Anti-Reflux Surgery in Cerebral Palsy Patients
|
|
|
- Madison White
- 5 years ago
- Views:
Transcription
1 Anti-Reflux Surgery in Cerebral Palsy Patients Cecostomy for Bowel Management Surgery for Prenatally Identified Congenital Lung Lesions Dr. Mike Giacomantonio IWK Health Centre, Halifax, NS
2 G. E. Reflux in Cerebral Palsy vs. Question of G. E. Reflux
3 G. E. Reflux associated with: Dental disease Laryngeal disease Respiratory Disease
4 Modern Proton Pump Inhibitors (PPI s) So effective, if problem not resolved with PPI s, question the diagnosis
5 Fundoplication in children: Complication rate > 50% in: Neurologically injured Infants < one year of age
6 Failure rate of Nissen Fundoplication: JAMA 2001 May 9;285(18): Spechler, S. J. et al: Medical vs surgical treatment for GERD No difference in antacid use after 10 years (> 50% in both groups)

7
8 Incidence of gagging and question of ongoing reflux unchanged in CP patients following fundoplication
9 Esophago-Gastric Dissociation
10 No impact on gagging or question of reflux
11 A Cautionary Tale Infant < one year of age, CP Difficulty feeding; significant gagging Question of GE reflux Request for G tube and Fundoplication


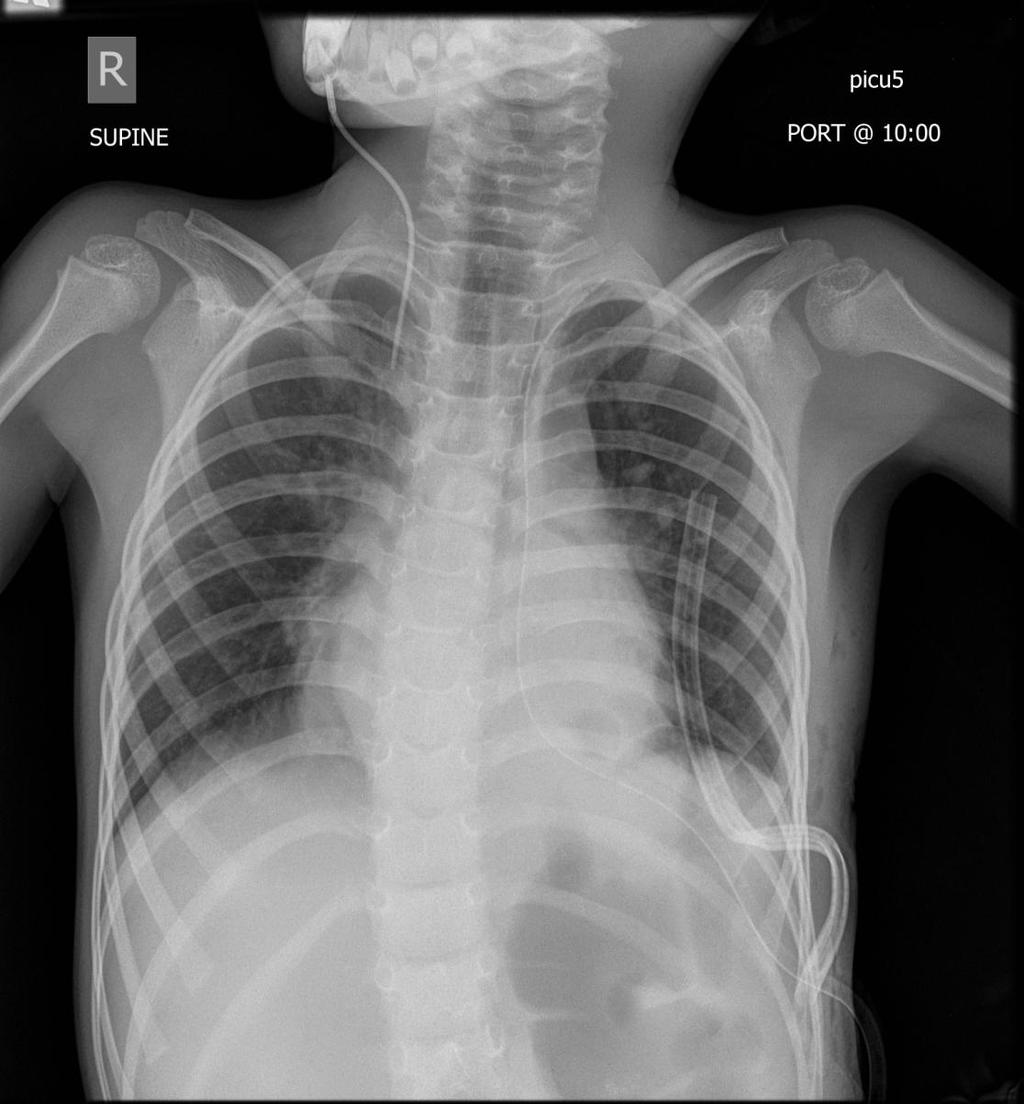
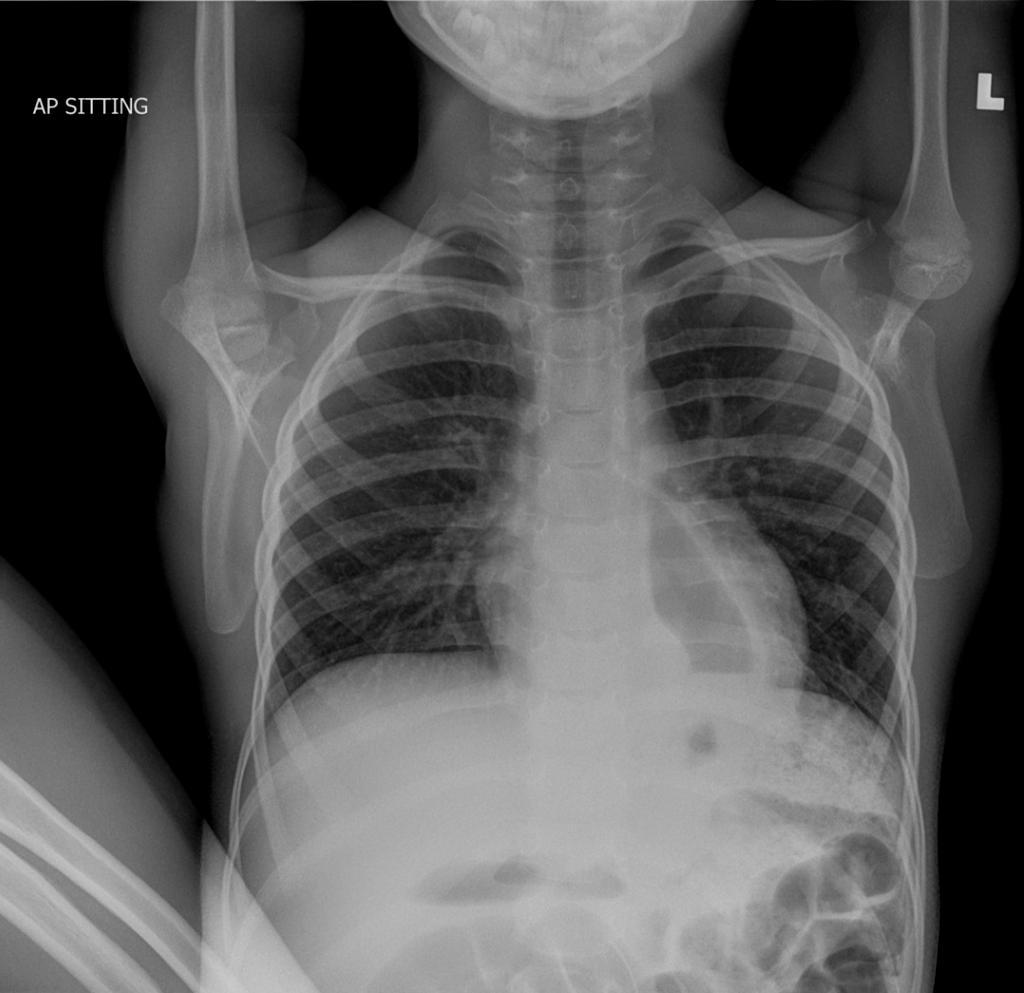
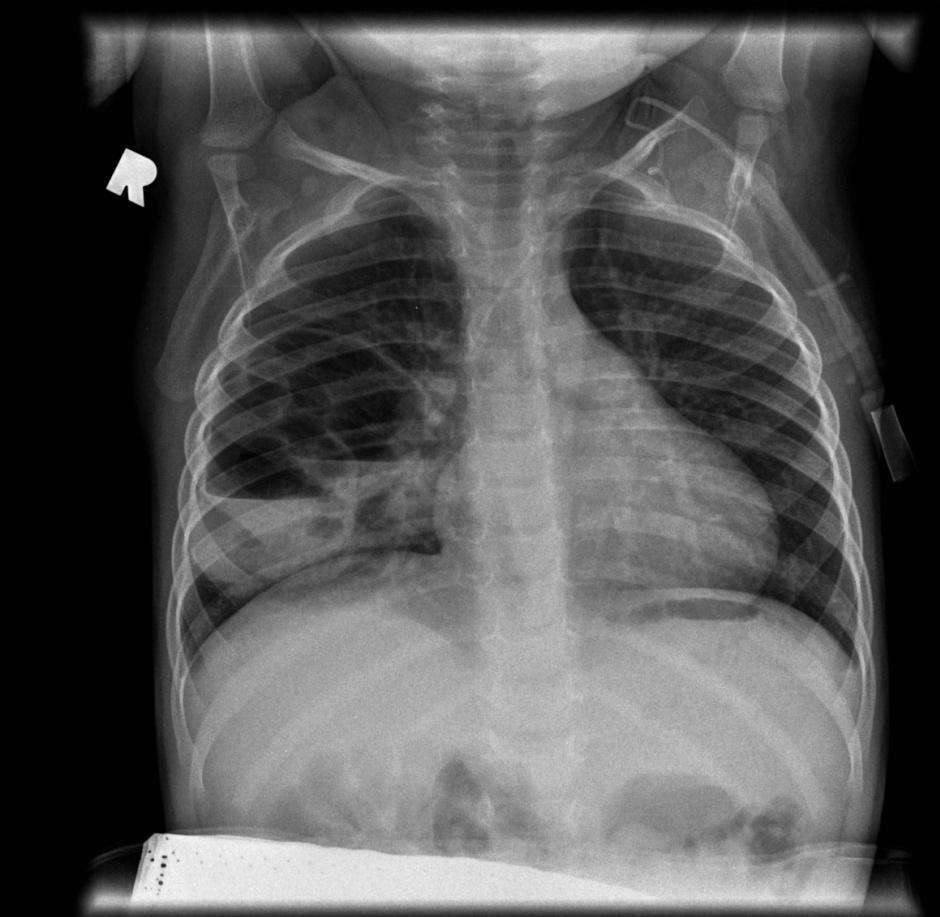
12 Chest and abdomen at birth

13 Upper GI series 30/01/09
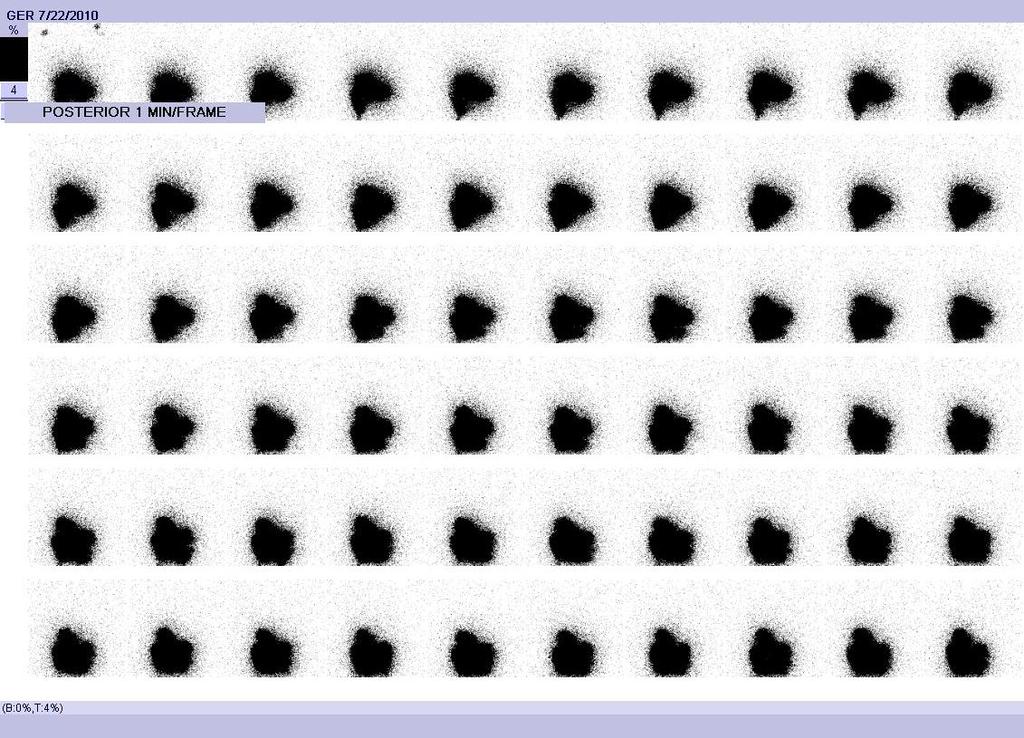
14 Gastroesophageal Reflux Scan
15 Had fundoplication and G Tube Gag persists Question of GE reflux persists Had esophago-gastric dissociation

16 18/08/12
17 Gag persists Question of reflux persists


18 12/11/12



19 UGI- 13/11/12
20 Had repair of paraesophageal hernia
21 08/02/14
22 Gag persists Question of reflux persists

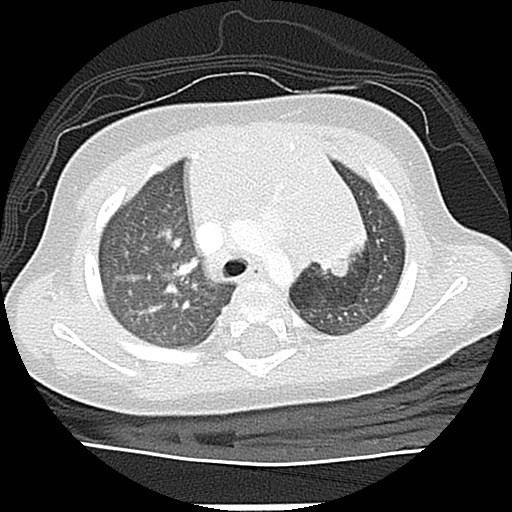
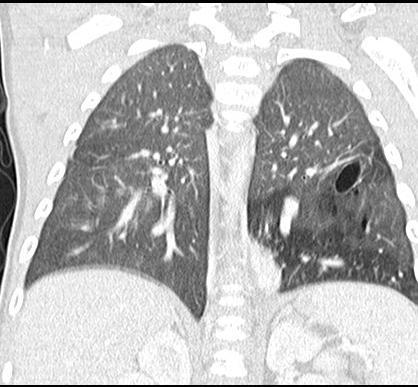
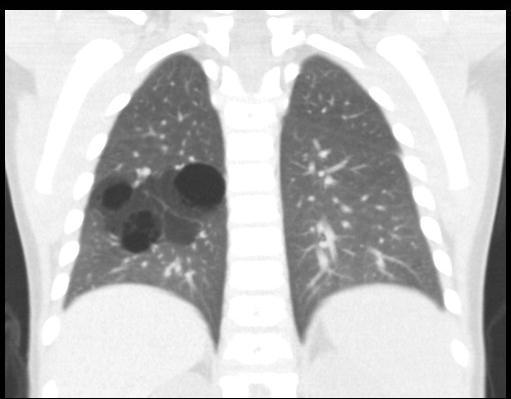
23 Coronal CT -12/08/14

24 15/09/14
25 Outcome: Gag and question of reflux unchanged
26 Observations: Neurologically injured children often have: Incoordination of swallowing with or without:» Food aversion» Pooled oropharyngeal secretions» aspiration Exaggerated gag reflex The combination of gagging, pooled secretions and aspiration commonly interpreted as caused by GE reflux

27
28 Recommendations: If feeding tube required: G-tube (PEG) if no concern about reflux J-tube (Roux en Y) plus anti-reflux medication if reflux a concern G-J tube plus anti-reflux medication if seemingly intolerant of any gastric secretions

29
30 Bowel Management
31 Bowel Management for: Spina Bifida Imperforate Anus Severe functional constipation
32 Severe Functional Constipation: Subtle innervation abnormality e.g. Intestinal neuronal dysplasia Anal achalasia (formerly ultra-short segment Hirschsprung s Disease)
33

34

35
36
37
38 Problem: Compromise of autonomic and/or somatic function Result: Compromise of control of evacuation Both inadequate evacuation (constipation) And inadequate control of evacuation (incontinence)
39 Management: Proportional to degree of compromise Behavioral modification Suppository (degrees of stimulation) Enemas (increasing volumes)
40 Pragmatic goal of management: Controlled timing of evacuation Sufficient evacuation to allow predictable period of freedom from soiling i.e., social continence
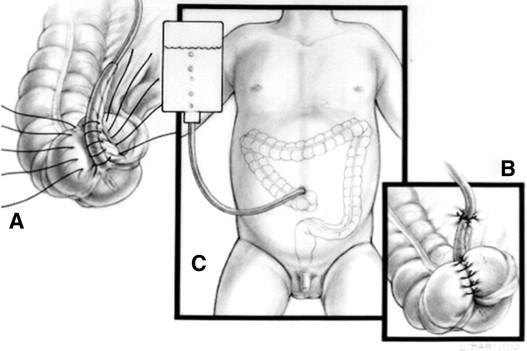
41 Cecostomy to allow antegrade colonic enema (ACE)



42 Benefits of Antegrade Colonic Enema Allows for washout of whole colon Produces a bowel movement at a convenient time and place Allows an extended, predictable time without soiling

43 MACE procedure Malone Antegrade Continence Enema Dr. P Malone - Appendicostomy - described in 1990

44 MACE

45 Disadvantages of the MACE procedure Appendix may not be available - appendicitis, neurogenic bladder, previous Mitrofanoff 30% stricture at skin level - ACE stopper Permanent, definitive


46 1996 Performed by interventional radiology Chait trapdoor
47 Percutaneous cecostomy placement steps Rectum/colon inflated with air Cecum accessed with needle/wire under US and fluoroscopic guidance T-bars


48 Percutaneous cecostomy placement steps Small catheter inserted over wire (Cooke pigtail catheter) T-bar anchor sutures cut at 14 days Replaced by Chait Trapdoor after 6-8 weeks
49 Complications with Cecostomies Anchors loosened peritonitis laparotomy Significant peritonitis successfully treated with IV antibiotics Site infections treated by family doctors Accidental removal of pigtail catheter replaced with foley Coil not evacuated obstruction Hypergranulation tissue treated with silver nitrate ( occasional excision during anaesthetic)
50 Laparoscopic Cecostomy PROS More control Direct vision CONS Abdominal surgery More invasive Chait inserted primarily - spares one anesthetic in young children
51 Cecostomy irrigations/enemas Frequency of irrigations daily to three times weekly Irrigation solutions: Glycerin used in combinations with saline or saline and sodium phosphate followed by saline sodium phosphate followed by saline in varying amounts. Co-lyte/Go-lytely/Peg-lyte followed by saline May still require oral medications (eg. PEG 3350)
52 Follow-up Individualized; can be daily, weekly, monthly or yearly Can access members of Bowel Management Team at any point in time Cecostomy trapdoors changed about every 12 months (interventional radiology)
53 Cecostomy Procedures to date at IWK: First 3 done open - catheters replaced with Bard buttons 1997 April 2001 first percutaneous procedure May 2014 first laparscopic procedure Age range when done 3 years to 33 years Spina Bifida 26 Spina Bifida/Imperforate Anus 2 Imperforate Anus 23 Hirschsprung s Disease 2 Caudal Regression 1 Cerebral Palsy 3 Chronic Constipation 10 Total 67
54 Prenatally Identified Congenital Lung Lesions




55 Screening Obstetrical US Echogenic Mass Left Lung
56 Initial differential: Congenital cystadenomatoid malformation (CCAM) Pulmonary sequestration
57 Observation: 10 X incidence of prenatally identified lung lesions than historical surgical experience


58 Post Natal Chest Radiograph Day 1
59 Operate or not operate? 2 opposing camps
60 Surgical findings: Frequent unremarkable findings Defence: Risk of missed lesions:» CCAM» Sequestration» Pleuro-pulmonary blastoma (new speculation)
61 Findings with conservative approach: Clinical and imaging follow-up: Some disappear Bronchial atresia Congenital lobar emphysema (CLE) Congenital segmental emphysema Sequestration Congenital cystadenomatoid malformation (CCAM) No congenital pleuropulmonary blastoma (reported by anyone)




62 Bronchial Atresia


63 Congenital Lobar Emphysema




64 Congenital Segmental Emphysema

65 CPAM with fluid levels






66 CT at 11 months of age Hybrid lesion (ILS,cysts, segmental emphysema)
67 Clinical consequence of conservative management: Rare infection before age 2 years Overall surgical incidence approximately 1 in 10 prenatal lesions
68 Protocol for prenatally identified pulmonary lesions: Symptomatic Asymptomatic
69 Symptomatic: Hydrops Fetal intervention Termination


70 Case 4:Large CPAM before and after stent
71 Asymptomatic: Clinical assessment at birth Chest X-ray at birth Chest X-ray at 3-6 months CT Scan at 6-12 months




72 CPAM RML
73 If potentially surgical lesion discuss Pros and Cons of surgery: Cons: Avoid surgery in > 50% of cases Pros: Eliminate risk of infection Eliminate concerns regards flying, insurance, etc. Surgical risks very low (?<5%)
74 Acknowledgement: Ms. Gail Creelman Dr. Kathy O Brien Dr. Mike VandenHof
Percutaneous Cecostomy Tube Placement
 Information About Your Child s Procedure Percutaneous Cecostomy Tube Placement Read this form so you understand the procedure and its risks. Please ask questions about anything you do not understand. What
Information About Your Child s Procedure Percutaneous Cecostomy Tube Placement Read this form so you understand the procedure and its risks. Please ask questions about anything you do not understand. What
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Management of Neurogenic Bowel Dysfunction. Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders
 Management of Neurogenic Bowel Dysfunction Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders DEFECATION Delivery of colon contents to the rectum Rectal compliance
Management of Neurogenic Bowel Dysfunction Fiona Paul, DNP, RN, CPNP Center for Motility and Functional Gastrointestinal Disorders DEFECATION Delivery of colon contents to the rectum Rectal compliance
Case Based Fetal Lung Masses
 Case Based Fetal Lung Masses Advances in Fetal and Neonatal Imaging Course Orlando, Florida, January 28, 2017 Leann E. Linam, MD Associate Professor Radiology University of Arkansas for Medical Sciences/
Case Based Fetal Lung Masses Advances in Fetal and Neonatal Imaging Course Orlando, Florida, January 28, 2017 Leann E. Linam, MD Associate Professor Radiology University of Arkansas for Medical Sciences/
Efficacy of Peristeen transanal irrigation system for neurogenic bowel in the pediatric population: Preliminary findings
 Efficacy of Peristeen transanal irrigation system for neurogenic bowel in the pediatric population: Preliminary findings Tiffany Gordon, MSN, RN, CRRN, CPN David Vandersteen, MD John Belew RN, PhD Gillette
Efficacy of Peristeen transanal irrigation system for neurogenic bowel in the pediatric population: Preliminary findings Tiffany Gordon, MSN, RN, CRRN, CPN David Vandersteen, MD John Belew RN, PhD Gillette
Pediatric Surgery MUHC MCH Siste. Objectives of Training
 Preamble A rotation in Pediatric Surgery must give residents the opportunity to become familiar with the unique needs of infants and children as surgical patients. Some of the surgical diseases encountered
Preamble A rotation in Pediatric Surgery must give residents the opportunity to become familiar with the unique needs of infants and children as surgical patients. Some of the surgical diseases encountered
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
The Malone Antegrade Continence Enema (MACE) Principle In Children: Is It Important If the Conduit Is Implanted In the Left or the Right Colon?
 Principle In Children: Is It Important If the Conduit Is Implanted In the Left or the Right Colon?") Pediatric Urology Malone Antegrade Continence Enema (MACE) International Braz J Urol Vol. 34 (2): 206-213, March - April, 2008 The Malone Antegrade Continence Enema (MACE) Principle In Children: Is It
Pediatric Urology Malone Antegrade Continence Enema (MACE) International Braz J Urol Vol. 34 (2): 206-213, March - April, 2008 The Malone Antegrade Continence Enema (MACE) Principle In Children: Is It
Non-Reversed Appendicostomy for Antegrade Continence Enema in the Treatment of Encopresis
 Original Article Annals of Pediatric Surgery Vol. 6, No 3,4 July, October 2010, PP 144-149 Non-Reversed Appendicostomy for Antegrade Continence Enema in the Treatment of Encopresis Kamal Abdel-Elah, Basem
Original Article Annals of Pediatric Surgery Vol. 6, No 3,4 July, October 2010, PP 144-149 Non-Reversed Appendicostomy for Antegrade Continence Enema in the Treatment of Encopresis Kamal Abdel-Elah, Basem
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Clinical Policy Title: Cecostomy for fecal incontinence
 Clinical Policy Title: Cecostomy for fecal incontinence Clinical Policy Number: 08.01.06 Effective Date: July 1, 2016 Initial Review Date: February 17, 2016 Most Recent Review Date: April 19, 2017 Next
Clinical Policy Title: Cecostomy for fecal incontinence Clinical Policy Number: 08.01.06 Effective Date: July 1, 2016 Initial Review Date: February 17, 2016 Most Recent Review Date: April 19, 2017 Next
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
BOWEL WASHOUTS USING AN ANTEGRADE COLONIC ENEMA (ACE)
") BOWEL WASHOUTS USING AN ANTEGRADE COLONIC ENEMA (ACE) This leaflet gives information for parents/carers whose child is having an ACE procedure and explains about giving bowel washouts. Why does my child
BOWEL WASHOUTS USING AN ANTEGRADE COLONIC ENEMA (ACE) This leaflet gives information for parents/carers whose child is having an ACE procedure and explains about giving bowel washouts. Why does my child
Nutrition in children with special needs. Dr. Meenakshi J.
 Nutrition in children with special needs Dr. Meenakshi J. 1 Factors affecting growth and nutrition in children with special nutritional factors Inadequate intake primarily related to feeding dysfunction
Nutrition in children with special needs Dr. Meenakshi J. 1 Factors affecting growth and nutrition in children with special nutritional factors Inadequate intake primarily related to feeding dysfunction
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
Bowel Washouts Using an Antegrade Colonic Enema (ACE)
") This leaflet gives information for parents/carers whose child is having an ACE procedure and explains about giving bowel washouts. Why does my child need bowel washouts? Bowel washouts are a method of
This leaflet gives information for parents/carers whose child is having an ACE procedure and explains about giving bowel washouts. Why does my child need bowel washouts? Bowel washouts are a method of
Unraveling childhood constipation: Pathophysiology, diagnostics and treatment Mugie, S.M.
 UvA-DARE (Digital Academic Repository) Unraveling childhood constipation: Pathophysiology, diagnostics and treatment Mugie, S.M. Link to publication Citation for published version (APA): Mugie, S. M. (2014).
UvA-DARE (Digital Academic Repository) Unraveling childhood constipation: Pathophysiology, diagnostics and treatment Mugie, S.M. Link to publication Citation for published version (APA): Mugie, S. M. (2014).
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal wall defects of, 375 385 gastroschisis, 379 382 omphalocele, 375 379 muscle flaps from, for diaphragmatic hernia repair, 368
Index Note: Page numbers of article titles are in boldface type. A Abdominal wall defects of, 375 385 gastroschisis, 379 382 omphalocele, 375 379 muscle flaps from, for diaphragmatic hernia repair, 368
Interpret clinical and laboratory tests to identify conditions that require surgical intervention, including:
 Pediatric Surgery Note: The goals and objectives described in detail below are not meant to be completed in a single one month block rotation but are meant to be cumulative, culminating in a thorough and
Pediatric Surgery Note: The goals and objectives described in detail below are not meant to be completed in a single one month block rotation but are meant to be cumulative, culminating in a thorough and
Issues in Enteral Feeding: Aspiration
 Issues in Enteral Feeding: Aspiration A webinar for HealthTrust Members February 11, 2019 Co-sponsored by HealthTrust and V NOS Continuing Education Provider Presented by: Kathleen Stoessel, RN, BSN, MS
Issues in Enteral Feeding: Aspiration A webinar for HealthTrust Members February 11, 2019 Co-sponsored by HealthTrust and V NOS Continuing Education Provider Presented by: Kathleen Stoessel, RN, BSN, MS
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
CONGENITAL LUNG LESION Round Table. Objectives. Congenital Lung Lesions: Anatomy and Physiology Leah Barefoot, DNP, CPNP-PC
 CONGENITAL LUNG LESION Round Table L. Barefoot, E. Paton, C. Schultz, R. Caskey, M. O Day Objectives Review the anatomy and pathophysiology of congenital lung lesions List the preoperative evaluation of
CONGENITAL LUNG LESION Round Table L. Barefoot, E. Paton, C. Schultz, R. Caskey, M. O Day Objectives Review the anatomy and pathophysiology of congenital lung lesions List the preoperative evaluation of
Fecal Incontinence. What is fecal incontinence?
 Scan for mobile link. Fecal Incontinence Fecal incontinence is the inability to control the passage of waste material from the body. It may be associated with constipation or diarrhea and typically occurs
Scan for mobile link. Fecal Incontinence Fecal incontinence is the inability to control the passage of waste material from the body. It may be associated with constipation or diarrhea and typically occurs
3/30/18. Common Radiology Studies in Pediatric Surgery. Disclosure Information. Objectives
 Common Radiology Studies in Pediatric Surgery A Scenario Based Approach to Interpretation for the Pediatric Nurse and Provider presented by Elizabeth A. Paton, DNP, RN-BC, PNP-A, PPCNP-BC, CPEN, FAEN Disclosure
Common Radiology Studies in Pediatric Surgery A Scenario Based Approach to Interpretation for the Pediatric Nurse and Provider presented by Elizabeth A. Paton, DNP, RN-BC, PNP-A, PPCNP-BC, CPEN, FAEN Disclosure
Imaging of the Lung in Children
 Imaging of the Lung in Children Imaging methods X-Ray of the Lung (Anteroposterior, ) CT, HRCT MRI USG Congenital developmental defects of the lungs Agenesis, aplasia, hypoplasia Tension pulmonary anomalies
Imaging of the Lung in Children Imaging methods X-Ray of the Lung (Anteroposterior, ) CT, HRCT MRI USG Congenital developmental defects of the lungs Agenesis, aplasia, hypoplasia Tension pulmonary anomalies
PEDIATRICS. Module Topic/Content Student Learning Outcomes Resources Clinical Assessment Activities Course/Clinical Outcomes
 PEDIATRICS N332 Outline 1 Welcome back: Instructor Role and Student Role Discuss course requirements. Explain personal learning style and study patterns. Explain critical thinking and clinical judgment
PEDIATRICS N332 Outline 1 Welcome back: Instructor Role and Student Role Discuss course requirements. Explain personal learning style and study patterns. Explain critical thinking and clinical judgment
ACE Malone (Antegrade Continence Enema)
") ACE Malone (Antegrade Continence Enema) What is the ACE Malone? The Antegrade Continence Enema (ACE) is a type of surgery designed for the child who has chronic bowel problems with bouts of constipation,
ACE Malone (Antegrade Continence Enema) What is the ACE Malone? The Antegrade Continence Enema (ACE) is a type of surgery designed for the child who has chronic bowel problems with bouts of constipation,
TUBES R US. Enteral Access & Management
 TUBES R US SHEILA BELL, MS, RN, CPNP PC Christine Gangi, RN, CPN Center for Gastrointestinal Motility and Functional Disorders Division of Pediatric Gastroenterology & Nutrition Enteral Access & Management
TUBES R US SHEILA BELL, MS, RN, CPNP PC Christine Gangi, RN, CPN Center for Gastrointestinal Motility and Functional Disorders Division of Pediatric Gastroenterology & Nutrition Enteral Access & Management
Hernia. emoryhealthcare.org
 Hernia Have you noticed a bulge or pain in your abdominal wall or groin? If so you may have a hernia. You may be in the process of confirming this diagnosis with your Primary Care Physician or already
Hernia Have you noticed a bulge or pain in your abdominal wall or groin? If so you may have a hernia. You may be in the process of confirming this diagnosis with your Primary Care Physician or already
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Joint Committee on Surgical Training. Guidelines for the award of a CCT in Paediatric Surgery
 Joint Committee on Surgical Training Guidelines for the award of a CCT in Paediatric Surgery All trainees seeking a CCT in Paediatric Surgery must: a) be fully registered with the GMC and have a licence
Joint Committee on Surgical Training Guidelines for the award of a CCT in Paediatric Surgery All trainees seeking a CCT in Paediatric Surgery must: a) be fully registered with the GMC and have a licence
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Peristeen and the Neurogenic Bowel Dysfunction Score (NBD) for pediatric patients with spina bifida
 for pediatric patients with spina bifida") Peristeen and the Neurogenic Bowel Dysfunction Score (NBD) for pediatric patients with spina bifida Coloplast develops products and services that make life easier for people with very personal and private
Peristeen and the Neurogenic Bowel Dysfunction Score (NBD) for pediatric patients with spina bifida Coloplast develops products and services that make life easier for people with very personal and private
Gastro Intestinal pg 1 of 6
 Gastro Intestinal pg 1 of 6 Diabetic Ketoacidosis -Treatment differences True Na: adjust upward 1.6 mleq/l for every 100 mg/dl increase in blood glucose Potential serious CNS effects; 2-5% mortality rate
Gastro Intestinal pg 1 of 6 Diabetic Ketoacidosis -Treatment differences True Na: adjust upward 1.6 mleq/l for every 100 mg/dl increase in blood glucose Potential serious CNS effects; 2-5% mortality rate
Surgical Evaluation for Benign Esophageal Disease. Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018
 Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Small Bowel and Colon Surgery
 Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Long-Term Bowel Symptoms Following Corrective Surgery
 HIRSCHSPRUNG'S DISEASE Samuel Nurko MD MPH Center for Motility and Functional Gastrointestinal Disorders Children s Hospital Medical Center, Boston Ma Long-Term Bowel Symptoms Following Corrective Surgery
HIRSCHSPRUNG'S DISEASE Samuel Nurko MD MPH Center for Motility and Functional Gastrointestinal Disorders Children s Hospital Medical Center, Boston Ma Long-Term Bowel Symptoms Following Corrective Surgery
There are four general types of congenital lung disorders:
 Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
Myogenic Control. Esophageal Motility. Enteric Nervous System. Alimentary Tract Motility. Determinants of GI Tract Motility.
 Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Esophageal Motility. Alimentary Tract Motility
 Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
Patient Solutions CARE AND MAINTENANCE OF FEEDING TUBES AND COMPLICATIONS MIEKE HABECK
 Patient Solutions CARE AND MAINTENANCE OF FEEDING TUBES AND COMPLICATIONS MIEKE HABECK CARE OF FEEDING TUBES - AGENDA Types of Tubes Tube Maintenance Stoma Care Complications - management and prevention
Patient Solutions CARE AND MAINTENANCE OF FEEDING TUBES AND COMPLICATIONS MIEKE HABECK CARE OF FEEDING TUBES - AGENDA Types of Tubes Tube Maintenance Stoma Care Complications - management and prevention
Certification Guidelines for Paediatric Surgery
 Certification Guidelines for Paediatric Surgery All trainees seeking certification in Paediatric Surgery must: a) be fully registered with the GMC and have a licence to practise. b) have undertaken 6 years
Certification Guidelines for Paediatric Surgery All trainees seeking certification in Paediatric Surgery must: a) be fully registered with the GMC and have a licence to practise. b) have undertaken 6 years
Bowel Management for Children with Anorectal Malformations by Kathleen Guardino, RN, MSN
 Bowel Management for Children with Anorectal Malformations by Kathleen Guardino, RN, MSN Dr. Alberto Peña, Chief of Surgery at Schneider Children's Hospital created the posterior sagittal anorectoplasty
Bowel Management for Children with Anorectal Malformations by Kathleen Guardino, RN, MSN Dr. Alberto Peña, Chief of Surgery at Schneider Children's Hospital created the posterior sagittal anorectoplasty
LINX Reflux Management System. Patient Information. Caution: Federal (USA) Law restricts this device to sale by or on the order of a physician.
 Law restricts this device to sale by or on the order of a physician.") LINX Reflux Management System Patient Information Caution: Federal (USA) Law restricts this device to sale by or on the order of a physician. 2 Table of Contents What is the LINX System? 3 Why doctors
LINX Reflux Management System Patient Information Caution: Federal (USA) Law restricts this device to sale by or on the order of a physician. 2 Table of Contents What is the LINX System? 3 Why doctors
David Markowitz, MD. Physicians and Surgeons
 Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions
Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions
PRODUCTS FOR. Gastroenterology
 PRODUCTS FOR Gastroenterology Contents Chait Percutaneous Cecostomy Set................................................. 2-3 Cope Gastrointestinal Suture Anchor Set..............................................
PRODUCTS FOR Gastroenterology Contents Chait Percutaneous Cecostomy Set................................................. 2-3 Cope Gastrointestinal Suture Anchor Set..............................................
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Bowel Function and Care. Pat Beierwaltes, Chair Paige Church Lusine Ambartsumyan Sharon Braille Julie Dicker Tiffany Gordon Sue Liebold
 Bowel Function and Care Pat Beierwaltes, Chair Paige Church Lusine Ambartsumyan Sharon Braille Julie Dicker Tiffany Gordon Sue Liebold Outcomes Primary Outcomes Maintenance of social continence as appropriate
Bowel Function and Care Pat Beierwaltes, Chair Paige Church Lusine Ambartsumyan Sharon Braille Julie Dicker Tiffany Gordon Sue Liebold Outcomes Primary Outcomes Maintenance of social continence as appropriate
Enteral Feeding Access: Your BFF or Frenemy?
 Enteral Feeding Access: Your BFF or Frenemy? Elizabeth Hood, APN/CPNP The Ann and Robert H. Lurie Children s Hospital of Chicago Chicago, IL Disclosure Information No disclosures to report Objectives The
Enteral Feeding Access: Your BFF or Frenemy? Elizabeth Hood, APN/CPNP The Ann and Robert H. Lurie Children s Hospital of Chicago Chicago, IL Disclosure Information No disclosures to report Objectives The
1. What evidence exists that prevention of constipation in the first year of life improves outcome of bowel management in later childhood?
 BOWEL FUNCTION AND CARE Overall Outcomes Primary Outcomes o Maintenance of social continence as appropriate for age level Secondary Outcomes o Maximization of independence with managing bowel program o
BOWEL FUNCTION AND CARE Overall Outcomes Primary Outcomes o Maintenance of social continence as appropriate for age level Secondary Outcomes o Maximization of independence with managing bowel program o
Certification Guidelines for Paediatric Surgery
 Certification Guidelines for Paediatric Surgery All trainees seeking certification in Paediatric Surgery must: a) be fully registered with the GMC and have a licence to practise. b) have completed a recognised
Certification Guidelines for Paediatric Surgery All trainees seeking certification in Paediatric Surgery must: a) be fully registered with the GMC and have a licence to practise. b) have completed a recognised
Congenital Lung Malformations: Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Atypical use of button gastrostomy tube for children with complex colorectal malformations (ileostomy, vesicostomy, vaginostomy)
") Atypical use of button gastrostomy tube for children with complex colorectal malformations (ileostomy, vesicostomy, vaginostomy) Christian PIOLAT, Yohann Robert, Pierre-Yves Rabattu, Youssef Teklali, Catherine
Atypical use of button gastrostomy tube for children with complex colorectal malformations (ileostomy, vesicostomy, vaginostomy) Christian PIOLAT, Yohann Robert, Pierre-Yves Rabattu, Youssef Teklali, Catherine
Gastrointestinal problems in individuals with CdLS. Peter Gillett Consultant Gastroenterologist RHSC Edinburgh UK Cork 2011
 Gastrointestinal problems in individuals with CdLS Peter Gillett Consultant Gastroenterologist RHSC Edinburgh UK Cork 2011 Major problems Gastro-oesophageal reflux and GORD Swallowing problems and
Gastrointestinal problems in individuals with CdLS Peter Gillett Consultant Gastroenterologist RHSC Edinburgh UK Cork 2011 Major problems Gastro-oesophageal reflux and GORD Swallowing problems and
UCSF UROLOGY TRANSITIONAL UROLOGY CLINIC
 UCSF UROLOGY TRANSITIONAL UROLOGY CLINIC Thank you for choosing the UCSF Transitional Urology Clinic. This clinic was created to serve patients with urologic conditions diagnosed in childhood as they become
UCSF UROLOGY TRANSITIONAL UROLOGY CLINIC Thank you for choosing the UCSF Transitional Urology Clinic. This clinic was created to serve patients with urologic conditions diagnosed in childhood as they become
Primary Repair of High and Intermediate Anorectal Malformations in the Neonates
 Annals of Pediatric Surgery, Vol 2, No 2, April 2006, PP 117-122 Original Article Primary Repair of High and Intermediate Anorectal Malformations in the Neonates Essam A. Elhalaby Departments of Pediatric
Annals of Pediatric Surgery, Vol 2, No 2, April 2006, PP 117-122 Original Article Primary Repair of High and Intermediate Anorectal Malformations in the Neonates Essam A. Elhalaby Departments of Pediatric
PEDIATRIC GASTROSTOMY TUBES: The Ins and Outs
 PEDIATRIC GASTROSTOMY TUBES: The Ins and Outs Jenifer Reitsma, MSN, RN, CPNP Pediatric Nurse Practitioner Pediatric Surgery & Trauma Sanford Children s Hospital I have no disclosures Objectives Learner
PEDIATRIC GASTROSTOMY TUBES: The Ins and Outs Jenifer Reitsma, MSN, RN, CPNP Pediatric Nurse Practitioner Pediatric Surgery & Trauma Sanford Children s Hospital I have no disclosures Objectives Learner
SEPTIC ABDOMEN IN SPINA BIFIDA: USING CRITICAL THINKING TO PRIORITISE CARE CONFLICT OF INTEREST / PERMISSION INTRODUCTION
 SEPTIC ABDOMEN IN SPINA BIFIDA: USING CRITICAL THINKING TO PRIORITISE CARE Alison Duggan, RN, PGDip HealthSc Canterbury District Health Board Christchurch, NZ CONFLICT OF INTEREST / PERMISSION I have no
SEPTIC ABDOMEN IN SPINA BIFIDA: USING CRITICAL THINKING TO PRIORITISE CARE Alison Duggan, RN, PGDip HealthSc Canterbury District Health Board Christchurch, NZ CONFLICT OF INTEREST / PERMISSION I have no
My patient has a feeding tube
 My patient has a feeding tube What does that mean? Martha Kliebenstein, MSN, RN Clinical Educator Types of tubes Gastrostomy (G-tube) Gastrostomy jejunostomy (G-J tube) Naso gastric (NG tube) Naso jejunal
My patient has a feeding tube What does that mean? Martha Kliebenstein, MSN, RN Clinical Educator Types of tubes Gastrostomy (G-tube) Gastrostomy jejunostomy (G-J tube) Naso gastric (NG tube) Naso jejunal
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
LINX Reflux Management System
 LINX Reflux Management System Patient Information Caution: Federal (USA) Law restricts this device to sale by or on the order of a physician. LINX Reflux Management System 2 Table of Contents What is the
LINX Reflux Management System Patient Information Caution: Federal (USA) Law restricts this device to sale by or on the order of a physician. LINX Reflux Management System 2 Table of Contents What is the
Physical Exam. Vitals stable on room air Abdomen soft, non-distented Normal external genitalia Patent anus No limb anomalies
 Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Certification Guidelines for Paediatric Surgery
 Certification Guidelines for Paediatric Surgery All trainees seeking certification in Paediatric Surgery must: a) be fully registered with the GMC and have a licence to practise (UK trainees) or be registered
Certification Guidelines for Paediatric Surgery All trainees seeking certification in Paediatric Surgery must: a) be fully registered with the GMC and have a licence to practise (UK trainees) or be registered
Clinical Policy Title: Cecostomy for fecal incontinence
 Clinical Policy Title: Cecostomy for fecal incontinence Clinical Policy Number: 08.01.06 Effective Date: July 1, 2016 Initial Review Date: February 17, 2016 Most Recent Review Date: March 6, 2018 Next
Clinical Policy Title: Cecostomy for fecal incontinence Clinical Policy Number: 08.01.06 Effective Date: July 1, 2016 Initial Review Date: February 17, 2016 Most Recent Review Date: March 6, 2018 Next
BOWEL MANAGEMENT FOR PATIENTS WITH FECAL INCONTINENCE
 BOWEL MANAGEMENT FOR PATIENTS WITH FECAL INCONTINENCE QUESTION #1: Under the best circumstances, the global results following the surgical treatment of anorectal malformations are: A) 75% chance of fecal
BOWEL MANAGEMENT FOR PATIENTS WITH FECAL INCONTINENCE QUESTION #1: Under the best circumstances, the global results following the surgical treatment of anorectal malformations are: A) 75% chance of fecal
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Supplemental Information
 Supplemental Information SUPPLEMENTAL TABLE 5 Comorbidities and AEs by Patient ID: Cycle 1 5 BoNT-A; Cycle 2 5 2 Sessions BoNT-A 5 Gastrostomy, swallowing problems, drooling, recurrent pain, spasticity
Supplemental Information SUPPLEMENTAL TABLE 5 Comorbidities and AEs by Patient ID: Cycle 1 5 BoNT-A; Cycle 2 5 2 Sessions BoNT-A 5 Gastrostomy, swallowing problems, drooling, recurrent pain, spasticity
FACE THE EXAMINER. Hirschsprung s Disease in Newborns. (This section is meant for residents to check their understanding regarding a particular topic)
") Journal of Neonatal Surgery 2013;2(4):51 FACE THE EXAMINER Hirschsprung s Disease in Newborns (This section is meant for residents to check their understanding regarding a particular topic) QUESTIONS 1.
Journal of Neonatal Surgery 2013;2(4):51 FACE THE EXAMINER Hirschsprung s Disease in Newborns (This section is meant for residents to check their understanding regarding a particular topic) QUESTIONS 1.
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
SWISS SOCIETY OF NEONATOLOGY. Prenatal diagnosis and postnatal management of meconium pseudocysts
 SWISS SOCIETY OF NEONATOLOGY Prenatal diagnosis and postnatal management of meconium pseudocysts September 2007 2 Burch E, Caduff JH, Hodel M, Berger TM, Neonatal and Pediatric Intensive Care Unit (BE,
SWISS SOCIETY OF NEONATOLOGY Prenatal diagnosis and postnatal management of meconium pseudocysts September 2007 2 Burch E, Caduff JH, Hodel M, Berger TM, Neonatal and Pediatric Intensive Care Unit (BE,
INTESTINAL OBSTRUCTION ESCAPED SURGERY: MECONIUM PLUG
 7 INTESTINAL OBSTRUCTION ESCAPED SURGERY: MECONIUM PLUG Oluwayemi IO 1 *, Ade-Ojo IP 2, Olofinbiyi BA 2 1. Department of Paediatrics, Ekiti State University Teaching Hospital, Ado-Ekiti, Ekiti State, Nigeria
7 INTESTINAL OBSTRUCTION ESCAPED SURGERY: MECONIUM PLUG Oluwayemi IO 1 *, Ade-Ojo IP 2, Olofinbiyi BA 2 1. Department of Paediatrics, Ekiti State University Teaching Hospital, Ado-Ekiti, Ekiti State, Nigeria
YOUR OPERATION EXPLAINED
 RIGHT HEMICOLECTOMY This leaflet is produced by the Department of Colorectal Surgery at Beaumont Hospital supported by an unrestricted grant to better Beaumont from the Beaumont Hospital Cancer Research
RIGHT HEMICOLECTOMY This leaflet is produced by the Department of Colorectal Surgery at Beaumont Hospital supported by an unrestricted grant to better Beaumont from the Beaumont Hospital Cancer Research
The Digestive System or tract extends from the mouth to the anus.
 The Digestive System or tract extends from the mouth to the anus. FUNCTION The Digestive System breaks down and absorbs food materials e.g. amino acids, glucose DEFINITIONS: Ingestion: Ingestion is the
The Digestive System or tract extends from the mouth to the anus. FUNCTION The Digestive System breaks down and absorbs food materials e.g. amino acids, glucose DEFINITIONS: Ingestion: Ingestion is the
POSTOPERATIVE CONGENITAL ESOPHAGEAL ATRESIA COMPLICATIONS: A REVIEW
 CHILDREN S HOSPITAL II POSTOPERATIVE CONGENITAL ESOPHAGEAL ATRESIA COMPLICATIONS: A REVIEW Dr. Nguyen Thuy Hanh Ngan Neonatal Department CONTENTS 1. Background 2. Classification 3. Management 4. Complications
CHILDREN S HOSPITAL II POSTOPERATIVE CONGENITAL ESOPHAGEAL ATRESIA COMPLICATIONS: A REVIEW Dr. Nguyen Thuy Hanh Ngan Neonatal Department CONTENTS 1. Background 2. Classification 3. Management 4. Complications
Patient Information Leaflet
 Patient Information Leaflet Background Faecal incontinence is a common health problem, affecting over 1% of community-dwelling adults (1;2). Chronic constipation may affect 3-5% of the population depending
Patient Information Leaflet Background Faecal incontinence is a common health problem, affecting over 1% of community-dwelling adults (1;2). Chronic constipation may affect 3-5% of the population depending
Key words: gastric cancer, postoperative complication, total gastrectomy
 Key words: gastric cancer, postoperative complication, total gastrectomy 115 (115) Fig. 1 Technique of esophagojejunostomy (Quotation from Shimotsuma M and Nakamura R')). A, Technique for hand suture for
Key words: gastric cancer, postoperative complication, total gastrectomy 115 (115) Fig. 1 Technique of esophagojejunostomy (Quotation from Shimotsuma M and Nakamura R')). A, Technique for hand suture for
Complication of Percutaneous Endoscopic Gastrostomy
 Complication of Percutaneous Endoscopic Gastrostomy Tube Ogori N. Kalu MD Morbidity & Mortality Conference General Surgery Service Kings County Hospital Center ACGME Core Competencies 1. Medical knowledge
Complication of Percutaneous Endoscopic Gastrostomy Tube Ogori N. Kalu MD Morbidity & Mortality Conference General Surgery Service Kings County Hospital Center ACGME Core Competencies 1. Medical knowledge
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Gastrointestinal Involvement in Adult Mitochondrial Disease
 Newcastle Mitochondrial Disease Guidelines At a glance guidelines: Gastrointestinal Involvement in Adult Mitochondrial Disease For full guideline visit: http://www.newcastle-mitochondria.com/service/patient-care-guidelines/
Newcastle Mitochondrial Disease Guidelines At a glance guidelines: Gastrointestinal Involvement in Adult Mitochondrial Disease For full guideline visit: http://www.newcastle-mitochondria.com/service/patient-care-guidelines/
Congenital lung anomalies: can we postpone resection?
 Journal of Pediatric Surgery (2012) 47, 87 92 www.elsevier.com/locate/jpedsurg Congenital lung anomalies: can we postpone resection? Nadja Colon a, Cameron Schlegel a, John Pietsch a, Dai H. Chung a,b,
Journal of Pediatric Surgery (2012) 47, 87 92 www.elsevier.com/locate/jpedsurg Congenital lung anomalies: can we postpone resection? Nadja Colon a, Cameron Schlegel a, John Pietsch a, Dai H. Chung a,b,
HIRSCHSPRUNG'S DISEASE*
 RESULTS WITH ABDOMINAL RESECTION IN HIRSCHSPRUNG'S DISEASE* BY F. REHBEIN and H. VON ZIMMERMANN From the Surgical Department of the Children's Hospital, Bremen For six years we have been practising abdominal
RESULTS WITH ABDOMINAL RESECTION IN HIRSCHSPRUNG'S DISEASE* BY F. REHBEIN and H. VON ZIMMERMANN From the Surgical Department of the Children's Hospital, Bremen For six years we have been practising abdominal
Congenital Diaphragmatic Hernia information for parents. David M Notrica MD FACS FAAP Pediatric Surgeons of Phoenix
 Congenital Diaphragmatic Hernia information for parents David M Notrica MD FACS FAAP Pediatric Surgeons of Phoenix CDH Congenital absence of a portion of the diaphragm allowing abdominal contents to migrate
Congenital Diaphragmatic Hernia information for parents David M Notrica MD FACS FAAP Pediatric Surgeons of Phoenix CDH Congenital absence of a portion of the diaphragm allowing abdominal contents to migrate
Pitfalls of the Pediatric Chest and Abdomen SPR 2017
 Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Interventional procedures guidance Published: 16 December 2015 nice.org.uk/guidance/ipg540
 Electrical stimulation of the lower oesophageal sphincter for treating gastro-oesophageal reflux disease Interventional procedures guidance Published: 16 December 2015 nice.org.uk/guidance/ipg540 Your
Electrical stimulation of the lower oesophageal sphincter for treating gastro-oesophageal reflux disease Interventional procedures guidance Published: 16 December 2015 nice.org.uk/guidance/ipg540 Your
Robotic Appendicovesicostomy
 Robotic Appendicovesicostomy Cheryl Baxter, MSN,RN,CPNP Daniel DaJusta, MD Kristina Booth, MSN,RN,FNP Roadmap for Presentation Part 1 Pre-surgical/historical neurogenic bladder- Baxter Part 2 Robotic appendicovesicostomy/
Robotic Appendicovesicostomy Cheryl Baxter, MSN,RN,CPNP Daniel DaJusta, MD Kristina Booth, MSN,RN,FNP Roadmap for Presentation Part 1 Pre-surgical/historical neurogenic bladder- Baxter Part 2 Robotic appendicovesicostomy/
What is Laparoscopy All About?
 Disclaimer This movie is an educational resource only and should not be used to manage surgical health. All decisions about the management of Laparoscopy must be made in conjunction with your Physician
Disclaimer This movie is an educational resource only and should not be used to manage surgical health. All decisions about the management of Laparoscopy must be made in conjunction with your Physician
HOW TO IMAGE AND DESCRIBE CONGENITAL LUNG MALFORMATIONS
 HOW TO IMAGE AND DESCRIBE CONGENITAL LUNG MALFORMATIONS Paul Thacker, MD Assistant Professor Departments of Radiology and Pediatrics Medical University of South Carolina DISCLOSURES I have no relevant
HOW TO IMAGE AND DESCRIBE CONGENITAL LUNG MALFORMATIONS Paul Thacker, MD Assistant Professor Departments of Radiology and Pediatrics Medical University of South Carolina DISCLOSURES I have no relevant
190 Index Case studies, abdominal pain, 2 Crohn s disease, 2 3, cyclic vomiting syndrome (CVS), 2 fecal incontinence (FI), 2 medical c
, 2 fecal incontinence (FI), 2 medical c") Index Abdominal pain, case study, 2 Achalasia, 75 Acupuncture 108 American Academy of Pediatrics, 49 Anxiety, 8 9, 98 Autism, GI disorders and, 25 27 BASC. See Behavior Assessment System for Children (BASC)
Index Abdominal pain, case study, 2 Achalasia, 75 Acupuncture 108 American Academy of Pediatrics, 49 Anxiety, 8 9, 98 Autism, GI disorders and, 25 27 BASC. See Behavior Assessment System for Children (BASC)
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Antigrade Colonic Enema (ACE) Information for patients Spinal Injuries
 Information for patients Spinal Injuries") Antigrade Colonic Enema (ACE) Information for patients Spinal Injuries page 2 of 8 This leaflet has been produced in support of the explanation and counselling provided by your urologist and nurse specialist.
Antigrade Colonic Enema (ACE) Information for patients Spinal Injuries page 2 of 8 This leaflet has been produced in support of the explanation and counselling provided by your urologist and nurse specialist.
Chapter 44 10/17/2015. Care of the Patient with a Gastrointestinal Disorder. The Digestive System. Organs of the Digestive System
 Chapter 44 Care of the Patient with a Gastrointestinal Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. The Digestive System Consists
Chapter 44 Care of the Patient with a Gastrointestinal Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. The Digestive System Consists
Duc M. Vo, MD, FACS Northwest Surgical Specialists
 Duc M. Vo, MD, FACS Northwest Surgical Specialists Disclosures none Outline Definition Etiologies Exam findings Additional testing Medical management Surgical options What is fecal incontinence? Recurrent
Duc M. Vo, MD, FACS Northwest Surgical Specialists Disclosures none Outline Definition Etiologies Exam findings Additional testing Medical management Surgical options What is fecal incontinence? Recurrent