Auskultation Inspektion. Perkussion
|
|
|
- Ernest Stewart
- 5 years ago
- Views:
Transcription



1 Auskultation Inspektion Perkussion



2 Different thorax shapes may have influence on lung function
3 Reasons for chest pain Cardiovascular AMI Aortic dissection Myocarditis Pericarditis Chest wall Cervical disc disease Costochondritis Fibrositis Herpes zoster (before the rash) Neuropathic pain Rib fracture Sternoclavicular arthritis Psychiatric Affective disorders (eg, depression) Anxiety disorders Hyperventilation Panic disorder Primary anxiety Somatiform disorders Thought disorders (eg, fixed delusions) Gastrointestinal Biliary Cholangitis Cholecystitis Choledocholithiasis Colic Esophageal Esophagitis Spasm RefluxRupture Pancreatitis Peptic ulcer disease Nonperforating Perforating Pulmonary Pleuritis Pneumonia Pulmonary embolus Pneumothorax cancer
4 Diagnoses when patient comes to doctor for chest pain! All ages.. Reason Prevalens (%) Muscle skeletal system 36 Stomach (GI) 19 Heart 16 Stabile angina 10.5 Unstabil angina 1.5 Andre 3.8 Psykriatrisk 8 lung 5 Uknown 16 1 år follow-up Klinkman et al. J Fam Pract 1994; 38: 345




5


6 Why do so few patients with lung disases have pain in the start of their disease med smerter??



7 No pain receptores!!


8 62 years old man Debut haemoptysis No Pain!!

9 Remember
10

11 Wardlaw AJ et al. Multidimensional phenotyping: towards a new taxonomy for airway disease. Clin Exp Allergy 2005;35:
12 Causes of isolated chronic cough Primary Cause of Cough No. of patients (%) Rhinitis 24 Asthma 17.6 Postviral 13.2 Eosinophilic bronchitis 13.2 Gastroesophageal reflux 7.7 Unexplained 6.6 COPD 6.6 Bronchiectasis 5.5 ACE inhibitor-induced cough 4.4 Lung cancer 2.2 Cryptogenic fibrosing alveolitis 1.1 Brightling CE et al. AJRCCM 1999

13 Wardlaw AJ et al. Multidimensional phenotyping: towards a new taxonomy for airway disease. Clin Exp Allergy 2005;35:
14 BRONCHIECTASIS Definition: Abnormal and permanent dilation of bronchi. Focal or diffuse distribution Clinical consequences chronic and recurrent infection and Pooling of secretions in dilated airways. Classification (ex: microscope): 1. Cylindrical (fusiform) 2. Saccular 3. Varicose

15 Bronchiectasis

16 Bronchiectasis:

17

18


19 Saccular Bronchiectasis:


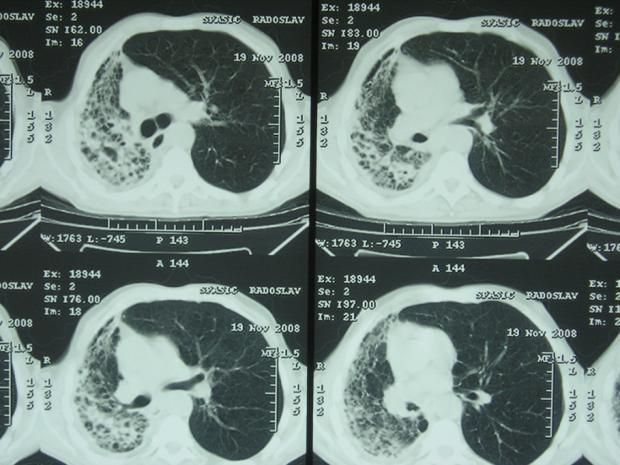
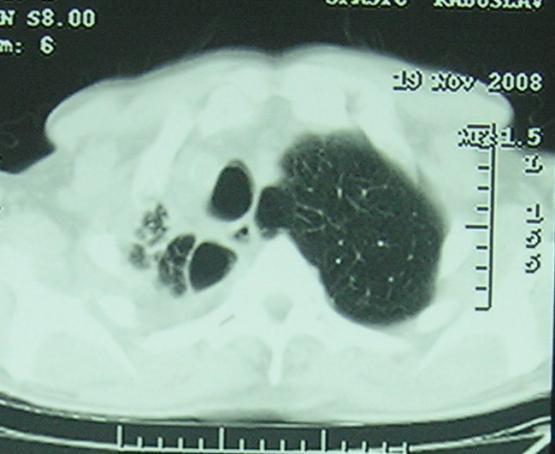
20 Destroyed lung- bronchiectasis

21


22
23 Pathogenesis - Bronchiectasis Obstruction Infection. Excess Mucous secretion Retention of secretion Secondary infection Destruction of bronchial wall Irregular, fixed inflamed dilated bronchus filled with pus.
24 Aetiology: A. Infections-Micro-organisms Measles and Pertussis Adeno & Influenza virus Bacterial infection with virulent organisms: S.aureus, Klebsiella Anaerobes Atypical mycobacteria Mycoplasma HIV Tuberculosis Fungi Tumor Cystic fibrosis Ciliar dyskinesia
25
26 CLINICAL MANIFESTATIONS Persistent or recurrent cough with purulent sputum. Haemoptysis Initiating episode: Severe pneumonia, or insidious onset of symptoms or asymptomatic or non-productive cough dry bronchiectasis in upper lobe, Dyspnoea, wheezing widespread bronchiectasis or underlying COPD. Exacerbation of infection: Sputum volume increase, purulence or blood.
27 PHYSICAL EXAMINATION Any combination of rhonchi, creps or wheezes. Clubbing of digits. Chronic hypoxaemia cor pulmonale R heart failure Amiloidosis (rare)
28 Epidemiology Increasing frequency in the 21 th century 2005: in the USA: pts treated for noncf bronchiectasis years: 4.2/ >75 years: 272/ Most frequently: in older women Causes: Widespread use of HRCT Increase in Non-TB Mycobacterial infections
29 Reasons for increase of bronchiectasis in developing countries emergence of drug-resistant microorganisms Increasing frequency of MDR TB Irregular and inadequate treatment cessation of medication shortly after symptom improvement lack of check-ups after treatment Recurrent pulmonary infections S. Eren et al. J Thorac Cardiovasc Surg 2007;134:
30 Bronchiectasis limited disease Left side predominance ( %) Lower lobes predominance Bilateral disease (9-21%) Unilateral - single lobe Unilateral - > single lobe Bilateral -
31 DIAGNOSIS - 1 Clinical Radiology: Chest XR: May be non-specific mild disease normal XRC advanced disease cysts + fluid levels peribronchial thickening, tram tracks, ring shadows CT Scan: Peribronchial thickening, dilated bronchioles. Sputum culture: Pseudomonas aeuruginosa, H.influenzae.

32
33 DIAGNOSIS - 2 Lung function: Airflow obstruction FEV1 decreased. Air trapping - RV increased Sweat test increased sodium and chloride in cystic fibrosis Bronchoscopy: Obstruction foreign body, tumor. Immunoglobulin Cilia function and structure Kartagener syndrome.

34

35 Contralateral Bronchography:

36 CT - experience diagnostic value: excellent anatomic distribution: inferior to bronchography R of the bronchus > R of the accompanying p. artery (1.5) Loss of normal tapering of airway towards periphery ( tram tracks )




37 CT pictures
38 TREATMENT Goals: 1. Eliminate cause 2. Improve tracheo bronchial clearance 3. Control infection 4. Reverse airflow obstruction
39 TREATMENT Immunoglobulin 2. Antituberculous drugs if TB 3. Corticosteroids (ABPA) 4. Remove aspirated material Chest physical therapy Mucolytics Bronchodilators
40 TREATMENT - 3 Antibiotics short course, prolonged course, intermittent regular courses, inhalation. Initial empiric Rx: Ampi, Amox, Ps.aeruginosa Quinolone, aminoglycoside, 3 rd generation cephalosporin, pipracillin. Surgery: Oxygen and diuretics Lung transplant
41 Limited disease indications for the operation (%) recurrent infections hemoptysis abscess undiagnosed lung mass pnth empyema no symptoms Fujimoto (n 92) Balkanli (n 238) Kutlay (n 166) Prieto ( n 119) Agasthian (n 134) exacerbations/year (North America, UK, Ireland) Chest 1998; 113:




42 Well perfused bronchiectasis

43 Well perfused bronchiectasis Clear destruction source of repeated infections

44 bronchiectasis


45 PLEURAL EFFUSIONS AND OTHER PLEURAL DISEASE: A SHORT OVERVIEW

46 Normal pleura Two layers: Visceral Parietal - accounts for most secretion and absorption of pleural fluid. Normal values: volume: 7-10ml protein: 15g/L cells: 1500/ ul
47 Pathogenesis of pleural effusion Elevated capillary hydrostatic pressure cardiac failure. Reduced capillary oncotic pressure - hypoalbuminemia. Enhanced capillary permeability - inflammation. Obstructed lymphatics - tumor. Movement of fluid from extrathoracic site - pancreatitis.

48 Clinical manifestations Symptoms: Asymptomatic pain- "pleuritic" or "dull ache" cough dyspnea Physical examination: enlarged hemithorax reduced vocal fremitus dullness to percussion decreased breath sounds, friction-rub
49 Types Hydrothorax Hemothorax Chylothorax Pyothorax or Empyema
 and semicircular meniscus on lateral films.")
50 Approach to a pleural effusion Plain chest X-ray Distribution is determined by gravity.. Obliteration of lateral costophrenic angle Fluid higher laterally (PA film) and semicircular meniscus on lateral films.. Detects > 175ml off fluid May be subpulmonic, loculated or "pseudotumor"


51 Clinical approach- cont.. Horizental x-rays Ultrasound CT Scan, MRI Pleuracentesis!!!! Pleural biopsy Thoracoscopy Open pleural biopsy
52 Exudative Narrowing the Differential of Etiology Pleural Effusions Local factors influencing accumulation of pleural fluid affected Transudative Etiology Imbalance between hydrostatic//oncotic force
53 Classification Transudate Ultrafiltrate of plasma Small group of etiologies Exudate Produced by host of inflammatory conditions Large group of etiologies
54 Modified Light s Criteria Pleural fluid protein > 2.9 g/dl Pleural cholesterol > 45 mg/dl Pleural LDH > 60 % ULN (upper limit of normal) Any ONE off the following defines an exudate. (Traditional Light s criteria: Protein P/S > 0.5 LDH P/S > 0.6 LDH > 2/3 ULN)
55 Workup: Laboratory LDH > 1000 IU/L Empyema, Malignancy, Rheumatoid Glucose < 30 mg/dl Empyema, Rheumatoid Glucose between mg/dl Lupus, Malignancy, TB
56 Albumin Gradient Light s criteria tend to overcall exudates Especially in transudative effusions after diuresis if difference between albumin in serum minus pleural fluid is > 1.2 than more likely a true transudate May misidentify 13%
57 Exudative or Transudative Sensitivity of Tests to Distinguish Exudative from Transudative Effusions
58 Transudates = ultra filtrate off serum CARDOSIS (CHF) due to increased pulmonary venous pressures, usually bilateral (R > L), usually resolves in 48 hours after diuresis NEPHROSIS low oncotic pressures CIRRHOSIS can preferentially form in pleural space, hepatic-hydrothorax
59 Other Transudates Atelectasis increased negative pleural pressure Congestive cardiac failure Peritoneal dialysis Glomerulonephritis Urinothorax Myxedema Pulmonary embolism Sarcoidosis.
60 Differential diagnosis- exudate Parapneumonic effusion Malignancy - lung, breast, lymphoma, mesothelioma Tuberculosis Pulmonary emboli Abdominal disease Esophageal perforation Collagen vascular disease
61 Differential diagnosis- exudates Drugs- nitrofurantoin, bromocryptine, amiodarone, methotrexate. Asbestos Dressler's syndrome Meig's syndrome, Yellow-nail syndrome, Sarcoidosis,, Uremia,, Myxedema
62 Total and Differential Cell Counts Neutrophil predominance (>50%) Implies acute process* 21 of 26 parapneumonic effusions (81 percent) 4 of 5 effusions secondary to pulmonary embolus (80 percent) 4 of 5 effusions secondary to pancreatitis (80 percent) But only 7 of 43 malignant effusions (16 percent) and none of 14 tuberculous effusions contained more than 50 percent neutrophils. Light RW, Erozan YS, Ball WC Jr. Cells in pleural fluid: their value in differential diagnosis. Arch Intern Med 1973;132:
63 Total and Differential Cell Counts Lymphocyte predominance (>50%) Implies chronic process Cancer, TB, or post CABG The combined data from two series*show that: 90 of 96 exudative pleural effusions consisting of more than 50 percent lymphocytes (94 percent) were due to cancer or tuberculosis.. In these series, 90 of 116 tuberculous pleural effusions (78 percent) contained more than 50 percent lymphocyttes.. *Yam LT. Diagnostic significance of lymphocytes in pleural effusions. Ann Intern M
64 Total and Differential Cell Counts Eosinophilia predominance 2/3 blood or air in pleural space (repeated thoracentesis) Drug reactions Dantrolene Bromocriptine Nitrofurantoin Exposure to asbestos, paragoniimiiasiis,, Churg Sttrauss syndrome..
65 Pleural Fluid Glucos Pleural Glucose < 60 mg/dl Rheumatoid pleural effusions can be < 10mg/dl. May have Increased cholesterol from cell debris. Empyema/ Complicated Parapneumonic Effusions Esophageal rupture high level of salivary amylase & very low ph Malignancy Rarely:: Chourg Strauss syndrome, Paragonimiasis (lung fluke),lupus pleuritis..


66 Workup: Imaging


67 Workup: Imaging
68 Workup: Imaging Ultrasound Aids in identification of loculated effusions Aids in differentiation of fluid from fibrosis Aids in identification of thoracentesis site Available at bedside
69 Workup: Imaging CT Scan Aids in differentiation of Lung consolidation vs. Pleural effusion Cystic vs. Solid lesions Peripheral lung abscess vs. Loculated emypema Aids in identification of Necrotic areas Pleural thickening, nodules, masses Extent of tumor
70 Treatment Treat underlying etiology Therapeutic thoracentesis

71



72 Ja, specielt hos patienter med bilateral hilus adenit, erytema nodosum vil sygdommen forsvinde igen inden for et år
Management of Pleural Effusion
 Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Dr. A.Torossian, M.D., Ph. D. Department of Respiratory Diseases
 Pleural effusions Dr. A.Torossian, M.D., Ph. D. Department of Respiratory Diseases A pleural effusion is an abnormal collection of fluid in the pleural space resulting from excess fluid production or decreased
Pleural effusions Dr. A.Torossian, M.D., Ph. D. Department of Respiratory Diseases A pleural effusion is an abnormal collection of fluid in the pleural space resulting from excess fluid production or decreased
Pleural Diseases. Dr Matthew J Knight Consultant Respiratory Physician
 Pleural Diseases Dr Matthew J Knight Consultant Respiratory Physician What do you need to know? What do you need to know? Pleura- normal anatomy and physiology Pleural effusions Causes and investigations
Pleural Diseases Dr Matthew J Knight Consultant Respiratory Physician What do you need to know? What do you need to know? Pleura- normal anatomy and physiology Pleural effusions Causes and investigations
PLEURAL EFFUSION. Prof. G. Zuliani
 PLEURAL EFFUSION Prof. G. Zuliani Anatomy of pleural membrane and pleural space Pleural membrane consists of parietal pleura and visceral pleura A space situated between parietal and visceral pleura is
PLEURAL EFFUSION Prof. G. Zuliani Anatomy of pleural membrane and pleural space Pleural membrane consists of parietal pleura and visceral pleura A space situated between parietal and visceral pleura is
Pulmonary Morning Report. Ashley Schmehl D.O. PGY-3 January,
 Pulmonary Morning Report Ashley Schmehl D.O. PGY-3 January, 8 2015 Pleural Effusion Unilateral versus Bilateral Associated symptoms Transudate versus Exudate Light s Criteria: Pleural protein: Serum protein
Pulmonary Morning Report Ashley Schmehl D.O. PGY-3 January, 8 2015 Pleural Effusion Unilateral versus Bilateral Associated symptoms Transudate versus Exudate Light s Criteria: Pleural protein: Serum protein
Diagnostic Approach to Pleural Effusion
 Diagnostic Approach to Pleural Effusion Objectives Define the leading causes of pleural effusion Classify the type of effusion Identify procedures and tests associated with diagnosis 2 Agenda Basic anatomy
Diagnostic Approach to Pleural Effusion Objectives Define the leading causes of pleural effusion Classify the type of effusion Identify procedures and tests associated with diagnosis 2 Agenda Basic anatomy
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Pleural fluid analysis
 Pleural fluid analysis Dr Akash Verma Senior Consultant- Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital, Singapore 308433 Adj A/Professor- Lee Kong Chian School of Medicine
Pleural fluid analysis Dr Akash Verma Senior Consultant- Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital, Singapore 308433 Adj A/Professor- Lee Kong Chian School of Medicine
Pleural Effusion. Exudative pleural effusion - Involve an increase in capillary permeability and impaired pleural fluid resorption
 Pleural Effusion Definition of pleural effusion Accumulation of fluid between the pleural layers Epidemiology of pleural effusion Estimated prevalence of pleural effusion is 320 cases per 100,000 people
Pleural Effusion Definition of pleural effusion Accumulation of fluid between the pleural layers Epidemiology of pleural effusion Estimated prevalence of pleural effusion is 320 cases per 100,000 people
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
PLEURAL DISEASES. (Pleural effusion & empyema) Menaldi Rasmin
 Menaldi Rasmin") PLEURAL DISEASES (Pleural effusion & empyema) Menaldi Rasmin Department of Pulmonology & Respiratory Medicine Faculty of Medicine, University of Indonesia Introduction Pleural effusion is the most common
PLEURAL DISEASES (Pleural effusion & empyema) Menaldi Rasmin Department of Pulmonology & Respiratory Medicine Faculty of Medicine, University of Indonesia Introduction Pleural effusion is the most common
Manejo Práctico del Derrame Pleural
 Manejo Práctico del Derrame Pleural San José, Costa Rica Junio 29, 2017 Rodrigo Cartín Ceba, MD, MSc Consultant, Pulmonary and Critical Care Medicine Associate Professor of Medicine Mayo Clinic 2010 MFMER
Manejo Práctico del Derrame Pleural San José, Costa Rica Junio 29, 2017 Rodrigo Cartín Ceba, MD, MSc Consultant, Pulmonary and Critical Care Medicine Associate Professor of Medicine Mayo Clinic 2010 MFMER
Bacterial pneumonia with associated pleural empyema pleural effusion
 EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
GUIDELINES FOR DIAGNOSIS OF UNILATERAL PLEURAL EFFUSION. Pakistan Chest Society
 GUIDELINES FOR DIAGNOSIS OF UNILATERAL PLEURAL EFFUSION Pakistan Chest Society Message by chairman guideline committee Guidelines for pleural disease working group Expert review committee INTRODUCTION
GUIDELINES FOR DIAGNOSIS OF UNILATERAL PLEURAL EFFUSION Pakistan Chest Society Message by chairman guideline committee Guidelines for pleural disease working group Expert review committee INTRODUCTION
Pleural Effusions. Kyle J Henry, MD Pulmonary/ CCM Fellow PGY4 (210) (602)
 (602)") Pleural Effusions Kyle J Henry, MD Pulmonary/ CCM Fellow PGY4 (210) 275 8583 (602) 202 0351 None Disclosures Objectives Understand the presentation of a pleural effusion How to diagnose and treat Differentiate
Pleural Effusions Kyle J Henry, MD Pulmonary/ CCM Fellow PGY4 (210) 275 8583 (602) 202 0351 None Disclosures Objectives Understand the presentation of a pleural effusion How to diagnose and treat Differentiate
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
APPROACH TO PLEURAL EFFUSIONS. Raed Alalawi, MD, FCCP
 APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
Pleural Disease. Disclosure. Normal Pleural Anatomy. Outline. Pleural Fluid Origins: Transudates. Pleural Fluid Origins: Exudates
 Disclosure Pleural Disease Anne L Fuhlbrigge MD MS Clinical Director Division of Pulmonary and Critical Care Medicine Brigham and Women s Hospital Channing Laboratory Harvard Medical School Boston, MA
Disclosure Pleural Disease Anne L Fuhlbrigge MD MS Clinical Director Division of Pulmonary and Critical Care Medicine Brigham and Women s Hospital Channing Laboratory Harvard Medical School Boston, MA
Chapter 16. Lung Abscess. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Asthma. - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness.
 Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Exam 2 Respiratory Disorders
 Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Pleural Fluid Analysis: Back to Basics
 Pleural Fluid Analysis: Back to Basics Tonya L. Page, MSN, RN, ACNP-BC Patrick A. Laird, DNP, RN, ACNP-BC 70 y/o female with complaints of shortness of breath and orthopnea for 1 month. Symptoms have worsened
Pleural Fluid Analysis: Back to Basics Tonya L. Page, MSN, RN, ACNP-BC Patrick A. Laird, DNP, RN, ACNP-BC 70 y/o female with complaints of shortness of breath and orthopnea for 1 month. Symptoms have worsened
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Malignant Effusions. Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital
 Malignant Effusions Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital Malignant Effusions Definition: Presence of malignant cells in the pleural space 75% are caused by
Malignant Effusions Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital Malignant Effusions Definition: Presence of malignant cells in the pleural space 75% are caused by
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Anatomy. The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs.
 Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
Key Difference - Pleural Effusion vs Pneumonia
 Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Respiratory Medicine
 Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
PLEURAL EFFUSION: DIAGNOSIS, MANAGEMENT AND DISPOSAL
 PLEURAL EFFUSION: DIAGNOSIS, MANAGEMENT AND DISPOSAL 1. This replaces the DGAFMS Medical Memorandum No.63 on Primary (Idiopathic) Pleural Effusion, which dealt with tubercular pleural effusion. 2. Normally
PLEURAL EFFUSION: DIAGNOSIS, MANAGEMENT AND DISPOSAL 1. This replaces the DGAFMS Medical Memorandum No.63 on Primary (Idiopathic) Pleural Effusion, which dealt with tubercular pleural effusion. 2. Normally
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Pneumonia, Pleurisy, Lung cancer
 Pneumonia, Pleurisy, Lung cancer Pneumonia is an infection of lung parenchyma, which leads to inflammation and exudates filling air spaces with fluid (consolidation). This leads to reduced lung compliance
Pneumonia, Pleurisy, Lung cancer Pneumonia is an infection of lung parenchyma, which leads to inflammation and exudates filling air spaces with fluid (consolidation). This leads to reduced lung compliance
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c)
 Diffuse bronchiectasis b) Cystic fibrosis c)") Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Serous fluids. Dr. Mohamed Saad Daoud
 Serous fluids 1 Reference Books: Urinanalysis and body fluids (Susan King Strasinger- Marjorie Schaub De Lorenzo) Fifth edition 2 The closed cavities of the body namely, the pleural, pericardial, and peritoneal
Serous fluids 1 Reference Books: Urinanalysis and body fluids (Susan King Strasinger- Marjorie Schaub De Lorenzo) Fifth edition 2 The closed cavities of the body namely, the pleural, pericardial, and peritoneal
WF RESPIRATORY SYSTEM. RESPIRATORY MEDICINE
 WF RESPIRATORY SYSTEM. RESPIRATORY MEDICINE 1 Societies 11 History 13 Dictionaries. Encyclopaedias. Bibliographies Use for general works only. Classify with specific aspect where possible 15 Classification.
WF RESPIRATORY SYSTEM. RESPIRATORY MEDICINE 1 Societies 11 History 13 Dictionaries. Encyclopaedias. Bibliographies Use for general works only. Classify with specific aspect where possible 15 Classification.
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
Diagnostic Approach to Pleural Effusion
 Original Article GCSMC J Med Sci Vol (IV) No (I) January-June 2015 Diagnostic Approach to Pleural Effusion Rushi Patel*, Viral Shah*, Deepali Kamdar** Abstract : Aim : Normally the pleural cavities contain
Original Article GCSMC J Med Sci Vol (IV) No (I) January-June 2015 Diagnostic Approach to Pleural Effusion Rushi Patel*, Viral Shah*, Deepali Kamdar** Abstract : Aim : Normally the pleural cavities contain
Teacher s Guide. Slide 2. Slide 3. Slide 4. Slide 5
 Teacher s Guide Slide 2 1. Before clicking on the slide, ask learners if they have heard of this concept before 2. If yes, explore what this term means to them and solicit examples 3. Click slide to reveal
Teacher s Guide Slide 2 1. Before clicking on the slide, ask learners if they have heard of this concept before 2. If yes, explore what this term means to them and solicit examples 3. Click slide to reveal
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
CLINICAL PRACTICE. Clinical Practice
 Clinical Practice This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines,
Clinical Practice This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines,
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Focus on Cystic Fibrosis. Cystic Fibrosis. Cystic Fibrosis
 Focus on (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Autosomal recessive, multisystem
Focus on (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Autosomal recessive, multisystem
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Pneumothorax lecture no. 3
 Pneumothorax lecture no. 3 Is accumulation of air in a pleural space or accumulation of extra pulmonary air within the chest, Is uncommon during childhood, may result from external trauma, iatrogenic,
Pneumothorax lecture no. 3 Is accumulation of air in a pleural space or accumulation of extra pulmonary air within the chest, Is uncommon during childhood, may result from external trauma, iatrogenic,
Lecture 3. Inflammatory Processes
 Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Diseases of the Lung and Respiratory Tract, Part I. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Pleural fluid. creatinine - urinothorax haematocrit -haemothorax bilirubin gut perforation. Fluid samples 1st Plain Universal ( cell count)
") Examination Purpose of test Sample 17725 Fluid Profile (appearance, culture, WBC differential, ph, total protein, glucose, amylase, triglyceride, albumin, HDL) Peritoneal/ascitic and pleural fluid are
Examination Purpose of test Sample 17725 Fluid Profile (appearance, culture, WBC differential, ph, total protein, glucose, amylase, triglyceride, albumin, HDL) Peritoneal/ascitic and pleural fluid are
Respiratory Pathophysiology
 Respiratory Pathophysiology Objectives: Respiratory infections and lung cancer. Pleural effusion & edema, pleuritis, pneumothorax and atelectasis. Obstructive airway disease and chronic interstitial lung
Respiratory Pathophysiology Objectives: Respiratory infections and lung cancer. Pleural effusion & edema, pleuritis, pneumothorax and atelectasis. Obstructive airway disease and chronic interstitial lung
Causes of pleural effusion and its imaging approach in pediatrics. M. Mearadji International Foundation for Pediatric Imaging Aid
 Causes of pleural effusion and its imaging approach in pediatrics M. Mearadji International Foundation for Pediatric Imaging Aid Pleural fluid A tiny amount of fluid in the pleural cavity is physiological.
Causes of pleural effusion and its imaging approach in pediatrics M. Mearadji International Foundation for Pediatric Imaging Aid Pleural fluid A tiny amount of fluid in the pleural cavity is physiological.
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Imaging of Pleural Effusion: Comparing Ultrasound, X-Ray and CT findings
 Imaging of Pleural Effusion: Comparing Ultrasound, X-Ray and CT findings Poster No.: C-2067 Congress: ECR 2017 Type: Educational Exhibit Authors: J. M. Almeida, N. Antunes, C. Leal, L. Figueiredo ; Lisboa/PT,
Imaging of Pleural Effusion: Comparing Ultrasound, X-Ray and CT findings Poster No.: C-2067 Congress: ECR 2017 Type: Educational Exhibit Authors: J. M. Almeida, N. Antunes, C. Leal, L. Figueiredo ; Lisboa/PT,
100 Chest X Rays for Study Group. by Dr. Suneet Khurana
 100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis?
. What is the diagnosis?") 1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
February 1, 2016 Body Fluid order changes
 February 1, 2016 Body order changes Laboratory will be making the following changes to Body tests: 1. Changing orders in Power plans (see below list). 2. All folders will be updated accordingly: If the
February 1, 2016 Body order changes Laboratory will be making the following changes to Body tests: 1. Changing orders in Power plans (see below list). 2. All folders will be updated accordingly: If the
Respiratory diseases in Ostrołęka County
 Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis?
 ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 12 Number 1 Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis? A Huaringa, S Malek, M Haro, L Tapia Citation A Huaringa, S Malek, M
ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 12 Number 1 Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis? A Huaringa, S Malek, M Haro, L Tapia Citation A Huaringa, S Malek, M
Disease spectrum. IPA Invasive pulmonary aspergillosis
 Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Pleural Effusions. Introduction. Causes of Pleural Effusion. imedpub Journals
 Short Communication imedpub Journals http://www.imedpub.com/ Vol. 3 No. 1:1 Pleural Effusions Received: January 15, ; Accepted: January 22, ; Published: February 05, Funda Ozturk Incekara*, Deniz Kaygusuz
Short Communication imedpub Journals http://www.imedpub.com/ Vol. 3 No. 1:1 Pleural Effusions Received: January 15, ; Accepted: January 22, ; Published: February 05, Funda Ozturk Incekara*, Deniz Kaygusuz
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
*according to content of fluid we can divide pleural effusion to 2 main types
 Pleural lesion and lesion of the Done by: Upper respiratory tract Saef Bassam ma'adat **Lets start with pleural lesion there is a little differet between pleural effustion and empyema accumulation of fluid
Pleural lesion and lesion of the Done by: Upper respiratory tract Saef Bassam ma'adat **Lets start with pleural lesion there is a little differet between pleural effustion and empyema accumulation of fluid
Care of the Patient with a Respiratory Disorder
 Care of the Patient with a Respiratory Disorder 1 Slide 1 Overview of Anatomy and Physiology External respiration Exchange of oxygen and carbon dioxide between the lung and the environment Internal respiration
Care of the Patient with a Respiratory Disorder 1 Slide 1 Overview of Anatomy and Physiology External respiration Exchange of oxygen and carbon dioxide between the lung and the environment Internal respiration
REFERRAL GUIDELINES RESPIRATORY
 REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
Complicated echinococcal cyst to Biopsy or not to biopsy. V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center
 Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Undergraduate Teaching
 Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Pathogenesis of pulmonary symptoms Dr. Rehab F. Gwada
 Pathogenesis of pulmonary symptoms Dr. Rehab F. Gwada Objectives of the lectures Identify main symptoms of pulmonary diseases & their pathogeneses Outline the graded of dyspnea Differentiate between bronchial
Pathogenesis of pulmonary symptoms Dr. Rehab F. Gwada Objectives of the lectures Identify main symptoms of pulmonary diseases & their pathogeneses Outline the graded of dyspnea Differentiate between bronchial
Surgical treatment of empyema in children
 Surgical treatment of empyema in children Jacques Janson Pierre Goussard Cardiothoracic Surgery, Paediatric Pulmonology Tygerberg Academic Hospital University of Stellenbosch Pleural space Netter, Frank
Surgical treatment of empyema in children Jacques Janson Pierre Goussard Cardiothoracic Surgery, Paediatric Pulmonology Tygerberg Academic Hospital University of Stellenbosch Pleural space Netter, Frank
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
EVALUATE DATA IN THE PATIENT RECORD
 EVALUATE DATA IN THE PATIENT RECORD Shawna Strickland, PhD, RRT-NPS, AE-C, FAARC Objectives At the end of this module, the learner will be able to identify the pertinent data from the patient chart for
EVALUATE DATA IN THE PATIENT RECORD Shawna Strickland, PhD, RRT-NPS, AE-C, FAARC Objectives At the end of this module, the learner will be able to identify the pertinent data from the patient chart for
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days
 1 week b) 24 days") Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide
The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress THE LAST GASP II: LUNGS AND THORAX David Holt, BVSc, Diplomate ACVS University of Pennsylvania School of Veterinary
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress THE LAST GASP II: LUNGS AND THORAX David Holt, BVSc, Diplomate ACVS University of Pennsylvania School of Veterinary
PROPAEDEUTICS OF INTERNAL DISEASES EXAMINATION SYLLABUS. Part I - General
 PROPAEDEUTICS OF INTERNAL DISEASES EXAMINATION SYLLABUS Part I - General 1. History taking plan of history taking, sections, questions. 2. History taking - rules. 3. Current state of health - study plan.
PROPAEDEUTICS OF INTERNAL DISEASES EXAMINATION SYLLABUS Part I - General 1. History taking plan of history taking, sections, questions. 2. History taking - rules. 3. Current state of health - study plan.
Introduction to Radiology for TB Nurses
 Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area