Congenital Heart Disease. Children s Hospital Zhejiang University School of Medicine
|
|
|
- Patrick Harrington
- 6 years ago
- Views:
Transcription

1 Congenital Heart Disease Children s Hospital Zhejiang University School of Medicine

2 Cardiovascular Development Key periods:the 2 nd ~8 th weeks
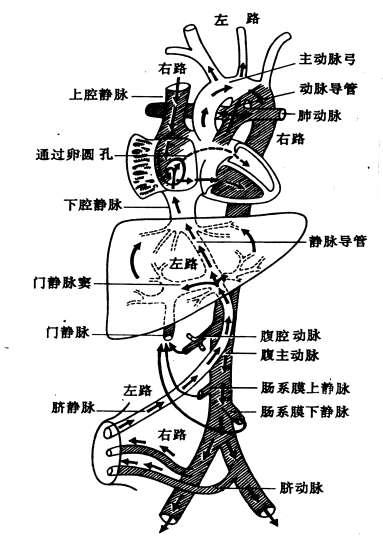
3 Fetal Circulation
4 Physiological Changes in the Circulation After Birth Changes in the pulmonary circulation Closure of the ductus arteriosus Closure of foramen ovale Arrest of circulation through the placenta
5 Epidemiology of Congenital Heart Disease Congenital heart disease occurs in approximately 8 of 1000 live births About 2-3 out of 1000 total newborn infants will be symptomatic with heart disease in the 1st yr of life
6 Etiology The etiology of most specific congenital heart defects is still unknown
7 Genetic Factors: (1) single gene mutation or multifactorial inheritance pattern (2) certain types of VSD (supracristal) are more common in children of Asian background (3) the recurrence risk of congenital heart disease increases from 0.8% to about 2-6% if a 1st degree relative is affected. (4) approximately 3% of patients with congenital heart disease have an identifiable single gene defect, such as Marfan or Noonan syndrome (5) 5-8% of patients with congenital heart disease have an associated chromosomal abnormality: 90% of trisomy 18, 50% of trisomy 21, 40% of Turner syndrome
8 Infective Factors: congenital rubella syndrome Environmental Factors: physical and chemical factors Drug Factors Maternal Diseases: Diabetes mellitus, SLE
9 Classification of Congenital Heart Disease Left to right Shunt Lesions: potential cyanotic CHD (ASD, VSD, PDA) Right to Left Shunt Lesions: cyanotic CHD (TOF, TGA) No Shunt Lesions: acyanotic CHD (PS, AS, COA, MS, MVP)
10 The Common Features of Left to Right Shunt CHD Potential cyanosis Systolic heart murmur in left sternal border (LSB) Pulmonary blood flow increase Systemic blood flow decrease
11 Diagnostic Methods History and Physical Examination ECG Chest X-ray Echocardiography M-mode, two dimension --- morphology Pulsed, continuous wave and colour doppler Transesophageal Echocardiography (TEE) Fetal Echocardiography
12 Catheterization pressure, resistance, oxygen saturation, cardiac output, pathway, angiocardiography, myocardial biopsy, electrophysiologic study, interventional treatment MRI, CT, ECT
13 Treatment in Patients with CHD Non-operation Drug: PGE 1, Indomethacin Interventional treatment Operation
14 Atrial Septal Defect (ASD)
15 Development of Atrial Septum
16 Classification of ASD Ostium Primum Defect (AV Canal or Endocardial Cushion or Atrioventricular septal defect) In the lower portion of the atrial septum and overlies the mitral and tricuspid valves, common with a cleft in the anterior leaflet of mitral valve and mitral regurgitation Ostium Secundum Defect Sinus Venosus Defect Patent foramen ovale Isolated patent foramen ovale is usually of no hemodynamic significance

17 Type of Secundum ASD
18 Pathophysiology of ASD
19 Pathophysiology of ASD SVC IVC ASD LV LA RA RV comparative pulmonary valve stenosis AO PV PA Hyperkinetic pulmonary hypertension extremely large pulmonary blood flow Obstructive pulmonary hypertension pulmonary arteriolar medial thickness pulmonary vascular obstructive disease RVP RAP RAP LAP RA to LA Shunt cyanosis-- Eisenmenger syndrome
20 Pathophysiology of ASD Left to right shunt can occur both in systole and diastole because the LA pressure is always little higher than the RA pressure both in systole and diastole The degree of Left-to-Right shunting is dependent on: 1. size of defect 2. relative compliances of the RV and LV 3. relative vascular resistances in the pulmonary and systemic circulations
21 Pathophysiology of ASD The large blood flow through the right side of the heart results in: l. enlargement of RA and RV and dilatation of PA 2. the pulmonary artery pressure (PAP) remains normal because of the absence of a high pressure communication between the pulmonary and systemic circulations 3. pulmonary vascular resistance remains low throughout childhood, but it may begin to increase in adulthood 4. the LV is normal in size
22 Clinical Manifestations Asymptomatic A soft systolic murmur at the 2nd intercostal space of LSB (increased RV blood flow across the pulmonary valve---comparative pulmonary valve stenosis) Typical wide and fixed splitting of P2 (The pulmonic 2nd heart sound) throughout the respiratory cycle (increased RV blood flow producing a prolonged pulmonary valve close constantly throughout the respiratory cycle)
23 Clinical Manifestations An early-to-mid diastolic murmur at the lower LSB (increased blood flow across the tricuspid valve---- comparative tricuspid valve stenosis) P 2 louder and pulmonic ejection click when pulmonary hypertension





24 Chest X-ray Enlargement of the RA and RV Pulmonary artery is large Pulmonary vascularity is increased LV is normal Enlargement of the LV in Ostium Primum Defect
 Enlargement of the LV in Ostium Primum")
25 ECG Right axis deviation Enlargement of the RA and RV Minor right ventricular conduction delay (ICRBBB: an rsr' pattern in the right precordial leads) Enlargement of the LV in Ostium Primum Defect


26 Echocardiography Enlargement of the RA and RV Ventricular septum and posterior wall of LV move in same direction Position and size of ASD Direction and degree of shunt in ASD
27 Catheterization Oxygen saturation in RA is higher than in SVC and IVC Right cardiac catheter is easy to enter LA through the ASD
28 Prognosis and Complications symptoms usually do not appear until the 3rd decade or later pulmonary hypertension and heart failure are late manifestations infective endocarditis is extremely rare
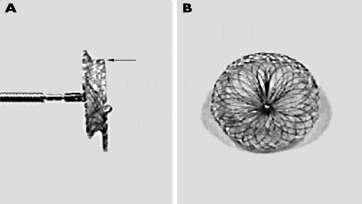
29 Treatment Surgery is advised for all symptomatic patients and also for asymptomatic patients with a shunt ratio of at least 2 : l The timing for elective closure is usually at some time prior to entry school Occlusion devices implanted by interventional cardiac catheterization

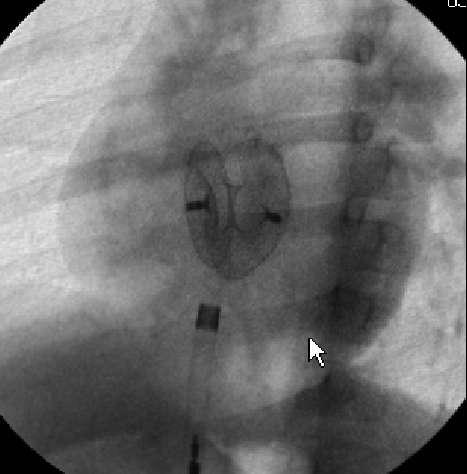
30 Interventional Treatment ASD 封堵器
31 Ventricular Septal Defect (VSD)
32 The most common cardiac malformation accounting for 25-50% of CHD


33 Classification of VSD Membranous VSD most common defect Outlet (supracristal, infundibular, subpulmonary) VSD situated just beneath the pulmonary valve Inlet VSD Muscular VSD
34 Pathophysiology of VSD AO VSD LV RVH PA LA PV Hyperkinetic pulmonary hypertension extremely large pulmonary blood flow Obstructive pulmonary hypertension pulmonary arteriolar medial thickness pulmonary vascular obstructive disease RVP RVP LVP RV to LV Shunt cyanosis-- Eisenmenger syndrome
35 Pathophysiology of VSD The degree of Left-to-Right shunting is dependent on: 1. size of defect 2. pulmonary and systemic vascular resistances Left to right shunt is only in systole because the LV pressure is higher than the RV pressure in systole, and the both pressure is equal in diastole
36 Pathophysiology of VSD The large blood flow through the VSD results in: l. Enlargement of LV and LA (volume overload), dilatation of PA, enlargement of RV when pulmonary hypertension 2. Pulmonary hypertension: early: extremely large pulmonary blood flow Hyperkinetic pulmonary hypertension late: pulmonary arteriolar medial thickness and pulmonary vascular obstructive disease Obstructive pulmonary hypertension When the ratio of pulmonary to systemic resistance approaches 1:1, the shunt become bidirectional, signs of heart failure abate, and the patient becomes cyanosis ---- Eisenmenger syndrome
37 Clinical Manifestations according to the size of defect and the pulmonary blood and pressure
38 Small VSD Asymptomatic A loud, harsh, or blowing holosystolic murmur at the 3rd - 4th intercostal space of LSB with thrill Chest X-ray: normal or minimal cardiomegaly and a borderline increase in pulmonary vasculature ECG: normal or left ventricular hypertrophy
39 Large VSD Dyspnea, feeding difficulties, poor growth, profuse perspiration, recurrent pulmonary infections and cardiac failure in early infancy Prominence of the left precordium and sternum, parasternal lift and systolic thrill A loud, harsh, or blowing holosystolic murmur at the 3rd - 4th intercostal space of LSB P 2 louder when pulmonary hypertension Mid-diastolic, low-pitched rumble at the apex: increased blood flow across the mitral valve

40 Large VSD Chest X-ray: Gross cardiomegaly with prominence of LV, RV, LA and PA Pulmonary vascular markings increase and frank pulmonary edema may be present Aortic knob is small ECG: Biventricular hypertrophy, P waves may be notched or peaked



41 Echocardiography Enlargement of the LA and LV, and RV and PA in patients with pulmonary hypertension Position and size of VSD Direction and degree of shunt in VSD
42 Catheterization Oxygen saturation in RV is higher than in RA RV and PA pressure are normal or increase Right cardiac catheter can enter LV and Aorta through defect in some very large VSD patients

43 Prognosis The natural course of VSD depends to a large degree on the size of the defect 30-50% of small perimembranous and muscular VSD will close spontaneously, most frequently during the 1st yr of life. The vast majority of defects that close will do so before age 4~5 yr. It is less common for moderate or large defects to close spontaneously. Outlet VSD is no possible to close spontaneously
44 Complications The large VSD: repeated episodes of respiratory infection, congestive heart failure (CHF) and failure to thrive, and pulmonary hypertension Infective endocarditis
45 Treatment Small VSD does not need restrictions of physical activity and surgery repair. These patients can be followed by a combination of clinical examinations and noninvasive laboratory tests until the defects has closed spontaneously Large and outlet VSD needs medical management to control CHF and to prevent the development of pulmonary vascular disease, and surgery repair early in patients with pulmonary hypertension

46 Interventional Treatment 肌部 VSD 封堵器

47 Interventional Treatment
48 Patent Ductus Arteriosus (PDA)

49 During fetal life, most of the pulmonary arterial blood is shunted through the ductus arteriosus into the aorta. Functional closure of the ductus normally occurs soon after birth Figure of PDA The aortic end of the ductus is just distal to the origin of the left subclavian artery, and the ductus enters the pulmonary artery at its bifurcation
50 Pathophysiology of PDA PDA AO PA PV LV LA Hyperkinetic pulmonary hypertension extremely large pulmonary blood flow Obstructive pulmonary hypertension pulmonary arteriolar medial thickness pulmonary vascular obstructive disease PAP AOP RVP RVH PA to AO Shunt Low extremity cyanosis (differential cyanosis)--- Eisenmenger syndrome

51 Pathophysiology of PDA Differential Cyanosis
52 Pathophysiology of PDA The degree of Left-to-Right shunting is dependent on: 1. the size of the ductus 2. ratio of pulmonary and systemic vascular resistances Left to right shunt can occur both in systole and diastole because the aortic pressure is always higher than the pulmonary arterial pressure both in systole and diastole
53 Pathophysiology of PDA The large blood flow through the PDA results in: 1. enlargement of LV and LA (volume overload), dilatation of PA, enlargement of RV when pulmonary hypertension 2. pulmonary hypertension: early: extremely large pulmonary blood flow --- Hyperkinetic pulmonary hypertension late: pulmonary arteriolar medial thickness and pulmonary vascular obstructive disease --- Obstructive pulmonary hypertension 3. when the ratio of pulmonary to systemic resistance approaches 1:1, the shunt becomes bidirectional, signs of heart failure abate, and the patient becomes cyanosis (differential cyanosis) --- Eisenmenger syndrome
54 Pathophysiology of PDA Small PDA: PAP, RVP and RAP are normal Large PDA: PAP may be elevated to systemic levels during both systole and diastole
55 Clinical Manifestations According to the size of the ductus: Small PDA: Asymptomatic Large PDA: poor feeding and retardation of physical growth, sometimes with hoarseness
56 Clinical Manifestations Prominence of the left precordium and apical impulse in large PDA Wide pulse pressure ( 40 mmhg) and bounding arterial pulse: peripheral blood vessel sign due to runoff of blood into pulmonary artery during diastole Thrill, maximal in the 2nd left intercostal space, may radiate toward the left clavicle, down LSB or toward apex, usually in systole, but also may be throughout the cardiac cycle
57 Clinical Manifestations Classic murmur: 1. Continuous, machinery and rolling thunder murmur 2. Begining soon after onset of the 1st sound, reaches maximal intensity at the end of systole, and wanes in late diastole 3. Located at the 2nd left intercostal space and radiate down the LSB or to left clavicle 4. When pulmonary vascular resistance increases or heart failure, the diastolic component of the murmur may be less prominent or absent


58 Chest X-ray Prominent pulmonary artery with increased intrapulmonary vascular markings Normal or minimal cardiomegaly in small PDA and marked cardiomegaly in large PDA. The chambers involved are LA and LV, and RV when pulmonary hypertension Aortic knob is prominent

59 ECG normal in small PDA left ventricular or biventricular hypertrophy in large PDA



60 Echocardiography enlargement of the LA and LV, and RV and PA in patients with pulmonary hypertension position, shape and size of PDA direction and degree of shunt in PDA
61 Catheterization 1. Oxygen saturation in PA is higher than in RV 2. RV and PA pressure are normal or increase 3. Right cardiac catheter can enter descending aorta through PDA in most of patients 4. Angiocardiography is needed in some patients with very tiny PDA
62 Prognosis and Complications The patients with a small PDA may live a normal span with few or no cardiac symptoms Spontaneous closure of the ductus after infancy is extremely rare The repeated episodes of respiratory infection, congestive heart failure, failure to thrive and pulmonary hypertension are common in large PDA Infective endocarditis may be seen at any age, pulmonary and systemic emboli may occur Aneurysmal dilatation of the pulmonary artery or the ductus
63 Treatment PDA in premature infant: indomethacin Irrespective of age, patients with PDA require treatment (including surgical and interventional closure) in order to prevent infective endocarditis, congestive heart failure and the development of pulmonary vascular disease


64 Interventional Treatment
65 Eisenmenger syndrome 艾森曼格综合征 Those patients with left to right shunt (VSD, PDA, ASD, et) whose shunts have become partially or totally right to left as a result of the development of pulmonary vascular disease 所有左向右分流的先天性心脏病 (ASD VSD PDA 等 ) 由于器质性肺血管病变导致梗阻性肺动脉高压, 右心系统压力等于或超过左心系统, 出现双向或右向左分流
66 Tetralogy of Fallot (TOF)
 Right ventricular")
67 Pathophysiology Obstruction to right ventricular outflow tract (infundibular stenosis) -- the most important malformation (sometimes with pulmonary valve and artery stenosis) Ventricular septal defect large and nonrestrictive VSD just below the aortic valve Override of the aorta (dextroposition of the aorta in 25% patients) Right ventricular hypertrophy
68 Pathophysiology The degree of right ventricular outflow obstruction determines the timing of onset of symptoms, the severity of cyanosis, and the degree of right ventricular hypertrophy The degree of right ventricular outflow obstruction and override of the aorta can become more and more severe with growth
69 Pathophysiology of TOF Obstruction to right ventricular outflow tract Spasm of Stenotic Infundibulum RVP Hypoxic Spells RVP LVP Pulmonary Blood Flow Collateral Artery From DAO RVH VSD Override of the aorta RV to LV Shunt Gas Exchange in Lung AO Blood from LV and RV Artery Oxygen Saturation Cyanosis Polycythemia Clubbing Squatting Cerebral thromboses Brain abscess
70 Clinical Manifestations Cyanosis Often is not present at birth, but with increasing hypertrophy of the RV infundibulum and growth, cyanosis occurs later in the 1st yr of life It is most prominent in the mucous membranes of the lips and mouth, and in the fingernails and toenails In infants with severe RV outflow obstruction, cyanosis is noted immediately in the neonatal period
71 Clinical Manifestations Paroxysmal hypercyanotic attacks (hypoxic spells) 1. Spasm of stenotic infundibulum pulmonary blood flow most of all RV blood into aorta severe systemic hypoxia and metabolic acidosis 2. A particular problem during the first 2 yr of life 3. Hyperpneic, restless, cyanosis increases, gasping respirations ensue and syncope
72 Clinical Manifestations 4. Frequently in the morning upon first awakening or following episodes of vigorous crying 5. Temporary disappearance or decrease in intensity of the systolic murmur due to the decrease of flow across the RV outflow tract 6. Last a few minutes or hours, rarely fatal. Followed by generalized weakness and sleep. Sevre spells may progress to anconsciousness and mnvulsions or hemiparesi
73 Clinical Manifestations Clubbing of fingers and toes Dyspnea and Squatting l. Squatting systemic artery pressure and resistance increase LVP increase 2. Squatting venous return decrease RVP decrease l, 2 Right to left shunt decrease through VSD and hypoxia can be improved Growth and development may be delayed in patients with severe untreated tetralogy of Fallot
74 Clinical Manifestations Left anterior hemithorax may bulge anteriorly due to RV hypertrophy Substernal right ventricular impulse Systolic thrill in the 3rd and 4th parasternal spaces along LSB in 50% cases
75 Clinical Manifestations Systolic Murmur 1. ejection or holosystolic, loud and harsh 2. most intense in the 2nd -4th intercostal space of LSB 3. caused by turbulence through the RV outflow tract due to the infundibular stenosis The 2nd heart sound is single or the pulmonic component is soft




76 Chest X-ray Narrow base, concavity of pulmonary artery and normal heart size Rounded apical shadow above the diaphragm than normal Pulmonary vascular marking decrease Large aorta and 25% cases with dextroposition of aortic arch Cardiac silhouette boot or wooden shoe

77 ECG Right axis deviation and RVH


78 Echocardiography The aorta widen and override on the large ventricular septal defect Obstruction to right ventricular outflow tract (infundibular stenosis) Right ventricular hypertrophy Left ventricular is small

79 Cardiac Catheterization and Angiocardiography RVP increases and equals to the LVP Oxygen saturation in Ao and LV decreases Angiocardiography in RV and LV can show the position and size of VSD, size of LV, width and overriding degree of aorta, and degree of obstruction of RVOT, et.
80 Prognosis and Complications Cerebral thromboses 1. usually in cerebral veins, occasionally in cerebral arteries 2. common in the presence of extreme polycythemia and dehydration under the age of 2 yr Brain abscess usually over the age of 2 yr Bacterial endocarditis Congestive heart failare unusually in TOF
81 Treatment of hypoxic spells Depending on the frequency and severity of hypercyanotic attacks, one or more of the following procedures should be instituted in sequence: 1. Knee-chest position 2. Administration of oxygen 3. injection of morphine subcutaneously in a dose not in excess of 0.2 mg/kg 4. Correction of metabolic acidosis with intravenous administration of sodium bicarbonate if the spell is unusually severe and there is lack of response to the foregoing therapy 5. β- Adrenergic blockade by intravenous administration of propranolol (0.1 to a maximum of 0.2 mg/kg) 6. Drugs that increase systemic vascular resistance, such as intravenous methoxamine or phenylephrine, decrease the right-to-left shunt
82 Treatment of TOF Depend on the severity of the RVOT obstruction palliative surgery total correction
83 Thank You 谢谢
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease. Mohamed Waheed Elsharief.
 Congenital Heart Disease Mohamed Waheed Elsharief. Objectives l By the end of this lecture you should be able to Fetal Circulation l For the fetus the placenta is the oxygenator so the lungs do little
Congenital Heart Disease Mohamed Waheed Elsharief. Objectives l By the end of this lecture you should be able to Fetal Circulation l For the fetus the placenta is the oxygenator so the lungs do little
بسم هللا الرحمن الرحيم. The cardio vascular system By Dr.Rawa Younis Mahmood
 بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Most common fetal cardiac anomalies
 Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Pediatric Board Review Congenital Heart Disease. Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University
 Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Paediatric Cardiology. Acyanotic CHD. Prof F F Takawira
 Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Congenital Heart Disease: Cyanotic Lesions. Amitesh Aggarwal
 Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Ummeenatrbilaoiasetptiwmsaiiri
 atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray
 Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acyanotic Congenital Heart Lesions. These podcasts are designed to give medical students an overview of key topics in
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acyanotic Congenital Heart Lesions. These podcasts are designed to give medical students an overview of key topics in
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
Clinical significance of cardiac murmurs: Get the sound and rhythm!
 Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
DORV: The Great Chameleon. Heart Conference October 15, 2016 Tina Kwan, MD
 DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
List of Videos. Video 1.1
 Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Cases in Adult Congenital Heart Disease
 Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cardiac Ausculation in the Elderly
 Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
What s That Sound? Pediatric Murmur Evaluation
 What s That Sound? Pediatric Murmur Evaluation Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director, Pediatric
What s That Sound? Pediatric Murmur Evaluation Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director, Pediatric
Heart sounds and murmurs. Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct
 Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
Cardiac Examination. Pediatrics Clinical Examination
 Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
Surgical Management Of TAPVR. Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital
 Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Atrial Septal Defect Closure. Stephen Brecker Director, Cardiac Catheterisation Labs
 Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ
 ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ European Accreditation in TTE, TEE and CHD Echocardiography NOTHING TO DECLARE ATRIAL SEPTAL DEFECT TYPES SECUNDUM
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ European Accreditation in TTE, TEE and CHD Echocardiography NOTHING TO DECLARE ATRIAL SEPTAL DEFECT TYPES SECUNDUM
Notes: 1)Membranous part contribute in the formation of small portion in the septal cusp.
Membranous part contribute in the formation of small portion in the septal cusp.") Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Nursing Care of Children and their Families: Alterations in Cardiac Function
 Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE. Sampling Rate M-Mode: 1800 / sec 2D: 30 / sec
 M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS
 Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS iib6@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition
Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS iib6@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition
Neonatal Cardiac Assessment and Congenial Heart Disease compiled by Violet Stephens based on the works of Patricia Hartley
 Neonatal Cardiac Assessment and Congenial Heart Disease compiled by Violet Stephens based on the works of Patricia Hartley Course Contents Purpose Objectives Introduction Fetal Circulation Neonatal Circulation
Neonatal Cardiac Assessment and Congenial Heart Disease compiled by Violet Stephens based on the works of Patricia Hartley Course Contents Purpose Objectives Introduction Fetal Circulation Neonatal Circulation
TGA atrial vs arterial switch what do we need to look for and how to react
 TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Cardiovascular Pathophysiology:
 Learning Objectives Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS iib6@columbia.edu Learn the relationships between pressure, blood flow, and resistance Review the transition
Learning Objectives Cardiovascular Pathophysiology: Left To Right Shunts Ismee A. Williams, MD, MS iib6@columbia.edu Learn the relationships between pressure, blood flow, and resistance Review the transition
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5
 DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
Stenosis of Pulmonary Veins
 Stenosis of Pulmonary Veins Report of a Patient Corrected Surgically Yasunaru Kawashima, M.D., Takeshi Ueda, M.D., Yasuaki Naito, M.D, Eiji Morikawa, M.D., and Hisao Manabe, M.D. ABSTRACT A 15-year-old
Stenosis of Pulmonary Veins Report of a Patient Corrected Surgically Yasunaru Kawashima, M.D., Takeshi Ueda, M.D., Yasuaki Naito, M.D, Eiji Morikawa, M.D., and Hisao Manabe, M.D. ABSTRACT A 15-year-old
Anomalous muscle bundle of the right ventricle
 British Heart Journal, 1978, 40, 1040-1045 Anomalous muscle bundle of the right ventricle Its recognition and surgical treatment M. D. LI, J. C. COLES, AND A. C. McDONALD From the Department of Paediatrics,
British Heart Journal, 1978, 40, 1040-1045 Anomalous muscle bundle of the right ventricle Its recognition and surgical treatment M. D. LI, J. C. COLES, AND A. C. McDONALD From the Department of Paediatrics,
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Case submission for CSI Asia-Pacific Case 2
 Case submission for CSI Asia-Pacific 2018- Case 2 Title Page Case category: Coarctation and ducts, valves Title: Simultaneous balloon aortic valvuloplasty with transcatheter closure of large hypertensive
Case submission for CSI Asia-Pacific 2018- Case 2 Title Page Case category: Coarctation and ducts, valves Title: Simultaneous balloon aortic valvuloplasty with transcatheter closure of large hypertensive
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
RVOTO adult and post-op
 Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Anomalous Systemic Venous Connection Systemic venous anomaly
 World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing. 5. Intensity 2. Shape. 6. Pitch 3. Location of maximum intensity
 Definition Items in description of Timing Shape Location of maximum intensity Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing 5. Intensity 2. Shape 6. Pitch 3. Location of maximum
Definition Items in description of Timing Shape Location of maximum intensity Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing 5. Intensity 2. Shape 6. Pitch 3. Location of maximum
AMERICAN ACADEMY OF PEDIATRICS 993 THE NATURAL HISTORY OF CERTAIN CONGENITAL CARDIOVASCULAR MALFORMATIONS. Alexander S. Nadas, M.D.
 AMERICAN ACADEMY OF PEDIATRICS 993 tnicular overload is the major problem and left ventricular failure occurs. Since for many years the importance of hepatomegaly in the diagnosis of cardiac failure has
AMERICAN ACADEMY OF PEDIATRICS 993 tnicular overload is the major problem and left ventricular failure occurs. Since for many years the importance of hepatomegaly in the diagnosis of cardiac failure has
The blue baby. Case 4
 Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Pattern of Congenital Heart Disease A Hospital-Based Study *Sadiq Mohammed Al-Hamash MBChB, FICMS
 Pattern of Congenital Heart Disease A Hospital-Based Study *Sadiq Mohammed Al-Hamash MBChB, FICMS ABSTRACT Background: The congenital heart disease occurs in 0,8% of live births and they have a wide spectrum
Pattern of Congenital Heart Disease A Hospital-Based Study *Sadiq Mohammed Al-Hamash MBChB, FICMS ABSTRACT Background: The congenital heart disease occurs in 0,8% of live births and they have a wide spectrum
Murmurs and the Cardiac Physical Exam. Carolyn A. Altman Texas Children s Hospital Advanced Practice Provider Conference Houston, TX April 6, 2018
 Murmurs and the Cardiac Physical Exam Carolyn A. Altman Texas Children s Hospital Advanced Practice Provider Conference Houston, TX April 6, 2018 The Cardiac Physical Exam Before applying a stethoscope..
Murmurs and the Cardiac Physical Exam Carolyn A. Altman Texas Children s Hospital Advanced Practice Provider Conference Houston, TX April 6, 2018 The Cardiac Physical Exam Before applying a stethoscope..
SPECIFIC HEART DEFECTS
 A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
THE SOUNDS AND MURMURS IN TRANSPOSITION OF THE
 Brit. Heart J., 25, 1963, 748. THE SOUNDS AND MURMURS IN TRANSPOSITION OF THE GREAT VESSELS BY BERTRAND WELLS From The Hospital for Sick Children, Great Ormond Street, London W. C.J Received April 18,
Brit. Heart J., 25, 1963, 748. THE SOUNDS AND MURMURS IN TRANSPOSITION OF THE GREAT VESSELS BY BERTRAND WELLS From The Hospital for Sick Children, Great Ormond Street, London W. C.J Received April 18,
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
CARDIAC EXAMINATION MINI-QUIZ
 CARDIAC EXAMINATION MINI-QUIZ 1. Sitting bolt upright, your dyspneic (short of breath) patient has visible jugular venous pulsations to the angle of his jaw, which is 12 cm above his sternal angle. What
CARDIAC EXAMINATION MINI-QUIZ 1. Sitting bolt upright, your dyspneic (short of breath) patient has visible jugular venous pulsations to the angle of his jaw, which is 12 cm above his sternal angle. What
Pathological physiology of cardiovascular system Congenital heart diseases
 Pathological physiology of cardiovascular system Congenital heart diseases Rácz Oliver, Sedláková Eva Institute of Pathological Physiology, Medical School, P.J. Šafárik University Oliver Rácz, Eva Sedláková
Pathological physiology of cardiovascular system Congenital heart diseases Rácz Oliver, Sedláková Eva Institute of Pathological Physiology, Medical School, P.J. Šafárik University Oliver Rácz, Eva Sedláková