Catheter Directed Interventions for Pulmonary Embolism
|
|
|
- Gyles Lee
- 6 years ago
- Views:
Transcription

1 Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh, PA Georgia Vascular Society 9/9/2017 1

2 Disclosures No financial disclosures Co-PI SUNSET-PE trial 2
3 PE - Increasing Incidence Most common preventable cause of in-hospital death 3 rd most common CV disease after MI and stroke 4% will develop Pulmonary Hypertension at 2-3 years Huang et al - Am J Med 2014
 thrombolysis Catheter-directed")
4 Introduction Acute pulmonary embolism (PE) Accounts for 5-10% of inhospital deaths Treatment strategies Anticoagulation Surgical thrombectomy IV (systemic) thrombolysis Catheter-directed thrombolysis


5 PE Clinical Presentation Non Homogenous Non Massive Low Risk No RVD No + Biomarkers Massive High Risk Hypotension Submassive Intermediate Risk +/- ECHO RVD +/- Biomarkers 5

6 CASE 57 year old man Sudden onset SOB Chest pain BP 100/60 HR 102 at rest RR 22/min Sat 89% 6

7 CASE Troponin 1.5 BNP 3,400 RV LV Will Removal of Thrombus Make a Difference in his Clinical Course and Outcome? 7


8 140 PUBMED CITATIONS PULMONARY EMBOLISM & CATHETER
9 Physiological Benefits of Early Clot Removal (Thrombolysis or Extraction) Improved clot resolution Faster? More complete? Improved angiographic flow and lung perfusion Reduction PA pressure and improvement RV function Stabilization of hemodynamics Less need for pressors and life support Jaff et al Circulation
10 Additional Theoretical Benefits of Early Clot Removal Fewer in hospital complications from PE Removal of threatening clot in transit Earlier discharge & return to functional baseline Reduced incidence of pulmonary hypertension Avgerinos ED, Chaer RA. J Vasc Surg


11 PE Treatment Guidance Low Evidence AHA 2011 Guidelines ESC 2014 Guidelines ACCP 2016 Guidelines No RV Dysfunction Evidence of RV Dysfunction or Myocardial Necrosis Sustained Hypotension Low-Risk Submassive Massive Low-Risk Intermediate -High Intermediate -Low High-Risk Insufficient Evidence Limits the Guidelines New PE trial Data may be Changing the Landscape Low-Risk Intermediate Risk High-Risk Anticoagulation Thrombolysis Thrombectomy Risk > benefit Potential benefit (Selected Patients) Benefit
 but more major bleeding events (OR 2.73) Mortality: 47% Relative Risk Reduction Major Bleed: 9.2% Stroke: 1.")
12 Systemic Thrombolysis Systemic thrombolysis vs. AC is associated with lower mortality (OR 0.53) but more major bleeding events (OR 2.73) Mortality: 47% Relative Risk Reduction Major Bleed: 9.2% Stroke: 1.5% Chatterjee et al JAMA 2014

13 Catheter Directed Interventions In intermediate risk PE ultrasound assisted catheter directed thrombolysis was superior to heparin alone in reversing RV dilatation at 24 hours, without an increase in bleeding events Kucher et al Circulation 2014 US National Inpatient Sample


14 Catheter Interventions for PE It is more than a catheter




15 Catheter Interventions for PE Standard Catheter Thrombolysis Ultrasound Assisted Thrombolysis Percutaneous clot extraction When to use them? Which technique?
16 Mortality Risk 15-30% 3-15% 1% Konstantinides, et al. European Heart J 2014

17 Interventions for PE Who to Intervene on? Careful patient selection Low bleeding risk Massive PE Submassive PE Severe RV strain Myocardial necrosis Deteriorating respiratory function Mortality Reduction Prevent Decompensation Pulm. Hypertension
18 Bleeding Risk Davies, et al. Ann Vasc Surg J 2016
19 Catheter Interventions for PE Catheter Directed Interventions (CDIs) Thrombolysis Catheter directed dripping Ultrasound assisted dripping Pharmacomechanical (PMT) Thrombus fragmentation/aspiration w/o lytics Combined techniques

20 Interventions for PE

21 Interventions for PE Thrombolysis Standard Catheter Thrombolysis Multisidehole catheter introduced within the clot hour tpa infusion 0.5-2mg/hour tpa penetrate & soften clot particles
22
 Most literature supporting it FDA approved ULTIMA RCT SEATTLE II Registry Multiple small series OPTALYSE PE No evidence of superiority UPMC Randomized Trial 2016 SUNSET PE EKOS vs")
23 Interventions for PE Thrombolysis Ultrasound Assisted Thrombolysis (EKOS) Technically similar to catheter directed dripping Ultrasound may reduce dripping time & tpa dose (?) Most literature supporting it FDA approved ULTIMA RCT SEATTLE II Registry Multiple small series OPTALYSE PE No evidence of superiority UPMC Randomized Trial 2016 SUNSET PE EKOS vs Standard Catheter Lysis

24
25 ULTIMA trial Randomized Controlled Trial of Ultrasound-Assisted Catheter-Directed Thrombolysis for Acute Intermediate-Risk Pulmonary Embolism Anticoagulation vs. USAT mg tpa over 15 hours USAT superior in reversing RV dilatation at 24 hrs. Equivalent hemodynamic outcomes at 90 days Circulation, November 2013




26 Interventions for PE Thrombolysis Pharmacomechanical Thrombolysis (mpe) Shorter procedural time Faster reperfusion Lower (or no) lytic dose Bradycardia / arrest Death Hemolysis Renal failure FDA Black box warning Rapid Lysis Lower rate of bleeding complications
27 Interventions for PE - Clot Extraction Thrombectomy Devices Small bore Aspiration Catheters/Systems Large bore Aspiration Catheters/Systems 27

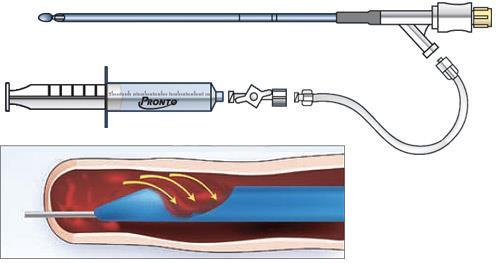
 Aspire (Control Medical")
28 Interventions for PE - Clot Extraction Thrombectomy Devices Small bore Aspiration Catheters/Systems Pronto Catheter (Vascular Solutions) Aspire (Control Medical Technology) 28


29 Interventions for PE
 Angiovac (Angiodynamics) en bloc removal Indigo (Penumbra Inc) Flowtriever (Inari medical)")
30 Interventions for PE Thrombectomy Devices Large bore Aspiration Catheters (Rapid debulking of proximal thrombus) Angiovac (Angiodynamics) en bloc removal Indigo (Penumbra Inc) Flowtriever (Inari medical) 30
, OTW Specialized funnel shaped")

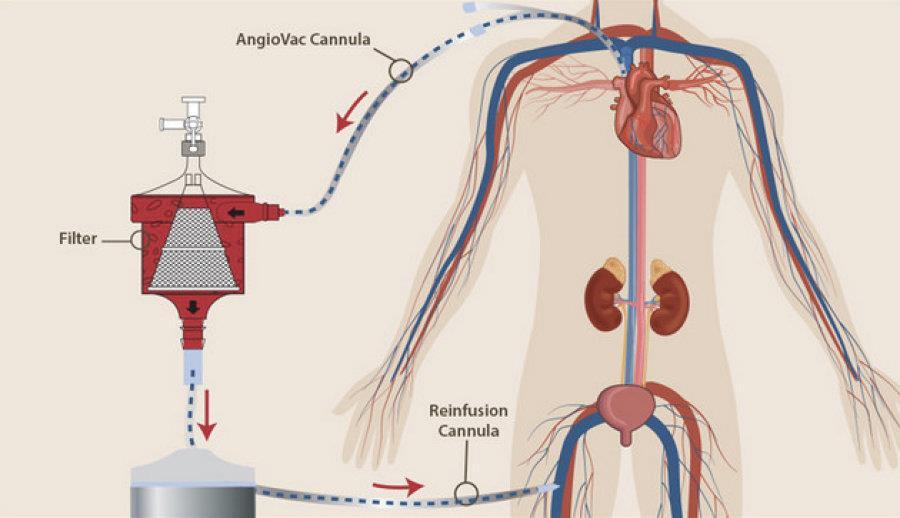
31 AngioVac (Angiodynamics) Open or Percutaneous DVT, PE Large bore (22F), OTW Specialized funnel shaped tip Remotely deployable Prevent vessel collapse No longer recommended for PE given the risk of valvular injury
32 Suction Thrombectomy Device Sheath size Mechanism of Action Penumbra Indigo 6-8 Fr Suction pump aspiration Inari Flowtriever 22 Fr Disruption, retraction, aspiration Angiovac 26 Fr Large volume aspiration with return of filtered blood Pronto XI Catheter 6-14 Fr Manual aspiration

33 Interventions for PE Efficacy & Safety Outcomes RCT Trial Pts CDI Failure Kuo et. al 2009 ULTIMA PERFECT 2015 SEATTLE II 2015 NIS Data 2015 Major Bleed ICH 594 ~13.5% ~3.2% 0.1% 30 0% 0% 0% 101 ~5.9% 0% 0% 150 ~14.0% 10% 0% 352 ~13.9% ~3.7% 0.3% 33
34 PE Catheter Treatment Guidelines AHA 2011 Guidelines ESC 2014 Guidelines ACCP 2016 Guidelines Intermediate High Risk Cath. Thrombectomy when 1. Lysis is contraindicated 2. Lysis failed Cath. Treatment when 1. Lysis is contraindicated Syst. Lysis should be preferred over Catheter lysis unless higher risk of bleeding High Risk (Massive) Cath. Thrombectomy when 1. Lysis is contraindicated 2. Lysis failed Cath. Treatment when 1. Lysis is contraindicated 2. Lysis failed Suction Thrombectomy when 1. Lysis is contraindicated 2. Lysis failed
35 Interventions for PE UPMC Experience Acute PE Team PERT (Pulmonary Embolism Response Team) Members Pulmonary Vascular Cardiology Cardiac Surgery Hematology Referring Physician pages the PE Team Consult (Pulmonary) Attending quickly reviews the case, assesses patient and consults oncall interventional teams PE Team discusses treatment options 35



36 PERT and Vascular Surgeons Who is the Pulmonary Interventionalist? PE intervention is not owned by any specialty Depends on each individual institution and local policies Whoever answers the call first 36
37 UPMC Algorithm High Risk Intermediate - High Intermediate - Low Low Risk Assess Bleed Risk AC vs IVC Filter Low Systemic tpa + Heparin +/- ECMO High Surg. Thrombectomy or Suction Thrombectomy +/- ECMO Low or Intermediate AC High IVC filter Low Intermediate High Catheterdirected tpa + AC AC IVC filter
38 Case presentation 67 year old female Admitted to outside hospital for nausea, vomiting, lightheadedness and syncope on 6/27/16 In setting of newly diagnosed colon cancer status post sigmoid resection and ileostomy creation May 2016 Last chemo 1 week before Treated with IVF and improving
39 HPI On 7/1/2016 had sudden PEA arrest Underwent 12 minutes of CPR and had ROSC Post-arrest EKG: New RBB Post-arrest Echo: RV strain Transferred to UPMC On presentation, hypotensive requiring levophed Large groin hematoma from central line placement
40 Exam Vitals HR 115 BP 126/69 (on levophed) Sats 100% on 100% FiO2 Responding to commands, moving all four extremities Right groin hematoma Pedal doppler signals
41 Laboratory H/H: 9.5/29.4 Platelets 85 Cr 1.69 Troponin 0.38
42 Imaging Echo RV strain RV hypokinesis with preserved apical function (McConnell sign) CTA Near occlusion of the distal left PA Clot burden extends into the left upper lobe lingula and left lower lobe PA branches Subocclusive clot within the branches of the right upper lobe right middle lobe as well as right lower lobe PAs

43 CTA

44 CTA

45 Mortality risk PESI Score: 187

46 Mortality risk 30d MORTALITY 52% 25% 11% 1%
47 Bleeding risk Recent CPR Right groin hematoma Thrombocytopenia High Risk of Bleed
48 UPMC Algorithm Assess Bleed Risk Low Systemic tpa + Heparin +/- ECMO High Surg. Thrombectomy or Catheter Intervention +/- ECMO
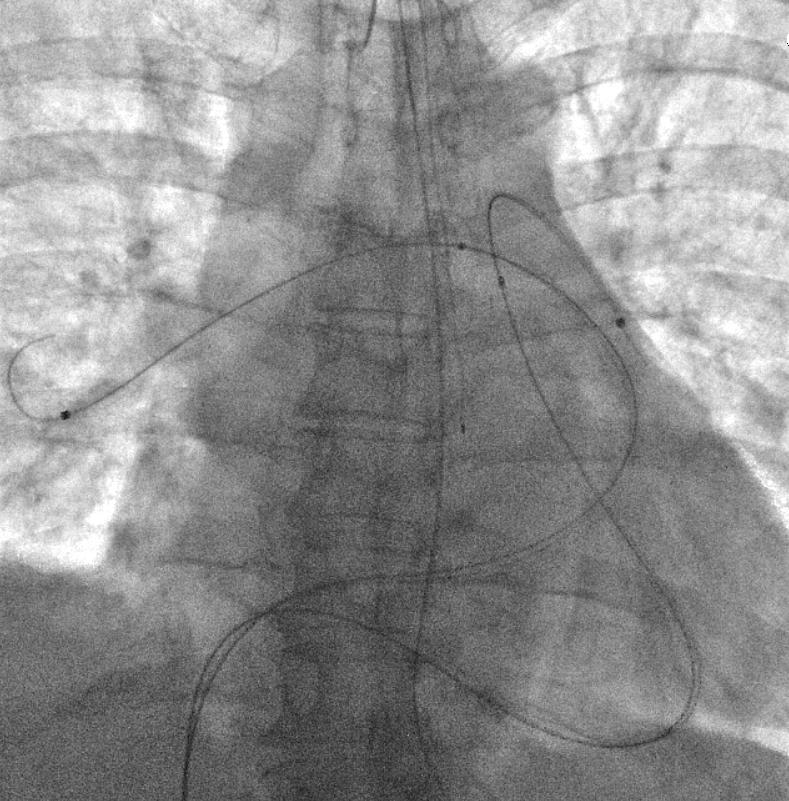
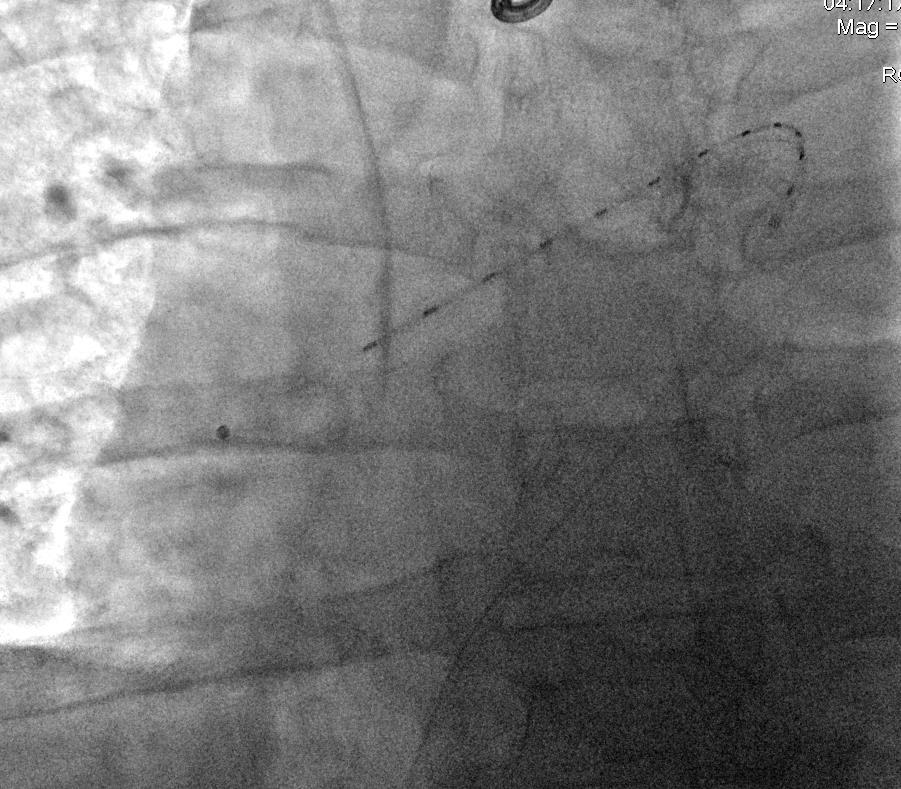
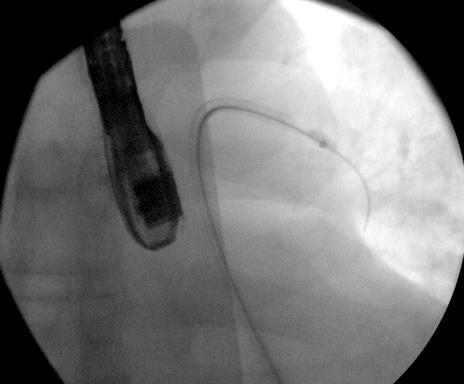
49 Intervention: Suction Thrombectomy
50 Intervention


51 Suction thrombectomy Initial PA pressure 53, HR 115

52 Suction thrombectomy

53 Suction thrombectomy Final PA Pressure 49, HR 80
54 Outcome Extubated the following day Expanding groin hematoma while transitioning to coumadin Managed conservatively Discharged to home on POD 9
55 Interventions for PE UPMC Experience ~135 cases (12% massive PE) over 4 years
56 Interventions for spe UPMC Experience Outcomes AC (64) spe CDI (64) P value Major Bleeding 3(4.7%) 4(6.3%) Minor Bleeding 0 6(9.4%) Stroke 0 0 Arrest 0 3 (4.7%) Decompensation 0 3 (4.7%) In hospital death 3 (4.7%) 1 (1.6%) In hospital PE 1(1.6%) 1(1.6%) death ICU Days 5.6± ± Day Death dependence at FU
57 Interventions for spe UPMC Experience Echocardiographic parameters: Trend for a greater decrease in the mean RV/LV ratio in the CDI group at 30 days: 0.27±0.15 vs. 0.17±0.12 for AC (P=.076),. At 1 year, echo parameters were similar between the groups and pulmonary hypertension (PAP>40mmHg) was present in 7/15 of the AC group vs 6/19 of the CDI group (P=.484). Dyspnea and/or oxygen dependence were present in 12% of patients in the AC group, vs. 14% in the CDI group (P=.774). 57
58 Interventions for PE UPMC Experience Clinical Success: 87% (Massive: 50%, Submassive: 92%) Faster RV function recovery (vs Anticoagulation or SL) 7.4% major adverse events (1 ischemic stroke) Systemic Bleed (7) Heart/valve Injury (2) Less complications than systemic lysis (more than AC) Conversion to surgical thrombectomy: 2.9% Mortality: 3%
59 CDT vs USAT. Presented at the AVF Demographics CDT (n=27) USAT (n=36) p Age ± ± Male Sex 37% 47% 0.45 PE Severity High risk 22% 6% Intermediate risk 78% 94% Hypercoagulable State 11% 8% 1.00 Recent Surgery 33% 17% 0.15 Malignancy 11% 19% 0.49 Hormone Therapy 7% 8% 1.00 Recent Travel 15% 22% 0.53 DVT 44% 56% 0.45 History of DVT 22% 14% 0.51 History of PE 22% 11% 0.30 CAD 15% 11% 0.72 CHF 4% 6% 1.00 Pulmonary HTN 4% 6% 1.00
60 Echocardiographic Changes at One Year CDT USAT Baseline 1-year Baseline 1-year P* RV/LV Ratio 1.10 ± ± ± ± Tricuspid Regurg. Jet Velocity (m/s) 3.25 ± ± ± ± Systolic PA Pressure (mmhg) ± ± ± ± RV Dilation 10 (90%) 2 (17%) 15 (100%) 6 (67%) 0.18 RV Systolic Dysfunction 10 (90%) 0 (0%) 11 (73%) 1 (7%) 1.00 * comparisons accounting for repeated measures
61 Conclusions CDT/USAT for spe can result in faster restoration of RV function and shorter ICU stay, though with similar midterm outcomes with AC alone. Lower dose of thrombolytic compared to systemic lysis Minimal bleeding complication There may be no difference in outcomes or adverse bleeding risk between CDT and USAT.
62 Conclusions Catheter Interventions are increasingly used in spe Catheter interventions are safe and effective Major bleed 2.9% (vs. 7.7% for SL (JAMA 2014)) 81% of patients showed ECHO RV dysfunction improvement
63 Conclusions Faster Clot removal & RV function recovery Prevention of RV failure / decompensation Prevention of Pulmonary Hypertension? The potential impact of CDI on mortality and pulmonary hypertension needs further investigation through larger studies They are not complication-free but complications are less than with systemic lysis Pulmonary Embolism Response Team function facilitates optimal decision making 63

64 UPMC VASCULAR SURGERY Thank you for your attention PITTSBURGH 64
Catheter Interventions for pulmonary embolism:
 Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions
 Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
 Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Thrombus Removal in Acute Pulmonary Embolism: When and How?
 Thrombus Removal in Acute Pulmonary Embolism: When and How? Kenneth Rosenfield, MD, MHCDS, MSCAI Cardiology Division Section of Vascular Medicine and Intvn MGH Kenneth Rosenfield, MD, MHCDS Conflicts of
Thrombus Removal in Acute Pulmonary Embolism: When and How? Kenneth Rosenfield, MD, MHCDS, MSCAI Cardiology Division Section of Vascular Medicine and Intvn MGH Kenneth Rosenfield, MD, MHCDS Conflicts of
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Use of EKOS Catheter in the management of Venous Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group
 Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
What is New in Acute Pulmonary Embolism? Interventional Treatment. Prof. Nils Kucher University Hospital Bern Switzerland
 What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
PULMONARY EMBOLISM AND PERT. Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology
 PULMONARY EMBOLISM AND PERT Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology No financial disclosures 1. What are the clinical signs/symptoms of submassive PE? 2.
PULMONARY EMBOLISM AND PERT Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology No financial disclosures 1. What are the clinical signs/symptoms of submassive PE? 2.
Interventional Management of Acute Pulmonary Embolism
 Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis
 Receiving Catheter- Directed Thrombolysis") Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
EKOS. Interventional Vascular 3 February, Imagine where we can go.
 EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
Management of Pulmonary Embolism. Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School
 Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
Management of Acute Pulmonary Embolism. Judith Hurdman Consultant Respiratory Physician
 Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Massive and Sub-Massive Pulmonary Embolism
 Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
How and Why to Form a PERT, Pulmonary Embolism Response Team
 Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
Bilateral Central Pulmonary Embolism and Recent History of Ischemic Stroke
 WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
Catheter-directed Thrombolysis for Pulmonary Embolism
 Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Case. Case. Management of Pulmonary Embolism in the ICU
 Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients
 The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment
 Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
Epidemiology: Incidence VTE: Mortality Morbidity Risk Factors: Acute Chronic : Genetic
 Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Acoustic Pulse Thrombolysis Treatment
 Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
Technique de recanalisation: mon expérience avec Aspirex
 JFICV 2017, Deauville Thrombose veineuse profonde aiguë en 2017 Technique de recanalisation: mon expérience avec Aspirex Romaric LOFFROY Département de Radiologie Diagnostique et Thérapeutique CHU Hôpital
JFICV 2017, Deauville Thrombose veineuse profonde aiguë en 2017 Technique de recanalisation: mon expérience avec Aspirex Romaric LOFFROY Département de Radiologie Diagnostique et Thérapeutique CHU Hôpital
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
4/24/2017 CATHETER-DIRECTED THERAPIES FOR ACUTE PE THE GREY AREA OF SUBMASSIVE PE DISCLOSURES OBJECTIVES: INTRAVASCULAR LYTIC THERAPY
 THE GREY AREA OF SUBMASSIVE PE CATHETER-DIRECTED THERAPIES FOR ACUTE PE Submassive PE PE with RV strain Saad Farooqi, MD Pulmonary/Critical Care Fellow Fatal PE Concept borrowed from Jeffrey A. Kline,
THE GREY AREA OF SUBMASSIVE PE CATHETER-DIRECTED THERAPIES FOR ACUTE PE Submassive PE PE with RV strain Saad Farooqi, MD Pulmonary/Critical Care Fellow Fatal PE Concept borrowed from Jeffrey A. Kline,
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
Emerging Tools for Lytic-Free, Single-Session Treatment of Venous Thromboembolic Disease
 FEATURED TECHNOLOGY THE CLOTTRIEVER AND FLOWTRIEVER SYSTEMS Emerging Tools for Lytic-Free, Single-Session Treatment of Venous Thromboembolic Disease The ClotTriever Outcomes (CLOUT) registry principal
FEATURED TECHNOLOGY THE CLOTTRIEVER AND FLOWTRIEVER SYSTEMS Emerging Tools for Lytic-Free, Single-Session Treatment of Venous Thromboembolic Disease The ClotTriever Outcomes (CLOUT) registry principal
Percutaneously Inserted AngioVac Suction Thrombectomy for the Treatment of Filter-Related. Iliocaval Thrombosis
 Percutaneously Inserted AngioVac Suction Thrombectomy for the Treatment of Filter-Related Iliocaval Thrombosis Faiz D. Francis, DO; Gianvito Salerno, MD; Sabbah D. Butty, MD Abstract In the setting of
Percutaneously Inserted AngioVac Suction Thrombectomy for the Treatment of Filter-Related Iliocaval Thrombosis Faiz D. Francis, DO; Gianvito Salerno, MD; Sabbah D. Butty, MD Abstract In the setting of
Methods of Thrombus Fragmentation & Extraction. Methods of Thrombus Extraction
 Thrombus Fragmentation and Extraction: Clinical Evidence and Practical Application No Relevant Disclosures Venita Chandra, MD Clinical Assistant Professor of Surgery Division of Stanford Medical School,
Thrombus Fragmentation and Extraction: Clinical Evidence and Practical Application No Relevant Disclosures Venita Chandra, MD Clinical Assistant Professor of Surgery Division of Stanford Medical School,
Percutaneous Mechanical Thrombectomy for Acute Iliofemoral DVT with the Aspirex Catheter: The Dijon Experience
 JFICV 2018, Beaune Percutaneous Mechanical Thrombectomy for Acute Iliofemoral DVT with the Aspirex Catheter: The Dijon Experience Prof. Romaric LOFFROY, MD, PhD, FCIRSE Chief, Department of Vascular and
JFICV 2018, Beaune Percutaneous Mechanical Thrombectomy for Acute Iliofemoral DVT with the Aspirex Catheter: The Dijon Experience Prof. Romaric LOFFROY, MD, PhD, FCIRSE Chief, Department of Vascular and
Epidemiology of Pulmonary Embolism (PE)
") Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Intervention for Deep Venous Thrombosis and Pulmonary Embolus
 Intervention for Deep Venous Thrombosis and Pulmonary Embolus Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard
Intervention for Deep Venous Thrombosis and Pulmonary Embolus Michael R. Jaff, DO Paul and Phyllis Fireman Endowed Chair in Vascular Medicine Massachusetts General Hospital Professor of Medicine Harvard
Pharmaco-mechanical techniques stand alone procedures? Peter Neglén, MD, PhD SP Vascular Center Limassol Cyprus
 Pharmaco-mechanical techniques stand alone procedures? Peter Neglén, MD, PhD SP Vascular Center Limassol Cyprus Faculty Disclosure Peter Neglén, M.D., Ph.D Stockholder/Founder of Veniti, Inc. Member, Medical
Pharmaco-mechanical techniques stand alone procedures? Peter Neglén, MD, PhD SP Vascular Center Limassol Cyprus Faculty Disclosure Peter Neglén, M.D., Ph.D Stockholder/Founder of Veniti, Inc. Member, Medical
Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT) Initial Results From a Prospective Multicenter Registry
 Initial Results From a Prospective Multicenter Registry") [ Original Research Pulmonary Vascular Disease ] Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT) Initial Results From a Prospective Multicenter Registry William
[ Original Research Pulmonary Vascular Disease ] Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT) Initial Results From a Prospective Multicenter Registry William
Catheter Based Therapy for PE: Who and How?
 Catheter Based Therapy for PE: Who and How? Jay Giri, MD MPH Assistant Professor of Medicine Director, Pulmonary Embolism Response Team Associate Director, Penn Cardiovascular Quality, Outcomes & Evaluative
Catheter Based Therapy for PE: Who and How? Jay Giri, MD MPH Assistant Professor of Medicine Director, Pulmonary Embolism Response Team Associate Director, Penn Cardiovascular Quality, Outcomes & Evaluative
Venous interventions in DVT
 Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Interventional Treatment VTE: Radiologic Approach
 Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Acute Management of Pulmonary Embolism
 Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Expanding Horizons: AngioVac Suction Thrombectomy at UTHealth
 Expanding Horizons: AngioVac Suction Thrombectomy at UTHealth Naveed Saqib, MD Assistant Professor Department of Cardiothoracic and Vascular Surgery McGovern Medical School The University of Texas Science
Expanding Horizons: AngioVac Suction Thrombectomy at UTHealth Naveed Saqib, MD Assistant Professor Department of Cardiothoracic and Vascular Surgery McGovern Medical School The University of Texas Science
Surgical Thrombectomy for PE: Is it Making a Comeback
 Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Management of sub-massive and massive pulmonary embolism:
 Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
SESSION 4 12:45 2:15 PM
 SESSION 4 12:45 2:15 PM Pulmonary Embolism Update SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza, MD, MS:
SESSION 4 12:45 2:15 PM Pulmonary Embolism Update SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza, MD, MS:
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support
 Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Acute and long-term treatment of VTE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Rationale for catheter directed therapy in pulmonary embolism
 Mini-Review Rationale for catheter directed therapy in pulmonary embolism Sailen G. Naidu, Martha-Gracia Knuttinen, J. Scott Kriegshauser, William G. Eversman, Rahmi Oklu Department of Radiology, Division
Mini-Review Rationale for catheter directed therapy in pulmonary embolism Sailen G. Naidu, Martha-Gracia Knuttinen, J. Scott Kriegshauser, William G. Eversman, Rahmi Oklu Department of Radiology, Division
Aggressive endovascular management of ilio-femoral DVT. thrombotic syndrome. is the key in preventing post
 CACVS 2017 Aggressive endovascular management of ilio-femoral DVT is the key in preventing post thrombotic syndrome ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HEALTH SYSTEM
CACVS 2017 Aggressive endovascular management of ilio-femoral DVT is the key in preventing post thrombotic syndrome ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HEALTH SYSTEM
Intraoperative Pulmonary Embolus
 PBLD Table #5 Intraoperative Pulmonary Embolus Holly Richter, M.D. and Sean Benton, D.O. Objectives 1. Determine patients who are at risk for perioperative pulmonary embolism 2. Form a differential diagnosis
PBLD Table #5 Intraoperative Pulmonary Embolus Holly Richter, M.D. and Sean Benton, D.O. Objectives 1. Determine patients who are at risk for perioperative pulmonary embolism 2. Form a differential diagnosis
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Case 1:
 12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Successful recanalisation of venous thrombotic occlusions with Aspirex mechanical thrombectomy. Michael K. W. Lichtenberg
 Successful recanalisation of venous thrombotic occlusions with Aspirex mechanical thrombectomy Michael K. W. Lichtenberg Disclosure Speaker name: Michael Lichtenberg... I have the following potential conflicts
Successful recanalisation of venous thrombotic occlusions with Aspirex mechanical thrombectomy Michael K. W. Lichtenberg Disclosure Speaker name: Michael Lichtenberg... I have the following potential conflicts
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION
 IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION Resident(s): George Athanasatos Attending(s): Daniel Golwyn Program/Dept: Interventional Radiology CHIEF
IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION Resident(s): George Athanasatos Attending(s): Daniel Golwyn Program/Dept: Interventional Radiology CHIEF
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
Recent advances in the management of pulmonary embolism. Kodati Rakesh SR Pulmonary medicine
 Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
Techniques for thrombus removal in acute DVT Benefits of an Endovascular Approach for Rapid Flow Restoration in DVT
 Techniques for thrombus removal in acute DVT Benefits of an Endovascular Approach for Rapid Flow Restoration in DVT Michael K. W. Lichtenberg, MD, FESC Vascular Centre Arnsberg, Germany Disclosure Speaker
Techniques for thrombus removal in acute DVT Benefits of an Endovascular Approach for Rapid Flow Restoration in DVT Michael K. W. Lichtenberg, MD, FESC Vascular Centre Arnsberg, Germany Disclosure Speaker
Reducing Thrombotic Burden in Arterial Interventions. Mario Galli, MD Cardiovascular Interventional Unit S. Anna Hospital, Como, Italy
 Reducing Thrombotic Burden in Arterial Interventions Mario Galli, MD Cardiovascular Interventional Unit S. Anna Hospital, Como, Italy Disclosure Speaker name: Mario Galli... I have the following potential
Reducing Thrombotic Burden in Arterial Interventions Mario Galli, MD Cardiovascular Interventional Unit S. Anna Hospital, Como, Italy Disclosure Speaker name: Mario Galli... I have the following potential
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
Emergency Pulmonary Embolectomy after Failed Thrombolysis in a Community Hospital: A Choice of Institutional Preference?
 ISPUB.COM The Internet Journal of Emergency Medicine Volume 5 Number 1 Emergency Pulmonary Embolectomy after Failed Thrombolysis in a Community Hospital: A Choice of F Vandy, G Fromm, P Guentert, W Halloran,
ISPUB.COM The Internet Journal of Emergency Medicine Volume 5 Number 1 Emergency Pulmonary Embolectomy after Failed Thrombolysis in a Community Hospital: A Choice of F Vandy, G Fromm, P Guentert, W Halloran,
The hallmark of percutaneous thrombus management
 Treating Venous Thromboembolism Without Lytic Medications What the present and the near future will bring in terms of techniques and devices to remove venous thrombus. BY CONSTANTINO S. PEÑA, MD; RIPAL
Treating Venous Thromboembolism Without Lytic Medications What the present and the near future will bring in terms of techniques and devices to remove venous thrombus. BY CONSTANTINO S. PEÑA, MD; RIPAL
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Update on Clinical Integration and Interventional Radiology Imaging
 Update on Clinical Integration and Interventional Radiology Imaging Carl M. Black, MD USR ISMEC Interventional Radiology Section Head, Director Neurointerventional Service Line, SIR, Staff interventional
Update on Clinical Integration and Interventional Radiology Imaging Carl M. Black, MD USR ISMEC Interventional Radiology Section Head, Director Neurointerventional Service Line, SIR, Staff interventional
The hallmark of percutaneous thrombus management
 Treating Venous Thromboembolism Without Lytic Medications What the present and the near future will bring in terms of techniques and devices to remove venous thrombus. BY CONSTANTINO S. PEÑA, MD; RIPAL
Treating Venous Thromboembolism Without Lytic Medications What the present and the near future will bring in terms of techniques and devices to remove venous thrombus. BY CONSTANTINO S. PEÑA, MD; RIPAL
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Τί κάνουμε όταν πάσχει η δεξιά κοιλία Οξεία πνευμονική εμβολή. Βασίλειος Σαχπεκίδης Επιμελητής Α Καρδιολογίας Γ.Ν.Θ. Παπαγεωργίου
 Τί κάνουμε όταν πάσχει η δεξιά κοιλία Οξεία πνευμονική εμβολή Βασίλειος Σαχπεκίδης Επιμελητής Α Καρδιολογίας Γ.Ν.Θ. Παπαγεωργίου No conflicts of interest RV anatomy Ho SY and Nihoyannopoulos P. Heart 2006;92
Τί κάνουμε όταν πάσχει η δεξιά κοιλία Οξεία πνευμονική εμβολή Βασίλειος Σαχπεκίδης Επιμελητής Α Καρδιολογίας Γ.Ν.Θ. Παπαγεωργίου No conflicts of interest RV anatomy Ho SY and Nihoyannopoulos P. Heart 2006;92
Should We Be More Aggressive in the Treatment of Acute DVT?
 DISCLOSURES Consultant Penumbra, Inc. UCSF Vascular Surgery Symposium April 6, 2017 K. Pallav Kolli, MD Assistant Professor of Clinical Radiology University of California, San Francisco 17 yo male, DVT
DISCLOSURES Consultant Penumbra, Inc. UCSF Vascular Surgery Symposium April 6, 2017 K. Pallav Kolli, MD Assistant Professor of Clinical Radiology University of California, San Francisco 17 yo male, DVT
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT
 THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT Tara D. Balint, MD FACS Sentara RMH Thursday, June 14, 2018 1 Objectives of treatment for DVT Prevent death from PE Prevent recurrent VTE Prevent post-thrombotic
THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT Tara D. Balint, MD FACS Sentara RMH Thursday, June 14, 2018 1 Objectives of treatment for DVT Prevent death from PE Prevent recurrent VTE Prevent post-thrombotic
VTE & Medical Patients: Case Scenario
 The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Management of Intermediate-Risk Pulmonary Embolism
 Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
Med Sci Monit, 2016; 22: Grade D. Quality Outstanding
 Ain and Jaff. Treatment of Submassive Pulmonary Embolism: Knowing When to be Aggressive and When to be Conservative. Curr Treat Options Cardio Med (2015) 17:25. Review Article Akin et al. Catheter-Directed
Ain and Jaff. Treatment of Submassive Pulmonary Embolism: Knowing When to be Aggressive and When to be Conservative. Curr Treat Options Cardio Med (2015) 17:25. Review Article Akin et al. Catheter-Directed
The spectrum of clinical outcome of PE
 Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
ACUTE LIMB ISCHEMIA Table of Contents
 ACUTE LIMB ISCHEMIA Table of Contents PERIPHERAL ARTERIAL DISEASE (PAD)... 1 INTERMITTENT CLAUDICATION (IC)... 1 CRITICAL LIMB ISCHEMIA (CLI)... 1 ACUTE LIMB ISCHEMIA (ALI)... 2 Risk Factors...2 Associated
ACUTE LIMB ISCHEMIA Table of Contents PERIPHERAL ARTERIAL DISEASE (PAD)... 1 INTERMITTENT CLAUDICATION (IC)... 1 CRITICAL LIMB ISCHEMIA (CLI)... 1 ACUTE LIMB ISCHEMIA (ALI)... 2 Risk Factors...2 Associated
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Ultrasound-assisted catheter-directed thrombolysis: Does it really work? The BERNUTIFUL trial
 Ultrasound-assisted catheter-directed thrombolysis: Does it really work? The BERNUTIFUL trial Rolf P. Engelberger Division of Angiology CHUV, Lausanne & Inselspital, Bern Switzerland Disclosure Speaker
Ultrasound-assisted catheter-directed thrombolysis: Does it really work? The BERNUTIFUL trial Rolf P. Engelberger Division of Angiology CHUV, Lausanne & Inselspital, Bern Switzerland Disclosure Speaker
Inferior Vena Cava Filters
 Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
The Evidence Base for Treating Acute DVT
 The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
Minimally Invasive Thrombectomy Using the AngioVac System. Brian J. deguzman, MD AmSECT Tampa, FL April 14, 2015
 Minimally Invasive Thrombectomy Using the AngioVac System Brian J. deguzman, MD AmSECT Tampa, FL April 14, 2015 Disclosure Biomet Microfixation Edwards LifeSciences Angiodynamics AtriCure Pavilion Medical
Minimally Invasive Thrombectomy Using the AngioVac System Brian J. deguzman, MD AmSECT Tampa, FL April 14, 2015 Disclosure Biomet Microfixation Edwards LifeSciences Angiodynamics AtriCure Pavilion Medical
Acute and long-term treatment of PE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15