 84%.
33 Survival ST Elevation 1 mm Lateral Leads YEARS
34 Survival ST Elevation 1 mm Inferior Leads YEARS
35 Survival ST Elevation 1 mm Inferior or Lateral Leads with J-Wave YEARS
36 Survival Global ST Elevation 1 mm (N=117) YEARS
37 Cox Hazards Adjustment was first for age, gender and Afro-American ethnicity and second adding resting heart rate, BMI and ECG abnormalities. Age, gender, resting HR and ECG abnormalities (LVH, MC for CAD, Q waves) were significant in the Cox Models but not race and BMI. The most striking finding is the decreased risk associated with the lateral lead only ST elevation alone or with any other pattern including lateral ST elevation. While the significance disappears with adjustment, the trend remains for both outcomes. This is consistent in the groups with global elevation and those with accompanying J-waves. There was a significant adjusted or unadjusted hazard of 2X found for inferior lead elevation only in non-african Americans.
38 Conclusions from Our Data In this outpatient clinical population using modern computer technology, there was no association of lateral patterns of ST elevation, J-waves or global elevation with cardiac or all cause mortality. Inferior ST Elevation had a multivariate adjusted HR of 2 for CV death in non-african Americans Our results do not support a clinical reason for considering Global or Lateral Lead STEL or J-wave classification to be associated with CV risk. 2 mm of STEL in the lateral or inferior leads is rare
39 Data Analysis Resolution of the main hypothesis Reading the tea leafs
 Total: Females = 1%")
40 ST Elevation Lateral Leads (1mm,any;Veterans) Total: Females = 1% vs Males = 5.6%
41 ST Elevation Lateral Leads (1mm,any;males)
42 ST Elevation Lateral Leads (1mm,any)
43 ST Elevation in Anterior Leads of 353 Male athletes

44 Is there Clinical Relevance?
45 ER vs Pathology Heart rate (low, not high) Age (young, not old) Gender (male, not female) ST level (<0.2 mv, not more) Ethnicity (Afro American, not other) Athletic status (yes, not sedentary)
46 What s Next? Develop Software to detect J- waves and R wave downward slurring Apply Software to digital VA DB and evaluate hazard of the new ER
47 The End (at last!) Thanks to all who have worked on the DB Thanks to the summer volunteers Thanks for your attention Questions?
48 Considerations Visual vs Computer analysis Ethnicity and Sport Contiguous vs any lead in an area QRS prolongation and STEL particularly in IdioVF/VT J-point: end of QRS vs peak of J-wave?
49 Potential Abstracts Racial STEL pattern differences (T wave inversion) Anterior STEL Comparison of Athletes to young clinical controls J wave prevalence and prognosis QRS prolongation and STEL Max normal STEL
MICS OF MYOCARDIAL ISCHEMIA AND INFARCTION REVISED FOR LAS VEGAS
 ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
Interpretation and Consequences of Repolarisation Changes in Athletes
 Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
Interpretation and Consequences of Repolarisation Changes in Athletes Professor Sanjay Sharma E-mail sasharma@sgul.ac.uk @SSharmacardio Disclosures: None Athlete s ECG Vagotonia Sinus bradycardia Sinus
6/19/2018. Background Athlete s heart. Ultimate question. Applying the International Criteria for ECG
 Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
at least 4 8 hours per week
 ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
Prevalence and QT Interval of Early Repolarization. in a Hospital-based Population
 Original Article in a Hospital-based Population Hideki Hayashi MD PhD, Akashi Miyamoto MD, Katsuya Ishida MD, Tomohide Yoshino MD, Yoshihisa Sugimoto MD PhD, Makoto Ito MD PhD, Minoru Horie MD PhD Department
Original Article in a Hospital-based Population Hideki Hayashi MD PhD, Akashi Miyamoto MD, Katsuya Ishida MD, Tomohide Yoshino MD, Yoshihisa Sugimoto MD PhD, Makoto Ito MD PhD, Minoru Horie MD PhD Department
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
ST-segment elevation in the absence of acute infarction
 Heart Failure Early Repolarization in an Ambulatory Clinical opulation Abhimanyu Uberoi, MD, MS; Nikhil A. Jain, BS; Marco erez, MD; Anthony Weinkopff, BS; Euan Ashley, MRC, Dphil; David Hadley, hd; Mintu.
Heart Failure Early Repolarization in an Ambulatory Clinical opulation Abhimanyu Uberoi, MD, MS; Nikhil A. Jain, BS; Marco erez, MD; Anthony Weinkopff, BS; Euan Ashley, MRC, Dphil; David Hadley, hd; Mintu.
J-wave syndromes: update on ventricular fibrillation mechanisms
 J-wave syndromes: update on ventricular fibrillation mechanisms Michael Nabauer University of Munich, Germany 28.8.2011 I have no conflicts of interest ECG labelling by Einthoven Circ 1998 Osborn wave
J-wave syndromes: update on ventricular fibrillation mechanisms Michael Nabauer University of Munich, Germany 28.8.2011 I have no conflicts of interest ECG labelling by Einthoven Circ 1998 Osborn wave
How to Read an Athlete s ECG. Sanjay Sharma BSc (Hons), MD, FRCP, FESC
, MD, FRCP, FESC") How to Read an Athlete s ECG Sanjay Sharma BSc (Hons), MD, FRCP, FESC Athlete s EKG Vagotonia Sinus bradycardia Sinus arrhythmia First degree AVB ST-elevation Tall T waves Increased chamber size Left ventricular
How to Read an Athlete s ECG Sanjay Sharma BSc (Hons), MD, FRCP, FESC Athlete s EKG Vagotonia Sinus bradycardia Sinus arrhythmia First degree AVB ST-elevation Tall T waves Increased chamber size Left ventricular
Early repolarization with horizontal ST segment may be associated with aborted sudden cardiac arrest: a retrospective case control study
 Kim et al. BMC Cardiovascular Disorders 2012, 12:122 RESEARCH ARTICLE Open Access Early repolarization with horizontal ST segment may be associated with aborted sudden cardiac arrest: a retrospective case
Kim et al. BMC Cardiovascular Disorders 2012, 12:122 RESEARCH ARTICLE Open Access Early repolarization with horizontal ST segment may be associated with aborted sudden cardiac arrest: a retrospective case
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
3/4/2018. March Martina Frost, PA C Desert Cardiology. Electricity moving towards/away from electrode create downward/upward directions of waves
 March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
J Wave Syndromes. Osama Diab Lecturer of Cardiology Ain Shams University
 J Wave Syndromes Osama Diab Lecturer of Cardiology Ain Shams University J Wave Syndromes Group of electric disorders characterized by > 1 mm elevation of the J point or prominent J wave with or without
J Wave Syndromes Osama Diab Lecturer of Cardiology Ain Shams University J Wave Syndromes Group of electric disorders characterized by > 1 mm elevation of the J point or prominent J wave with or without
Disclosure. 3. ST depression indicative of ischemia is most commonly observed in leads: 1. V1-V2. 2. I and avl 3. V
 Interpreting Stress Induced Ischemia by ECG, Bundle Branch Block & Arrhythmias Disclosure Gregory S Thomas MD, MPH Medical Director, MemorialCare Heart & Vascular Institute, Long Beach Memorial Astellas
Interpreting Stress Induced Ischemia by ECG, Bundle Branch Block & Arrhythmias Disclosure Gregory S Thomas MD, MPH Medical Director, MemorialCare Heart & Vascular Institute, Long Beach Memorial Astellas
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
The New Definition of Early Repolarisation. Peter W. Macfarlane. Institute of Cardiovascular and Medical Sciences University of Glasgow
 1 The New Definition of Early Repolarisation Peter W. Macfarlane Institute of Cardiovascular and Medical Sciences University of Glasgow Address for Correspondence: Electrocardiology Group Level 1, New
1 The New Definition of Early Repolarisation Peter W. Macfarlane Institute of Cardiovascular and Medical Sciences University of Glasgow Address for Correspondence: Electrocardiology Group Level 1, New
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
Current ECG interpretation guidelines in the screening of athletes
 REVIEW ARTICLE 7 How to differentiate physiological adaptation to intensive physical exercise from pathologies Current ECG interpretation guidelines in the screening of athletes Gemma Parry-Williams, Sanjay
REVIEW ARTICLE 7 How to differentiate physiological adaptation to intensive physical exercise from pathologies Current ECG interpretation guidelines in the screening of athletes Gemma Parry-Williams, Sanjay
Conflict of Interest and Funding
 Conflict of Interest and Funding Funding: French National grant («Programme Hospitalier de Recherche Clinique») The authors have no conflicts to declare Outcome of patients with syncope and Early Repolarization
Conflict of Interest and Funding Funding: French National grant («Programme Hospitalier de Recherche Clinique») The authors have no conflicts to declare Outcome of patients with syncope and Early Repolarization
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
Considerations about the polemic J point location
 Considerations about the polemic J point location V) The J-point of the electrocardiogram Approximate point of convergence between the end of QRS complex and the onset of ST segment. It is considered the
Considerations about the polemic J point location V) The J-point of the electrocardiogram Approximate point of convergence between the end of QRS complex and the onset of ST segment. It is considered the
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
J Wave Syndrome: Clinical Diagnosis, Risk Stratification And Treatment Kamal K Sethi,Kabir Sethi,Surendra K Chutani
 J Wave Syndrome: Clinical Diagnosis, Risk Stratification And Treatment Kamal K Sethi,Kabir Sethi,Surendra K Chutani Division of Cardiology and Cardiac Electrophysiology,Delhi Heart & Lung Institute,New
J Wave Syndrome: Clinical Diagnosis, Risk Stratification And Treatment Kamal K Sethi,Kabir Sethi,Surendra K Chutani Division of Cardiology and Cardiac Electrophysiology,Delhi Heart & Lung Institute,New
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director
 December 2018 ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director To obtain best results Select Slide Show from the ribbon at the top of your PowerPoint screen Select From Beginning on the
December 2018 ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director To obtain best results Select Slide Show from the ribbon at the top of your PowerPoint screen Select From Beginning on the
ECG INTERPRETATION MANUAL
 Lancashire & South Cumbria Cardiac Network ECG INTERPRETATION MANUAL THE NORMAL ECG Lancashire And South Cumbria Cardiac Physiologist Training Manual THE NORMAL ECG E.C.G CHECKLIST 1) Name, Paper Speed,
Lancashire & South Cumbria Cardiac Network ECG INTERPRETATION MANUAL THE NORMAL ECG Lancashire And South Cumbria Cardiac Physiologist Training Manual THE NORMAL ECG E.C.G CHECKLIST 1) Name, Paper Speed,
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
Normal ECG And ECHO Findings in Athletes
 Normal ECG And ECHO Findings in Athletes Dr.Yahya Kiwan Consultant Interventional Cardiologist Head Of Departement Of Cardiology Canadian Specialist Hospital Sinus Bradycardia The normal heartbeat is initiated
Normal ECG And ECHO Findings in Athletes Dr.Yahya Kiwan Consultant Interventional Cardiologist Head Of Departement Of Cardiology Canadian Specialist Hospital Sinus Bradycardia The normal heartbeat is initiated
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
/$ -see front matter 2012 Heart Rhythm Society. All rights reserved. doi: /j.hrthm
 Effect of sodium-channel blockade on early repolarization in inferior/lateral leads in patients with idiopathic ventricular fibrillation and Brugada syndrome Hiro Kawata, MD,* Takashi Noda, MD, PhD,* Yuko
Effect of sodium-channel blockade on early repolarization in inferior/lateral leads in patients with idiopathic ventricular fibrillation and Brugada syndrome Hiro Kawata, MD,* Takashi Noda, MD, PhD,* Yuko
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
The Early Repolarization ECG Pattern An Update
 Acta Medica Marisiensis 2017;63(4):165-169 DOI: 10.1515/amma-2017-0032 REVIEW The Early Repolarization ECG Pattern An Update István Adorján Szabó 1, Annamária Fárr 2, Ildikó Kocsis 1, Lehel Máthé 3, László
Acta Medica Marisiensis 2017;63(4):165-169 DOI: 10.1515/amma-2017-0032 REVIEW The Early Repolarization ECG Pattern An Update István Adorján Szabó 1, Annamária Fárr 2, Ildikó Kocsis 1, Lehel Máthé 3, László
A few new tools for better detection and understanding of STEMIs in the field.
 A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Ablative Therapy for Ventricular Tachycardia
 Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Marcin Dada, MD December 03, 2013
 STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
also aid the clinician in recognizing both the obvious and subtle abnormalities that may help guide therapy.
 Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
Notch in ekg st wave
 P ford residence southampton, ny Notch in ekg st wave with tallest R waves. Note high take off of the ST segment in leads V4-6; the ST elevation in V2-3 is generally seen in most normal ECG's; the ST elevation
P ford residence southampton, ny Notch in ekg st wave with tallest R waves. Note high take off of the ST segment in leads V4-6; the ST elevation in V2-3 is generally seen in most normal ECG's; the ST elevation
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart.
 Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart. Hanne Rasmusen Consultant cardiologist, PhD Dept. of Cardiology Bispebjerg University Hospital
Exercise guidelines in athletes with isolated repolarisation abnormalities and structurally normal heart. Hanne Rasmusen Consultant cardiologist, PhD Dept. of Cardiology Bispebjerg University Hospital
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know
 Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Solutions for Every Day Problems Cardiologists and the ECG: Are We Really That Good at It? Part II Daniel José Piñeiro Profesor Titular de Medicina,
 Solutions for Every Day Problems Cardiologists and the ECG: Are We Really That Good at It? Part II Daniel José Piñeiro Profesor Titular de Medicina, Universidad de Buenos Aires, Argentina Member, Membership
Solutions for Every Day Problems Cardiologists and the ECG: Are We Really That Good at It? Part II Daniel José Piñeiro Profesor Titular de Medicina, Universidad de Buenos Aires, Argentina Member, Membership
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
Treatment of VT of Purkinje fiber origin: ablation targets and outcome
 Treatment of VT of Purkinje fiber origin: ablation targets and outcome Ch. Piorkowski University Leipzig - Heart Center - Dept. of Electrophysiology Leipzig, Germany Presenter Disclosure Information Gerhard
Treatment of VT of Purkinje fiber origin: ablation targets and outcome Ch. Piorkowski University Leipzig - Heart Center - Dept. of Electrophysiology Leipzig, Germany Presenter Disclosure Information Gerhard
15 th Sukaman Memorial Lecture ST Segment Elevation: New Electrocardiographic Insights in 2014
 DOI 10.7603/s40602-016-0006-3 ASEAN Heart Journal http://www.globalsciencejournals.com/journal/40602 Vol. 24, no.1, 98 105 (2016) ISSN: 2315-4551 15 th Sukaman Memorial Lecture ST Segment Elevation: New
DOI 10.7603/s40602-016-0006-3 ASEAN Heart Journal http://www.globalsciencejournals.com/journal/40602 Vol. 24, no.1, 98 105 (2016) ISSN: 2315-4551 15 th Sukaman Memorial Lecture ST Segment Elevation: New
2/7/ LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
 12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
The frontier between normal and abnormal electrocardiogram in athletes
 The frontier between normal and abnormal electrocardiogram in athletes ESC Congress 2011 Paris F. Carré University Rennes 1-Pontchaillou Hospital Inserm U642, Rennes - F-35000 Cardiovascular preparticipation
The frontier between normal and abnormal electrocardiogram in athletes ESC Congress 2011 Paris F. Carré University Rennes 1-Pontchaillou Hospital Inserm U642, Rennes - F-35000 Cardiovascular preparticipation
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Signal Processing of Stress Test ECG Using MATLAB
 Signal Processing of Stress Test ECG Using MATLAB Omer Mukhtar Wani M. Tech ECE Geeta Engineering College, Panipat Abstract -Electrocardiography is used to record the electrical activity of the heart over
Signal Processing of Stress Test ECG Using MATLAB Omer Mukhtar Wani M. Tech ECE Geeta Engineering College, Panipat Abstract -Electrocardiography is used to record the electrical activity of the heart over
12 Lead Interpretation
 12 Lead Interpretation Objectives Ischemia, injury and infarction ECG complex review J point ST segment STEMI recognition Ischemia to Infarct Infarction is an evolving process As the infarct evolves ECG
12 Lead Interpretation Objectives Ischemia, injury and infarction ECG complex review J point ST segment STEMI recognition Ischemia to Infarct Infarction is an evolving process As the infarct evolves ECG
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
Prevalence and Characteristics of Early Repolarization in the CASPER Registry
 Journal of the American College of Cardiology Vol. 58, No. 7, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.04.022
Journal of the American College of Cardiology Vol. 58, No. 7, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.04.022
ECG Practice Strips Discussion part 1:
 ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
Understanding basics of EKG
 Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Prevention of Sudden Death in ARVC
 ESC Munich, August 29, 2012 Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC): Prevention of Sudden Death in ARVC Thomas Wichter, MD, FESC Professor of Medicine - Cardiology Marienhospital Osnabrück
ESC Munich, August 29, 2012 Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC): Prevention of Sudden Death in ARVC Thomas Wichter, MD, FESC Professor of Medicine - Cardiology Marienhospital Osnabrück
EKG screening in athletics
 Use of PPE EKG screening in athletics Stefan Montgomery MD, ATC 4/27/18 The overall role of the preparticipation physical evaluation (PPE) is to evaluate the health of the athlete to optimize safe sports
Use of PPE EKG screening in athletics Stefan Montgomery MD, ATC 4/27/18 The overall role of the preparticipation physical evaluation (PPE) is to evaluate the health of the athlete to optimize safe sports
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
Synopsis of Management on Ventricular arrhythmias. M. Soni MD Interventional Cardiologist
 Synopsis of Management on Ventricular arrhythmias M. Soni MD Interventional Cardiologist No financial disclosure Premature Ventricular Contraction (PVC) Ventricular Bigeminy Ventricular Trigeminy Multifocal
Synopsis of Management on Ventricular arrhythmias M. Soni MD Interventional Cardiologist No financial disclosure Premature Ventricular Contraction (PVC) Ventricular Bigeminy Ventricular Trigeminy Multifocal
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Degrees AV blocks in athletes
 Degrees AV blocks in athletes Name: BCA Age: 22yo Sex: Male Race: Black Weight: 82 kg Height: 1.96m Biotype: Athletic rofession: professional basketball player Date: 2/09/2001 Clinical diagnosis: athlete
Degrees AV blocks in athletes Name: BCA Age: 22yo Sex: Male Race: Black Weight: 82 kg Height: 1.96m Biotype: Athletic rofession: professional basketball player Date: 2/09/2001 Clinical diagnosis: athlete
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ELECTROCARDIOGRAPH. General. Heart Rate. Starship Children s Health Clinical Guideline
 General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
Case 1. Case 2. Case 3
 Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Chapter 2 Practical Approach
 Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Electrocardiogram ECG. Hilal Al Saffar FRCP FACC College of medicine,baghdad University
 Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Index. cardiacep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
EHRA/EUROPACE 2011 Madrid, Spain June
 EHRA/EUROPACE 2011 Madrid, Spain June 26.-29.2011 Implementing modern management in atrial fibrillation patients Proceedings from the 3rd AFNet/EHRA consensus conference EHRA Special Session Different
EHRA/EUROPACE 2011 Madrid, Spain June 26.-29.2011 Implementing modern management in atrial fibrillation patients Proceedings from the 3rd AFNet/EHRA consensus conference EHRA Special Session Different
Distinguishing benign from malignant early repolarization : The value of the ST-segment morphology
 Distinguishing benign from malignant early repolarization : The value of the ST-segment morphology Raphael Rosso, MD,* Eran Glikson,* Bernard Belhassen, MD,* Amos Katz, MD, Amir Halkin, MD,* Arie Steinvil,
Distinguishing benign from malignant early repolarization : The value of the ST-segment morphology Raphael Rosso, MD,* Eran Glikson,* Bernard Belhassen, MD,* Amos Katz, MD, Amir Halkin, MD,* Arie Steinvil,
Blocks & Dissociations. Reading Assignment (p47-52 in Outline )
") Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block: