Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
|
|
|
- Christopher Morton
- 5 years ago
- Views:
Transcription
1 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows


2 Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid Hemorrhage Hydrocephalus Malignant Infarction Cerebral Edema CNS Infections Hepatic Encephalopathy


3 Introduction Goal: To prevent secondary Injury to brain How: Ensure the brain is well perfused and minimize ischemic and pressure induced problems especially parts that are most susceptible





4 Assessment Clinically Monitors Standard Specific ICP CT SVO 2 Cortical PO 2 PRx TCD Cerebral Microdialysis EEG
 Normal Cerebral Blood Flow 50 ml/min/100g tissue Delivers 750 ml/min of blood (15 % CO) O 2 extraction: 35-50")
5 Cerebral Physiology Significant Energy Requirements 3-5 ml O 2 /min/100g tissue (94 % gray matter) Anesthesia, Hypothermia (27 C) (2 ml/min/ 100 gm tissue) Normal Cerebral Blood Flow 50 ml/min/100g tissue Delivers 750 ml/min of blood (15 % CO) O 2 extraction: %

6 Autoregulation

7 CBF in relation to PaCO 2, PaO 2 and ICP
8 Cerebral autoregulation. Dunn L T J Neurol Neurosurg Psychiatry 2002;73:i23-i by BMJ Publishing Group Ltd



9 Etiology of Cerebral Injury Lack of Nutrients/O 2 Isolated deficiency (hypoxia) Decreased perfusion Focal Insult Infarction Ischemic penumbra Avoid Hypoxia Hypotension Hypo or hypercarbia Hyperthermia Hypo or hyperglycemia
10 ICP Monitoring
 Constant drainage of venous blood to make room for arterial blood 1840 s idea of CSF was")
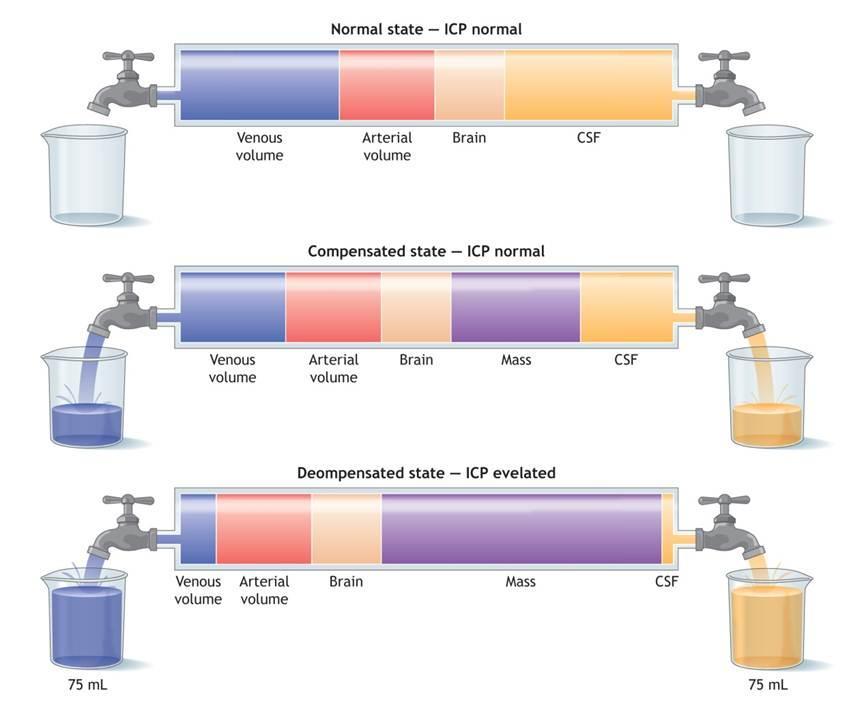
11 Historical Monro-Kellie Doctrine (1783) 1) Brain encased rigid structure 2) Brain is incompressible 3) Volume of blood in cranial vault is constant 4) Constant drainage of venous blood to make room for arterial blood 1840 s idea of CSF was accepted

12


13 Spatial Reserve ml in young individuals ml elderly due to cerebral atrophy
14

15 Cranial Contents Brain Blood CSF ICP Management Selective resection Craniectomy Osmolar therapy (Mannitol, HTS) Decrease metabolic rate -hypothermia -sedation / paralysis Head of the bed 30 degrees Mannitol Hyperventilate Drainage Mass Resection






16 Monitoring ICP Useful in Head Injury High Grade SAH ICH Mass lesions Meningitis Stroke Transducer Value of ICP Waveform Analysis Calculation of CPP Information on Intracerebral Compliance

17 ICP Monitoring Reasons for raised ICP Mass lesion Hypercapnea Hypoxemia hyperemia GCS 3-8 and: Abnormal CT: hematoma, contusion, swelling, herniation and compressed cisterns Normal CT: with 2 of the following Age> 40 Uni or bilateral posturing SBP < 90 mmhg
 Tympanic membrane Displacement (TMD) Optic Nerve Sheath Diameter MRI and CT Scans")
18 Methods to Measure ICP Invasive External Ventricular Drain (EVD) Microtransducer ICP Monitoring Devices Non Invasive Transcranial Doppler (TCD) Tympanic membrane Displacement (TMD) Optic Nerve Sheath Diameter MRI and CT Scans Fundoscopy/papilledema


19 Global versus Local Pressure Smaller pressure gradients within CNS exist across specific compartments No significant gradients under physiological conditions ICP probably best monitored as close to expanding lesion as possible No conclusive data as to circumstances of pressure gradients in CNS nor where routine bilateral ICP monitoring should be done

20 Anatomical Locations for Invasive Monitoring




21 EVD Gold Standard Monitoring, drainage of csf, administration of medication Insertion: traditional coronal burr hole at kocher s point with tip of evd in 3 rd ventricle



22 Bleeding: 5.7 % ( ) 0.61% clinically important (neurological deficits/surgical intervention) Infection Various sites, incorrect placement (reoperation), catheter defect 0-27% (3-12%) OR, prophylactic abx, tunnel catheter, minimal handling,? Silver impregnated catheters
")


23 Normal ICP: varies with age and position (supine) adult: 5-15 mmhg Children: 3-7 mmhg Infants: mmhg CPP: MAP- ICP Normal autoregulation between mmhg
 arterial pulsation")
 (?")
24 ICP Signal Normal ICP waveform has flow of 3 upstrokes P1: (percussion wave) arterial pulsation P2: (tidal wave) intracranial compliance P3: (dicrotic notch) (? Venous pulsation / aortic valve closure) P1 P2 P3
25 The volume pressure curve. Dunn L T J Neurol Neurosurg Psychiatry 2002;73:i23-i by BMJ Publishing Group Ltd

26 ICP treatment Elevated ICP can lead to herniation and irreversible brain damage and death Elevated ICP may lead to increased brain damage and increase cerebral edema Any cerebral lesion may cause set of vasomotoric paralysis and disrupt autoregulation

27 Intracranial herniations. Dunn L T J Neurol Neurosurg Psychiatry 2002;73:i23-i by BMJ Publishing Group Ltd
28
29 Waveform Analysis
30 Cerebral autoregulation. Dunn L T J Neurol Neurosurg Psychiatry 2002;73:i23-i by BMJ Publishing Group Ltd

31



32 Lundberg A, B and C Waves Lundberg A: *** Plateau Waves*** Pathological, severe loss of autoregulation, irregularly and without warning Rapid increase and decrease in pressure of mmhg lasting 5-20 min indicative of impending herniation Lundberg B: oscillations of waves/min crescendo manner to 5-30 mmhg higher than baseline associated with unstable ICP and vasospasm and velocity in MCA Lundberg C: 4-8 waves/min, smaller amplitude physiological interaction of cardiac and respiratory system
33


34

35

36 With one line change make the equation true IV = III + III VI = III + III III + III = III III = III = III Cognitively impaired, sleep deprived






37 Using ICP Calculating CPP CPP=MAP-ICP Looking at tissue perfusion pressure Goal mmhg (? 75 mmhg) Probably closer to MAP of May look at affects on ICP Perhaps another technology Relationship between ICP and Outcome Sustained elevation (>20 mmhg) associated with poor outcome My have lower mortality when ICP monitored and acted upon




38 ICP Despite newer technologies Remains robust Valuable information gained Therapeutic device Informs patient management decisions Has been the Cornerstone of management in the ICU of Acute Brain Injury How good is the foundation??
39 GCS 8 + abnormal CT: 53 63% had increased ICP GCS 8 + normal CT: 13 % had increased ICP Patients >40 years, SBP < 90 mmhg or posturing had similar rates of increased ICP as group with abnormal CT head
40

41
42

43
44

45
46 Outcome GCS >= OR a 3.07 se b 1.49, 95% CI c p- value <0.01 Hospital 28- day Mortality Mortality Overall , GCS < , GCS >= , < 0.01 a OR= odds ratio adjusted for age, apache, increased ICP on CT, mannitol, year of admission, craniotomy, subdural hematoma, diffuse axonal injury, systolic blood pressure < 90 mmhg and arterial oxygen tension < 70 mmhg b standard error c 95% confidence intervals p= 0.01, p=0.03 for interaction


47

48
49


50 Criticisms of study: External validity Ecuador & Bolivia E.g. 19% used barbiturates Access to rehabilitation Intraparenchymal monitors vs. EVD Is ICP the correct intervention? Is a trial of ICP monitoring the right question?
51 SjVO 2 Monitoring Cerebral Oxygen Use 1980 s-1990 s: Fiberoptic technologies Bedside oximetry SjVO 2 Monitoring Determination for ischemia Monitor effects of therapy for raised ICP



52 SjVO2 Monitoring Insertion Retrograde IJ line insertion usually Right Catheter Cannula: intermittent aspiration/sampling Fiberoptic: continuous


53 SjVO 2 Monitoring Problems Line Placement Contamination Slow blood aspiration Impede venous drainage
54 SjVO 2 Monitoring Normal % Global measure Doesn t detect local ischemia Specific not sensitive measurement tool May be useful in determining ICP treatment interventions Ex. hyperventilation

 Reduced Demand Sedation/ paralysis")
55 SjVO 2 Monitoring SjVO 2 < 50 % Increased demand High ICP Pain Seizure Decreased Supply Hypoxemia Hypotension Low cardiac output Anemia hyperventilation SjVO 2 > 80 % Brain hyperemia Seizures/shunt Sepsis Brain death (necrosis) Reduced Demand Sedation/ paralysis hypothermia

56 SjVO 2 Monitoring Cerebral Oxygen Extraction CEO 2 = SAO 2 -SjVO 2 SAH with Vasospasm CEO 2 may increase prior to neurological deficits May be able to track vasospasm with CEO 2



57 SjVO 2 Monitoring Limitations Invasive Sampling errors Low values trend toward poor outcomes Never shown as sole treatment to affect outcome Uses Assessing risk of ischemia Adjuvant to ICP monitoring
 Newer Direct")


58 Cortical PBO 2 Monitor (LICOX) Newer Direct placement of PBO 2 sensing electrode on cerebral cortex at time of craniotomy Monitors PbO2, PbCO2, ph and temperature PbO2: mmhg


59 Critical range: < 10 mmhg is high risk for ischemia Probably target values > mmhg Where do you insert? Contusion Penumbra Normal


60 Does PbO2 add anything to current regimen?: May target areas that are vulnerable that are currently assessed by our available modalities Weaknesses: Focal hypoxemia, not global Does not actually measure intracellular hypoxia Role of Microdialysis!

61 Neurosurgery 2011;69:1037
62 J Neurosurg 2010;113:571
63 J Neurosurg Nov;103(5):
64 In TBI, cerebral autoregulation is lost especially in peri-injury neuronal tissue and CBF becomes linearly dependent on CPP (therefore, directly proportional to MAP and inversely proportional to ICP) Resuscitation. 2001;22:
 Correlation coefficient of MAP & ICP Ranges between - 1 and")
65 Normal physiology Autoregulation maintains constant CBF Increased MAP = cerebral vasoconstriction Decreased MAP = cerebral vasodilation Pressure reactivity index (PRx) Correlation coefficient of MAP & ICP Ranges between - 1 and +1



66 PRx Positive values cerebral autoregulation lost A raised MAP results in increased ICP Negative values cerebral autoregulation intact Reflects a finding of the MAP and ICP varying in opposite directions Aim Find a CPP at which the brain is autoregulating
67 What do you need? Continuous ICP and MAP monitoring ICM+ software Integrates fluctuations of MAP & ICP Generates a continuous correlation coefficient (PRx)

68

69

70

71

72

73

74




75 Transcranial Ultrasound (TCD)


76 Transcranial Ultrasound Non invasive method to measure CBF velocity Continuous or intermittent Most described for vasospasm post SAH Vasospasm: Increased flow velocity (Poiseulle) Ratio of ICA :MCA allows monitoring independent of ICP rise Surg Neurol 2006; 65: BJA 2005; 94:

77 EEG Diagnosis of Seizure Intermittent versus Continuous Subclinical Seizure Limited versus Multichannel

78 Seizure and underlying pathology Condition Seizures % Status % Nonneurologic ICU Ischemic stroke SAH ICH HIE TBI Crit Care Med. 2013;41:1

79 Crit Care Med. 2013;41:1


80 Clinical utility in TBI Seizures result in increased CMRO 2 CMRO 2 = CBF = ICP Without ceeg, the cause of increased ICP is missed Consequence Ineffective therapeutic strategies utilized for ICP control Osmotherapy, temperature control, decompression etc





81 Cerebral Microdialysis So far Global view only Not exactly sure about areas at greatest risk Concept of local monitoring Described in 1960 s available since the 1990 s Hollow fibers miniaturization


82 Cerebral Microdialysis Semipermeable membrane Perfuse with RL Molecular transfer relative to concentrations Regular sampling or continuous online analysis




83 Cerebral Microdialysis Allows local molecular concentration analysis In theory any dialysate molecule Neuro: Lactate Glutamate Lactate/Pyruvate ratio Neurotransmitters Glucose Glycerol Problems Equilibrium incomplete Calibration of assay needed Placement? Clinical

 Subdural Superior to Epidural Drift up to 2 mmhg a day Cannot be")
84 Camino Transmit light via fiber optic cable towards displaceable mirror Change in ICP move mirror and difference in intensity reflected in ICP value Most commonly placed intraparenchymal Epidural poor accuracy (overestimate mean of 9 mmhg up to 30 mmhg) Subdural Superior to Epidural Drift up to 2 mmhg a day Cannot be recalibrated

85 Summary Cerebral Monitoring Essential as Clinical Information may be limited ICP Monitoring probably useful may not be as helpful in isolation Diagnosis Treatment Monitoring of Response Others are adjuvant but maybe of significant value
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Blood Brain Barrier (BBB)
") Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Current bedside monitors of brain blood flow and oxygen delivery
 24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS. Martha Richter, MSN, CRNA
 NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
ICP (Intracranial Pressure) Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry
 Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry") ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Positron Emission Tomography Imaging in Brain Injured Patients
 Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
TCD IN THE NICU, PICU AND OTHER APPLICATIONS. Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C.
 TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY. Dr Nick Taylor MBBS FACEM
 PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Cosa chiedo alla PtO 2
 Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury
 Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Functional cerebral monitoring in patients with critically illness
 Functional cerebral monitoring in patients with critically illness Anne-Marie Guerguerian MD PhD Assistant Professor of Critical Care Medicine & Pediatrics Scientist in Neurosciences & Mental Health, Research
Functional cerebral monitoring in patients with critically illness Anne-Marie Guerguerian MD PhD Assistant Professor of Critical Care Medicine & Pediatrics Scientist in Neurosciences & Mental Health, Research
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
Precision Medicine in Neurocritical Care: Should we individualize care?
 Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
INTRACRANIAL PRESSURE MONITORING
 INTRACRANIAL PRESSURE MONITORING A Handbook for the Nursing Professional 2 Why do we care about measuring intracranial pressure (ICP)? The intracranial compartment is very different from other regions
INTRACRANIAL PRESSURE MONITORING A Handbook for the Nursing Professional 2 Why do we care about measuring intracranial pressure (ICP)? The intracranial compartment is very different from other regions
DISCLOSURES. Specific TCD clinical applications for patients with traumatic brain injury 1/10/2015. FTE, Private Practice for profit TBI TBI: SCOPE
 DISCLOSURES Specific TCD clinical applications for patients with traumatic brain injury FTE, Private Practice for profit Alexander Razumovsky, PhD, FAHA 38 35 th Annual Meeting 38 35 th Annual Meeting
DISCLOSURES Specific TCD clinical applications for patients with traumatic brain injury FTE, Private Practice for profit Alexander Razumovsky, PhD, FAHA 38 35 th Annual Meeting 38 35 th Annual Meeting
Increased Intracranial Pressure 2.0 Contact Hours Presented by: CEU Professor
 Increased Intracranial Pressure 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of
Increased Intracranial Pressure 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
ESCMID Online Lecture Library. by author
 Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Cerebral autoregulation is a complex intrinsic control. Time course for autoregulation recovery following severe traumatic brain injury
 J Neurosurg 111:695 700, 2009 Time course for autoregulation recovery following severe traumatic brain injury Clinical article Gi l l E. Sv i r i, M.D., M.Sc., 1 Ru n e Aa s l i d, Ph.D., 2 Co l l e e
J Neurosurg 111:695 700, 2009 Time course for autoregulation recovery following severe traumatic brain injury Clinical article Gi l l E. Sv i r i, M.D., M.Sc., 1 Ru n e Aa s l i d, Ph.D., 2 Co l l e e
9/16/2018. Recognizing & Managing Seizures in Pediatric TBI. Objectives. Definitions and Epidemiology
 Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS
 GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
Continuous cerebral autoregulation monitoring
 Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Multimodal monitoring to individualize care in TBI
 Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Neurosurgery Review. Mudit Sharma, MD May 16 th, 2008
 Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Management of head injury in the intensive-care unit
 Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Trauma is the leading cause of death in the first four decades of life, with head injury being
 Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Bedside microdialysis for early detection of cerebral hypoxia in traumatic brain injury
 Neurosurg Focus 9 (5):E2, 2000 Bedside microdialysis for early detection of cerebral hypoxia in traumatic brain injury ASITA S. SARRAFZADEH, M.D., OLIVER W. SAKOWITZ, M.D., TIM A. CALLSEN, M.D., WOLFGANG
Neurosurg Focus 9 (5):E2, 2000 Bedside microdialysis for early detection of cerebral hypoxia in traumatic brain injury ASITA S. SARRAFZADEH, M.D., OLIVER W. SAKOWITZ, M.D., TIM A. CALLSEN, M.D., WOLFGANG
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
Neurotrauma. Béla Faludi Dept.. of Neurology University of PécsP
 Neurotrauma Béla Faludi Dept.. of Neurology University of PécsP Emergency!!! Why here? Opened cranial injury visible: neurosurgery Closed injuries sometimes diagnosed by neurologist Masking situation:
Neurotrauma Béla Faludi Dept.. of Neurology University of PécsP Emergency!!! Why here? Opened cranial injury visible: neurosurgery Closed injuries sometimes diagnosed by neurologist Masking situation:
EEG in the ICU: Part I
 EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia
 Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED
 ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
Continuous monitoring of jugular venous oxygen saturation in head-injured patients
 J Neurosurg 76:212-217, 1992 Continuous monitoring of jugular venous oxygen saturation in head-injured patients MICHAEL SHEINBERG, B.S., MALCOLM,J. KANTER~ M.D., CLAUDIA S. ROBERTSON, M.D., CHARLES F.
J Neurosurg 76:212-217, 1992 Continuous monitoring of jugular venous oxygen saturation in head-injured patients MICHAEL SHEINBERG, B.S., MALCOLM,J. KANTER~ M.D., CLAUDIA S. ROBERTSON, M.D., CHARLES F.