ARDS AND ECLS DEPARTMENT OF CRITICAL CARE JOSHUA HUELSTER, MD ABBOTT NORTHWESTERN HOSPITAL
|
|
|
- Alyson Dennis
- 6 years ago
- Views:
Transcription
1 ARDS AND ECLS JOSHUA HUELSTER, MD DEPARTMENT OF CRITICAL CARE ABBOTT NORTHWESTERN HOSPITAL


2 DISCLOSURES I have no financial disclosures I have no conflicts of interest I have my own biases (we all do)
3 OBJECTIVES Discuss the management of ARDS patients Discuss the rationale behind this care Briefly review veno-venous extra corporeal membrane oxygenation (VV ECMO)
4 WHAT I M LEAVING OUT Driving pressure: evidence suggests lower is better, but is this a target or a surrogate for severity? We don t know yet Esophageal balloons: surrogate measure of transpulmonary pressure. Promising early data, but waiting for more definitive evidence and not widely used, yet Recruitment maneuvers: no evidence of benefit and recent evidence of harm HFOV: stick a fork in it ECCO 2 R: Not approved in the US studies underway
5 CASE PRESENTATION 52-YEAR-OLD WOMAN CC: Cough and dyspnea PMHx: Dermatomyositis Obesity Anemia Migraines Family Hx: HTN Father Cancer - Mother Social Hx: Married; 4 children Never smoker, no alcohol Allergies: hydrocodone - acetaminophen Medications: Prednisone 40 mg daily Methotrexate 15 mg weekly Folic acid 1 mg daily Trazodone 100 mg qhs Omeprazole 40 mg daily Zolpidem 10 mg daily
6 ADMISSION HPI: Three day history of increasing and progressive dyspnea Non-productive cough and fever to 103F Recent diagnosis of dermatomyositis On prolonged prednisone taper current dose 50 mg daily No pneumocystis prophylaxis Started methotrexate 15 mg weekly Seen in Pulmonary clinic for cough no evidence for ILD Exam: T 103F BP 113/66 HR 110 SpO2 94% (4L NC) Gen: mild distress CV: tachycardic, regular Pulm: diffuse crackles Abd: obese, soft Skin: no rash Neuro: awake and alert

7 ADMISSION CXR Bilateral infiltrates Right greater than left Possible small effusion Infection vs pulmonary edema
8 ACUTE RESPIRATORY DISTRESS SYNDROME (A BRIEF HISTORY) First described by Ashbaugh and colleagues in 1967 (Lancet) 12 patients with tachypnea, refractory hypoxia and bilateral infiltrates after infection or trauma 7 died 6 of 7 had hyaline membranes lining alveoli at autopsy Up to then thought only to occur in neonates First named Adult Respiratory Distress Syndrome
9 AECC DEFINITION 1994 An acute condition with bilateral pulmonary infiltrates and severe hypoxemia: Acute Lung Injury : P/F* ratio less than 300 Acute Respiratory Distress Syndrome : P/F < 200 No evidence of cardiogenic pulmonary edema (PCWP < 18) *P/F: PaO2/FiO2 ratio
10 BERLIN DEFINITION 2012 Hypoxemic respiratory failure with bilateral opacities consistent with pulmonary edema on CXR or CT Onset within 7 days of known clinical insult or new or worsening respiratory symptoms Severity stratification (minimum PEEP or CPAP of 5 cm H2O): Mild: P/F mm Hg Moderate: P/F mm Hg Severe: P/F 100 mm Hg
. Thompson BT et al.")
11 Berlin Definition of the Acute Respiratory Distress Syndrome (ARDS). Thompson BT et al. N Engl J Med 2017;377:
12 THE CASE CONTINUED 52-YEAR-OLD WOMAN Likely community acquired pneumonia with sepsis Ceftriaxone and azithromycin plus sulfamethoxazole/trimethopr im due to steroid use and possible pneumocystis jiroveci pneumonia Continued steroids ABG 7.39/38/96/22.5 (10L O2 via oxymask)
13 DAY OF ADMISSION Seen by Pulmonary day of admission with plan for bronchoscopy Progressed to respiratory failure and intubated with transfer to ICU Vent: PRVC RR18 Vt 500 PEEP 5 FiO2 0.6 Her height = 64 inches PBW = 55 Kg Vt 6 ml/kg = 330 ml
14 ARDSNet NEJM 2000 Landmark trial Compared tidal volume 6 ml/kg PBW to 12 ml/kg PBW and Compared Pplateau 30 vs 50 cm H20 Stopped early due to significantly increased survival in low Vt group
15 Probability of Survival and of Being Discharged Home and Breathing without Assistance during the First 180 Days after Randomization in Patients with Acute Lung Injury and the Acute Respiratory Distress Syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000;342:


16 ARDS net TABLE
17 HYPOXEMIA IS BAD; IS HYPEROXIA? Retrospective study by Aggarwal et al in latest issue of CCM Dataset from 10 ARDSnet trials Patients with PaO2 > 80 and FiO2 > 0.5 above goal Association between higher above goal score and worse mortality Other studies support this idea, but none are definitive Conclusion (ie my bias): resist increasing FiO2 if PaO2 > 60 and SaO2 > 88%
18 ICU DAY 1 Continued worsening hypoxia ABG 7.32/46/67/23 Vent: PRVC* RR 22 Vt 300 PEEP 10 FiO2 1.00

19 Optimal PEEP level is not known, but there is an association to better outcomes if higher PEEP leads to lower tidal volume
20 LUNG SAFE TRIAL 2014 International, multicenter, prospective cohort study 10.4% (3022/29144) of ICU patients met criteria for ARDS Mild 30.0% Moderate 46.6% Severe 23.4% Recognition was only 51.3% for mild and 78.5% for severe Less than 2/3 received Vt 8 ml/kg; 82.6% had PEEP < 12 Only 16.3% of severe ARDS patients were proned Mortality Mild: 34.9% Moderate 40.3% Severe 46.1%
21 ICU DAY 1 Continued worsening hypoxia ABG 7.32/46/67/23 Vent: PRVC RR 22 Vt 300 PEEP 10 FiO Inhaled epoprostenol started without improvement in oxygenation
22 INHALED EPOPROSTENOL AND NITRIC OXIDE
23 HYPOXIC PULMONARY VASOCONSTRICTION Pulmonary arteries constrict in presence of moderate hypoxia Goal is to maintain ventilation-perfusion (V/Q) ratio during localized alveolar hypoxia Disease states, however, often lead to global hypoxia resulting in increased PVR and increased load on the right ventricle
24 RATIONALE FOR USE For use in Type I respiratory failure (Hypoxemic) Inhaled vasodilators selectively dilate ventilated areas of lung (because delivery via inhalation)

25 MECHANISM OF ACTION

26 MECHANISM OF ACTION
27 WHICH ONE TO USE? NEITHER has been shown to improve mortality BOTH improve oxygenation and pulmonary vascular resistance

28 ino IS X MORE $$$$
29 OTHER CONSIDERATIONS Inhaled nitric oxide (ino) may lead to methemoglobinemia ino is rapidly inactivated by oxyhemoglobin to form nitrosylmethemoglobin Occurs in pulmonary capillaries limiting systemic vasodilation Significant MetHgb formation should not occur below 40 ppm inhalation UK recommends testing within 6 hours of start and after every dose change There is an association between ino and acute kidney injury Both inhibit platelet aggregation variable clinical significance via inhaled route ino used in acute RHF and as vasodilator challenge in PAH (inhaled prostacyclin, as well) No clear evidence of additive effect by using both
30 MY BIAS ino only indicated if used as rescue therapy beyond all the other rescue therapies you can think of (meaning: I ve used it once in my albeit brief career for refractory hypoxemia)
31 ICU DAY 1 (IT GETS WORSE) Continued worsening hypoxia ABG 7.32/46/67/23 Vent: PRVC RR 22 Vt 300 PEEP 10 FiO Flolan started without improvement in oxygenation Proned
32 PRONE POSITIONING Has long been known to improve oxygenation PROSEVA trial showed a significant mortality benefit Now recommended by all societies involved in critical care for patients with severe ARDS
33 PROSEVA TRIAL NEJM 2013 Severe ARDS P/F < 150 FiO2 0.6, PEEP 5 Vt about 6 ml/kg IBW Less than 36 hours from onset Criteria confirmed after hours of MV in ICU Patients proned at least 16 hours

34 PROSEVA TRIAL NO INCREASE IN COMPLICATIONS


35 PRONING Pictures courtesy of the interwebs

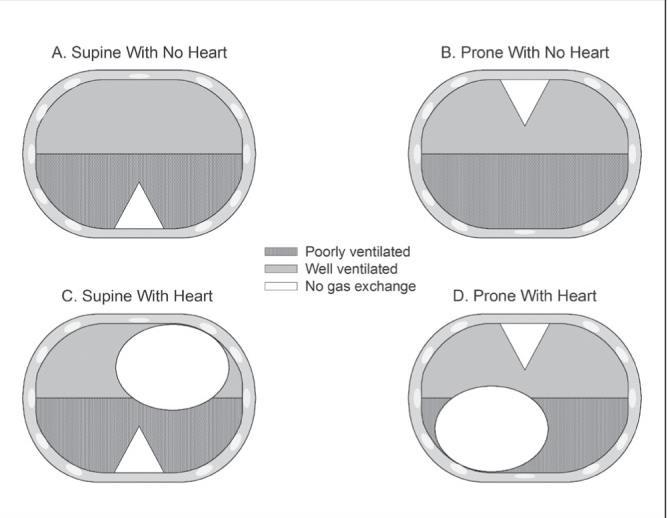
36 HOW IT WORKS SPONGE model of lung Proning changes pleural pressure of dorsal and ventral lung units Dorsal units open Ventral units may collapse Net effect is more ventilated units and better oxygenation
37
38 CONTRAINDICATIONS? High intracranial pressure (> 30 mm Hg) Massive hemoptysis Recent tracheal surgery or sternotomy Recent cardiac pacemaker placement Serious facial trauma Unstable spine, femur or pelvic fractures Others?
39 WHAT S MISSING? PARALYSIS!
40 ACURASYS TRIAL - NEJM 2010 Double blinded randomized control trial Cisatracurium vs placebo in severe ARDS (P/F < 150 with PEEP 5 and Vt 6-8 ml/kg) Given for 48 hours after diagnosis Primary outcome was mortality at 90 days Mortality: 31.6% study group vs 40.7% in placebo group No difference in ICU weakness
41 ICU DAY 1 (RAPID DECLINE) Continued worsening hypoxia ABG 7.32/46/67/23 Vent: PRVC RR 22 Vt 300 PEEP 10 FiO Flolan started without improvement in oxygenation Proned No improvement with increased PEEP and continued proning VV ECMO initiated and patient transferred to ECMO center
42 VV ECMO Veno-venous Extracorporeal Membrane Oxygenation Essentially this is bypass for lung support Blood is removed from the body via a large bore venous cannula Blood pumped through an oxygenator (gas exchange) Oxygenated/decarboxylated blood is returned to the vena cava/right ventricle Allows for lung rest : very low tidal volumes at low pressure

43 THE CIRCUIT NORTH/SOUTH CANNULATION: Drainage via femoral vein Return in SVC Some centers use opposite setup Can do bifemoral, but more problems BICAVAL CANNULATION: Single dual lumen catheter Drainage and return Drainage from SVC and IVC Return aimed at tricuspid valve



44 THE CIRCUIT FLOW SWEEP FIO2
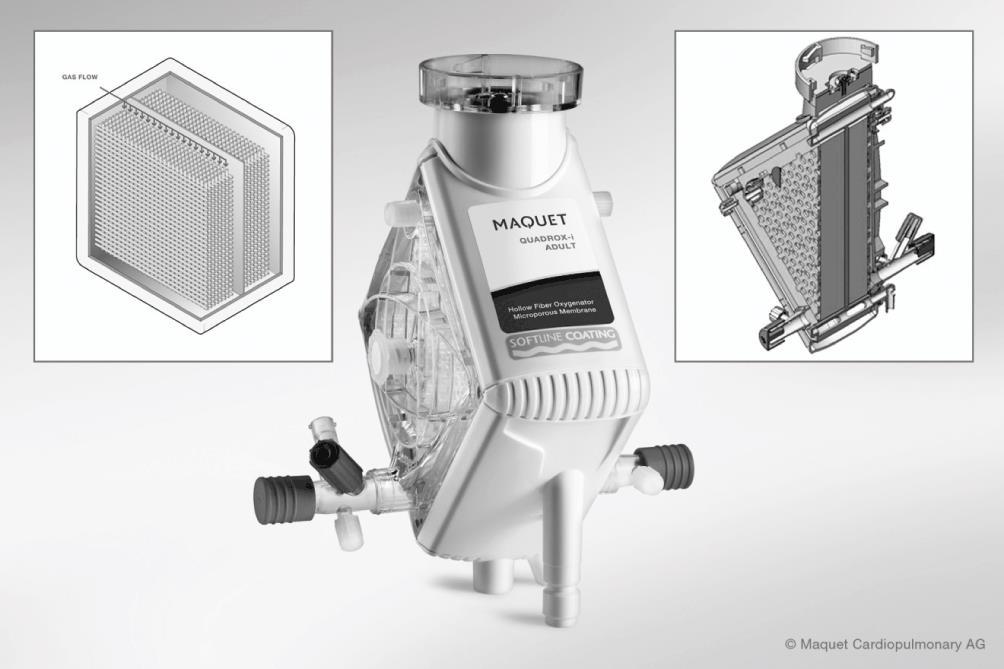
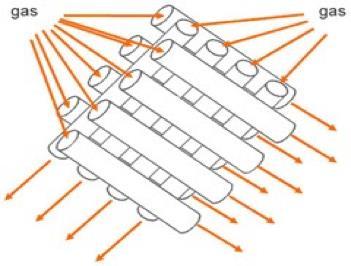
45 THE OXYGENATOR

46 QUICK CO2 PHYSIOLOGY CO2 removal much more efficient than oxygenation CO2 clearance is almost exclusively dependent on sweep gas flow To improve ventilation increase sweep Rarely need the vent to clear CO2
47 QUICK O2 PHYSIOLOGY VV ECMO oxygenation depends on: Amount of flow through the circuit Achieving at least 60% of patient cardiac output Limiting recirculation To raise PaO2 Increase circuit flow Increase circuit FiO2 Decrease recirculation Decrease patient cardiac output and/or oxygen consumption (treat fever, sedation/paralysis, decrease inotropes)
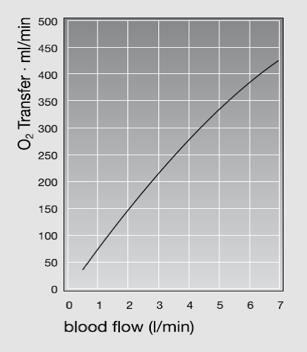
48 QUICK O2 PHYSIOLOGY

49 WHY NOT VENO ARTERIAL ECMO? Differential hypoxia! AKA Harlequin Syndrome Native cardiac output pushes mixing cloud down Poorly oxygenated blood from lungs supplied to: Head Neck Right arm before left Right radial blood gas! learnecmo.com

50 ECMO DAY 1 XRAY THESE LUNGS NEED REST! (THOUGH I CAN T REALLY PROVE IT )
51 CESAR TRIAL LANCET 2009 UK-based multicenter trial Severe ARDS for less than 7 days Randomized to transfer to ECMO center or continued usual care Primary outcome was death or severe disability at 6 months Referral patients did better 63% vs 47%, BUT ONLY 75% of referred patients actually received ECMO Conslusion: referral to an ECMO center is better (but didn t prove ECMO was better )



52 RESOURCE ALLOCATION? HCMC UM ABBOTT UK Population: 66 million. MN pop: 5.57 million MAYO
53 MECHANICAL VENTILATION WHILE ON VV ECMO No data to support any particular mode of ventilation Expert consensus supports: Low driving pressure Low respiratory rate Low FiO2 Example: Ppl < 20-25, PEEP 10-15, RR 10, FiO2 0.3 (CESAR trial) Some patients will have such low Vt the ventilator must be set to Pediatric mode (if able)
54 WEANING FROM VV ECMO WHEN? As with ventilator settings there is no established ideal Generally when you feel patient s lungs have recovered and think you can support patient with low Ppl Vt 6 ml/kg? Ppl < 25? RR < 25 to maintain ventilation? Depends on the underlying condition Really just a gut feeling which is the worst level of evidence
55 WEANING FROM VV ECMO HOW? DO NOT reduce flow of the circuit Increase vent support while decreasing sweep gas Clamp sweep gas When sweep gas is off, patient is off ECMO If tolerates 4-24 hours, then decannulate Timing is another judgment call


56 ECMO DAY 38 Decannulated Day 43 LTACH for 2.5 months Walked back into the ICU to visit several months later

57 CXR 3 MONTHS POST ECMO
58 CONCLUSION: ARDS Still has high mortality/morbidity Remains underdiagnosed and undertreated Use enough PEEP (but not too much) Use enough oxygen (but not too much) Paralyze patients with P/F 150 Prone patients with moderate to severe ARDS Avoid ino, but maybe try epoprostenol Strongly consider transferring severe ARDS patients to an ECMO center
59 CONCLUSION: VV ECMO Facilitates lung rest (ultra-low tidal volumes) Though increasingly popular there is a lack of RCT s to support widespread use (bias warning: I m a believer) Best evidence in severe patients (P/F < 100) EOLIA trial is in the pipeline will this give the answer?
60 QUESTIONS?
61 REFERENCES 1. Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet 1967;2: Thompson BT, Chambers RC and Liu KD. Acute Respiratory Distress Syndrome. NEJM 2017;377: Ferguson ND, Fan E, Camporota L, et al. The Berlin definition of ARDS: an expanded rationale, justification, and supplementary material. Intensive Care Med 2012;38: The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. NEJM 2000; 342: ARDSnet.org accessed 3/ Aggarwal NR, Brower RG, Hager DN, et al; for the National Institutes of Health Acute Respiratory Distress Syndrome Network Investigators: Oxygen Exposure Resulting in Arterial Oxygen Tensions Above the Protocol Goal Was Associated With Worse Clinical Outcomes in Acute Respiratory Distress Syndrome. Crit Care Med 2018; 46: Bellani G, Laffey J, Pham T; et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016;315(8): Briel M et al Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA (9): Aaronson P., Robertson TP, Knock GA, Becker S, Lewis TH, Snetkov V, Ward J. Hypoxic pulmonary vasoconstriction: mechanisms and controversies. J Physiol Jan1; 570(Pt 1): Griffiths M, Evans TW. Inhaled Nitric Oxide Therapy in Adults. NEJM : Torbic H, Szumita PM, Anger KE, Nuccio P, LaGambina S, Weinhouse G. Inhaled epoprostenol vs inhaled nitric oxide for refractory hypoxemia in critically ill patients. J Crit Care 2013;28(5): Yen-Chun Lai et al. Classic vasodilator and vasoconstrictor systems and their translational therapies for pulmonary arterial hypertension (PAH). Circ Res. 2014;115: Papazian L et al. Neuromuscular blockers in early acute respiratory distress syndrome. NEJM 2010; 363: Maquet AG. Maquet.com accessed 3/30/ Schmidt M et al. Blood oxygenation and decarboxylation determinants during venovenous ECMO for respiratory failure in adults. Intensive Care Med. 2013;39(5): Peek G, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 2009;374:
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Adult Extracorporeal Life Support (ECLS)
") Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
ECMO and refractory Hypoxemia
 ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS
 ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Extracorporeal support in acute respiratory failure. Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London
 Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
BASIC CRITICAL CARE OF THE PATIENT. Hannelisa Callisen PA C February 2017
 BASIC CRITICAL CARE OF THE PATIENT Hannelisa Callisen PA C February 2017 Disclosures Industry: None ECMO is off label Objectives ECMO initiation selection, cannulation Physiology : Review of DO2 on ECMO
BASIC CRITICAL CARE OF THE PATIENT Hannelisa Callisen PA C February 2017 Disclosures Industry: None ECMO is off label Objectives ECMO initiation selection, cannulation Physiology : Review of DO2 on ECMO
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014
 USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
ECMO/ECCO 2 R in Acute Respiratory Failure
 ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support
 The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Ventilation update Anaesthesia departmental PGME. Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care
 Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
ECLS as Bridge to Transplant
 ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure
 Guidelines for Pediatric Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
(almost) 4/22/2016 Updated. AllinaHealthSystem. Things To Know About
 4/22/2016 Updated. AllinaHealthSystem. Things To Know About") (almost) Susan C Seatter MD Abbott Northwestern Hospital Intensivists Advanced Circulatory Support for the Critically Ill Adult April 22, 2016 1 Consider ECMO Early 2 Don t Use The Lungs 3a Know Your Circuit
(almost) Susan C Seatter MD Abbott Northwestern Hospital Intensivists Advanced Circulatory Support for the Critically Ill Adult April 22, 2016 1 Consider ECMO Early 2 Don t Use The Lungs 3a Know Your Circuit
SCVMC RESPIRATORY CARE PROCEDURE
 Page 1 of 7 New: 12/08 R: 4/11 R NC: 7/11, 7/12 B7180-63 Definitions: Inhaled nitric oxide (i) is a medical gas with selective pulmonary vasodilator properties. Vaso-reactivity is the evidence of acute
Page 1 of 7 New: 12/08 R: 4/11 R NC: 7/11, 7/12 B7180-63 Definitions: Inhaled nitric oxide (i) is a medical gas with selective pulmonary vasodilator properties. Vaso-reactivity is the evidence of acute
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Section: Therapy Effective Date: October 15, 2016 Subsection: Original Policy Date: June 19, 2015 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 30 Summary Extracorporeal membrane oxygenation (ECMO) provides extracorporeal circulation and physiologic gas exchange for temporary cardiorespiratory
Last Review Status/Date: September 2016 Page: 1 of 30 Summary Extracorporeal membrane oxygenation (ECMO) provides extracorporeal circulation and physiologic gas exchange for temporary cardiorespiratory
PATIENT SELECTION FOR ACUTE APPLICATION OF ECMO, ECCOR, ETC.
 PATIENT SELECTION FOR ACUTE APPLICATION OF ECMO, ECCOR, ETC. J. CHRISTOPHER FARMER, MD PROFESSOR OF MEDICINE CHAIR OF CRITICAL CARE MEDICINE MAYO CLINIC PHOENIX, AZ Dr. Chris Farmer is a critical care
PATIENT SELECTION FOR ACUTE APPLICATION OF ECMO, ECCOR, ETC. J. CHRISTOPHER FARMER, MD PROFESSOR OF MEDICINE CHAIR OF CRITICAL CARE MEDICINE MAYO CLINIC PHOENIX, AZ Dr. Chris Farmer is a critical care
Management of Respiratory Failure: The Surgical Perspective. When Traditional Respiratory Support Techniques fail. ARDS: Evidence Based Practice
 Critical Care Medicine and Trauma Management of Respiratory Failure: The Surgical Perspective Jasleen Kukreja, M.D. Division of Cardiothoracic Surgery University of California San Francisco When Traditional
Critical Care Medicine and Trauma Management of Respiratory Failure: The Surgical Perspective Jasleen Kukreja, M.D. Division of Cardiothoracic Surgery University of California San Francisco When Traditional
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015
: Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015") Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE)
") Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
Extracorporeal Membrane Oxygenation (ECMO)
") Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 01/01/2017 Section: Other/Miscellaneous
Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 01/01/2017 Section: Other/Miscellaneous
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
RESCUE VENTILATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Extracorporeal Membrane Oxygenation (ECMO)
") Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/01/2014 Section: Other/Miscellaneous
Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/01/2014 Section: Other/Miscellaneous
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Inhaled epoprostenol vs inhaled nitric oxide for refractory hypoxemia in critically ill patients
 Journal of Critical Care (2013) 28, 844 848 Inhaled epoprostenol vs inhaled nitric oxide for refractory hypoxemia in critically ill patients Heather Torbic PharmD, BCPS a,, Paul M. Szumita PharmD, BCPS
Journal of Critical Care (2013) 28, 844 848 Inhaled epoprostenol vs inhaled nitric oxide for refractory hypoxemia in critically ill patients Heather Torbic PharmD, BCPS a,, Paul M. Szumita PharmD, BCPS
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Artificial Lung: A New Inspiration
 Artificial Lung: A New Inspiration Joseph B. Zwischenberger MD Johnston-Wright Professor and Chairman: Department of Surgery j.zwische@uky.edu The University of Kentucky Lexington, Kentucky Presenter Disclosure
Artificial Lung: A New Inspiration Joseph B. Zwischenberger MD Johnston-Wright Professor and Chairman: Department of Surgery j.zwische@uky.edu The University of Kentucky Lexington, Kentucky Presenter Disclosure
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA?
 WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
The GOLD Study. Goal of Open Lung Ventilation in Donors. Michael A. Matthay M.D. and Lorraine B. Ware, MD. Disclosures
 The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
Hypoxemia in the ED. Joseph Shiber, MD, FACP, FACEP, FCCM Director Advanced Lung/ECMO Service Professor of Emergency Medicine, Neurology, and Surgery
 Hypoxemia in the ED Joseph Shiber, MD, FACP, FACEP, FCCM Director Advanced Lung/ECMO Service Professor of Emergency Medicine, Neurology, and Surgery 19 y/o woman SOB s/p bicyclist struck Helmeted, no LOC
Hypoxemia in the ED Joseph Shiber, MD, FACP, FACEP, FCCM Director Advanced Lung/ECMO Service Professor of Emergency Medicine, Neurology, and Surgery 19 y/o woman SOB s/p bicyclist struck Helmeted, no LOC
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Healing Breath. Disclosures. anuola. Extracorporeal Membrane Oxygenation Principles: Rest your lungs. Objectives ECMO: 8/28/17
 anuola Healing Breath ECMO Program of Hawaii Extracorporeal Membrane Oxygenation Principles: Rest your lungs Len Y. Tanaka, MD September 12, 2017 Disclosures No financial disclosures. However this presentation
anuola Healing Breath ECMO Program of Hawaii Extracorporeal Membrane Oxygenation Principles: Rest your lungs Len Y. Tanaka, MD September 12, 2017 Disclosures No financial disclosures. However this presentation
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
10/16/2017. Review the indications for ECMO in patients with. Respiratory failure Cardiac failure Cardiorespiratory failure
 Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Inhaled nitric oxide: clinical evidence for use in adults
 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided