Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN
|
|
|
- Samson Rogers
- 6 years ago
- Views:
Transcription
1 Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 1 1 st CCU in the world opened in March 1962 was in Toronto, Canada In May of 1962 the 1 st CCU in the US opened at Bethany Hospital in Kansas City, Kansas by Dr. Hugh Day Early cardiac monitoring focused on observing heart rates and monitoring for life threatening arrhythmias Monitoring equipment has changed greatly over the past 50+ years 2 Key Choice / CNEA 1
2 Dr. Desmond Julian opened 1 st CCU in Sydney Australia in Nov 1962 noted: All wards admitting patients with acute myocardial infarction should have a system capable of sounding an alarm at the onset of an important rhythm change and recording the rhythm automatically on an ECG.the provision of the appropriate apparatus would not be prohibitively expensive if these patients were admitted to special intensive care units. Such units should be staffed by suitably experienced people throughout the 24 hours. 3 4 Key Choice / CNEA 2
3 Despite advances in technology, the need for human over site in the interpretation of the ECG is as important as it was 50 years ago for the following reasons: With the high sensitivity capabilities of the current monitors numerous alarms must be evaluated to prevent over treatment More aggressive approaches to treatment of myocardial ischemia improves outcomes requiring ongoing surveillance Complex device technology requires expert analysis of ECG monitoring data Many more drugs have been that prolong QT intervals failure to identify patients at risk increases the incidence of sudden cardiac death Only humans not monitors can determine the goals of monitoring for individual patients 5 Nurses role in bedside monitoring Educating nurses to utilize clinical judgment and critical thinking skills to make determinations regarding the best lead selection for each individual patient. Decisions should be based on the patient and his/her condition. 6 Key Choice / CNEA 3

4 Understanding Your Monitor s Capabilities Understanding Arrhythmias Skin prep Lead placement Setting Gain Setting alarms Responding to alarms Reporting arrhythmias Treating arrhythmias Documenting arrhythmias Lead identification Onset and offset of arrhythmias Physician notification 7 8 Key Choice / CNEA 4


5 The ECG is a graphic recording of electrical activity spreading through the heart 12 lead ECG provides 12 different views of electrical activity Each bedside monitoring lead provides one view 9 SA Node AV Node Bundle of His AV Junction Right and Left Bundle Branches Anterior and Posterior Fascicles Purkinge Fibers 10 Key Choice / CNEA 5
6 WAVES and COMPLEXES QRS P P wave: atrial depolarization QRS: ventricular depolarization T wave: ventricular repolarization PR interval: AV conduction time QRS width: intraventricular conduction time ST Segment: entire ventricular depolarization QT interval: used to reflect ventricular repolarization time QT Interval T PR Interval QRS ST Segment 11 Lead 1 + Left Arm High Lateral Wall LAD (Diagonal) Axis Quadrant avr + Right Arm P Wave always V1 + 4 th ICS, RSB Septal Wall & RV LAD (Septal) Ectopy VS Aberrancy RBBB LBBB LVT RVT Reciprocal to Posterior V4 + L MCL, 5 th ICS Anterior Wall LAD Lead 2 + Left Leg Inferior Wall RCA L Ant Hemi rs P Wave always + avl + Left Arm High Lateral Wall LAD (Diagonal) Reciprocal to Lead 3 V2 + 4 th ICS, LSB Septal Wall LAD (Septal) Reciprocal to Posterior V5 + L anterior axillary, same level as V 4 Low Lateral Wall Circumflex (Marginal) Lead 3 + Left Leg Inferior Wall RCA L Ant Hemi rs Reciprocal to avl ST Segment Lead RCA avf + Left Leg Inferior Wall RCA L Ant Hemi rs Axis Quadrant V3 + Midway Between V 2 & V 4 Anterior Wall LAD Reciprocal to Posterior ST Segment Lead LAD V6 + L midaxillary line, same level as V 4 Low Lateral Wall Circumflex (Marginal) Ectopy VS Aberrancy RBBB LBBB ST Segment Lead Circ 12 Key Choice / CNEA 6

7 Dual Electrode Leads Single Electrode Leads 13 Dual Electrode Leads One positive electrode One negative electrode Records difference in electrical potential between selected electrodes Leads I, II, and III Single Electrode Leads One positive electrode One negative reference point Zero electrical potential Center of heart Leads avr, avl, avf V1-V6 14 Key Choice / CNEA 7


8 15 Consider the positive pole of each lead as the camera (exploring electrode) RA RV LA - + LV + 16 Key Choice / CNEA 8
9 17 Note: Nothing travels toward the right leg as a positive electrode. The right leg is the ground used to absorb any excess electrical activity. Key Choice / CNEA 9
")


10 19 Standard Limb Leads (Dual Electrode Leads) Leads I, II, III RA Left Arm + RA Left leg + _ Lead I + RA LA LA Left leg + + LL + 20 Key Choice / CNEA 10
 avr, avl, avf + RA LA + - Right Arm + LL + Left Arm + Left Leg + 22 Key Choice /")
11 Augmented Limb Leads Leads avr, avl, avf 21 Augmented Limb Leads (Single Electrode Leads) avr, avl, avf + RA LA + - Right Arm + LL + Left Arm + Left Leg + 22 Key Choice / CNEA 11


12 23 24 Key Choice / CNEA 12

13 RA LV V6 RV + 4 th ICS, RSB + L MCL, 5 th ICS V5 + 4 th ICS, LSB + L anterior axillary, same level as V 4 V1 V2 V3 V4 + Midway Between V 2 & V 4 + L midaxillary line, same level as V 4 25 RA Left Arm + Right Arm th ICS, RSB + L MCL, 5 th ICS RA Left leg + Left Arm th ICS, LSB + L anterior axillary, same level as V 4 LA Left leg + Left Leg + + Midway Between V 2 & V 4 + L midaxillary line, same level as V 4 26 Key Choice / CNEA 13


14 Posterior wall of the left ventricle and the right ventricle are not captured on the standard 12 lead ECG Septum depolarizes from left to right 2. Both ventricles depolarize from endocardium to epicardium 3. Basal portions of ventricles depolarize last 4. Mean direction of depolarization is downward, leftward, and posterior 28 Key Choice / CNEA 14

15 If positive electrode sees depolarization approaching it, it records an upright complex If positive electrode sees depolarization heading away from it, it records a negative complex. 29 Lead 1 avr V1 V4 + Left Arm High Lateral Wall + Right Arm + 4 th ICS, RSB Septal Wall + L MCL, 5 th ICS Anterior Wall Lead 2 avl V2 V5 + Left Leg Inferior Wall + Left Arm High Lateral Wall + 4 th ICS, LSB Septal Wall + L anterior axillary, same level as V 4 Low Lateral Wall Lead 3 avf V3 V6 + Left Leg Inferior Wall + Left Leg Inferior Wall + Midway Between V 2 & V 4 Anterior Wall + L midaxillary line, same level as V 4 Low Lateral Wall 30 Key Choice / CNEA 15
16 Bedside Monitoring 12 Lead ECG Remember View of Positive Electrode (Camera) Importance of Lead Placement Identify Correct Lead on Rhythm Strip 31 Many Options: 3 lead 5 lead 6 lead Derived ECG Hard Wired Telemetry 32 Key Choice / CNEA 16

17 Circulation. 2004;110: doi: /01.CIR Class I Recommendations Cardiac monitoring indicated in most, if not all, patients in this group. Class II Recommendations Cardiac monitoring may be of benefit in some patients but is not considered essential for all patients. Class III Recommendations Cardiac monitoring is not indicated because a patient s risk of a serious event is so low that monitoring has no therapeutic benefit. 34 Key Choice / CNEA 17
18 Arrhythmia Detection Ischemia Monitoring QT Interval Monitoring Key Choice / CNEA 18
19 Candidates Primary purpose for all patients on cardiac monitor Purpose Detection of and prompt intervention for life threatening arrhythmias Best Leads V1 (or MCL1 if 3 lead cable) V6 (or MCL6) 37 Patients resuscitated from cardiac arrest Patients in early phase of Acute Coronary Syndromes (including Rule Outs ) Patients with unstable coronary syndromes and newly diagnosed high-risk coronary lesions Adults and children who have undergone cardiac surgery Patients after nonurgent percutaneous coronary interventions with complications Patients after ICD implant or pacer lead placement if pacer dependent Patients with temporary pacemaker or transcutaneous pacing pads Patients with AV block 38 Key Choice / CNEA 19

20 Patients with Arrhythmias complicating Wolff- Parkinson-White Syndrome with rapid anterograde conduction over an accessory pathway Patients with Long-QT Syndrome and associated ventricular arrhythmias Patients with intraaortic balloon pump Patients with acute heart failure/ pulmonary edema Patients with indications for intensive care Patient under going diagnostic / therapeutic procedures requiring conscious sedation or anesthesia Patients with any other hemodynamically unstable arrhythmias Diagnosis of arrhythmias in pediatric patients 39 Ectopy versus Aberrancy 40 Key Choice / CNEA 20
21 Lead 1 avr V1 V4 + Left Arm High Lateral Wall + Right Arm + 4 th ICS, RSB Septal Wall VT vs Aberrancy + L MCL, 5 th ICS Anterior Wall Lead 2 avl V2 V5 + Left Leg Inferior Wall + Left Arm High Lateral Wall + 4 th ICS, LSB Septal Wall + L anterior axillary, same level as V 4 Low Lateral Wall Lead 3 avf V3 V6 + Left Leg Inferior Wall + Left Leg Inferior Wall + Midway Between V 2 & V 4 Anterior Wall + L midaxillary line, same level as V 4 Low Lateral Wall VT vs Aberrancy 41 What does P wave represent? Can we see sinus node? What does normal PR interval represent (prolonged?)? What does skinny QRS represent? Wide QRS? What pacemaker options exist? What should be the end result of each sinus impulse? Key Choice / CNEA 21
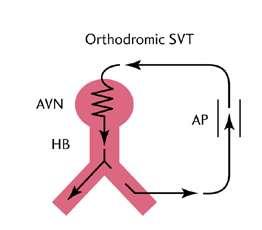
22 Why in JR can P wave appear 3 ways on ECG P wave preceding QRS with short PR interval No P wave visible at all P wave following QRS with short R-P interval 43 Disorder of impulse initiation Abnormal or enhanced automaticity Triggered mechanism: disturbance in recovery or repolarization (less common) Early or delayed after depolarizations Disorder of impulse conduction Reentrant Circuit (Most common) 44 Key Choice / CNEA 22


23 Key Choice / CNEA 23



24 > 90% of monomorphic VT is associated with scar! Ectopic focus in paroxysmal atrial fib (near pulmonary veins) Ectopic focus in VT from ischemia or electrolyte abnormalities Key Choice / CNEA 24


25 Key Choice / CNEA 25 49
26 Wide complex tachycardia presumed to be VT if diagnosis is unclear DC cardioversion with sedation if hemodynamically unstable Don t assume VT cannot be well tolerated! The rate, size of the heart and presence of additional complications are often more important than the source of the tachycardia Check the patient (need to defib?) Check the blood pressure (need to cardiovert?) Check the ECG (determine the rhythm) 51 Patient history / assessment QRS Width AV Dissociation Concordance Axis Morphology Note: VT is much more common than supraventricular tachycardia with bundle branch aberration. In wide QRS tachycardias VT is the right answer up to 80% of the time. A wide complex tachycardia is always considered ventricular in origin if the diagnosis is uncertain 52 Key Choice / CNEA 26
 The wider the QRS VT is favored However: SVT with LBBB will have a wider QRS than SVT with RBBB QRS will be wider in pre-existing BBB Other causes of SVT with wider than expected QRS: antidromic")
 is diagnostic for ventricular ectopy Ventricular tachycardia may also have retrograde P waves (retrograde P waves do not")
27 Acute ischemia / injury (Abnormal automaticity) Post myocardial infarction / ischemic cardiomyopathy (Reentrant circuit within myocardium) Non ischemic dilated cardiomyopathy (Bundle branch reentrant VT) The wider the QRS VT is favored However: SVT with LBBB will have a wider QRS than SVT with RBBB QRS will be wider in pre-existing BBB Other causes of SVT with wider than expected QRS: antidromic tachycardia and patients on Class IC or IA antiarrhythmics or amiodarone Not all VT is significantly wide VT originating from septum more narrow than VT from free wall If QRS more narrow than sinus rhythm = VT 53 Independent atrial and ventricular activity (AV dissociation) is diagnostic for ventricular ectopy Ventricular tachycardia may also have retrograde P waves (retrograde P waves do not confirm VT) 54 Key Choice / CNEA 27


28 55 56 Key Choice / CNEA 28

29 Axis Right Superior (Extreme / Northwest) axis deviation is strong indicator of ventricular ectopy Ventricular tachycardia rarely occurs with normal axis Ventricular tachycardia can occur with right or left axis deviation 57 Use Lead I and avf Left hand represents QRS in Lead I Right hand represents QRS in avf Fingertips will point in the same direction as the QRS complex If hands are different, always place the left hand over the right. Handy Method of Axis Calculation developed by J. Cooper, PhD., American College of CV Nursing 58 Key Choice / CNEA 29

30 I avf I avf I I avf avf 59 Lead 1 avr V1 V4 + Left Arm High Lateral Wall + Right Arm + 4 th ICS, RSB Septal Wall VT vs Aberrancy + L MCL, 5 th ICS Anterior Wall AXIS Lead 2 avl V2 V5 + Left Leg Inferior Wall + Left Arm High Lateral Wall + 4 th ICS, LSB Septal Wall + L anterior axillary, same level as V 4 Low Lateral Wall Lead 3 avf V3 V6 + Left Leg Inferior Wall + Left Leg Inferior Wall AXIS + Midway Between V 2 & V 4 Anterior Wall + L midaxillary line, same level as V 4 Low Lateral Wall VT vs Aberrancy 60 Key Choice / CNEA 30

31 Wide Complex Tachycardia: Ventricular Ectopy or SVT with BBB Aberration Morphology Challenges: BBB Reentrant VT Idiopathic RVOT Antidromic tachycardia 61 LBBB RBBB LVT RVT V1 and V6 are gold standard monitoring leads for ectopy versus aberrancy Bundle branch block patterns and ventricle ectopy can be differentiated by using the morphology of these leads. DON T rely on Lead II!! 62 Key Choice / CNEA 31

32 63 Standard 6 Lead Placement 64 Key Choice / CNEA 32



33 MCL6 Standard 5 Lead Placement V1 & V6 Modified 5 lead Placement V1 & MCL6 Monitor Settings: V and III Key Choice / CNEA 33
34 Not every QRS complex contains a Q wave, R wave and S wave!! Q always negative (below baseline) R first positive above the baseline R second positive above the baseline S always negative deflection following the R wave or second component to entirely negative [[; /complex 67 Let s Practice QS qr QR Qr qrs R RS rs Rs rsr 69 Key Choice / CNEA 34

35 Ectopy versus Aberrancy 70 SVT WITH ABERRANCY SVT with RBBB Aberration SVT with LBBB Aberration VENTRICULAR TACHYCARDIA VT with LBBB Pattern Right VT VT with RBBB Pattern Left VT 71 Key Choice / CNEA 35
36 2 V 6 1 QRS sec V 1 72 V 6 = qrs V6 V 1 = rsr V1 QRS =.12 sec or more 73 Key Choice / CNEA 36


37 rsr qr 74 V 6 = wide R V 1 = QS V6 V1 QRS =.12 sec or more V1 = rs 75 Key Choice / CNEA 37
38 Nadir is the distance from the onset of the QRS complex to the lowest point of the S Wave Measure from the beginning of the QRS complex to the bottom valley or peak of the QRS The nadir in V1 should be < 0.06 sec for LBBB (slick down stroke) 76 RBBB LBBB Left ventricle first Right ventricle first VT from Left Ventricle VT from Right Ventricle Left ventricle first Right ventricle first 77 Key Choice / CNEA 38
39 Right Bundle Branch shaped R wave with an early left peak (Rr ) R wave with a single peak q wave followed by R wave 78 LBBB shaped Primarily negative wide rs complex delay to the nadir > 0.06 sec r wave broader than 0.03 sec Slurring on the down stroke Note: LBBB shaped VT can come from RV or septum. VT from RV includes: Idiopathic VT, BB Reentrant VT, Arrhythmogenic right ventricular dysplasia, VT from Brugada Syndrome 79 Key Choice / CNEA 39
40 VT with RBBB pattern or LVT VT with LBBB pattern or RVT 80 RBBB with Aberration LBBB with Aberration VT from Left Ventricle VT from Right Ventricle 81 Key Choice / CNEA 40
41 RBBB LBBB 82 Left Ventricular Tachycardia Right Ventricular Tachycardia QS complex r wave followed by S wave with R:S ratio < 1 - Any Q Wave - QS wave 83 Key Choice / CNEA 41

42 SVT RBBB SVT LBBB VT VT Key Choice / CNEA 42


43 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT 86 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT 87 Key Choice / CNEA 43


44 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT 88 AV Dissociation or Negative Concordance Extreme Axis or V6 Negative SVT RBBB LVT SVT LBBB RVT 89 Key Choice / CNEA 44

45 SVT RBBB SVT LBBB LVT RVT 90 SVT RBBB SVT LBBB LVT RVT 91 Key Choice / CNEA 45

46 SVT RBBB SVT LBBB LVT RVT 92 SVT RBBB SVT LBBB LVT RVT 93 Key Choice / CNEA 46

47 SVT RBBB SVT LBBB LVT RVT 94 SVT RBBB SVT LBBB 12 Lead ECG Post Inferior STEMI on Arrival to CCU LVT RVT 95 Key Choice / CNEA 47


48 96 SVT RBBB SVT LBBB LVT RVT 97 Key Choice / CNEA 48

49 SVT RBBB SVT LBBB LVT RVT Key Choice / CNEA 49
50 STRIP 1 STRIP STRIP 1 STRIP 2 Learn to recognize RBBB and LBBB morphology in lead V1 (and document) when patients are in SR. Will be better prepared to differentiate between VT and SVT with BBB (aberrancy) when a wide complex tachycardia develops. Strip 1: Atrial flutter with normal QRS width. Strip 2: Wide complex tachycardia Now 2:1 atrial flutter with an increased ventricular rate Results in right bundle becoming refractory Therefore conducts with a RBBB. 101 Key Choice / CNEA 50
51 Beta Blockers Suppresses ventricular arrhythmias Reduces incidence of SCD Amiodarone Suppresses ventricular arrhythmias No definite survival benefit Complex drug interactions and many adverse side effects Sotalol Suppresses ventricular arrhythmias No definite survival benefit More pro-arrhythmic than amiodarone Antiarrhythmics (excluding beta blockers) not used as primary therapy for prevention Patients with VT who do not meet criteria for ICD Beta-blocker first line Amiodarone or sotalol if not effective Patients with ICD with recurrent VT Sotalol or Combination of amiodarone and betablocker 102 Stable Ventricular Tachycardia (Preserved LV Function) Monomorphic Procainamide Sotalol * Amiodarone Lidocaine Polymorphic Normal QT Beta Blockers (or) Lidocaine (or) Amiodarone (or) Procainide (or) Sotalol (or) Polymorphic Prolonged QT Magnesium (or) Lidocaine (or) Isoproterenol (or) Phenytoin (or) Stable Ventricular Tachycardia (Monomorphic or Polymorphic: Normal or Prolonged QT) (Impaired Cardiac Function) * Amiodarone (or) Lidocaine 103 Key Choice / CNEA 51
52 V-fib seldom is seldom preceded by warning arrhythmias Prophylactic lidocaine not indicated R on T PVCs are typically only important first 24 hours of myocardial infarction Bigeminy may need treated if cardiac output effected Ventricular ectopy (as infrequent as 15% burden) can result in heart failure Potential reversible causes Hypokalemia: K < 3.2 meq/l (cause or result) Magnesium < 1.5 meq/dl Ischemia Use of inotropic agents Key Choice / CNEA 52
53 Three Reasons for Bedside Cardiac Monitoring Arrhythmia Detection Ischemia Monitoring QT Interval Monitoring 106 Left Main Coronary Artery (LM) Left Anterior Descending Artery (LAD) Diagonal Branch Left Circumflex Artery (LCirc) Obtuse Marginal (OM) Ramus intermedius Right Coronary Artery Marginal Branch Posterior Descending Artery (PDA) Concept of dominance 107 Key Choice / CNEA 53
54 LAD Anterior LV High Lateral LV Septum (anterior 2/3) Bundle Branches Left Circumflex Low Lateral LV Posterior LV Left Atrium Anterolateral papillary muscle of the mitral valve SA Node (45%) AV Node (10%) 108 RCA Inferior LV Septum (lower 1/3) Right Ventricle (marginal branch) Posterior LV (PDA) Posterior LBB Posteromedial papillary muscle Right Atrium SA Node (55%) AV Node (90%) 109 Key Choice / CNEA 54
55 Purpose To monitor changes in ST segments (compared to baseline) in select leads Leads of Choice Based on area of known or potential ischemia Anterior wall / Left anterior descending coronary Lead V3 Inferior wall / Right Coronary artery Lead III Lateral wall / Circumflex coronary artery Lead V6 110 Lead 1 + Left Arm High Lateral Wall avr + Right Arm V1 + 4 th ICS, RSB Septal Wall VT vs Aberrancy V4 + L MCL, 5 th ICS Anterior Wall Lead 2 + Left Leg Inferior Wall avl + Left Arm High Lateral Wall V2 + 4 th ICS, LSB Septal Wall V5 + L anterior axillary, same level as V 4 Low Lateral Wall Lead 3 + Left Leg Inferior Wall ST - RCA avf + Left Leg Inferior Wall V3 + Midway Between V 2 & V 4 Anterior Wall ST - LAD V6 + L midaxillary line, same level as V 4 Low Lateral Wall VT vs Aberrancy ST - Circ 111 Key Choice / CNEA 55
56 Patients in early phase of Acute Coronary Syndromes (including Rule Out ) Patients who present to ED with chest pain or anginal equivalent symptoms Patients who have had nonurgent percutaneous coronary interventions with suboptimal results Patients with possible variant angina resulting from coronary vasospasm 112 Patients postacute MI Patients after nonurgent uncomplicated percutaneous coronary intervention Patients at high risk for ischemia after cardiac or noncardiac surgery Pediatric patients at risk of ischemia or infarction resulting from congenital or acquired conditions 113 Key Choice / CNEA 56

57 Patients with left bundle branch block Patients with ventricular paced rhythms Patients with other confounding arrhythmias that obscure the ST Segment Patients who are agitated 114 Identification of body position changes Careful skin preparation Consistent lead placement Tailoring alarm parameters to patients baseline ST level Understand goals of monitoring in the individual patient Analyze ECG print out rather than just graphic trends 115 Key Choice / CNEA 57
58 STs may fluctuate with body position changes May cause false alarms ST should be evaluated with patient in the supine position ECG noise impedes accurate diagnosis Skin prep essential to good tracing Clipping to remove hair Remove skin oils with abrasion (dry 4x4) Keep electrodes in original package start to dry 20 minutes after opening Mark electrode placement Waveform changes may occur with as little as 1cm change in location Assess change in ST for true change or change lead location 116 Alarms must be set to reflect each individual patient s baseline 1mm above and below for precordial leads 0.5 mm for limb leads 2mm reasonable in the more stable patient (helps eliminate false alarms) Monitor for silent ischemia Monitor for recurrent ischemia Bad Alarm Monitor for ST recovery after intervention with fibrinolytic or PCI Good Alarm Graphic trends are capable on most monitors with ST segment monitoring Convenient for quick identification of ischemia Should never replace evaluation of rhythm strips When in doubt always verify with a 12 lead ECG 117 Key Choice / CNEA 58


59 Voltage or amplitude Measured in millivolts(mv) or millimeters (mm) EKG machine calibrated so that 1 mv produces a deflection measuring exactly 10 mm tall 1 small box = 1 mm high 1 large box = 5 mm high 118 BE THE BEST THAT YOU CAN BE EVERY DAY. YOUR PATIENTS ARE COUNTING ON IT! cindy@cardionursing.com Final slides will be available at next week 119 Key Choice / CNEA 59




60 120 Let s continue on our journey!! 121 Key Choice / CNEA 60


61 In limb leads the ST segment is normally isoelectric but may be slightly elevated or depressed by less than 1mm In precordial leads ST segment elevation is normally not more than 1 to 2 mm (small elevation normal in many people) 122 ST segments are measured 60 to 80 msec from J point to avoid atrial repolarization wave. 123 Key Choice / CNEA 61



 to 10 mm")
62 Point where the QRS complex and the ST segment meet. 124 Represents ventricular repolarization Slightly asymmetrical Usually upright Most likely abnormal If inverted in two contiguous leads Not normally > than 5mm (limb leads) to 10 mm (precordial) high 125 Key Choice / CNEA 62
 Assess for T wave inversion next Non STEMI or Unstable")
 OR")

63 1) Assess for ST segment elevation first ST elevation and need for reperfusion 2) Assess for T wave inversion next Non STEMI or Unstable angina ischemia 3) Assess for ST segment depression thirdly Supply and demand ischemia (often in V5 regardless of vessel occlusion) OR reciprocal changes to ST elevation Clinical application: Supply and demand ischemia is typically not the primary problem in patients at rest 126 Key Choice / CNEA 63

64 Key Choice / CNEA 64

65 Key Choice / CNEA 65


66 T wave should be positive in lead I and II Inversion in lead III, avl and avf may be normal Inversion in V1 is common - always compare to previous ECG Key Choice / CNEA 66



67 Wellen s Warning when seen in chest leads(v2-v3) of undiagnosed patient Represents LAD occlusion that spontaneously reperfused prior to the ECG (lesion at risk for reocclusion) Seen on ECG done during pain free period Can be UA / NSTEMI 134 Can be seen in exercise stress testing with supply and demand ischemia. Often seen with left ventricular hypertrophy. 135 Key Choice / CNEA 67
68 ECG Be suspicious of horizontal ST segment depression in patient at rest. Suspect left main disease (or significant 3 vessel disease) when diffuse depression and ST elevation in lead avr (and V1 to lesser extent) Presentation Assess for reasons for supply and demand ischemia at rest (i.e. low hemoglobin). Rule out medical reason for falls, motor vehicle crashes, and other trauma (i.e. syncope or near syncope due to cardiac cause). 136 T wave inversion is a warning for ACS (either unstable angina or NonSTEMI) unless T wave inversion occurs after a STEMI After a STEMI T wave inversion is expected Terminal T wave inversion is a sign of reperfusion after a STEMI Symmetrical T wave inversion will develop after terminal T inversion 137 Key Choice / CNEA 68

69 138 Evolutionary changes occur due to prolongation of the cardiac action potential in regions of stunned myocardium adjacent to the necrotic area. Prolongation in repolarization affects the voltage and polarity of the T wave. Ventricular remodeling can produce differences in electrical fields that may be responsible for the evolutionary changes. 139 Key Choice / CNEA 69
70 ST segment back to baseline occurs as result of myocardial cell death and reduction in injury current. One of final evolutionary changes. Abrupt resolution of ST elevation indicates reperfusion. Persistent ST elevation is predicator of adverse outcomes Key Choice / CNEA 70


71 ST segment back to baseline occurs as result of myocardial cell death and reduction in injury current. One of final evolutionary changes. Abrupt resolution of ST elevation indicates reperfusion. Persistent ST elevation is predicator of adverse outcomes Hours Post STEMI Lead III 36 Hours Post STEMI Lead III 143 Key Choice / CNEA 71



72 Key Choice / CNEA 72


73 Key Choice / CNEA 73
.")
74 A SUCCESS Story!! The next 2 slides show the following: 1. Admission ECG for a patient with an anteroseptal / lateral wall STEMI. 2. ECG post intervention for same patient. 1. Note: The T waves have not yet inverted post intervention. Ideally T waves will begin to invert after an intervention showing evidence of reperfusion. REMEMBER: T wave must invert within hours after a STEMI (the sooner the better). Failure of T waves to invert after a STEMI is indicative of post infarction regional pericarditis and the patient is at higher risk for myocardial rupture Key Choice / CNEA 74

75 150 The strip below assessing ST segments in V3 was done 48 hours post STEMI (same patient as previous 2 ECGs.). The failure of the T waves to invert is indicative of post infarction regional pericarditis with increased risk of myocardial rupture. The patient was hypotensive, which raises the concern for cardiac tamponade as the etiology of the hypotension. This assessment finding was communicated to the cardiologist. The patient s echocardiogram showed a large pericardial effusion and the patient subsequently underwent a surgical pericardial window. 151 Key Choice / CNEA 75
 ST Depression (ischemia) Reciprocal Changes ST segment depression in leads")



76 Primary Change is most important look for: ST Elevation: ACS (STEMI) T Wave Inversion: ACS (Non STEMI or UA) ST Depression (ischemia) Reciprocal Changes ST segment depression in leads reciprocal (opposite) those with ST elevation Reciprocal changes can help confirm primary changes 152 Lead 1 avr V1 V4 Left Arm High Lateral Wall Right Arm 4 th ICS, RSB Septal Wall L MCL, 5 th ICS Anterior Wall Posterior Wall Lead 2 avl V2 V5 Left Leg Inferior Wall Left Arm High Lateral Wall 4 th ICS, LSB Septal Wall L anterior axillary, same level as V 4 Low Lateral Wall Lead 3 avf V3 V6 Left Leg Inferior Wall Left Leg Inferior Wall Midway Between V 2 & V 4 Anterior Wall L midaxillary line, same level as V 4 Low Lateral Wall 154 Key Choice / CNEA 76


77 Key Choice / CNEA 77
78 These are vulnerable areas of myocardium: Not directly assessed on 12 Lead! 157 ST depression in V1-V3 Think posterior injury Isolated ST elevation in VI (But don t rely on V1) Think RV involvement 158 Key Choice / CNEA 78

79 V3 V Key Choice / CNEA 79


80 VI V4 V2 V5 V3 V6 161 VIR V4R V2R V5R V3R V6R 162 Key Choice / CNEA 80


81 Note: V1 and V2 may also be reversed with V1 on LSB and V2 on RSB. If so, these are labeled V1R and V2R. 163 Right Ventricular Leads Posterior Leads 164 Key Choice / CNEA 81
82 Original V Leads V1 V2 V3 V4 V5 V6 New V Leads V4R V5R V6R V7 V8 V9 165 Place electrode in V4R Position 5 th ICS Right MCL Attach V monitoring lead (Brown Lead) to electrode Assure monitor lead selector is on V Run strip and clearly mark V4 Right Chest Lead Place electrode in V8 position Under tip of left scapula same level as V6 Attach V monitoring lead (Brown Lead) to electrode Assure monitor lead selector is on V Run strip and clearly mark V8 Posterior Lead 166 Key Choice / CNEA 82

83 Patient post cardiac arrest on hypothermia. 167 Inferior STEMI: ST Elevation in II, III, avf Reciprocal depression in Leads I and avl ST Depression in V2 and V3: Reciprocal changes from Posterior STEMI Ideal patient for an extended lead ECG to assess for injury to the right ventricle and posterior wall of the left ventricle. 168 Key Choice / CNEA 83
84 Same Patient as Previous 12 Lead: Due to hypotension the point of care nurse used the V lead from bedside monitoring to record a V4R lead. This recording confirms RV injury and this knowledge was used to guide treatment. ST segment elevation in lead V4R demonstrates high risk for high grade AV node block (Wellen & Conover, 2006). 169 Support for Continuous ST Segment Monitoring Key Choice / CNEA 84
85 61 year old Caucasian male with increasing SOB and cough for 2-3 days. Treated by his PCP with ATB, Tessalon Perles and Flonase for asthmatic bronchitis. Presented to ED (via EMS) later that evening with severe DOE. Was hypoxic on arrival. + cough with yellow sputum, wheezing, SOB. Admitted and placed on IV steroids of bronchitis. Obstructive sleep apnea (noncompliant with CPAP) HTN Psoriatic arthritis DM, Type II Obesity Tobaccoism ETOH use (daily) Key Choice / CNEA 85

86 Troponin 0.01, 0.02, 0.14 Myoglobin 89, 323 WBC 15,000; Hgb 13.9; Plt 239,000 Glucose 419, Na 135, BUN 17, Cr 1.16, K 4.4 Rapid flu neg CXR: no acute process Key Choice / CNEA 86
87 Symptoms did not suggest ACS, but due to risk factors another troponin was drawn. Troponin bump was felt to be due to hypoxia. A Lexiscan stress test was recommended once his pulmonary status improved. Troponin 0.36 Patient more SOB Repeat ECG ordered Patient down in heart lab for echocardiogram. ECG done 1 hour later. Key Choice / CNEA 87
. EF 55%.")
88 Patient emergently to the cardiac cathetrization lab (called as a STEMI) and received PCI with DES to RCA (100% occluded). EF 55%. Was also a RV infarct Key Choice / CNEA 88

89 Key Choice / CNEA 89


90 Key Choice / CNEA 90


91 Key Choice / CNEA 91


92 Key Choice / CNEA 92


93 Key Choice / CNEA 93
94 Three Reasons for Bedside Cardiac Monitoring Arrhythmia Detection Ischemia Monitoring QT Interval Monitoring 189 Purpose To monitor for increase in QT interval to identify and intervene in patients at high risk for Torsades de Pointes Leads of Choice Lead where an accurate QT Interval can be measured Patient can be changed to another lead to run a strip to measure QT or 12 lead can be done if QT not easily measured in V1 or V 6 Notes: QT interval needs to be adjusted for HR QT does not adjust to HR on a beat to beat basis V2 and V3 usually have the longest QT Dynamic changes are most important Abnormal findings are uncovered during abrupt changes in the R to R 190 Key Choice / CNEA 94
95 Key Choice / CNEA 95
96 Measured from beginning of QRS complex to the end of the T wave Reflects both ventricular depolarization (QRS) and ventricular repolarization (T wave) Used most specifically to reflect ventricular repolarization 193 Role of QRS width in QT interval Manual versus computer generated measurement U waves End of T wave in biphasic T wave Which lead for measurement RR interval in irregular rhythms Calculated measurement via 12 Lead ECG Bedside monitor calculation via e-calipers Continuous QT interval monitoring software Qtip Study 194 Key Choice / CNEA 96
97 QT usually measures longest V2 or V3 T wave is often clearest V5 or V6 For repetitive QT interval monitoring in an inpatient setting: Pick a lead with a well defined T wave Use the same lead consistently 195 U Waves and Biphasic T waves. 196 Key Choice / CNEA 97
98 QT interval needs to be adjusted for HR QT does not adjust to HR on a beat to beat basis Dynamic changes are most important Abnormal findings are uncovered during abrupt changes in the R to R Irregular heart rhythms (i.e. atrial fibrillation) remain a clinical challenge 197 Print a long rhythm strip to assess over the course of the strip if the interval from the R wave to the peak of the following T wave is more than 50% of the proceeding RR interval. If so this is considered too long a QT interval and the risk for Torsades de Pointes is increased. Source: Sommargren & Drew, Key Choice / CNEA 98
; over estimates QT interval at fast HRs QT Dynamics Linear regression analysis 199 HR 70")
99 Measurements are using seconds. Bazett Formula Formula not reliable at slow rates (under estimates); over estimates QT interval at fast HRs QT Dynamics Linear regression analysis 199 HR 70 QT =.43 sec R to R =.84 sec.43 /.9165 = QTc.469 HR 38 QT =.80 R to R = 1.56 sec.80 / 1.28 = QTc Key Choice / CNEA 99
100 1 to 15 Years Adult Males Adult Females Normal <.44 seconds <.43 seconds <.45 seconds Borderline.44 to.46 seconds.43 to.45 seconds.45 to.47 seconds Prolonged >.46 seconds >.45 seconds >.47 seconds Source: Moss AJ, Robinson JL. Long QT Syndromes. Heart Dis Stroke. 1992; QTc.50 sec (500 msec or more is dangerous and should be considered an ominous sign of impending Torsade's de Pointes) Key Choice / CNEA 100
101 Places of unequal repolarization can set up for reentrant tachyarrhythmias There can be the development of early after depolarizations 203 Right after repolarization (or during) there is a transient sub threshold depolarization Can occur during Phase II or III of the cardiac action potential If an early after depolarization reaches threshold a second upstroke occurs and a triggered beat follows The triggered beat may have its own after depolarization that reaches threshold thus causing another triggered beat Thought to be etiology of Torsade's de Pointes Acquired Congenital 204 Key Choice / CNEA 101
 205 206 Key Choice / CNEA")
102 Precipitating Factors Hypokalemia Hypomagnesemia Heightened sympathetic tone Slow heart rate Prolonged repolarization (QT interval) Key Choice / CNEA 102
103 Patients administered an antiarrhythmic drug know to cause Torsades de Pointes Patients who overdose from a potentially proarrhythmic agent Patients with new onset bradyarrhythmias Patients with severe hypokalemia or hypomagnesemia 207 Patients who require treatment with antipsychotics or other drugs with possible risk of Torsades de Pointes Patients with acute neurologic events Healthy patients administered drugs that pose little risk for Torsades de Pointes 208 Key Choice / CNEA 103
104 Long QT Syndrome (LQTS) Brugada disease Idiopathic short QT < 300 to 340 msec Diagnosed by family history and ECG Note: Patients with heart failure can develop channelopathies QTc > 450 ms Genetic defect in either potassium (LQT1 or LQT2) or sodium (LQT3) channels Delayed repolarization (1 and 2) LQT1 and LQT2 = 95% Beta blockers LQT3 = 5% Beta blockers may be harmful Autosomal dominant trait 1 in 2500 QT prolongation important risk factor for SCD QTc < 440 ms / < 5% QTc 460 to 500 ms / 20% QTc > 500 ms / 50% Key Choice / CNEA 104

105 Interestingly some acquired Torsade's may be preceded by T wave morphology looking like congenital LQTS Long QT 1: wide, broad-based T waves Long QT 2: low amplitude, often notched T waves Long QT 3: long ST segment and tall, peaked T waves Key Choice / CNEA 105


106 Key Choice / CNEA 106

107 Disorder of cardiac sodium channel Autosomal dominant Most common in Asia Typical patient young male age 30 to 50 who is otherwise healthy. ST elevation in anterior precordial leads Cove Saddleback ECG can be dynamic In children temperature spike may uncover Treat aggressively Syncope 2 year risk of SCD approximately 30% ICD recommended Key Choice / CNEA 107

108 Quinidine and Isoproteronol two most common drugs use to prevent electrical storms. 217 Recognition of this life-threatening arrhythmia is important because it is not treated like other VTs Two groups: Acquired and congenital Acquired Drugs prolonging repolarization Most often as a result of blocking the potassium channel Electrolyte abnormalities Low potassium Low magnesium Severe bradycardias / pauses 218 Key Choice / CNEA 108
109 Class Ia and Class III antiarrhythmics Antihistamines Antibiotics Antipsychotics Antidepressants Sedatives Gastric motility agents Anticancer agents Opiate agonists Risk Possible Risk Conditional Key Choice / CNEA 109
110 Rapid (IV) administration of QT prolonging agent Renal or hepatic dysfunction Female gender (particularly for drug induced) Advanced age Anorexia Heart disease Poly pharmacy 221 CNEA / Key Choice 222 Key Choice / CNEA 110
111 CNEA / Key Choice 223 Increase QTc from predrug baseline of 60 ms, Marked QTc interval prolongation.500 ms T-U wave distortion that becomes more exaggerated in the beat after a pause Visible (macroscopic) T-wave alternans New-onset ventricular ectopy, couplets Nonsustained polymorphic ventricular tachycardia initiated in the beat after a pause. Key Choice / CNEA 111


112 226 Class I Discontinue offending drugs Note: Class IA drug induced TdP usually appears soon after the initial administration of the drug Correct electrolytes Magnesium Potassium Increase HR Isoproteronol 2 mcg/min then titrate to HR of 100 beats per minute Temporary pacing at rate of 100 to 110 Magnesium is considered treatment of choice. Permanent pacing if bradycardia or CHB cannot be resolved. Defibrillation if sustained However, continue to assess for and treat cause 227 Key Choice / CNEA 112
113 2 Gm IV bolus over 1-2 minutes Followed in 15 minutes by another bolus if necessary May start continuous infusion at rate of 3-20 mg/min Benefit occurs without shortening of QT interval and in presence of normal Magnesium level Key Choice / CNEA 113

114 Key Choice / CNEA 114

115 Patient admitted for syncope after having motor vehicle crash while driving. Long standing history of paroxysmal atrial fibrillation on dofetilide (Tykosin) for several years. Recent chemotherapy for breast CA resulting in a reduction of EF. Recent increase in carvedilol and lisinopril per general cardiology to improve EF. Next slide is admission ECG. Note the QTc interval Key Choice / CNEA 115
116 1. Strip 1: QTc consistent with admission ECG. 2. Strip 2: Marked QTc prolongation when patient asleep. 3. Initial run of ventricular tachycardia initiated by PVC firing at end of T wave, 234 Same patient with sustained Torsades de Pointes. Treated effectively with 2 grams IV Magnesium (magnesium level was normal at baseline). Magnesium is the drug of choice to stabilize the cardiac membrane. Dofetilide (Tikosyn) was also discontinued. Note: Although the patient had been on dofetilide (Tikosyn) for several years, the recent change in ejection fraction and increase in beta blocker therapy increased her risk for Torsades de Pointes. 235 Key Choice / CNEA 116

117 Seen frequently in ischemic conditions Think revascularization Think beta blockers 236 DC cardioversion with sedation when unstable IV beta-blockers if ischemia suspected Improve mortality IV amiodarone in absence of abnormal repolarization Amiodarone better than placebo Magnesium not better than placebo Urgent angiography to exclude ischemia Lidocaine may be reasonable if ischemia suspected Check electrolytes Consider any other potential reversible cause 237 Key Choice / CNEA 117

118 238 The Lewis Lead When P waves are not clearly seen in a rhythm strip (see lead 3 above), the Lewis lead can be very helpful in assessing for the presence of atrial activity. As seen in the Lewis lead above this patient is clearly in an atrial flutter. The atrial flutter is not as obvious in the lead III rhythm strip. Key Choice / CNEA 118



119 V1 MCL6 MCL6 Key Choice / CNEA 119


120 Telemetry Pack R A Lead 1 L A 242 Critical Thinking Guideline for Cardiac Monitoring 243 Key Choice / CNEA 120
121 Patient Characteristics Ejection fraction < 30% Implantable cardioverter defibrillator Non ischemic cardiomyopathy Syncope as reason for admission Current frequent premature beats or short runs of tachycardias Monitoring Priorities Arrhythmia monitoring: Use V1 and V6 (or MCL6) as primary monitoring leads. 244 Patient Characteristics Stable acute coronary syndrome (ACS) or rule out ACS as reason for admission Admission symptoms suspicious for ischemia (shortness of breath, nausea, fatigue, etc) Admission with heart failure with history of recent revascularization Monitoring Priorities Ischemic monitoring: Use V3 and lead III as primary ischemia detection leads if area of ischemia or culprit vessel is unknown. If known, choose ischemia monitoring leads based on ECG footprint during active ischemia document reason for use of chosen leads. Perform ECG with posterior leads (or record lead V 8 ) during symptomatic episodes with non diagnostic standard 12 Lead. Simultaneously monitor in V1 for arrhythmia detection for patients admitted to ICU or step down level of care. Note: Whenever possible in ICU and step down level patients a 6 lead telemetry system should be used in order to monitor V1 for arrhythmia detection and the second V lead for ischemia monitoring. 245 Key Choice / CNEA 121
122 Patient Characteristics New administration of class I or class III antiarrhythmics Electrolyte abnormalities (hypokalemia, hypomagnesemia, hypocalcemia) QTc >.45 seconds Receiving Haldol or other high risk medications Monitoring Priorities Use arrhythmia monitoring leads as baseline monitoring leads (V1 & V6). Measure QTc interval q 4 hours with rhythm interpretation in lead where QT interval can be clearly defined. Document and record lead used for measurement. Use consistent lead in the measuring of QTc. 246 Patient Characteristics High risk (hemodynamic or electrical instability) ACS Monitoring Priorities V1 for arrhythmia assessment Secondary monitoring can be a limb lead or modified chest lead to aid in either arrhythmia interpretation or ischemia detection. 247 Key Choice / CNEA 122


123 Key Choice / CNEA 123


124 250 BE THE BEST THAT YOU CAN BE EVERY DAY. YOUR PATIENTS ARE COUNTING ON IT! Final slides will be available at next week 251 Key Choice / CNEA 124
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 1
 Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 1 1 st CCU in the world opened in March 1962 was in Toronto, Canada In May of 1962 the 1 st CCU in
Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN 1 1 st CCU in the world opened in March 1962 was in Toronto, Canada In May of 1962 the 1 st CCU in
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
Ability is what you are capable of doing. Motivation determines what you do. Attitude determines how well you do it. - Lou Holtz
 Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Ability is what you are capable of doing. Motivation determines what you do. Attitude determines how
Presented By: Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Ability is what you are capable of doing. Motivation determines what you do. Attitude determines how
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Knowing is not enough; we must apply. Willing is not enough; we must do.
 Cardiovascular Boot Camp Basic Training Day 2: Cardiac Arrhythmias and Emergency Treatment Overview Cardiac Arrhythmias: Physiologic Links to Recognition and Management NTI 2014 Denver 2014 Karen Marzlin
Cardiovascular Boot Camp Basic Training Day 2: Cardiac Arrhythmias and Emergency Treatment Overview Cardiac Arrhythmias: Physiologic Links to Recognition and Management NTI 2014 Denver 2014 Karen Marzlin
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants
 Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
Introduction to Electrocardiography
 Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
12 Lead EKG. The Basics
 12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead ECG Interpretation: Color Coding for MI s
 12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
The Fundamentals of 12 Lead EKG. ECG Recording. J Point. Reviewing the Cardiac Conductive System. Dr. E. Joe Sasin, MD Rusty Powers, NRP
 The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
Electrocardiogram ECG. Hilal Al Saffar FRCP FACC College of medicine,baghdad University
 Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
3/4/2018. March Martina Frost, PA C Desert Cardiology. Electricity moving towards/away from electrode create downward/upward directions of waves
 March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
This presentation will deal with the basics of ECG description as well as the physiological basics of
 Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
ECG Interpretation. Introduction to Cardiac Telemetry. Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services
 ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
CORONARY ARTERIES HEART
 CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
RN-BC, MS, CCRN, FAHA
 Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! 1 A. Atropine
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! 1 A. Atropine
2009 Unit-Based Competencies
 2009 Unit-Based Competencies Alameda County Medical Center Highland Hospital Emergency Department Janis Farnholtz Provinse, RN, MS, CNS, CEN, ED Clinical Nurse Specialist Nurses play a pivotal role in
2009 Unit-Based Competencies Alameda County Medical Center Highland Hospital Emergency Department Janis Farnholtz Provinse, RN, MS, CNS, CEN, ED Clinical Nurse Specialist Nurses play a pivotal role in
PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART I
 1 PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART I Cynthia Webner DNP, RN, CCNS, CCRN-CMC Karen Marzlin DNP, RN, CCNS, CCRN-CMC 2 PROFESSIONAL NURSING PRACTICE CAN ONLY ADVANCE AS MUCH AS INDIVIDUAL
1 PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART I Cynthia Webner DNP, RN, CCNS, CCRN-CMC Karen Marzlin DNP, RN, CCNS, CCRN-CMC 2 PROFESSIONAL NURSING PRACTICE CAN ONLY ADVANCE AS MUCH AS INDIVIDUAL
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO
 Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! What is a
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! What is a
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
12 Lead ECG Interpretation: The Basics and Beyond
 12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
December 2018 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
ECG Practice Strips Discussion part 1:
 ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Chapter 2 Practical Approach
 Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Ventricular arrhythmias
 Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists
 PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Case 1. Case 2. Case 3
 Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
also aid the clinician in recognizing both the obvious and subtle abnormalities that may help guide therapy.
 Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천
 The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic