Recent advances in the management of pulmonary embolism. Kodati Rakesh SR Pulmonary medicine
|
|
|
- Abner Bishop
- 6 years ago
- Views:
Transcription
1 Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine
2 Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies IVC filter Subsegmental PE
3 Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies IVC filter Subsegmental PE
4 Clinical decision rules Dyspnoea at rest or on exertion, pleuritic chest pain, haemoptysis and syncope None are specific for the presence of PE Clinical decision rules (CDRs) standardize the diagnostic approach identify patients in whom a less or more extensive diagnostic work-up is required have been validated and introduced in clinical practice
5 Clinical decision rules
6 Clinical decision rules

7 Clinical decision rules % < 1 % Prometheus Study Group, Douma RA et al, Ann Intern Med. 2011
8 11 studies were included Sensitivity Specificity Wells score 63.8 to 79.3 % 48.8 to 90 % Revised Geneva score 55.3 to 73.6 % 51.2 to 89 % Wells score was more effective than the revised Geneva score in discriminate PE in suspected patients Jun-Hua Shen et al, J Thromb Thrombolysis 2016
9 D- dimer testing Highly sensitive D dimer assays (ELISA, ELFA or latex quantitative assay) Sensitivity is over 95 % Specificity is % Normal D-dimer level excludes acute PE with either a low or a moderate pre-test probability (rule out) Not useful for confirmation of PE
10 D- dimer testing Conventional cut-off of 500 μg/l combined with a unlikely clinical probability can safely rule out the diagnosis in upto 1/3 rd of patients with suspected PE Specificity decreased markedly with age, from 67% in those 40 years old to 10% in those 80 years old Douma RA et al; BMJ 2010
11 Doubling of D dimer Prospective non interventional study in 4 centres of US Of 678 patients enrolled, 126 (19%) were PE+ and 93 (14%) had pneumonia RGS 6 and threshold < 500 ng /ml (n = 678) Exclusion rate PE (16%) 4/110 (3.8%) RGS 6 and a threshold < 1000 ng / ml Increase in specificity from 19.2 % to 35.7 % 208 (31%) 11/208 (5.3%) (10 of these 11 had isolated, subsegmental filling defects ) Doubling the threshold for a positive D-dimer with a PE unlikely probability could reduce CTPA scanning with a slightly increased risk of missed isolated subsegmental PE Kline JA et al; J Thromb Haemost 2012

12 Age adjusted D dimer Douma RA et al; BMJ 2010
13 Age adjusted D dimer New age dependent D-dimer cut-off point in patients aged > 50 years in a derivation set based on ROC curves (Patient s age 10) μg/l in patients aged >50 years Douma RA et al; BMJ 2010
14 Age adjusted D dimer All patients >80 No (%) of patients (14) 211 (16) 265 (20) 198 (15) No. below conventional cutoff value No. below age adjusted cut-off value Absolute increase in % Relative increase in % 477 (36 %) 97 (51) 63 (30) 40 (15) 11 (6) 560 (42%)` 102 (54) 76(36) 75 (28) 41 (21) Douma RA et al; BMJ 2010
15 Age adjusted D dimer Multicenter, prospective management outcome study in 19 centres of Europe Objective Interventions Follow up Outcome To prospectively validate whether an age-adjusted D-dimer cutoff, is associated with an increased diagnostic yield of D-dimer in elderly patients with suspected PE Sequential diagnostic strategy Clinical probability (simplified Geneva score / 2-level Wells score) Highly sensitive D-dimer measurement & CTPA D-dimer value between the conventional cutoff of 500 μg/l and their age-adjusted cutoff did not undergo CTPA and were left untreated and formally followed-up for a 3-month period Failure rates of this diagnostic strategy Thromboembolic risk in the subgroup between conventional and age related cut off Marc Righini et al, The ADJUST-PE Study; JAMA 2014
16 Age adjusted D dimer Multicenter, prospective management outcome study in 19 centres of Europe (n = 3324) D-Dimer Level Lower Than 500 μg/l (n =810) D-Dimer Level Between 500 μg/l and the Age-Adjusted Cutoff (n =331) Age > 75 years and PE unlikely (n =673) 2 deaths and 8 suspected VTE during follow-up 1 adjudicated VTE (0.1 %) 7 deaths and 7 suspected VTE during follow-up 1 adjudicated VTE (0.3%) 43 conventional (6.4%) 200 age adjusted cut off (29.7 %) No confirmed VTE Marc Righini et al, The ADJUST-PE Study; JAMA 2014
17 Age adjusted D dimer Age-adjusted cutoff increased 5-fold the proportion of patients in whom PE could be ruled out without further imaging in patients 75 years or older Improvement of cost-effectiveness or quality of care remains yet to be demonstrated Marc Righini et al, The ADJUST-PE Study; JAMA 2014
18 Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies IVC filter Subsegmental PE
19 Outpatient anticoagulation Introduction of LMWHs and DOACs has enabled early discharge or even complete out of hospital treatment for VTE Lead to patient satisfaction Reduced health care costs Less iatrogenic complications in hospital
20 Outpatient anticoagulation Various parameters were used in selecting home treatment Hestia criteria NT probnp level PESI Preferable method for low risk patient selection is unclear
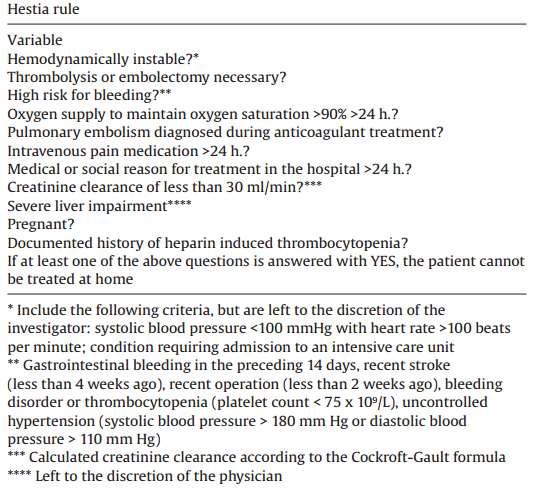
21 Outpatient anticoagulation
22 Outpatient anticoagulation Meta analysis (Wendy Zondag et al, ERJ 2013) 13 studies (1657 patients) No statistical significance in outpatient vs inpatient Rate of recurrent VTE (1.7 vs 1.2 %) mortality (1.9 vs 0.74 %) major bleeding events (0.97 vs 1 %) Home treatment or early discharge of selected low-risk patients with PE is as safe as inpatient treatment
23 Outpatient anticoagulation To compare the safety of the Hestia criteria alone with the Hestia criteria combined with NT-proBNP testing den Exter PL et al; AJRCCM 2016 Randomized non-inferiority trial 17 Dutch hospitals 550 patients NT pro BNP group 34/275 elevated levels Primary endpoint (30 days) 0% Direct discharge 275 subjects 1.1 % Assessment of outpatient eligibility could be based on a clinical decision rule alone, irrespective of NT-proBNP levels proportion of patients with elevated NT-proBNP levels was considerably lower
24 Outpatient anticoagulation PM Roy et al, J Thromb Haemost 2017 Study design Retrospective cohort study inpatients vs 505 outpatients* Primary outcome 14 day rate of adverse events 13.0 % vs 3.3 % OR month rate of adverse events 21.7 % vs 6.9 % OR 4.9 High risk (PESI III/IV) 16.5 % vs 4.5 % OR 4.16 * patients discharged directly from the emergency room and patients discharged within 48 hours of admission.
25 Outpatient anticoagulation Hospitalized normotensive patients have a higher risk of recurrent VTE, major bleedings or deaths than patients managed as outpatient Immobilisation in hospital Couldn't analyse the comorbidites in in-patient *Opinion of the physician in charge, underlying medical and social conditions and how outpatient care provided are more important than severity criteria, to define out patient Rx PM Roy et al, J Thromb Haemost 2017
26 Outpatient anticoagulation In patients with low-risk PE and whose home circumstances are adequate, we suggest treatment at home or early discharge over standard discharge (Grade 2B) *Grade 2B recommendation, CHEST 2016
27 Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies IVC filter Subsegmental PE
28 Thrombolysis in PTE Systemic thrombolytic therapy accelerates resolution of PE as evidenced by more rapid lowering of pulmonary artery pressure increases in arterial oxygenation resolution of perfusion defects
29 Thrombolysis in PTE Net mortality benefit has been uncertain Depends on an individual patient s baseline risk of dying from acute PE and risk of bleeding Young patients are less likely to suffer major bleeding, but might also be more able than the elderly to overcome the right ventricle strain and vice versa
30 Thrombolysis in PTE 4 meta-analyses in 2014 Efficacy and safety of thrombolysis Slightly different conclusions among them Cao et al and Nakamura et al Stable PE Thrombolysis failed to improve overall mortality or recurrent PE with similar risk of major bleeding Marti et al and Chatterjee et al All PE studies combined Significant reduction in overall mortality with thrombolysis
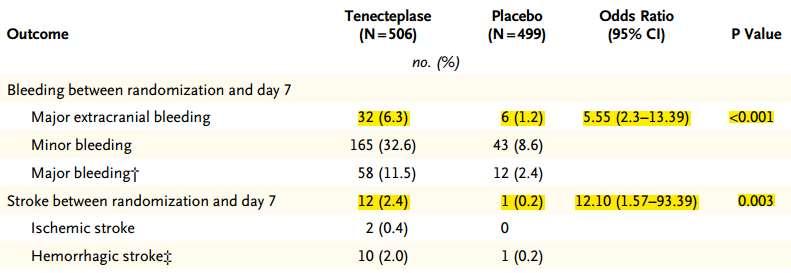
31 Thrombolysis in PTE Large clinical trial of 1005 subjects in 2014 Double blind placebo controlled trial Objectively confirmed normotensive acute PE with an onset below 15 days RV dysfunction on ECHO/CT scan (RV/LV diameter >0.9, RV free wall HK, tricuspid systolic velocity >2.6m/s, RV EDd > 30 mm)) Myocardial injury by positive Troponin T/I Guy Meyer et al; PEITHO trial, NEJM 2014
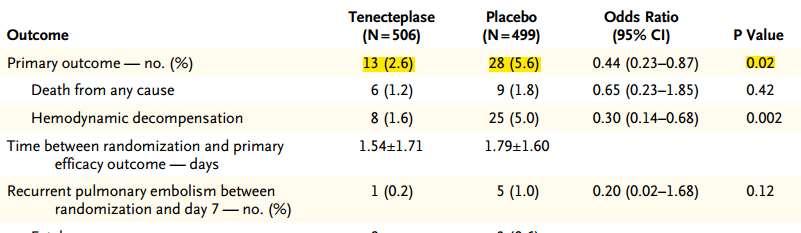
32 Thrombolysis in PTE
33 Thrombolysis in PTE
34 Thrombolysis in PTE In intermediate-risk pulmonary embolism, fibrinolytic therapy prevented hemodynamic decompensation but increased the risk of major hemorrhage and stroke Great caution is warranted when considering fibrinolytic therapy for hemodynamically stable patients with pulmonary embolism (> 75 years and female gender) Guy Meyer et al; PEITHO trial, NEJM 2014
35 Safe dose thrombolysis Randomized, single- centre open study that enrolled 121 adult patients Symptomatic moderate PE CT scan > 70 % involvement of thrombus in 2 lobar or left or right MPA [or] High probability V/Q scan showing mismatch in 2 lobes RV enlargement or hypokinesia and elevation of biomarkers of RV injury although measured, were not a requirement for enrollment Mohsen sharifi et al, MOPETT trial, Am J Cardiol 2013
36 Safe dose thrombolysis Dose of tpa was 50% of the standard dose (100 mg) 50 kg, the total dose was 50 mg < 50 kg, the total dose was calculated as 0.5 mg/kg 10 mg was given as bolus f/b remainder within 2 hrs Mohsen sharifi et al, MOPETT trial, Am J Cardiol 2013
37 Safe dose thrombolysis Mohsen sharifi et al, MOPETT trial, Am J Cardiol 2013
38 Safe dose thrombolysis Mohsen sharifi et al, MOPETT trial, Am J Cardiol 2013
39 Thrombolysis in PTE Wang TF et al; Blood 2015
40 Thrombolysis in PTE Wang TF et al; Blood 2015
41 Thrombolysis in PTE Wang TF et al; Blood 2015
42 Thrombolysis in PTE Thrombolysis reduced overall mortality in all PE but not in stable PE with clearly defined RVD* Systemic thrombolytic therapy is associated with a significant reduction of overall mortality in patients with PE, but this reduction is not statistically significant after exclusion of studies including high-risk PE Consistently increased major bleeding and intracranial bleeding events *Wang TF et al; Blood 2015 Christophe Marti et al; Eur Heart J 2015
43 Thrombolysis in PTE In patients with acute PE associated with hypotension (SBP <90 mm Hg) who do not have a high bleeding risk, we suggest systemically administered thrombolytic therapy over no such therapy (Grade 2B) In most patients with acute PE not associated with hypotension, we recommend against systemically administered thrombolytic therapy (Grade 1B) Antithrombotic Therapy for VTE Disease, CHEST 2016; 149(2)
44 Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies IVC filter Subsegmental PE
45 Choice of anticoagulation Direct oral anticoagulants are now the preferred agents for long-term anticoagulation in patients who are not pregnant do not have active cancer severe renal insufficiency *Grade 2B recommendation, CHEST 2016
46 NOACs Direct thrombin inhibitors Dabigatran Oral Xa inhibitors Rivaroxaban Apaxiban Edoxaban
47 NOACs Large phase III clinical trials comparing VKAs with NOACs for VTE Non inferiority trials Similar efficacy Lower risk of bleeding
48 Study Design Intervention Primary outcome Safety outcome RE COVER 1 Acute VTE UFH or LMWH for 8 2.4% In dabigatran Major bleed 1.6% vs. NEJM to 11 days f/b group 1.9% Randomized Dabigatran 150mg BD HR 0.82 Double blind ( ) Double dummy 0r warfarin (INR 2-3) 2.1% in warfarin Non-inferiority trial group Any bleed 16.1% vs. HR 1.10 ( ) 21.9% RE-COVER 2 Acute VTE UFH or LMWH for 5 2.3% In dabigatran Any bleed 15.6% vs patients to 11 days f/b group 22.1% (Circulation Dec (20% Asians) Dabigatran 150mg BD 2014) Randomized 0r warfarin (INR 2-3) 2.2% in warfarin Major bleed 1.2% vs. Double blind group 1.7% Double dummy HR 1.08 ( ) HR 0.73 Non-inferiority trial ( )
49 Study Design Intervention Primary outcome Safety outcome EINSTEIN PE N Engl J Med 366;14 April 5, patients Randomized Open label Non-inferiority trial Rivaroxaban 15 mg BD 3 weeks f/b 20 mg OD Enoxaparin sc f/b warfarin/acenocoumarol 2.1% vs. 1.8% HR 1.12 ( ) Any bleed 10.3% vs. 11.4% Major bleed 1.1% vs. 2.2% HR 0.49 ( ) AMPLIFY Acute VTE Apixaban 10 mg BD 7 2.3% vs. 2.7% Any bleed 4.3% vs patients days f/b 5 mg BD for 6 9.7% N Engl J Med. Aug months (Significant reduction) 2013; 369(9) Randomized Vs. Double blind Enoxaparin sc for 7 days Non-inferiority trial f/b warfarin (INR 2-3) Hokusai VTE study 4921 DVT patients Initial LMWH f/b 3.2% vs. 3.5% Clinically relevant 3319 PTE patients Edoxaban 60 mg OD bleed 8.5% vs. 10.3% J Thromb Hemost (30 mg-crcl < o13 online ; 1 (17) Randomized ml/m) (symptomatic Double blind Vs. recurrent VTE)
50 NOACs First recurrent VTE or VTE related death, Heterogeneity: I 2 = 0%; P =.53 Nick van Es et al, Blood, 2014
51 NOACs Bleeding, Heterogeneity: I 2 = 51 %; P =.07 Nick van Es et al, Blood, 2014
52 NOACs avoided in.. Severe renal failure Mechanical heart valves Concomitant and indispensable use of drugs that are strong inhibitors or inducers of P- glycoprotein and/or CYP 3A4 Caution in patients with extreme body weights
53 Choice of anticoagulation LMWH was suggested over VKA therapy or DOACs in patients with DVT of the leg or PE and cancer ( cancer-associated thrombosis ) *Grade 2C recommendation, CHEST 2016
54 Choice of anticoagulation in cancer LMWH was more effective than VKA in patients with cancer Substantial rate of recurrent VTE in patients cancer who are on VKA Difficulty of keeping VKA in therapeutic range Difficulty with oral therapy (eg, vomiting) Easier to withhold or adjust for invasive interventions or thrombocytopenia develops
55 Choice of anticoagulation in cancer CLOT trial 2003 Dalteparin Vs Warfarin in DVT, PE in cancer 672 subjects 27 of 336 vs 53 of 336 (P=0.002) No difference in bleeding In patients with cancer and acute VTE, dalteparin was more effective than an coumarin in reducing the risk of recurrent VTE without increasing the risk of bleeding Agnes YY Lee et al; N Engl J Med 2003;349
56 Choice Study of Design anticoagulation Intervention Primary in cancer Safety outcome outcome CATCH trial Randomized Tinzaparin Recurrent VTE Major bleed JAMA 2015;314(7) Open label trial 900 patients with active cancer & documented 175 IU/kg OD for 6 months vs Tinzaparin for 5 to 10 days f/b 31/449 vs 45/ % vs 10 % (p = 0.07) HR [95% CI, ] 2.7 % vs 2.4 % Non major bleed 10.9 % vs 15.3 % (P = 0.004) proximal DVT warfarin at a INR or PE, with a life ( ) for 6 m expectancy > 6 months
57 Choice of anticoagulation in cancer Agnes YY Lee et al; JAMA 2015;314(7)
58 Choice of anticoagulation in cancer Role of NOACs in cancer related VTE Clinically attractive drugs for the treatment in v/o their fixed-dose regimens and oral administration Systematic review and meta analysis 2015 Subgroup analyses of RCTs which included very few and highly selected patients with cancer
59 Choice of anticoagulation in cancer VTE Recurrence in cancer Maria Cristina Vedovati et al, CHEST 2015; 147(2):
60 Choice of anticoagulation in cancer Major bleeding with NOACs Maria Cristina Vedovati et al, CHEST 2015; 147(2):
61 Choice of anticoagulation in cancer Analysis is not powered to show differences among individual agents No studies specific to the cancer population have been conducted so far No trials of NOACs comparing with LMWH available, which is the standard of care Maria Cristina Vedovati et al, CHEST 2015; 147(2):
62 Duration of anticoagulation PE provoked by surgery or non surgical transient risk factors recommended for 3 months First unprovoked PE Low or moderate bleeding risk suggested extended therapy High bleeding risk 3 months recommended Antithrombotic Therapy for VTE Disease, CHEST 2016; 149(2)
63 Duration of anticoagulation Second unprovoked PE Low risk recommend extended Moderate risk suggest extended High risk suggest 3 months In all patients who receive extended anticoagulant therapy, the continuing use of treatment should be reassessed at periodic intervals Antithrombotic Therapy for VTE Disease, CHEST 2016; 149(2)
64 PADIS - PE trial JAMA 2015;314(1) Study Design Intervention Primary outcome Secondary Duration of anticoagulation outcome Randomized Double blind trial 371 adults with first unprovoked symptomatic PE Randomization after 6 months of VKA VKA for 18 months (n= 184) vs Placebo for 18 months (n= 187) Recurrent VTE or major bleed 6/184 vs 25/ % vs 13.5 % (p = 0.001) HR VTE 1.7 % vs 13.5 % (p < 0.001) HR m follow up composite outcome 33 (20.8 %) vs 42 (24.0 %) P = 0.22 Major bleed 2.2 % vs 0.5 % P = 0.22
65 Duration of anticoagulation High rate of recurrent VTE was noted in placebo group than warfarin with HR 0.15 (CI ) Additional extended therapy reduced the composite outcome of recurrent venous thrombosis and major bleeding compared with placebo However, benefit was not maintained after discontinuation of anticoagulation therapy Francis Couturaud et al; JAMA 2015;314(1)
66 Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies IVC filter Subsegmental PE

67 Catheter directed therapies Fragmentation, aspiration and fibrinolysis Wissam A. Jaber et al; JACC 2016
68 Catheter directed therapies Pulmonary arterial injury Pericardial tamponade Major bleeding Hemodynamic deterioration Distal embolization Access site bleeding Wissam A. Jaber et al; JACC 2016

69 Catheter directed thrombolysis
70 Catheter directed thrombolysis In emergent situations, systemic thrombolytic therapy can be given while CDT is being arranged, and active thrombus fragmentation and aspiration can be combined with CDT Antithrombotic Therapy for VTE Disease, CHEST 2016; 149(2)
71 Catheter directed thrombolysis Ultrasound Accelerated Thrombolysis of Pulmonary Embolism (ULTIMA) trial Participants Intervention Results (mean RV/LV ratio at 24 hrs) Conclusion 59 subjects with intermediate risk PE (Confirmed by CT) RV/LV chamber ratio >1 in apical 4 chamber view USAT regimen of 10 mg rtpa over 15 hours per treated lung via the EkoSonic Endovascular System (n=30) Or UFH alone (n=29) USAT group (1.28 ± 0.19 to 0.99 ± 0.17 )(P < 0.001) Heparin group, (1.20 ± 0.14 and 1.17 ± 0.20)(P = 0.31) The mean decrease in RV/LV ratio from baseline to 24 hours was 0.30 ± 0.20 vs 0.03 ± 0.16 (P < 0.001) No major bleeding or recurrent VTE in either group at 90 d f/u Standardized USAT regimen was superior to anticoagulation with heparin alone in reversing RV dilatation at 24 hours Nil Kucher et al; Circulation 2014
72 Catheter directed thrombolysis The SEATTLE II Study, prospective, single-arm, multicenter trial to evaluate the safety and efficacy of ultrasound-facilitated, catheter-directed, low-dose fibrinolysis Participants Intervention 150 patients with acute massive (n =31) or sub massive (n = 119) PE and CT RV/LV mg of t PA administered as 1 mg/h for 24 h with a U/L catheter or 1 mg/h/catheter for 12 h with B/L catheters Results Reduction of RV/LV diameter (1.55 to 1.13) (p <0.001) PA systolic pressure (51.4 to 36.9 measured at 48 hrs (p <0.001) 17 major bleeding events Conclusion CDT improved RV function, thrombus burden and minimized intracranial hemorrhage Gregory Piazza et al; JACC 2015
73 Catheter directed thrombolysis Improved short term, surrogate outcomes Effect on clinical and long term outcomes not known No randomized trials comparing with systemic thrombolytic therapy are available FDA approved
74 Catheter directed therapies 594 patients in 35 studies Clinical success rate from CDT was 86.5% which increased to 91.2 % with co administered thrombolysis Minor procedural complications - 7.9% Major procedural complications - 2.4% WT kuo et al; J Vasc Interv Radiol 2009
75 Nish Patel et al; Catheterization and Cardiovascular Interventions 2015 Systemic vs Catheter directed thrombolysis In hospital mortality In hospital mortality + ICH Hemorrhage requiring transfusion Systemic lysis (n= 1169) CDT ( n= 352) Odds ratio % % 0.55 ( ) % % 0.52 ( ) ( ) 0.38 LOS 7 (5 10) 7 (5 10) 0.82 ( ) 0.09 P value Costs 17,713 24,714 - <0.0001
76 Catheter based thrombus removal Aspiration thrombectomy Thrombus fragmentation Rotational embolectomy Rheolytic thrombectomy



77 Angiovac device Removal of large proximal pulmonary emboli, intracardiac masses and caval thrombus
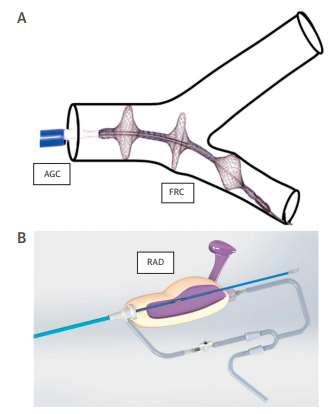
78 Flowtriever device
79 Catheter directed therapies Catheter-directed therapies may be considered for patients with persistent hemodynamic instability despite systemic thrombolysis those at risk of death before systemic thrombolysis can manifest effectiveness those at high risk of bleeding Antithrombotic Therapy for VTE Disease, CHEST 2016; 149(2)
80 Catheter directed therapies Decrease major bleeding including ICH Higher risk of vascular access-related complications contrast induced nephropathy costs Never be performed faster than systemic lysis Reserved for use in centers with appropriate expertise
81 Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies IVC filter Subsegmental PE
82 IVC filter Acute VTE and inability to anticoagulate ACCP AHA ACR SIR Anticoagulation failure Hemodynamically unstable patients, as an adjunct to anticoagulation Massive PE treated with thrombolysis Mobile thrombus Iliocaval DVT Prophylaxis in high risk (polytrauma & bariatric sx)
83 IVC filter Permanent IVC filter initially reduced the occurrence of symptomatic or asymptomatic PE who are having proximal DVT It was offset by a significant increase in recurrent DVTs, which could be related to thrombosis at the filter site No effect was observed on either immediate or long-term mortality PREPIC study N Engl J Med 1998;338:409-15

84 IVC filter
85 Retrieval IVC filter Optional filters (rivcf) are designed to be retrieved or left in place after the temporary risk of PE or contraindication to anticoagulation has resolved Provide benefit without long term risks Lack of trials to support indications for the selective use of temporary filters
86 Retrieval IVC filter No RCTs have been performed comparing the performance of rivcf and pivcf rivcfs have higher complication rates than pivcf Adverse events increase proportionally with prolonged filter dwell time Filter migration, filter fracture, and perforation of the caval wall or adjacent structures by filter components

87 Retrieval IVC filter Jessica M. Andreoli et al; J Vasc Interv Radiol 2014


88
89 Study Design Intervention Outcomes Patrick Mismett et Randomized Full-dose Recurrent PE at 3 m al; Open labelled trial anticoagulation for 3 % vs 1.5 % PREPIC 2 TRIAL JAMA 2015;313(6) 400 patients of acute PE with acute lower limb at least 6 months (p = 0.50) DVT or superficial VT 1 severity criteria Filter group (n= 200) Recurrent PE at 6 m 3.5 % vs 2.0% (p = 0.54) > 75 years cancer, chronic vs Mortality at 6 m cardiorespiratory insufficiency, stroke in last 6 m, large DVT Control group (n= 199) 6 months follow up 10.6 % vs 7.5 % (p = 0.29)
90 IVC filter Decision which IVC filters to use, when to use them, and for how long they should remain in place remains a highly complex process with many variables to consider Mechanical prophylaxis not entirely benign Morbidity risks increase over time Should be removed when risk for PE has resolved Post placement clinical follow-up is critical to optimizing retrieval rates
91 Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies IVC filter Subsegmental PE
92 Subsegmental PE Fourth order arteries with diameter of 3mm Advent of multi-detector CTPA has allowed better assessment of PE regarding visualisation of the peripheral pulmonary arteries, increasing its rate of diagnosis Incidence of isolated SSPE 4.7% of patients with PE by single-detector CT 9.4% of patients with PE by multi-detector CT
93 Subsegmental PE Clinical impact of a SSPE diagnosis is unknown Could be imaging artifacts Low inter-observer variability between radiologists 60 patients with SSPE diagnosed by CTPA & no DVT who did not receive anticoagulation Rx have been reported in the literature None of these patients suffered recurrent symptomatic VTE (PE or DVT) during the 3- month follow-up period Carrier M et al, J Thromb Haemost 2012
 Patients with symptomatic SSPE appear to mimic those with segmental or more proximal PE as regards their risk profile and short-term clinical course Risk profile and clinical")
94 Subsegmental PE SSPE and more proximal PE. 3-month risk of recurrent VTE (3.6% vs 2.5%; P = 0.42) Mortality (10.7% vs 6.5%; P =0.17) Patients with symptomatic SSPE appear to mimic those with segmental or more proximal PE as regards their risk profile and short-term clinical course Risk profile and clinical outcome of symptomatic subsegmental acute PE, Blood 2013
95 Subsegmental PE Ongoing cohort study A Study to Evaluate the Safety of Withholding Anticoagulation in Patients with subsegmental PE Who Have a Negative Serial Bilateral Lower Extremity Ultrasound (SSPE) NCT
96 Subsegmental PE To perform a CTPA only when necessary, i.e. in patients with a high clinical probability or a positive D-dimer Review of SSPE expert thoracic radiologist DVT scan should be done in all If DVT is detected, patients require anticoagulation If DVT is not detected, there is uncertainty whether patients should be anticoagulated Antithrombotic Therapy for VTE Disease, CHEST 2016; 149(2)
97 Subsegmental PE It should be individualized, taking into account the bleeding risk and risk of recurrent VTE If a decision is made not to anticoagulate, there is the option of doing one or more follow-up US examinations of the legs to detect (and then treat) evolving proximal DVT Antithrombotic Therapy for VTE Disease, CHEST 2016; 149(2)
98 Take home message Age adjusted D dimer and CDRs excludes PE in low clinical probability Thrombolysis in intermediate PE can be done with caution in selected subjects NOACs are recommended for anticoagulation unless contraindicated Duration and indication of IVCF usage is unclear
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Acute and long-term treatment of PE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Acute and long-term treatment of VTE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Pulmonary embolism: Acute management. Cecilia Becattini University of Perugia, Italy
 Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
Management of Acute Pulmonary Embolism. Judith Hurdman Consultant Respiratory Physician
 Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Use of EKOS Catheter in the management of Venous Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group
 Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
The spectrum of clinical outcome of PE
 Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
Cancer Associated Thrombosis: six months and beyond. Farzana Haque Hull York Medical School
 Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Management of Pulmonary Embolism. Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School
 Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
Heart Health ESC Guidelines on the diagnosis and management of acute pulmonary embolism
 Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Focus: l embolia polmonare Per quanto la terapia anticoagulante orale? Giulia Magnani 27 Gennaio, 2018
 Focus: l embolia polmonare Per quanto la terapia anticoagulante orale? Giulia Magnani 27 Gennaio, 2018 NO DISCLOSURE Pulmonary Embolism Venous thromboembolism (VT) is the third most common cause of cardiovascular
Focus: l embolia polmonare Per quanto la terapia anticoagulante orale? Giulia Magnani 27 Gennaio, 2018 NO DISCLOSURE Pulmonary Embolism Venous thromboembolism (VT) is the third most common cause of cardiovascular
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC
 David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC") Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Venous Thromboembolic Disease Update
 Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions
 Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Management of Intermediate-Risk Pulmonary Embolism
 Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
What is New in Acute Pulmonary Embolism? Interventional Treatment. Prof. Nils Kucher University Hospital Bern Switzerland
 What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Risk-Based Evaluation and Management of VTE
 12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go?
 Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
VTE General Background
 VTE General Background VTE incidence is about 1:1000 persons annually >250,000 admissions for VTE annually >100,000 people die of PE annually >90% of PE s arise from lower limb DVT 50% of DVT at diagnosis
VTE General Background VTE incidence is about 1:1000 persons annually >250,000 admissions for VTE annually >100,000 people die of PE annually >90% of PE s arise from lower limb DVT 50% of DVT at diagnosis
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Catheter-directed Thrombolysis for Pulmonary Embolism
 Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment
 Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
Epidemiology: Incidence VTE: Mortality Morbidity Risk Factors: Acute Chronic : Genetic
 Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
IDEAL MANAGEMENT OF PULMONARY EMBOLISM DISCLOSURES
 IDEAL MANAGEMENT OF PULMONARY EMBOLISM Samuel Z. Goldhaber, MD Section Head, Vascular Medicine Director, Thrombosis Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine
IDEAL MANAGEMENT OF PULMONARY EMBOLISM Samuel Z. Goldhaber, MD Section Head, Vascular Medicine Director, Thrombosis Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine
Venous Thromboembolism (VTE) in Myeloma. Christine Chen May 2017
 in Myeloma. Christine Chen May 2017") Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Evidences for real-life use in fragile patients: Renal failure and cancer
 Evidences for real-life use in fragile patients: Renal failure and cancer Cecilia Becattini Medicina Interna e Cardiovascolare Stroke Unit Università di Perugia Approval number: L.IT.MA.11.2016.1839 Evidences
Evidences for real-life use in fragile patients: Renal failure and cancer Cecilia Becattini Medicina Interna e Cardiovascolare Stroke Unit Università di Perugia Approval number: L.IT.MA.11.2016.1839 Evidences
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
The clinical relevance of AMPLIFY programme
 Venice October 16th 2015 The clinical relevance of AMPLIFY programme Francesco Dentali Department of Clinical Medicine Insubria University Varese Disclosures Bayer Bristol-Myers Squibb/Pfizer Boehringer
Venice October 16th 2015 The clinical relevance of AMPLIFY programme Francesco Dentali Department of Clinical Medicine Insubria University Varese Disclosures Bayer Bristol-Myers Squibb/Pfizer Boehringer
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis
 Receiving Catheter- Directed Thrombolysis") Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
The latest on the diagnosis and treatment of venous thromboembolism
 The latest on the diagnosis and treatment of venous thromboembolism Vicky Tagalakis MD FRCP Division of General Internal Medicine Jewish General Hospital McGill University Disclosures Advisory board Pfizer
The latest on the diagnosis and treatment of venous thromboembolism Vicky Tagalakis MD FRCP Division of General Internal Medicine Jewish General Hospital McGill University Disclosures Advisory board Pfizer
Catheter Interventions for pulmonary embolism:
 Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Duration of Anticoagulation? Peter Verhamme MD, PhD Department of Cardiovascular Medicine University of Leuven Belgium
 Duration of Anticoagulation? Peter Verhamme MD, PhD Department of Cardiovascular Medicine University of Leuven Belgium Disclosures Honoraria and research support: Daiichi-Sankyo, Boehringer Ingelheim,
Duration of Anticoagulation? Peter Verhamme MD, PhD Department of Cardiovascular Medicine University of Leuven Belgium Disclosures Honoraria and research support: Daiichi-Sankyo, Boehringer Ingelheim,
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
 Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL
 PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
Interventional Management of Acute Pulmonary Embolism
 Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren
 Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren Paul Kyrle Allgemeines Krankenhaus Wien Disclosures relevant for this presentation Consultancies, member of advisory boards, speaker
Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren Paul Kyrle Allgemeines Krankenhaus Wien Disclosures relevant for this presentation Consultancies, member of advisory boards, speaker
Optimal Management of Intermediate-Risk Pulmonary Embolism
 Optimal Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University
Optimal Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital
 Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
La terapia del TEV nel paziente oncologico nell'era dei DOAC
 XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
Management of Massive and Sub-Massive Pulmonary Embolism
 Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
incidence of cancer-associated thrombosis (CAT) is further increased by additional risk factors such as chemotherapeutic 2
 is further increased by additional risk factors such as chemotherapeutic 2") CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for
: Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for") The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
DOACs in CAT. Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD
 DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
Management of Cancer Associated VTE
 Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
Catheter Directed Interventions for Pulmonary Embolism
 Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS
 ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS
 UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS Armando Mansilha MD, PhD, FEBVS 16 th National Congress of the Italian Society of Vascular and Endovascular Surgery Bologna, 2017 Disclosure I have the following
UPDATE ON TREATMENT OF ACUTE VENOUS THROMBOSIS Armando Mansilha MD, PhD, FEBVS 16 th National Congress of the Italian Society of Vascular and Endovascular Surgery Bologna, 2017 Disclosure I have the following
The Evidence Base for Treating Acute DVT
 The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
SESSION 4 12:45 2:15 PM
 SESSION 4 12:45 2:15 PM Pulmonary Embolism Update SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza, MD, MS:
SESSION 4 12:45 2:15 PM Pulmonary Embolism Update SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza, MD, MS:
Update on the Management of Cancer Associated VTE
 Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Frequently Asked Questions about Cancer Associated Thrombosis
 + Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
+ Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
Venous Thrombo-Embolism. John de Vos Consultant Haematologist RSCH
 Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Controversies in Venous Thromboembolism
 Controversies in Venous Thromboembolism Menaka Pai, BSc MSc MD FRCPC Assistant Professor, Department of Medicine, McMaster University Associate Member, Department of Pathology and Molecular Medicine, McMaster
Controversies in Venous Thromboembolism Menaka Pai, BSc MSc MD FRCPC Assistant Professor, Department of Medicine, McMaster University Associate Member, Department of Pathology and Molecular Medicine, McMaster
Perioperative Management of the Anticoagulated Patient
 Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
EKOS. Interventional Vascular 3 February, Imagine where we can go.
 EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1
 CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation
 ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation Stephan Moll Department of Medicine, Division of Hematology-Oncology, University of North Carolina School of
ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation Stephan Moll Department of Medicine, Division of Hematology-Oncology, University of North Carolina School of
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Thromboembolism and cancer: New practices. Marc Carrier
 Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Management of sub-massive and massive pulmonary embolism:
 Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
Inferior Vena Cava Filters
 Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center
 Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
Θεραπεία και Πρόληψη Θρομβώσεων και Πνευμονικών Εμβολών Τι μάθαμε το 2017; Τι περιμένουμε το 2018;
 Θεραπεία και Πρόληψη Θρομβώσεων και Πνευμονικών Εμβολών Τι μάθαμε το 2017; Τι περιμένουμε το 2018; Stavros V. Konstantinides, MD, PhD, FESC Professor of Cardiology Democritus University of Thrace, Greece
Θεραπεία και Πρόληψη Θρομβώσεων και Πνευμονικών Εμβολών Τι μάθαμε το 2017; Τι περιμένουμε το 2018; Stavros V. Konstantinides, MD, PhD, FESC Professor of Cardiology Democritus University of Thrace, Greece
Keynote lecture: Oral anticoagulation and DVT
 Keynote lecture: Oral anticoagulation and DVT What is the evidence? Is there a need to anticoagulate every lower leg DVT? Disclosure Speaker name:...sebastian Schellong... I have the following potential
Keynote lecture: Oral anticoagulation and DVT What is the evidence? Is there a need to anticoagulate every lower leg DVT? Disclosure Speaker name:...sebastian Schellong... I have the following potential
PULMONARY EMBOLISM -CASE REPORT-
 University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Acute Management of Pulmonary Embolism
 Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Epidemiology of Thrombosis in Patients with Malignancy. Cancer and Venous Thromboembolism. Chew HK, Arch Int Med, Feb Blom et al, JAMA, Feb 2005
 Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
New Guidance in AT10 Clive Kearon, MD, PhD,
 New Guidance in AT10 Clive Kearon, MD, PhD, Professor, Department of Medicine, McMaster University; Program Director, McMaster Clinical Investigator Program, McMaster University Head, Clinical Thromboembolism
New Guidance in AT10 Clive Kearon, MD, PhD, Professor, Department of Medicine, McMaster University; Program Director, McMaster Clinical Investigator Program, McMaster University Head, Clinical Thromboembolism
A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism
 Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
4/18/2018. Objectives. Background. 1) Compare and contrast the various validated tools for the identification of patients with pulmonary embolism
 Compare and contrast the various validated tools for the identification of patients with pulmonary embolism") Pulmonary Embolism: Assessment, risk-stratification, and treatment plan for the outpatient management of low-risk patients Presentation by Joshua T. Wood, PharmD/PGY-1 Resident Providence St. Patrick Hospital;
Pulmonary Embolism: Assessment, risk-stratification, and treatment plan for the outpatient management of low-risk patients Presentation by Joshua T. Wood, PharmD/PGY-1 Resident Providence St. Patrick Hospital;