Anaesthesia in the Beach Chair Posi0on. NEURO SIG Mee0ng Queenstown Mark Hayman MBBS, MPH, FANZCA
|
|
|
- Roland Stone
- 6 years ago
- Views:
Transcription

1 Anaesthesia in the Beach Chair Posi0on NEURO SIG Mee0ng Queenstown Mark Hayman MBBS, MPH, FANZCA
2 Outline 1. Incidence of strokes during beach chair posi0oning (BCP) 2. Physiology of CBF in upright posi0on 3. Monitoring for inadequate CBF 4. Management sugges0ons 5. Conclusions
3 None! Disclosures
4 Case Report: NSW yo former rugby player died of a massive stroke during arthroscopic shoulder surgery in beach- chair posi0on...caused by a failure to es0mate and maintain an appropriate level of mean arterial pressure in the blood supply of the brain (NSW coroner) recommenda/on that all anaesthe0c departments develop guidelines for the appropriate adjustment for the hydrosta0c gradient by anaesthe0sts when calcula0ng MAP for beach- chair surgery.
5 Other case reports 4 cases reported by Pohl & Cullen in 2005, ages recent cases from France with GA & interscalene block, ages Common features: young pa0ents, minor comorbi0es & periods of intra- op hypotension. Morbidity presumed to be result of ischaemic stroke due to cerebral hypoperfusion. Pohl & Cullen, J Clin Anesth, 2005 Villevieille, Ann Fr Anesth, 2012
? ACom? PCom CTA: incomplete circle of willis.")
6 Case: Incomplete Circle of Willis 50yo male, 180cm tall, smoker, Pre- op BP 110/75 arm = mmHg, lowest MAP=61mmHg ( Head)? ACom? PCom CTA: incomplete circle of willis. 2 months: Lei Anterior & Middle Cerebral Artery territory infarct Drummond, A&A, 2012
7 Incidence of Brain Injury following surgery in N=5177 Retrospec1ve Series Shoulder Surgery Neuro Cases Beach Chair Posi0on? BP Measureme nt A Line (heart) n=682 NIBP n=3545 A line (heart) n=422 A Line (head) n=528 Av. Mean BP Average BP Drop % % Pa1ents >1 episode BP Drop >40% from baseline % % No immediate postopera0ve catastrophic outcomes occurred, upper 95% CI = 7 per Average Hypotensio n Time per episode 16.6min 52% 16.7min Pin- On & Munis, A&A 2013


8 Incidence of Intraopera0ve Stroke Survey of orthopaedic surgeons, cases > 200K Es0mated stroke rate: 0.004% All events occurred in pa0ents in the BCP Friedman, Orthopaedics, 2009 And yet hypotension is common in the BCP posi0on. Pin- On, 2013, Friedman 2009, Yadeau 2011, Rohrbaugh 2013 So is hypotension the cause? Perhaps Lam & Baldwin, Blood Pressure & Adverse Periopera/ve Neurologic Outcomes: An Uncomfortable Posi/on, A&A 2012


9 What is Hypotension? BP while asleep: drop 30% from baseline SBP MAP Soo et al, Anaesthesia, 2011



10 Blood Pressure what is baseline? Pre- op baseline MAP mmhg Day0me median - 9.5% Sleep median % Sleep nadir Intra- op nadir % % Soo et al, Anaesthesia, 2011


11 Siphon Model of CBF Head? A V Flow α A - V

12 Does a Siphon exist in upright humans? CVP IJV CVP EJV IJVP=Internal Jugular Venous Base of skull Dawson et al, Standing up to the challenge of standing: a siphon does not support CBF in humans, ajpregu, 2004.

13 & in Giraffa camelopardalis MAP = 118 Cranial VP = - 4 5m MAP = 200 CVP = 4 Brondum, Jugular venous pooling during lowering of the head affects blood pressure of the anesthe/zed giraffe, AmJPhysiolRegulIntegrCompPhsiol, 2009.

14 Monitoring NIRS BP TCD?EEG


15 Cerebral Oximetry (SctO2) OXIPLEX Con0nuous wave technology: interpret photon scaver & absorp0on Frequency domain systems differen0ate scaver & absorp0on. Davie et al, Anesthesiology, 2012
16 NIRS in Sixng versus Lateral Posi0on Cerebral Desatura0on Events (CDEs) LDP = 0% BCP = 80% Murphy, A&A, 111(2), 2010
17 SctO 2 & Upright posi0on N=20 SctO2 LeN SctO2 Right Head Awake Supine Upright Min Value 57* 59* ~30 * p < 0.05 comapred to awake & compared to supine asleep Decrease of >20% in SctO 2 in >80% pa0ents. Decreases in SctO 2 correlated with BP drops (R= 0.6) & EtCO 2 (R = 0.47) Moerman et al, Eur J Anaesthesiology, 2012
18 Influence of BP on Cerebral Perfusion & Oxygena0on SctO2 vs MAP MCAv mean vs MAP Change in MAP (mmhg) Change in MAP (mmhg) Lucas, Blood Pressure & Cerebral Autoregula/on, Hypertension, 2010
19 SctO2 with phenylephrine & head up posi0on? N=34 RCT Saline Phenylephrine SCO2% MAP MCAv SCO2% MAP MCAv Rm Air Pre- O Post Induc0on Post Infusion Upright Posi0on MAP: level of head Soeding et al, BJA 2013
20 Sct0 2 & SjVO 2 SctO 2 SjVO 2 Brassard, BJA, 2009

21 Cerebral Oximetry & SjvO2% SctO2% SjvO2% Jeong et al, Anesthesiology, 2012


22 NIRS & Extracranial Contamina0on % change from baseline of SctO2 Davie & Grocoa, Anesthesiology, 2012

23 Theore0cal explana0on for SctO2 changes seen with phenylephrine. Modified from Meng & Gelb, BJA, 2012

24 Transcranial Doppler (TCD) Hypercapnia used to validate TCD against Xenon. Correla0on: R = MCAv Reac0vity (Doppler) CBF Reac0vity (Xenon) Bishop et al, Stroke, 1986.
25 TCD & Hypotension with Beach Chair Posi0oning Possible mechanisms for reduced MCAv: 1. Impaired autoregulatory response 2. Cerebral arterial pressure may have been below lower limit of autoregula0on head <50mmHg in 11 of 19 pa0ents. McCulloch et al, AAIC, 2010
26 Components of Autoregulatory response azfp McCulloch et al, AAIC, 2010
27 Influence of BP on MCAv Lucas, Blood Pressure & Cerebral Autoregula/on, Hypertension, 2010
28 The impact of Cardiac Output on MCAv? MCAv Cardiac Output l/min Ogoh, et al, J Physiol, 2005

29 Management Sugges0ons
30 Avoid Sixng Posi0on US Survey of Shoulder Surgeons Low rate of stroke reported rate in the beach chair posi0on % % But.. All cerebrovascular events were associated with surgeries in the beach chair posi0on. Friedman, Orthopedics, 2009, 32(4)
31 Avoid GA? Koh & Murphy et al, J Shoulder Elbow Surg, 2013
32 Maintain a Normal BP Supine with 20% BP level of heart Beach Chair with 20% BP drop Awake

33 Maintain or augment Cardiac Output MAP CO SctO2 Supine pa0ents, controlled ven0la0on, propofol/remi. Meng, BJA, 2011
34 Head Posi0on Toole J, Arch Neurol, 1960


35 Vola0le vs Propofol? Jeong et al, 2012
36 Other Monitors: Cerebral Oximtery or TCD? Interpret Cerebral Oximetry with cau0on. Future studies may provide clinical outcome data. TCD probably more robust but less convenient and unlikely to become a standard monitor.
37 Summary Incidence of stroke in BCP: seems to be low. Mechanism is likely to be hypoperfusion in these cases. Cerebral Oximetry as monitor of cerebral oxygena0on in BCP is problema0cal, par0cularly following vasopressor use. TCD is a more robust but less convenient monitor of CBF BP measurement or calcula0on at level of head should be standard of care (there is no siphon) Maintenance of pre- op BP is probably reasonable approach. Consider augmen0ng CO rather than simply BP support. Consider use of regional & seda0on rather than GA. Maintain neutral head posi0on. If GA used aim for mild hypercapnia & perhaps use vola0le rather than propofol based GA.

38 Discouraging data on the anti-depressant
Anesthesia and the beach chair position
 Anesthesia and the beach chair position Paul Picton Associate Professor Senior Associate Chair of Clinical Affairs and Quality University of Michigan Medical School, Ann Arbor NIH UL1TR000433 Disclosures
Anesthesia and the beach chair position Paul Picton Associate Professor Senior Associate Chair of Clinical Affairs and Quality University of Michigan Medical School, Ann Arbor NIH UL1TR000433 Disclosures
Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology
 Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology") Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
TCD in Anaesthesiology
 TCD in Anaesthesiology Background: TCD has often been used to evaluate the impact of narcotics on cerebral autoregulation. This was related to general research reasons and is not relevant for daily monitoring
TCD in Anaesthesiology Background: TCD has often been used to evaluate the impact of narcotics on cerebral autoregulation. This was related to general research reasons and is not relevant for daily monitoring
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2): Oxford University Press
: Oxford University Press") Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
Managing Hypertension in the Perioperative Arena
 Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Effects of Positioning on Cerebral Oxygenation
 Curr Anesthesiol Rep (2013) 3:184 196 DOI 10.1007/s40140-013-0020-y NEUROANESTHESIA (JJ PASTERNAK, SECTION EDITOR) Effects of Positioning on Cerebral Oxygenation Paul Soeding Published online: 23 May 2013
Curr Anesthesiol Rep (2013) 3:184 196 DOI 10.1007/s40140-013-0020-y NEUROANESTHESIA (JJ PASTERNAK, SECTION EDITOR) Effects of Positioning on Cerebral Oxygenation Paul Soeding Published online: 23 May 2013
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Parien' JJ, Mongardon N, Megarbane B et al. Intravascular Complica'ons of Central Venous Catheteriza'on by Inser'on Site. New England Journal of
 Parien' JJ, Mongardon N, Megarbane B et al. Intravascular Complica'ons of Central Venous Catheteriza'on by Inser'on Site. New England Journal of Medicine 2015; 373: 1220-9 The Study 3SITES Study Mul'na'onal,
Parien' JJ, Mongardon N, Megarbane B et al. Intravascular Complica'ons of Central Venous Catheteriza'on by Inser'on Site. New England Journal of Medicine 2015; 373: 1220-9 The Study 3SITES Study Mul'na'onal,
Fluid management. Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center
 Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases
 Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy
 Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy A 44 year old female undergoing 10 hour Cytoreductive (CRS) procedure followed by Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy A 44 year old female undergoing 10 hour Cytoreductive (CRS) procedure followed by Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
Regional Anaesthesia for Caesarean Section Warwick D. Ngan Kee
 Regional Anaesthesia for Caesarean Section Warwick D. Ngan Kee Chair, Department of Anesthesiology Sidra Medicine Doha, Qatar D I S C L O S U R E S No financial disclosures No industry affiliations No
Regional Anaesthesia for Caesarean Section Warwick D. Ngan Kee Chair, Department of Anesthesiology Sidra Medicine Doha, Qatar D I S C L O S U R E S No financial disclosures No industry affiliations No
Agonistic Autoantibodies to Angiotensin II Type I Receptor Contributes Partly to Placental Ischemia-Induced Cerebrovascular Abnormalities
 Agonistic Autoantibodies to Angiotensin II Type I Receptor Contributes Partly to Placental Ischemia-Induced Cerebrovascular Abnormalities Junie Paula Warrington 1, Fan Fan 1, Babbette B. LaMarca 1, Ralf
Agonistic Autoantibodies to Angiotensin II Type I Receptor Contributes Partly to Placental Ischemia-Induced Cerebrovascular Abnormalities Junie Paula Warrington 1, Fan Fan 1, Babbette B. LaMarca 1, Ralf
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
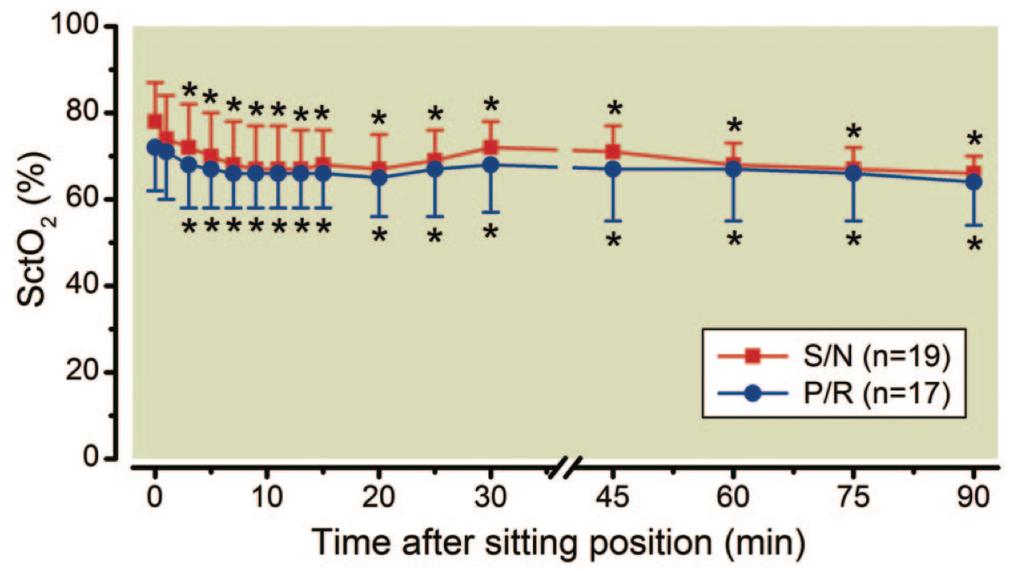
Cerebral Oximetry Readings in the Sitting Position Versus Supine Position for Patients Undergoing General Anesthesia
 The University of Southern Mississippi The Aquila Digital Community Doctoral Nursing Capstone Projects Fall 12-11-2015 Cerebral Oximetry Readings in the Sitting Position Versus Supine Position for Patients
The University of Southern Mississippi The Aquila Digital Community Doctoral Nursing Capstone Projects Fall 12-11-2015 Cerebral Oximetry Readings in the Sitting Position Versus Supine Position for Patients
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy
 Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
The Case: A 64 yo man with chronic back pain has elective multilevel lumbar spinal surgery
 The Case: A 64 yo man with chronic back pain has elective multilevel lumbar spinal surgery The Case: Upon awakening from anesthesia, he is blind in both eyes After Non-Ocular Surgeries Nancy J. Newman,
The Case: A 64 yo man with chronic back pain has elective multilevel lumbar spinal surgery The Case: Upon awakening from anesthesia, he is blind in both eyes After Non-Ocular Surgeries Nancy J. Newman,
Brain under pressure Impact of vasopressors
 Brain under pressure Impact of vasopressors Brain dysfunction in sepsis Incidence: - Varying nomenclature: sepsis-associated encephalopathy, delirium, brain dysfunction - Consistently recognized as frequent:
Brain under pressure Impact of vasopressors Brain dysfunction in sepsis Incidence: - Varying nomenclature: sepsis-associated encephalopathy, delirium, brain dysfunction - Consistently recognized as frequent:
Continuous monitoring of cardiac output: why and how
 33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Influence of variations in systemic blood flow and pressure on cerebral and systemic oxygen saturation in cardiopulmonary bypass patients
 British Journal of Anaesthesia 111 (4): 619 26 (2013) Advance Access publication 5 June 2013. doi:10.1093/bja/aet197 Influence of variations in systemic blood flow and pressure on cerebral and systemic
British Journal of Anaesthesia 111 (4): 619 26 (2013) Advance Access publication 5 June 2013. doi:10.1093/bja/aet197 Influence of variations in systemic blood flow and pressure on cerebral and systemic
Evalua&on and Management of Obstruc&ve Sleep Apnea in the Periopera&ve Period. Clinical Commi=ee Society of Anesthesia and Sleep Medicine
 Evalua&on and Management of Obstruc&ve Sleep Apnea in the Periopera&ve Period Clinical Commi=ee Society of Anesthesia and Sleep Medicine Goals 1. Introduc0on 2. Preopera0ve Evalua0on 3. Intraopera0ve Risk
Evalua&on and Management of Obstruc&ve Sleep Apnea in the Periopera&ve Period Clinical Commi=ee Society of Anesthesia and Sleep Medicine Goals 1. Introduc0on 2. Preopera0ve Evalua0on 3. Intraopera0ve Risk
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Impact of phenylephrine administration on cerebral tissue oxygen saturation and blood volume is modulated by carbon dioxide in anaesthetized patients
 British Journal of Anaesthesia 108 (5): 815 22 (2012) Advance Access publication 4 March 2012. doi:10.1093/bja/aes023 Impact of phenylephrine administration on cerebral tissue oxygen saturation and blood
British Journal of Anaesthesia 108 (5): 815 22 (2012) Advance Access publication 4 March 2012. doi:10.1093/bja/aes023 Impact of phenylephrine administration on cerebral tissue oxygen saturation and blood
Closed-loop Double-pump Automated System Manual Boluses
 Closed-loop Double-pump Automated System versus Manual Boluses to treat Hypotension during Spinal Anaesthesia for Caesarean Section: randomised controlled trial Dr. Ban Leong SNG MBBS, MMED, FANZCA, FFPMANZCA,
Closed-loop Double-pump Automated System versus Manual Boluses to treat Hypotension during Spinal Anaesthesia for Caesarean Section: randomised controlled trial Dr. Ban Leong SNG MBBS, MMED, FANZCA, FFPMANZCA,
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Why is my pa*ent in shock?
 Why is my pa*ent in shock? Eric Schmidt, MD Denver Health Medical Center University of Colorado School of Medicine Case vigne*e You are called to the ER to see a 27 year old female with three days of nausea,
Why is my pa*ent in shock? Eric Schmidt, MD Denver Health Medical Center University of Colorado School of Medicine Case vigne*e You are called to the ER to see a 27 year old female with three days of nausea,
Perioperative Infarcts: Epidemiology, predictors and post-op monitoring
 Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
Faculty Disclosure. Sanjay P. Singh, MD, FAAN. Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion
 Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Controversies in Carotid Endarterectomy
 Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research
Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research
Declaring Brain Death. Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
 Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Labor Epidural: Local Anesthetics and Beyond
 Goals: Labor Epidural: Local Anesthetics and Beyond Pedram Aleshi MD The Changing Practice of Anesthesia September 2012 Review Concept of MLAC Local anesthetic efficacy Local anesthetic sparing effects:
Goals: Labor Epidural: Local Anesthetics and Beyond Pedram Aleshi MD The Changing Practice of Anesthesia September 2012 Review Concept of MLAC Local anesthetic efficacy Local anesthetic sparing effects:
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Dynamic autoregulatory response after severe head injury
 J Neurosurg 97:1054 1061, 2002 Dynamic autoregulatory response after severe head injury ROMAN HLATKY, M.D., YU FURUYA, M.D., PH.D., ALEX B. VALADKA, M.D., JORGE GONZALEZ, M.D., ARI CHACKO, M.D., YASU MIZUTANI,
J Neurosurg 97:1054 1061, 2002 Dynamic autoregulatory response after severe head injury ROMAN HLATKY, M.D., YU FURUYA, M.D., PH.D., ALEX B. VALADKA, M.D., JORGE GONZALEZ, M.D., ARI CHACKO, M.D., YASU MIZUTANI,
Continuous cerebral autoregulation monitoring
 Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Yuko Kondo, Kaoru Sakatani, Noriya Hirose, Takeshi Maeda, Jitsu Kato, Setsuro Ogawa, and Yoichi Katayama
 Chapter 16 Effect of Spinal Anesthesia for Elective Cesarean Section on Cerebral Blood Oxygenation Changes: Comparison of Hyperbaric and Isobaric Bupivacaine Yuko Kondo, Kaoru Sakatani, Noriya Hirose,
Chapter 16 Effect of Spinal Anesthesia for Elective Cesarean Section on Cerebral Blood Oxygenation Changes: Comparison of Hyperbaric and Isobaric Bupivacaine Yuko Kondo, Kaoru Sakatani, Noriya Hirose,
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Cesarean section for breech presentation. Jonathan H. Waters, M.D.
 Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
On behalf of the education Committee of the SNACC
 Neuro Quiz 36 Cerebral Oximetry Shobana Rajan M.D, Assistant Professor Anesthesiology Cleveland Clinic Quiz Team; Suneeta Gollapudy M.D, Angele Marie Theard M.D, Verghese Cherian M.D On behalf of the education
Neuro Quiz 36 Cerebral Oximetry Shobana Rajan M.D, Assistant Professor Anesthesiology Cleveland Clinic Quiz Team; Suneeta Gollapudy M.D, Angele Marie Theard M.D, Verghese Cherian M.D On behalf of the education
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP?
 7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Precision Medicine in Neurocritical Care: Should we individualize care?
 Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
NEWROSIM. Traumatic Brain Injury & Stroke Care Training Solution
 NEWROSIM Traumatic Brain Injury & Stroke Care Training Solution 10 Preprogrammed TBI and Stroke Scenarios NewroSim Scenario Guidebook Powerful computer-based hemodynamic model Interactive transcranial
NEWROSIM Traumatic Brain Injury & Stroke Care Training Solution 10 Preprogrammed TBI and Stroke Scenarios NewroSim Scenario Guidebook Powerful computer-based hemodynamic model Interactive transcranial
ECMO and VAD implantation
 1 Udine ECMO Workshop ECMO and VAD implantation Prof. Tomaso Bottio Division of Cardiac Surgery (Director Prof. Gino gerosa) ECMO Extracorporeal membrane oxygena1on (ECMO) is a rescue therapy to support
1 Udine ECMO Workshop ECMO and VAD implantation Prof. Tomaso Bottio Division of Cardiac Surgery (Director Prof. Gino gerosa) ECMO Extracorporeal membrane oxygena1on (ECMO) is a rescue therapy to support
Anesthesia for Total Hip and Knee Arthroplasty
 Anesthesia for Total Hip and Knee Arthroplasty Typical approach Describe anesthesia technique Rather Describe issues with THA and TKA How anesthesia can modify Issues Total Hip Total Knee Blood Loss ++
Anesthesia for Total Hip and Knee Arthroplasty Typical approach Describe anesthesia technique Rather Describe issues with THA and TKA How anesthesia can modify Issues Total Hip Total Knee Blood Loss ++
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
REGIONAL/LOCAL ANESTHESIA and OBESITY
 REGIONAL/LOCAL ANESTHESIA and OBESITY Jay B. Brodsky, MD Stanford University School of Medicine Jbrodsky@stanford.edu Potential Advantages Regional compared to General Anesthesia Minimal intra-operative
REGIONAL/LOCAL ANESTHESIA and OBESITY Jay B. Brodsky, MD Stanford University School of Medicine Jbrodsky@stanford.edu Potential Advantages Regional compared to General Anesthesia Minimal intra-operative
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
The contribution of the external carotid artery to cerebral perfusion in carotid disease
 The contribution of the external carotid artery to cerebral perfusion in carotid disease Shirley J. Fearn, PhD, FRCS, Andrew J. Picton, BSc, Andrew J. Mortimer, MD, FRCA, Andrew D. Parry, MBChB, FRCS,
The contribution of the external carotid artery to cerebral perfusion in carotid disease Shirley J. Fearn, PhD, FRCS, Andrew J. Picton, BSc, Andrew J. Mortimer, MD, FRCA, Andrew D. Parry, MBChB, FRCS,
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN
 Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation
 Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
Ancillary Testing in Death
 Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease
 The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
Acute Stroke Treatment: Mechanical Thrombectomy
 Acute Stroke Treatment: Mechanical Thrombectomy Rudy Noppens Department of Anesthesiology & Perioperative Medicine CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure
Acute Stroke Treatment: Mechanical Thrombectomy Rudy Noppens Department of Anesthesiology & Perioperative Medicine CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure
Defining intra-operative hypotension a pilot comparison of blood pressure during sleep and general anaesthesia*
 doi:10.1111/j.1365-2044.2011.06657.x ORIGINAL ARTICLE Defining intra-operative hypotension a pilot comparison of blood pressure during sleep and general anaesthesia* J. C. L. Soo, 1 S. Lacey, 2 R. Kluger
doi:10.1111/j.1365-2044.2011.06657.x ORIGINAL ARTICLE Defining intra-operative hypotension a pilot comparison of blood pressure during sleep and general anaesthesia* J. C. L. Soo, 1 S. Lacey, 2 R. Kluger
Fluid Balance in an Enhanced Recovery Pathway. Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017
 Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
occlusions. Cerebral perfusion is driven fundamentally by regional cerebral
 Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How to manage the left subclavian and left vertebral artery during TEVAR
 How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
Klinikum Frankfurt Höchst
 Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA?
 INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA? - A Case Report - DIDEM DAL *, AYDIN ERDEN *, FATMA SARICAOĞLU * AND ULKU AYPAR * Summary Choroidal melanoma is the most
INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA? - A Case Report - DIDEM DAL *, AYDIN ERDEN *, FATMA SARICAOĞLU * AND ULKU AYPAR * Summary Choroidal melanoma is the most
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
IMPROVE PATIENT OUTCOMES AND SAFETY IN ADULT CARDIAC SURGERY.
 Clinical Evidence Guide IMPROVE PATIENT OUTCOMES AND SAFETY IN ADULT CARDIAC SURGERY. With the INVOS cerebral/somatic oximeter An examination of controlled studies reveals that responding to cerebral desaturation
Clinical Evidence Guide IMPROVE PATIENT OUTCOMES AND SAFETY IN ADULT CARDIAC SURGERY. With the INVOS cerebral/somatic oximeter An examination of controlled studies reveals that responding to cerebral desaturation
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Neuro Quiz 25 - Monitoring
 Neuro Quiz 25 - Monitoring This quiz is being published on behalf of the Education Committee of the SNACC Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey, PA Quiz Team Shobana
Neuro Quiz 25 - Monitoring This quiz is being published on behalf of the Education Committee of the SNACC Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey, PA Quiz Team Shobana
Extracranial to intracranial bypass for intracranial atherosclerosis
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
An algorithmic approach to the very high risk surgical patient
 An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Anesthesia Monitoring and Pa0ent Safety. Lauren Kreisberg, RVT
 Anesthesia Monitoring and Pa0ent Safety Lauren Kreisberg, RVT laurenkrvt@gmail.com Pa0ent History Presen0ng Complaint Age Sex (current estrus cycle in intact females) Medica0on history including all OTC
Anesthesia Monitoring and Pa0ent Safety Lauren Kreisberg, RVT laurenkrvt@gmail.com Pa0ent History Presen0ng Complaint Age Sex (current estrus cycle in intact females) Medica0on history including all OTC
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS
 GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
Why I m afraid of occlusive devices
 Why I m afraid of occlusive devices Cannes 28.06.2008 Carlo Cernetti Cardiology Department Mirano (Venice) MEET 2008 CANNES I HAVE NOT FINACIAL INTEREST/ARRANGEMENT OR AFFILIATION CONFLICT Obstructive
Why I m afraid of occlusive devices Cannes 28.06.2008 Carlo Cernetti Cardiology Department Mirano (Venice) MEET 2008 CANNES I HAVE NOT FINACIAL INTEREST/ARRANGEMENT OR AFFILIATION CONFLICT Obstructive
Cosa chiedo alla PtO 2
 Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
CATCH A WAVE.. INTRODUCTION NONINVASIVE HEMODYNAMIC MONITORING 4/12/2018
 WAVES CATCH A WAVE.. W I S C O N S I N P A R A M E D I C S E M I N A R A P R I L 2 0 1 8 K E R I W Y D N E R K R A U S E R N, C C R N, E M T - P Have you considered that if you don't make waves, nobody
WAVES CATCH A WAVE.. W I S C O N S I N P A R A M E D I C S E M I N A R A P R I L 2 0 1 8 K E R I W Y D N E R K R A U S E R N, C C R N, E M T - P Have you considered that if you don't make waves, nobody
WHICH CARDIAC OUTPUT MONITOR IN COLORECTAL ENHANCED RECOVERY? :
 WHICH CARDIAC OUTPUT MONITOR IN COLORECTAL ENHANCED RECOVERY? : RANDOMISED CONTROLLED NON-INFERIORITY TRIAL COMPARING LiDCOrapid AND OESOPHAGEAL DOPPLER MONITORS J van Dellen, S McCorkell, AB Williams
WHICH CARDIAC OUTPUT MONITOR IN COLORECTAL ENHANCED RECOVERY? : RANDOMISED CONTROLLED NON-INFERIORITY TRIAL COMPARING LiDCOrapid AND OESOPHAGEAL DOPPLER MONITORS J van Dellen, S McCorkell, AB Williams