The real picture. Prorenin (Renin) PRR AT3 AT4. AT4 receptor. PAI 1 Abassi, Biochem Pharm, 2009
|
|
|
- Brett McBride
- 6 years ago
- Views:
Transcription
 PRR AT3-8")

1 The real picture. Prorenin (Renin) PRR AT3-8 AT4 AT10-12 AT3 AT4 receptor PAI 1 Abassi, Biochem Pharm, 2009
2 Resistant Hypertension; Case based discussion Moving Targets? RAAS blockade in hypertensive CKD Sarah Roxburgh Dialysis Nephrology Transplantation Meeting March 30 th 2011
3 Mr RH, age 72 Referral August 2010 Thanks for seeing regarding his hypertensive management along with associated diabetic/ hypertensive nephropathy
4 Background T2DM; > 30 yr duration Insulin requiring since early 2010 No diabetic retinopathy, mild Sx peripheral neuropathy No macrovascular disease Multiagent Hypertension Hyperlipidaemia Ex smoker C2H5OH, prior excess Family history; father RIP ESKD/ T2DM, age 72
5 Presenting issues Small bowel obstruction June 2010, conservative management Normal upper and lower endoscopies 7 kg weight gain over past year, associated increasing peripheral oedema BPs increasingly labile over past 2 3 months; up to 210/ 95 in GP office
6 Medications at presentation Metoprolol 50 mg bd Prazosin 2.5 mg bd Ramipril 10 mg po mane Lercanidipine 20 mg po nocte Aspirin 100 mg po daily Atorvastatin 20 mg po nocte Lantus bd
7 Physical examination BP 170/90 L and R. HR 56. Weight 87.2 kg, BMI 33, waist circumference 103 cm. JVP 3 cm, small bibasal effusions, pitting peripheral oedema to upper 1/3 calves ABND. HS dual +nil No renal/ epigastric bruit. PPP. Nil carotid or femoral bruit. UA; 3+ protein, trace blood, no leukocytes Reduced reflexes in lower limbs
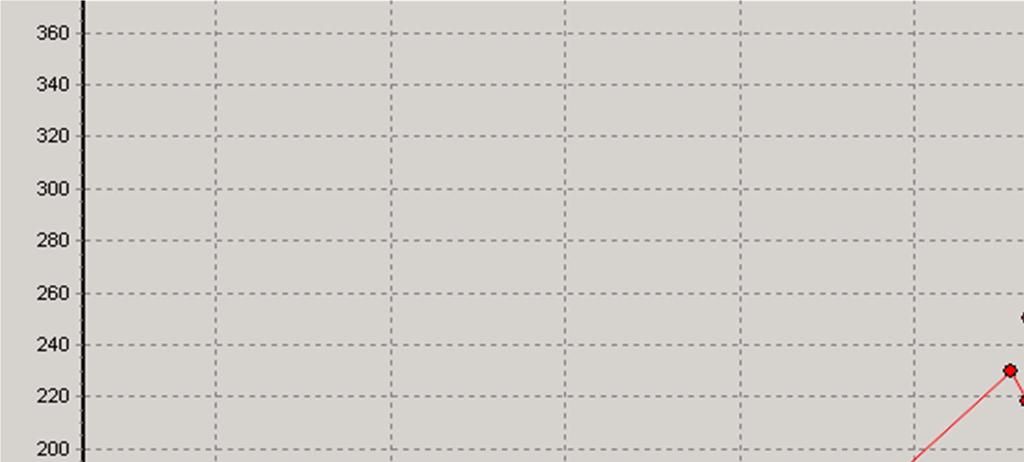
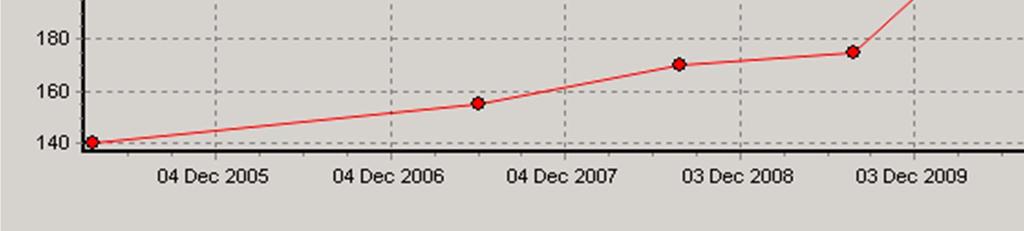
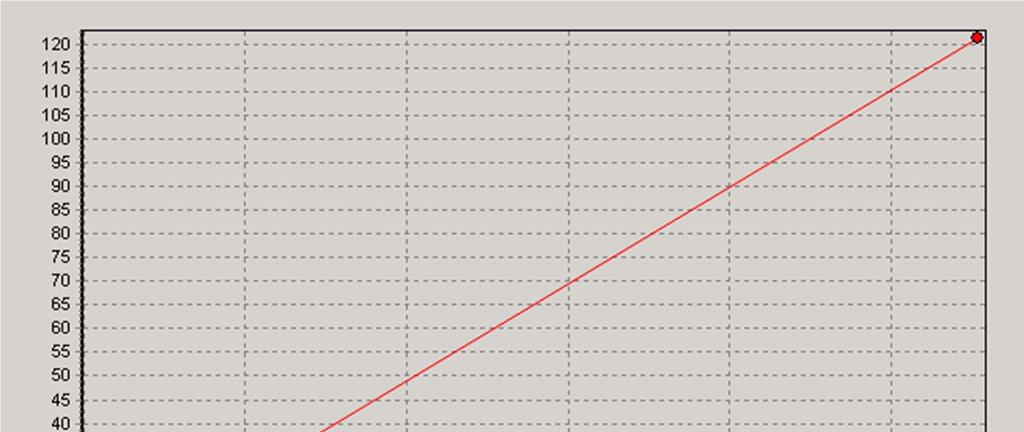
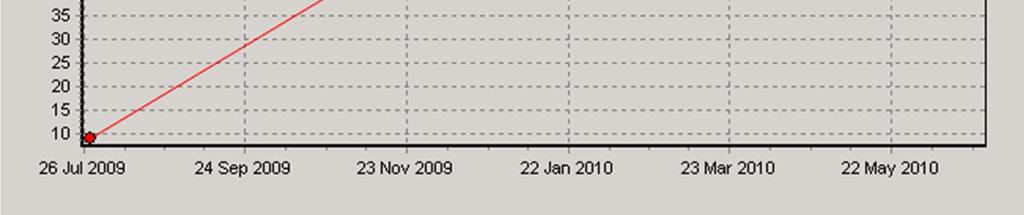
8 Serum creatinine
9 Albuminuria

10 HbA1c
11 Other results Hb 118 NNA. Iron stores; ferritin 96, iron sats 16 % 24 hr urine; 1.9 g total protein, urinary creatinine clearance 28 mls/minute Albumin 41, LFTs normal, PTH 19 pg/l, Corr Ca 2.34, PO4 1.2 Sediment; nil microhaematuria / casts/ other Igs, C3/ C4, ANA, EPG/IEPG all normal/ negative Renal ultrasound; right kidney 11.1 cm, left 12.1 cm suggestion of increased echogenicity and some parenchymal thinning
12 Summary 1. Multiagent hypertension poor control 2. Proteinuric CKD Stage 4 (1.9 g) No biopsy (for now?) Presumed hypertensive small vessel ischaemic nephropathy +/ diabetic glomerulosclerosis +/ secondary FSGS
13 ? Other workup
14 ? Other workup TTE; normal LV function, mild concentric LVH Renal artery dopplers; elevated RIs, no RAS
15 Initial management; BP reduction What is the BP target? What anti hypertensive cocktail will you use to achieve it?
16 BP target? A. 140/90 B. 130/80 C. 125/75 D. other?



17 September 2010
18 The ESCAPE Trial Group. N Engl J Med 2009;361: October 2009

19 Results of Efficacy Outcomes in Randomized, Controlled Trials of Blood Pressure Targets (Low Versus Usual) in Adults With CKD. No benefit of / over 140/90 Upadhyay A et al. Ann Intern Med doi: /


20 Results of Interaction Tests and Subgroup Analyses by Baseline Proteinuria in Trials of Blood Pressure Targets (Low Versus Usual) in Patients With Chronic Kidney Disease. Upadhyay A et al. Ann Intern Med doi: /
21 Author s conclusions In summary, evidence does not conclusively show that a currently recommended blood pressure target less than 130/80 mm Hg improves clinical outcomes more than a conventional target less than 140/90 mm Hg in adults with CKD. A lower target may be beneficial in persons with proteinuria greater than 300 to 1000 mg/d. We suggest that practitioners use discretion in patients with CKD and proteinuria and base the blood pressure target on individualized risk benefit assessment and the patient's tolerance and preferences. Treatment to a lower target may require greater vigilance to monitor for and avoid possible symptoms and adverse events from hypotension.
22 What agent will you use? A. ARB B. Diuretic; thiazide v loop C. Uptitrate alpha blocker D. Aldosterone antagonist E. Other?
23 Prevention of progression CKD Combination anti hypertensives; ACE/ dihydropyridine

24 The Lancet, April 2010
25 Prevention of progression CKD Combination anti hypertensives;? ACE/ ARB


26
27
28 OnTarget, albuminuria and mortality CV mortality (%) P< P< Baseline value Doubling of urinary albumin excretion Halving of urinary albumin excretion Schmeider ESH Abstract July 2010 Doubling of ACR associated with 47% increased mortality Halving of ACR associated with 15% reduced mortality
29 Circulation January 2011 ON TARGET ; no benefit renal or cardiovascular TRANSCEND; significant towards harm in the normoalbuminemic group trend towards benefit in the micro/ macroalbuminuria
30 Canadian Medical association Journal March 2011

31 Development of ESKD and progression of micro to macroalbuminuria were reduced significantly with ACE v placebo and ARB v placebo, but not with combined ACE/ ARB v monotherapy
32 Prevention of progression CKD Aldosterone Antagonists

33 Clinical JASN 2009
34 Aldo antagonist +ACEi/ARB Vs ACEi /ARB alone Aldo antagonist +ACEi/ARB Vs ACEi /ARB alone Aldo antagonist +ACEi/ARB Vs ACEi /ARB alone Spironolactone Eplerenone Total Proteinuria Change in GFR Incidence of hyperkalaemia Navaneethan et al, Clinical JASN 2009
35 Follow up; 2 weeks Bumetanide commenced 1 mg tds Significant diuresis, 3 kg weight loss, peripheral oedema improved BP in GP rooms; 155 /80 Creatinine 272. Urinary PCR 90. I brought in those films you asked to look at


36


37 Plasma aldosterone/ renins; performed off ACE/ beta blockade/ diuretic/ calcium channel blockers 10/7. On Prazosin 5 mg tds.
38 24 hr urinary aldosterone; 30 micrograms/ 24 hrs Adrenal vein sampling; Aldosterone levels are all high. Ratios for LAV and RAV all higher than low IVC/ SRV ratios suggesting patient has Bilateral Adrenal Hyperplasia (R > L) 24 hr urinary catecholamines/ plasma metanephrines normal studies Interval 3 month MR left adrenal lesion ; consistent with an adrenal haematoma
39 Summary 1. Multiagent hypertension 2. Primary hyperaldosteronism Bilateral adrenal hyperplasia 3. Proteinuric CKD Stage 4 (approx 700 mg) No biopsy Presumed hypertensive small vessel ischaemic nephropathy +/ diabetic glomerulosclerosis +/ secondary FSGS 4. Adrenal haematoma (probable)
40 Discussion Aldosterone antagonism?

41 Serum creatinine Aldactone ceased Aldactone commenced
42 Update March 2011 partial left laparoscopic adrenalectomy Macro; adrenal haematoma complicating underlying adrenal adenoma; pathology pending 2 weeks post surgery; BP 125/65. Loop diuretic ceased. Creatinine 310 (egfr 17 mls/min) stable. Attending renal education sessions.
43 Hypothetical; Needs CABG? Role of preoperative cessation RAAS blockade
44 Medications at presentation Metoprolol 50 mg bd Prazosin 2.5 mg bd Ramipril 10 mg po mane Lercanidipine 20 mg po nocte Aspirin 100 mg po daily Atorvastatin 20 mg po nocte Lantus bd
45 RAAS blockade in coronary artery surgery: Retrospective cohort study of 10,023 pts Pre operative RAAS blockade associated with doubling of the risk of death, increased need for inotropic support and incidence of renal dysfunction Miceli, JACCC, 2009
46 RAAS blockade in non cardiac surgery: Prospective observational study of 65,043 Patients undergoing perioperative therapy with ACEi or ARBs in combination with diuretic showed: More periods with SBP less than 70mmHg Periods with greater than 50% decrease in SBP Increased vasopressor requirement Kheterpal et al, J Cardiothor and Vasc Anaesthesias, 2008
47 Thankyou
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Professor Suetonia Palmer
 Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영
 만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Diabetes and Kidney Disease. Kris Bentley Renal Nurse practitioner 2018
 Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets
 Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Diabetes in Renal Patients. Contents. Understanding Diabetic Nephropathy
 Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Colin Edwards. Cardiologist Auckland Heart Group Waitemata Health
 Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Diabetes Complications Guideline Based Screening, Management, and Referral
 Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Hypertension and obesity. Dr Wilson Sugut Moi teaching and referral hospital
 Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
in patients with diabetes, nephropathy and/or chronic kidney disease Summary of recommendations July 2017
 Association of British Clinical Diabetologists (ABCD) and Renal Association clinical guidelines: Hypertension management and reninangiotensin-aldosterone system blockade in patients with diabetes, nephropathy
Association of British Clinical Diabetologists (ABCD) and Renal Association clinical guidelines: Hypertension management and reninangiotensin-aldosterone system blockade in patients with diabetes, nephropathy
Prof. Armando Torres Nephrology Section Hospital Universitario de Canarias University of La Laguna Tenerife, Canary Islands, Spain.
 Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
Caring for Australians with Renal Impairment. BP lowering and CVD
 Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus
 Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Renal Protection Staying on Target
 Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Chronic Kidney Disease. Paul Cockwell Queen Elizabeth Hospital Birmingham
 Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Blood Pressure. Michelle Bertram- Nephrology- OBH
 Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
CKD IN THE CLINIC. Session Content. Recommendations for commonly used medications in CKD. CKD screening and referral
 CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
Chronic Pediatric Hypertension
 Chronic Pediatric Hypertension Nephrology Grand Round 3/13/2015 Mahmoud Kallash M.D Outline Definition of hypertension (HTN) Challenges in diagnosing HTN Epidemiology Causes and evaluation of HTN Management
Chronic Pediatric Hypertension Nephrology Grand Round 3/13/2015 Mahmoud Kallash M.D Outline Definition of hypertension (HTN) Challenges in diagnosing HTN Epidemiology Causes and evaluation of HTN Management
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease
 Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Diabetes Renal Disease Management. Dr Paul Laboi Dr Vijay Jayagopal York Hospital
 Diabetes Renal Disease Management Dr Paul Laboi Dr Vijay Jayagopal York Hospital 0 Diabetic Nephropathy Diabetic nephropathy is a clinical syndrome characterised by the following: Persistent albuminuria
Diabetes Renal Disease Management Dr Paul Laboi Dr Vijay Jayagopal York Hospital 0 Diabetic Nephropathy Diabetic nephropathy is a clinical syndrome characterised by the following: Persistent albuminuria
Diabetic Kidney Disease: Update. GKA Master Class. Istanbul 2011
 Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
PRE-DIALYSIS CARE IN CHRONIC KIDNEY DISEASE PATIENTS DR O. A ADEJUMO MBBS, FWACP, FMCP
 PRE-DIALYSIS CARE IN CHRONIC KIDNEY DISEASE PATIENTS DR O. A ADEJUMO MBBS, FWACP, FMCP OUTLINE INTRODUCTION BURDEN OF CKD DEFINITION OF PRE-DIALYSIS CARE (PDC) GOALS OF PDC IN CKD COMPONENTS OF PDC ADVANTAGES
PRE-DIALYSIS CARE IN CHRONIC KIDNEY DISEASE PATIENTS DR O. A ADEJUMO MBBS, FWACP, FMCP OUTLINE INTRODUCTION BURDEN OF CKD DEFINITION OF PRE-DIALYSIS CARE (PDC) GOALS OF PDC IN CKD COMPONENTS OF PDC ADVANTAGES
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Rationale: Objectives: Indication: Diabetes Mellitus, Type 2 Study Investigators/Centers: 300 physicians in 292 clinics Research Methods: Data Source:
 GSK Medicine: N/A Study No.: 112255 Title: A Korean, multi-center, nation-wide, cross-sectional, epidemiology study to identify prevalence of diabetic nephropathy in hypertensive patients with type 2 diabetes
GSK Medicine: N/A Study No.: 112255 Title: A Korean, multi-center, nation-wide, cross-sectional, epidemiology study to identify prevalence of diabetic nephropathy in hypertensive patients with type 2 diabetes
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
CHRONIC KIDNEY DISEASE DIAGNOSIS
 CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Cardiovascular risk reduction in diabetes Lipids (NICE CG181)
") Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors