E.N.T. HEAD AND NECK DEPT UBTH DR. OSEGHALE -DR. BLACKIE -DR. AKPALABA
|
|
|
- Marion Allison
- 5 years ago
- Views:
Transcription

1 E.N.T. HEAD AND NECK DEPT UBTH DR. OSEGHALE -DR. BLACKIE -DR. AKPALABA
2 OUTLINE INTRODUCTION CASE PRESENTATIONS RELEVANT ANATOMY EPIDEMIOLOGY AETIOLOGY PATHOGENESIS MANAGEMENT-HX -EXAMINATION -INVESTIGATIONS -DIFFERENTIAL DIAGNOSIS -RX /COMPLICATIONS -PREVENTION -RECENT ADVANCES -LOCAL EXPERIENCE CONCLUSION
3 INTRODUCTION It is abnormal narrowing of the central air passages of the larynx and trachea. It may be in a single location or at multiple locations along the laryngotracheal airway. The causes are varied and it could be life threatening prompt diagnosis and treatment is necessary.
4 CASE 1 A.M 29YRS Female Esan Christian Teacher Textile mill rd
5 Presented 4 years ago Via referral from O and G team. C/O--difficulty in breathing X 4/52 Was on mechanical ventilation via endotracheal intubation x 6weeks in ICU here in UBTH for intrapartum eclampsia. Nil other throat complains Nil history of previous head or neck trauma or surgery
6 ENT examination then revealed RR- 48CPM ICR,SCR biphasic stridor, tracheal tugging. BS- decreased with rhonchi in both lung fields.
7 X ray soft tissue neck revealed narrowing of the air way at the level of c5-c6. A diagnosis of subglottic stenosis secondary to prolonged intubation was made.
8 Tracheostomy and D/L was done. D/L done revealed subglottic stenosis with a little opening. She further had dilatation and laryngotracheal stenting She was subsequently decannulated,observed and discharged home.
9 She however represented 2weeks later in airway obstruction. She had repeat tracheostomy and direct laryngoscopy Findings Posterior Laryngeal Web was billed for micro laryngoscopy and clearance She however became pregnant and this delayed treatment. She represented 8 weeks ago, 6months after delivery for clearance. Finding at op were web in the posterior aspect of the laryngeal inlet with resultant reduced laryngeal inlet.
10 Web was cleared. Observed for 48 hrs Decannulated, thereafter, discharged She represented 24hrs later in airway obstruction. Had reinsertion of t.tube and flexible laryngoscopy FBL revealed freely mobile VC and subglottic stenosis. She was adequately counselled is being worked up for laryngofissure and stenting.
11 CASE 2 A.E 24YRS Male Isoko Christian Wood worker Ugbogui village
12 C/O- Difficulty in breathing x 24hrs Progressively worsening assoc with noisy breathing. Positive history of aphasia Nil other throat symptoms Nil nose and ear symptoms
13 He was previously managed by the neurosurgeons for head injury. Sustained via an industrial accident
14 He was unconscious and was intubated for 17days. Intubation was in A/E and he had several extubations one on account of a blocked tube, once he extubated himself.
15 O/E by the ENTTOC in A/E He was acutely ill looking afebrile not pale anicteric with oral endotracheal tube insitu. CVS ; PR-112BPM BP -120/70MMHG HS S1 S2
16 Chest RR- 28CPM BS-vesicular with wide spread transmitted sounds. CNS- GCS-9/15 Left facial nerve palsy
17 Eyes; bilateral periorbital ecchymosis. bilateral chemosis worse on left good RE opening with right pupil reactive to light inability to open left eye spontaneously left pupil dilated and unresponsive to light
18 Ears nil abnormalities Nose nil abnormalities Oral cavity/oropharynx- nil abnormalities
19 Fiberoptic laryngoscopy freely mobile vocal cords good glottic opening with a subglottic web posteriorly located. X-ray soft tissue neck revealed a soft tissue shadow at the level of the subglottis.
20 A diagnosis of subglottic stenosis secondary to prolonged intubation was made. He had tracheostomy done and was admitted into the ward.
21 However while in the wards worsening left eye chemosis was noticed and ophthalmology team reviewed. A diagnosis of carotico carvenous fistula was made he was placed on topical antibiotics and left eye padding.
22 He has being discharged and is being worked up for a microlaryngoscopy and stenting.
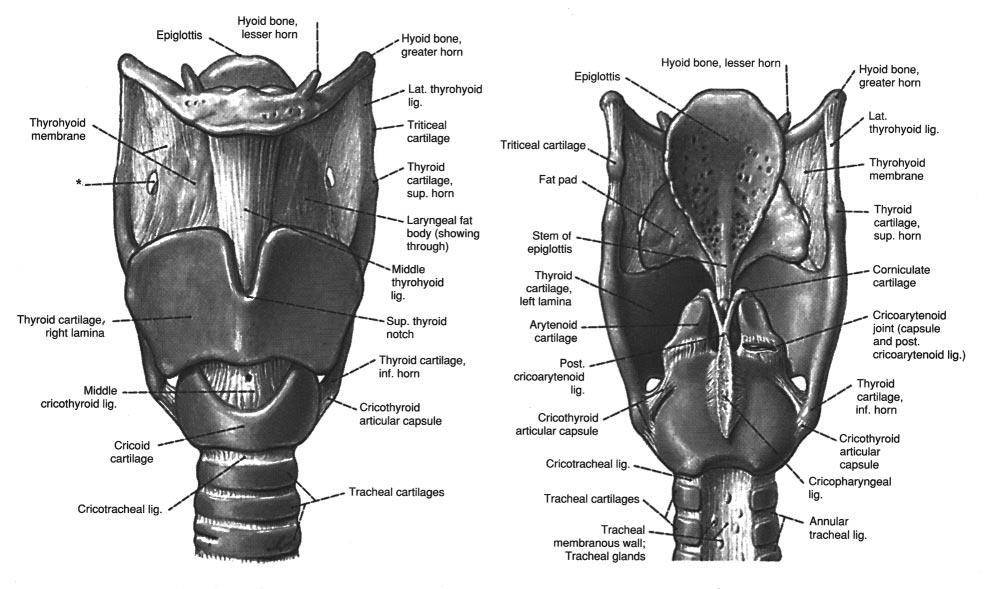
23 RELEVANT ANATOMY The larynx is the upper end of the lower respiratory tract. It is averagely 44mm long and 36mm wide and in the midline opposite c3-c6 vertebrae. It is made up of cartilages connected by ligaments and membranes lined by mucus membranes and moved by muscles.
24
 - Cuneiform (Wrisberg) Unpaired - Epiglottis -")
25 Laryngeal cartilages Paired - Arytenoid - Corniculate (Santorini) - Cuneiform (Wrisberg) Unpaired - Epiglottis - Thyroid - Cricoid

26 Joints of larynx Cricothyroid joint Crico-arytenoid joint Rotation and gliding
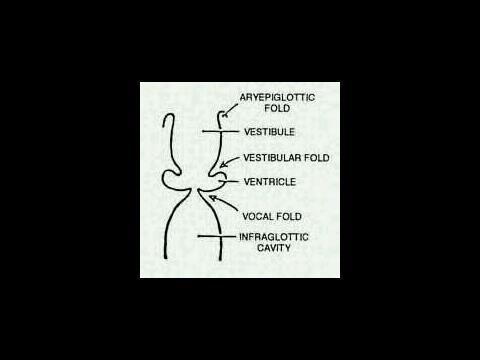
27 CAVITY OF THE LARYNX Starts at the laryngeal inlet where it communicates with the pharynx. And ends at the lower border of the cricoid cartilage where it is continues with the lumen of the trachea.
28 CAVITY OF THE LARYNX 2 pairs of folds vestibular and vocal divide the cavity into 3 parts. which are the vestibule, ventricle and subglottic space.
29
30 Laryngeal cavity Supraglottic - Vestibule - Ventricule Glottic - 2.5cm male - 1.6cm female Infraglottic /subglottic
31 Functions of the larynx Biological Respiration Protection of the lower airway Fixation of the chest Non biological Phonation.
32

33
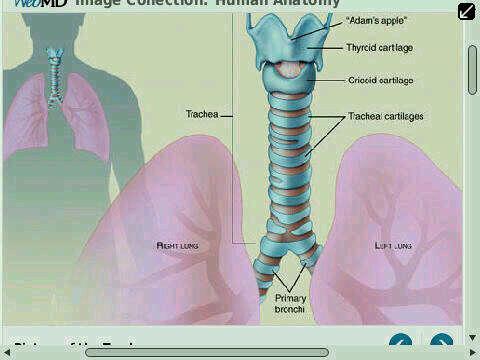
34 It continues with the trachea. the trachea is 11.5 cm in length and 2.5cm wide. Terminates at t4/t5 by bifurcating. held patent by C-shaped cartilages deficient posteriorly and completed by fibrous tissue and trachealis muscle.
35
36 Functions of the trachea Connects the central air passage of the larynx to the lungs. It is lined with cells that produce mucus which traps particles to clean before it reaches the lungs. It is the pathway of air pressure from the lungs to the larynx for phonation. Its flexible and collapses slightly to allow food bolus go down oesophagus.
37 EPIDEMIOLOGY Children Adult -- Laryngeal trauma M>F 3:1
38 AETIOLOGY Acquired and congenital External laryngotracheal trauma:- - Penetrating tissue injury - Blunt force neck trauma; high or low velocity impact Internal laryngotracheal trauma:- - Endotracheal intubation - Post tracheostomy
39 cont d - Post microlaryngoscopy and resection - Post radiotherapy - Endotracheal burns:chemical, thermal Infection:- - Tuberculosis - Scleroma - Fungal histoplasmosis Chronic inflammatory disease: - sarcoidosis
40 Cont d Collagen vascular disease:- - Wegner s granulomatosis - Relapsing polychondritis Prematurity (Birth weight less than 1500g) GERD
41 PATHOGENESIS INTUBATION:- Mechanical trauma of placement or its contact pressure. Mucosal edema and hyperaemia- mucosal necrosis perichondrium exposure infection of perichondrium subglottic scar. SOFT TISSUE DAMAGE:- Mucosal loss, formation of adhesion and the organisation of haematoma within the paraglottic,
42 Cont d Pre-epiglottic and interarytenoid space Arthrodesis of arytenoids into an unsatisfactory position web formation Disruption of the cartilage framework will heal by fibrous tissue Removal of a piece of tracheal cartilage during tracheostomy
43 CLASSIFICATION Supraglottic:- occurs at the laryngeal inlet, caused by trauma. Subglottic region:- narrowest, commonest. Glottic:- - Anterior glottic web from thyroid cartilage fracture, intubation, iatrogenic mm extension of a web can cause dyspnea
44 Cont d Posterior glottic stenosis:- Intubation -scar tissue between the arytenoids,with fixation of one or both of them Subglottic region:- narrowest, commonest. Bogdasarian and Oslon :- Four types Type I- vocal cord process adhesion Type II- post. Commissure stenosis,with scaring in the interarytenoid plane
45 Cont d Type III :- posterior commissure stenosis + unilateral cricoarytenoid joint ankylosis Type IV :- posterior commissure stenosis + bilateral cricoarytenoid joint ankylosis
46 cont d Subglottic stenosis By Cotton Myers: - -Grade I -Grade II -Grade III -Grade IV
47 COTTON MYERS GRADING
48 Cont d Tracheal stenosis :- 3 types Cicatricia (connective tissue scar) Anterior wall collapse(post tracheostomy) Complete stenosis
49

50 -MANAGEMENT
51 HISTORY Congenital LTS At birth (moderate or severe) Acquired LTS 2-4 weeks Post trauma/insult *mild form (asymptomatic, Subsequent airway insult)
52 HISTORY Hoarse/husky voice / muffle /aphonic, Difficulty in breathing Barking cough Poor cry
53 HISTORY Birth history (Prematurity) Feeding / Voice / Breathing difficulties? Reflux? Intubation Tracheostomy laryngeal Surgery / Interventional therapy RTA
54 HISTORY cont d Burns Foreign body inhalation/ Aspiration Rheumatoid arthritis Infection (Diphtheria, Epiglottitis, TB) Respiratory Papillomatosis Tumour Idiopathic
55 PHYSICAL EXAMINATION Dyspnoeic,tachypnoiec Stridulous Cyanosed Febrile
56 INVESTIGATIONS
57 FLEXIBLE LARYNGOSCOPY Supraglottis Structure abnormalities Glottis VC mobility Clefts/webs/masses Subglottis - stenosis
58 RIGID ENDOSCOPY Is the gold standard Largest ETT Sites Length Other airway anomalies (clefts, webs, cricoarytenoid joint fixation neoplasms) Reflux changes.

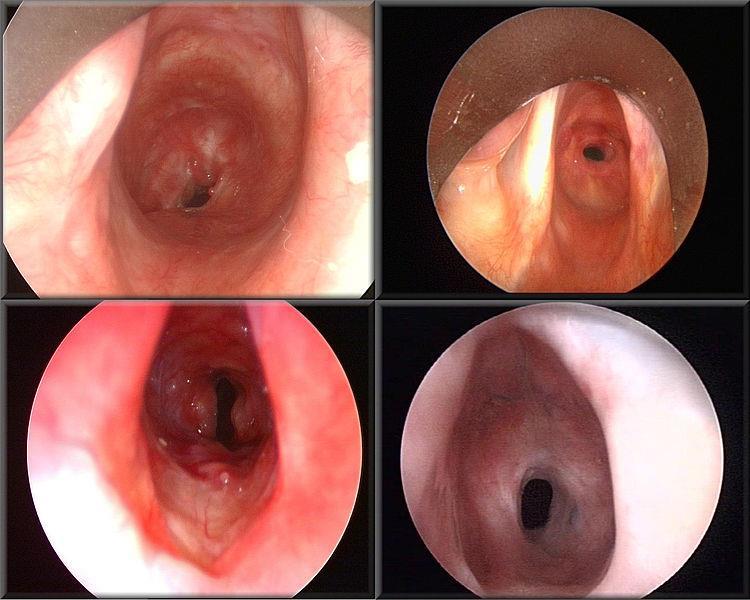
59 LARYNGEAL INLET STENOSIS

60 CONGENITAL GLOTTIC STENOSIS

61 POSTERIOR GLOTTIC BAND

62 SUBGLOTTIC STENOSIS SUBGLOTTIC STENOSIS
63 RADIOLOGIC EVALUATION Plain film Quick cost effective CT Scan Neck Site Length MRI Ancilliary tests surgical planning
")
64 Soft Tissue Film (xeroradiograph)

65
66 Cotton-Myer Grading
67 McCaffrey (1992) subsites (trachea, subglottis, glottis) length of stenosis not lumen diameter Grade I: subglottis or trachea <1cm long Grade II: subglottis >1cm long Grade III: Subglottic and tracheal Grade IV: Glottic involvement
68 DIFFERENTIAL DIAGNOSIS Laryngomalacia Tracheomalacia Vocal cord paralysis Laryngeal cleft Congenital cysts Viral laryngotracheobron chitis (croup) GERD Recurrent respiratory papillomatosis Mass Hemangioma Foreign body
69 TREATMENT
70 GOAL To produce: 1. Adequate airway 2. Competent Larynx 3. Acceptable voice *Ultimately the goal is to treat the stenotic segment while preserving native normal segments
71 TREATMENT -OPTIONS Tracheostomy Endoscopic -Dilation -Laser excision Open procedure: -Expansion procedure (one-stage, with stent) -Segmental resection (cricotracheal resection - CTR )


72 TRACHEOSTOMY

73
74 TRACHEOSTOMY Adequate airway Smallest tube Allows air leakage (pressure injury, phonation). Temporary *(suprastomal granulation tissue --> failed decannulation) *accidental decannulation
75 ENDOSCOPIC REPAIR Dilation Early disease Scar excision with laser Minimal damage Avoids bleeding, edema, Grade I or II stenosis Requires multiple procedures

76 TRACHEAL DILATATION RIGID BRONCHOSCOPE

77 CO 2 LASER
78 Open procedure --LTR -Expansion procedure (one-stage, with stent) * Anterior cricoid split +/_cartilage graft* * Posterior cricoid split +/_cartilage graft* *Anterior and posterior cricoid split with cartilage graft -Segmental resection (cricotracheal resection - CTR) * Primary CTR *Salvage CTR *Extended CTR CTR +/_expansion
79

80 OPEN REPAIRS LARYNGOFISSURE
81 External Expansion Surgery Grade III and IV stenosis, Refractory grade II Cricoid split + cartilage grafts + stenting Repair at youngest age possible: Improved speech and language development Decreased tracheostomy mobidity/mortality
82 ANTERIOR CRICOID SPLIT 1980 Cotton Alternative (Tracheostomy) Splits cricoid and first 2 tracheal rings ET tube in place (stent ). ICU -Intubated, sedated, paralyzed 7-14 days Mild anterior narrowing

83 ANTERIOR CRICOID SPLIT
84 Anterior Grafts: Modified boat shape
85 Placement of anterior graft
86 Costal Cartilage Grafts Abundant Can obtain any size necessary Generally use the 5 th rib Stenting (several days)
87 Approach to obtaining graft
88 Other grafts Auricular cartilage Thyroid alar cartilage Hyoid bone
89 Anterior laryngofissure with graft Good for: Anterior stenosis Anterior wall collapse Perichondrium of the anterior graft is placed on the lumen side Re-epithelialization Barrier to infection Large external flange (prolapse)
90 Laryngofissure with posterior cricoid division +/- grafting Indications: Posterior subglottic or glottic stenosis Circumferential stenosis Cricoid deformity Key points / complications Avoid complete laryngofissure to avoid damage to anterior commissure Knots buried to keep them extraluminal Patients often receive stenting 3-6 months

91 Posterior Grafts: boat shape
92 Single-staged Laryngotracheal Reconstruction (SS-LTR) Allows for shorter stenting period Anterior graft, posterior graft, or both ET tube initially to support the graft 2-4 days if Anterior graft only 7 days if Posterior graft is used as well Best results if patient >4Kg and >30wks
93 Two-Staged LTR The main difference is that a more permanent stent is used to maintain the airway while the graft heals Montgomery T-tubes (silastic) Aboulker Stents (teflon) Stents can be left for months *Considered to be inert and prevent tissue injury
94 STENTS Counteract scar contractures Scaffold for the airway. Hold grafts in place Types -Endotracheal tubes, -Silastic sheet rolls, -Montgomery T-tubes, -Laryngeal stents : *Teflon stents [Aboulker stent, *Silastic stents (Montgomery stents:
95 Montgomery T-tube Stent

96

97 Aboulker Stent
98 Aboulker Stent: wired-in tracheostomy tube

99
100 Stent complication Granulation tissue formation S. aureus and P.aeruginosa Antibiotics.

101 TRACHEAL RECONSTRUCTION composite nasal septal cartilage graft

102 TRACHEAL RECONSTRUCTION Cryo-preserved aortic allograft.
103 Cricotracheal Resection (CTR)


104 Tracheal Resection and Anastomosis

105 Tracheal Resection and Anastomosis
106 CTR Complications Anastomotic webbing asymptomatic Arytenoid prolapse (45%) Asymptomatic partial laser arytenoidectomy Restenosis Tracheostomy dependent Postoperative infection Recurrent laryngeal nerve palsy Anastomotic dehiscence
107 POST OP CARE ICU Nasotracheal Intubation 7-14 days Sedation and paralysis Steroids 12 hours preop 5 days after decannulation Leak test prior to extubation Precedex during tracheal extubation Antibiotics 2 weeks MonthsAnti-reflux medications Chest physiotherapy
108 PREVENTION Awareness & Education Good ANC Duration (Tracheostomy) Technique (Traumatic intubation) Size / type Movement Number of re-intubations, Infection while intubated High tracheostomy
109 RECENT ADVANCES Transplanted trachea + stem cells ( Ciaran's stem cells)
110 LOCAL EXPERIENCE 4 confirmed cases 3 (F) 1 (M) 4 undocumented
111 CONCLUSION Laryngotracheal stenosis Rare condition Prolonged intubation Management very challenging

112 THANK YOU
113 References 1. Cummings: Otolaryngology: Head & Neck Surgery, 4th ed. 2. Muller CD and Pou AM. Subglottic Stenosis. Quinn s Online Textbook of Otolaryngology. November 13, Whited RE: A study of endotracheal tube injury to the subglottis. Laryngoscope. 95: , Carretta A, Melloni G, Ciriaco P, et al: Preoperative assessment in patients with postintubation tracheal stenosis. Rigid and flexible bronchoscopy versus CT scan with multiplanar reconstruction. Surg Endosc 20: , Koufman JA. The otolarngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour ph monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope 1991; 101(suppl 53): Walner DL et al. Gastroesophageal reflux in patients with subglottic stenosis. Arch Otolaryngol Head Neck Surg 1998; 124(5): Burton DM. Gastroesophageal reflux. In: Holinger LD, Lusk RP, Green CG, eds. Pediatric Laryngology and Bronchoesophagology. Philadelphia, Pa: JB Lippincott Raven; 1997: Lano, CF et. al. Laryngotracheal reconstruction in the adult: a ten year experience. Ann Otlo Rhinol Laryngol 1998; 107: McCaffrey TV. Classification of laryngotracheal stenosis. Laryngoscope 1992:102: Prescott CA. Protocol for management of the interposition cartilage graft laryngotracheoplasty. Ann Otol Rhinol Laryngol. 1988;97(3, pt 1): Herrington, H. C., Webber, S. M., Anderson, P. E. (2006). Modern management of laryngotracheal stenosis. Laryngoscope. 116(9): Cotton RT, Seid AB: Management of the extubation problem in the premature child: Anterior cricoid split as an alternative to tracheotomy. Ann Otolo Rhinol Laryngol 1980; 89: Saunders MW, Thirlwall A, Jacob A, Albert DM. Single- or two-stage laryngotracheal reconstruction: comparison of outcomes. Int J Pediatr Otorhinolaryngol.1999;50(1): Smith LP, Zur KB, Jacobs IN. Single- vs Double-Stage Laryngotracheal Reconstruction. Arch Otolaryngol Head Neck Surg 2010,136: Younis RT, Lazar RH, Bustillo A. Revision single-stage laryngotracheal reconstruction in children. Ann Otol Rhinol Laryngol May;113(5): Koltai PJ, Ellis B, Chan J, Calabro A. Anterior and posterior cartilage graft dimensions in successful laryngotracheal reconstruction. Arch Otolaryngol Head Neck Surg 2006;132: Nouraei SA, Petrou MA, Randhawa PS, Singh A, Howard DJ, Sandhu GS: Bacterial colonization of airway stents: a promoter of granulation tissue formation following laryngotracheal reconstruction. Arch Otolaryngol Head Neck Surg 2006,132: White DR, Cotton RT, Bean JA, Rutter MJ. Pediatric cricotracheal resection: surgical outcomes and risk factor analysis. Arch Otolaryngol Head Neck Surg. 2005;131(10): Rutter MJ, Hartley BE, Cotton RT. Cricotracheal resection in children. Arch Otolaryngol Head Neck Surg. 2001;127(3): Jaquet Y, Lang F, Pilloud R, Savary M, Monnier P. Partial cricotracheal resection for pediatric subglottic stenosis: long-term outcome in 57 patients. J Thorac Cardiovasc Surg. 2005;130(3): Idonomidis C, George M, Jaquet Y, Monnier P. Partial cricotracheal resection in children weighing less than 10 kilograms. Otolaryngology - Head and Neck Surgery 2010; 142(1): Gupta P, Tobias J, Goyal S et al. Perioperative care following complex laryngotracheal reconstruction in infant and children. Saudi Journal Anaesthesia 2010; 4(3):
114 References 1. Saunders MW, Thirlwall A, Jacob A, Albert DM. Single- or two-stage laryngotracheal reconstruction: comparison of outcomes. Int J Pediatr Otorhinolaryngol.1999;50(1): Smith LP, Zur KB, Jacobs IN. Single- vs Double-Stage Laryngotracheal Reconstruction. Arch Otolaryngol Head Neck Surg 2010,136: Younis RT, Lazar RH, Bustillo A. Revision single-stage laryngotracheal reconstruction in children. Ann Otol Rhinol Laryngol May;113(5): Koltai PJ, Ellis B, Chan J, Calabro A. Anterior and posterior cartilage graft dimensions in successful laryngotracheal reconstruction. Arch Otolaryngol Head Neck Surg 2006;132: Nouraei SA, Petrou MA, Randhawa PS, Singh A, Howard DJ, Sandhu GS: Bacterial colonization of airway stents: a promoter of granulation tissue formation following laryngotracheal reconstruction. Arch Otolaryngol Head Neck Surg 2006,132: White DR, Cotton RT, Bean JA, Rutter MJ. Pediatric cricotracheal resection: surgical outcomes and risk factor analysis. Arch Otolaryngol Head Neck Surg. 2005;131(10): Rutter MJ, Hartley BE, Cotton RT. Cricotracheal resection in children. Arch Otolaryngol Head Neck Surg. 2001;127(3): Jaquet Y, Lang F, Pilloud R, Savary M, Monnier P. Partial cricotracheal resection for pediatric subglottic stenosis: long-term outcome in 57 patients. J Thorac Cardiovasc Surg. 2005;130(3): Idonomidis C, George M, Jaquet Y, Monnier P. Partial cricotracheal resection in children weighing less than 10 kilograms. Otolaryngology - Head and Neck Surgery 2010; 142(1): Gupta P, Tobias J, Goyal S et al. Perioperative care following complex laryngotracheal reconstruction in infant and children. Saudi Journal Anaesthesia 2010; 4(3):
Surgical Management of Advanced and Recurrent Subglottic Stenosis October 2011
 TITLE: Surgical Management of Advanced and Recurrent Subglottic Stenosis SOURCE: Grand Rounds Presentation, University of Texas Medical Branch (UTMB Health), Department of Otolaryngology DATE: October
TITLE: Surgical Management of Advanced and Recurrent Subglottic Stenosis SOURCE: Grand Rounds Presentation, University of Texas Medical Branch (UTMB Health), Department of Otolaryngology DATE: October
Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis
 Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
Complex Airway problems - Paediatric Perspective
 Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Aetiology. Poor tube management. Small cricoid (acquired on congenital) Reflux Poor general status. Size of tube (leak) Duration of intubation
 Reflux Poor general status. Size of tube (leak) Duration of intubation") Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Basic Science Review Wound Healing
 Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
The surgical management of subglottic stenosis (SGS)
") Original Research Pediatric Otolaryngology Short- versus Long-term Stenting in Children with Subglottic Stenosis Undergoing Laryngotracheal Reconstruction Otolaryngology Head and Neck Surgery 2018, Vol.
Original Research Pediatric Otolaryngology Short- versus Long-term Stenting in Children with Subglottic Stenosis Undergoing Laryngotracheal Reconstruction Otolaryngology Head and Neck Surgery 2018, Vol.
Unilateral Supraglottoplasty for Severe Laryngomalacia in Children. Nasser A Fageeh, MD, FRCSC, FACS*
 Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
SURGERY FOR PEDIATRIC SUBGLOTTIC STENOSIS: DISEASE-SPECIFIC OUTCOMES
 Ann Otol Rhinol Laryngol 110:2001 Ann Otol Rhinol Laryngol 110:2001 REPRINTED FROM ANNALS OF OTOLOGY, RHINOLOGY & LARYNGOLOGY December 2001 Volume 110 Number 12 COPYRIGHT 2001, ANNALS PUBLISHING COMPANY
Ann Otol Rhinol Laryngol 110:2001 Ann Otol Rhinol Laryngol 110:2001 REPRINTED FROM ANNALS OF OTOLOGY, RHINOLOGY & LARYNGOLOGY December 2001 Volume 110 Number 12 COPYRIGHT 2001, ANNALS PUBLISHING COMPANY
Slide thyrocricotracheoplasty for the treatment of high-grade subglottic stenosis in children
 Journal of Pediatric Surgery (2010) 45, 2317 2321 www.elsevier.com/locate/jpedsurg Slide thyrocricotracheoplasty for the treatment of high-grade subglottic stenosis in children Seong Min Kim a, Jae Ho
Journal of Pediatric Surgery (2010) 45, 2317 2321 www.elsevier.com/locate/jpedsurg Slide thyrocricotracheoplasty for the treatment of high-grade subglottic stenosis in children Seong Min Kim a, Jae Ho
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant. Tara Brennan, MD 2,3
 Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other
 Internal trauma (Endotracheal intubation, tracheostomy) Other") Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Contents. Part A Clinical Evaluation of Laryngeal Disorders. 3 Videostroboscopy and Dynamic Voice Evaluation with Flexible Laryngoscopy...
 Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Subglottic stenosis in infants and children
 Original Article Singapore Med J 010; 51(1 1) : 88 Subglottic stenosis in infants and children Choo K K M, Tan H K K, Balakrishnan A Yong Loo Lin School of Medicine, National University of Singapore, 10
Original Article Singapore Med J 010; 51(1 1) : 88 Subglottic stenosis in infants and children Choo K K M, Tan H K K, Balakrishnan A Yong Loo Lin School of Medicine, National University of Singapore, 10
Laryngotracheal stenosis in children
 Eur Arch Otorhinolaryngol (1998) 255 : 12 17 Springer-Verlag 1998 LARYNGOLOGY M. M. Lesperance G. H. Zalzal Laryngotracheal stenosis in children Received: 8 March 1977 / Accepted: 31 July 1997 Abstract
Eur Arch Otorhinolaryngol (1998) 255 : 12 17 Springer-Verlag 1998 LARYNGOLOGY M. M. Lesperance G. H. Zalzal Laryngotracheal stenosis in children Received: 8 March 1977 / Accepted: 31 July 1997 Abstract
Pediatric Endoscopic Airway Management With Posterior Cricoid Rib Grafting
 The Laryngoscope VC 2011 The American Laryngological, Rhinological and Otological Society, Inc. Pediatric Endoscopic Airway Management With Posterior Cricoid Rib Grafting Matthew J. Provenzano, MD; Stephanie
The Laryngoscope VC 2011 The American Laryngological, Rhinological and Otological Society, Inc. Pediatric Endoscopic Airway Management With Posterior Cricoid Rib Grafting Matthew J. Provenzano, MD; Stephanie
Subglottic Stenosis November 2002
 TITLE: Subglottic Stenosis SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 13, 2002 RESIDENT PHYSICIAN: Christopher D. Muller, M.D. FACULTY PHYSICIAN: Anna M. Pou, M.D.
TITLE: Subglottic Stenosis SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 13, 2002 RESIDENT PHYSICIAN: Christopher D. Muller, M.D. FACULTY PHYSICIAN: Anna M. Pou, M.D.
Partial cricotracheal resection for pediatric subglottic stenosis: Long-term outcome in 57 patients
 General Thoracic Surgery Partial cricotracheal resection for pediatric subglottic stenosis: Long-term outcome in 57 patients Yves Jaquet, MD, Florian Lang, MD, Raphaelle Pilloud, MD, Marcel Savary, MD,
General Thoracic Surgery Partial cricotracheal resection for pediatric subglottic stenosis: Long-term outcome in 57 patients Yves Jaquet, MD, Florian Lang, MD, Raphaelle Pilloud, MD, Marcel Savary, MD,
Evaluation and Management of Pediatric Stridor
 Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
I enjoy open airway surgery In 2010: LTRs 28 CTRs 6 Clefts 4 Slides 20
 Michael J. Rutter, FRACS Department of Pediatric Otolaryngology- Head & Neck Surgery Aerodigestive and Esophageal Center Cincinnati Children s Hospital Medical Center Cincinnati, Ohio IPSA Denver, CO June
Michael J. Rutter, FRACS Department of Pediatric Otolaryngology- Head & Neck Surgery Aerodigestive and Esophageal Center Cincinnati Children s Hospital Medical Center Cincinnati, Ohio IPSA Denver, CO June
Management Of Acquired Laryngotracheal Stenosis Our Experience.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 2 Ver. XII (Feb. 2016), PP 32-36 www.iosrjournals.org Management Of Acquired Laryngotracheal
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 2 Ver. XII (Feb. 2016), PP 32-36 www.iosrjournals.org Management Of Acquired Laryngotracheal
Chapter 34: Stenosis of the larynx. J. N. G. Evans
 Chapter 34: Stenosis of the larynx J. N. G. Evans Stenosis of the larynx is more frequent than tracheal stenosis; in a review of 752 cases of stridor seen at The Hospital for Sick Children, Great Ormond
Chapter 34: Stenosis of the larynx J. N. G. Evans Stenosis of the larynx is more frequent than tracheal stenosis; in a review of 752 cases of stridor seen at The Hospital for Sick Children, Great Ormond
Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience
 1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
Organ preservation in laryngeal cancer
 Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children
 Case Reports in Otolaryngology, Article ID 304593, 4 pages http://dx.doi.org/10.1155/2014/304593 Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children Aliye Filiz
Case Reports in Otolaryngology, Article ID 304593, 4 pages http://dx.doi.org/10.1155/2014/304593 Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children Aliye Filiz
OTOLARYNGOLOGIC CLINICS ISSUE: PAEDIATRIC LARYNGOTRACHEAL RECONSTRUCTION. Edited by Dr Peter Koltai
 OTOLARYNGOLOGIC CLINICS ISSUE: PAEDIATRIC LARYNGOTRACHEAL RECONSTRUCTION Edited by Dr Peter Koltai Single and Multi Stage Pediatric Laryngotracheal Reconstruction Simone J Boardman, David M Albert Great
OTOLARYNGOLOGIC CLINICS ISSUE: PAEDIATRIC LARYNGOTRACHEAL RECONSTRUCTION Edited by Dr Peter Koltai Single and Multi Stage Pediatric Laryngotracheal Reconstruction Simone J Boardman, David M Albert Great
Subglottic stenosis in paediatric patients
 Pediatr Pol 2018; 93 (1): 80 85 DOI: https://doi.org/10.5114/polp.2018.74772 Submitted: 4.10.2017, Accepted: 15.11.2017, Published: 28.02.2018 PEDIATRIA Polska PISMO POLSKIEGO TOWARZYSTWA PEDIATRYCZNEGO
Pediatr Pol 2018; 93 (1): 80 85 DOI: https://doi.org/10.5114/polp.2018.74772 Submitted: 4.10.2017, Accepted: 15.11.2017, Published: 28.02.2018 PEDIATRIA Polska PISMO POLSKIEGO TOWARZYSTWA PEDIATRYCZNEGO
Laryngeal split and rib cartilage interpositional grafting: Treatment option for glottic/subglottic stenosis in adults
 General Thoracic Surgery Terra et al Laryngeal split and rib cartilage interpositional grafting: Treatment option for glottic/subglottic stenosis in adults Ricardo Mingarini Terra, MD, Hélio Minamoto,
General Thoracic Surgery Terra et al Laryngeal split and rib cartilage interpositional grafting: Treatment option for glottic/subglottic stenosis in adults Ricardo Mingarini Terra, MD, Hélio Minamoto,
Laryngo-tracheal stenosis is a congenital or. A Multi-Modality Surgical Management in Laryngeal Stenosis. Case Series
 Case Series A Multi-Modality Surgical Management in Laryngeal Stenosis Ashfaque Ansari, 1 Annju Thomas 1 ABSTRACT Introduction Postintubation laryngo-tracheal stenosis requires a precise diagnosis and
Case Series A Multi-Modality Surgical Management in Laryngeal Stenosis Ashfaque Ansari, 1 Annju Thomas 1 ABSTRACT Introduction Postintubation laryngo-tracheal stenosis requires a precise diagnosis and
Early management of laryngeal injuries'
 656 Journal of the Royal Society of Medicine Volume 74 September 1981 Early management of laryngeal injuries' A G D Maran MD FRCS Department of Otolaryngology, P M Stell chm FRCS Department of Otolaryngology,
656 Journal of the Royal Society of Medicine Volume 74 September 1981 Early management of laryngeal injuries' A G D Maran MD FRCS Department of Otolaryngology, P M Stell chm FRCS Department of Otolaryngology,
Subject Index. Bacterial infection, see Suppurative lung disease, Tuberculosis
 Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation
 Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Congenital Laryngeal Anomalies November 2002
 TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 20, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, M.D. FACULTY ADVISOR: Ronald W. Deskin,
TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 20, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, M.D. FACULTY ADVISOR: Ronald W. Deskin,
ORIGINAL ARTICLE. Factors Associated With Staged Reconstruction and Successful Stoma Closure in Tracheal Resection and End-to-End Anastomosis
 ORIGINAL ARTICLE Factors Associated With Staged Reconstruction and Successful Stoma Closure in Tracheal Resection and End-to-End Anastomosis Soon-Hyun Ahn, MD; Myung-Whun Sung, MD; Kwang Hyun Kim, MD Background:
ORIGINAL ARTICLE Factors Associated With Staged Reconstruction and Successful Stoma Closure in Tracheal Resection and End-to-End Anastomosis Soon-Hyun Ahn, MD; Myung-Whun Sung, MD; Kwang Hyun Kim, MD Background:
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September ISSN
 International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
ORIGINAL ARTICLE. Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty
 ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
Surgical Treatment of Benign Subglottic Stenosis. JLKasperbauer MD Mayo Clinic Rochester, MN USA
 Surgical Treatment of Benign Subglottic Stenosis JLKasperbauer MD Mayo Clinic Rochester, MN USA Goals Review Subglottic Stenosis Anatomy, Airway Dynamics, Etiology Idiopathic Subglottic Stenosis Definition,
Surgical Treatment of Benign Subglottic Stenosis JLKasperbauer MD Mayo Clinic Rochester, MN USA Goals Review Subglottic Stenosis Anatomy, Airway Dynamics, Etiology Idiopathic Subglottic Stenosis Definition,
A Randomized Study of Suprastomal Stents in Laryngotracheoplasty Surgery for Grade III Subglottic Stenosis in Children
 The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. TRIOLOGICAL SOCIETY CANDIDATE THESIS A Randomized Study of Suprastomal Stents in Laryngotracheoplasty Surgery
The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. TRIOLOGICAL SOCIETY CANDIDATE THESIS A Randomized Study of Suprastomal Stents in Laryngotracheoplasty Surgery
Surgical treatment for patients with tracheal and subgllotic stenosis
 Original Research Medical Journal of the Islamic Republic of Iran.Vol. 23, No. 3, November, 2009. pp. 132-138 Surgical treatment for patients with tracheal and subgllotic stenosis Mohammad Naeimi, MD.
Original Research Medical Journal of the Islamic Republic of Iran.Vol. 23, No. 3, November, 2009. pp. 132-138 Surgical treatment for patients with tracheal and subgllotic stenosis Mohammad Naeimi, MD.
ORIGINAL ARTICLE. Open Excision of Subglottic Hemangiomas to Avoid Tracheostomy
 ORIGINAL ARTICLE Open Excision of Subglottic Hemangiomas to Avoid Tracheostomy Shyan Vijayasekaran, FRACS; David R. White, MD; Benjamin E. J. Hartley, FRCS(ORL); Michael J. Rutter, FRACS; Ravindhra G.
ORIGINAL ARTICLE Open Excision of Subglottic Hemangiomas to Avoid Tracheostomy Shyan Vijayasekaran, FRACS; David R. White, MD; Benjamin E. J. Hartley, FRCS(ORL); Michael J. Rutter, FRACS; Ravindhra G.
Subglottic stenosis, with involvement of the lower larynx
 Laryngotracheal Resection and Reconstruction John D. Mitchell, MD n, Subglottic stenosis is being recognized with increasing frequency in adults, and may be the most frequent indication for airway intervention
Laryngotracheal Resection and Reconstruction John D. Mitchell, MD n, Subglottic stenosis is being recognized with increasing frequency in adults, and may be the most frequent indication for airway intervention
Idiopathic laryngotracheal stenosis
 Surgical Technique Idiopathic laryngotracheal stenosis Christina L. Costantino, Douglas J. Mathisen Massachusetts General Hospital, Boston, MA 02114, USA Correspondence to: Douglas J. Mathisen, MD. Massachusetts
Surgical Technique Idiopathic laryngotracheal stenosis Christina L. Costantino, Douglas J. Mathisen Massachusetts General Hospital, Boston, MA 02114, USA Correspondence to: Douglas J. Mathisen, MD. Massachusetts
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD
 CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
College Hospital, London, over the last five years.
 Archives of Disease in Childhood, 1986, 61, 686-690 Management of subglottic stenosis: two centres experience from R E QUINEY, M G SPENCER, C M BAILEY, J N G EVANS, AND J M GRAHAM Royal Ear Hospital, University
Archives of Disease in Childhood, 1986, 61, 686-690 Management of subglottic stenosis: two centres experience from R E QUINEY, M G SPENCER, C M BAILEY, J N G EVANS, AND J M GRAHAM Royal Ear Hospital, University
Congenital Laryngeal Anomalies
 Congenital Laryngeal Anomalies Prof. Hesham Abd Al-Fattah Alexandria - Egypt Embryology Resp primordium 3 rd wk Resp primordium separated by tracheoesophageal folds Fuse to form septum (4-5 wks) Larynx
Congenital Laryngeal Anomalies Prof. Hesham Abd Al-Fattah Alexandria - Egypt Embryology Resp primordium 3 rd wk Resp primordium separated by tracheoesophageal folds Fuse to form septum (4-5 wks) Larynx
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
Subglottic Stenosis: Current Concepts and Recent Advances
 ijhns IJHNS Review Article Subglottic Stenosis: Current 10.5005/jp-journals-10001-1272 Concepts and Recent Advances Subglottic Stenosis: Current Concepts and Recent Advances 1 Oshri Wasserzug, 2 Ari DeRowe
ijhns IJHNS Review Article Subglottic Stenosis: Current 10.5005/jp-journals-10001-1272 Concepts and Recent Advances Subglottic Stenosis: Current Concepts and Recent Advances 1 Oshri Wasserzug, 2 Ari DeRowe
CASE PRIMERS. Pediatric Anesthesia Fellowship Program. Laryngotracheal Reconstruction (LTR) Tufts Medical Center
 Tufts Medical Center") CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction
 The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
Use of the Silicone T-tube to Treat Tracheal Stenosis or Tracheal Injury
 Use of the Silicone T-tube to Treat Stenosis or Injury Chang-Jer Huang MD Backgound: stenosis or tracheal is a troublesome disease. Traditional temporary tracheostomy and reconstruction can resolve some
Use of the Silicone T-tube to Treat Stenosis or Injury Chang-Jer Huang MD Backgound: stenosis or tracheal is a troublesome disease. Traditional temporary tracheostomy and reconstruction can resolve some
Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy
 Case Report Brunei Int Med J. 2014; 10 (1): 55-59 Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy Zara
Case Report Brunei Int Med J. 2014; 10 (1): 55-59 Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy Zara
Review of literature suggests that there are three basic theories that attempt to explain the development of laryngomalacia.
 TITLE: Current Concepts in Diagnosis and Management of Laryngomalacia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 FACULTY PHYSICIANS: Shraddha Mukerji, MD and
TITLE: Current Concepts in Diagnosis and Management of Laryngomalacia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 FACULTY PHYSICIANS: Shraddha Mukerji, MD and
Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center
 Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center Children s Hospital of New Orleans Assistant Professor, Otolaryngology-Head & Neck Surgery, Louisiana State University. I do not have any
Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center Children s Hospital of New Orleans Assistant Professor, Otolaryngology-Head & Neck Surgery, Louisiana State University. I do not have any
Section 4.1 Paediatric Tracheostomy Introduction
 Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Steroid Therapy for Tracheal Stenosis in Children
 Steroid Therapy for Tracheal Stenosis in Children Clinical Experience in 4 Children with Severe Strictures H. Biemann Othersen, Jr., M.D. ABSTRACT Recently a refinement in the treatment of tracheal stenosis
Steroid Therapy for Tracheal Stenosis in Children Clinical Experience in 4 Children with Severe Strictures H. Biemann Othersen, Jr., M.D. ABSTRACT Recently a refinement in the treatment of tracheal stenosis
Clinical Presentation and Outcome Laryngotracheal Stenosis: A Retrospective Analysis
 Original Article DOI: 10.17354/ijss/2015/369 Clinical Presentation and Outcome Laryngotracheal Stenosis: A Retrospective Analysis L Somu 1, Prasanna Kumar Saravanam 1, A Ravikumar 2, Raadhika Shree 3 1
Original Article DOI: 10.17354/ijss/2015/369 Clinical Presentation and Outcome Laryngotracheal Stenosis: A Retrospective Analysis L Somu 1, Prasanna Kumar Saravanam 1, A Ravikumar 2, Raadhika Shree 3 1
ORIGINAL ARTICLE. Posterior Cricoidotomy Lumen Augmentation for Treatment of Subglottic Stenosis in Children
 Posterior Cricoidotomy Lumen Augmentation for Treatment of Subglottic Stenosis in Children Robert Thomé, PhD; Daniela Curti Thomé, MD ORIGINAL ARTICLE Objectives: To determine the results of posterior
Posterior Cricoidotomy Lumen Augmentation for Treatment of Subglottic Stenosis in Children Robert Thomé, PhD; Daniela Curti Thomé, MD ORIGINAL ARTICLE Objectives: To determine the results of posterior
4. Neoplastic: benign & malignant. 5. Allergic rhinitis & nasal polyp. 6. hypertrophied tonsils or adenoids. L 5
 L 5 Stertor& Stridor Stertor& stridor are both auditory manifestation of disordered respiratory function. Stertor: Is a low pitched snoring or snuffly sound caused by obstruction of the airway above the
L 5 Stertor& Stridor Stertor& stridor are both auditory manifestation of disordered respiratory function. Stertor: Is a low pitched snoring or snuffly sound caused by obstruction of the airway above the
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Airway Concerns. Trouble Breathing. Anywhere from nose to lungs. Neonates are obligate nasal breathers. Nasal symptoms:
 Pediatric Airway Naren Venkatesan, MD Mentor: Harold Pine, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology Head & Neck Surgery Grand Rounds Presentation April 26, 2013
Pediatric Airway Naren Venkatesan, MD Mentor: Harold Pine, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology Head & Neck Surgery Grand Rounds Presentation April 26, 2013
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction. Nathan Page, MD Pediatrics in the Red Rocks June?
 Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Audra Fuller MD, Mark Sigler MD, Shrinivas Kambali MD, Raed Alalawi MD
 Clinical Series Successful treatment of post-intubation tracheal stenosis with balloon dilation, argon plasma coagulation, electrocautery and application of mitomycin C Audra Fuller MD, Mark Sigler MD,
Clinical Series Successful treatment of post-intubation tracheal stenosis with balloon dilation, argon plasma coagulation, electrocautery and application of mitomycin C Audra Fuller MD, Mark Sigler MD,
Tracheal Trauma: Management and Treatment. Kosmas Iliadis, MD, PhD, FECTS
 Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Neonatal Stridor. Neonatology Roy Rajan, MD. Assistant Professor, Pediatric Otolaryngology Emory University
 Neonatal Stridor Neonatology 2015 Roy Rajan, MD Assistant Professor, Pediatric Otolaryngology Emory University Disclosures None 2 Goals/Objectives Describe embryology related to laryngeal development Define
Neonatal Stridor Neonatology 2015 Roy Rajan, MD Assistant Professor, Pediatric Otolaryngology Emory University Disclosures None 2 Goals/Objectives Describe embryology related to laryngeal development Define
Management of Pediatric Tracheostomy
 Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Dr. Sami Zaqout Faculty of Medicine IUG
 The Nose External Nose Nasal Cavity External Nose Blood and Nerve Supplies of the External Nose Blood Supply of the External Nose The skin of the external nose Branches of the ophthalmic and the maxillary
The Nose External Nose Nasal Cavity External Nose Blood and Nerve Supplies of the External Nose Blood Supply of the External Nose The skin of the external nose Branches of the ophthalmic and the maxillary
Preliminary Results of Intraoperative Mitomycin-C in the Treatment and Prevention of Glottic and Subglottic Stenosis
 Journal of Voice Vol. 14, No. 2, pp. 282-286 2000 Singular Publishing Group Preliminary Results of Intraoperative Mitomycin-C in the Treatment and Prevention of Glottic and Subglottic Stenosis *Reza Rahbar,
Journal of Voice Vol. 14, No. 2, pp. 282-286 2000 Singular Publishing Group Preliminary Results of Intraoperative Mitomycin-C in the Treatment and Prevention of Glottic and Subglottic Stenosis *Reza Rahbar,
Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic Pause: Experience in 5 Children
 BioMed Research International, Article ID 397295, 4 pages http://dx.doi.org/10.1155/2014/397295 Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic
BioMed Research International, Article ID 397295, 4 pages http://dx.doi.org/10.1155/2014/397295 Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic
James H. Liu, M.D., FAAP Curriculum Vitae
 James H. Liu, M.D., FAAP Curriculum Vitae EDUCATION/WORK 09/1985-05/1988 University of Houston; Houston, TX, B.S. Biology 09/1988-05/1992 Baylor College of Medicine; Houston, TX, Medical Degree 07/1992-06/1994
James H. Liu, M.D., FAAP Curriculum Vitae EDUCATION/WORK 09/1985-05/1988 University of Houston; Houston, TX, B.S. Biology 09/1988-05/1992 Baylor College of Medicine; Houston, TX, Medical Degree 07/1992-06/1994
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
PANELISTS. Controversial Issues In Common Interventions In ORL 4/10/2014
 Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
IAEM Clinical Guideline 9 Laryngomalacia. Version 1 September, Author: Dr Farah Mustafa
 IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Stridor in Children. Agrício Nubiato Crespo and Rodrigo Cesar e Silva
 Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Airway Management in the ICU
 Airway Management in the ICU New developments in management of epistaxis. April 28, 2008 Methods of airway control Non surgical BIPAP CPAP Mask ventilation Laryngeal Mask Intubation Surgical Cricothyrotomy
Airway Management in the ICU New developments in management of epistaxis. April 28, 2008 Methods of airway control Non surgical BIPAP CPAP Mask ventilation Laryngeal Mask Intubation Surgical Cricothyrotomy
Surgical Management of Subglottic Stenosis
 Surgical Management of Subglottic Stenosis Cameron D. Wright, MD ubglottic stenosis is usually due to either endotracheal S tube ischemic necrosis or idiopathic larygotracheal stenosis. The ischemic area
Surgical Management of Subglottic Stenosis Cameron D. Wright, MD ubglottic stenosis is usually due to either endotracheal S tube ischemic necrosis or idiopathic larygotracheal stenosis. The ischemic area
Airway Endoscopy The Basics Neonatal Progressive Acute Quiz
 Endoscopy of the Airway Dave Albert Airway Endoscopy The Basics Neonatal Progressive Acute Quiz The laws of Poiseuille and Bernoulli French physician,physicist mathemetician and Dutch Swiss mathemetician
Endoscopy of the Airway Dave Albert Airway Endoscopy The Basics Neonatal Progressive Acute Quiz The laws of Poiseuille and Bernoulli French physician,physicist mathemetician and Dutch Swiss mathemetician
4/24/2017. Tracheal Stenosis. Tracheal Stenosis. Tracheal Stenosis. Tracheal Stenosis. Tracheal Stenosis Endoscopic & Surgical Management
 Endoscopic & Surgical Management Pressure ulceration Healing: granulation cicatrization contraction Ann Surg 1969;169:334-348 Gary Schwartz, MD Department of Thoracic Surgery and Lung Transplantation Baylor
Endoscopic & Surgical Management Pressure ulceration Healing: granulation cicatrization contraction Ann Surg 1969;169:334-348 Gary Schwartz, MD Department of Thoracic Surgery and Lung Transplantation Baylor
12 Larynx. I - Cartilages. Learning Objectives
 12 Larynx Learning Objectives By the end of this topic you should be able to: Identify the cartilages, membranes, muscles and nerves of the larynx. Describe the attachments of the larynx to other structures
12 Larynx Learning Objectives By the end of this topic you should be able to: Identify the cartilages, membranes, muscles and nerves of the larynx. Describe the attachments of the larynx to other structures
A study on paediatric stridor causes and management: case series
 International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
T1/T2 LARYNX CANCER. Click to edit Master Presentation Date. Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery
 ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
STRIDOR. Respiratory system. Lecture
 STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
Pediatric tracheal procedures are uncommon and represent
 ORIGINAL ARTICLES: GENERAL THORACIC Pediatric Tracheal Surgery Cameron D. Wright, MD, Brian B. Graham, M Eng, Hermes C. Grillo, MD, John C. Wain, MD, and Douglas J. Mathisen, MD Division of General Thoracic
ORIGINAL ARTICLES: GENERAL THORACIC Pediatric Tracheal Surgery Cameron D. Wright, MD, Brian B. Graham, M Eng, Hermes C. Grillo, MD, John C. Wain, MD, and Douglas J. Mathisen, MD Division of General Thoracic
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience. Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore
 Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Eosinophilic Esophagitis: Extraesophageal Manifestations
 Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Ovid: Van Den Abbeele: Laryngoscope, Volume 109(8).August
.August") Full Text The American Laryngological, Rhinological & Otalogical Society, Inc. Volume 109(8), August 1999, pp 1281-1286 Surgical Removal of Subglottic Hemangiomas in Children [Independent Papers] Van Den
Full Text The American Laryngological, Rhinological & Otalogical Society, Inc. Volume 109(8), August 1999, pp 1281-1286 Surgical Removal of Subglottic Hemangiomas in Children [Independent Papers] Van Den
Hyoid Bone. Lower Airway. Aspiration. Larynx. Cartilages of the Larynx. Larynx Tracheobronchial Tree (TB Tree) Trachea Bronchi Bronchioles
 Trachea Bronchi Bronchioles") Lower Airway Larynx Tracheobronchial Tree (TB Tree) Trachea Bronchi Bronchioles Respiratory Terminal Hyoid Bone Not part of the larynx. The Hyoid bone is an anchor for the anterior muscles of the neck
Lower Airway Larynx Tracheobronchial Tree (TB Tree) Trachea Bronchi Bronchioles Respiratory Terminal Hyoid Bone Not part of the larynx. The Hyoid bone is an anchor for the anterior muscles of the neck
BILATERAL ABDUCTOR VOCAL CORD PALSY. Dr NITYA G Final year PG KIMS
 BILATERAL ABDUCTOR VOCAL CORD PALSY Dr NITYA G Final year PG KIMS INTRODUCTION Vocal cord paralysis is a sign of a disease It results from dysfunction of Recurrent laryngeal nerves on both sides Paralysis
BILATERAL ABDUCTOR VOCAL CORD PALSY Dr NITYA G Final year PG KIMS INTRODUCTION Vocal cord paralysis is a sign of a disease It results from dysfunction of Recurrent laryngeal nerves on both sides Paralysis
Role of Montgomery T-tube in laryngotracheal stenosis
 International Journal of Otorhinolaryngology and Head and Neck Surgery Rakesh BS et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Jan;3(1):61-65 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937 Original
International Journal of Otorhinolaryngology and Head and Neck Surgery Rakesh BS et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Jan;3(1):61-65 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937 Original
90 th Annual Meeting The American Association for Thoracic Surgery May 1, 2010 Toronto, Ontario, Canada. Slide Tracheoplasty
 90 th Annual Meeting The American Association for Thoracic Surgery May 1, 2010 Toronto, Ontario, Canada Congenital Skills Course Slide Tracheoplasty Carl Lewis Backer, MD A.C. Buehler Professor of Surgery
90 th Annual Meeting The American Association for Thoracic Surgery May 1, 2010 Toronto, Ontario, Canada Congenital Skills Course Slide Tracheoplasty Carl Lewis Backer, MD A.C. Buehler Professor of Surgery
The Paediatric Voice Clinic
 The Paediatric Voice Clinic Smillie I 1, McManus K 1, Cohen W 2, Wynne D1. Department of Paediatric Otolaryngology, Royal Hospital for Sick Children, Glasgow. 2 School of Psychological Sciences and Health,
The Paediatric Voice Clinic Smillie I 1, McManus K 1, Cohen W 2, Wynne D1. Department of Paediatric Otolaryngology, Royal Hospital for Sick Children, Glasgow. 2 School of Psychological Sciences and Health,
Lecture Overview. Respiratory System. Martini s Visual Anatomy and Physiology First Edition. Chapter 20 - Respiratory System Lecture 11
 Martini s Visual Anatomy and Physiology First Edition Martini Ober Chapter 20 - Respiratory System Lecture 11 1 Lecture Overview Overview of respiration Functions of breathing Organs of the respiratory
Martini s Visual Anatomy and Physiology First Edition Martini Ober Chapter 20 - Respiratory System Lecture 11 1 Lecture Overview Overview of respiration Functions of breathing Organs of the respiratory
Pediatrics Grand Rounds 25 October University of Texas Health Science Center at San Antonio, Texas
 PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-