dr. Judit Tőke DISEASES OF THE PARATHYROID GLAND METABOLIC BONE DISEASES OSTEOPOROSIS SEMMELWEIS UNIVERSITY 2nd Department of Medicine
|
|
|
- Janel Webster
- 6 years ago
- Views:
Transcription



1 DISEASES OF THE PARATHYROID GLAND METABOLIC BONE DISEASES OSTEOPOROSIS dr. Judit Tőke SEMMELWEIS UNIVERSITY 2nd Department of Medicine
2 Diseases of the parathyroid gland Outline Primary hyperparathyroidism Primary hypoparathyroidism Metabolic bone diseases Disorders in Vitamin D action (rickets and osteomalatia) Secondary hyperparathyroidism in chronic kidney disease Osteogenesis imperfecta Paget s Disease of Bone Osteoporosis

.")
3 The last anatomical discovery... Sandström IV: On a new gland in man and several mammals glandulae parathyroideae. Upsala Läk Förenings Förh ;15: Swedish Ivar Sandström, That remarkable discovery was made in 1877 at the Anatomical Department in Uppsala. At that time Sandström was a young medical student, who had worked as an assistant at the department since Virchow declined its publication in his journal, because of the length of the paper (30 pages)... Johansson H: The Uppsala anatomist Ivar Sandström and the parathyroid gland. Ups J Med Sci May; 120(2): 72 77
 - double adenoma (1-2%) - hyperplasia (10-15%) - carcinoma (<1%) - cyst")
4 Primary hyperparathyroidism (PHPT) Prevalence of PHPT: - North-America: 1/ North-Europe: 3-4/ in the population oldre than 75 years: 20/ women:men=2-3:1 Pathology of parathyroid glands causing PHPT: - single adenoma (80-85%) - double adenoma (1-2%) - hyperplasia (10-15%) - carcinoma (<1%) - cyst (1-3%)
5 Symptoms of PHPT Skeleton: Joints: Muscles: Renal: Gastrointestinal: Psychiatric: - bone pain - fractures - decrease of BMD: osteopenia/osteoporosis - osteitis fibrosa cystica - arthralgy - weakness of proximal muscles - muscle atrophy - renal stones - nephrocalcinosis - nephrogene diabetes insipidus - renal insufficiency - peptic ulcer - acute pancreatitis - depression Rare: Hypercalcemic crisis!! Causes: - parathyroid npl. hemorrhage/necrosis - infection - exsiccosis
6 Changes in clinical picture of PHPT Author Cope Heath Mallette Silverberg (%) (%) (%) (%) Renal stones Skeletal symptoms Hypercalciuria NA Asymptomatic John P. Bilezikian and Shonni J. Silverberg Reviews in Endocrine & Metabolic Disorders 2000;
7 Diagnosis of PHPT - Laboratorical investigations elevated or normal PTH concentration > 63 pg/ml AND hypercalcaemia: total serum calcium corrected to albumin > 2.63 mmol/l ionized serum calcium > 1.25 mmol/l N.B:in the absence of conditions mimicking PHPT (thiazide diuretics or lithium) Diagnosis of PHPT Radiological investigations CT, MRI: sensitivity:50-70% Ultrasound: sensitivity: 40-80% 99mTc-sestamibi substraction isotope: sensitivity for single adenoma: 90% for the diagnosis of ectopic parathyroid tissue

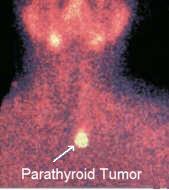

8 99m Tc-sestaMIBI scan (MIBI = methoxyisobutylisonitrile)


9 Indications for surgery for the treatment of PHPT Khan AA et al: Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos Int (1):1-19
10 Surgery for the treatment of symptomatic PHPT Parathyroidectomy (PTx) is the only curative approach to this disease. Cure rates following PTx ~ 95 % Post-PTX: reductions in the risk of all fractures decrease of renal stone risk IOPTH: intraoperative PTH - measurement with a rapid assay is of value in confirming adequate resection of abnormal parathyroid tissue and increases surgical success rates Persistent PHPT = development of hypercalcemia within 6 months of PTx If there is a contraindication for surgery: Vitamin D supplementation goal: serum 25OHD > 50nmol/l antiresorptive therapy (bisphosphonates) in patients with osteoporosis cinacalcet
11 Management of asymptomatic PHPT Monitoring appears to be a safe option for possibly up to 8 to 10 years for patients with asymptomatic PHPT Bilezikian et al. Guidelines for the Management of Asymptomatic Primary Hyperparathyroidism: Summary Statement from the Fourth International Workshop. J Clin Endocrinol Metab, 2014, Aug 27
12 Familial syndromes with PHPT More than one parathyroid gland are affected in 15% of all cases and half of them is a part of a familial syndrome (5-8% of all cases) Multiplex endocrine neoplasia type 1 -prevalence: 30-40/million MEN1-2% of all cases Multiplex endocrine neoplasia type 2A -prevalence: 40/million Hyperparathyreosis-jaw tumor syndrome Familial isolated primary hyperparathyroidism Familial hypocalciuric hypercalcemia MEN2A HPT-JT FIHP FHH
13 Primary hypoparathyroidism Iatrogen: neck irradiation, neck surgery (thyroid!!!) Infiltrativ / destructive diseases: haemochromatosis, sarcoidosis, Wilson-disease, amyloidosis Genetic disease: DiGeorge-syndrome APS-1 syndrome: - Hypoparathyroidism diabetes mellitus type 1 - Addison-disease autoimmune thyroid disease - Mucocutan candidiasis chronic active hepatitis alopecia vitiligo
14 Definition of hypocalcemia: Serum calcium < 2.23 mmol/l, Ionic calcium < 1.05 mmol/l Symptoms of hypocalcemia: It depends on: - the rate of the development - the severity of the hypocalcemia - and the elapsed time from the begining * neuromuscular : enhanced excitation in neurons paresthesia, tetania, laryngospasmus, bronchospasmus * neurol-psych : intracran. calcification (basal ggl, cortex), change in personality, parkinsonism, psychosis * skin : dry skin, atopic ekzema, caries * GI : dysphagia, abdominal pain, colica in bile ducts * pulmonary : dyspnoe, wheezing * cardiovascular : longer QT-interval, congestive heart failure, cardiomyopathy
15 Disorders in Vitamin D action Rickets: defects in mineralisation of bone and cartilage during childhood Osteomalatia: defects in mineralisation of bone in adulthood Serum levels 24h urinary calcium excretion Etiology Calcium Phosphorous ipth Bone specific ALP Hypocalcemic e.g. vitamin D deficiency Low to low normal Low Elevated Elevated Low Hypophosphatemic e.g. X-linked hypophosphatemia Normal Low Normal to low normal Elevated Low to elevated No abnormality in mineral homeostasis e.g. hypophosphatasia Normal Normal Normal Low Normal From: Disorders in Vitamin D Action Endotext [Internet]. De Groot LJ, Chrousos G, Dungan K, et al., editors. South Dartmouth (MA): MDText.com, Inc.;
16 Rickets Clinical features: weakness, bone pain, bone deformity, fracture 0-1 years: craniotabes, widening of the wrists, rachitic rosary, deformed rib cage > 2 years: bow legs (genu varum) or knock-knee (genu valgum), widening of the end of long bones
 biconcave vertebrae From: Disorders in Vitamin D Action Endotext [Internet]. De Groot LJ, Chrousos G, Dungan K, et al., editors. South Dartmouth (MA): MDText.")
17 Osteomalatia Clinical features: bone pain or low back pain, muscle weakness, hypotonia acute fracture of the long bones, pubic ramii, ribs, or spine Looser-zones (pseudofractures) biconcave vertebrae From: Disorders in Vitamin D Action Endotext [Internet]. De Groot LJ, Chrousos G, Dungan K, et al., editors. South Dartmouth (MA): MDText.com, Inc.;

18 Michael P.Whyte, Rajesh V.Thakker: Rickets and osteomalacia. Medicine 33 (12) p70-74, 2005

19 Secondary hyperparathyroidism in chronic kidney disease Clinical features: usually silent disease severe osteitis fibrosa clinical signs of hyperca, hyperp Treatment: Vitamin D: active vitamin D calcitriol! Calcimimetics Phosphate binders Oral phosphate restriction Kobama H: FGF23-parathyroid interaction: implications in chronic kidney disease. Kidney Int. 77(4):292-8, 2010
20 Osteogenesis imperfecta Clinically and genetically heterogeneous group of heritable disorders of connective tissue (collagen related disorder) 85%: AD mutations in the genes that encode type I collagen, COL1A1 and COL1A2 Clinical features: bone fragility, bone deformity, growth deficiency macrocephaly, blue sclerae, dentinogenesis imperfecta, hearing loss, neurological defects (macrocephaly and basilar invagination) cardiopulmonary complications Treatment: physical rehabilitation, supplemented with orthopedic intervention as needed oral bisphosphonates gene therapy?
21 Paget s Disease of Bone Clinical features: skeletal deformity which evolves over many years: skull and lower extremities. pathological fractures in the femurs. pain of skeletal, joint, neurologic or muscle origin. The radiologic features: 1. localized area of osteolysis which advances very slowly 2. the lesion becomes osteosclerotic 3. entire bone is affected the entire lesion is sclerotic with areas of osteolysis Treatment: iv. zoledronate surgery: lower extremity joint replacement correction of deformities of the lower extremity.

22 Osteoporosis Osteoporosis is a systemic, progressive disease. Decreased bone mass, altered microarchitecture --- fragile bones which are at an increased risk for fractures.

23 Diagnosis 1. Fracture risk assessment
24 Diagnosis 2. Finding secondary causes
25 Osteoporosis prevention 1. Physical activity 2. Optimal diet with mg calcium daily 3. Optimal vitamind with supplementation ( IU cholecalciferol daily), if needed 4. Discontinuation of smoking
26 I: Antiresorptive mediactaions Treatment Bisphosphonates: Alendronate oral; prevents vertebral, non-vertebral-, hip fractures in postmenopausal women Risedronate oral; prevents vertebral, non-vertebral-, hip fractures in postmenopausal women Ibandronate oral or iv. ; prevents vertebral fractures Zoledronate iv; prevents vertebral, non-vertebral-, hip fractures in postmenopausal women Caution: in high doses, increases the risk of osteonecrosis of jaw Raloxifene oral; prevents vertebral fractures in postmenopausal women Caution: may increases the risk of thromboembolic disease and stroke Denosumab sc; prevents vertebral, non-vertebral-, hip fractures in postmenopausal women Calcitonin intranasal spray; : Reduces incidence of vertebral fractures in post-menopausal women Consider as an alternative when other more effective drugs cannot be used Effective in decreasing acute pain associated with vertebral osteoporotic fractures Hormone replacement therapy mainly in those women who have symptoms of menopause Caution: increase the risk of breast carcnoma, thromboembolic disease, ischaemic heart disease (gestagen containing drugs!!) II. Bone-forming medication Teriparatide sc; prevents vertebral and non-vertebral fractures in postmenopausal women with severe OP
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
Primary Hyperparathyroidism
 Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Agents that Affect Bone & Mineral Homeostasis
 Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy
 "Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
UPDATES ON PRIMARY HYPERPARATHYROIDISM. Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY
 UPDATES ON PRIMARY HYPERPARATHYROIDISM Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY Disclosures Speaker (Honorarium): Shire Off-label use of estrogen, raloxifene
UPDATES ON PRIMARY HYPERPARATHYROIDISM Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY Disclosures Speaker (Honorarium): Shire Off-label use of estrogen, raloxifene
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Overview. Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases. People Centred Positive Compassion Excellence
 Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand
 International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Magnesium Homeostasis
 ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
Awaisheh. Mousa Al-Abbadi. Abdullah Alaraj. 1 Page
 f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hyperparathyroidism (primary): diagnosis, assessment and initial management
: diagnosis, assessment and initial management") National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
Osteoporosis Agents Drug Class Prior Authorization Protocol
 Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Practical Management Of Osteoporosis
 Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes.
 Academic lectures 3rd year of Medical faculty Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes. ENDOCRINOLOGY
Academic lectures 3rd year of Medical faculty Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes. ENDOCRINOLOGY
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Osteoporosis Clinical Guideline. Rheumatology January 2017
 Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Normal Bone Health and Bone Disease. Mr Ryan Trickett Consultant Hand and Wrist Surgeon 6 th February 2017
 Normal Bone Health and Bone Disease Mr Ryan Trickett Consultant Hand and Wrist Surgeon 6 th February 2017 Learning outcomes Understand the structure and function of bone and articular cartilage Explain
Normal Bone Health and Bone Disease Mr Ryan Trickett Consultant Hand and Wrist Surgeon 6 th February 2017 Learning outcomes Understand the structure and function of bone and articular cartilage Explain
Hypercalcemia may be detected incidentally. Practice CMAJ. Primary hyperparathyroidism. Primer. Key points. The case. What causes hypercalcemia?
 CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
Calcium and Parathyroid Disorders
 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Case study Group 2 presentation
 Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Hyper and hypocalcaemia. Prof Tricia Tan
 Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
Since the advent of multichannel serum chemistry
 ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
4/20/2015. The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy. Learning Objectives
 Testing During Surgical Parathyroidectomy. Learning Objectives") The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones
 Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Osteoporosis. When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of.
 Osteoporosis When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of. Osteoblasts by definition are those cells present in the bone and are involved
Osteoporosis When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of. Osteoblasts by definition are those cells present in the bone and are involved
Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012.
 Levels Shireen Fatemi, M.D. April, 2012.") Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012 Disclosures I have no financial relationships with commercial interests,
Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012 Disclosures I have no financial relationships with commercial interests,
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Parathyroid Imaging. A Guide to Parathyroid Surgery
 Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Osteoporosis. Treatment of a Silently Developing Disease
 Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus
 Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus The Harvard community has made this article openly available. Please
Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus The Harvard community has made this article openly available. Please
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
CALCIUM BALANCE. James T. McCarthy & Rajiv Kumar
 CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
DIAGNOSING X-LINKED HYPOPHOSPHATEMIA (XLH) BIOCHEMICAL TESTING CONSIDERATIONS
 BIOCHEMICAL TESTING CONSIDERATIONS") DIAGNOSING X-LINKED HYPOPHOSPHATEMIA (XLH) BIOCHEMICAL TESTING CONSIDERATIONS XLH IS CHARACTERIZED BY CHRONIC HYPOPHOSPHATEMIA XLH is a hereditary, progressive, lifelong disorder. In children and adults,
DIAGNOSING X-LINKED HYPOPHOSPHATEMIA (XLH) BIOCHEMICAL TESTING CONSIDERATIONS XLH IS CHARACTERIZED BY CHRONIC HYPOPHOSPHATEMIA XLH is a hereditary, progressive, lifelong disorder. In children and adults,
Diagnosis and Treatment of Primary Hyperparathyroidism. Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic
 Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
This house believes that HRT should be the first-line prevention for postmenopausal osteoporosis: the case against
 This house believes that HRT should be the first-line prevention for postmenopausal osteoporosis: the case against Juliet Compston Professor of Bone Medicine University of Cambridge School of Clinical
This house believes that HRT should be the first-line prevention for postmenopausal osteoporosis: the case against Juliet Compston Professor of Bone Medicine University of Cambridge School of Clinical
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary
 Prior Authorization with Quantity Limit Program Summary") Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Hypoparathyroidism By John Halpern, DO, FACEP Coauthored by N. Ewen Wang, MD
 Hypoparathyroidism By John Halpern, DO, FACEP Coauthored by N. Ewen Wang, MD Reprinted with permission from: E-Medicine: Instant Access to the Minds of Medicine http://www.emedicine.com/emerg/topic276.htm
Hypoparathyroidism By John Halpern, DO, FACEP Coauthored by N. Ewen Wang, MD Reprinted with permission from: E-Medicine: Instant Access to the Minds of Medicine http://www.emedicine.com/emerg/topic276.htm
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
PRIMARY HYPERPARATHYROIDISM WITH RICKETS. KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College
 PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Hypercalcemia. Brian Rose, M.D. Bozeman Health June 6, 2018
 Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Chapter 5: Evaluation and treatment of kidney transplant bone disease Kidney International (2009) 76 (Suppl 113), S100 S110; doi: /ki.2009.
 76 (Suppl 113), S100 S110; doi: /ki.2009.") http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
Cases in Endocrinology
 Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Pediatric metabolic bone diseases
 Pediatric metabolic bone diseases Classification and overview of clinical and radiological findings M. Mearadji International Foundation for Pediatric Imaging Aid www.ifpia.com Introduction Metabolic bone
Pediatric metabolic bone diseases Classification and overview of clinical and radiological findings M. Mearadji International Foundation for Pediatric Imaging Aid www.ifpia.com Introduction Metabolic bone
Summary of the risk management plan by product
 Summary of the risk management plan by product 1 Elements for summary tables in the EPAR 1.1 Summary table of Safety concerns Summary of safety concerns Important identified risks Important potential risks
Summary of the risk management plan by product 1 Elements for summary tables in the EPAR 1.1 Summary table of Safety concerns Summary of safety concerns Important identified risks Important potential risks
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
CKD-MBD CKD mineral bone disorder
 CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma
 ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor
 Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
Osteoporosis and Lupus. Andrew Ruthberg, MD University Rheumatologists
 Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Metabolic Bone Disease Related to Chronic Kidney Disease
 Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
BARTS ENDOCRINE E-PROTOCOLS CALCIUM DISORDERS AND BONE
 HYPERCALCAEMIA CALCIUM DISORDERS Clinical features to record Symptoms: Thirst, polyuria, nocturia, tiredness, poor concentration, depression, constipation, episodes of renal colic/calculi, hypertension,
HYPERCALCAEMIA CALCIUM DISORDERS Clinical features to record Symptoms: Thirst, polyuria, nocturia, tiredness, poor concentration, depression, constipation, episodes of renal colic/calculi, hypertension,
HYPERCALCAEMIA 101 FOR THE INTERNIST
 HYPERCALCAEMIA 101 FOR THE INTERNIST Dr Chionh Siok Bee Dept of Medicine, National University Hospital siok_bee_chionh@nuhs.edu.sg Medicine Review Course 18/09/2011 Outline of Talk Definition of hypercalcaemia
HYPERCALCAEMIA 101 FOR THE INTERNIST Dr Chionh Siok Bee Dept of Medicine, National University Hospital siok_bee_chionh@nuhs.edu.sg Medicine Review Course 18/09/2011 Outline of Talk Definition of hypercalcaemia
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary
 Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
International Journal of Biological & Medical Research. An Uncommon Case of Persistent Hypercalcaemia following Parathyroid Surgery
 Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
Bone Disorders in CKD
 Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
OSTEOPOROSIS AND WHAT TO DO AFTER A VERTEBRAL FRACTURE. Lydia Au Geriatrics Ng Teng Fong Hospital
 OSTEOPOROSIS AND WHAT TO DO AFTER A VERTEBRAL FRACTURE Lydia Au Geriatrics Ng Teng Fong Hospital LET S START WITH WHAT YOU WANT TO KNOW AND DO WITH A VERT FRACTURE Vertebral fractures Most common (550K
OSTEOPOROSIS AND WHAT TO DO AFTER A VERTEBRAL FRACTURE Lydia Au Geriatrics Ng Teng Fong Hospital LET S START WITH WHAT YOU WANT TO KNOW AND DO WITH A VERT FRACTURE Vertebral fractures Most common (550K
Primary hyperparathyroidism
 How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
The Skeletal Response to Aging: There s No Bones About It!
 The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Iperparatiroidismo normocalcemico: vero o falso?
 Iperparatiroidismo normocalcemico: vero o falso? Bari, 7-10 novembre 2013 TERAPIA E FOLLOW-UP A. Piovesan SCDU Endocrinologia Oncologica AO Città della Salute e della Scienza Molinette Torino THE THIRD
Iperparatiroidismo normocalcemico: vero o falso? Bari, 7-10 novembre 2013 TERAPIA E FOLLOW-UP A. Piovesan SCDU Endocrinologia Oncologica AO Città della Salute e della Scienza Molinette Torino THE THIRD
Bisphosphonates. Making intelligent drug choices
 Making intelligent drug choices Bisphosphonates are a first choice for treating osteoporosis, according to Kedrin E. Van Steenwyk, DO, an obstetrician/gynecologist at Sycamore Women s Center, Miamisburg,
Making intelligent drug choices Bisphosphonates are a first choice for treating osteoporosis, according to Kedrin E. Van Steenwyk, DO, an obstetrician/gynecologist at Sycamore Women s Center, Miamisburg,
When the level of calcium in the blood falls too low, the parathyroid glands secrete just enough PTH to restore the blood calcium level.
 Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Hypocalcemia 6/8/12. Normal value. Physiologic functions. Nephron a functional unit of kidney. Influencing factors in Calcium and Phosphate Balance
 Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Effective Health Care
 Number 12 Effective Health Care Comparative Effectiveness of Treatments To Prevent Fractures in Men and Women With Low Bone Density or Osteoporosis Executive Summary Background Osteoporosis is a systemic
Number 12 Effective Health Care Comparative Effectiveness of Treatments To Prevent Fractures in Men and Women With Low Bone Density or Osteoporosis Executive Summary Background Osteoporosis is a systemic
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Sachin Soni DNB Pediatrics
 Sachin Soni DNB Pediatrics Vitamin D physiology Introduction Etiology Clinical feature Radiology Diagnosis Lab Treatment Source: -Fish, liver and oil, - Human milk (30-40 IU/L) - Exposure to sun light
Sachin Soni DNB Pediatrics Vitamin D physiology Introduction Etiology Clinical feature Radiology Diagnosis Lab Treatment Source: -Fish, liver and oil, - Human milk (30-40 IU/L) - Exposure to sun light
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to
 Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland