Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #4 - Thursday, July 06, 2017
|
|
|
- Loraine Watts
- 5 years ago
- Views:
Transcription


1 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #4 - Thursday, July 06, 2017
2 Welcome and Introductions Today s objectives: 1. Tier 3: Implementation of the Sepsis Bundles 2. Addressing barriers to implementation 3. Stopping Sepsis Project Updates 4. Next steps 2







3 Your Sepsis Support Team Deborah Smith MLT(ASCP), BSN, CIC, CPHQ Improvement Consultant Candy Hamner RN, BA, MA Improvement Consultant Betsy Cole Archer, MS, ASCP Sr. Director, Performance Improvement Wanda Clevenger BSN, RN, MBA Director, Performance Improvement Kathleen Vollman, MSN,RN, CCNS, FCCM, FAAN Sepsis Content Expert 3

4 Sepsis Practice Collaborative Model Tier 3: Implementation of the Sepsis Bundles Kathleen M. Vollman RN, MSN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING LLC Sepsis Solutions International LLC Northville, Michigan 4 Sepsissolutionsinternational LLC 2017
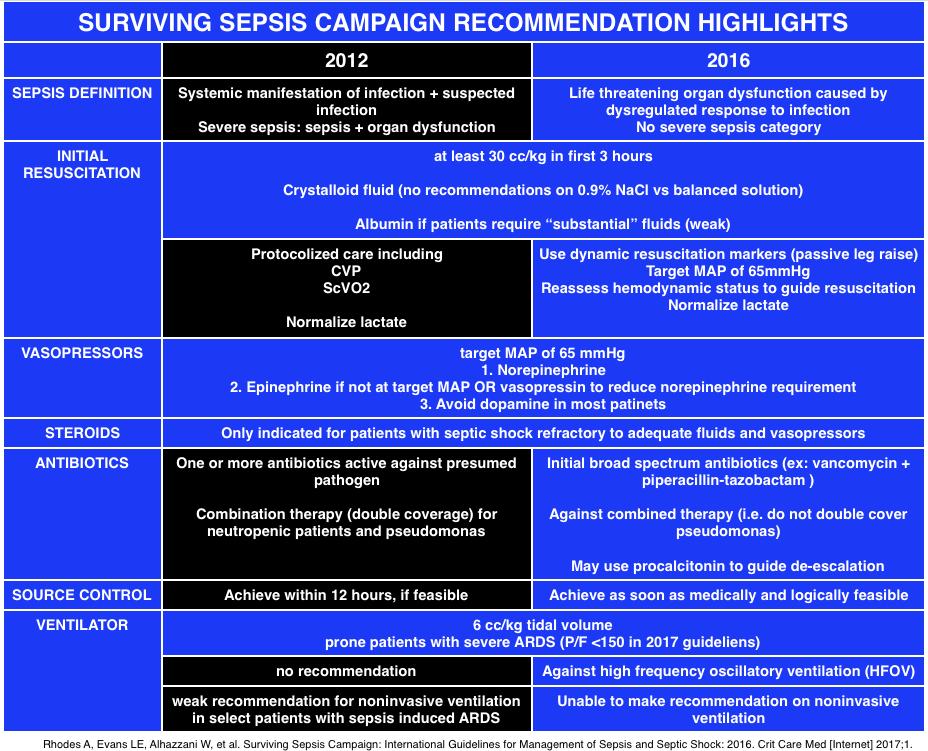
5 2016 SURVIVING SEPSIS GUIDELINES BEST PRACTICE STATEMENT SEPSIS (SEVERE SEPSIS) AND SEPTIC SHOCK ARE MEDICAL EMERGENCIES, AND WE RECOMMEND THAT TREATMENT AND RESUSCITATION BEGIN IMMEDIATELY Rhodes A, Evans LE et.al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2016 CCM Mar 2017
6 Components of TIER III Milestones and checklist Understand current process for caring for septic shock patients Go and See work Baseline data Order sets Common Barriers/Issues: identified Gaps from Go and See work Educational plan Implementation plan Unit champions Prospective rounding Independent checks
7
8 SEP-1 TO BE COMPLETED WITHIN 3 HOURS OF TIME OF PRESENTATION : 1. Measure lactate level 2. Obtain blood cultures prior to administration of antibiotics 3. Administer broad spectrum antibiotics 4. Administer 30ml/kg crystalloid for hypotension or lactate 4mmol/L time of presentation is defined as the time of earliest chart annotation consistent with all elements severe sepsis or septic shock ascertained through chart review.
9 Time Zero a. Will always be when the chart annotation suggests signs and symptoms are all present. b. May be from nursing charting/screens, lab flow sheets, physician documentation, order sets, anything with a time stamp. c. Will = triage time if all signs and symptoms are present at triage. d. It does not require MD documentation of the clock starting; relying on this alone in the ED would likely result in late clock starts. Sepsis coding is increasing and is accurate. More aggressive treatment seen from 2003 to 2013 Law A & Klompas M, Infect Control & Hosp Epid, 2015 Slides courtesy of Sean Townsend
10 SEP-1 TO BE COMPLETED WITHIN 6 HOURS OF TIME OF PRESENTATION: 5. Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation) to maintain a mean arterial pressure (MAP) 65mmHg 6. In the event of persistent hypotension after initial fluid administration (MAP < 65 mm Hg) or if initial lactate was 4 mmol/l, re-assess volume status and tissue perfusion and document findings according to table Re-measure lactate if initial lactate elevated.
11 SEP-1 TABLE 1: DOCUMENT REASSESSMENT OF VOLUME STATUS AND TISSUE PERFUSION: Repeat focused exam(after initial fluid resuscitation) by licensed independent practitioner including vital signs, cardiopulmonary, capillary refill, pulse and skin findings. Or Document Two of the following: Measure CVP Measure ScvO2 Bedside cardiovascular ultrasound Dynamic assessment of fluid responsiveness with passive leg raise or fluid challenge



12 Audience Polling Question 1 What do you feel is the biggest challenge with the 3 hour bundle? Obtaining lactic acid Obtaining blood cultures Obtaining blood cultures prior to antibiotics Giving antibiotics Giving the 30ml/kg fluid bolus




13 Audience Polling Question 2 What is your biggest challenge with the 6 hour bundle? Obtaining the repeat lactate Administering the vasopressor for persistent hypotension The physical reassessment The 2/4 options (ScvO2, CVP, PLR, ultrasound)
14 STUDIES SUPPORTING THE 3 AND 6 HOUR BUNDLES
15 Serum Lactate is Associated with Sepsis Mortality Objective: Design: a. Test whether the association between initial serum lactate level and mortality in patients presenting to the ED with severe sepsis is independent of organ dysfunction and shock a. Retrospective, single center cohort study b. Academic teaching hospital Patients: a. 830 adults admitted with severe sepsis in the ED b. Stratified lactate into 3 groups: low (<2), intermediate (2-3.9) and high (> or equal to 4) Mikkelsen, Mark et al CCM 2009 Vol 37 No 5

16 Serum Lactate is Associated with Sepsis Mortality Results: Intermediate and high serum lactate significantly associated with mortality regardless of the presence of shock or other organ dysfunction A single serum lactate seems to risk-stratify patients independent of organ dysfunction or hemodynamic instability Mikkelsen, Mark et al CCM 2009 Vol 37 No 5

17 Initiation of Inappropriate Antimicrobial Therapy Results in a Fivefold Reduction of Survival in Human Septic Shock a. Objective: determine the impact of the initiation of inappropriate antimicrobial therapy on survival to hospital discharge of patients with septic shock b. Retrospective review of 5,715 patients from 22 different hospitals in Canada, US and Saudi Arabia c. Data collected from Kumar A. et al. Chest, 2009; 136;
18 Initiation of Inappropriate Antimicrobial Therapy Result in a 5-Fold Reduction of Survival in Human Septic Shock 5,715 patients in septic shock in three countries 55% of cases were from community acquired infection Decrease in survival with inappropriate initial antibiotics was fivefold Kumar A. et al. Chest, 2009; 136;

19 Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock *2,154 septic shock patients *Effective antimicrobial administration within the 1 st hour of documented hypotension was associated with increased survival in patients with septic shock. CCM 2006 Vol. 34 No.6 *Each hour of delay over the next 6 hours was associated with an average decrease in survival of 7.6% (range %)
20 Mortality by Time to Antibiotics Severe Sepsis: SSC Database 5% Increase in Mortality for Every Hour Delayed Time to Abx HOURS OR CI CI P value Prob of Death CI CI < < < < < < Surviving Sepsis Campaign: Association Between Performance Metrics and Outcomes in a 7.5-Year Study Levy, M etal CCM 2015
21 Mortality by Time to Antibiotics Septic Shock: SSC Database 5% Increase in Mortality for Every Hour Delayed Time to Abx HOURS OR CI CI P Value Prob of Death < < < < < < CI CI Surviving Sepsis Campaign: Association Between Performance Metrics and Outcomes in a 7.5-Year Study Levy, M etal CCM 2015
22 Early Goal Directed Therapy Methodology: 263 severe sepsis patients a.early Goal-Directed Therapy (EGDT) Continuous ScvO2 monitoring & tx with fluids, blood, inotropes &/or vasoactives to maintain: ScvO2 >70%, SaO2 > 93%, Hct > 30%, CI/VO2 CVP > 8-12 MAP > 65 UO >.5ml/kg/hr a.standard Therapy CVP > 8-12 MAP > 65 UO >.5ml/kg/hr Rivers et. al. N Engl J Med. 2001;345;19:
23 Early Goal-Directed Therapy Results % Standard Therapy n= day Mortality P = 0.01* 33.3% EGDT n=130 NNT = 7-8 *Key difference was in sudden CV collapse, not MODS Rivers et. al. N Engl J Med. 2001;345;19:
24 The Changing Paradigm of Septic Shock Management a. ProCESS trial-randomized, 31 centers, 1341 patients b. ARISE trial- randomized, 51 centers(mostly Australia and New Zealand), 1600 patients c. Promise randomized, UK, 56 centers, 1260 patients

25

26 Society of Critical Care Medicine
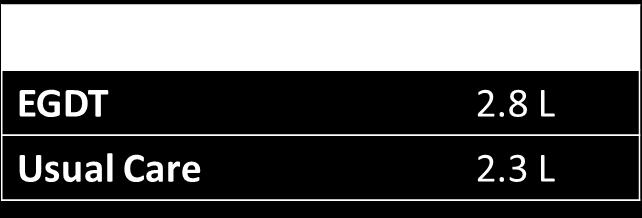
27 Results of 3 International Studies a. ARISE and Promise had two groups: EGDT and Usual care b. ProCess had three groups: EGDT, structured resuscitation and usual care c. Before randomization all patients received antibiotics and an average of 2500ml of NS (equal to 30ml/kg), had blood cultures and lactate drawn d. No statistically significant difference in mortality between groups (control and protocol) e. Mortality rate 18% for ARISE & ProCess f. Mortality rate 30% for Promise ProCESS Investigators, 2014; 370: ARISE Investigators et al. N Engl J Med 2014; 371: Mouncey PR, et al. N Engl J of Med, 2015; 372:
28 Common Barriers/Issues a. Timely antibiotics b. Fluid bolus (30ml/kg) c. Repeat focus exam
29 Antibiotics Appropriate initial antibiotics Guide for providers recommending the appropriate antibiotic based on whether hospital or community acquired, source and your hospital s antibiogram Turnaround time---from indication to hanging ED vs ICU vs Floor Understand your current process and the gaps Make antibiotics rapidly available Factors that showed delay of administration Higher APACHE, older, presence of co-morbidities, HLOS before hypotension, dx of pneumonia, admin to academic hospitals & transfer from medical wards Amaral ACKB, et al. Crit Care Med;2016;44:
30 Fluid Bolus - Considerations How fast should they be given? Gravity or pressure bag not by infusion pump What about dialysis patients? What about patients with CHF or low EF? Fluid bolus is given rapidly, IV wide open, pressure bag if necessary; goal is 500ml every minutes

31 Fact a. One liter of normal saline adds 275 ml to the patient s plasma volume Slides courtesy of Sean Townsend
32 Heart Failure Going to Flood My Patient a. Not Based in Evidence b. Rivers et al Study: % Ventilated Patients Chronic coexisting conditions-chf: Control 30.2% EGDT 36.7% Rivers E, et al. N Engl J Med 2001;345:
, Mean initial lactate level was 2.8 mmol/l. 86% received intravenous antibiotics within 180 min. 64% had intravenous fluid initiated within 30 min.")
33 Impact of Early Fluid & Amount Prospective, observational cohort of all ED severe sepsis or septic shock patients during 13 months 90,000 average ER visits 1,866 subjects; 53.6% were men, 72.5% were white, mean age was 72 years (SD 16.6 years), Mean initial lactate level was 2.8 mmol/l. 86% received intravenous antibiotics within 180 min. 64% had intravenous fluid initiated within 30 min. Leismean D, et al. Annals of Emerg Med,2015;66(4):S149
34 Impact of Early Fluid and Amount Results Mortality in 30 minutes group (159 [13.3%] versus 123 [18.3%]) Median hospital length of stay (6 days versus 7 days) Adjustment for age, lactate, hypotension, acute organ dysfunction, and Emergency Severity Index score, intravenous fluid within 30 minutes was associated with lower mortality Mortality with later fluid administration 13.3% (30 minutes) versus 16.0% (31 to 60 minutes) versus 16.9% (61 to 180 minutes) versus 19.7% (>180 minutes) Leismean D, et al. Annals of Emerg Med,2015;66(4):S149
35 Clinical Scenario w/questions 80yr old w/chf and ESRD arrives at ED w/severe sepsis and a MAP of 55 a. Receives 1.5 liter (15ml/kg) and his MAP increases to 70 & never drops again. No more fluids are given. b.his Lactate is 1.0-pt would fail the measure because didn t get 30/ml/kg response Clinician s questions: a. Is that correct? b. If it is correct why? I assume you would agree with me that giving such a patient another 1.5/L has strong possibility of more harm than benefit c. If you agree with me that more fluid is not indicated-reviewers would score that as a fall out d. If 3 is correct-do you still try to convince physicians to give entire 30/ml/kg-if so what evidence to support?
36 Dr. Townsend s Response 4 major trials on shock patients, each of the new trials found the patients received an average of 30/ml/kg There is no trial specific to your patient-but trials have averages and patient characteristics CHF & renal failure-no evidence exists that mortality increases if they received the 30 ml/kg Rivers trial-chf with more fluids & EGDT had less mechanical ventilation Not an absolutist-he tells peoples do what you think is clinically correct The long and short is 30ml/kg is evidence based average. People should deviate from the average if they have strong clinical doubts and accept the failure. If you are falling out all the time something is wrong
37 Why Do All Severe Sepsis Patients Need Volume? a. Vascular volume is lost into interstitial space do to diffuse capillary leaking from cytokine release b. Both venous and arteriolar tone is reduced & blood volume occupies a larger intravascular space than normal c. Many patients also have GI and Skin losses d. Only 40% of NS stays intravascular the rest goes into the interstitial space. An initial BP response is not an indication to not give full bolus Large trial before and after bundle implementation for patients with intermediate lactate values >2 < 4. in hospital mortality in the bundle implementation group was observed in the patient with CHF and kidney disease compared with patients without Received more fluid with the bundle approach Liy VX, et al Am J of Respir and Crit Care Med, 2016;193:
38 Application of Fluid Resuscitation in Adult Septic Shock User s Guide to the 2016 Surviving Sepsis Guidelines Dellinger, CCM published ahead of print
39 Reassessment for Volume Status and Perfusion Team decides how to support all options in table 1 Focused exam templated notes? Specific form? Making sure it is done between, after fluid bolus and before 6 hours Do you have all the correct equipment and tools and training for: CVP (IJ, Subclav or femoral) ScvO2 (intermittent vs continuous) Bedside cardiovascular ultrasound Dynamic assessment of fluid responsiveness with passive leg raise or fluid challenge (must be able to monitor CI, SV pulse contour technology, non-invasive or PA catheter,)

40 Optimize Cardiac Performance Fluid Bolus to define place on curve: Record SV Give NS bolus over 15minutes Record SV If see greater than a10% increase in SV pt is on steep portion of curve and will still respond to fluid (fluid responsive)

41 Algorithm for Stroke Volume Optimization Johnson, A. Ahrens, T. Critical Care Nurse 2015; 35(1) 11-28
42 Monnet X, et al. Intensive Care Med, 2016;42: Passive Leg Raise Meta-analysis of 21 studies of 991 patients whom 995 fluid challenges were performed, found changes in cardiac output induced by a passive leg raise test highly reliable in predicting fluid responsiveness Sensitivity of.85 & Specificity.91
43 If Using CVP and ScvO2 Provider confidence/competency in placing central lines Defined who will place central line when pt has lactate>4mmol/l or still hypotensive after initial fluid bolus ED or ICU? What happens on off shifts and weekends? Adequate equipment in ED/ICU to insert and monitor CVP Educate nurses in ED/ICU on hemodynamic monitoring and ScvO2 Is there sufficient nursing staff to handle the acuity and intensity of these patients in the ED? Why do I need a CVP? Research shows that CVPs don t accurately reflect volume status.
44 Focused Examination a. Vital Signs a. Temp, HR, BP, RR b. Cardiopulmonary a. Rhythm, S1/2/3/4, presence of murmur and lung sounds c. Peripheral Pulses a. 1+, 2+ or absent d. Capillary Refill a. Brisk, <2 sec, >2 sec e. Skin a. Mottled vs no mottling, to what level. Warm vs cold, etc Study compared physical findings of ineffective circulation (cap refill >2, skin mottling and cool extremities) to PA catheter- Physical findings not useful predictor of low cardiac index or low mixed venous Grissom CK, et al. Crit Care Med, 2009;37:
45 CMS Documentation Change a. Documentation indicating a physician/apn/pa has performed, or attested to performing a physical examination, perfusion (re-perfusion) assessment, or sepsis (severe sepsis or septic shock) focused exam is acceptable. If documented this this way, reference to skin color, appearance, or condition is not required. Specifications Manual for National Hospital Inpatient Quality Measures Discharges (1Q17) through (4Q17) Version 5.2
46

47 Sepsis Checklist

48 HRET Sepsis Mortality Reduction: 2017 Update Health Research & Educational Trust (2017, February). Sepsis and Septic Shock Change Package: Chicago, IL: Health Research & Educational Trust. Accessed at 48
49 Sepsis Program Action Plan Item Responsibility Due Date Status 1. Assemble team 2. Identify executive sponsor 3. Educate team on evidence 4. Project Charter 5. Baseline data 6. Define screening tool and process for ED, ICU, Floor, RRT 7. Define screening audit process 8. Develop triggers/processes to alert staff when time to move from first 3 hrs to shock bundle 9. Develop & implement an educational plan for all staff: 10. Develop an implementation plan 11. Data measurement & feedback
50 Stopping Sepsis Project Updates BOX Folders: Remember to update your Self Reported Sepsis Process Measure Data Template Sepsis Outcome Measure Data for CY2016 available Health Systems have consolidated Outcome Measure reports 50

51 All Sepsis Mortality Data Source: CMS Part A Claims for Medicare FFS Beneficiaries, Qtrs. 1 to

52 Severe Sepsis/Septic Shock Mortality Data Source: CMS Part A Claims for Medicare FFS Beneficiaries, Qtrs. 1 to

53 Sepsis on Admission Data Source: CMS Part A Claims for Medicare FFS Beneficiaries, Qtrs. 1 to

54 % of Sepsis Discharges Readmitted w/in 30 Days Data Source: CMS Part A Claims for Medicare FFS Beneficiaries, Qtrs. 1 to
55 Project Updates Cont. Hospital Site Visits 52% of participating hospitals visited Contact or go to Stopping Sepsis Site Visit Dates Look for information soon on upcoming cross setting regional meetings. 55
56 56 Upcoming Stopping Sepsis Webinars
57 Contact Information Wanda Clevenger Director, Performance Improvement (804) Kathleen Vollman Clinical Nurse Specialist/Consultant 57
58 Set Up Your BOX Accounts BOX is a SECURE file replaces encryption You received invitation with a link from Sarah Helen or Deb Smith ACT immediately this invite expires in 7 days Detailed instructions with screen shots from Deb Smith or Wanda Clevenger Linda Harris will be resending invites every 7 days 58
59 Where do you go for BOX HELP Trouble accessing BOX Sarah Helen Hospital data report questions
60 Resources Sepsis Mortality Reduction 2017 Update A Users Guide to the 2016 Surviving Sepsis Guidelines: Dellinger, R. Phillip; Schorr, Christa A.; Levy, Mitchell M. Critical Care Medicine. 45(3): , March doi: /CCM Centers for Disease Control 60
61 Q & A This material was prepared by Health Quality Innovators (HQI), the Medicare Quality Innovation Network- Quality Improvement Organization for Maryland and Virginia, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. HQI 11SOW
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
SUCCESS IN SEPSIS MORTALITY REDUCTION. Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar
 SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Inpatient Quality Reporting (IQR) Program
 Program") The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting (IQR)
The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting (IQR)
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Steps to Success in Sepsis ASHNHA Quality Webinar. Maryanne Whitney, RN, CNS, MSN Improvement Advisor, Cynosure Health
 1 Steps to Success in Sepsis ASHNHA Quality Webinar Maryanne Whitney, RN, CNS, MSN Improvement Advisor, Cynosure Health Goals for Today State the Problem: Create Awareness & Will Unravel the mysteries
1 Steps to Success in Sepsis ASHNHA Quality Webinar Maryanne Whitney, RN, CNS, MSN Improvement Advisor, Cynosure Health Goals for Today State the Problem: Create Awareness & Will Unravel the mysteries
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
Overview. Hosted by Nicole Kenny, Virox Technologies Inc Overview. Severe Sepsis: A Significant Healthcare Challenge
 Severe Sepsis: Early Recognition and Management Saves Lives SepsisSolutionsInternational 2013 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant Sepsis Solutions
Severe Sepsis: Early Recognition and Management Saves Lives SepsisSolutionsInternational 2013 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant Sepsis Solutions
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
SEP-1 CHALLENGING CASES WITH DR. TOWNSEND
 UW MEDICINE PATIENTS ARE FIRST SEP-1 CHALLENGING CASES WITH DR. TOWNSEND AMADAE AREVALO RN, MSN, CCRN KATIE MEHRING RN, BSN, CCDS AMANDA SIGALA, RN, BSN, MPH, CPHQ JUNE 12, 2018 OBJECTIVES 1. Summarize
UW MEDICINE PATIENTS ARE FIRST SEP-1 CHALLENGING CASES WITH DR. TOWNSEND AMADAE AREVALO RN, MSN, CCRN KATIE MEHRING RN, BSN, CCDS AMANDA SIGALA, RN, BSN, MPH, CPHQ JUNE 12, 2018 OBJECTIVES 1. Summarize
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Sepsis: Getting to ZERO Probable or Impossible?
 Sepsis: Getting to ZERO Probable or Impossible? Carol A Rauen, RN-BC, MS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant. Burn Trauma ICU, Sentara Norfolk General, VA Sepsis
Sepsis: Getting to ZERO Probable or Impossible? Carol A Rauen, RN-BC, MS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant. Burn Trauma ICU, Sentara Norfolk General, VA Sepsis
A Critical Review of Early Goal Directed Therapy and Government Endorsement
 A Critical Review of Early Goal Directed Therapy and Government Endorsement Charles Natanson M.D. Critical Care Medicine Department Clinical Center National Institutes of Health Clinical Center None Conflicts
A Critical Review of Early Goal Directed Therapy and Government Endorsement Charles Natanson M.D. Critical Care Medicine Department Clinical Center National Institutes of Health Clinical Center None Conflicts
Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia
 Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia Early goal-directed therapy in septic shock 2001 Proof-of-concept EGDT trial published NEJM 16%
Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia Early goal-directed therapy in septic shock 2001 Proof-of-concept EGDT trial published NEJM 16%
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Saving Lives: Focusing on Severe Sepsis and Septic Shock
 Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.3a Measure Updates Questions and Answers Speaker Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.3a Measure Updates Questions and Answers Speaker Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.5a Measure FAQs Presentation Transcript Noel Albritton, MSN, RN Lead Solutions Specialist, Hospital Inpatient and Outpatient Process and Structural
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.5a Measure FAQs Presentation Transcript Noel Albritton, MSN, RN Lead Solutions Specialist, Hospital Inpatient and Outpatient Process and Structural
Inpatient Quality Reporting (IQR) Program
 Program") Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
Guidebook for ED and Inpatient Sepsis Order Set Initiatives 2018
 Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
ADVANCING NURSING LLC
 Sepsis 2015: Early Recognition and Management Saves Lives Kathleen M. Vollman RN, MSN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING LLC kvollman@comcast.net Northville,
Sepsis 2015: Early Recognition and Management Saves Lives Kathleen M. Vollman RN, MSN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING LLC kvollman@comcast.net Northville,
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Surviving Sepsis: Early Management Saves Lives
 Surviving Sepsis: Early Management Saves Lives Pat Posa RN, BSN, MSA, CCRN-K, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Ann Arbor, MI patposa07@gmail.com Objectives Understand the incidence
Surviving Sepsis: Early Management Saves Lives Pat Posa RN, BSN, MSA, CCRN-K, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Ann Arbor, MI patposa07@gmail.com Objectives Understand the incidence
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
SEPSIS: GETTING STARTED
 SEPSIS: GETTING STARTED Ohio Sepsis Initiative July 15, 2015 SEPSIS INCIDENCE Definition: the number of severe sepsis or septic shock encounters using the following ICD-9 codes (995.91 Sepsis, 995.92 severe
SEPSIS: GETTING STARTED Ohio Sepsis Initiative July 15, 2015 SEPSIS INCIDENCE Definition: the number of severe sepsis or septic shock encounters using the following ICD-9 codes (995.91 Sepsis, 995.92 severe
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
Sepsis Update: Early Identification and Management
 Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis. Reliability- can we achieve Dr Ron Daniels
 Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Sepsis - A Year in Transition
 Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center
 UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
Rapid Response Teams. January 17, Safe Table Webinar
 Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Surviving Sepsis Campaign update
 Surviving Sepsis Campaign update Christopher W. Seymour, MD MSc Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures Received funding
Surviving Sepsis Campaign update Christopher W. Seymour, MD MSc Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures Received funding
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Looking for sepsis. Sepsis: Update. Prevalence of High Profile Dzs. Screening and risk stratification. Mortality of High Profile Diseases
 Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Jarisch A. Kreislauffragen, Dünser et al. Critical Care 2013, 17:326 Sunday, March 30, 14
 It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2a Commonly Asked Questions & v5.3 Measure Updates Presentation Transcript Moderator Candace Jackson, RN Project Lead Hospital Inpatient Quality
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2a Commonly Asked Questions & v5.3 Measure Updates Presentation Transcript Moderator Candace Jackson, RN Project Lead Hospital Inpatient Quality