Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey
|
|
|
- Edith Heath
- 5 years ago
- Views:
Transcription
1 Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey

2 Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections Salivary glands* will not be covered specifically here use basic principles Neck dissections
3 Introduction Most complex head and neck specimens are for primary neoplasia of oropharynx, larynx, jaws and salivary glands Most commonly smoking and alcoholrelated SCC Other main group is HPV related SCC tonsil / tongue base (maybe other sites!) Other primary and secondary malignancy
4 Correlate correlate correlate! Diagnosis should be established by preoperative biopsy (always check before starting, may only have cytology) Correlate with radiology if possible (what structures may be involved - target your dissection) Correlate with surgeon - which margin / margins are they most worried about? IF IT DOESNT MAKE SENSE DONT START! Photographs - correlate with micro (eg. does the cancer extend beyond macro impression) Macro margins - correlate with micro
5 Identify the anatomy and orient components
6
7
8 What blocks are needed to complete the staging and minimum dataset?




9 What blocks are needed to complete the staging and minimum dataset? tumour Bone Skin with ulcer bone SMG LN

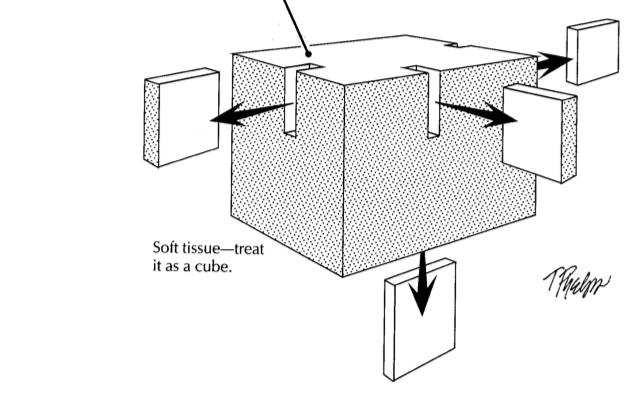
10 If you use clock-face orientation remember to convert back to anatomical margins in your report *establish a memorable colour scheme
.")


11 Lip cancers Vermillion border (sun damage). Need to assess... *Size of lesion *Depth of invasion *Peripheral and deep margins mucocutaneous junction mucosa skin

12 Measure the tumour macroscopically (unless larger microscopically) Depth of invasion of >5mm upstages from T1 to T2 in TNM8 and >10mm from T2 to T3

 Remember fixation can shrink")
13 Measure margins microscopically Try to avoid approximating margins (eg. >2mm as what constitutes a clear margin is highly subjective) Remember fixation can shrink and fold mucosa at the edges
 grading (well,")


14 Cohesive vs non-cohesive growth pattern Text Text Text Text Text Conventional (Broder) grading (well, moderate, poorly differentiated) correlates poorly with patient outcome in head and neck cancer. Cohesive vs non-cohesive growth pattern is the best predictor of overall survival (even when assessed in small biopsies)
 * Basaloid or darker staining with comedo necrosis, scanty cytoplasm, infiltrating lymphocytes, no")
15 HPV-related non-k SCC Compared with typical keratinising SCC these are... * Usually tonsil or tongue base primary (primary often occult or tiny with cystic neck mass) * Basaloid or darker staining with comedo necrosis, scanty cytoplasm, infiltrating lymphocytes, no keratin pearls or whorls (can have focal keratinisation) * Resemble reticulated epithelium of tonsillar crypt (therefore better described as well differentiated!) * younger patients higher socioeconomic not smokers or drinkers * better response to treatment and more than 50% survival benefit (smoking adversely affects this prognostic benefit)


16 p16 HPV-ISH Clinical rationale for testing to predict outcome, reassure patient and identify eligibility for trials Useful for pathologists to confirm diagnosis in poorly differentiated and identify likely primary site in metastatic lymph node with occult primary
 Smokers disease Often deeply invasive below a small ulcer Have a low")

17 Tongue Cancer Most commonly lateral borders of anterior 2/3 tongue (oral tongue. compare with HPV disease) Smokers disease Often deeply invasive below a small ulcer Have a low threshold for embedding whole specimen *Size of lesion (T1 <2cm, T2 2-4cm, T3 >4cm) *Depth of invasion *Peripheral and deep margins * T4 disease usually needs radiology correlation or when bone or extrinsic muscles included in resection
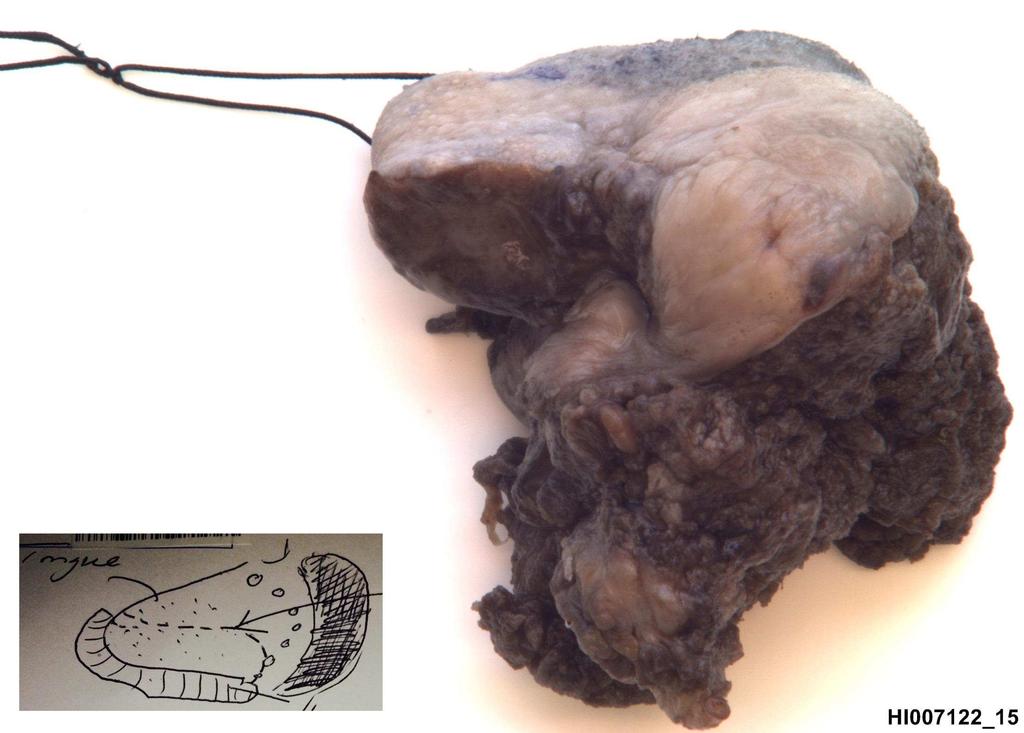
18
 Decalcify with 10% formic acid (about 10 days optimal) Take blocks to correlate macro and micro size, depth of invasion and")
19 Maxilla Correlate with radiology Ink and trim mucosal margins (Don t confuse sinuses for surgical margins!) Decalcify with 10% formic acid (about 10 days optimal) Take blocks to correlate macro and micro size, depth of invasion and assess for bone invasion


20 Mandible
21 lingual buccal lingual buccal Text Confirming bone invasion and margin status is most important. SCC on gingiva is often associated with dysplasia
22
23 Text measure size of tumour, location of centre of tumour to crest of vocal cord and extent of supraglottic/subglottic extension
24 Base of tongue / vallecular margin usually critically important Trim mucosal margins and decal in 10% formic acid, or bone saw and decalcify in the blocks

25 Megablocks are great for demonstrating tumour and correlating pathology with cross-sectional imaging

26 Megablock at level of vocal cord showing SCC invading right arytenoid cartilage and superficial SCC crossing midline at the anterior commisure
27 Saggital sections can be useful to show relationship of tumour to vocal cord and demonstrate subglottic extension, ideally combined with at least one megablock

28 Larynx or pharynx tumour?

29

30 Larynx Arytenoid cartilage Cricoid cartilage Hypopharynx Oesophagus

31 Carcinoma in situ bordering the ulcer in the hypopharynx. Tumour extends into larynx under the mucosa. Therefore this was a hypopharyngeal SCC invading the larynx not vice versa (Radiology and ENT surgeon took a lot of
32 Neck Dissections
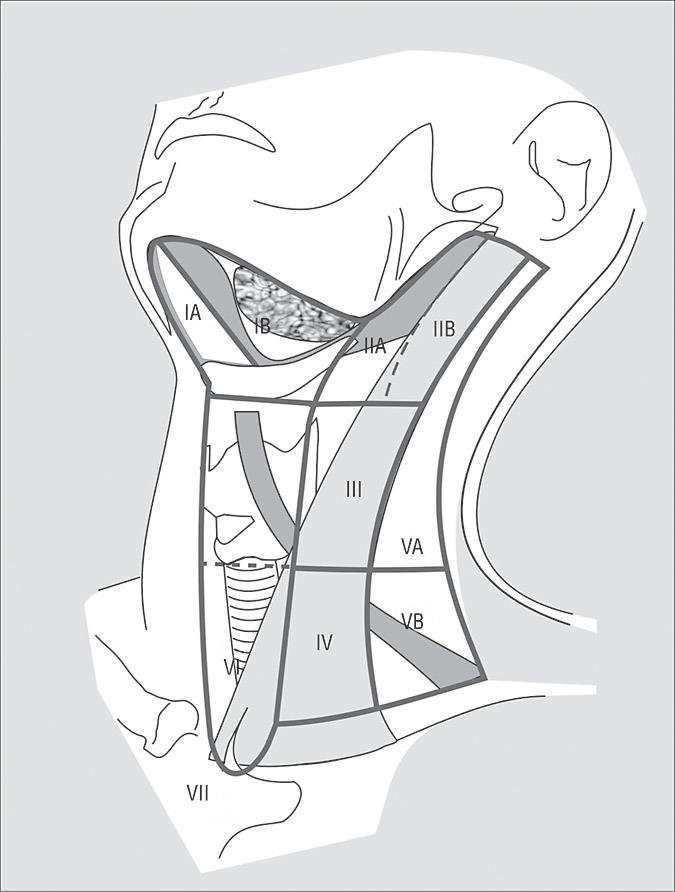
33 Most commonly levels I-IV In separate pots or pinned to a sponge or cork board with levels labelled (if you re very lucky!) If not labelled, levels I-IV can be approximated by location of submandibular gland and sternomastoid muscle
34 Which side of the neck?
35 Cervical Lymph Nodes - anatomical levels and nodal characteristics Level Usual number Shape/Size of nodes Sites drained I 6-10 Spherical <18mm Lower lip, FOM, oral tongue II Bean-shaped, flat or round <25mm Submental, submandibular, occipital, parotid, oropharynx and larynx III 5-10 Long, slender, flat <20mm Upper jugular nodes, oropharynx, mid-portion of oral tongue IV 5-10 V Bean-shaped, and Upper and middle jugular spherical <25mm nodes, tip of tongue, anterior FOM, hypopharynx, thyroid, cervical oesophagus and larynx Flat, round and Occipital and posterior bean-shaped, auricular nodes. Nasopharynx, <15mm skin of scalp and neck VI Small, ovoid, <10mm Thyroid gland, glottic and subglottic larynx, apex of piriform fossa, cervical oesophagus
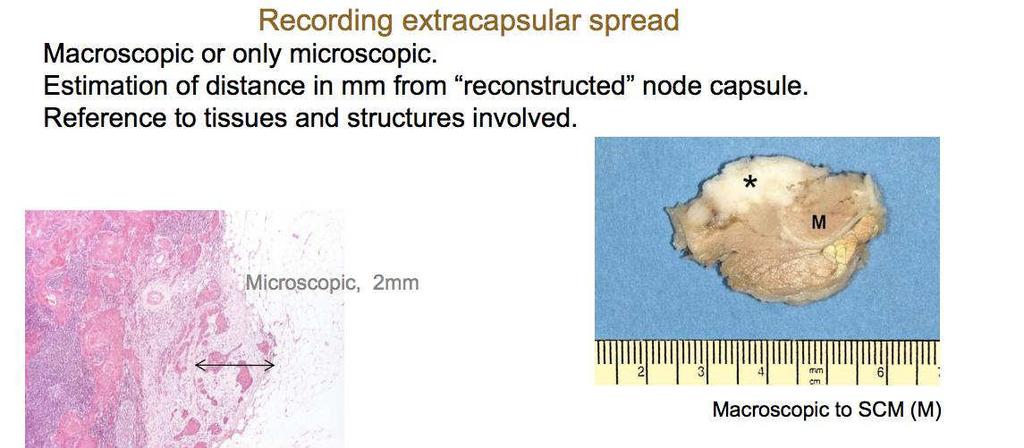
36 Reporting neck dissections Place multiple small nodes whole in a single cassette Sections of larger nodes (try to predict involvement in your macro and estimate number of nodes per cassette) Identify the largest node in each level and whether it shows extracapsular spread. *Large nodal mets only need the extracapsular areas sampled for histology Look for invasion of fat or muscle fibres - if equivocal, RCPath recommends stating as present, as there should be a low threshold for adjuvant therapy in these cases Combine data with any previous excisions (eg. tongue or tonsil tumour) to complete the TNM stage eg. pt2 (25mm tonsil HPV +ve SCC) N2b (3 of 22 lymph nodes, largest met 32mm in LII with ECS) No clear guidance yet about how to report sterile nodes post

37
38 Basic principles of cutup apply to head and neck Summary specimens Review anatomy and radiology and be prepared to focus your sampling towards staging parameters and important margins SCC is better assessed by examining growth pattern (cohesive and non-cohesive) than conventional grading (particularly in HPV related disease). Neck nodes are often bigger than the (sometimes occult) primary tonsil/tongue base tumour Mucosal margins can be sampled before bone decalcification Exact margins (eg. not >2mm) should be stated to allow pathology reports to survive changes in staging definitions

39

40 I am extremely grateful to Gary Doel who raised fund s for the Exakt pathology saw consequently reduced t urnaround times and accuracy of Plymouth head and neck cancer rep orting

41 References and Acknowledgments Please do not reproduce images without permission d.pdf RCPath minimum datasets Dr Miranda Pring UBHT / Bristol University Dr Julia Woolgar - Consultant Histopathologist (University of Liverpool) USA Professors Justin Bishop (UT Southwestern) William Westra (Johns Hopkins) and for remote
Head and Neck Pathology. Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital)
") Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
2. Guidelines for Reporting Head and Neck Tumours
 39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Physician to Physician AJCC 8 th Edition. Head and Neck. Summary of Changes. AJCC Cancer Staging Manual, 7 th Ed. Head and Neck Chapters
 Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
CERVICAL LYMPH NODES
 CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]](/thumbs/82/86783199.jpg "Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]") CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
Head and Neck Case 1 PATIENT HISTORY
 Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
NAACCR Webinar Series
 NAACCR 2009-2010 Webinar Series Collecting Cancer Data: Lip & Oral Cavity 8/5/2010 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes! NAACCR 2009/2010
NAACCR 2009-2010 Webinar Series Collecting Cancer Data: Lip & Oral Cavity 8/5/2010 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes! NAACCR 2009/2010
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Q&A. Fabulous Prizes. Collecting Cancer Data: Pharynx 12/6/12. NAACCR Webinar Series Collecting Cancer Data Pharynx
 Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Lecture 07. Lymphatic's of Head & Neck. By: Dr Farooq Amanullah Khan PMC
 Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
L ARYNX S TAGING F ORM
 CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
Head and Neck Tumours
 Head and Neck Tumours Introductory Notes The following sites are included: Lip, oral cavity Pharynx: oropharynx, nasopharynx, hypopharynx Larynx: supraglottis, glottis, subglottis Nasal cavity and paranasal
Head and Neck Tumours Introductory Notes The following sites are included: Lip, oral cavity Pharynx: oropharynx, nasopharynx, hypopharynx Larynx: supraglottis, glottis, subglottis Nasal cavity and paranasal
Head & Neck Contouring
 Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
(formalin fixed) 6 non-neoplastic spots (6 spots) Corresponding normal tissues with cancers: Yes Diameter: 1. 0 mm
 6 non-neoplastic spots (6 spots) Corresponding normal tissues with cancers: Yes Diameter: 1. 0 mm") CBA729-Test slide, Head and neck cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 6 Tissue type: Test slide, Head and neck cancer tissues No. of spots: 6 spots from each
CBA729-Test slide, Head and neck cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 6 Tissue type: Test slide, Head and neck cancer tissues No. of spots: 6 spots from each
10. HPV-Mediated (p16+) Oropharyngeal Cancer
 Oropharyngeal Cancer") 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
A220: Larynx cancer tissues. (formalin fixed)
") A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
Human Papillomavirus Testing in Head and Neck Carcinomas
 Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Head & Neck Case # 1
 DISCHARGE SUMMARY Head & Neck Case # 1 Date of Admission: 10/30/2010 Date of Discharge: 11/02/2010 Present Medical History: The patient is a 33-year-old lady with a history of right superior alveolar ridge
DISCHARGE SUMMARY Head & Neck Case # 1 Date of Admission: 10/30/2010 Date of Discharge: 11/02/2010 Present Medical History: The patient is a 33-year-old lady with a history of right superior alveolar ridge
Head & Neck Staging. Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging
 AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging. Head & Neck Staging. Learning Objectives. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide
 The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
LYMPHATIC DRAINAGE IN THE HEAD & NECK
 LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
Neck-2. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
ANATOMICAL PATHOLOGY TARIFF
 ANATOMICAL PATHOLOGY TARIFF A GUIDE TO UTILISATION. The following guidelines have been agreed by consensus of Anatomical Pathologists who are members of the Anatomical Pathologist s Group, or the National
ANATOMICAL PATHOLOGY TARIFF A GUIDE TO UTILISATION. The following guidelines have been agreed by consensus of Anatomical Pathologists who are members of the Anatomical Pathologist s Group, or the National
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
A Pathologist s Guide to Neck Dissection. Neck Dissections. Lymphatics of head and neck. Neck Dissections
 A Pathologist s Guide to Neck Dissection North American Society for Head and Neck Pathology Companion Meeting 2006 Sigrid Wayne, M.D. Department of Pathology University of Iowa The presence of cervical
A Pathologist s Guide to Neck Dissection North American Society for Head and Neck Pathology Companion Meeting 2006 Sigrid Wayne, M.D. Department of Pathology University of Iowa The presence of cervical
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
NAACCR Webinar Series 1
 Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Cervical Lymph Nodes
 Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
6 th Reprint Handbook Pages AJCC 7 th Edition
 6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
Volumi di trattamento del cavo orale
 SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
Salivary ultrasound. Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK
 Salivary ultrasound Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK Two main groups of patients with presenting symptoms of: Obstructive or chronic inflammatory symptoms (salivary
Salivary ultrasound Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK Two main groups of patients with presenting symptoms of: Obstructive or chronic inflammatory symptoms (salivary
Veins of the Face and the Neck
 Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Chapter 13: Mass in the Neck. Raymond P. Wood II:
 Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic space
 Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Dr Nick McIvor. Dr John Chaplin. Head & Neck Surgeon Auckland City Hospital Auckland. Auckland Head & Neck Surgeon Gillies Hospital Auckland
 Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
CLINICAL MEDICATION POLICY
 CLINICAL MEDICATION POLICY Policy Name: Opdivo (nivolumab) injection Policy Number: Approved By: Medical Management, Clinical Pharmacy Products: Highmark Health Options Application: All participating hospitals
CLINICAL MEDICATION POLICY Policy Name: Opdivo (nivolumab) injection Policy Number: Approved By: Medical Management, Clinical Pharmacy Products: Highmark Health Options Application: All participating hospitals
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
SITES (ALPHABETICAL) HPV CS SITE SPECIFIC FACTOR
 HPV CS SITE SPECIFIC FACTOR") SITES (ALPHABETICAL) HPV CS SITE SPECIFIC FACTOR Anus: Anal Canal; Anus, NOS; Other Parts of Rectum C21.0-C21.2, C21.8 C21.0 Anus, NOS (excludes skin of anus and perianal skin C44.5) C21.1 Anal canal C21.2
SITES (ALPHABETICAL) HPV CS SITE SPECIFIC FACTOR Anus: Anal Canal; Anus, NOS; Other Parts of Rectum C21.0-C21.2, C21.8 C21.0 Anus, NOS (excludes skin of anus and perianal skin C44.5) C21.1 Anal canal C21.2
Neck Dissection. Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)
, BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)") Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
Vincent Grégoire, Radiation Oncologist, Brussels, Belgium Cai Grau, Radiation Oncologist, Aarhus, Denmark. Tunis March 2017
 Guidelines for the delineation of the primary tumour Clinical Target Volumes (CTV) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity SCC (version 5.1) Vincent Grégoire, Radiation Oncologist,
Guidelines for the delineation of the primary tumour Clinical Target Volumes (CTV) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity SCC (version 5.1) Vincent Grégoire, Radiation Oncologist,
The Neck the lower margin of the mandible above the suprasternal notch and the upper border of the clavicle
 The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
INTRA/EXTRA ORAL EXAMINATION
 INTRA/EXTRA ORAL EXAMINATION www.dentalelle.com Dentalelle Tutoring Intraoral/Extraoral Examination 1. If you notice a typical finding after reviewing the head and neck on a new patient, what does this
INTRA/EXTRA ORAL EXAMINATION www.dentalelle.com Dentalelle Tutoring Intraoral/Extraoral Examination 1. If you notice a typical finding after reviewing the head and neck on a new patient, what does this
Nasal Cavity CS Tumor Size (Revised: 02/03/2010)
") Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Collaborative Staging Manual and Coding Instructions Part II: Primary Site Schema
 C44.0-C44.9, C51.0-C51.2, C51.8-C51.9, C60.0-C60.2, C60.8-C60.9, C63.2 (M-8720-8790) C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of ear and unspecified parts of face C44.4 Skin of
C44.0-C44.9, C51.0-C51.2, C51.8-C51.9, C60.0-C60.2, C60.8-C60.9, C63.2 (M-8720-8790) C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of ear and unspecified parts of face C44.4 Skin of
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY
 PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]](/thumbs/71/65936251.jpg "Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]") MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
AJCC update Disclosures. AJCC TNM staging system. Objectives:
 Disclosures AJCC update 2018 Remy Lobo, MD remylobo@med.umich.edu remy.lobo@hsc.utah.edu No relevant disclosures Information is based on the 8 th AJCC manual Amin MB, Edge SB, Greene FL et al, eds. AJCC
Disclosures AJCC update 2018 Remy Lobo, MD remylobo@med.umich.edu remy.lobo@hsc.utah.edu No relevant disclosures Information is based on the 8 th AJCC manual Amin MB, Edge SB, Greene FL et al, eds. AJCC
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
HPV and Head and Neck Cancer: What it means for you and your patients
 HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient
 Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma
 Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx
 Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Merkel Cell Carcinoma Case # 2
 DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Update of the role of Human Papillomavirus in Head and Neck Cancer
 Update of the role of Human Papillomavirus in Head and Neck Cancer 2013 International & 12 th National Head and Neck Tumour Conference Shanghai, 11 13 Oct 2013 Prof. Paul KS Chan Department of Microbiology
Update of the role of Human Papillomavirus in Head and Neck Cancer 2013 International & 12 th National Head and Neck Tumour Conference Shanghai, 11 13 Oct 2013 Prof. Paul KS Chan Department of Microbiology
The PHARYNX. Dr. Nabil Khouri MD Ph.D
 The PHARYNX Dr. Nabil Khouri MD Ph.D PHARYNX Fibromuscular tube lined with mucous membrane extends from base of skull to lower border of cricoid cartilage (C-6). 12-14 cm long At the lower border of cricoid
The PHARYNX Dr. Nabil Khouri MD Ph.D PHARYNX Fibromuscular tube lined with mucous membrane extends from base of skull to lower border of cricoid cartilage (C-6). 12-14 cm long At the lower border of cricoid
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Head and Neck Cancer Service
 Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Penile cancer teams in UK. Common variants. Penile cancer teams. Basaloid squamous carcinoma. The Pathology of Penile Tumours
 The Pathology of Penile Tumours Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Penile cancer teams in UK 12 centres for penile cancer work (10 in England and Wales, 2 in Scotland)
The Pathology of Penile Tumours Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Penile cancer teams in UK 12 centres for penile cancer work (10 in England and Wales, 2 in Scotland)
Management of metastatic squamous cell carcinoma cervical lymphadenopathy with occult primary The role of surgery
 Management of metastatic squamous cell carcinoma cervical lymphadenopathy with occult primary The role of surgery Dr Gary Fetter General surgeon Waterfall City Hospital Midrand Excalibur II Garable Lector
Management of metastatic squamous cell carcinoma cervical lymphadenopathy with occult primary The role of surgery Dr Gary Fetter General surgeon Waterfall City Hospital Midrand Excalibur II Garable Lector