Irina Kovatch, PGY 4 Kings County Medical Center Morbidity and Mortality December 9, 2010
|
|
|
- Felicity Bradley
- 5 years ago
- Views:
Transcription


1 Irina Kovatch, PGY 4 Kings County Medical Center Morbidity and Mortality December 9, 2010
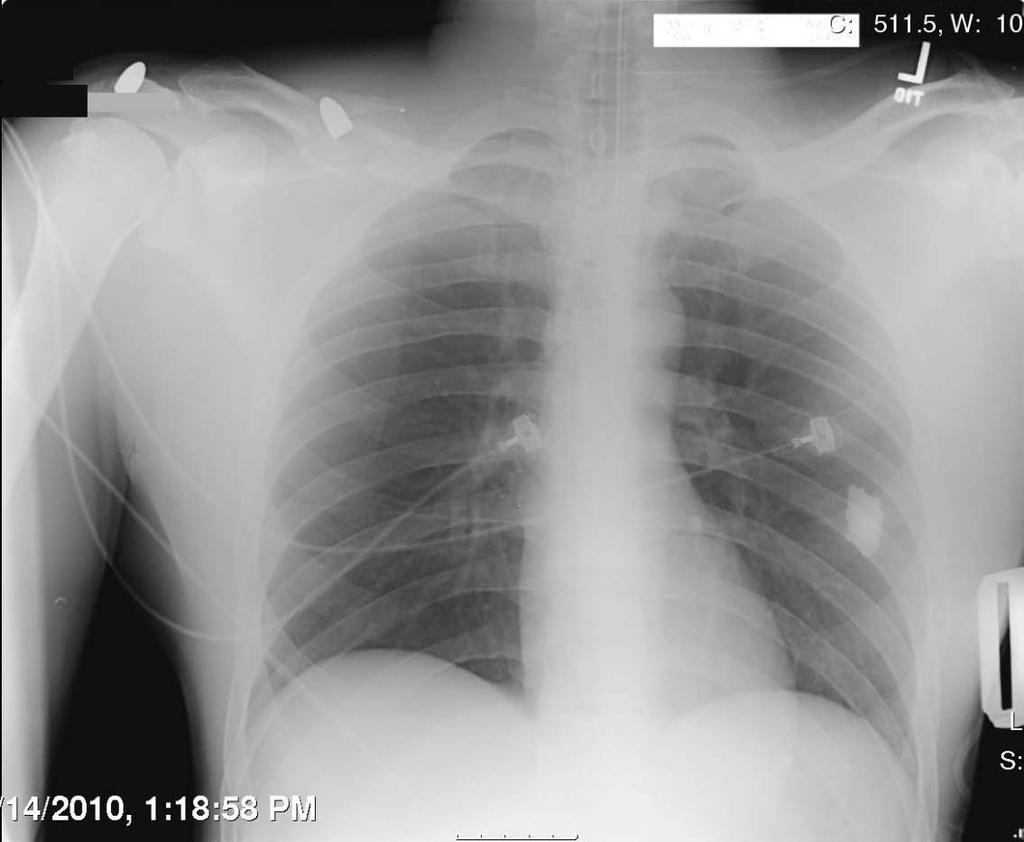
2 29 yo M BIBEMS as a trauma code on 10/14/2010 Multiple GSW: right chest, RUE, RLE VS: 98, 165/90, 110, 22, 100% A&O, agitated, c/o severe pain in RLE, oozing from wounds in RUE and chest with nonexpanding hematomas PMH: denied Case Presentation PSH: s/p ex-lap, left nephrectomy for GSW 11 years ago at Brookdale Hospital Intubated for airway protection IVFs/PRBCs transfusion initiated
3 Head: NC/AT, intubated Abd: soft, NT/ND, BS+, midline laparotomy scar Wounds - 10 Physical Exam Right chest: anterior and posterior axillary folds, axilla RUE: medial and lateral proximal arm, lateral distal arm, lateral and medial forearm - no radial pulse, fingers warm, pink with good cap refill RLE: anterior proximal thigh, posterior distal thigh - gross deformity, thigh swelling, good distal foot pulses
4 CBC /14.4/42.4/216 BMP - 136/3.8/100/22/19/1.47/144 LFTs - 7.7/4.4/52/21/47/0.4 Amylase/Lipase - 65/52 Lactic Acid VBG /69/24/20.8/-0.2 EtOH <10 UA neg Labs Utox positive for cocaine, not confirmed
5 Imaging CXR - 2 bullets projecting over the right acromion process and mid clavicle with associated comminuted fxs, no PTX Right humerus XRay - metallic shrapnel adjacent to humeral head and comminuted fracture of the greater tubercle R forearm XRay - no fxs Pelvis XRay - neg Femur XRay - severely comminuted fracture of the mid femoral shaft with associated metallic shrapnel Transfer to IR for angiogram of RUE and RLE Vascular surgery and orthopedic surgery consults
6

7
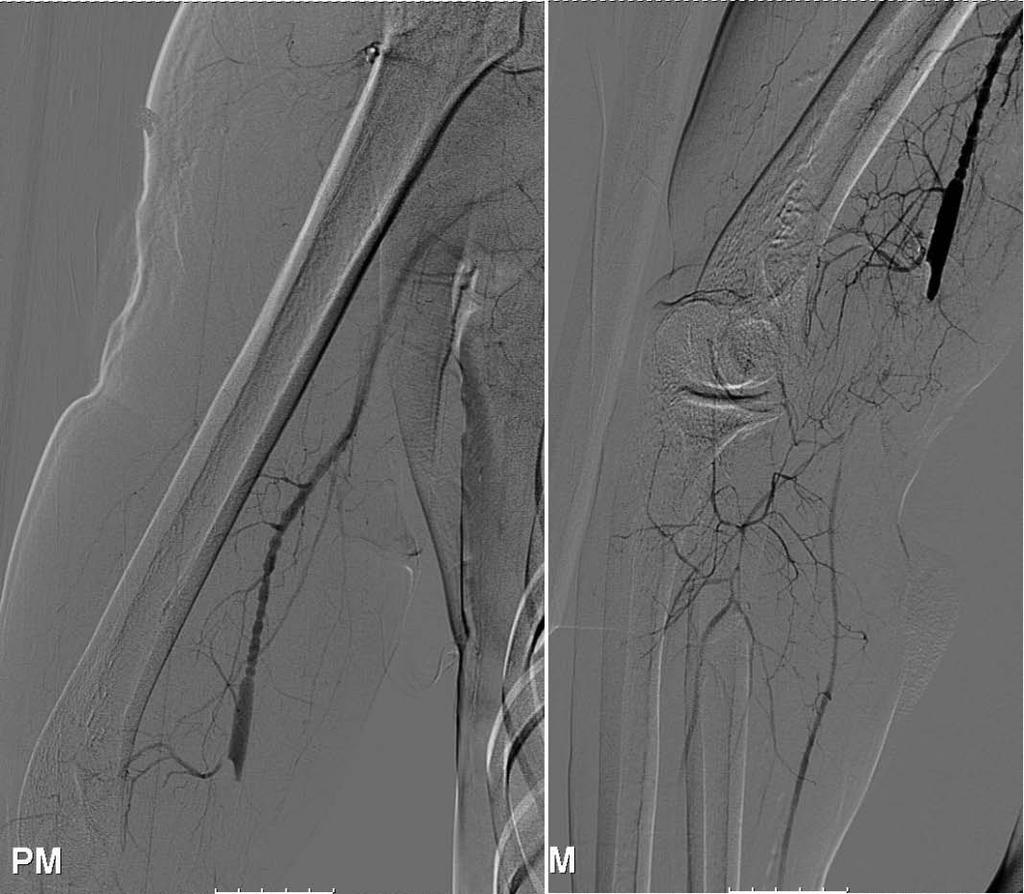
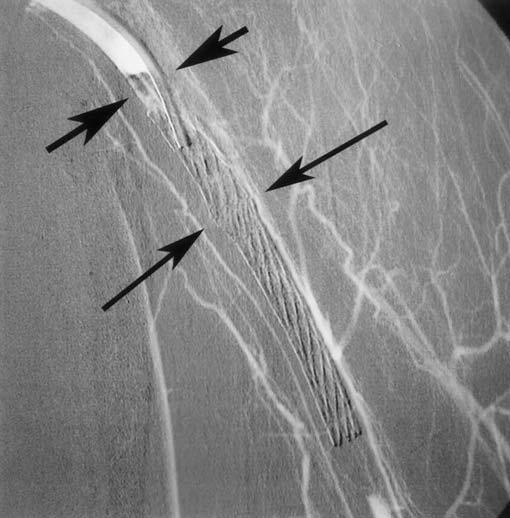
8 Angiogram RUE vasospasm and injury to the distal brachial artery, no bleeding, no other injuries the area of injury bridged and a 6 mm x 5 cm Viabahn stent graft deployed distal runoff with vasospasm - 4 boluses of 200 mcg of nitroglycerine achieved temporary relief, however spasm returned observe, if limb threat becomes apparent - exploration right hand viable, good cap refill RLE no major vascular injury

9

10
11
12
13 Serial doppler and compartment checks Flexor compartment 10 mm Hg Ortho - RLE traction Total transfusion: 10 Units PRBC and 5U FFP Stable overnight HD 1 - ICU
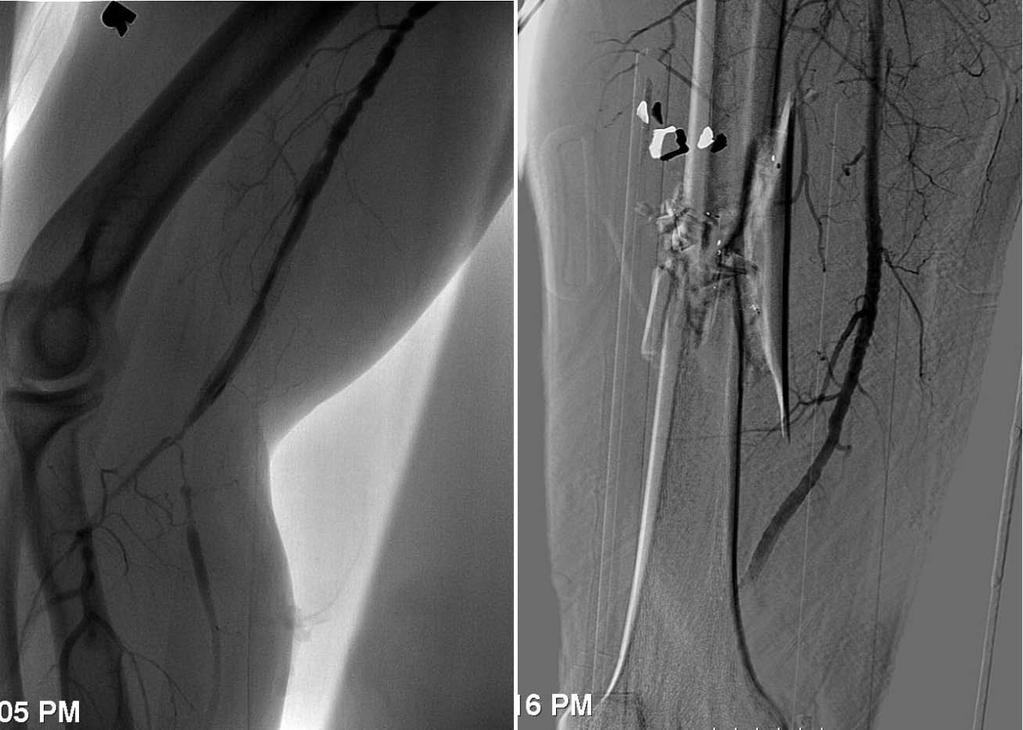
14 Forearm SBP: left 120, right 70 - possibly occluded stent graft, no compartment, good cap refill Repeat angiogram - thrombosis of the stent with distal filling of the radial and ulnar arteries via collaterals OR for vascular repair Ortho: External fixation of right femur awaiting ICU clearance for definitive fixation IVC filter placement by IR HD 2
15
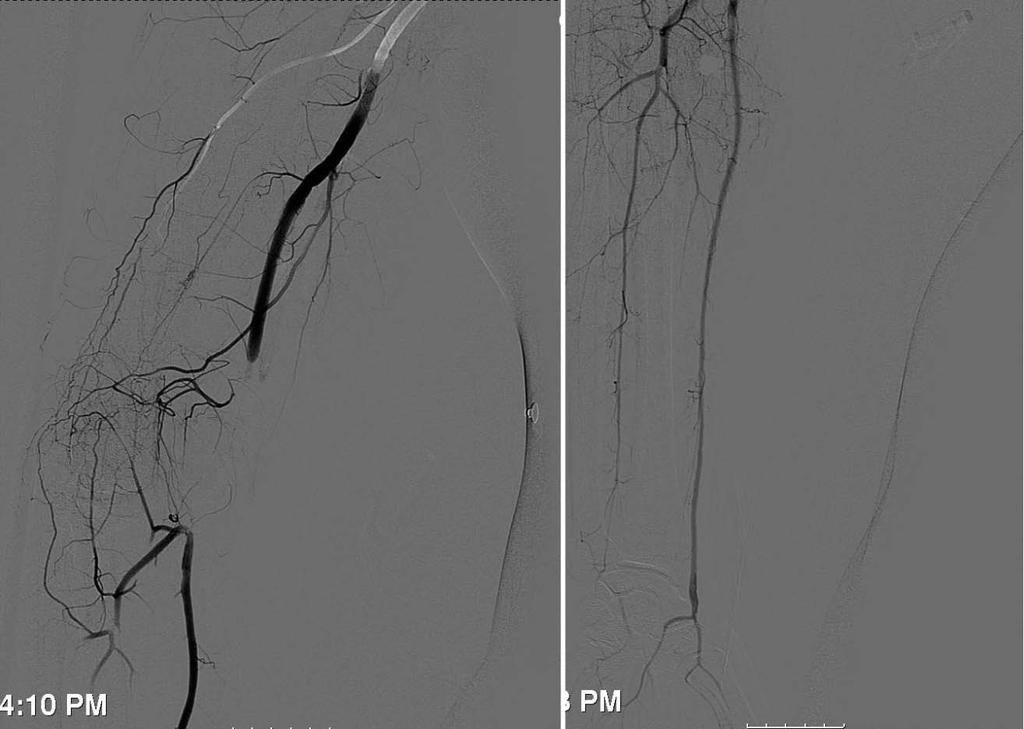
16 Vascular Surgery Exploration of right brachial artery via lazy S incision Arterial injury identified: blast effect and ~ 1.5 cm destruction of the intima (vein completely transected) Stent-graft removed, artery transected to attain healthy intima at proximal and distal ends Proximal Fogarty thrombectomy 3 cm basilic vein harvested, reversed Proximal anastomosis Distal thrombectomy and anastomosis, SubQ and skin closed, JP left Excellent radial pulse, no compartment
17 Hospital Course HD 3 - extubated, sling for RUE HD 5 Ortho: removal of ex-fix, IM nailing of right femur POD 1 - RLE WBAT HD 6 Transfer to floor, neuro and rehab consults Neuro: exam limited due to pain, decreased motion of the RUE, decreased grip - pain control, rehab, EMG in 2-3 weeks as outpatient Dispo: acute rehab placement

18

19 Questions
20 Peripheral Vascular Trauma Initial assessment and care control of external hemorrhage diagnosis of limb ischemia neurologic status of the injured extremity compartment syndrome Identifying the arterial segment involved Window of opportunity for salvage varies site and nature of injury the presence of efficient collaterals patient's age and hemodynamic status
21 Hard Signs of Vascular Injury Presence of hard signs mandates immediate intervention Pulsatile bleeding Expanding hematoma Absent distal pulses Cold, pale limb Palpable thrill Audible bruit If the site of injury is obvious angiography is unnecessary Otherwise, angiography can be performed emergently in the OR, unnecessary interventions and investigations should be avoided to minimize the delay of definitive care
22 Investigation or exploration of patients with soft signs alone is not warranted peripheral nerve deficit Soft Signs of Vascular Injury history of moderate hemorrhage at scene reduced but palpable pulse injury in proximity to a major artery Patients should be admitted and observed for 24 hours
23 Noninvasive Diagnostic Adjuncts Pulse oximetry reduction in readings in one limb is suggestive of, but neither confirms nor excludes a significant vascular injury Doppler Ultrasound presence of a doppler signal in a pulseless limb does not imply a less severe or less urgent injury reduction in the ABI in the presence of a palpable pulse does not indicate the presence of a vascular injury requiring intervention Duplex Ultrasound can detect intimal tears, thrombosis, false aneurysms and arteriovenous fistulae and has a high sensitivity
24 Angiography Remains the gold-standard for investigation and delineation of vascular injury Best performed in the operating room, with the surgeon exposing the vessel proximal to the injury for control Transfer to the radiology suite should be restricted to hemodynamically stable patients with proximal injuries Angiography may be used to treat certain selected injuries, where expertise and technical facilities are available
25 Angiography Pros & Cons Pros can evaluate multiple levels of injury in the same blood vessel can be used to image vascular structures within the thorax, abdomen, retroperitoneum, or extremities at the same time allows for control of vascular injury at the time of diagnostic angiography Cons may not necessarily grade the severity of vascular injury accurately does not image all vascular structures, therefore does not evaluate venous injury very well
26 Surgical Clinics of North America - Volume 81, Issue 6 (December 2001) Interventional Techniques in Vascular Trauma Scalea T, Sclafani S. Definitive hemostasis - embolization Torso pelvic, lumbar, peripancreatic, perinephric, hepatic Extremity injuries limited use due to distal ischemia, may be used for profunda femoris, axillary and popliteal artery branches Vascular control - balloon occlusion Mediastinal vascular injuries left subclavian, axillary Neck Zone 1 and Zone 3 Lower extremity for injury at the level of inguinal ligament Vascular repair - limited experience with transcatheter stenting for trauma, theoretical therapeutic options include use for Zone 3 carotid injury from blunt trauma traumatic aortic and popliteal vascular injury
27 The Journal of Trauma: Injury, Infection, and Critical Care downstatesurgery.org Issue: Volume 60(6), June 2006, pp Results of a Multicenter Trial for the Treatment of Traumatic Vascular Injury with a Covered Stent White R, Krajcer Z, Johnson M, et al. Prospective, multicenter, nonrandomized registry trial with a historical control to surgical management 62 patients treated with Wallgraft Endoprosthesis for arterial trauma ( ) Endpoints exclusion success at procedure and at 12-months primary patency and freedom-from-bypass at 12-months major adverse events Locations of arterial injuries iliac (33), subclavian (18), femoral (11) Indication for treatment perforation/rupture (33) acute pseudoaneurysm (10) AV fistula (16) and dissection (3)
28 The Journal of Trauma: Injury, Infection, and Critical Care Issue: Volume 60(6), June 2006, pp Results of a Multicenter Trial for the Treatment of Traumatic Vascular Injury with a Covered Stent White R, Krajcer Z, Johnson M, et al. Results post-procedure exclusion in 58 of 62 cases (93.5%) 1-year exclusion rates % iliac, 90.0% subclavian, and 62.3% femoral 1-year primary patency rates % iliac, 85.7% subclavian, and 85.7% femoral freedom-from-bypass - in 74.3% iliac and 100% femoral and subclavian injuries most common adverse events - stenosis 4.8%, occlusion 7.9% no device- or procedure-related deaths rates and severity of complications - less than those associated with surgical repair
29 29 yo M s/p fall from a bucket truck (height - 7 m) Multiple injuries to the left arm, right leg, and pelvis Evaluation VS: 90/60, 98, 24 downstatesurgery.org The Journal of Trauma: Injury, Infection, and Critical Care Issue: Volume 56(6), June 2004, pp Endovascular Repair of Brachial Artery Transection Associated with Trauma - Case 1 Maynar M, Baro M, Qian Z, et al extensive soft tissue laceration on the left arm and axilla no distal pulses in the LUE left forearm and hand were cold, pale, and edematous multiple fractures in the pelvis and right tibia and fibula
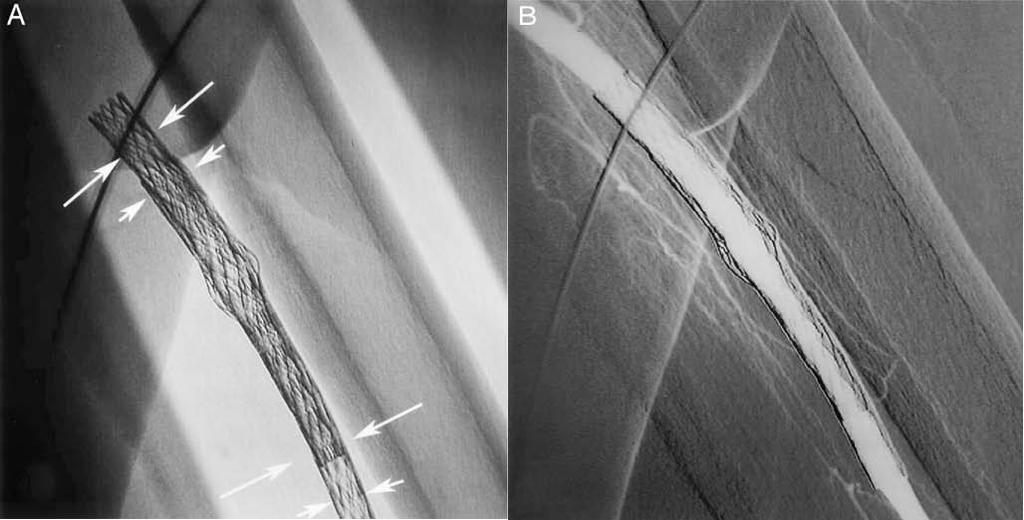
30 The Journal of Trauma: Injury, Infection, and Critical Care Issue: Volume 56(6), June 2004, pp Endovascular Repair of Brachial Artery Transection Associated with Trauma - Case 1 Maynar M, Baro M, Qian Z, et al Angiography - brachial artery transection above elbow with extravasation and non-visualization of distal arteries 6 58-mm Teflon-covered Jostent deployed over a wire Repeat angiogram - no extravasation, distal runoff intact Patient started on LMW heparin for 3 months Immediate return of pulses, increased temperature, shorter capillary refill time, and improved skin color Segmental blood pressure, Doppler ultrasound, tissue oximetry - significant improvement of distal circulation Penetrating wound surgically repaired, ortho repairs, patient continued on antibiotics throughout hospital stay

31
32 The Journal of Trauma: Injury, Infection, and Critical Care Issue: Volume 56(6), June 2004, pp Endovascular Repair of Brachial Artery Transection Associated with Trauma - Case 1 Maynar M, Baro M, Qian Z, et al Patient required repeated LUE wound debridements in OR HD 16 paresthesia/intense pain in left forearm and hand PE - diminished pulse in the left forearm Angiography - complete occlusion at the level of the proximal end of the stent-graft Occluded segment was dilated with angioplasty balloon and a second Jostent was placed over the original one Repeat angiogram showed a fully patent graft with excellent runoff in the radial and ulnar arteries
33
34
35 The Journal of Trauma: Injury, Infection, and Critical Care Issue: Volume 56(6), June 2004, pp Endovascular Repair of Brachial Artery Transection Associated with Trauma - Case 1 Maynar M, Baro M, Qian Z, et al Fibrinolytic therapy was initiated (urokinase) for partially occluded interosseous artery Next day, a patent interosseous artery was demonstrated Discharged from the hospital 8 weeks after the event Last follow-up (7 months) the stent-graft is patent, with good distal runoff Patient remains free of vascular symptoms and continues to receive PT for his injured hand
36 67 yo F s/p fall downstatesurgery.org The Journal of Trauma: Injury, Infection, and Critical Care Issue: Volume 56(6), June 2004, pp Endovascular Repair of Brachial Artery Transection Associated with Trauma - Case 2 Maynar M, Baro M, Qian Z, et al PMH: Parkinson s disease, s/p multiple bilateral shoulder dislocations VS: BP 182/84, HR 95 Conscious but anxious, agitated, pale, and sweating Right axillary hematoma cm Right arm and hand pale, swollen, and pulseless Xray - right shoulder dislocation, no fracture
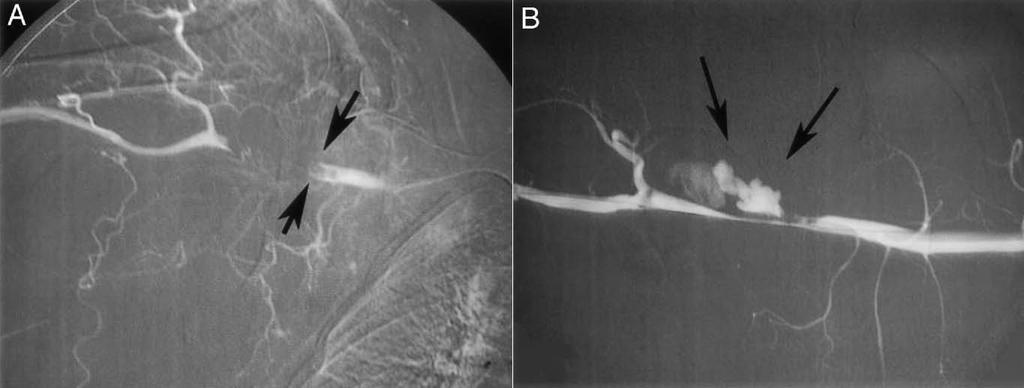
37 The Journal of Trauma: Injury, Infection, and Critical Care Issue: Volume 56(6), June 2004, pp Endovascular Repair of Brachial Artery Transection Associated with Trauma - Case 2 Maynar M, Baro M, Qian Z, et al Angiography - abrupt discontinuation of the right proximal end of the brachial artery with opacification of the distal artery via collaterals (45 mm segment) Attempts to cross the injured segment via femoral approach were unsuccessful A guidewire was advanced to subclavian artery via a retrograde approach from the ipsilateral brachial artery Repeat angiogram - contrast extravasation suggestive of a partial transection
38
39 The Journal of Trauma: Injury, Infection, and Critical Care Issue: Volume 56(6), June 2004, pp Endovascular Repair of Brachial Artery Transection Associated with Trauma - Case 2 Maynar M, Baro M, Qian Z, et al Two covered stents (Jostent) used to repair the injury (6 58 mm and 7 58 mm with 20 mm overlap) Post-procedural angiography - complete bridging of the partially transected brachial artery, no leak Urokinase bolus given for slow distal runoff with improved blood flow after injection Distal pulses, limb temperature, and skin color improved Significant improvement in segmental blood pressure, Doppler ultrasound, and tissue oximetry Patient transferred for orthopedic treatment the next day 1 month post-procedure - excellent flow across the stented segment by Doppler ultrasound

40
41 Conclusion Catheter-based therapy has an increasing role in the management of vascular trauma to the extremity Described areas of treatment of arterial injury with application of covered stents include subclavian, brachial, iliofemoral, and infrageniculate arteries Application of these techniques is fairly new, long-term results remain to be seen Endovascular treatment of arterial lesions should be considered in centers with sufficient experience and available personnel to perform the procedure expediently
Combat Extremity Vascular Trauma
 Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
KNEE DISLOCATION. The most common injury will be an anterior dislocation, and this usually results from a hyperextension mechanism.
 KNEE DISLOCATION Introduction Dislocation of the knee is a severe injury associated with major soft tissue injury and a high incidence of damage to the popliteal artery. There is displacement of the tibia
KNEE DISLOCATION Introduction Dislocation of the knee is a severe injury associated with major soft tissue injury and a high incidence of damage to the popliteal artery. There is displacement of the tibia
Chapter 48 Vascular Trauma
 Chapter 48 Vascular Trauma Episode Overview: 1. List three types/mechanisms of occlusive and four types of non-occlusive vascular injuries. 2. What are the hard and soft signs of peripheral vascular injury?
Chapter 48 Vascular Trauma Episode Overview: 1. List three types/mechanisms of occlusive and four types of non-occlusive vascular injuries. 2. What are the hard and soft signs of peripheral vascular injury?
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Resident Teaching Conference 3/12/2010
 Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
Epidemiology. 16% incidence in knee. dislocation
 Epidemiology Highest risk group: Young male between 15 and 45 years (USA) Mortality Ratio after trauma : male/female: 7/1 Peripheral vascular injuries : 70%-80% of all cases of vascular trauma : Vascular
Epidemiology Highest risk group: Young male between 15 and 45 years (USA) Mortality Ratio after trauma : male/female: 7/1 Peripheral vascular injuries : 70%-80% of all cases of vascular trauma : Vascular
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
A BULLET TO THE CHEST
 Originally Posted: October, 01, 2014 A BULLET TO THE CHEST Resident: Gustavo A. Elias, MD Attendings: Gordon S. Morano, MD; Brian J. Strife, MD; Daniel J. Komorowski, MD; Malcolm K. Sydnor, MD Program/Dept:
Originally Posted: October, 01, 2014 A BULLET TO THE CHEST Resident: Gustavo A. Elias, MD Attendings: Gordon S. Morano, MD; Brian J. Strife, MD; Daniel J. Komorowski, MD; Malcolm K. Sydnor, MD Program/Dept:
Vascular Injuries. Chapter 27
 Vascular Injuries Chapter 27 Vascular Injuries Introduction History. ο World War II: Popliteal artery injuries were routinely ligated with a 73% amputation rate. ο Korean War: Formal repair of peripheral
Vascular Injuries Chapter 27 Vascular Injuries Introduction History. ο World War II: Popliteal artery injuries were routinely ligated with a 73% amputation rate. ο Korean War: Formal repair of peripheral
Mangled Extremity and Vascular Repair. Jason Sulkowski, MD
 Mangled Extremity and Vascular Repair Jason Sulkowski, MD Case Presentation 9:50AM 34 y F BIBEMS as pedestrian struck, + LOC, GCS 15 in field Primary Survey: A: intact, speaking B: bilateral breath sounds,
Mangled Extremity and Vascular Repair Jason Sulkowski, MD Case Presentation 9:50AM 34 y F BIBEMS as pedestrian struck, + LOC, GCS 15 in field Primary Survey: A: intact, speaking B: bilateral breath sounds,
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of June 4, 2018 Thrombolysis, Thrombectomy & Angioplasty
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of June 4, 2018 Thrombolysis, Thrombectomy & Angioplasty
Case 37 Clinical Presentation
 Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Evaluation & Management of Penetrating Wounds to the NECK
 Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
PEDIATRIC PENETRATING TRAUMA. Laura Boomer 11/18/15
 PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
Social History. Retired internist 2 scotches a day 50 pack-year history, stopped in 2005
 April 17, 2008 HPI 78 year old internist complains of 10 days of tingling and discomfort in left toes Unable to walk or sleep due to severe pain Pain worse with movement Redness in left toes Bilateral
April 17, 2008 HPI 78 year old internist complains of 10 days of tingling and discomfort in left toes Unable to walk or sleep due to severe pain Pain worse with movement Redness in left toes Bilateral
Traumatic A-V A V Fistula
 Traumatic A-V A V Fistula PRESENT HISTORY PAST HISTORY 30 year-old, male ( XX); Denied other systemic disease before. PRESENT HISTORY A deep stabbing wound (3*1 cm) noted on 07/01/2002 over Right anterior
Traumatic A-V A V Fistula PRESENT HISTORY PAST HISTORY 30 year-old, male ( XX); Denied other systemic disease before. PRESENT HISTORY A deep stabbing wound (3*1 cm) noted on 07/01/2002 over Right anterior
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die
 account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
SCAI Fall Fellows Course Subclavian/Innominate Case Presentation
 SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Crash, Bonk, Thud! (Trauma Case Studies) John Beuerle, M.D.
 John Beuerle, M.D.") Crash, Bonk, Thud! (Trauma Case Studies) John Beuerle, M.D. Case 1 (22 y.o. female, wakeboarding injury) Case 1 (22 y.o. female, wakeboarding injury) Arrives via EMS cc: left leg injury HPI: Patient
Crash, Bonk, Thud! (Trauma Case Studies) John Beuerle, M.D. Case 1 (22 y.o. female, wakeboarding injury) Case 1 (22 y.o. female, wakeboarding injury) Arrives via EMS cc: left leg injury HPI: Patient
How to Triage Orthopaedic Care. David W. Gray, M.D.
 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
PEARL Registry Update Overview Venous Arterial AV Access
 PEARL Registry Update Overview Venous Arterial AV Access PEARL Registry Overview (as of 10 Sep12*) Overview Venous Arterial AV Access HOME Topic Data Support Comments Study Design Prospective, non-randomized,
PEARL Registry Update Overview Venous Arterial AV Access PEARL Registry Overview (as of 10 Sep12*) Overview Venous Arterial AV Access HOME Topic Data Support Comments Study Design Prospective, non-randomized,
Non-invasive examination
 Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
PUT YOUR BEST FOOT FORWARD
 PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm
 Case Reports in Vascular Medicine, Article ID 716752, 4 pages http://dx.doi.org/10.1155/2014/716752 Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm Ahsan Syed Khalid,
Case Reports in Vascular Medicine, Article ID 716752, 4 pages http://dx.doi.org/10.1155/2014/716752 Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm Ahsan Syed Khalid,
Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft
 MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
Georgia Vascular Society 6th Annual Scientific Sessions September 14 16, 2018 Ritz-Carlton Reynolds, Lake Oconee Greensboro, GA
 The Gamete of Pediatric Vascular Surgery: One Surgeon s Experience Georgia Vascular Society 6th Annual Scientific Sessions September 14 16, 2018 Ritz-Carlton Reynolds, Lake Oconee Greensboro, GA Mohammed
The Gamete of Pediatric Vascular Surgery: One Surgeon s Experience Georgia Vascular Society 6th Annual Scientific Sessions September 14 16, 2018 Ritz-Carlton Reynolds, Lake Oconee Greensboro, GA Mohammed
Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents
 Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents Jesus Contreras, D.O. PGY-4 John Yasmer, D.O. Department of Radiology No Disclosures Objectives Introduce
Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents Jesus Contreras, D.O. PGY-4 John Yasmer, D.O. Department of Radiology No Disclosures Objectives Introduce
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of October 29, 2018 Mesenteric Arteriogram & Thrombectomy/Thrombolysis
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of October 29, 2018 Mesenteric Arteriogram & Thrombectomy/Thrombolysis
Arterial Map of the Thorax, Abdomen and Pelvis 2017 Edition
 Arterial Map of the Thorax, Abdomen and Pelvis Angiography 75605 (-26) Aortography, thoracic 75625 (-26) Aortography, abdominal by serialography 75630 (-26) Aortography, abdominal + bilat iliofemoral 75705
Arterial Map of the Thorax, Abdomen and Pelvis Angiography 75605 (-26) Aortography, thoracic 75625 (-26) Aortography, abdominal by serialography 75630 (-26) Aortography, abdominal + bilat iliofemoral 75705
Indications: following: embolization. artery that has diseases 5. The evaluation. of suspected. such entities. a cold hand. biopsy
 Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Bare Metal Stents vs Stent Grafts
 Bare Metal Stents vs Stent Grafts ASDIN 12th Annual Scientific Meeting Phoenix, AZ, February 20, 2016 Dirk Hentschel, MD Director, Interventional Nephrology Brigham and Women s Hospital Disclosure Consultant:
Bare Metal Stents vs Stent Grafts ASDIN 12th Annual Scientific Meeting Phoenix, AZ, February 20, 2016 Dirk Hentschel, MD Director, Interventional Nephrology Brigham and Women s Hospital Disclosure Consultant:
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Introduction 3. What is Peripheral Vascular Disease? 5. What Are Some of the Symptoms of Peripheral Vascular Disease? 6
 Patient Information Table of Contents Introduction 3 What is Peripheral Vascular Disease? 5 What Are Some of the Symptoms of Peripheral Vascular Disease? 6 What Causes Peripheral Vascular Disease? 7 How
Patient Information Table of Contents Introduction 3 What is Peripheral Vascular Disease? 5 What Are Some of the Symptoms of Peripheral Vascular Disease? 6 What Causes Peripheral Vascular Disease? 7 How
Arterial Access for Diagnosis and Intervention T-Woei Tan, MD, FACS
 Arterial Access for Diagnosis and Intervention T-Woei Tan, MD, FACS Assistant Professor of Surgery Vascular Endovascular Surgery Louisiana State University Health - Shreveport Disclosures None Objective
Arterial Access for Diagnosis and Intervention T-Woei Tan, MD, FACS Assistant Professor of Surgery Vascular Endovascular Surgery Louisiana State University Health - Shreveport Disclosures None Objective
Pediatric emergencies. Emergent Neuroimaging Acute chest (non-trauma) Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma
 Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma") Department of Clinical Radiology, Munich University Hospital Pediatric emergencies Emergent Neuroimaging Acute chest (non-trauma) Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma
Department of Clinical Radiology, Munich University Hospital Pediatric emergencies Emergent Neuroimaging Acute chest (non-trauma) Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma
7/23/2018 DESCRIBING THE FRACTURE. Pattern Open vs closed Location BASIC PRINCIPLES OF FRACTURE MANAGEMENT. Anjan R. Shah MD July 21, 2018.
 BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
ADDITIONS. The following codes have been added.
 ADDITIONS The following codes have been added. 99446 Interprofessional telephone/internet assessment and management service provided by treating/requesting physician or other qualified health care professional;
ADDITIONS The following codes have been added. 99446 Interprofessional telephone/internet assessment and management service provided by treating/requesting physician or other qualified health care professional;
Management of Brachial Plexus & Peripheral Nerves Blast Injuries. First Global Conflict Medicine Congress
 Management of Brachial Plexus & Peripheral Nerves Blast Injuries Joseph BAKHACH First Global Conflict Medicine Congress Hand & Microsurgery Department American University of Beirut Medical Centre Brachial
Management of Brachial Plexus & Peripheral Nerves Blast Injuries Joseph BAKHACH First Global Conflict Medicine Congress Hand & Microsurgery Department American University of Beirut Medical Centre Brachial
Aortoiliac occlusive disease
 Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
DISCLOSURE TEST YOUR WAVEFORM IQ. Partial volume artifact. 86 yo female with right arm swelling, picc line. AVF on left? Dx?
 Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Access (Antegrade, Retrograde, Pedal)
") Access (Antegrade, Retrograde, Pedal) ARCH St. Louis Craig M. Walker, MD, FACC, FACP Clinical Professor of Medicine Tulane University School of Medicine New Orleans, LA Clinical Professor of Medicine LSU
Access (Antegrade, Retrograde, Pedal) ARCH St. Louis Craig M. Walker, MD, FACC, FACP Clinical Professor of Medicine Tulane University School of Medicine New Orleans, LA Clinical Professor of Medicine LSU
Axillary artery lesions from humeral neck fracture: A study in relation to repair
 328 Axillary artery lesions from humeral neck fracture: A study in relation to repair QUAN ZHANG 1, SHILONG WANG 1, CHAOLIANG TANG 1, WENJUN CHEN 1, YE ZHANG 1 and LIN CHEN 2 Departments of 1 Orthopaedic
328 Axillary artery lesions from humeral neck fracture: A study in relation to repair QUAN ZHANG 1, SHILONG WANG 1, CHAOLIANG TANG 1, WENJUN CHEN 1, YE ZHANG 1 and LIN CHEN 2 Departments of 1 Orthopaedic
Proximal Humerus Fractures
 Proximal Humerus Fractures Trafford General Hospital, June 2010 Nehmat Singh, Jawad Sultan Anatomy of the Proximal Humerus Consists of four parts: humeral head, surgical neck and greater and lesser tubercles
Proximal Humerus Fractures Trafford General Hospital, June 2010 Nehmat Singh, Jawad Sultan Anatomy of the Proximal Humerus Consists of four parts: humeral head, surgical neck and greater and lesser tubercles
2018 CPT CODING CHANGES
 17 2018 CPT coding changes by Samuel Smith, MD, FACS; Megan McNally, MD, FACS; and Jan Nagle, MS, RPh JAN 2018 BULLETIN American College of Surgeons 18 Significant changes in Current Procedural Terminology
17 2018 CPT coding changes by Samuel Smith, MD, FACS; Megan McNally, MD, FACS; and Jan Nagle, MS, RPh JAN 2018 BULLETIN American College of Surgeons 18 Significant changes in Current Procedural Terminology
Introduction What Causes Peripheral Vascular Disease? How Do Doctors Treat Peripheral Vascular Disease?... 9
 Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Schedule of Benefits. for Professional Fees Vascular Procedures
 Schedule of Benefits for Professional Fees 2018 Vascular Procedures ANASTOMOSIS RULES 820 Arteriovenous anastomosis in arm 1453 Arteriovenous anastomosis, open by basilic vein transposition 1465 Splenorenal
Schedule of Benefits for Professional Fees 2018 Vascular Procedures ANASTOMOSIS RULES 820 Arteriovenous anastomosis in arm 1453 Arteriovenous anastomosis, open by basilic vein transposition 1465 Splenorenal
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
Basic Care of Common Fractures Utku Kandemir, MD
 Basic Care of Common Fractures Utku Kandemir, MD Assistant Clinical Professor Trauma & Sports Medicine Dept. of Orthopaedic Surgery UCSF / SFGH History Physical Exam Radiology Treatment History Acute trauma
Basic Care of Common Fractures Utku Kandemir, MD Assistant Clinical Professor Trauma & Sports Medicine Dept. of Orthopaedic Surgery UCSF / SFGH History Physical Exam Radiology Treatment History Acute trauma
Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles
 1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Intended Learning Outcomes
 2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
Morbidity Audit and Logbook Tool SNOMED Board Reporting Terms for SET and IMG Vascular Surgery AMPUTATION AORTA
 SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
Mohammad Ayati,M.D Department of Orthopaedics, Yazd University of Medical Science.
 IN THE NAME OF GOD Mohammad Ayati,M.D Department of Orthopaedics, Yazd University of Medical Science. Devastating injury resulting from : high-energy usually from MVC or fall from height commonly a dashboard
IN THE NAME OF GOD Mohammad Ayati,M.D Department of Orthopaedics, Yazd University of Medical Science. Devastating injury resulting from : high-energy usually from MVC or fall from height commonly a dashboard
CY2017 Hospital Outpatient: Vascular Procedure APCs and Complexity Adjustments
 CY2017 Hospital Outpatient: Vascular Procedure APCs and Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) In CY2015 and in an effort to help pay providers for quality, not
CY2017 Hospital Outpatient: Vascular Procedure APCs and Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) In CY2015 and in an effort to help pay providers for quality, not
Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease
 Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease Arash Bornak, MD FACS Vascular & Endovascular Surgery University of Miami Miller School of Medicine No disclosure BACKGROUND
Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease Arash Bornak, MD FACS Vascular & Endovascular Surgery University of Miami Miller School of Medicine No disclosure BACKGROUND
Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Case 1:
 12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
12/16/2015 Not all Leg DVT s are the Same: Which Patients Benefit from Interventional Therapy? Constantino S.Peña, FSIR, FSCCT, FAHA Interventional Radiologist Medical Director, Vascular Imaging Miami
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles. Striated Skeletal. Smooth
 1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
Sample page. POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
 2018 Complete Guide for Interventional Radiology An in-depth guide to interventional radiology coding, billing, and reimbursement for facilities and physicians POWER UP YOUR CODING with Optum360, your
2018 Complete Guide for Interventional Radiology An in-depth guide to interventional radiology coding, billing, and reimbursement for facilities and physicians POWER UP YOUR CODING with Optum360, your
An unusual shoulder injury
 An unusual shoulder injury Authors: AJ Moss, D Valenti, SC Fraser, J Murie Location: Queen Elizabeth Hospital, Norfolk, UK Citation: Moss AJ, Valenti D, Fraser S, Murie J. An unusual shoulder injury. 2011.
An unusual shoulder injury Authors: AJ Moss, D Valenti, SC Fraser, J Murie Location: Queen Elizabeth Hospital, Norfolk, UK Citation: Moss AJ, Valenti D, Fraser S, Murie J. An unusual shoulder injury. 2011.
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Disclosure. Pediatric Orthopedic Emergencies. I have no actual or potential conflict of interest in relation to this program or presentation.
 Pediatric Orthopedic Emergencies Robin Pearce MSN, RN-BC Trauma Performance Improvement Manager Henrico Doctors Hospital, Forest Disclosure I have no actual or potential conflict of interest in relation
Pediatric Orthopedic Emergencies Robin Pearce MSN, RN-BC Trauma Performance Improvement Manager Henrico Doctors Hospital, Forest Disclosure I have no actual or potential conflict of interest in relation
YOU MUST BRING GLOVES FOR THIS ACTIVITY
 ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 5e. All text references are for this textbook. 2) Observe and sketch histology slide
ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 5e. All text references are for this textbook. 2) Observe and sketch histology slide
VESSELS: GROSS ANATOMY
 ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
Primary to non-coronary IVUS
 codes 2018 2018 codes Primary to non-coronary IVUS Page 2 All coding, coverage, billing and payment information provided herein by Philips is gathered from third-party sources and is subject to change.
codes 2018 2018 codes Primary to non-coronary IVUS Page 2 All coding, coverage, billing and payment information provided herein by Philips is gathered from third-party sources and is subject to change.
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Infected Lower Extremity Aneurysms C. Stefan Kénel-Pierre, MD
 Infected Lower Extremity Aneurysms C. Stefan Kénel-Pierre, MD University Hospital of Brooklyn Department of Surgery History 52F c PMHx of HTN, asthma p/w fever, malaise s/p one week of ABx for presumed
Infected Lower Extremity Aneurysms C. Stefan Kénel-Pierre, MD University Hospital of Brooklyn Department of Surgery History 52F c PMHx of HTN, asthma p/w fever, malaise s/p one week of ABx for presumed
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
5/24/16. Matthew Rennels, DO Ryan Szepiela, MD Promedica Toledo Hospital Primary Care Sports Medicine Fellowship
 Matthew Rennels, DO Ryan Szepiela, MD Promedica Toledo Hospital Primary Care Sports Medicine Fellowship! The patient is a 26-year-old male professional baseball pitcher (righthanded) who presented with
Matthew Rennels, DO Ryan Szepiela, MD Promedica Toledo Hospital Primary Care Sports Medicine Fellowship! The patient is a 26-year-old male professional baseball pitcher (righthanded) who presented with
Step by step Hybrid procedures in peripheral obstructive disease. Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery
 Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Upper Extremity Venous Duplex. Michigan Sonographers Society Fall Ultrasound Symposium October 15, 2016
 Upper Extremity Venous Duplex Michigan Sonographers Society Fall Ultrasound Symposium October 15, 2016 Patricia A. (Tish) Poe, BA RVT FSVU Director of Quality Assurance Navix Diagnostix Patricia A. Poe
Upper Extremity Venous Duplex Michigan Sonographers Society Fall Ultrasound Symposium October 15, 2016 Patricia A. (Tish) Poe, BA RVT FSVU Director of Quality Assurance Navix Diagnostix Patricia A. Poe
Traumatic Posterior Tibial Pseudoaneursym: A rare late complication repaired conventionally
 Volume 2 Issue 3 Article 3 2016 Traumatic Posterior Tibial Pseudoaneursym: A rare late complication repaired conventionally Farzad Amiri, MD; Zachary Sanford; and Constantinous Constantinou, MD Follow
Volume 2 Issue 3 Article 3 2016 Traumatic Posterior Tibial Pseudoaneursym: A rare late complication repaired conventionally Farzad Amiri, MD; Zachary Sanford; and Constantinous Constantinou, MD Follow
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury. Conflict of Interest. Hypotensive shock 5/5/2014. none
 EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
CY2015 Hospital Outpatient: Endovascular Procedure APCs and Complexity Adjustments
 CY2015 Hospital Outpatient: Endovascular Procedure APCs Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) CMS finalized the implementation of 25 Comprehensive APC to further
CY2015 Hospital Outpatient: Endovascular Procedure APCs Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) CMS finalized the implementation of 25 Comprehensive APC to further
Upper Extremity Fractures
 Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Presented at 2015 TQIP conference. Developed by a panel of experts. Evidence based with expert opinion as needed
 Presented at 2015 TQIP conference Developed by a panel of experts Evidence based with expert opinion as needed Orthopaedic Trauma Best Practice Guidelines (BPG) Goals Offer guidance on what is practical
Presented at 2015 TQIP conference Developed by a panel of experts Evidence based with expert opinion as needed Orthopaedic Trauma Best Practice Guidelines (BPG) Goals Offer guidance on what is practical
Vascular Emergencies. Scott M Surowiec, MD Assistant Professor of Surgery Upstate Vascular and Crouse Hospital September 29, 2015
 Vascular Emergencies Scott M Surowiec, MD Assistant Professor of Surgery Upstate Vascular and Crouse Hospital September 29, 2015 Introduction Main vascular emergencies include Ruptured Abdominal Aortic
Vascular Emergencies Scott M Surowiec, MD Assistant Professor of Surgery Upstate Vascular and Crouse Hospital September 29, 2015 Introduction Main vascular emergencies include Ruptured Abdominal Aortic
Case. 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds
 Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Compartment Syndrome
 Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Peripheral Arterial Disease: A Practical Approach
 Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Vascular Surgery Cases: Detours. Brian F. Stull, RDMS, RVT UNC REX Healthcare Vascular Specialists
 Vascular Surgery Cases: Detours Brian F. Stull, RDMS, RVT UNC REX Healthcare Vascular Specialists Brian.Stull@Unchealth.unc.edu Objectives Anatomy of a bypass graft Where does it connect, where does it
Vascular Surgery Cases: Detours Brian F. Stull, RDMS, RVT UNC REX Healthcare Vascular Specialists Brian.Stull@Unchealth.unc.edu Objectives Anatomy of a bypass graft Where does it connect, where does it
Goals. Initial management skeletal trauma. Physical Exam ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT 12/4/2010
 ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm
 Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case
PROXIMAL HUMERUS FRACTURE TSHT 2017
 PROXIMAL HUMERUS FRACTURE TSHT 2017 ANIL DUTTA, M.D. ASSOCIATE PROFESSOR Displacement > 1 cm Angulation > 45 degree SHOULDER AND ELBOW SURGERY UNIVERSITY OF TEXAS HEALTH SCIENCE CENTER SAN ANTONIO DISCLOSURE
PROXIMAL HUMERUS FRACTURE TSHT 2017 ANIL DUTTA, M.D. ASSOCIATE PROFESSOR Displacement > 1 cm Angulation > 45 degree SHOULDER AND ELBOW SURGERY UNIVERSITY OF TEXAS HEALTH SCIENCE CENTER SAN ANTONIO DISCLOSURE
Access Preservation: Recurrent Central Venous Stenosis, Pacemaker Wires and other Nightmares. Who am I? Disclosures
 Access Preservation: Recurrent Central Venous Stenosis, Pacemaker Wires and other Nightmares Jason Burgess, MD RVT Surgical Specialists of Charlotte CMC-Mercy Charlotte, NC Disclosures Gore Vascular- Consultant
Access Preservation: Recurrent Central Venous Stenosis, Pacemaker Wires and other Nightmares Jason Burgess, MD RVT Surgical Specialists of Charlotte CMC-Mercy Charlotte, NC Disclosures Gore Vascular- Consultant
Anesthesia Cross Coder. Essential links from CPT codes to ICD-9-CM and HCPCS codes
 Anesthesia Cross Coder Essential links from CPT codes to ICD-9-CM and HCPCS codes 2009 Contents Introduction... i CPT Anesthesia to Procedure Crosswalk...i Format...i Icon Key...ii CPT Codes...ii Code
Anesthesia Cross Coder Essential links from CPT codes to ICD-9-CM and HCPCS codes 2009 Contents Introduction... i CPT Anesthesia to Procedure Crosswalk...i Format...i Icon Key...ii CPT Codes...ii Code
Coding Changes for 2018
 Coding Changes for 2018 An overview of changes to interventional CPT coding that you need to know for practicing in 2018. BY KATHARINE L. KROL, MD, FSIR, FACR There are several coding changes for endovascular
Coding Changes for 2018 An overview of changes to interventional CPT coding that you need to know for practicing in 2018. BY KATHARINE L. KROL, MD, FSIR, FACR There are several coding changes for endovascular