Pediatric Trauma. July 27 th, Suzana Buac, PGY4. Dr. Neil Merritt
|
|
|
- Jeffery Paul
- 6 years ago
- Views:
Transcription
1 Pediatric Trauma July 27 th, Suzana Buac, PGY4 Dr. Neil Merritt
2 Case
3 5yoM fall from roof Fall from roof of home while father was shingling
4 5yoM fall from roof Fall from roof of home while father was shingling, 8 ft. high No loss of consciousness, ambulating immediately after injury, actual fall not witnessed Previously healthy No home meds, no allergies, immunizations up to date
5 Speaking, airway protected, patent GAEB, trachea midline, 98%SpO2 on RA HR 115, BP 111/65, FAST Positive, Abdomen tender diffusely, guarding Bilateral tenderness/edema/bruising at wrists
6 CT head, c-spine, C/A/P Head/C-spine/Thorax no injury Segment 7/8 Liver Grade 4 laceration, extravasation of contrast, free fluid
7 Objectives
8 Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most common injuries occurring in various age groupings. 2. Identify unique anatomic or physiologic differences in children, when compared to adult patients. 3. Discuss the components of the primary survey in the pediatric trauma patient 4. Outline the secondary survey, and identify controversies in pediatric shock trauma management 5. Differentiate between mild, moderate, and severe head injuries in children
9 Objectives Medical Expert 6. Describe unique traumatic injuries to the spine that occur in children and measures to treat these injuries 7. Differentiate the types of cardiothoracic trauma, and list appropriate management of each type 8. Identify signs, symptoms, and management of pediatric abdominal and genitourinary trauma 9. Recognize the risks and appropriate management of traumatic amputation and soft tissue trauma in children 10. Recognize the risks and appropriate interventions in the management of orthopedic pediatric trauma
10 Objectives - Collaborator 1. Understand the post injury components of care for pediatric trauma patients 2. Describe the levels of pediatric trauma care and how to prepare an ER for treatment of the injured child
11 Objectives Health Advocate 1. Describe the impact of pediatric trauma on Canadian society and healthcare. 2. Identify the importance of pain management with practical strategies for managing pain in pediatric trauma patients 3. Outline the role of family centered care in pediatric trauma
12 Objectives - Scholar 1. Identify and understand the implications of one recent sentinel paper in pediatric trauma care
13 Pediatric Trauma
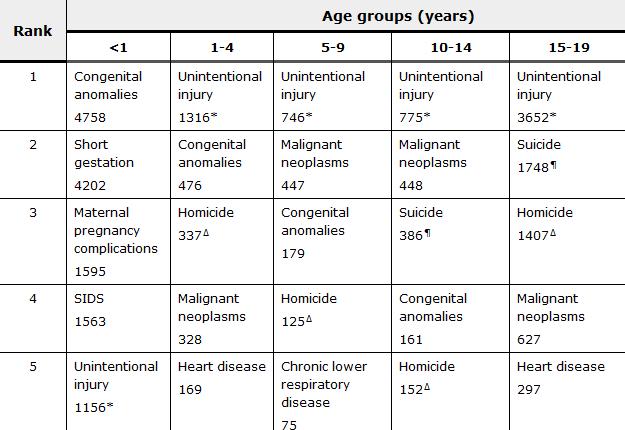
14 Background Trauma is the leading cause of death in children and adolescents Most due to preventable injuries For every injury mortality, estimated 25 hospitalizations and 925 emergency room visits Leading cause of years of life lost Leading cause of medical costs Emotional trauma for parents and families
15 Background Injury prevention through awareness and increased safety measures has lead to the reduction in death from trauma in Canada Seatbelts Vehicle Design Car seats Reduction in drunk driving Child resistant packaging Safety awareness Improved medical care
16
17 Mortality Incident Change Motor vehicle 3,587 2,431 32% crash Drowning 1, % Pedestrian injury 1, % Fire and/or burn 1, % injury Suffocation % Falls % Poisoning % Firearm %
18
19
20 Approach to injured child
21 ATLS Based on trimodal death distribution First peak seconds to minutes immediately after injury (only prevention can affect mortality) Second peak minutes to hours rapid assessment and treatment can improve mortality Third peak days to weeks multi-organ system failure definitive care at specialized pediatric center may mitigate delayed mortality
22 Injury classification Many pediatric trauma classification systems used to predict mortality, morbidity, resources, operative intervention, etc. GCS, Trauma Score, Revised Trauma Score, Pediatric Trauma Score, Age-specific pediatric trauma score, Anatomic systems, abbreviated injury scale, injury severity score, mechanism, etc. Objectives are in 1) triage decision support in prehospital setting and 2) predicting severity of illness and mortality
23 Injury classification Extent multiple (two or more body areas) vs. localized; may be obvious or evolve over time Type blunt vs. penetrating Severity mechanism of injury, vita signs, physical exam findings
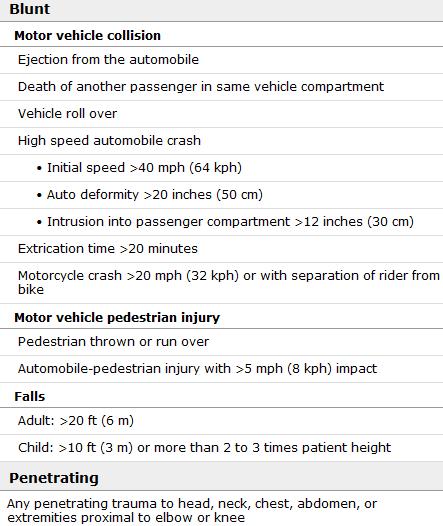
24 Mechanism

25 Physical findings
26 Goals Rapidly assess injuries, determine management priorities, provide critical interventions Primary survey, resuscitation, adjuncts to primary survey, secondary survey, continued resuscitation and monitoring, adjuncts to secondary survey, transition to definitive care
27 What is different about children?
28 ANATOMY
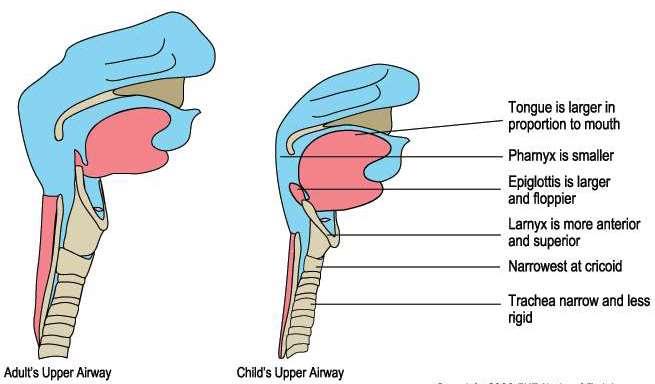
29 Airway Differences from adult airways: 1. small oral cavity and large tongue - obstruction 2. large occiput, neck flexion obstruction, c-spine 3. larynx cephalad/anterior, floppy epiglottis 4. short narrow trachea, narrow distance between rings
30 Airway What is the narrowest point in the pediatric airway? Would you use a cuffed or un-cuffed tube?
31 Airway
32 Breathing More or less compliant than adult?
33 Diaphragmatic Breathing
34 Summary Anatomy PEDIATRIC ADULT Tongue Large Normal Epiglottis Shape Floppy, omega shaped Firm, flatter Epiglottis Level Level of C3 - C4 Level of C5 - C6 Trachea Smaller, shorter Wider, longer Larynx Shape Funnel shaped Column Larynx Position Angles posteriorly away Straight up and down from glottis Narrowest Point Sub-glottic region At level of Vocal cords Lung Volume 250ml at birth 6000 ml as adult
35 Abdomen Thin abdominal wall Which two organs are more likely to be injured in children? Which organ is intra-abdominal in infants but not adults?
36 Bones When do children reach skeletal maturity? Why is this important?

37 Bones What is a green stick fracture? Why do they occur in children and not adults?

38 Skull When do anterior fontanelles close?
39 General Smaller size increased likelihood for injury to multiple organ systems Higher metabolic rate and larger surface area to body-mass ratio increased heat loss
40 What is different about children?
41 PHYSIOLOGY
42 Circulation Blood volume is larger but absolute volume is smaller A relatively small amount of blood loss can be a significant % of total blood volume Need to record even small volume loses you might ignore in an adult
43 Circulation Fixed Stroke Volume in infants Hypotension is a late sign of shock. What s a better indicator?

44 Normal Vitals

45 Shock
46 Intravenous Fluids Access is typically more challenging in pediatrics How much fluid to give? What kind?
47 Access/Fluids
48 Head/Spinal Injury
49 Head Leading cause of death from trauma leading to significant lifelong disability However, over 80% are mild traumatic brain injury Classification: Mild (Ped-GCS 13-15) Moderate (Ped-GCS 9-12) Severe (Ped-GCS <8)
50 Head - Management Principles: Airway Avoiding hypoxia (02) Avoiding hypotension Ensuring adequate resuscitation ICP monitoring in those with severe head injury Raised ICP: Hypertonic saline 0.1-1cc/kg Mannitol cc/kg
51 Spine Very rare in children younger than 17 year olds C2 lesions in young, C4 in teen (A-O dislocation) Mechanism MVC in young, sports in teens SCIWORA need high suspicion of injury (PH Exam) Neurologic Recovery Likely better compared to adult population No evidence for hypothermia/steroids
52 Case
53 15 yom ATV crash from community Not helmeted, thrown off ATV, landed on right side No loss of consciousness, but amnesia Taken to community ER, HD stable, Chest Xray showed right pneumo/haemo, chest tube placed (750mL blood) Transferred to LHSC Peds Emerg
54 Healthy, allergy to penicillin Airway patent, protected, speaking Decreased AE on the right, midline trachea, no sub/q emphysema, 96% on 5L, continuous air leak No further blood drained on transfer, HR 110, BP 132/90, abdomen soft, no obvious long bone fractures, FAST negative, peripheral pulses palpable PEARL. GCS 15.

55 CT scan C/A/P Right pneumothorax Right lung contusion Grade 1 liver laceration Bilateral scapular fractures
56 Cardiothoracic
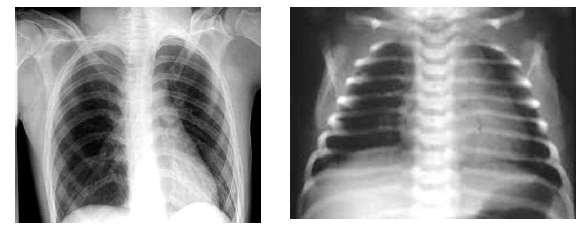
57 Thoracic Much less common secondary to small size Approximately 6%, almost all of which are blunt 3:1 male to female ratio Greater flexibility results in more pulmonary contusions or pneumatoceles with no rib fractures 30-40% of injuries are missed on initial CXR Vast majority only require observation or chest tube
58 Thoracic Hemothorax or Pneumothorax Clinical findings of a tension pneumothorax may be impressive (mobile mediastinum) Nipple Level
59 Thoracic Rib # Marker of energy transfer OR child abuse 1 st or 2 nd rib fractures raise suspicion for vascular injury Management Analgesia Suspicion of pulmonary contusion if deteriorating
60 Abdominal
61 Case
62 5yoM fall from 8 ft height Fall from roof of home while father was shingling No loss of consciousness, ambulating immediately after injury, actual fall not witnessed Previously healthy
63 Speaking, airway protected, patent GAEB, trachea midline, 98%SpO2 on RA HR 115, BP 111/65, FAST Positive, Abdomen tender diffusely, guarding Bilateral tenderness/edema/bruising at wrists

64 CT head, c-spine, C/A/P Head/C-spine/Thorax no injury Segment 7/8 Liver Grade 4 laceration, extravasation of contrast, free fluid
65 Abdominal Solid Organs 8-12% of pediatric trauma Spleen and liver most common Current management is largely non-operative (>90% success even in high grade injuries) Management Non-operative Continued instability operating room for laparotomy, control of bleeding and packing

66 Abdominal Solid Organs
67 Abdominal Hollow Viscous Injury Crush, burst and sheer injuries Rapid contamination of abdominal cavity Serial physical exams are more sensitive than CT Management Early recognition and repair are key High index of suspicion in unwell patients
68 Pain Management
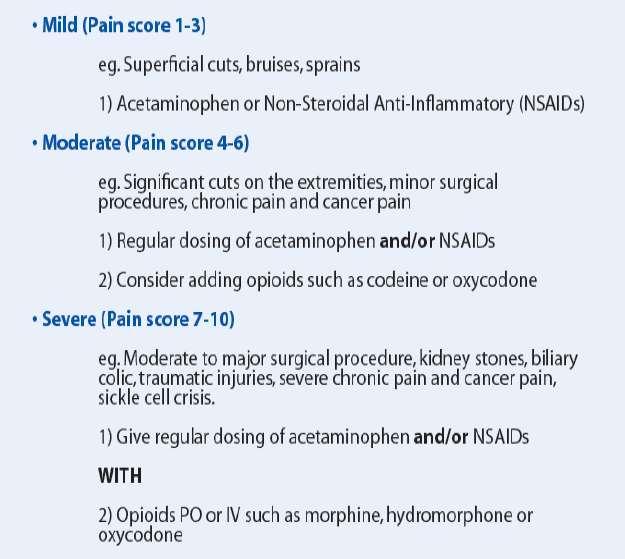
69 Pain
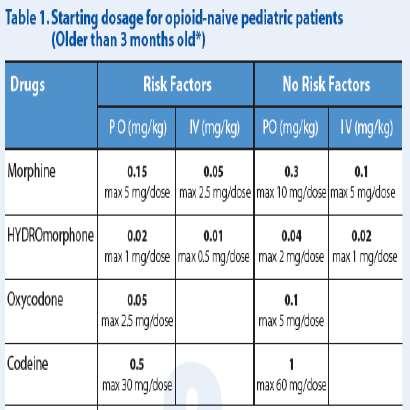
70 Pain
71 Papers for Discussion
72
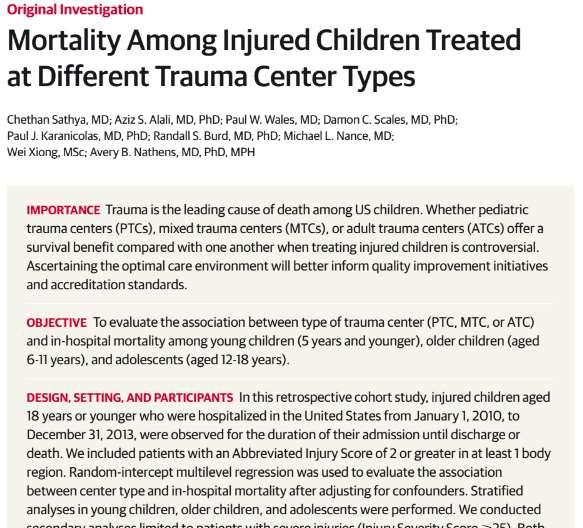
73 Sathya et al 2015 Retrospective cohort study of children 18 and younger in US from Jan 2010 to Dec 2013 of Abbreviated Injury Score 2 or higher from 252 Level I and II trauma centers participating in the Trauma Quality Improvement Program Compared in hospital mortality in children treated at adult trauma centers, mixed trauma centers, pediatric trauma centers
74 Sathya et al 2015 Performed multilevel regression analysis to evaluate association between center type and mortality Also did stratified analysis in different ages Secondary analyses in patients with severe injuries (ISS over 25)
75 Sathya et al 2015 After adjustment, children had higher mortality at ATCs and MTCs than PTCs Younger children had this association but not older children or adolescents Similar results for severely injured children
76
77 Webman et al 2016 Differences in mortality between different trauma centers have not previously been consistent for adolescents Data from National Trauma Bank using injured adolescents from 2010 in Level I and II trauma centers Multilevel models accounting for center specific effects Mortality was higher among adolescents treated at ATCs and MTCs rather than PTCs
78 Questions?

79 Drugs in Pediatric Trauma
80 Case 1
")
81 Case 1 8 yom helmeted cyclist struck by car Unresponsive on arrival, tachypnea with pale, dusky extremities HR 144 RR 38 BP 84/60 GCS 5 (E = 1; V = 2; M = 2)

82 What is the most common cause of cardiac arrest in pediatric trauma?
 + 4 Predicted Size for Cuffed Tube = (Age / 4)")
83 Endotrachial Tubes Predicted Size for Un-cuffed Tube = (Age / 4) + 4 Predicted Size for Cuffed Tube = (Age / 4) + 3
Pediatric Trauma. Sept 2nd, Patrick Murphy Neil Merritt
 Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Paediatric Trauma. A/Prof Drew Richardson. The Canberra Hospital May MB BS (Hons) FACEM Grad CertHE MD
 FACEM Grad CertHE MD") Paediatric Trauma A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Identify unique anatomic and physiologic characteristics of injured children Describe
Paediatric Trauma A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Identify unique anatomic and physiologic characteristics of injured children Describe
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Trauma Registry Documentation December 16, 2014
 Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Cases from the Streets. Kelly Buchanan MD, ATC/L EMS Fellow December, 2011
 Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Pediatric Trauma Karim Rafaat, MD
 Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
Objectives. Review ATLS from the pediatric perspective Convince you that children aren t simply little. Impress you with my Power Point mastery
 Pediatric Trauma Objectives Review ATLS from the pediatric perspective Convince you that children aren t simply little adults (especially when it comes to trauma) Impress you with my Power Point mastery
Pediatric Trauma Objectives Review ATLS from the pediatric perspective Convince you that children aren t simply little adults (especially when it comes to trauma) Impress you with my Power Point mastery
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System EMS System Policy Change Coversheet EMS SYSTEM POLICY CHANGE COVERSHEET Policy Number and Name: 605: Prehospital Trauma Triage Date: May 27, 2014
County of Santa Clara Emergency Medical Services System EMS System Policy Change Coversheet EMS SYSTEM POLICY CHANGE COVERSHEET Policy Number and Name: 605: Prehospital Trauma Triage Date: May 27, 2014
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
CLINICAL MANUAL. Trauma System Activation Trauma Code Criteria
 CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pediatric Trauma Cases
 Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Paramedic Trauma
 Western Technical College 10531920 Paramedic Trauma Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 Total Hours 72.00 This course teaches the
Western Technical College 10531920 Paramedic Trauma Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 Total Hours 72.00 This course teaches the
They re not little adults, but they are little humans. Pearls for your next pediatric trauma patient. Children are little humans
 They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
Chapter 34. Objectives. Objectives 01/09/2013. Chest Trauma
 Chapter 34 Chest Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 34 Chest Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY
 SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY PURPOSE: To identify those patients who are at greatest risk for severe injury and determine the most appropriate facility to transport persons with different
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY PURPOSE: To identify those patients who are at greatest risk for severe injury and determine the most appropriate facility to transport persons with different
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Pediatric Patient Overview
 Emergency Medical Services Seattle/King County Public Health 401 5th Avenue, Suite 1200 Seattle, WA 98104 206.296.4863 Last Updated December 14, 2015 Pediatric Patient Overview Contents PEDIATRIC BASICS...
Emergency Medical Services Seattle/King County Public Health 401 5th Avenue, Suite 1200 Seattle, WA 98104 206.296.4863 Last Updated December 14, 2015 Pediatric Patient Overview Contents PEDIATRIC BASICS...
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Pediatric Trauma Management For EMS
 Pediatric Trauma Management For EMS Michael D. McGonigal MD Objectives Discuss important concepts in initial pediatric trauma care, including sports and head injuries Review several pediatric trauma cases
Pediatric Trauma Management For EMS Michael D. McGonigal MD Objectives Discuss important concepts in initial pediatric trauma care, including sports and head injuries Review several pediatric trauma cases
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
EMS System for Metropolitan Oklahoma City and Tulsa 2018 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Focused History and Physical Examination of the
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY
 SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
Penetrating Trauma in Pediatric Patients. Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017
 Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
History Data Panel. Case 030 Preg Trauma. Presenting Complaint Altered mental status s/p MVC. Person Giving Information EMS
 History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D.
 1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions
 83 Questions") Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Chapter 2 Triage. Introduction. The Trauma Team
 Chapter 2 Triage Chapter 2 Triage Introduction Existing trauma courses focus on a vertical or horizontal approach to the ABCDE assessment of an injured patient: A - Airway B - Breathing C - Circulation
Chapter 2 Triage Chapter 2 Triage Introduction Existing trauma courses focus on a vertical or horizontal approach to the ABCDE assessment of an injured patient: A - Airway B - Breathing C - Circulation
BODY SYSTEMS BODY CAVITIES THE RESPIRATORY SYSTEM. Movements BODY CAVITIES. Pediatric Considerations In Respiratory System
 BODY SYSTEMS A body system is a group of organs and other structures work together to carry out specific functions. The following systems work together to carry out a function needed for life: Respiratory
BODY SYSTEMS A body system is a group of organs and other structures work together to carry out specific functions. The following systems work together to carry out a function needed for life: Respiratory
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT
 The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application
 Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Yaniv Berliner EMS STABILIZATION
 Yaniv Berliner EMS STABILIZATION Scene survey EMS must first evaluate the safety of the scene. Downed power lines, fire, traffic Is there a need for specialized equipment for extrication. Is there a need
Yaniv Berliner EMS STABILIZATION Scene survey EMS must first evaluate the safety of the scene. Downed power lines, fire, traffic Is there a need for specialized equipment for extrication. Is there a need
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
Chapter 30 Putting It All Together for the Trauma Patient
 Chapter 30 Putting It All Together for the Trauma Patient Putting It All Together Balance need for prompt transport vs. treatment on scene. Select critical interventions to implement at scene of multipletrauma
Chapter 30 Putting It All Together for the Trauma Patient Putting It All Together Balance need for prompt transport vs. treatment on scene. Select critical interventions to implement at scene of multipletrauma
McCann Technical School 70 Hodges Cross Road North Adams, MA Medical Assisting Program
 MA 104 MEDICAL SOCIAL SCIENCE 4 Credits Fall Semester Part IV FIRST RESPONDER Syllabus McCann Technical School 70 Hodges Cross Road North Adams, MA 01247 Medical Assisting Program INSTRUCTORS: Laurie Tuper,
MA 104 MEDICAL SOCIAL SCIENCE 4 Credits Fall Semester Part IV FIRST RESPONDER Syllabus McCann Technical School 70 Hodges Cross Road North Adams, MA 01247 Medical Assisting Program INSTRUCTORS: Laurie Tuper,
ESCAMBIA COUNTY TRAUMA TRANSPORT
 TRAUMA ALERT CRITERIA are established state mandated criteria. ADULT TRAUMA ALERT CRITERIA (Physical and anatomical characteristics of a person 16 years of age or older) Any 1 of the following: 1. Airway:
TRAUMA ALERT CRITERIA are established state mandated criteria. ADULT TRAUMA ALERT CRITERIA (Physical and anatomical characteristics of a person 16 years of age or older) Any 1 of the following: 1. Airway:
Paediatric Resuscitation. EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009
 Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Assessment and Scoring Tools
 Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Injury caused by an object breaking the skin and entering the body. immediate intervention to repair internal
 1 Chapter 16: Trauma & Trauma Systems 2 Trauma Leading killer of persons under in US. -150,000 Deaths annually -44,000 MVC -28,000 GSW Most medical problem in terms of lost wages, initial care, rehabilitation,
1 Chapter 16: Trauma & Trauma Systems 2 Trauma Leading killer of persons under in US. -150,000 Deaths annually -44,000 MVC -28,000 GSW Most medical problem in terms of lost wages, initial care, rehabilitation,
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY
 NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
PEDIATRIC TRAUMA EMERGENCIES
 PEDIATRIC TRAUMA EMERGENCIES Last Revised: January 2015 1 PEDIATRIC COMA SCALE Indicator Eye Opening Spontaneous 4 To verbal stimuli 3 To pain only 2 No response 1 Verbal Response Oriented, appropriate
PEDIATRIC TRAUMA EMERGENCIES Last Revised: January 2015 1 PEDIATRIC COMA SCALE Indicator Eye Opening Spontaneous 4 To verbal stimuli 3 To pain only 2 No response 1 Verbal Response Oriented, appropriate
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Trauma resuscitation in the Elderlyfrom a physiological perspective
 6 November 2017 Trauma resuscitation in the Elderlyfrom a physiological perspective Joseph Mathew Consultant, Emergency/ 6 November 2017 2 http://www.who.int/ageing/publications/global_health.pdf 6 November
6 November 2017 Trauma resuscitation in the Elderlyfrom a physiological perspective Joseph Mathew Consultant, Emergency/ 6 November 2017 2 http://www.who.int/ageing/publications/global_health.pdf 6 November
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Z19.2 Cross Reference to Patient Care Maps & Clinical Care Procedures
 2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
Chapter 11 - The Primary Assessment
 Introduction to Emergency Medical Care 1 OBJECTIVES 11.1 Define key terms introduced in this chapter. Slides 11 12, 14, 19 21, 28 11.2 Explain the purpose of the primary assessment. Slides 11 13 OBJECTIVES
Introduction to Emergency Medical Care 1 OBJECTIVES 11.1 Define key terms introduced in this chapter. Slides 11 12, 14, 19 21, 28 11.2 Explain the purpose of the primary assessment. Slides 11 13 OBJECTIVES
Pediatric Trauma Practice. Guideline for Management of the Child in Shock. Background
 Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Assessment of the Trauma Patient
 CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
Summary of Pediatric Trauma Patients
 Santa Rosa Memorial Hospital Trauma Services Summary of Pediatric Trauma Patients Reporting Dates Jan 1, 2004 May 31, 2006 The mission of the Santa Rosa Memorial Hospital Trauma Services is to provide
Santa Rosa Memorial Hospital Trauma Services Summary of Pediatric Trauma Patients Reporting Dates Jan 1, 2004 May 31, 2006 The mission of the Santa Rosa Memorial Hospital Trauma Services is to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
DATA COLLECTION AND MANAGEMENT
 DATA COLLECTION AND MANAGEMENT PURPOSE To specify the components of the data collection and management processes. RELATED POLICIES Patient Care Record, # 8115; Quality Improvement and System Evaluation,
DATA COLLECTION AND MANAGEMENT PURPOSE To specify the components of the data collection and management processes. RELATED POLICIES Patient Care Record, # 8115; Quality Improvement and System Evaluation,
Selective Spine Assessment & Spinal Motion Restriction
 Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
Pediatric Trauma. Andrea L. Williams, PhD, RN
 Pediatric Trauma Andrea L. Williams, PhD, RN Clinical Associate Professor UW School of Nursing Emergency Education Specialist UW Emergency Education Center Why Are Traumatic Injuries Different in Children
Pediatric Trauma Andrea L. Williams, PhD, RN Clinical Associate Professor UW School of Nursing Emergency Education Specialist UW Emergency Education Center Why Are Traumatic Injuries Different in Children
Polytrauma. Same stuff-different day! 9/14/2012. Managing the difficult airway in Multi-Systems Trauma. Jerry J Ryman CRT
 Managing the difficult airway in Multi-Systems Trauma Jerry J Ryman CRT Polytrauma More than 1 organ system involved Pulmonary Circulatory Neurological Integumentary Musculo-skeletal Genito-urinary Endocrine
Managing the difficult airway in Multi-Systems Trauma Jerry J Ryman CRT Polytrauma More than 1 organ system involved Pulmonary Circulatory Neurological Integumentary Musculo-skeletal Genito-urinary Endocrine
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions