Management of sub-massive and massive pulmonary embolism:
|
|
|
- Geraldine Fisher
- 5 years ago
- Views:
Transcription
1 Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief, Division of Pulmonary and Critical Care Medicine Department of Medicine, Khon Kaen University Khon Kaen, 40002, THAILAND
 VTE?")

2 AGENDA CLINICAL SPECTRUM OF ACUTE PULMONARY EMBOLISM (APE) CLASSIFICATION OF APE: THEN AND NOW WHAT IS LIFE THREATENING (CRITICAL, SEVERE) VTE? SUB-MASSIVE VS MASSIVE PULMONARY EMBOLISM CURRENT EVIDENCE-BASED APPROACH ON MANAGEMENT OF APE ANTICOAGULANT THERAPY MANAGEMENT OF MASSIVE PE THROMBOLYTIC THERAPY UNSUCCESSFUL INITIAL THROMBOLYSIS: CATHETER-BASED THERAPY, SURGICAL EMBOLECTOMY, OR REPEAT THROMBOLYSIS, MANAGEMENT OF SUB-MASSIVE PE IS THERE ROLES OF THROMBOLYSIS IN SUB-MASSIVE PE? IVC FILTER FOR APE & EXTENSIVE PROXIMAL DVT SUMMARY
3 CONFLICT OF INTEREST I have no conflict of interest about methods, machines, and products use in this lecture.
4 Incidence of Pulmonary Embolism Per Year in the United States* Total Incidence 630,000 89% Survival >1hr 563,000 Death within 1 hr 67,000 11% 71% 29% Dx not made Dx made, therapy 400,000 instituted 163,000 70% 30% 92% 8% Survival Death Survival Death 280, , , ,000 *Progress in Cardiovascular Diseases, Vol. XVII, No. 4 (Jan/Feb 1975)
5 Classification of APE: Then and now
6 Pathological Classification According to Clot Burden Small PE : Pulmonary vascular bed (PVB) occlusion ~30-50% PAP ~ normal or slightly elevate Moderate PE : PVB occlusion ~50-75 %, significantly elevate PAP & evidence of RV dilatation/akinesia Massive PE: PVB occlusion >75 %, Less correlate with clinical presentation and mortality Miller GA, et al., Br Med J 1971; 2:681-4


7 Risk Stratification In APE: Clinical Features & Diagnostic Tests Mortality Clinical Status At Presentation 65% Cardiac Arrest 25% Shock 15% Hypotension without hypoperfusion 8.1% Normal BP with RV dysfunction Higher Risk Predictions History/Physical Diagnostic Studies EKG CXR ABG D-Dimer Troponin, BNP Echocardiography Confirmatory Studies 0-1% Normal BP and RV function Lower Risk V/Q CT Angiography Angiography MAPPET Kasper JACC 1997; 30:
8
9 RV dysfunction-echocardiogram Arch Intern Med. 2005;165:
10
 Massive No Yes Yes 4.2-20% 25 % (11.6-33.7%) Sub-massive No No Yes 32% 5.8-11.2% Non-massive No No No 48% 0.4-0.")
11 Prognostic Categories of Pulmonary Embolism Category Presenting Symptoms and Signs Prevalence Mortality Cardiac arrest/ Need CPR Shock RV. Dysfunction Massive Yes Yes Yes 10 % 65 % ( %) Massive No Yes Yes % 25 % ( %) Sub-massive No No Yes 32% % Non-massive No No No 48% % CPR, cardiopulmonary resuscitation; RVD, right ventricular dysfunction
12 Clinical Presentations and Outcomes of Pulmonary Embolism Mortality 100% Normotensive, normal RV function Normotensive, RV dysfunction Sudden death 70% 50% Non-massive 48 % Sub-massive 32% Massive 20 % Cardiac arrest 30% Shock 10% 0% Severity Spectrum» Embolism size» Cardiopulmonary reserve
13 What is life threatening APE? Sub-massive VS Massive PE
14 Classification based on Severity Spectrum of Acute Pulmonary embolism Asymptomatic Mild Symptoms RV Dysfunction Non-massive Sub-massive Shock >> CPR Massive Normotensive Hypotensive Life-threatening APE
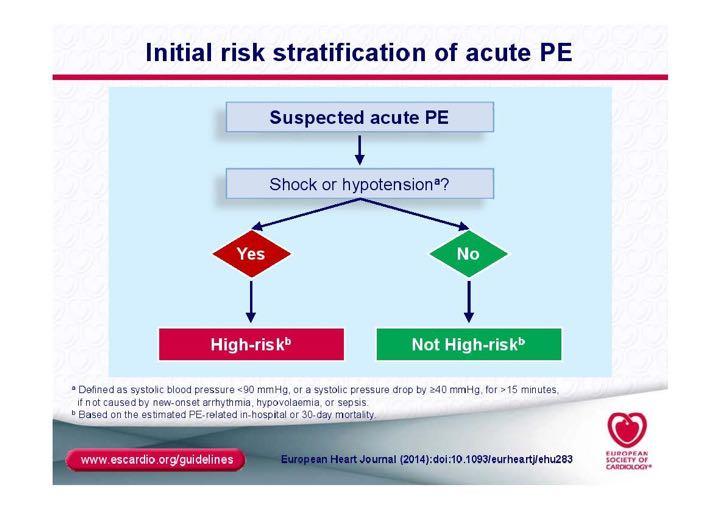
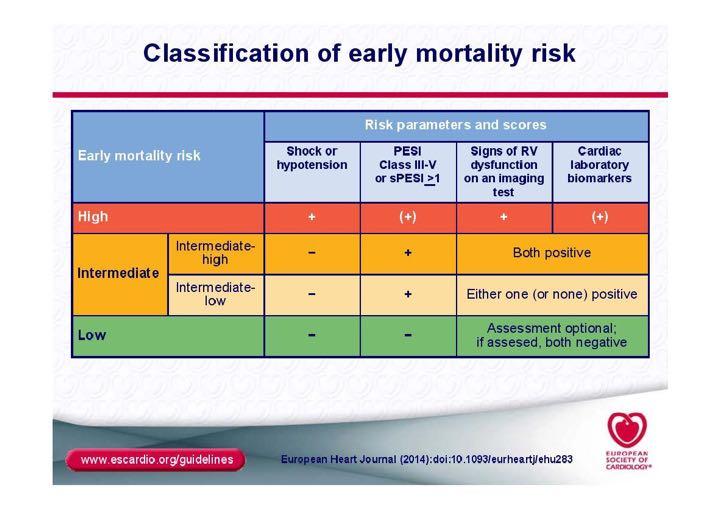
15 Sub-massive or Massive PE? Sub-massive PE APE without systemic hypotension but with either RV dysfunction or myocardial necrosis RV dysfunction : the presence of at least 1 of the following ECG: new RBBB or anteroseptal elevation or T-wave inversion RV dilatation (RV/LV Ø > 0.9) by echo. or CT. BNP > 90 pg/ml. NT pro BNP >500 pg/ml. & either Troponin I > 0.4 ng/ml. or Troponin T> 0.1 ng/ml Massive PE APE with sustained hypotension (BPs <90 mmhg.) for at least 15 min. or requiring vasopressor (not for other explanable cause(s) of shock APE present with cardiac arrest The International Cooperative Pulmonary Embolism Registry (ICOPER) Amer J Respir Crit Care Med 2005:172:
16 Current evidence-based approach on Management of Acute pulmonary Embolism (APE)
17 2014
18 2012
19 2012
20 Management of Massive and Submassive Pulmonary Embolism, Iliofemoral Deep Vein Thrombosis, and Chronic Thromboembolic Pulmonary Hypertension by Michael R. Jaff, M. Sean McMurtry, Stephen L. Archer, Mary Cushman, Neil Goldenberg, Samuel Z. Goldhaber, J. Stephen Jenkins, Jeffrey A. Kline, Andrew D. Michaels, Patricia Thistlethwaite, Suresh Vedantham, R. James White, Brenda K. Zierler, and 2011 Circulation Volume 123(16): April 26, 2011 Copyright American Heart Association, Inc. All rights reserved.
21 Options of APE Management Thrombolystics Catheter-based therapy Options Heparin & anticoagulants Surgical embolectomy
22 Anticoagulant Therapy
23 RECOMMENDATIONS FOR INITIAL ANTICOAGULATION FOR ACUTE PE 1. Therapeutic anticoagulation during the diagnostic workup should be given to patients with intermediate or high clinical probability of PE and no contraindications to anticoagulation (Class I; Level of Evidence C).
24 In Critical (Major) Pulmonary Embolism Diagnostic confirmatory studies can delay definitive treatment and contribute to additional mortality; 14%- 67% Mortality decreasing with early anticoagulant therapy, but variable (16% - 46%) Sub-therapeutic level of anticoagulant in the first 24 hours may contribute additional mortality
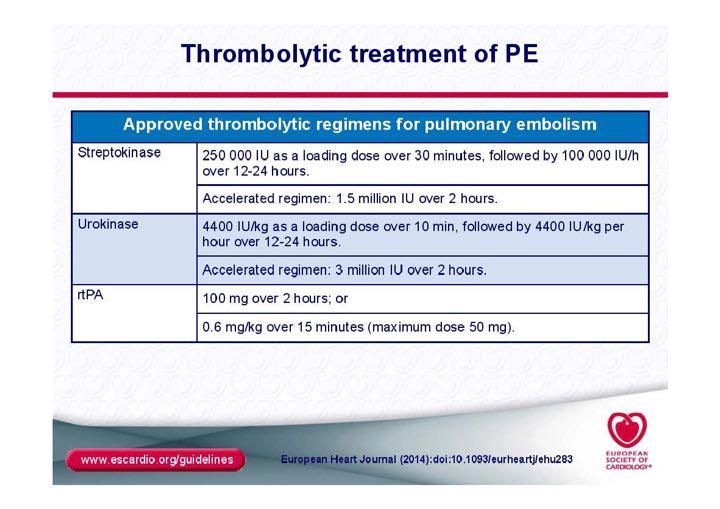
25 Thrombolytics Therapy In Massive PE
26 Massive Pulmonary Embolism (MPE) Prevalence and mortality The MAPPET (Germany based) APE with hypotension MR 25 %, APE required CPR MR 65% as compared to other Massive PE: 90 day Mortality rate 52.4 % Hemodynamic stable APE (non-massive & submassive) MR 8 % ICOPER 2005 Kasper W, et al. J Am Coll Cardiol 1997; 30:
:2414-2421. doi:10.1001/jama.2014.5990 Date of download: 8/29/2015 Copyright 2015 American Medical Association.")
27 From: Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage: A Meta-analysis JAMA. 2014;311(23): doi: /jama Date of download: 8/29/2015 Copyright 2015 American Medical Association. All rights reserved.
28 From: Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage: A Meta-analysis JAMA. 2014;311(23): doi: /jama Odds of Mortality in Patients With Pulmonary Embolism Treated With Thrombolytic Therapy vs AnticoagulationEvaluated using the Peto method of meta-analysis. MOPETT indicates Moderate Pulmonary Embolism Treated with Thrombolysis trial; PEITHO, Pulmonary Embolism Thrombolysis trial; PIOPED, Prospective Investigation of Pulmonary Embolism Diagnosis; TIPES, Tenecteplase Italian Pulmonary Embolism Study; TOPCOAT, Tenecteplase or Placebo: Cardiopulmonary Outcomes At Three Months; ULTIMA, Ultrasound Accelerated Thrombolysis of Pulmonary Embolism trial; UPETSG, Urokinase Pulmonary Embolism Trial Stage 1. Date of download: 8/29/2015 Copyright 2015 American Medical Association. All rights reserved.
29 From: Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage: A Meta-analysis JAMA. 2014;311(23): doi: /jama Odds of Mortality in Patients With Pulmonary Embolism Treated With Thrombolytic Therapy vs AnticoagulationEvaluated using the Peto method of meta-analysis. MOPETT indicates Moderate Pulmonary Embolism Treated with Thrombolysis trial; PEITHO, Pulmonary Embolism Thrombolysis trial; PIOPED, Prospective Investigation of Pulmonary Embolism Diagnosis; TIPES, Tenecteplase Italian Pulmonary Embolism Study; TOPCOAT, Tenecteplase or Placebo: Cardiopulmonary Outcomes At Three Months; ULTIMA, Ultrasound Accelerated Thrombolysis of Pulmonary Embolism trial; UPETSG, Urokinase Pulmonary Embolism Trial Stage 1. Date of download: 8/29/2015 Copyright 2015 American Medical Association. All rights reserved.
30 RECOMMENDATIONS FOR FIBRINOLYSIS FOR ACUTE PE-1 1. Fibrinolysis is reasonable for patients with massive acute PE and acceptable risk of bleeding complications (Class IIa; Level of Evidence B).
31 Cardiac Arrest Shock > 15 min. NO Absolute contraindications Prolonged CPR not CI
32
33 Contraindications to Thrombolytic Therapy Absolute Contraindications Major trauma, surgery, head trauma (within 3 weeks) Relative Contraindications Cancer Prior hemorrhagic stroke Age > Ischemic stroke within prior 6 months Central nervous system neoplasm Gastrointestinal bleeding within one month Concurrent active bleeding Transient ischemic attack within 6 months Oral anticoagulant therapy Non-compressible punctures Traumatic resuscitation Refractory hypertension Advanced liver disease Infective endocarditis Active peptic ulcer Pregnancy or within one week postpartum * Torbicki A, Perrier A, Konstantinides S, et al. Eur Heart J. 2008;29(18): Kasper W, Konstantinides S, Geibel A, et al. J Am Coll Cardiol. 1997;30(5):

34 Thrombolytics Therapy In Sub-massive PE

35 RV Necrosis
36 Clinical Presentations and Outcomes of Pulmonary Embolism Mortality 100% Normotensive, normal RV function Normotensive, RV dysfunction Sudden death 70% 50% Non-massive 48 % Sub-massive 32% Massive 20 % Cardiac arrest 30% Shock 10% 0% Severity Spectrum» Embolism size» Cardiopulmonary reserve

37 How many subgroups in Sub-massive Acute Pulmonary Embolism:
38 Central Debate for last 3 Centuries Thrombolytic in Sub-massive PE Pros o Feel better quicker o Resolve clots faster? o Improved RV function o Decrease PA pressure Cons oincreased ICH rate oincreased other life threatening hemorrhage oincreased cost ono survival benefit



39 Indicators of RV dysfunction use in studies EKG Echocardiography S 1 Q 3 T 3 and T wave changes RV Dilation, RV: LV 1, leftward septal bowing RV hypokinesia Estimated RVSP> 40 mmhg Cardiac Biomarkers: BNP >100 pg/ml or pro-bnp >900 pg/ml)
40 NO CLEAR TREND IN BENEFIT S U B M A S S I V E P E Wan S, Circ 110:744, 2004

41 No SURVIVAL BENEFIT but with significant risk Wan S, Circ 110:744

42 30% of normotensive PE have RV dysfunction 10 % further developed hypotension 5 % mortality during admission
43
44


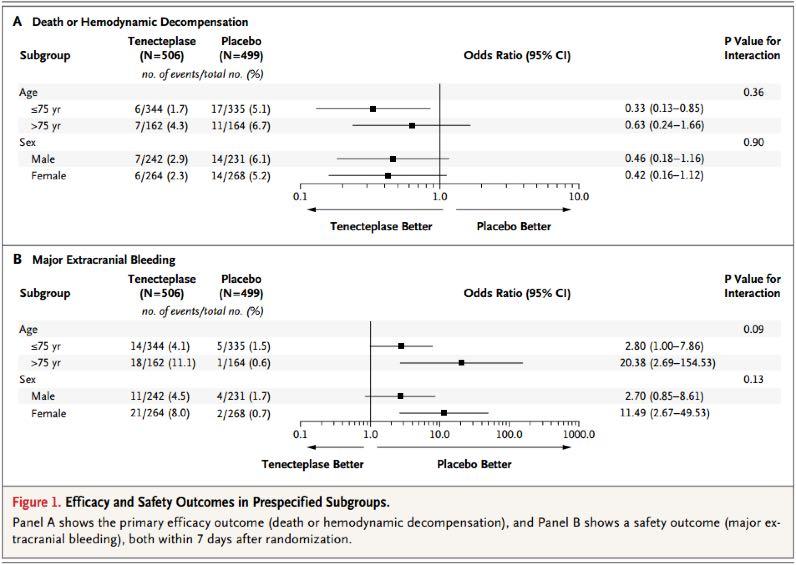
45 The PEITHO Trial 2014
46 From: Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage: A Meta-analysis JAMA. 2014;311(23): doi: /jama Odds of Mortality in Patients With Intermediate-Risk Pulmonary Embolism Treated With Thrombolytic Therapy vs Anticoagulation Evaluated using the Peto method of meta-analysis. The standard practice in meta-analysis of odds ratios (ORs) and risk ratios is to exclude studies from the meta-analysis where there are no events in either group. A 0-cell or continuity correction was not used based on recommendations regarding calculation of a Peto OR for studies with 0 events in only 1 group. MOPETT indicates Moderate Pulmonary Embolism Treated with Thrombolysis trial; PEITHO, Pulmonary Embolism Thrombolysis trial; TIPES, Tenecteplase Italian Pulmonary Embolism Study; TOPCOAT, Tenecteplase or Placebo: Cardiopulmonary Outcomes At Three Months; ULTIMA, Ultrasound Accelerated Thrombolysis of Pulmonary Embolism trial. Copyright 2015 American Medical Date of download: 8/29/2015 Association. All rights reserved.
47
48 RECOMMENDATIONS FOR FIBRINOLYSIS FOR ACUTE PE-2 2. Fibrinolysis may be considered for patients with submassive acute PE judged to have clinical evidence of adverse prognosis (new hemodynamic instability, worsening respiratory insufficiency, severe RV dysfunction, or major myocardial necrosis) and low risk of bleeding complications (Class IIb; Level of Evidence C).
49 RECOMMENDATIONS FOR FIBRINOLYSIS FOR ACUTE PE-2 3. Fibrinolysis is not recommended for patients with low-risk PE (Class III; Level of Evidence B) or submassive acute PE with minor RV dysfunction, minor myocardial necrosis, and no clinical worsening (Class III; Level of Evidence B). 4. Fibrinolysis is not recommended for undifferentiated cardiac arrest (Class III; Level of Evidence B).
50
51 Probability of PE above treatment threshold Submassive without RV Strain (Low risk PE) Submassive with RV strain (Abnormal echo or biomarkers) Systolic blood pressure < 90 mmhg for >15 min Heparin Anticoagulation Heparin Anticoagulation Heparin Anticoagulation Assess for evidence of increased severity that suggests potential for benefit of fibrinolysis 1. EVIDENCE OF SHOCK OR RESPIRATORY FAILURE: Any hypotension (SBP<90 mm Hg) OR Shock index >1.0 OR Respiratory distress (SaO2 <95% with Borg score >8, or altered mental status, or appearance of suffering) 2. EVIDENCE OF MODERATE TO SEVERE RV STRAIN: RV dysfunction (RV hypokinesis or estimated RVSP> 40 mmhg) OR Clearly elevated biomarker values (e.g., troponin above borderline value, BNP >100 pg/ml or pro-bnp >900 pg/ml) No contraindications to fibrinolysis Alteplase 100 mg over 2 h IV
52
53
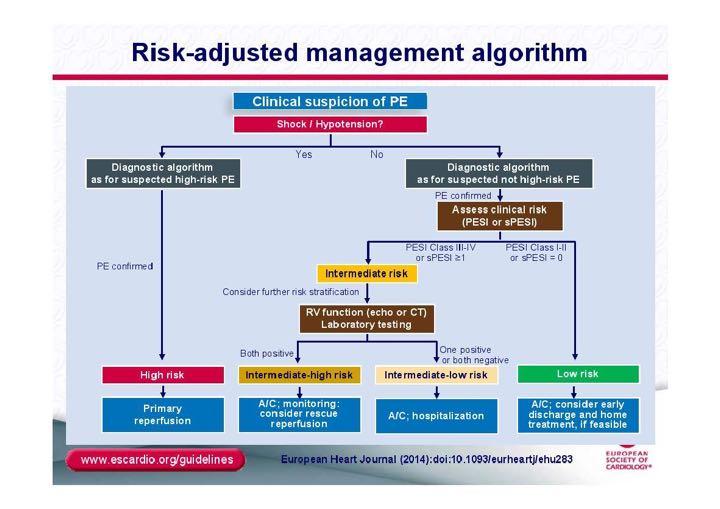
54 Suspected acute life threatening PE Hypotensive Optimize fluid status Persisting Hypotension > 15 min. Massive PE Anatomical diagnosis of PE TTE/TEE or CTPA Thrombolysis Normotensive Evidences of RV function Normotensive Clinical signs of RV failure ECG: RV strain. IRBBB Biomarkers: Troponin, BNP Echocardiography: TTE, TEE CTPA Evidence of RV dysfunction Sub-massive PE Hypotensive UFH No evidence of RV dysfunction Non-massive PE Achieve Hemodynamic goals 2 nd Thrombolysis or Surgical embolectomy or Catheter-based thrombectomy LMWH or UFH Anticoagulant and/or IVC filter Suggested algorithm for acute life threatening pulmonary embolism. PE, pulmonary embolism; RV, right ventricle; ECG, electrocardiography; BNP, brain natriuretic peptide; TTE, transthoracic echocardiography, TEE, trans-esophageal echocardiography; CTPA, computerize tomography pulmonary angiography; UFH, unfractionated heparin; LMWH, low molecular weight heparin
55 Catheter-Based Interventions
56 Contemporary Catheter Techniques 1. Conventional Catheter-Directed Thrombolysis 2. Thrombus Fragmentation 3. Rheolytic Thrombectomy 4. Suction Thrombectomy 5. Rotational Thrombectomy 6. Ultrasound Assisted Catheter-Direct Thrombolysis (USAT) 7. Pharmaco-mechanical Thrombolysis Rolf P. Engelberger, and Nils Kucher. Circulation Volume 124(19): November 8, 2011

57 Catheter Embolectomy & Fragmentation An alternative in high-risk PE patients when thrombolysis is absolutely contraindicated or has failed Kucher N Chest 2007;132:
58 Goals of Catheter-Based Therapy 1.Rapidly reducing pulmonary artery pressure, RV strain, and pulmonary vascular resistance 2.Increasing systemic perfusion 3.Facilitating RV recovery

59 Angio-Jet AngioJet-a catheter that breaks up the clot with a high speed jet of saline, heparin, or tpa that then sucks up clot using Bernoulli physics. Very little systemic drug is delivered.

60 Angio-Vac This device uses an ECMO-like system to suck up clot and then return the de-clotted blood to the venous circulation. It requires huge introducer sheaths. Oren alluded to its main benefit being intra-cavitary or vena cavae clots. Some are billing this as a replacement for embolectomy in many cases.
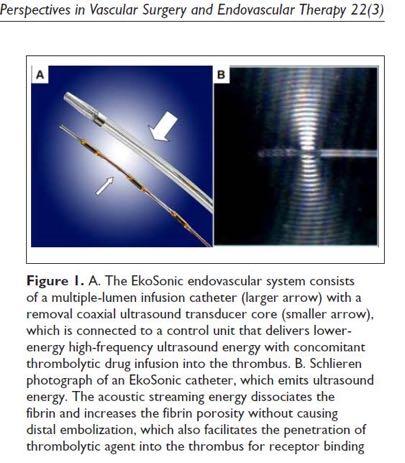
61 Eko-sonic Endovascular Catheter

62 Embolism_Systematic_Review_and_Meta-analysis_of_Modem_Techniques?enrichId=rgreq-f e32- cebef0fa7bc2&enrichsource=y292zxjqywdlozm4mduzntqyo0ftojiwnzmzmzg0nzi0ndgwmuaxndi2ndqznjq5otgw&el=1_ x_2
63 Catheter-directed Therapy for Massive Pulmonary Embolism From the overall 35 studies: 594 patients treated with catheterbased therapy, 86.5 % success rate, 2.5 % major bleeding WT Kuo 2009
64 Surgical Thrombo-embolectomy
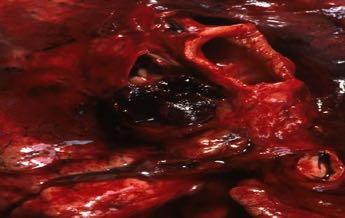

65 Surgical Embolectomy in APE: Massive
: Intimal thickening and fibrosis with or without organized thrombus proximal to segmental arteries.")
: Fibrosis, intimal webbing, and thickening with or without organized thrombus within distal segmental and subsegmental arteries only.")
66 Representative pulmonary endarterectomy specimens A, Type 1 disease (25% of cases of thromboembolic pulmonary hypertension): Fresh thrombus in the main or lobar pulmonary arteries. B, Type 2 disease (40% of cases): Intimal thickening and fibrosis with or without organized thrombus proximal to segmental arteries. In these cases, only thickened intima can be seen on initial dissection into the pulmonary arteries, occasionally with webs in the main or lobar arteries. C, Type 3 disease (30% of cases): Fibrosis, intimal webbing, and thickening with or without organized thrombus within distal segmental and subsegmental arteries only. No occlusion of vessels can be seen initially.

67 Boonsong Patjanasoontorn, MD, FCCP, FCCM

68
69 Repeated thrombolytic Therapy 8% (40 of 488 massive PE need further Mx after 1st thrombolysis)
70 RECOMMENDATIONS FOR CATHETER EMBOLECTOMY AND FRAGMENTATION & SURGICAL EMBOLECTOMY 1. Depending on local expertise, either catheter embolectomy and fragmentation or surgical embolectomy is reasonable for patients with massive PE and contraindications to fibrinolysis (Class IIa; Level of Evidence C). 2. Repeat thrombolysis or catheter embolectomy and fragmentation or surgical embolectomy is reasonable for patients with massive PE who remain unstable after receiving fibrinolysis (Class IIa; Level of Evidence C).( with in 1 hour)
71 RECOMMENDATIONS FOR CATHETER EMBOLECTOMY AND FRAGMENTATION & SURGICAL EMBOLECTOMY 3. Either catheter embolectomy or surgical embolectomy may be considered for patients with submassive acute PE judged to have clinical evidence of adverse prognosis (new hemodynamic instability, worsening respiratory failure, severe RV dysfunction, or major myocardial necrosis) (Class IIb; Level of Evidence C). 4. Catheter embolectomy and surgical thrombectomy are not recommended for patients with low-risk PE or submassive acute PE with minor RV dysfunction, minor myocardial necrosis, and no clinical worsening (Class III; Level of Evidence C).
72 Inferior Vena Cava Filters
 performed")
73 Inferior Vena Cava Filter Greenfield filter A filter placed in IVC to prevent emboli from moving into pulmonary circulation while maintaining caval patency Firstly placed in1967, but most of the IVC filter insertion (>70%) performed in the 1990s.
74 Inferior Vena Cava Filter Type of IVC Filters The Greenfield filter The Vena Tech filter The Bird s Nest filter The Nitinol filter Indications; Contraindication to anticoagulation Complication of anticoagulation Failure of anticoagulation Prophylaxis in patient with already significantly compromised pulmonary vascular bed & after embolectomy
75 Inferior Vena Cava Filter Theoretically benefits by prevent recurrent PE but Fatal complication 0.12 %, Other complications thrombosis, filter migration, filter erosion, and IVC obstr. (5-18 %) Boonsong Patjanasoontorn, MD, FCCP, FCCM
76 RECOMMENDATIONS ON IVC FILTERS IN ACUTE PE 1. Adult patients with any confirmed acute PE (or proximal DVT) with contraindications to anticoagulation or with active bleeding complication should receive an IVC filter (Class I; Level of Evidence C). 2. Anticoagulation should be resumed in patients with an IVC filter once contraindications to anticoagulation or active bleeding complications have resolved (Class I; Level of Evidence B). 3. Patients who receive retrievable IVC filters should be evaluated periodically for filter retrieval within the specific filter s retrieval window (Class I; Level of Evidence C).
77 RECOMMENDATIONS ON IVC FILTERS IN ACUTE PE 4. For patients with recurrent acute PE despite therapeutic anticoagulation, it is reasonable to place an IVC filter (Class IIa; Level of Evidence C). 5. For DVT or PE patients who will require permanent IVC filtration (eg, those with a long-term contraindication to anticoagulation), it is reasonable to select a permanent IVC filter device (Class IIa; Level of Evidence C).
78 RECOMMENDATIONS ON IVC FILTERS IN ACUTE PE 5. For DVT or PE patients with a time-limited indication for an IVC filter (eg, those with a short-term contraindication to anticoagulation therapy), it is reasonable to select a retrievable IVC filter device (Class IIa; Level of Evidence C). 6. Placement of an IVC filter may be considered for patients with acute PE and very poor cardiopulmonary reserve, including those with massive PE (Class IIb; Level of Evidence C). 7. An IVC filter should not be used routinely as an adjuvant to anticoagulation and systemic fibrinolysis in the treatment of acute PE (Class III; Level of Evidence C).

79 Summary-I Patient with clinical suspicious PE and evidence of hypotension or hypoperfusion need urgent evaluation of other possibility cause of shock and anatomically confirmation of MPE When clinical suspicion for PE is reasonable high, anticoagulant therapy should be start during further work up Anatomically confirmed Massive PE with persistent hypotension > 15 min. despite optimized fluid therapy, who don t have an absolute contraindication for, should start thrombolysis promptly PE2012: Boonsong Patjanasoontorn, MD, FCCP, FCCM

80 Summary-II The options for unsuccessful 1 st thrombolysis with confirmed residual clot are Cather-based endovascular treatment Surgical embolectomy or 2 nd Thrombolysis Patients with absolute C/I for thrombolysis, catheter-based clot fragmentation or surgical embolectomy should be considered PE2012: Boonsong Patjanasoontorn, MD, FCCP, FCCM

81 Summary-III UFH is the preferred anticoagulant of choice for submassive PE Evidence support is limited regarding thrombolytic therapy in sub-massive PE (subgroup categorization) Need further large clinical trial or meta-analysis enough to demonstrate a survival benefit & safety profile of thrombolysis compared to anticoagulation alone in submassive PE Consider IVC filter for patients with C/I, serious hemorrhagic complications, or failure anticoagulation PE2012: Boonsong Patjanasoontorn, MD, FCCP, FCCM

82 6 3 E=M.C E = m.c2



83 E = m.c 2 Albert Einstein In Physics E = m 6.c 3 Pat Boonsong In Critical Care Medicine E M C 1 C 2 C 3 = Excellence in Critical Care Medicine = Mastering of Sciences = Commitment = Competence = Compassion

84 Thank you for your attention

85
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
What is New in Acute Pulmonary Embolism? Interventional Treatment. Prof. Nils Kucher University Hospital Bern Switzerland
 What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Pulmonary Embolism 2016:
 Pulmonary Embolism 2016: Evidences & Controversies Boonsong Patjanasoontorn, MD, FRCPT FACP, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief, Division of Pulmonary
Pulmonary Embolism 2016: Evidences & Controversies Boonsong Patjanasoontorn, MD, FRCPT FACP, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief, Division of Pulmonary
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions
 Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Epidemiology of Pulmonary Embolism (PE)
") Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Use of EKOS Catheter in the management of Venous Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group
 Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Management of Pulmonary Embolism. Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School
 Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Case. Case. Management of Pulmonary Embolism in the ICU
 Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Catheter-directed Thrombolysis for Pulmonary Embolism
 Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
 Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Management of Massive and Sub-Massive Pulmonary Embolism
 Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis
 Receiving Catheter- Directed Thrombolysis") Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
Epidemiology: Incidence VTE: Mortality Morbidity Risk Factors: Acute Chronic : Genetic
 Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Management of Acute Pulmonary Embolism. Judith Hurdman Consultant Respiratory Physician
 Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
Interventional Management of Acute Pulmonary Embolism
 Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Acute and long-term treatment of VTE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
October 2017 Pulmonary Embolism
 October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment
 Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Catheter Directed Interventions for Pulmonary Embolism
 Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Interventional Treatment VTE: Radiologic Approach
 Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Pulmonary embolism: Acute management. Cecilia Becattini University of Perugia, Italy
 Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
Heart Health ESC Guidelines on the diagnosis and management of acute pulmonary embolism
 Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
How and Why to Form a PERT, Pulmonary Embolism Response Team
 Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
Management of Intermediate-Risk Pulmonary Embolism
 Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
Management of Acute Pulmonary Embolism: Anticipating and Responding to Complexity Ahmed Zaky, M.D., M.P.H. University of Alabama, Birmingham, AL
 Session: L213 Session: L403 Management of Acute Pulmonary Embolism: Anticipating and Responding to Complexity Ahmed Zaky, M.D., M.P.H. University of Alabama, Birmingham, AL Disclosures: This presenter
Session: L213 Session: L403 Management of Acute Pulmonary Embolism: Anticipating and Responding to Complexity Ahmed Zaky, M.D., M.P.H. University of Alabama, Birmingham, AL Disclosures: This presenter
Optimal Management of Intermediate-Risk Pulmonary Embolism
 Optimal Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University
Optimal Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University
The spectrum of clinical outcome of PE
 Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go?
 Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Catheter Interventions for pulmonary embolism:
 Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
VTE & Medical Patients: Case Scenario
 The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients
 The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Rationale for catheter directed therapy in pulmonary embolism
 Mini-Review Rationale for catheter directed therapy in pulmonary embolism Sailen G. Naidu, Martha-Gracia Knuttinen, J. Scott Kriegshauser, William G. Eversman, Rahmi Oklu Department of Radiology, Division
Mini-Review Rationale for catheter directed therapy in pulmonary embolism Sailen G. Naidu, Martha-Gracia Knuttinen, J. Scott Kriegshauser, William G. Eversman, Rahmi Oklu Department of Radiology, Division
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
Sachin Kumar Amruthlal Jain, 1 Brijesh Patel, 2 Wadie David, 2 Ayad Jazrawi, 1 and Patrick Alexander Introduction
 Hindawi Publishing Corporation Case Reports in Medicine Volume 2014, Article ID 297951, 8 pages http://dx.doi.org/10.1155/2014/297951 Case Report Unloading of Right Ventricle and Clinical Improvement after
Hindawi Publishing Corporation Case Reports in Medicine Volume 2014, Article ID 297951, 8 pages http://dx.doi.org/10.1155/2014/297951 Case Report Unloading of Right Ventricle and Clinical Improvement after
Interventional treatment for patients with acute pulmonary embolism
 Interventional treatment for patients with acute pulmonary embolism I. Petrov, I. Martinov Cardiology department Tokuda Hospital Sofia I. Petrov, Treatment and prophylaxis of PE Treatment of PE: 1.) Systemic
Interventional treatment for patients with acute pulmonary embolism I. Petrov, I. Martinov Cardiology department Tokuda Hospital Sofia I. Petrov, Treatment and prophylaxis of PE Treatment of PE: 1.) Systemic
Acute and long-term treatment of PE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
Bilateral Central Pulmonary Embolism and Recent History of Ischemic Stroke
 WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
Recent advances in the management of pulmonary embolism. Kodati Rakesh SR Pulmonary medicine
 Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
Acute Management of Pulmonary Embolism
 Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Thrombus Removal in Acute Pulmonary Embolism: When and How?
 Thrombus Removal in Acute Pulmonary Embolism: When and How? Kenneth Rosenfield, MD, MHCDS, MSCAI Cardiology Division Section of Vascular Medicine and Intvn MGH Kenneth Rosenfield, MD, MHCDS Conflicts of
Thrombus Removal in Acute Pulmonary Embolism: When and How? Kenneth Rosenfield, MD, MHCDS, MSCAI Cardiology Division Section of Vascular Medicine and Intvn MGH Kenneth Rosenfield, MD, MHCDS Conflicts of
Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski. Department of Surgery Grand Rounds March 24, 2008
 Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski Department of Surgery Grand Rounds March 24, 2008 History of Vena Cava Filters Virchow-1846-Proposes PE originate from veins
Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski Department of Surgery Grand Rounds March 24, 2008 History of Vena Cava Filters Virchow-1846-Proposes PE originate from veins
Pulmonary Embolectomy:
 Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Pulmonary Embolism Newer Concepts and Role of Thrombolysis
 CHAPTER 69 Pulmonary Embolism Newer Concepts and Role of Thrombolysis J. P. S. Sawhney, A. Bakhshi, B. Kandpal Introduction Pulmonary embolism (PE) is a common cardiovascular and cardiopulmonary illness
CHAPTER 69 Pulmonary Embolism Newer Concepts and Role of Thrombolysis J. P. S. Sawhney, A. Bakhshi, B. Kandpal Introduction Pulmonary embolism (PE) is a common cardiovascular and cardiopulmonary illness
Risk-Based Evaluation and Management of VTE
 12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital
 Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
Diagnosis and initial treatment of patients with suspected pulmonary thromboembolism
 Diagnosis and initial treatment of patients with suspected pulmonary thromboembolism Pulmonary thromboembolism (PTE) remains a frequently occurring diagnostic problem, with an incidence of approximately
Diagnosis and initial treatment of patients with suspected pulmonary thromboembolism Pulmonary thromboembolism (PTE) remains a frequently occurring diagnostic problem, with an incidence of approximately
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Guideline for Thrombolysis Therapy in Pulmonary Embolism
 Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
Acoustic Pulse Thrombolysis Treatment
 Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
CARDIAC PROBLEMS IN PREGNANCY
 CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
Oxford Medicine Online
 Oxford Medicine Online The ESC Textbook of Intensive and Acute Cardiovascular Care (2 ed.) Edited by Marco Tubaro, Pascal Vranckx, Susanna Price, and Christiaan Vrints Latest update This online textbook
Oxford Medicine Online The ESC Textbook of Intensive and Acute Cardiovascular Care (2 ed.) Edited by Marco Tubaro, Pascal Vranckx, Susanna Price, and Christiaan Vrints Latest update This online textbook
Venous interventions in DVT
 Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
4/18/2018. Objectives. Background. 1) Compare and contrast the various validated tools for the identification of patients with pulmonary embolism
 Compare and contrast the various validated tools for the identification of patients with pulmonary embolism") Pulmonary Embolism: Assessment, risk-stratification, and treatment plan for the outpatient management of low-risk patients Presentation by Joshua T. Wood, PharmD/PGY-1 Resident Providence St. Patrick Hospital;
Pulmonary Embolism: Assessment, risk-stratification, and treatment plan for the outpatient management of low-risk patients Presentation by Joshua T. Wood, PharmD/PGY-1 Resident Providence St. Patrick Hospital;
EKOS. Interventional Vascular 3 February, Imagine where we can go.
 EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
ORIGINAL INVESTIGATION. Thrombolysis vs Heparin in the Treatment of Pulmonary Embolism
 Thrombolysis vs Heparin in the Treatment of Pulmonary Embolism A Clinical Outcome Based Meta-analysis ORIGINAL INVESTIGATION Giancarlo Agnelli, MD; Cecilia Becattini, MD; Timo Kirschstein, MD Background:
Thrombolysis vs Heparin in the Treatment of Pulmonary Embolism A Clinical Outcome Based Meta-analysis ORIGINAL INVESTIGATION Giancarlo Agnelli, MD; Cecilia Becattini, MD; Timo Kirschstein, MD Background:
Chapter 1. Introduction
 Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Med Sci Monit, 2016; 22: Grade D. Quality Outstanding
 Ain and Jaff. Treatment of Submassive Pulmonary Embolism: Knowing When to be Aggressive and When to be Conservative. Curr Treat Options Cardio Med (2015) 17:25. Review Article Akin et al. Catheter-Directed
Ain and Jaff. Treatment of Submassive Pulmonary Embolism: Knowing When to be Aggressive and When to be Conservative. Curr Treat Options Cardio Med (2015) 17:25. Review Article Akin et al. Catheter-Directed
4/24/2017 CATHETER-DIRECTED THERAPIES FOR ACUTE PE THE GREY AREA OF SUBMASSIVE PE DISCLOSURES OBJECTIVES: INTRAVASCULAR LYTIC THERAPY
 THE GREY AREA OF SUBMASSIVE PE CATHETER-DIRECTED THERAPIES FOR ACUTE PE Submassive PE PE with RV strain Saad Farooqi, MD Pulmonary/Critical Care Fellow Fatal PE Concept borrowed from Jeffrey A. Kline,
THE GREY AREA OF SUBMASSIVE PE CATHETER-DIRECTED THERAPIES FOR ACUTE PE Submassive PE PE with RV strain Saad Farooqi, MD Pulmonary/Critical Care Fellow Fatal PE Concept borrowed from Jeffrey A. Kline,
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Surgical Thrombectomy for PE: Is it Making a Comeback
 Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary embolism. Paweł Balsam
 Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
ORIGINAL INVESTIGATION
 ORIGINAL INVESTIGATION Prognostic Role of Echocardiography Among Patients With Acute Pulmonary Embolism and a Systolic Arterial Pressure of 90 mm Hg or Higher Nils Kucher, MD; Elisa Rossi, BS; Marisa De
ORIGINAL INVESTIGATION Prognostic Role of Echocardiography Among Patients With Acute Pulmonary Embolism and a Systolic Arterial Pressure of 90 mm Hg or Higher Nils Kucher, MD; Elisa Rossi, BS; Marisa De
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Emergency Pulmonary Embolectomy after Failed Thrombolysis in a Community Hospital: A Choice of Institutional Preference?
 ISPUB.COM The Internet Journal of Emergency Medicine Volume 5 Number 1 Emergency Pulmonary Embolectomy after Failed Thrombolysis in a Community Hospital: A Choice of F Vandy, G Fromm, P Guentert, W Halloran,
ISPUB.COM The Internet Journal of Emergency Medicine Volume 5 Number 1 Emergency Pulmonary Embolectomy after Failed Thrombolysis in a Community Hospital: A Choice of F Vandy, G Fromm, P Guentert, W Halloran,
Surgical Management in Chronic Thromboembolic Pulmonary Hypertension. Michael Bates, MD, FACS Ochsner Health System, New Orleans, LA
 Surgical Management in Chronic Thromboembolic Pulmonary Hypertension Michael Bates, MD, FACS Ochsner Health System, New Orleans, LA Disclosures No industry conflicts I am a surgeon and always disclose
Surgical Management in Chronic Thromboembolic Pulmonary Hypertension Michael Bates, MD, FACS Ochsner Health System, New Orleans, LA Disclosures No industry conflicts I am a surgeon and always disclose
Inferior Vena Cava Filters
 Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Systemic or local thrombolysis in high-risk pulmonary embolism
 original article Cardiology Journal 2015, Vol. 22, No. 4, 467 474 DOI: 10.5603/CJ.a2014.0103 Copyright 2015 Via Medica ISSN 1897 5593 Systemic or local thrombolysis in high-risk pulmonary embolism Liviu
original article Cardiology Journal 2015, Vol. 22, No. 4, 467 474 DOI: 10.5603/CJ.a2014.0103 Copyright 2015 Via Medica ISSN 1897 5593 Systemic or local thrombolysis in high-risk pulmonary embolism Liviu
Handbook for Venous Thromboembolism
 Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Supplementary Online Content
 Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC
 David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC") Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
Epidermiology Early pulmonary embolism
 Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION
 IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION Resident(s): George Athanasatos Attending(s): Daniel Golwyn Program/Dept: Interventional Radiology CHIEF
IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION Resident(s): George Athanasatos Attending(s): Daniel Golwyn Program/Dept: Interventional Radiology CHIEF
Severe pulmonary embolism: surgical aspects. Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland
 Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism
Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism