Increased Gradients After Aortic Valve Replacement With The Perceval Valve: The Role of Oversizing
|
|
|
- Janel Rosemary King
- 6 years ago
- Views:
Transcription
1 Accepted Manuscript Increased Gradients After Aortic Valve Replacement With The Perceval Valve: The Role of Oversizing Alfredo Giuseppe Cerillo, MD, Francesca Amoretti, MD, Massimiliano Mariani, MD, Emanuele Cigala, MD, Michele Murzi, MD, Tommaso Gasbarri, MD, Marco Solinas, MD, Dante Chiappino, MD PII: DOI: Reference: ATS S (18) /j.athoracsur To appear in: The Annals of Thoracic Surgery Received Date: 16 August 2017 Revised Date: 8 November 2017 Accepted Date: 18 December 2017 Please cite this article as: Cerillo AG, Amoretti F, Mariani M, Cigala E, Murzi M, Gasbarri T, Solinas M, Chiappino D, Increased Gradients After Aortic Valve Replacement With The Perceval Valve: The Role of Oversizing, The Annals of Thoracic Surgery (2018), doi: /j.athoracsur This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.

2
3 Increased Gradients After Aortic Valve Replacement With The Perceval Valve: The Role of Oversizing Short Title: Increased gradients in sutureless AVR Alfredo Giuseppe Cerillo, MD 1, Francesca Amoretti, MD 2, Massimiliano Mariani, MD 3, Emanuele Cigala, MD 3, Michele Murzi, MD 1, Tommaso Gasbarri, MD 1, Marco Solinas, MD 1, Dante Chiappino, MD 2 Operative Units of Cardiac Surgery 1, Radiology 2, and Cardiology 3, G. Pasquinucci Hospital, G. Monasterio Foundation, Via Aurelia Sud, 54100, Massa, Italy Article Word Count: 4492 Abstract Word Count: 247 Address for correspondence: Dr Alfredo Giuseppe Cerillo, G. Pasquinucci Hospital, Via Aurelia Sud 54100, Massa, Italy. acerillo@yahoo.com
4 ABSTRACT Background. Significant underexpansion or distortion of valved stents may be associated with altered leaflet function, leading to increased transprosthetic gradients and, possibly, early structural degeneration. We investigated the relationship between a computed tomography (CT) measure of the degree of oversizing and the early haemodynamic and clinical outcomes in patients undergoing aortic valve replacement with the Perceval sutureless aortic valve. Methods. The degree of oversizing of the implanted prosthesis was calculated as the ratio between the patients' aortic annulus cross-sectional area (CSA) and the ex-vivo CSA of the implanted prosthesis in 151 perceval patients that had a preoperative cardiac CT. This value was then entered in a multivariate analysis to ascertain its role as a predictor of increased postoperative gradient. Results. The operative mortality was 1.3%. Procedural success, defined as having a normofunctioning valve in the proper anatomical location, was achieved in 150 patients (99.3%). The mean transprosthetic gradient was 13.4±5.0 mmhg, and twenty-three patients (15.2%) showed a gradient 20 mmhg at discharge or at the 1 month follow-up. The degree of oversizing of the implanted prosthesis was the single, most important predictor of increased postoperative gradient (OR:1.264; 95% CI: ; p<0.0001). Interestingly, other relevant factors (patients' BSA, prosthesis size) were not associated with increased gradients. Conclusions. Our study demonstrates that in Perceval patients excessive oversizing should be avoided, and suggests that a different sizing algorithm, possibly based on cardiac CT, should be developed. Further studies are needed to optimize the sizing strategy for the Perceval S valve. Key Words: aortic valve replacement, sutureless aortic valve, cardiac ct
5 The Perceval sutureless aortic bioprosthesis (Livanova, Saluggia, Italy) is a bovine pericardium valve mounted in a Nitinol stent, that can be compressed and positioned in a valve delivery system. The stent is deployed under direct vision in the open heart by turning a release screw. After the deployment, a balloon catheter may be used to expand the stent and post-dilate it at a pressure between 2-4 atm (1,2). Similarly to transcatheter aortic valve implantation (TAVI) devices, the anchoring and good sealing of the Perceval bioprosthesis relies on oversizing the stent frame compared to the native aortic annulus. In recent years, cardiac computed tomography (CT) has become the gold standard technique for measuring the aortic annulus in patients undergoing TAVI, and the CT derived axial image of the aortic Virtual basal ring (VBR) is considered as the reference for sizing by most of the transcatheter valves manufacturers (3). Interestingly, the VBR lies exactly on the plane passing through the nadir of the three aortic cusps, that is where, according to the instructions for use (IFU), a correctly positioned Perceval valve should be deployed (2). Since the Perceval valve stent is a self-expandable nitinol stent with relatively low radial force, the area of the aortic annulus VBR could provide a good estimate of the final cross-sectional area of the stent after deployment, and could therefore be used to calculate the degree of oversizing (or underexpansion) of the valve. Recent evidence in TAVI patients suggests that significant underexpansion or distortion of valved stents may be associated with altered leaflet function, leading to increased transprosthetic gradients and possibly predisposing to other negative outcomes, like valve thrombosis, low platelet counts, thrombo-embolic events and early degeneration (4,5). Moreover, there is evidence that excessive oversizing of the Perceval valve is detrimental (6,7). However, a systematic analysis of the relationship between the degree of oversizing and the haemodynamic performance of the Perceval valve is lacking. The aim of the present study is to investigate the relationship between the CT-derived measure of the degree of oversizing and the early haemodynamic and clinical outcomes in patients undergoing sutureless aortic valve replacement with the Perceval sutureless aortic valve.
6 MATERIAL AND METHODS Patients From March 2011 to December 2015, 617 patients underwent aortic valve replacement with the Perceval at our institution. A base-line, preoperative cardiac CT allowing for correct sizing of the aortic annulus was available for 159 patients. Eight patients were excluded from the analysis due to the presence of a bicuspid aortic valve, or because they underwent concomitant mitral procedures. The remaining 151 patients constitute the population of the present study. The demographic and clinical patients' characteristics are reported in Table 1. All the data presented in the study were prospectively collected and entered in our institutional database which includes ten sections that are filled in consecutively by anesthesiologists, surgeons, perfusionist, intensive care unit and ward doctors. The study was approved by the clinical audit committee of the G. Pasquinucci Heart Hospital to meet ethical and legal requirements, and individual consent was waived. Surgical Procedure In the 137 patients undergoing isolated aortic valve replacement (AVR), the operation was performed through a minimally invasive approach (right anterior minithoracotomy in 101 patients and upper partial sternotomy in 36 patients). The remaining 14 patients underwent associated procedures, and were operated through a full sternotomy. The aortic root was accessed through a high aortotomy, at the level of the aortic fat pad or immediately below it. The aortic valve leaflets were resected and the annulus decalcified accurately. Sizing was performed as per the IFU: the size of the prosthesis to be implanted was indicated by the sizer for whom the transparent obturator passed through the annulus but the white obturator did not (3). Although the procedures were performed by six different surgeons, an experienced senior surgeon with more than 100 Perceval implants supervised the sizing process and valve deployment performed by less experienced operators. CT Protocol and Sizing For the purposes of this study, only patients with a suitable preoperative cardiac CT scan performed at our institution were considered. Cardiac CT was performed with a 320 slices multidetector CT scanner (Toshiba Aquilion ONE, Toshiba Medical Systems S.R.L., Rome, Italy). The scan was done using retrospective ECG
7 gating in spiral technique. Eighty ml of contrast media were injected at 4 ml/sec and bolus tracking was used. The reconstructed slice width was of 1 mm or less, and all the measurements were done in diastole (70% of the cardiac cycle), in order to maximize the image quality, and to avoid variation due to the fact that the systolic images were not available for all patients. The patients CT scan dicom files were downloaded from our institutional images server, anonymized, and independently analyzed. The area and perimeter of the aortic valve virtual basal ring were measured on the 3D multi-planar reconstructions as recommended for TAVI (2, 9). To obtain a measure of the ex vivo cross-sectional area of the Perceval valve, a CT scan of a sample prosthesis for each of the four available measures (S, M, L, XL) was performed. In order to obtain homogeneous measurements and to establish a reference point, the cross-sectional area (CSA) and perimeter of the prosthesis inflow stent were measured at the nadir of the three prosthetic cusps (prosthetic virtual basal ring), on the external surface of the metal stent, with fixed values for the Window Level and the Window Width (Figure 1). All the measurements were blindly repeated three times by four independent investigators, totaling 12 measurements for each size. The average measure was then used for the analysis (table 2). The degree of oversizing of the implanted prosthesis was calculated as the ratio between the patients' native aortic annulus CSA and the ex-vivo CSA of the implanted valve, according to the formula (1-native VBR/prosthesis CSA) x 100. Clinical Management and Haemodynamic Assessment All patients were managed according to our routine institutional protocol. At the end of the surgical procedure, the prosthetic valve function was assessed by an expert cardiologist or cardiac anesthesiologist. Transthoracic echocardiography was always repeated before discharge, and at 1 month postoperatively. Continuous-wave Doppler was used to assess the flow velocity across the prosthetic valve. Peak velocity was averaged from three velocity envelopes, and mean velocity was calculated by averaging the instantaneous velocities measured throughout the velocity complexes. The peak and mean transprosthetic gradients were calculated with the modified Bernoulli equation. Outcome Variables Definitions and Statistical Analysis
8 The clinical and haemodynamic outcomes are defined according to the VARC 2 guidelines (10). Procedure success was defined as having a single, normo-functioning valve in the proper anatomical position. A mean trans-prosthetic gradient of 20 mmhg was defined as increased transprosthetic gradient. Continuous variables are expressed as mean ± standard error, dichotomous variables are expressed as percentages. The association of preoperative, intraoperative and postoperative variables with an increased postoperative gradient was investigated by the Fisher s exact test (dichotomous variables), or by the unpaired Student s t-test (continuous variables). Non-normally distributed continuous variables were analyzed by the Mann Whitney U-test. Factors resulting significantly associated to the end point of the study were then included in a logistic multivariate regression model to ascertain their independent role. Also factors for which the univariate analysis gave a P value 0.1, or of known biologic significance, but failing to meet the critical α level, were included. Odds ratio (OR) and 95% confidence interval (CI) were calculated. Receiver operating characteristic (ROC) curves were calculated to single out the best cutoff value of prosthesis oversizing predicting an increased postoperative gradient. The accuracy of the test was assessed measuring the area under the ROC curve (AUC). The statistical significance of difference of AUC from that of the line of no information was evaluated by Mann Whitney U-statistic. A P value <0.05 was considered significant. Statistical analysis was conducted using SPSS software version 10.1 (SPSS Inc, Chicago, IL). RESULTS Procedural Outcome and Complications The postoperative outcome and complications are reported in table 3. The operative mortality was 1.3%. One patient with multiple comorbidities undergoing combined CABG and AVR developed low cardiac output and multi-organ failure, and died on postoperative day 12. A second patient was discharged to a rehabilitation facility on postoperative day 6 and went home on postoperative day 13. On postoperative day 14 he developed 3 rd degree AV block, and underwent emergency pace-maker implantation at another institution. The post-procedure course was complicated and the patient died on day 45. Procedural success, defined as having a single, normofunctioning valve in the proper anatomical location at the end of the procedure, was achieved in 150 patients (99.3%). One patient that had received an M size prosthesis was reoperated on postoperative day 1 due to the presence of paravalvular leakage with moderate
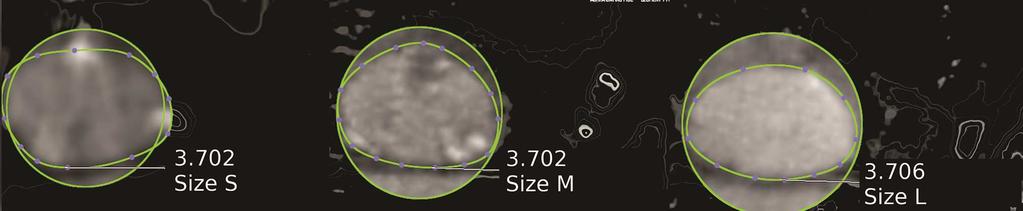
9 to severe aortic regurgitation. The prosthesis was explanted and a bulk annular calcification was removed. An L size prosthesis was then implanted with a good final result. CT Measurements and Prosthesis Oversizing The size of the implanted prosthesis was S in 16 patients (10.5%), M in 46 (30.4%), L in 76 (50.3%) and XL in 13 (8.6%). The mean aortic annulus area at the level of the virtual basal ring was of 3.494±0.002 cm 2, 3.86±0.001 cm 2, 4.66±0.001 cm 2, and 5.57±0.05 cm 2 in S, M, L, and XL patients, respectively. The mean aortic annulus perimeter at the level of the virtual basal ring was of 6.7±0.002 cm, 7.1±0.001, 7.74±0.001 cm, and 8.45±0.04 cm. There was a significant variation in degree of oversizing of the implanted prosthesis, from 6.5% to 49.5% for size S, from 8.9% to 48.9% for size M, from 2.9% to 41.3% for size L, and from 1.1% to 36.5% for size XL. Also, there was a significant overlapping between the four valve sizes (Figure 2, Figure 3). Ecohocardiographic Assessment of Prosthetic Valve Function The mean transprosthetic gradient at discharge was 13.4±5.0 mmhg, and twenty-three patients (15.2%) had a transprosthetic gradient 20 mmhg at discharge or at the 1 month follow-up. Twenty-one of these patient were available for subsequent follow-up. The transprosthetic gradient was reduced in 4, stable in 7 and increased in 10 patients. Factors associated with increased transprosthetic gradient are reported in table 4. At multivariate analysis, the degree of oversizing of the implanted prosthesis was the single, most important predictor of increased postoperative gradient (OR: 1.264; 95% CI: ; p < ). Interestingly, other factors traditionally associated with increased transprosthetic gradients, like the nominal size of the implanted prosthesis or the patients' BSA, showed no impact on the early postoperative gradient at multivariate analysis. According to the ROC curve analysis, the best threshold value of prosthesis oversizing for predicting an increased postoperative gradient was 29.9% (ROC area, ± , P < 0.001). This cutoff value showed a sensitivity of and a specificity of (figure 4): a prosthesis oversizing of more than 30% was associated with a 16-fold increase of the risk of developing an increased postoperative gradient.
10 COMMENT Our study demonstrates that excessive oversizing of the Perceval valve is associated with increased transprosthetic gradients, and should be avoided. Grossly oversized Perceval bioprostheses tend to recoil causing loss of contact between the prosthesis and the annulus, which results in paravalvular leakage and, possibly, in significant aortic regurgitation. Recoiling has been observed in the clinical setting and in the laboratory (6, 7). However, a mean to measure the degree of oversizing in Perceval patients has not been reported to date, and the haemodynamic and clinical effects of different degrees of oversizing when recoil does not occur are not known. In our experience, an oversizing 30% in terms of annular CSA was associated with a 16-fold increase of the risk of developing increased postoperative gradients. In our series, some typical predictors of PPM like the patients' BSA and the size of the implanted prosthesis were not related to the outcome, while a greater degree of oversizing was associated with increased gradients. This apparent paradox is, in our opinion, well explained by the fact that the full expansion of the valved stent inside the patient aortic annulus could be associated with smoother leaflet kinetics, improved valve opening and increased EOA, while the stent compression or deformation that follows the implantation of a prosthesis that is too big with respect to the patient annulus could lead to altered leaflets' kinetics, incomplete valve opening and increased gradients. In fact, the Perceval valve has an in vitro EOA that is much higher than that of conventional sutured bioprostheses (10,11): for the S size, the in vitro EOA ranges from 2.07 to 2.2 cm 2 (10), an in a study of patients with small annuli the measured in vivo EOAI was 1.12 ± 0.2 cm 2 /m 2 versus 0.82 ± 0.1 cm 2 /m 2 for small size conventional, sutured valves (12), indicating that the fluidodynamics of valved stents might be superior to that of conventional surgical valves. The observation that the use of transcatheter aortic valves is associated with higher EOAI and with a reduced incidence of PPM would also support this idea (12). A secondary finding of our study is that intraoperative sizing for the Perceval valve, as recommended by the IFU, does not reflect the true in-vivo measure of the aortic annulus, and could be misleading. Surgical, obturator-based sizing is a complex process that converts several non numerical inputs (visual assessment, tactile feedback, stiffness of the cardiac tissues, the amount and distribution of calcium, the fragility of the aortic wall or the height of the coronary arteries, and others) in a number. Furthermore, both the surgical sizers and the sizing strategy differ significantly between different prostheses, making the sizing process even more complex (13). In our series, there was an impressive degree of overlapping between the four prosthetic sizes
11 (Figure 2, Figure 3). Surgical sizing resulted in a mean oversizing of more than 20%, and probably led to the implantation of a too big prosthesis in a significant proportion of patients. Other Authors have reported difficulties with the Perceval S sizing process. Baert and co-workers recently reported valve recoiling due to excessive oversizing in four patients (2.9% of their Perceval population). They suggested to modify the sizing process and to implant the valve size Given by the sizer of which the white obturator pass the annulus with friction (7). This would certainly reduce the number of grossly oversized prostheses, but not the fact that the choice between different valve sizes in patients with similar annular dimensions would remain arbitrary. In our opinion, cardiac CT could offer a simple solution to this problem. In fact, it has become a very standardized process, and it is used with and extremely high rate of success in thousands of TAVI patients every year. Given the surprising forgivingness of the Perceval valve, the development of a CT-based sizing reference chart would not be complex: the valve showed good haemodynamic performance in a wide range of conditions, and still behaved acceptably in the extreme conditions of virtually no to almost 50% oversizing (Table 5). Our study has some limitations than need to be acknowledged. It is a single institution, retrospective analysis of prospectively collected data in a non-consecutive patients population. Only 25% of patients receiving a Perceval valve at our institution had a preoperative cardiac CT, mainly done for coronary assessment, or in the setting of a screening for TAVI. This could have resulted in selection bias. However, the base-line, procedural and postoperative features of this population did not differ significantly from those observed in our general Perceval patients population (14), and we believe that the present findings and conclusions could be easily replicated in other series. Moreover, the implanting surgeons were usually not aware of the CT-derived annular measurements, and the choice of the prosthesis to be implanted was not affected by the availability of CT data. The ex-vivo CSA of the prosthesis as measured at CT, rather than the true measure made by micrometers, was used as a caliper for all our analysis. CT sizing in the presence of metal objects can be tricky, and our sizing protocol could have been affected by metal artifacts. However, precise sizing was not the aim of our research: we tried to establish a relationship between the degree of under-expansion of the valved stent and its haemodynamic performance, and we are convinced that the exactness of the absolute measures was far less important that the derived, relative estimate of oversizing.
12 Our study focused on the early postoperative period. Increased gradients early after aortic valve replacement can be related to many reversible factors, may disappear with time, and are often of limited clinical significance. In our opinion, however, increased gradients in patients with Perceval valves should not be neglected. In fact, as observed above the presence of an increased gradient could indicate altered leaflets kinetics, and may herald other negative outcomes, like subclinical valve thrombosis and early degeneration, at least in some patients (15). The observation that in our series the increased gradients persisted over time would support this concept. By avoiding the need to stitch the annulus and to tie dozens of knots, sutureless aortic valve prostheses have the potential to make aortic valve replacement faster, easier and safer. However, sutureless prostheses are relatively new, and their in-vivo behavior could be different from the expected. Our study demonstrates that in Perceval patients excessive oversizing should be avoided, and suggests that a different sizing algorithm, possibly based on cardiac CT, should be developed. Further studies are needed to optimize the sizing strategy for the Perceval S valve, in order to take advantage of the full potential of this valve.
13 References 1. Glauber M, Moten SC, Quaini E, Solinas M, Folliguet TA, Meuris B, et al. International Expert Consensus on Sutureless and Rapid Deployment Valves in Aortic Valve Replacement Using Minimally Invasive Approaches. Innovations 2016;11: Pfeiffer S, Sirch J, Vogt F, Fischlein T, Santarpino G. Implantation of the Sorin Perceval sutureless aortic valve: a step by step approach. Minerva Cardioangiol Apr;65(2): Achenbach S, Delgado V, Hausleiter J, Schoenhagen P, Min JK, Leipsic JA. SCCT expert consensus document on computed tomography imaging before transcatheter aortic valve implantation (TA- VI)/transcatheter aortic valve replacement (TAVR). J Cardiovasc Comput Tomogr. 2012;6: Hansson NC, Grove EL, Andersen HR, Leipsic J, Mathiassen ON, Jensen JM, et al. Transcatheter Aortic Valve Thrombosis: Incidence, Predisposing Factors, and Clinical Implications. J Am Coll Cardiol Nov 8;68: Makkar RR, Fontana G, Jilaihawi H, Chakravarty T, Kofoed KF, de Backer O, et al. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N Engl J Med ;373: Di Eusanio M, Saia F, Pellicciari G, et al. In the era of the valve-in-valve: is transcatheter aortic valve implantation in sutureless valves feasible? Annals of Cardiothoracic Surgery 2015;4: Baert J, Astarci P, Noirhomme P, de Kerchove L, The Risk of Oversizing with the Perceval S Suturless Bioprosthesis in Small Aortic Annulus. J Thorac Cardiovasc Surg 2017;153: Piazza N, de Jaegere P, Schultz C, Becker AE, Serruys PW, Anderson RH. Anatomy of the aortic valvar complex and its implications for transcatheter implantation of the aortic valve. Circ Cardiovasc Interv Aug;1: Kappetein AP, Head SJ, Généreux P, Piazza N, van Mieghem NM, Blackstone EH, et al. Valve Academic Research Consortium (VARC)-2. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document (VARC- 2). Eur J Cardiothorac Surg. 2012;42:S45-60.
14 10. Belluschi I, Moriggia S, Giacomini A, Del Forno B, Di Sanzo S, Blasio A, et al. Can Perceval sutureless valve reduce the rate of patient-prosthesis mismatch? Euur J Cardiothorac Surg 2017;51: Tasca G, Vismara R, Mangini A, Romagnoni C, Contino M, Redaelli A, et al. Comparison of the Performance of a Sutureless Bioprosthesis With Two Pericardial Stented Valves on Small Annuli: An In Vitro Study. Ann Thorac Surg. 2017;103: Shalabi A, Spiegelstein D, Sternik L, Feinberg MS, Kogan A, Levin S, et al. Sutureless Versus Stented Valve in Aortic Valve Replacement in Patients With Small Annulus. Ann Thorac Surg. 2016;102: Doenst T, Amorim PA, Al-Alam N, Lehmann S, Mukherjee C, Faerber G. Where is the common sense in aortic valve replacement? A review of hemodynamics and sizing of stented tissue valves. J Thorac Cardiovasc Surg. 2011;142: Concistrè G, Chiaramonti F, Bianchi G, Cerillo A, Murzi M, Margarian R, et al. Aortic valve replacement with Perceval bioprosthesis: single center experience with 617 implants. Ann Thorac Surg 2017, in press. 15. Cerillo AG, Amoretti F, Mariani M, Chiappino D. Sutureless valve thrombosis: the role of stent geometry. Ann Thorac Surg 2017, in press.
15 Table 1. Baseline and operative patients characteristics Age (years) 76±0.4 Sex (f, %) 93 (61.5) BSA (m 2 ) 1.8±0.2 Hypertension, (%) 105 (69.5) Diabetes, (%) 36 (23.8) COPD, (%) 26 (17.2) Chronic renal failure, (%) 4 (2.6) Coronary artery disease, (%) 21 (13.9) Left ventricular dysfunction, (%) 16 (10.5) Peripheral vascular disease, (%) 28 (18.5) EuroSCORE II 4.2±3.9 STS score 3.8±4.1 Aortic VBR area (cm 2 ) 4.37±0.062 Aortic VBR perimeter (cm) 7.48±0.052 Implanted prosthesis Size Surgical approach Size S, (%) 16 (10.5) Size M, (%) 46 (30.4) Size L, (%) 76 (50.3) Size XL, (%) 13 (8.6) Sternotomy, (%) 14 (9.2) Right anterior minithoracotomy, (%) 101 (66.9) Partial sternotomy, (%) 36 (23.8) Associated CABG, (%) 14 (9.2) ACC time (min) 53.7±0.13 CPB time (min) 72.6±0.23 VBR: virtual basal ring; CABG: coronary artery bypass grafting; ACC: aortic cross clamp; CPB: Cardiopulmonary bypass.
16 Table 2. Average CT derived area and perimeter of the Perceval sutureless prosthesis CSA area (cm 2 ), mean±se CSA perimeter (cm), mean±se Size S 4.429± ±0.004 Size M 5.235± ±0.005 Size L 6.21± ±0.003 Size XL 7.05± ±0.006
17 Table 3. Early outcome and complications Operative mortality, (%) 2 (1.3) Procedural Success, (%) 150 (99.3) Stroke, (%) 4 (2.6) Acute renal failure, (%) 1 (0.6) Acute respiratory failure, (%) 6 (3.9) Pace-maker implantation, (%) 7 (4.6) Reoperation for bleeding, (%) 4 (2.6) Time on ventilator (hours), mean±se 8±0.2 ICU stay (days), mean±se 1±0.06 Hospital stay (days), mean±se 5.2±0.2 Echocardiographic data Left ventricular ejection fraction, mean±se 55.4±0.8 Mean pressure gradient, mean±se 13.4±5.0 Transprosthetic gradient > 20 mmhg, (%) 23 (15.2) Residual aortic regurgitation Mild 12 (7.9) Moderate* 2 (1.3) Severe - ICU: intensive care unit. * Moderate residual aortic regurgitation was intraprosthetic in both cases
18 Table 4. Predictors of increased postoperative gradient Univariate Multivariate OR 95% CI p OR 95% CI p Age ns Sex (f) BSA Prosthesis size VBR area (cm 2 ) ns VBR perimeter (cm) ns Oversizing (%) < < Oversizing > 30% <0.0001
19 Table 5. A sizing algorithm for the Perceval S valve. The model is based on the CT-derived virtual basal ring area (mm 2 ), and is designed to obtain an oversizing ranging from 5% to 25%. Min Max S M L XL
20 FIGURE LEGENDS Figure 1. An ex-vivo Perceval S valve sized at CT. (a) To obtain a good visualization of the prosthetic cusps, a Brain preset (Window Level: 50; Window Width: 100) was used. (b) The nadir of the first cusp is identified and marked. (c) The operation is repeated on the nadir of the remaining cusps, and the plane of the prosthetic Virtual basal ring is identified. (d) To reduce the metal artifacts, the measurements of the stent crosssectional area were performed using a Bone preset (Window Level: 300; Window Width: 1500). Figure 2. Scatterplot demonstrating the distribution of the patients' aortic VBR area (top) and perimeter (bottom) according to the prosthesis size implanted. There is a considerable overlapping between the four valve sizes. Figure 3. Double oblique axial CT images of the virtual basal ring from six different patients. Upper line: three patients with virtually identical aortic annular sizes (3.7 cm 2, red boxes) that received three different prosthesis sizes (S, M and L respectively). The ex-vivo area of the implanted prostheses (grey boxes) has been represented with three closed circles for comparison. Middle line: three patients with virtually identical aortic annular sizes (4.1 cm 2, red boxes) that received three different prosthesis sizes (S, M and L respectively). Bottom line: the VBR area of this patient (4.14 cm 2, center) is depicted against the ex-vivo area of the S, M and L Perceval valve (left). The patient received a M valve. The post-implant area of the VBR was 4.18 cm 2, indicating minimal expansion of the aortic annulus after the implantation. The patient underwent valvein-valve implantation with a 23 mm Sapien 3 valve (Edwards Lifesciences, Irvine, Ca) for valve failure three years after the original operation. Figure 4. Receiver operating characteristic curve for the prediction of increased postoperative gradients. The best predictive value of oversizing was 29.9%. AUC=0.885; 95% CI= P<





21
22



23


24
Does Patient-Prosthesis Mismatch Affect Long-term Results after Mitral Valve Replacement?
 Original Article Does Patient-Prosthesis Mismatch Affect Long-term Results after Mitral Valve Replacement? Hiroaki Sakamoto, MD, PhD, and Yasunori Watanabe, MD, PhD Background: Recently, some articles
Original Article Does Patient-Prosthesis Mismatch Affect Long-term Results after Mitral Valve Replacement? Hiroaki Sakamoto, MD, PhD, and Yasunori Watanabe, MD, PhD Background: Recently, some articles
TAVI Versus Suturless Valve In Intermediate Risk Patients
 TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison
 Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
National Institute for Health and Care Excellence IP865/2 Sutureless Aortic Valve Replacement for aortic stenosis
 National Institute for Health and Care Excellence IP865/2 Sutureless Aortic Valve Replacement for aortic stenosis IPAC 14/06/18: 1 1 NHS professional 2 1 NHS professional ments 1.1 1.1 Current evidence
National Institute for Health and Care Excellence IP865/2 Sutureless Aortic Valve Replacement for aortic stenosis IPAC 14/06/18: 1 1 NHS professional 2 1 NHS professional ments 1.1 1.1 Current evidence
Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic,
 Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic, transplantation and Vascular Surgery Hannover Medical School, Germany
Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic, transplantation and Vascular Surgery Hannover Medical School, Germany
AVR with Sutureless Valves State of the Art
 AVR with Sutureless Valves State of the Art T. Fischlein Department of Cardiac Surgery, Cardiovascular Center Klinikum Nürnberg Paracelsus Medical University Nuremberg, Germany Disclosures Consultant and
AVR with Sutureless Valves State of the Art T. Fischlein Department of Cardiac Surgery, Cardiovascular Center Klinikum Nürnberg Paracelsus Medical University Nuremberg, Germany Disclosures Consultant and
REDUCING THE IMPACT OF SURGERY AND FACILITATING FASTER RECOVERY
 REDUCING THE IMPACT OF SURGERY AND FACILITATING FASTER RECOVERY AORTIC SOLUTIONS PERCEVAL VALVE PERCEVAL THE BIOLOGICAL VALVE OF CHOICE IN AVR 0914 RE0210195/A AORTIC SOLUTIONS PERCEVAL THE BIOLOGICAL
REDUCING THE IMPACT OF SURGERY AND FACILITATING FASTER RECOVERY AORTIC SOLUTIONS PERCEVAL VALVE PERCEVAL THE BIOLOGICAL VALVE OF CHOICE IN AVR 0914 RE0210195/A AORTIC SOLUTIONS PERCEVAL THE BIOLOGICAL
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
Successful Transfemoral Edwards Sapien Aortic. Valve Implantation in a Patient with Previous. Mitral Valve Replacement
 Advanced Studies in Medical Sciences, Vol. 2, 2014, no. 1, 37-45 HIKARI Ltd, www.m-hikari.com http://dx.doi.org/10.12988/asms.2014.31213 Successful Transfemoral Edwards Sapien Aortic Valve Implantation
Advanced Studies in Medical Sciences, Vol. 2, 2014, no. 1, 37-45 HIKARI Ltd, www.m-hikari.com http://dx.doi.org/10.12988/asms.2014.31213 Successful Transfemoral Edwards Sapien Aortic Valve Implantation
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Cite this article as:
 doi: 10.21037/acs.2018.09.05 Cite this article as: Cheung A. Early experience of TIARA transcatheter mitral valve replacement system.. doi: 10.21037/acs.2018.09.05 This is a PDF file of an edited manuscript
doi: 10.21037/acs.2018.09.05 Cite this article as: Cheung A. Early experience of TIARA transcatheter mitral valve replacement system.. doi: 10.21037/acs.2018.09.05 This is a PDF file of an edited manuscript
Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation
 ESC Congress 2010 28 Aug 2010-01 Sep 2010 Stockholm - Sweden Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation Gian Paolo Ussia, MD Director of Interventional
ESC Congress 2010 28 Aug 2010-01 Sep 2010 Stockholm - Sweden Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation Gian Paolo Ussia, MD Director of Interventional
Reverse left atrium and left ventricle remodeling after aortic valve interventions
 Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland
 Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
SOLO SMART. The smart way to return to life. Native-like performance now with stented-like implantability
 SOLO SMART TM The smart way to return to life Native-like performance now with stented-like implantability MANY PATIENTS NEED SUPERIOR HEMODYNAMIC PERFORMANCE TO RETURN TO THEIR NORMAL LIFESTYLE. 2 SOLO
SOLO SMART TM The smart way to return to life Native-like performance now with stented-like implantability MANY PATIENTS NEED SUPERIOR HEMODYNAMIC PERFORMANCE TO RETURN TO THEIR NORMAL LIFESTYLE. 2 SOLO
King s Research Portal
 King s Research Portal DOI: 10.1016/j.amjcard.2016.03.028 Document Version Peer reviewed version Link to publication record in King's Research Portal Citation for published version (APA): Eskandari, M.,
King s Research Portal DOI: 10.1016/j.amjcard.2016.03.028 Document Version Peer reviewed version Link to publication record in King's Research Portal Citation for published version (APA): Eskandari, M.,
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
TAVR for low-risk patients in 2017: not so fast.
 TAVR for low-risk patients in 2017: not so fast. Enrico Ferrari, MD, FETCS Cardiac Surgery Department Cardiocentro Ticino Foundation Lugano, Switzerland Conflicts of Interest Consultant and proctor for
TAVR for low-risk patients in 2017: not so fast. Enrico Ferrari, MD, FETCS Cardiac Surgery Department Cardiocentro Ticino Foundation Lugano, Switzerland Conflicts of Interest Consultant and proctor for
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital,
 Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Comments restricted to Sapien and Corevalve 9/12/2016. Disclosures: Core Lab contracts with Edwards Lifesciences, Middlepeak, Medtronic
 Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Transcatheter Mitral Valve Replacement How Close Are We?
 Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Stent valve implantation in conventional redo aortic valve surgery to prevent patient prosthesis mismatch
 Interactive CardioVascular and Thoracic Surgery 24 (2017) 319 323 doi:10.1093/icvts/ivw397 Advance Access publication 31 December 2016 ADULT CARDIAC Cite this article as: Ferrari E, Franciosi G, Clivio
Interactive CardioVascular and Thoracic Surgery 24 (2017) 319 323 doi:10.1093/icvts/ivw397 Advance Access publication 31 December 2016 ADULT CARDIAC Cite this article as: Ferrari E, Franciosi G, Clivio
PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients
 O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
Jonathon Leipsic MD FRCPC FSCCT. Vice Chairman of Radiology University of British Columbia. Disclosures
 Jonathon Leipsic MD FRCPC FSCCT Vice Chairman of Radiology University of British Columbia Disclosures Speaker s bureau: GE Healthcare and Edwards LifeSciences Grant Support- CIHR, GE Healthcare Advisory
Jonathon Leipsic MD FRCPC FSCCT Vice Chairman of Radiology University of British Columbia Disclosures Speaker s bureau: GE Healthcare and Edwards LifeSciences Grant Support- CIHR, GE Healthcare Advisory
Transcatheter valve-in-valve implantation for degenerated surgical bioprostheses
 Review Article Transcatheter valve-in-valve implantation for degenerated surgical bioprostheses Dale J. Murdoch, John G. Webb Centre for Heart Valve Innovation, St. Paul s Hospital, Vancouver, Canada Contributions:
Review Article Transcatheter valve-in-valve implantation for degenerated surgical bioprostheses Dale J. Murdoch, John G. Webb Centre for Heart Valve Innovation, St. Paul s Hospital, Vancouver, Canada Contributions:
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
PPM: How to fit a big valve in a small heart
 PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
TAVR for Valve-In-Valve. Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology
 TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Transcatheter aortic valve implantation for severe aortic valve stenosis with the ACURATE neo2 valve system: 30-day safety and performance outcomes
 All cited trademarks are the property of their respective owners. CAUTION: The law restricts these devices to sale by or on the order of a physician. Indications, contraindications, warnings and instructions
All cited trademarks are the property of their respective owners. CAUTION: The law restricts these devices to sale by or on the order of a physician. Indications, contraindications, warnings and instructions
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves
 Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Aortic valve calcium load before TAVI: Is it important?
 Research Highlight Aortic valve calcium load before TAVI: Is it important? Martin Haensig 1, Ardawan Julian Rastan 2 1 Department of Cardiac Surgery, Heart Center, University of Leipzig, Germany; 2 Department
Research Highlight Aortic valve calcium load before TAVI: Is it important? Martin Haensig 1, Ardawan Julian Rastan 2 1 Department of Cardiac Surgery, Heart Center, University of Leipzig, Germany; 2 Department
Effect of Valve Suture Technique on Incidence of Paraprosthetic Regurgitation and 10-Year Survival
 Effect of Valve Suture Technique on Incidence of Paraprosthetic Regurgitation and 10-Year Survival Sukumaran K. Nair, FRCS (C Th), Gauraang Bhatnagar, MBBS, Oswaldo Valencia, MD, and Venkatachalam Chandrasekaran,
Effect of Valve Suture Technique on Incidence of Paraprosthetic Regurgitation and 10-Year Survival Sukumaran K. Nair, FRCS (C Th), Gauraang Bhatnagar, MBBS, Oswaldo Valencia, MD, and Venkatachalam Chandrasekaran,
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
30-Day Outcomes Following Implantation of a Repositionable Self-Expanding Aortic Bioprosthesis: First Report From the FORWARD Study
 30-Day Outcomes Following Implantation of a Repositionable Self-Expanding Aortic Bioprosthesis: First Report From the Study Stephan Windecker Department of Cardiology Bern University Hospital - INSELSPITAL
30-Day Outcomes Following Implantation of a Repositionable Self-Expanding Aortic Bioprosthesis: First Report From the Study Stephan Windecker Department of Cardiology Bern University Hospital - INSELSPITAL
Tissue vs Mechanical What s the Data??
 Biological (Tissue) Valve in a 60 year old patient: Debate Tissue vs Mechanical What s the Data?? Joseph E. Bavaria, MD Immediate-Past President - Society of Thoracic Surgeons (STS) Brooke Roberts-William
Biological (Tissue) Valve in a 60 year old patient: Debate Tissue vs Mechanical What s the Data?? Joseph E. Bavaria, MD Immediate-Past President - Society of Thoracic Surgeons (STS) Brooke Roberts-William
Thrombocytopenia in Moderate- to High-Risk Sutureless Aortic Valve Replacement
 Korean J Thorac Cardiovasc Surg 2018;51:172-179 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2018.51.3.172 Thrombocytopenia in Moderate- to High-Risk
Korean J Thorac Cardiovasc Surg 2018;51:172-179 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2018.51.3.172 Thrombocytopenia in Moderate- to High-Risk
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.
, FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.") Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration in 2018?
 Joint Meeting 1 Aortic and Mitral Club Chairpersons: S.Adamopoulos, M. Vavuranakis, L. Michalis, P. Nihoyannopoulos PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration
Joint Meeting 1 Aortic and Mitral Club Chairpersons: S.Adamopoulos, M. Vavuranakis, L. Michalis, P. Nihoyannopoulos PVL Assessment. Is paravalvular regurgitation after TAVR still an important consideration
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Aortic valve repair: Techniques and Pitfalls. Allan Stewart, MD Columbia University Medical Center New York, NY
 Aortic valve repair: Techniques and Pitfalls Allan Stewart, MD Columbia University Medical Center New York, NY Take Away Points 1. Valve anatomy is essential to assess repair 2. Unique Decisions with Aneurysm/AI
Aortic valve repair: Techniques and Pitfalls Allan Stewart, MD Columbia University Medical Center New York, NY Take Away Points 1. Valve anatomy is essential to assess repair 2. Unique Decisions with Aneurysm/AI
CROWN PRT. Inservice implantation guide
 Inservice implantation guide DEVICE DESCRIPTION The Crown PRT aortic pericardial heart valve consists of a single piece of bovine pericardium that is preserved with glutaraldehyde and sewn onto a polyester
Inservice implantation guide DEVICE DESCRIPTION The Crown PRT aortic pericardial heart valve consists of a single piece of bovine pericardium that is preserved with glutaraldehyde and sewn onto a polyester
TAVI: Transapical Procedures
 Cardiology Update Davos TAVI: Transapical Procedures Volkmar Falk, MD University Hospital Zürich TA-AVI: antegrade, simple, safe The front door approach! Transapical TAVI Technical advantages of TA approach
Cardiology Update Davos TAVI: Transapical Procedures Volkmar Falk, MD University Hospital Zürich TA-AVI: antegrade, simple, safe The front door approach! Transapical TAVI Technical advantages of TA approach
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D.
 Charles T. Klodell, M.D.") Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Accepted Manuscript. MAC: Mitral Annular Calcification or a Modern Approach to Concept learning in surgery
 Accepted Manuscript MAC: Mitral Annular Calcification or a Modern Approach to Concept learning in surgery Serge Kobsa, MD, PhD, Hiroo Takayama, MD, PhD PII: S0022-5223(18)31805-1 DOI: 10.1016/j.jtcvs.2018.06.058
Accepted Manuscript MAC: Mitral Annular Calcification or a Modern Approach to Concept learning in surgery Serge Kobsa, MD, PhD, Hiroo Takayama, MD, PhD PII: S0022-5223(18)31805-1 DOI: 10.1016/j.jtcvs.2018.06.058
Dr Winnie Sze-Wun Chan. Cardiac Team Deputy Team Head Department of Radiology and Imaging Queen Elizabeth Hospital Hong Kong
 Dr Winnie Sze-Wun Chan Cardiac Team Deputy Team Head Department of Radiology and Imaging Queen Elizabeth Hospital Hong Kong Why? Is CT reliable? How to perform the CT study? How to interpret the CT study?
Dr Winnie Sze-Wun Chan Cardiac Team Deputy Team Head Department of Radiology and Imaging Queen Elizabeth Hospital Hong Kong Why? Is CT reliable? How to perform the CT study? How to interpret the CT study?
Standarized definition of bioprosthetic valve deterioration and failure
 Translational aortic valve research. From biology to treatment Standarized definition of bioprosthetic valve deterioration and failure Anna Sonia Petronio, MD, FESC Head of Cardiac Catheterization Lab
Translational aortic valve research. From biology to treatment Standarized definition of bioprosthetic valve deterioration and failure Anna Sonia Petronio, MD, FESC Head of Cardiac Catheterization Lab
Trend and Outcomes of Direct Transcatheter Aortic Valve Replacement from a Single-Center Experience
 Cardiol Ther (2018) 7:191 196 https://doi.org/10.1007/s40119-018-0115-0 BRIEF REPORT Trend and Outcomes of Direct Transcatheter Aortic Valve Replacement from a Single-Center Experience Anthony A. Bavry.
Cardiol Ther (2018) 7:191 196 https://doi.org/10.1007/s40119-018-0115-0 BRIEF REPORT Trend and Outcomes of Direct Transcatheter Aortic Valve Replacement from a Single-Center Experience Anthony A. Bavry.
Dr Nikolaos Baikoussis
 Dr Nikolaos Baikoussis Cardiac Surgeon Evangelismos General Hospital of Athens, Greece STS database: any procedure not performed with a full sternotomy (FS) and cardiopulmonary bypass (CPB)..(TAVI) Schmitto
Dr Nikolaos Baikoussis Cardiac Surgeon Evangelismos General Hospital of Athens, Greece STS database: any procedure not performed with a full sternotomy (FS) and cardiopulmonary bypass (CPB)..(TAVI) Schmitto
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval?
 Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
TAVI EN INSUFICIENCIA AORTICA
 TAVI EN INSUFICIENCIA AORTICA Cesar Moris Profesor Cardiología Director Departamento del Corazón Hospital Universitario Central de Asturias Universidad de Oviedo OVIEDO -- ESPAÑA CONFLICTO DE INTERESES
TAVI EN INSUFICIENCIA AORTICA Cesar Moris Profesor Cardiología Director Departamento del Corazón Hospital Universitario Central de Asturias Universidad de Oviedo OVIEDO -- ESPAÑA CONFLICTO DE INTERESES
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR)
") Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
Nouvelles indications/ Nouvelles valves
 Nouvelles indications/ Nouvelles valves Sadra Lotus Valve system Boston Scientific A. Tirouvanziam Institut Thorax Nantes SH-31314-AC Sept 2012 Slide 1 of 53 SH-31314-AC Sept 2012 Slide 2 of 53 Building
Nouvelles indications/ Nouvelles valves Sadra Lotus Valve system Boston Scientific A. Tirouvanziam Institut Thorax Nantes SH-31314-AC Sept 2012 Slide 1 of 53 SH-31314-AC Sept 2012 Slide 2 of 53 Building
MEMO 3D RECHORD. Ready to repair. Guiding standards in Mitral valve repair
 MEMO 3D RECHORD TM Ready to repair Guiding standards in Mitral valve repair CARDIAC SURGERY SOLUTIONS A 45-year long history of innovative records in cardiac surgery LivaNova s relentless commitment to
MEMO 3D RECHORD TM Ready to repair Guiding standards in Mitral valve repair CARDIAC SURGERY SOLUTIONS A 45-year long history of innovative records in cardiac surgery LivaNova s relentless commitment to
Evolut R in bicuspid valve anatomies
 Evolut R in bicuspid valve anatomies U. Gerckens MD University of Rostock, Germany Potential conflicts of interest Speaker's name: Ulrich Gerckens I have the following potential conflicts of interest to
Evolut R in bicuspid valve anatomies U. Gerckens MD University of Rostock, Germany Potential conflicts of interest Speaker's name: Ulrich Gerckens I have the following potential conflicts of interest to
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Aortic valve implantation using the femoral and apical access: a single center experience.
 Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Corrado Tamburino, MD, PhD
 Paravalvular leak: acceptable or not Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate School of Cardiology Chief Cardiovascular Department, Director Cardiology Division,
Paravalvular leak: acceptable or not Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate School of Cardiology Chief Cardiovascular Department, Director Cardiology Division,
Indications and Late Results of Aortic Valve Repair
 Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Minimally invasive aortic valve replacement in high risk patient groups
 Review Article Minimally invasive aortic valve replacement in high risk patient groups Daniel Fudulu, Harriet Lewis, Umberto Benedetto, Massimo Caputo, Gianni Angelini, Hunaid A. Vohra Department of Cardiac
Review Article Minimally invasive aortic valve replacement in high risk patient groups Daniel Fudulu, Harriet Lewis, Umberto Benedetto, Massimo Caputo, Gianni Angelini, Hunaid A. Vohra Department of Cardiac
SAPIEN 3 Sizing Considerations:
 SAPIEN 3 Sizing Considerations: Oversizing, Undersizing, or Volume reduction? John Webb MD St Paul s Hospital University of British Columbia Vancouver Disclosure Statement of Financial Interest Within
SAPIEN 3 Sizing Considerations: Oversizing, Undersizing, or Volume reduction? John Webb MD St Paul s Hospital University of British Columbia Vancouver Disclosure Statement of Financial Interest Within
Pre-procedural CT angiography for Transcatheter Aortic Valve Implantation: What a Radiologist Needs to Know?
 Pre-procedural CT angiography for Transcatheter Aortic Valve Implantation: What a Radiologist Needs to Know? E O Dwyer, C O Brien, I Murphy, C Shortt, O Buckley Department of Radiology, AMNCH, Dublin,
Pre-procedural CT angiography for Transcatheter Aortic Valve Implantation: What a Radiologist Needs to Know? E O Dwyer, C O Brien, I Murphy, C Shortt, O Buckley Department of Radiology, AMNCH, Dublin,
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
APOLLO TMVR Trial Update: Case Presentation
 APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical. The Houston Aortic Symposium February 23-25, 2017
 James S. Gammie, MD Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical The Houston Aortic Symposium February 2-25, 2017 Disclosure Statement of Financial Interest Within
James S. Gammie, MD Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical The Houston Aortic Symposium February 2-25, 2017 Disclosure Statement of Financial Interest Within
Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis
 Page 1 of 5 Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis Authors Athina Chasapi, Adam Hobbs, Theodore Velissaris & Benoy N Shah. Wessex Cardiac &
Page 1 of 5 Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis Authors Athina Chasapi, Adam Hobbs, Theodore Velissaris & Benoy N Shah. Wessex Cardiac &
Progress In Transcatheter Aortic Valve Implantation
 Progress In Transcatheter Aortic Valve Implantation Gerald Yong MBBS (Hons) FRACP FSCAI Interventional Cardiologist Royal Perth Hospital Western Australia 4 th APCASH 8 th Sept 2013 Disclosure Statement
Progress In Transcatheter Aortic Valve Implantation Gerald Yong MBBS (Hons) FRACP FSCAI Interventional Cardiologist Royal Perth Hospital Western Australia 4 th APCASH 8 th Sept 2013 Disclosure Statement
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
22/06/2017. Oxford City. Transcatheter aortic valve replacement 2017 guidelines. 1. First time I have heard about it. 2.
 Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Transcatheter heart valve thrombosis
 Transcatheter heart valve thrombosis Jeroen J Bax Dept Cardiology Leiden, The Netherlands New York, 2017 The department of Cardiology of the Leiden University Medical center received research grants from
Transcatheter heart valve thrombosis Jeroen J Bax Dept Cardiology Leiden, The Netherlands New York, 2017 The department of Cardiology of the Leiden University Medical center received research grants from
Presenter Disclosure. Patrick O. Myers, M.D. No Relationships to Disclose
 Presenter Disclosure Patrick O. Myers, M.D. No Relationships to Disclose Aortic Valve Repair by Cusp Extension for Rheumatic Aortic Insufficiency in Children Long term Results and Impact of Extension Material
Presenter Disclosure Patrick O. Myers, M.D. No Relationships to Disclose Aortic Valve Repair by Cusp Extension for Rheumatic Aortic Insufficiency in Children Long term Results and Impact of Extension Material
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Makkar RR, Fontana G, Jilaihawi H, et al. Possible subclinical
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Makkar RR, Fontana G, Jilaihawi H, et al. Possible subclinical
Introducing transcatheter aortic valve implantation with a new generation prosthesis: Institutional learning curve and effects on acute outcomes
 Neth Heart J (2017) 25:106 115 DOI 10.1007/s12471-016-0925-4 ORIGINAL ARTICLE Introducing transcatheter aortic valve implantation with a new generation prosthesis: Institutional learning curve and effects
Neth Heart J (2017) 25:106 115 DOI 10.1007/s12471-016-0925-4 ORIGINAL ARTICLE Introducing transcatheter aortic valve implantation with a new generation prosthesis: Institutional learning curve and effects
CoreValve Evolut R Technology review and Clinical Results. Paul TL Chiam
 CoreValve Evolut R Technology review and Clinical Results Paul TL Chiam MBBS (S pore), MMed, MRCP (UK), FAMS FRCP (Edin), FESC (EU), FACC (USA), FSCAI (USA) Cardiologist Mount Elizabeth Hospital Singapore
CoreValve Evolut R Technology review and Clinical Results Paul TL Chiam MBBS (S pore), MMed, MRCP (UK), FAMS FRCP (Edin), FESC (EU), FACC (USA), FSCAI (USA) Cardiologist Mount Elizabeth Hospital Singapore
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
 Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Keywords: Computed Tomography; Transesophageal Echocardiography; Transcatheter Aortic Valve Replacement
 Cronicon OPEN ACCESS EC CARDIOLOGY Research Article Computed Tomography Versus Transesophageal Echocardiography for Sizing of Transcatheter Aortic Valve Replacement: A Meta-Analysis to Assess Differences
Cronicon OPEN ACCESS EC CARDIOLOGY Research Article Computed Tomography Versus Transesophageal Echocardiography for Sizing of Transcatheter Aortic Valve Replacement: A Meta-Analysis to Assess Differences
My Choice For Percutaneous Mitral Valve Replacement. Jose Luis Navia, MD.
 My Choice For Percutaneous Mitral Valve Replacement Jose Luis Navia, MD. Disclosure Edwards Lifescienses St. Jude Medical MAQUET NaviGate Consultant, Investigator Consultant, Investigator Consultant, Investigator
My Choice For Percutaneous Mitral Valve Replacement Jose Luis Navia, MD. Disclosure Edwards Lifescienses St. Jude Medical MAQUET NaviGate Consultant, Investigator Consultant, Investigator Consultant, Investigator