Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment
|
|
|
- Meredith O’Brien’
- 5 years ago
- Views:
Transcription



1 Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland
2 Overview Reperfusion treatment - Systemic thrombolysis - PETHO Trial - TOPCOAT Trial - Catheter-based therapy - ULTMA - PERFECT - SEATTLE - Surgical thrombectomy Perspectives Conclusion


3 Reperfusion therapy Konstantinides et al, JACC 2016

4 Haemodynamic collapse in acute PE Reperfusion Therapy Konstantinides et al, 2014 ESC Guidelines, EHJ 2014
5 Reperfusion therapy for acute PE Aim: Early resolution of pulmonary obstruction, decrease thrombus burden Reduction of pulmonary artery pressure and resistance mprovement of RV function Konstantinides et al, 2014 ESC Guidelines, EHJ 2014
6 Overall mortali COPER: PE Mortality 100 N = Massive PE BPsys < Non-massive PE BPsys > Days Kucher et al. Circulation 2006
7

8 Courtesy of Prof S. Konstantinides
9 Courtesy of Prof S. Konstantinides
10 Courtesy of Prof S. Konstantinides

11 Courtesy of Prof S. Konstantinides

12 Courtesy of Prof S. Konstantinides

13 Courtesy of Prof S. Konstantinides

14 Courtesy of Prof S. Konstantinides
15 Kline Multicenter, double blinded RCT Subjects: 83 pts with intermediate-risk PE (RV strain by Echo or biomarkers) ntervention: - Weight adapted single bolus of tenecteplase + LMWH (n=40) - Placebo + LMWH (n= 43) Patient-oriented outcomes Kline et al J Thromb Haemost 2014
16 Kline Primary outcomes: a) Early (first 5 days): Composite of death, shock, intubation or major hemorrhage within 5 d - Placebo: 3 pts (1x death, 2x intubation) - Tenecteplase: 1 pts (fatal intracranial hemorrhage) b) Mid-term (at 90 day follow-up): Composite of recurrent PE, poor functional capacity (RV dysfunction with dyspnoe/exercise intolerance), or SF36 physical component summary score <30 - Placebo: 13 pts (30%) - Tenecteplase: 5 pts (13%) Overall, 16 (37%) pts treated with placebo and 6 (15%) treated with tenecteplase had an adverse outcome (p<0.02) Kline et al J Thromb Haemost 2014

17 With 15 trials involving 2057 patients Marti et al, EHJ 2015
18 Efficacy outcomes: Bleeding complications: Marti et al, EHJ 2015


19 Kearon et al, Chest 2016


20 Stein et al, Am J Med 2012

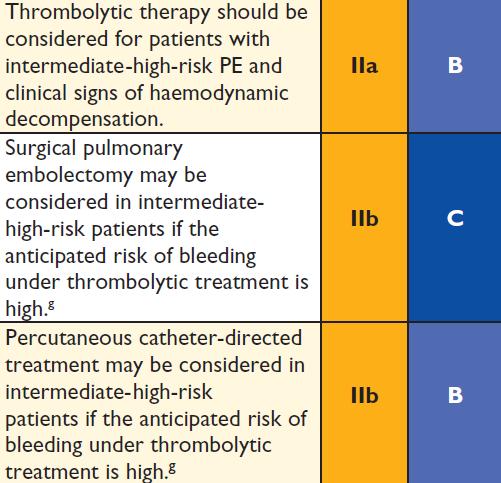
21 Approved thrombolytic regimens Konstantinides et al, 2014 ESC Guidelines, EHJ 2014

22 Contraindications for thrombolytic therapy Konstantinides et al, 2014 ESC Guidelines, EHJ 2014
 confirmed flow reversal proximal to the embolic occlusion and rapid wash out (0.40-0.")
23 ntraclot versus Systemic Thrombolysis for PE Blood Flow Pattern in Occlusive Pulmonary Embolism n-vitro pulmonary artery glas modell (5 l/min) simulating blood flow using illuminated suspended microspheres: High-velocity vortex formation proximal to the leading edge of the occlusion n-vivo tests (6 dogs) confirmed flow reversal proximal to the embolic occlusion and rapid wash out ( s) into non-occluded arteries even if the injection was performed directly proximal to the occlusion Schmitz-Rode T, et al. Cardiovasc ntervent Radiol 1998; 21:



24 Catheter-based therapy for acute PE


25 Catheter intervention without local thrombolysis Adapted from Engelberger/Kucher, Circulation 2011


26 Catheter intervention with local thrombolysis Adapted from Engelberger/Kucher, Circulation 2011
27 Complications Vascular access complications Right ventricular failure from distal embolization or contrast injections Bleeding from anticoagulation or thrombolysis Hemolysis, hemoglobinuria Arrhythmia Contrast-induced anaphylaxis and contrastinduced nephropathy Pulmonary hemorrhage/ hemoptysis

28 ULTrasound Accelerated Thrombolyss of PulMonAry Embolism Kucher et al, Circulation 2014



 Pulses of")

29 Ultrasound accelerated thrombolysis Ultrasound pulses Mechanism of Action Fibrin separation Active drug delivery by acoustic streaming Ultrasound delivered in: High frequency (2.2 Mhz) Low power (0.5 W per element) Pulses of varying waveforms Fibrin without Ultrasound Fibrin With Ultrasound Braaten et al. Thromb Haemost 1997; 78:

30 Ultrasound accelerated thrombolysis EKOS EkoSonic Mach 4e Endovascular System 5.4 F Drug Delivery Catheter Ultrasound Core wire nfusion side-hole catheter with a multi-element ultrasound core 12 cm nominal treatment zone length typically used for PE therapy


31 nclusion criteria Acute symptomatic PE confirmed by contrast-enhanced chest CT with embolus located in at least one main or proximal lower lobe pulmonary artery RV/LV ratio > 1 on echocardiography
32 Hemodynamically stable patients with acute symptomatic PE UFH 80 U/kg Bolus V, UFH continuous infusion of 18 U/kg/min V (max 1800 U/h) Contrast-Enhanced Chest CT: Filling defect in at least one main or proximal lower lobe pulmonary artery Baseline ECHO: RV/LV ratio > 1 4 hours UFH V alone (N=25 with evaluable RV/LV ratio on echocardiograms at baseline and 24 hours) UFH V + EkoSonic procedure: Ultrasound-assisted tpa of 10 mg over 15 hours per catheter (Maximum total dose 20 ± 1 mg over 15 ± 1 hours) (N=25 with evaluable RV/LV ratio on echocardiograms at baseline and 24 hours) Primary endpoint assessed by blinded core-lab: Reduction in RV/LV ratio from baseline to 24h Secondary endpoints: Mortality, recurrent PE, major & minor bleeding at 90 days

33
34 RV/LV Ratio 1,5 Primary endpoint: RV/LV ratio P< P< P< P=0.31 1,28 1,20 1,17 1,0 0,99 0,95 0,98 0,5 Baseline 24 hrs 90 days Baseline 24 hrs 90 days EKOS+Heparin Heparin
35 Reduction in RV/LV Ratio Primary endpoint: RV/LV ratio 0,6 P< P=0.03 0,4 0,2 0,0 0,30 Baseline to 24 hrs 0,38 Baseline to 90 days EKOS+Heparin 0,03 Baseline to 24 hrs Heparin 0,22 Baseline to 90 days
36 Secondary endpoint analysis Clinical outcomes at 90 days EKOS + Heparin Heparin N = 30 N = 29 p-value Death 0 0% 1* 3% 0.49 Recurrent venous thromboembolism 0 0% 0 0% 1.00 Major bleeding 0 0% 0 0% 1.00 Minor bleeding 3** 10% 1 3% 0.61 * rehospitalization and death from advanced pancreatic cancer ** two patients with transient mild hemoptysis without medical intervention, one patient with groin hematoma requiring manual compression one patient with transient anal bleeding following endoscopic removal ofcolon polyp
37 Conclusions n intermediate-risk PE, low-dose (up to 20 mg rt-pa over 15 hours) USAT was superior to anticoagulation with heparin alone in reversing RV dilatation and dysfunction at 24 hours, without an increase in bleeding complications Although there was a late catch up with heparin alone, we found greater improvement in RV dilatation and RV dysfunction after low-dose USAT at 90 days Kucher et al, Circulation 2014

38 Engelberger et al, EHJ 2015
39 Clinical presentation ntermediaterisk PE (n=38) High-risk PE (n=14) Transient hypotension* without vasopressors Transient hypotension with vasopressors Prolonged hypotension despite vasopressors Active cardiopulmonary resuscitation - 36 % - 29 % - 14 % - 21 % * Defined as systolic blood pressure < 90mmHg for at least 15 minutes 1 1 Jaff MR, et al. Circulation. 2011
40 Clinical course during procedure ntermediaterisk PE (n=38) High-risk PE (n=14) Symptom improvement 94 % 72 % Stabilisation of hemodynamics* 94 % 93 % Resolution of hypoxemia** 83 % 36 % * Hypotension resolved, vasopressor dose reduced or discontinued, cardiogenic shock resolved, signs of RV failure improved) within 24h of the end of the procedure ** Oxygen saturation of >92% on room air within 24 h of the end of the procedure
41 Complications ntermediaterisk PE (n=38) High-risk PE (n=14) Bleeding 1 Minor 16 % 35 % Major 3 % 7 % 3-month mortality 0 % 14 % Overall 3.8 % (95% C %) nternational society on thrombosis and haemostasis: Major bleeding : 1) Fatal bleeding, and/or 2) Symptomatic bleeding in a critical area or organ, such as intracranial, intraspinal, intraocular, retroperitoneal, intraarticular or pericardial, or intramuscular with compartment syndrome, 3) and/or Bleeding causing a fall in hemoglobin level of 20 g/l, or leading to transfusion of two or more units of whole blood or red cells. 1 Schulman S, Kearon C. J Thromb Haemost. 2005
42 [mmhg] Mean pulmonary artery pressure 60 mean pulmonary artery pressure before after Jaff et al, Circulation 2011
43 [L/min/m 2 ] Cardiac index 6 cardiac index before after
44 Echocardiographic RV/LV-Ratio 2,5 Echocardiographic RV/LV-Ratio 2 1,5 1 0,5 0 before TPES trial: weight-adjusted iv tenecteplase vs heparin in patients with intermediate-risk PE patients after Becattini et al, Thromb Res 2010

45 Piazza et al, JACC CV interv 2015
46 SEATTLE Single-arm, multicenter trial for low-dose USAT including 150 pts 31 with massive and 119 with submassive PE nclusion criteria: - Proximal PT with RV/LV ratio 0.9 on CT, with Sx for < 14d Treatment regimen: - 24 mg tpa (1mg/h for 24h with unilateral catheter, or 1mg/h/catheter for 12h with bilateral catheter) Primary outcomes: - Efficacy outcome: change in RV/LV ratio at 48h - Safety outcome: major periprocedural (<72h) bleeding Piazza et al, JACC CV interv 2015


47 SEATTLE Piazza et al, JACC CV interv 2015
48 Kuo et al, Chest 2015
49 PERFECT Registry Prospective multicenter registry including 101 pts: 28 massive and 73 submassive PE Catheter-directed therapy - Submassive PE: CDT (64%) or USAT (36%) with 0.5-1mg/h tpa (or U/h urokinase) - Massive PE: immediate catheter-directed mechanical or pharmacomechanical thrombectomy using catheter-directed fragmentation of PE, +/- intraclot lytic injection and aspiration. Following mechanical clot debulking, a potential low-dose hourly drug infusion - Outcomes - Clinical success - was defined as meeting all the following criteria: stabilization of hemodynamics; improvement in pulmonary hypertension, right-sided heart strain, or both; and survival to hospital discharge. - Primary safety outcomes - were major procedure-related complications and major bleeding events Kuo et al, Chest 2015
50 PERFECT Registry Outcomes Clinical success was achieved in 24 of 28 (86%) pts with massive PE 71 of 73 (97%) pts with submassive PE Complications 6 deaths 4 in massive PE (14%) 2 in submassive PE (3%) No major procedure-related complications, major hemorrhages, or hemorrhagic strokes. Kuo et al, Chest 2015


51 PERFECT: CDT versus USAT Kuo et al, Chest 2015

52 Summary Catheter-based therapy Kuo et al, Chest 2015
53 Comparison systemic thrombolysis vs CDT - No randomized trials - USA: National npatient Sample database out of pts hospitalized for PE treated with «thrombolysis» - Systemic thrombolysis in 1169 pts - CDT in 352 pts - Outcomes - Primary: in-hospital mortality - Secondary: combined in-hospital mortality and CH - Propensity-matched comparison (1:3) Patel et al, Catheter Cardiovasc nterv 2015
54 Comparison systemic thrombolysis vs CDT Patel et al, Catheter Cardiovasc nterv 2015
55 Long-term benefit of early hemodynamic improvement? RCT systemic thrombolysis (100mg alteplase over 2 hours) vs heparine alone in submassive PE patients 1 After 6 months: persistent improvement of echocardiographic parameters of RV function RCT systemic thrombolysis (urokinase or streptokinase) vs heparine alone 2 After mean FU of 7.4 years, assessed with right heart catheter: At rest, mean PAP and PVR significantly higher in the heparin group compared with the thrombolytic group (22 vs. 17 mmhg, p<0.05, and 351 vs. 171 dynes s(-1) cm(-5), p<0.02, respectively) During exercise both parameters rose to a significantly higher level in the heparin group 1 Fasullo et al, Am J Med Sci Sharma et al, Vasc Med 2000
56 Perspectives for catheter-based reperfusion therapy Optimal duration/drug dose for USAT (CDT)? Optimum Duration of Acoustic Pulse Thrombolysis Procedure in Acute Pulmonary Embolism (OPTALYSE PE) RCT comparing 2h (4/8mg rtpa), 4h (4/8mg), 6h (6/12 vs 12/24mg) No randomized data USAT vs other catheterbased reperfusion therapies No long-term data Catheter-based treatment instead of systemic thrombolysis? NCT
57 The SPECAL Trial Surgical Pulmonary Embolectomy versus Catheterdirected thrombolysis n the treatment of pulmonary embolism: a monocentric randomized phase non-inferiority study Primary objective: Non-inferiority of catheter-directed thrombolysis to surgical pulmonary embolectomy regarding efficacy in reversal of RV dilatation in high- and intermediate-high risk patients with acute PE Principal nvestigators: Profs Nils Kucher & Lars Englberger, nselspital
58 NOAC and reperfusion therapy? NOAC Trials patients with RECOVER: - pulmonary embolism with hemodynamic instability or requiring thrombolytic therapy AMPLFY & ENSTEN PE & HOKUSA - Thrombectomy, insertion of a caval filter, or use of a fibrinolytic agent to treat the current episode of venous thromboembolism (VTE). were excluded Schulman et al, NEJM 2009; Buller et al, NEJM 2012; Agnelli et al, NEJM 2013; Buller NEJM 2013


59 Reperfusion therapy for acute PE

60

61 ESC 2014 High-risk PE

62 ESC 2014 ntermediate- or low-risk PE
63

64 ACCP 2016: PE with hypotension


65 ACCP 2016: PE with hypotension

66 ACCP 2016: PE without hypotension

67 ACCP 2016: Systemic thrombolysis vs CDT?
68 Conclusion Reperfusion therapies have an important place in the managment of selected PE patients Systemic thrombolysis with more randomized trials, remain preferred reperfusion therapy according to the latest guidelines Catheter-based therapies have several advantages over systemic thrombolysis Role of catheter-based therapies needs to be better defined

69 Thank you for your attention
What is New in Acute Pulmonary Embolism? Interventional Treatment. Prof. Nils Kucher University Hospital Bern Switzerland
 What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Use of EKOS Catheter in the management of Venous Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group
 Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Interventional Management of Acute Pulmonary Embolism
 Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions
 Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Management of Massive and Sub-Massive Pulmonary Embolism
 Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Catheter-directed Thrombolysis for Pulmonary Embolism
 Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Epidemiology of Pulmonary Embolism (PE)
") Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Ultrasound-assisted catheter-directed thrombolysis: Does it really work? The BERNUTIFUL trial
 Ultrasound-assisted catheter-directed thrombolysis: Does it really work? The BERNUTIFUL trial Rolf P. Engelberger Division of Angiology CHUV, Lausanne & Inselspital, Bern Switzerland Disclosure Speaker
Ultrasound-assisted catheter-directed thrombolysis: Does it really work? The BERNUTIFUL trial Rolf P. Engelberger Division of Angiology CHUV, Lausanne & Inselspital, Bern Switzerland Disclosure Speaker
Acoustic Pulse Thrombolysis Treatment
 Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
 Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
EKOS. Interventional Vascular 3 February, Imagine where we can go.
 EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
Catheter Interventions for pulmonary embolism:
 Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis
 Receiving Catheter- Directed Thrombolysis") Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Management of Acute Pulmonary Embolism. Judith Hurdman Consultant Respiratory Physician
 Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Catheter Directed Interventions for Pulmonary Embolism
 Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Management of Intermediate-Risk Pulmonary Embolism
 Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
Optimal Management of Intermediate-Risk Pulmonary Embolism
 Optimal Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University
Optimal Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University
Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT) Initial Results From a Prospective Multicenter Registry
 Initial Results From a Prospective Multicenter Registry") [ Original Research Pulmonary Vascular Disease ] Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT) Initial Results From a Prospective Multicenter Registry William
[ Original Research Pulmonary Vascular Disease ] Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT) Initial Results From a Prospective Multicenter Registry William
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients
 The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Rationale for catheter directed therapy in pulmonary embolism
 Mini-Review Rationale for catheter directed therapy in pulmonary embolism Sailen G. Naidu, Martha-Gracia Knuttinen, J. Scott Kriegshauser, William G. Eversman, Rahmi Oklu Department of Radiology, Division
Mini-Review Rationale for catheter directed therapy in pulmonary embolism Sailen G. Naidu, Martha-Gracia Knuttinen, J. Scott Kriegshauser, William G. Eversman, Rahmi Oklu Department of Radiology, Division
Pulmonary embolism: Acute management. Cecilia Becattini University of Perugia, Italy
 Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Acute and long-term treatment of PE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Management of sub-massive and massive pulmonary embolism:
 Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
Management of Pulmonary Embolism. Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School
 Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Epidemiology: Incidence VTE: Mortality Morbidity Risk Factors: Acute Chronic : Genetic
 Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
Med Sci Monit, 2016; 22: Grade D. Quality Outstanding
 Ain and Jaff. Treatment of Submassive Pulmonary Embolism: Knowing When to be Aggressive and When to be Conservative. Curr Treat Options Cardio Med (2015) 17:25. Review Article Akin et al. Catheter-Directed
Ain and Jaff. Treatment of Submassive Pulmonary Embolism: Knowing When to be Aggressive and When to be Conservative. Curr Treat Options Cardio Med (2015) 17:25. Review Article Akin et al. Catheter-Directed
How and Why to Form a PERT, Pulmonary Embolism Response Team
 Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
Recent advances in the management of pulmonary embolism. Kodati Rakesh SR Pulmonary medicine
 Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
October 2017 Pulmonary Embolism
 October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
VTE & Medical Patients: Case Scenario
 The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
Risk-Based Evaluation and Management of VTE
 12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
Case. Case. Management of Pulmonary Embolism in the ICU
 Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Surgical Thrombectomy for PE: Is it Making a Comeback
 Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
Guideline for Thrombolysis Therapy in Pulmonary Embolism
 Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
SESSION 4 12:45 2:15 PM
 SESSION 4 12:45 2:15 PM Pulmonary Embolism Update SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza, MD, MS:
SESSION 4 12:45 2:15 PM Pulmonary Embolism Update SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza, MD, MS:
Acute and long-term treatment of VTE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Pharmaco-mechanical techniques stand alone procedures? Peter Neglén, MD, PhD SP Vascular Center Limassol Cyprus
 Pharmaco-mechanical techniques stand alone procedures? Peter Neglén, MD, PhD SP Vascular Center Limassol Cyprus Faculty Disclosure Peter Neglén, M.D., Ph.D Stockholder/Founder of Veniti, Inc. Member, Medical
Pharmaco-mechanical techniques stand alone procedures? Peter Neglén, MD, PhD SP Vascular Center Limassol Cyprus Faculty Disclosure Peter Neglén, M.D., Ph.D Stockholder/Founder of Veniti, Inc. Member, Medical
Supplementary Online Content
 Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Case 1:
 12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
Heart Health ESC Guidelines on the diagnosis and management of acute pulmonary embolism
 Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
4/24/2017 CATHETER-DIRECTED THERAPIES FOR ACUTE PE THE GREY AREA OF SUBMASSIVE PE DISCLOSURES OBJECTIVES: INTRAVASCULAR LYTIC THERAPY
 THE GREY AREA OF SUBMASSIVE PE CATHETER-DIRECTED THERAPIES FOR ACUTE PE Submassive PE PE with RV strain Saad Farooqi, MD Pulmonary/Critical Care Fellow Fatal PE Concept borrowed from Jeffrey A. Kline,
THE GREY AREA OF SUBMASSIVE PE CATHETER-DIRECTED THERAPIES FOR ACUTE PE Submassive PE PE with RV strain Saad Farooqi, MD Pulmonary/Critical Care Fellow Fatal PE Concept borrowed from Jeffrey A. Kline,
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
The spectrum of clinical outcome of PE
 Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Acute Management of Pulmonary Embolism
 Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Interventional treatment for patients with acute pulmonary embolism
 Interventional treatment for patients with acute pulmonary embolism I. Petrov, I. Martinov Cardiology department Tokuda Hospital Sofia I. Petrov, Treatment and prophylaxis of PE Treatment of PE: 1.) Systemic
Interventional treatment for patients with acute pulmonary embolism I. Petrov, I. Martinov Cardiology department Tokuda Hospital Sofia I. Petrov, Treatment and prophylaxis of PE Treatment of PE: 1.) Systemic
Should We Be More Aggressive in the Treatment of Acute DVT?
 DISCLOSURES Consultant Penumbra, Inc. UCSF Vascular Surgery Symposium April 6, 2017 K. Pallav Kolli, MD Assistant Professor of Clinical Radiology University of California, San Francisco 17 yo male, DVT
DISCLOSURES Consultant Penumbra, Inc. UCSF Vascular Surgery Symposium April 6, 2017 K. Pallav Kolli, MD Assistant Professor of Clinical Radiology University of California, San Francisco 17 yo male, DVT
Iliofemoral DVT: Miminizing Post-Thrombotic Syndrome
 Iliofemoral DVT: Miminizing Post-Thrombotic Syndrome Catherine K. Chang, MD FACS Vascular Surgery San Diego Southern California Permanente Medical Group Acute Deep Venous Thrombosis Incidence & Outcomes
Iliofemoral DVT: Miminizing Post-Thrombotic Syndrome Catherine K. Chang, MD FACS Vascular Surgery San Diego Southern California Permanente Medical Group Acute Deep Venous Thrombosis Incidence & Outcomes
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
IDEAL MANAGEMENT OF PULMONARY EMBOLISM DISCLOSURES
 IDEAL MANAGEMENT OF PULMONARY EMBOLISM Samuel Z. Goldhaber, MD Section Head, Vascular Medicine Director, Thrombosis Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine
IDEAL MANAGEMENT OF PULMONARY EMBOLISM Samuel Z. Goldhaber, MD Section Head, Vascular Medicine Director, Thrombosis Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine
Intervention for Deep Venous Thrombosis and Pulmonary Embolus
 Intervention for Deep Venous Thrombosis and Pulmonary Embolus Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard
Intervention for Deep Venous Thrombosis and Pulmonary Embolus Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
PULMONARY EMBOLISM AND PERT. Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology
 PULMONARY EMBOLISM AND PERT Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology No financial disclosures 1. What are the clinical signs/symptoms of submassive PE? 2.
PULMONARY EMBOLISM AND PERT Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology No financial disclosures 1. What are the clinical signs/symptoms of submassive PE? 2.
Chapter 1. Introduction
 Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach
 Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Venous interventions in DVT
 Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Systemic or local thrombolysis in high-risk pulmonary embolism
 original article Cardiology Journal 2015, Vol. 22, No. 4, 467 474 DOI: 10.5603/CJ.a2014.0103 Copyright 2015 Via Medica ISSN 1897 5593 Systemic or local thrombolysis in high-risk pulmonary embolism Liviu
original article Cardiology Journal 2015, Vol. 22, No. 4, 467 474 DOI: 10.5603/CJ.a2014.0103 Copyright 2015 Via Medica ISSN 1897 5593 Systemic or local thrombolysis in high-risk pulmonary embolism Liviu
Bilateral Central Pulmonary Embolism and Recent History of Ischemic Stroke
 WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
Massive Pulmonary Embolism
 Massive Pulmonary Embolism Objectives 1. Review the pathophysiology of a pulmonary embolism. 2. Describe the signs and symptoms of a patient experiencing a pulmonary embolism. 3. Identify treatment modalities
Massive Pulmonary Embolism Objectives 1. Review the pathophysiology of a pulmonary embolism. 2. Describe the signs and symptoms of a patient experiencing a pulmonary embolism. 3. Identify treatment modalities
ORIGINAL INVESTIGATION. Thrombolysis vs Heparin in the Treatment of Pulmonary Embolism
 Thrombolysis vs Heparin in the Treatment of Pulmonary Embolism A Clinical Outcome Based Meta-analysis ORIGINAL INVESTIGATION Giancarlo Agnelli, MD; Cecilia Becattini, MD; Timo Kirschstein, MD Background:
Thrombolysis vs Heparin in the Treatment of Pulmonary Embolism A Clinical Outcome Based Meta-analysis ORIGINAL INVESTIGATION Giancarlo Agnelli, MD; Cecilia Becattini, MD; Timo Kirschstein, MD Background:
Management of Acute Pulmonary Embolism: Anticipating and Responding to Complexity Ahmed Zaky, M.D., M.P.H. University of Alabama, Birmingham, AL
 Session: L213 Session: L403 Management of Acute Pulmonary Embolism: Anticipating and Responding to Complexity Ahmed Zaky, M.D., M.P.H. University of Alabama, Birmingham, AL Disclosures: This presenter
Session: L213 Session: L403 Management of Acute Pulmonary Embolism: Anticipating and Responding to Complexity Ahmed Zaky, M.D., M.P.H. University of Alabama, Birmingham, AL Disclosures: This presenter
Respiratory Review of 2014: Pulmonary Thromboembolism
 REVIEW http://dx.doi.org/10.4046/trd.2014.77.3.105 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2014;77:105-110 Respiratory Review of 2014: Pulmonary Thromboembolism Jae Seung Lee, M.D. Department
REVIEW http://dx.doi.org/10.4046/trd.2014.77.3.105 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2014;77:105-110 Respiratory Review of 2014: Pulmonary Thromboembolism Jae Seung Lee, M.D. Department
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center
 Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
PULMONARY EMBOLISM -CASE REPORT-
 University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
Controversies in Venous Thromboembolism
 Controversies in Venous Thromboembolism Menaka Pai, BSc MSc MD FRCPC Assistant Professor, Department of Medicine, McMaster University Associate Member, Department of Pathology and Molecular Medicine, McMaster
Controversies in Venous Thromboembolism Menaka Pai, BSc MSc MD FRCPC Assistant Professor, Department of Medicine, McMaster University Associate Member, Department of Pathology and Molecular Medicine, McMaster
Optimal Utilization of Thrombolytics
 April 8-9, 2011 New York LaGuardia Marriott COMPLETE MANAGEMENT OF VENOUS DISEASE Optimal Utilization of Thrombolytics Anthony J. Comerota, MD, FACS, FACC Director, Jobst Vascular Institute Adjunct Professor
April 8-9, 2011 New York LaGuardia Marriott COMPLETE MANAGEMENT OF VENOUS DISEASE Optimal Utilization of Thrombolytics Anthony J. Comerota, MD, FACS, FACC Director, Jobst Vascular Institute Adjunct Professor
The Evidence Base for Treating Acute DVT
 The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of Interventional procedure overview of ultrasound-enhanced, catheterdirected thrombolysis
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of Interventional procedure overview of ultrasound-enhanced, catheterdirected thrombolysis
Aggressive endovascular management of ilio-femoral DVT. thrombotic syndrome. is the key in preventing post
 CACVS 2017 Aggressive endovascular management of ilio-femoral DVT is the key in preventing post thrombotic syndrome ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HEALTH SYSTEM
CACVS 2017 Aggressive endovascular management of ilio-femoral DVT is the key in preventing post thrombotic syndrome ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HEALTH SYSTEM
Τί κάνουμε όταν πάσχει η δεξιά κοιλία Οξεία πνευμονική εμβολή. Βασίλειος Σαχπεκίδης Επιμελητής Α Καρδιολογίας Γ.Ν.Θ. Παπαγεωργίου
 Τί κάνουμε όταν πάσχει η δεξιά κοιλία Οξεία πνευμονική εμβολή Βασίλειος Σαχπεκίδης Επιμελητής Α Καρδιολογίας Γ.Ν.Θ. Παπαγεωργίου No conflicts of interest RV anatomy Ho SY and Nihoyannopoulos P. Heart 2006;92
Τί κάνουμε όταν πάσχει η δεξιά κοιλία Οξεία πνευμονική εμβολή Βασίλειος Σαχπεκίδης Επιμελητής Α Καρδιολογίας Γ.Ν.Θ. Παπαγεωργίου No conflicts of interest RV anatomy Ho SY and Nihoyannopoulos P. Heart 2006;92
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence Document Final information (version number/stage of process) Addendum to Clinical Guideline 144, Venous thromboembolic diseases in adults: diagnosis, management
National Institute for Health and Care Excellence Document Final information (version number/stage of process) Addendum to Clinical Guideline 144, Venous thromboembolic diseases in adults: diagnosis, management
Pulmonary Embolectomy:
 Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Systemic Fibrinolytic Therapy in the Presence of Absolute Contraindication; a Case Series
 Emergency. 2018; 6 (1): e25 CASE REPORT Systemic Fibrinolytic Therapy in the Presence of Absolute Contraindication; a Case Series Mahdi Pishgahi 1, Toktam Alirezaei 1, Behzad Hajimoradi 1, S. Mojtaba Nekooghadam
Emergency. 2018; 6 (1): e25 CASE REPORT Systemic Fibrinolytic Therapy in the Presence of Absolute Contraindication; a Case Series Mahdi Pishgahi 1, Toktam Alirezaei 1, Behzad Hajimoradi 1, S. Mojtaba Nekooghadam
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Pulmonary embolism. Paweł Balsam
 Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Thrombus Removal in Acute Pulmonary Embolism: When and How?
 Thrombus Removal in Acute Pulmonary Embolism: When and How? Kenneth Rosenfield, MD, MHCDS, MSCAI Cardiology Division Section of Vascular Medicine and Intvn MGH Kenneth Rosenfield, MD, MHCDS Conflicts of
Thrombus Removal in Acute Pulmonary Embolism: When and How? Kenneth Rosenfield, MD, MHCDS, MSCAI Cardiology Division Section of Vascular Medicine and Intvn MGH Kenneth Rosenfield, MD, MHCDS Conflicts of
This chapter will describe the effectiveness of antithrombotic
 Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,