HYPERCALCAEMIA 101 FOR THE INTERNIST
|
|
|
- Steven Carpenter
- 5 years ago
- Views:
Transcription
1 HYPERCALCAEMIA 101 FOR THE INTERNIST Dr Chionh Siok Bee Dept of Medicine, National University Hospital Medicine Review Course 18/09/2011
2 Outline of Talk Definition of hypercalcaemia Aetiology of hypercalcaemia Clinical manifestations of hypercalcaemia Diagnostic approach to hypercalcaemia Treatment of hypercalcaemia Case study to illustrate the approach to the investigation of hypercalcaemia No conflicts of interest to declare
3 Definition of Hypercalcaemia Corrected total serum Calcium above the normal range (NUH: mmol/l) Ionised Calcium above mmol/l Calcium is 45% bound to protein Correct for albumin level 10% bound to anions 45% free (ionised) Affected by ph
4 Aetiology of Hypercalcaemia Endocrine Disorders causing Hypercalcaemia With excess PTH - Hyperparathyroidism (HPT) Without excess PTH Malignancy-Associated Hypercalcaemia (MAH) With excess PTH-related peptide (PTHrP) With other systemic factors PHPT and MAH account for 90% of hypercalcaemia
5 Aetiology of Hypercalcaemia Inflammatory Disorders Chronic Granulomatous Disorders: activation of extra-renal 1-α hydroxylase 1,25(OH) 2 D = Calcitriol Non-infectious: Sarcoidosis, Wegener s, Berylliosis, Eosinophilic granulomatosis, silicone-induced and paraffin-induced granulomatosis, infantile fat necrosis Infectious: TB, histoplasmosis, candidiasis, leprosy, coccidiomycosis, cat-scratch disease AIDS HIV, CMV, HTLV-III
6 Aetiology of Hypercalcaemia Drug-related Thiazides Renal reabsorption of Ca Ur Ca Lithium Theophylline toxicity Teriparatide (rhpth1-34) Vitamin D and Vitamin D analogues e.g. Calcitriol Excessive Vitamin A and analogues: cis- or transretinoic acid Oestrogens and Antioestrogens Aluminium Intoxication Milk-Alkali Syndrome (> 3 G elemental Calcium/day) alkalosis, Ur Ca, nephrocalcinosis, renal failure Parenteral nutrition
7 Aetiology of Hypercalcaemia Hypercalcaemia of Unknown Aetiology Williams Syndrome elfin facies cardiac abnormalities, esp AS Idiopathic Infantile Hypercalcaemia Miscellaneous Causes Rhabdomyolysis ARF diuretic phase Immobilisation in Paget s Disease
8 Endocrine Causes of Hypercalcaemia Endocrine Disorders causing Hypercalcaemia With Excess PTH: Sporadic Primary Hyperparathyroidism % of PHPT is due to a single adenoma 10-15% due to polyglandular hyperplasia 1% due to parathyroid carcinoma Very rare: Autoimmune Hypocalciuric Hypercalcaemia due to Ab against the CaSR Familial Primary Hyperparathyroidism Tertiary Hyperparathyroidism

9 Endocrine Causes of Hypercalcaemia: Familial HPT CaSR gene MEN 1 gene HRPT2 gene RET Protooncogene From Endotext.com
10 Endocrine Causes of Hypercalcaemia Endocrine Disorders causing Hypercalcaemia Without Excess PTH Primary hyperthyroidism up to 20% of thyrotoxic patients bone turnover and resorption Adrenal insufficiency Phaeochromocytoma? PTH-rP Acromegaly Jansen's Metaphyseal Chondrodysplasia activating mutation of PTHR short-limbed dwarf
11 Malignancy-Associated Hypercalcaemia (MAH) Hypercalcaemia occurs in up to 10% of cancers MAH with Excess Circulating PTHrP Absent or few skeletal mets Ca, PO4, Ur Ca not pure osteolysis 50-90% of solid tumours with hypercalcaemia Squamous cell ca, esp lung; renal cell, bladder and Ovarian ca 20-60% of haematological malignancies with hypercalcaemia NHL, CML, CLL, ATL, Myeloma
12 Malignancy-Associated Hypercalcaemia (MAH) MAH without Excess Circulating PTHrP Other Systemic Factors Calcitriol e.g. in NHL Cytokines such as IL-6, RANKL Ectopic PTH e.g. ovarian, lung, thyroid, thymic carcinoma Osteolytic mets Local PTH-rP Myeloma also produce cytokines, RANKL, DKK-1 hypercalcaemia exacerbated by renal failure
13 Clinical Manifestations of Hypercalcaemic Disorders Symptoms and signs of underlying disorder Symptoms and Signs of Hypercalcamia More symptoms if acute onset or severe with Total Ca > 3.0 mmol/l, as is seen with MAH Fewer symptoms if chronic and mild, as in most cases of PHPT T Ca usually < 2.75
14 Clinical Manifestations of Hypercalcaemia Gastrointestinal Renal Neuro-muscular Cardiac Acute Anorexia, nausea, vomiting Polyuria, polydipsia, ARF Depression, fatigue, confusion, stupor, coma Short QT, Bradycardia, first degree atrioventricular block Chronic Dyspepsia, constipation, pancreatitis, peptic ulcer Nephrolithiasis, nephrocalcinosis, Distal RTA, Nephrogenic DI, CRF Muscle weakness, bone pain, Osteoporosis/Osteopaenia Hypertension, digitalis sensitivity Adapted from Endotext.com
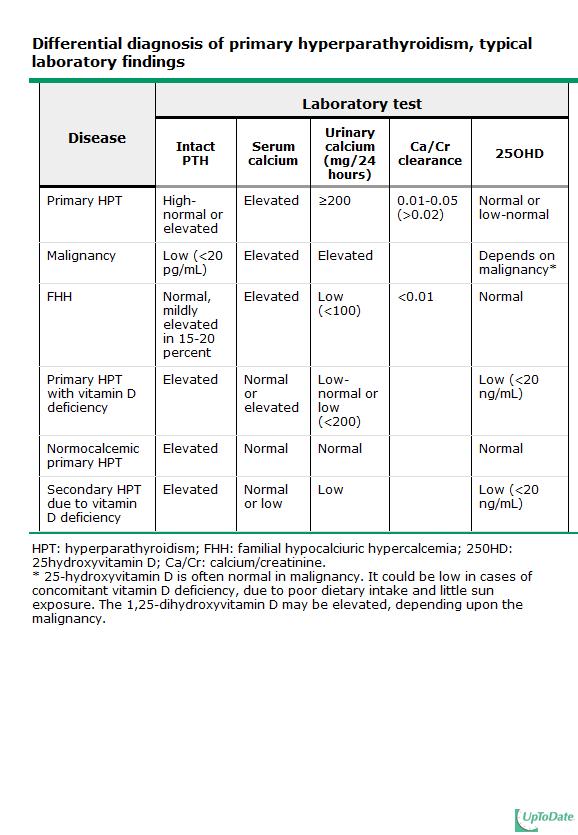
15 If severe: Repeat with PTH immediately -PTH must be paired with Ca and Sx, FHx, DHx, PE PTH if non-urgent: Fasting sample, in plain tube on ice FBC, ESR U/E/Cr PO4, ALP PTH<2 pmol/l $500 each not necessary if malignancy clinically obvious 25 (OH)D, TSH, Myeloma screen (UCa/ SCa) (Ucr x 100 / SCr) Adapted from UpToDate
16 US and Sestamibi scan
17
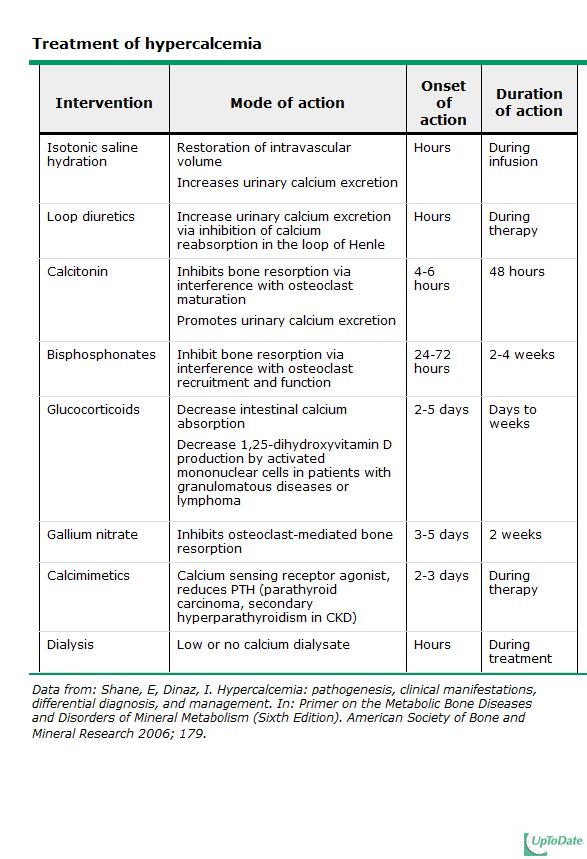
18 Treatment of Severe Hypercalcaemia (Total Ca > 3.5 mmol/l) Hydration IV N/S 3-4 L over hours ( ml/h then adjust for urinary output of ml/h) Inhibition of Bone Resorption SC/IM Calcitonin 4-8 units/kg 6-12 hrly Reduces T Ca by 0.5 mm; tachyphylaxis occurs after 48 h IV Bisphosphonate: caution if S Cr > 400 umol/l Zoledronic acid 4 mg over minutes Pamidronate mg over 4 hrs IV Plicamycin mg/kg over 4-6 hrs Toxic to kidney, liver and bone marrow
19 Treatment of Severe Hypercalcaemia Calciuresis when re-hydrated - with loop diuretic Frusemide mg especially if PTHrP if oedema occurs Glucocorticoid eg IV Hydrocortisone 100 mg 8 hourly for 3-5 days Haematological malignancies e.g. lymphoma and myeloma Vitamin D toxicity and granulomatous disease
20 Treatment of Severe Hypercalcaemia Gallium nitrate 200 mg/m 2 x 5/7 Dialysis if refractory hypercalcaemia or in renal or heart failure Haemodialysis or Peritoneal dialysis Mobilisation
21
22 Treatment of Mild Hypercalcaemia (Total Ca < 3 mmol/l, No Acute Sx) Avoid factors that aggravate hypercalcaemia e.g. drugs like thiazide diuretics, dehydration, high-calcium diet (elemental Ca >1000 mg/day), prolonged bed rest Adequate hydration with 8 glasses of H 2 O/ day
23 Treatment of Hypercalcaemia Treatment of underlying disorder Primary hyperparathyroidism parathyroidectomy unless very mild and asymptomatic Calcimimetic e.g. Cinacalcet for unresectable parathyroid carcinoma
24 Treatment of Mild Primary Hyperparathyroidism Guidelines for parathyroid surgery in asymptomatic primary hyperparathyroidism from the NIH Workshop of Measurement Surgery Recommended 2 T Ca >1.0 mg/dl (0.25 mmol/l) above normal CCT (calculated) Below 60ml/min /1.73 m2) T score < -2.5 SD at spine, hip (total or femoral BMD neck) or radius (distal 1/3 site) or presence of fragility fracture Age Age < 50 years 1 Surgery is also indicated in patients for whom medical surveillance is neither desired nor possible. 2 If any one of these criteria are met, the patient is considered to be a candidate for parathyroid surgery.
25 Summary Hypercalcaemia can be acute or chronic and can be mild, moderate or severe Diagnostic approach is primarily based on clinical features and presence or absence of excess PTH 90% of hypercalcaemia is due to Sporadic Primary Hyperparathyroidism or Malignancy Treatment of symptomatic hypercalcaemia of > 3.5 mmol/l is urgent
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Hypercalcemia. Brian Rose, M.D. Bozeman Health June 6, 2018
 Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Calcium and Parathyroid Disorders
 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Symptom management: Hypercalcemia
 Symptom management: Hypercalcemia Dr Claire Higham 10.11.16 NLCFN National Conference 2016 Consultant Endocrinologist The Christie Hospital Manchester, UK Hypercalcemia of malignancy 2-30% of patients
Symptom management: Hypercalcemia Dr Claire Higham 10.11.16 NLCFN National Conference 2016 Consultant Endocrinologist The Christie Hospital Manchester, UK Hypercalcemia of malignancy 2-30% of patients
Hyper and hypocalcaemia. Prof Tricia Tan
 Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
Clinical biochemistry of calcium and vitamin D
 Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
Management of hypercalcemia of malignancy
 Integrative Cancer Science and Therapeutics Research Article ISSN: 2056-4546 Management of hypercalcemia of malignancy Sonia Amin Thomas (Sonia Patel)* and Soo-Hwan Chung Philadelphia College of Osteopathic
Integrative Cancer Science and Therapeutics Research Article ISSN: 2056-4546 Management of hypercalcemia of malignancy Sonia Amin Thomas (Sonia Patel)* and Soo-Hwan Chung Philadelphia College of Osteopathic
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
LRI Children s Hospital
 Calcium Disorders in Children LRI Children s Hospital Staff relevant to: Medical & Nursing staff caring for Children identified with having a Calcium disorder Team approval date: January 2019 Version:
Calcium Disorders in Children LRI Children s Hospital Staff relevant to: Medical & Nursing staff caring for Children identified with having a Calcium disorder Team approval date: January 2019 Version:
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy
 "Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
Hypocalcemia 6/8/12. Normal value. Physiologic functions. Nephron a functional unit of kidney. Influencing factors in Calcium and Phosphate Balance
 Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
CALCIUM BALANCE. James T. McCarthy & Rajiv Kumar
 CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
Primary Hyperparathyroidism
 Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
What this study adds: - Sustained hypercalacemia affects 1 in 500 children in a general hospital setting
 FREQUENCY AND AETIOLOGY OF HYPERCALCAEMIA McNeilly JD 1, Boal R 2, Shaikh MG 2, Ahmed SF 2 1 Dept of Clinical Biochemistry, Queen Elizabeth University Hospital, Greater Glasgow & Clyde NHS Trust, Glasgow,
FREQUENCY AND AETIOLOGY OF HYPERCALCAEMIA McNeilly JD 1, Boal R 2, Shaikh MG 2, Ahmed SF 2 1 Dept of Clinical Biochemistry, Queen Elizabeth University Hospital, Greater Glasgow & Clyde NHS Trust, Glasgow,
BARTS ENDOCRINE E-PROTOCOLS CALCIUM DISORDERS AND BONE
 HYPERCALCAEMIA CALCIUM DISORDERS Clinical features to record Symptoms: Thirst, polyuria, nocturia, tiredness, poor concentration, depression, constipation, episodes of renal colic/calculi, hypertension,
HYPERCALCAEMIA CALCIUM DISORDERS Clinical features to record Symptoms: Thirst, polyuria, nocturia, tiredness, poor concentration, depression, constipation, episodes of renal colic/calculi, hypertension,
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Since the advent of multichannel serum chemistry
 ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
SUMMARY OF PRODUCT CHARACTERISTICS
 SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Colecalciferol Meda 800 IU tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 800 IU
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Colecalciferol Meda 800 IU tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 800 IU
Disclosure. Topic Outline. Calcium, Vitamin D, PTH Disorders. PTH/Calcium-Normal Physiology. I have nothing to disclose
 Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia
 BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director
 W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director It is our duty to each learner to honor your right to expect
W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director It is our duty to each learner to honor your right to expect
Dosage in renal impairment Kalcipos-D chewable tablets should not be used in patients with severe renal impairment.
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D 500 mg/400 IU chewable tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains: calcium 500 mg as
SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D 500 mg/400 IU chewable tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains: calcium 500 mg as
Hypercalcemia may be detected incidentally. Practice CMAJ. Primary hyperparathyroidism. Primer. Key points. The case. What causes hypercalcemia?
 CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
Current Management of Metastatic Bone Disease
 Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Summary of Product Characteristics
 1 NAME OF THE MEDICINAL PRODUCT Desunin 4000 IU Tablets Summary of Product Characteristics 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 4000 IU (equivalent
1 NAME OF THE MEDICINAL PRODUCT Desunin 4000 IU Tablets Summary of Product Characteristics 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 4000 IU (equivalent
Calcium metabolism and the Parathyroid Glands. Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands
 Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Importance of Calcium CALCIUM DISORDERS. Hypercalcaemia. Calcium homeostasis. Effects on total calcium
 CALCIUM DISORDERS Reto Neiger Klinik für Kleintiere (Innere Medizin) Justus-Liebig Universität Giessen Importance of Calcium Bone formation and resorption, Enzymatic reactions, Membrane transport and stability,
CALCIUM DISORDERS Reto Neiger Klinik für Kleintiere (Innere Medizin) Justus-Liebig Universität Giessen Importance of Calcium Bone formation and resorption, Enzymatic reactions, Membrane transport and stability,
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
Agents that Affect Bone & Mineral Homeostasis
 Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Hypercalcemia of malignancy. Apirom Laocharoenkeat
 Hypercalcemia of malignancy Apirom Laocharoenkeat ผ ป วยหญ งอาย 51ป เป นมะเร งเต านมชน ดแพร กระจาย CC : ม อาการ nausea /vomiting และ mental changes HPI:ได ร บ docetaxel cycle 4 เม อ 18 ว นก อน ญาต ผ ป
Hypercalcemia of malignancy Apirom Laocharoenkeat ผ ป วยหญ งอาย 51ป เป นมะเร งเต านมชน ดแพร กระจาย CC : ม อาการ nausea /vomiting และ mental changes HPI:ได ร บ docetaxel cycle 4 เม อ 18 ว นก อน ญาต ผ ป
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory OSTOCALCIUM TABLETS. Calcium and Phosphorus with Vitamin D3 Tablets
 For the use only of Registered Medical Practitioners or a Hospital or a Laboratory OSTOCALCIUM TABLETS Calcium and Phosphorus with Vitamin D3 Tablets QUALITATIVE AND QUANTITATIVE COMPOSITION Each uncoated
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory OSTOCALCIUM TABLETS Calcium and Phosphorus with Vitamin D3 Tablets QUALITATIVE AND QUANTITATIVE COMPOSITION Each uncoated
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
Thyroid and Parathyroid Surgery
 Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory OSTOCALCIUM FORTE TABLETS
 For the use only of Registered Medical Practitioners or a Hospital or a Laboratory OSTOCALCIUM FORTE TABLETS Calcium and Phosphorus with Vitamin D3 Tablets QUALITATIVE AND QUANTITATIVE COMPOSITION Each
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory OSTOCALCIUM FORTE TABLETS Calcium and Phosphorus with Vitamin D3 Tablets QUALITATIVE AND QUANTITATIVE COMPOSITION Each
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012.
 Levels Shireen Fatemi, M.D. April, 2012.") Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012 Disclosures I have no financial relationships with commercial interests,
Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012 Disclosures I have no financial relationships with commercial interests,
Skeletal. Parathyroid hormone-related protein Analyte Information
 Skeletal Parathyroid hormone-related protein Analyte Information 1 2012-04-04 Parathyroid hormone related protein (PTHrP) Introduction Parathyroid hormone-related protein (PTHrP) is actually a family of
Skeletal Parathyroid hormone-related protein Analyte Information 1 2012-04-04 Parathyroid hormone related protein (PTHrP) Introduction Parathyroid hormone-related protein (PTHrP) is actually a family of
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones
 Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Disodium pamidronate for treating severe hypercalcemia in a hemodialysis patient
 Disodium pamidronate for treating severe hypercalcemia in a hemodialysis patient Hernán Trimarchi, Fernando Lombi, Mariano Forrester, Cristina Elizondo, Deirdre Sawinski, Horacio Pereyra and Emilio Freixas
Disodium pamidronate for treating severe hypercalcemia in a hemodialysis patient Hernán Trimarchi, Fernando Lombi, Mariano Forrester, Cristina Elizondo, Deirdre Sawinski, Horacio Pereyra and Emilio Freixas
Hypercalcaemia with undetectable parathormone levels
 Case Review Hypercalcaemia with undetectable parathormone levels Ilaria Muller, clinical research fellow, 1,2 Lakdasa D Premawardhana, consultant physician 2,3 1 Thyroid Research Group, Division of Infection
Case Review Hypercalcaemia with undetectable parathormone levels Ilaria Muller, clinical research fellow, 1,2 Lakdasa D Premawardhana, consultant physician 2,3 1 Thyroid Research Group, Division of Infection
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Hospice Palliative Care Program Symptom Guidelines. Hypercalcemia in Malignant Disease (Palliative Management)
") Hospice Palliative Care Program Symptom Guidelines Hypercalcemia in Malignant Disease (Palliative Management) (Palliative Management) Rationale This guideline is adapted for inter-professional primary
Hospice Palliative Care Program Symptom Guidelines Hypercalcemia in Malignant Disease (Palliative Management) (Palliative Management) Rationale This guideline is adapted for inter-professional primary
GUIDELINE FOR THE MANAGEMENT AND PREVENTION OF ACUTE TUMOUR LYSIS SYNDROME IN HAEMATOLOGICAL MALIGNANCIES
 GUIDELINE FOR THE MANAGEMENT AND PREVENTION OF ACUTE TUMOUR LYSIS SYNDROME IN HAEMATOLOGICAL MALIGNANCIES Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target
GUIDELINE FOR THE MANAGEMENT AND PREVENTION OF ACUTE TUMOUR LYSIS SYNDROME IN HAEMATOLOGICAL MALIGNANCIES Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target
SUMMARY OF THE PRODUCT CHARACTERISTICS
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D mite 500 mg/200 IU film-coated tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains 500 mg
SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D mite 500 mg/200 IU film-coated tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains 500 mg
Oncological emergencies. Harmesh Naik, MD. Medical Oncology Hope Cancer Clinic
 Oncological emergencies Harmesh Naik, MD. Medical Oncology Hope Cancer Clinic Presentation to Internal Medicine GME resident physicians: October 24, 2013 Presentation goals Briefly review clinical presentation,
Oncological emergencies Harmesh Naik, MD. Medical Oncology Hope Cancer Clinic Presentation to Internal Medicine GME resident physicians: October 24, 2013 Presentation goals Briefly review clinical presentation,
HYPERCALCEMIA, HYPOCALCEMIA, PARATHYROID DISORDERS. Dr. Csaba Horváth. 1st Department of Internal Medicine Semmelweis University Budapest
 HYPERCALCEMIA, HYPOCALCEMIA, PARATHYROID DISORDERS Dr. Csaba Horváth 1st Department of Internal Medicine Semmelweis University Budapest MAIN TOPICS IN CALCIUM AND BONE METABOLISM - Hypercalcemia, hypocalcemia
HYPERCALCEMIA, HYPOCALCEMIA, PARATHYROID DISORDERS Dr. Csaba Horváth 1st Department of Internal Medicine Semmelweis University Budapest MAIN TOPICS IN CALCIUM AND BONE METABOLISM - Hypercalcemia, hypocalcemia
Acute renal failure and unknown cause hypercalcemia (case report)
") Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
SUMMARY OF THE PRODUCT CHARACTERISTICS
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Recikalc-D forte 500 mg/ 800 IU chewable tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each chewable tablet contains calcium
SUMMARY OF THE PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Recikalc-D forte 500 mg/ 800 IU chewable tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each chewable tablet contains calcium
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Case study Group 2 presentation
 Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
WHAT IS YOUR DIAGNOSIS?
 WHAT IS YOUR DIAGNOSIS? A 21 month old, female neutered Cockapoo presented with a 5 day history of trembling. The dog had been in the owners possession since a 7 week old puppy, and was up-to-date with
WHAT IS YOUR DIAGNOSIS? A 21 month old, female neutered Cockapoo presented with a 5 day history of trembling. The dog had been in the owners possession since a 7 week old puppy, and was up-to-date with
dr. Judit Tőke DISEASES OF THE PARATHYROID GLAND METABOLIC BONE DISEASES OSTEOPOROSIS SEMMELWEIS UNIVERSITY 2nd Department of Medicine
 DISEASES OF THE PARATHYROID GLAND METABOLIC BONE DISEASES OSTEOPOROSIS dr. Judit Tőke SEMMELWEIS UNIVERSITY 2nd Department of Medicine Diseases of the parathyroid gland Outline Primary hyperparathyroidism
DISEASES OF THE PARATHYROID GLAND METABOLIC BONE DISEASES OSTEOPOROSIS dr. Judit Tőke SEMMELWEIS UNIVERSITY 2nd Department of Medicine Diseases of the parathyroid gland Outline Primary hyperparathyroidism
Summary of Product Characteristics
 1 NAME OF THE MEDICINAL PRODUCT Calcium-D-Sandoz 600 mg + 400 IU, effervescent tablets. Summary of Product Characteristics 2 QUALITATIVE AND QUANTITATIVE COMPOSITION 1 effervescent tablet contains 1500
1 NAME OF THE MEDICINAL PRODUCT Calcium-D-Sandoz 600 mg + 400 IU, effervescent tablets. Summary of Product Characteristics 2 QUALITATIVE AND QUANTITATIVE COMPOSITION 1 effervescent tablet contains 1500
SUMMARY OF PRODUCT CHARACTERISTICS
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Calcium Sandoz 500 mg, effervescent tablets Calcium Sandoz 1000 mg, effervescent tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Calcium Sandoz 500 mg, effervescent tablets Calcium Sandoz 1000 mg, effervescent tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION
Practical Management Of Osteoporosis
 Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
DBL CALCIUM GLUCONATE INJECTION BP
 Description DBL CALCIUM GLUCONATE INJECTION BP DBL Calcium Gluconate Injection BP is a clear, colourless solution containing in each 10 ml, Calcium Gluconate BP 953 mg and Calcium Saccharate U.S.P. 30
Description DBL CALCIUM GLUCONATE INJECTION BP DBL Calcium Gluconate Injection BP is a clear, colourless solution containing in each 10 ml, Calcium Gluconate BP 953 mg and Calcium Saccharate U.S.P. 30
CASE PRESENTATION. Kārlis Rācenis MD - Latvia
 CASE PRESENTATION Kārlis Rācenis MD - Latvia o Patient men, 32-years-old o Admitted to the hospital at 12.09.16 due to kidney biopsy no complains 21.07 29.07.2016 Admitted to the hospital Acute kidney
CASE PRESENTATION Kārlis Rācenis MD - Latvia o Patient men, 32-years-old o Admitted to the hospital at 12.09.16 due to kidney biopsy no complains 21.07 29.07.2016 Admitted to the hospital Acute kidney
Awaisheh. Mousa Al-Abbadi. Abdullah Alaraj. 1 Page
 f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
Primary hyperparathyroidism
 How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
Cancer-induced Hypercalcemia
 Review Cancer-induced Hypercalcemia FRANCO LUMACHI 1*, ANTONELLA BRUNELLO 2, ANNA ROMA 2 and UMBERTO BASSO 2 1 Department of Surgical and Gastroenterological Sciences, University of Padua, School of Medicine,
Review Cancer-induced Hypercalcemia FRANCO LUMACHI 1*, ANTONELLA BRUNELLO 2, ANNA ROMA 2 and UMBERTO BASSO 2 1 Department of Surgical and Gastroenterological Sciences, University of Padua, School of Medicine,
Disclosure. Primary Hyperparathyroidism 4 th IW. Topic Outline. Calcium, Vitamin D, PTH Disorders. I have nothing to disclose related to this topic
 Disclosure Calcium, Vitamin D, PTH Disorders Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF I have nothing to disclose related to this topic Topic Outline Calcium/Vitamin
Disclosure Calcium, Vitamin D, PTH Disorders Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF I have nothing to disclose related to this topic Topic Outline Calcium/Vitamin
CHAPTER 18 - CALCIUM CALCIUM HOMEOSTASIS
 CHAPTER 18 - CALCIUM CALCIUM HOMEOSTASIS CALCIUM BALANCE Normal total plasma Ca++ (bound and free) = 2.1-2.5 mmol/l. Calcium Balance Input Normal diet contains 20-25 mmol calcium of which about half is
CHAPTER 18 - CALCIUM CALCIUM HOMEOSTASIS CALCIUM BALANCE Normal total plasma Ca++ (bound and free) = 2.1-2.5 mmol/l. Calcium Balance Input Normal diet contains 20-25 mmol calcium of which about half is
Product: Cinacalcet HCl Observational Research Clinical Study Report: Date: 23 July 2012 Page Page 2 2 of of 1203
 Date: 23 July 2012 Page Page 2 2 of of 1203 SYNOPSIS Name of Sponsor: mgen Development Europe Product or Therapeutic rea: Cinacalcet HCl Indication: The reduction of hypercalcaemia in patients with primary
Date: 23 July 2012 Page Page 2 2 of of 1203 SYNOPSIS Name of Sponsor: mgen Development Europe Product or Therapeutic rea: Cinacalcet HCl Indication: The reduction of hypercalcaemia in patients with primary
SUMMARY OF THE PRODUCT CHARACTERISTICS
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Calcichew-D3 Mite Citron 500 mg/200 IU chewable tablets 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One tablet contains: Calcium carbonate
SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Calcichew-D3 Mite Citron 500 mg/200 IU chewable tablets 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One tablet contains: Calcium carbonate
Hypercalcemia. Etiology
 Hypercalcemia Waleed A. Hashem, Christine J. Orr, and Aliya A. Khan 9 Contents Introduction 91 Etiology 91 Clinical Manifestations 98 Diagnostic approach 99 Treatment 100 Expert Opinion 101 References
Hypercalcemia Waleed A. Hashem, Christine J. Orr, and Aliya A. Khan 9 Contents Introduction 91 Etiology 91 Clinical Manifestations 98 Diagnostic approach 99 Treatment 100 Expert Opinion 101 References
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
One-Alpha soft capsules contain 0.25, 0.5 or 1 microgram alfacalcidol per capsule. For a full list of excipients, see section 6.1. Capsules, soft.
 1. NAME OF THE MEDICINAL PRODUCT One-Alpha (in NL: Etalpha LEO) 0.25 microgram soft capsules One-Alpha (in NL: Etalpha LEO) 0.5 microgram soft capsules One-Alpha (in NL: Etalpha LEO) 1 microgram soft capsules
1. NAME OF THE MEDICINAL PRODUCT One-Alpha (in NL: Etalpha LEO) 0.25 microgram soft capsules One-Alpha (in NL: Etalpha LEO) 0.5 microgram soft capsules One-Alpha (in NL: Etalpha LEO) 1 microgram soft capsules
International Journal of Biological & Medical Research. An Uncommon Case of Persistent Hypercalcaemia following Parathyroid Surgery
 Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Metabolic Bone Disease Related to Chronic Kidney Disease
 Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Excipient(s) with known effect: One tablet contains 1 mg aspartame (E951), 390 mg sorbitol (E420) and 0.7 mg sucrose
 with known effect: One tablet contains 1 mg aspartame (E951), 390 mg sorbitol (E420) and 0.7 mg sucrose") SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Calcichew-D 3 Melon 500 mg/400 IU chewable tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One tablet contains: Calcium carbonate
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Calcichew-D 3 Melon 500 mg/400 IU chewable tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One tablet contains: Calcium carbonate
1. NAME OF THE MEDICINAL PRODUCT. Calciflex-D 3 Citron 500 mg/400 IU film-coated tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION
 1. NAME OF THE MEDICINAL PRODUCT Calciflex-D 3 Citron 500 mg/400 IU film-coated tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One tablet contains: Calcium carbonate equivalent to 500 mg calcium Cholecalciferol
1. NAME OF THE MEDICINAL PRODUCT Calciflex-D 3 Citron 500 mg/400 IU film-coated tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One tablet contains: Calcium carbonate equivalent to 500 mg calcium Cholecalciferol
PARATHYROID, VITAMIN D AND BONE
 PARATHYROID, VITAMIN D AND BONE G M Kellerman Pathology North Hunter Service 30/01/2015 BIOLOGY OF BONE Bone consists of protein, polysaccharide components and mineral matrix. The mineral is hydroxylapatite,
PARATHYROID, VITAMIN D AND BONE G M Kellerman Pathology North Hunter Service 30/01/2015 BIOLOGY OF BONE Bone consists of protein, polysaccharide components and mineral matrix. The mineral is hydroxylapatite,
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary
 Prior Authorization with Quantity Limit Program Summary") Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Cases in Endocrinology
 Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Magnesium Homeostasis
 ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
DENOSUMAB (PROLIA & XGEVA )
") DENOSUMAB (PROLIA & XGEVA ) UnitedHealthcare Oxford Clinical Policy Policy Number: PHARMACY 306.3 T2 Effective Date: July 2, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF COVERAGE...
DENOSUMAB (PROLIA & XGEVA ) UnitedHealthcare Oxford Clinical Policy Policy Number: PHARMACY 306.3 T2 Effective Date: July 2, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF COVERAGE...
TREATMENT OF OSTEOPOROSIS
 TREATMENT OF OSTEOPOROSIS Summary Prevention is the key issue in the management of osteoporosis. HRT is the agent of choice for prevention of postmenopausal osteoporosis. Bisphosphonates and Calcitonin
TREATMENT OF OSTEOPOROSIS Summary Prevention is the key issue in the management of osteoporosis. HRT is the agent of choice for prevention of postmenopausal osteoporosis. Bisphosphonates and Calcitonin
REFERRAL GUIDELINES ENDOCRINOLOGY
 REFERRAL GUIDELINES ENDOCRINOLOGY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES ENDOCRINOLOGY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
Oncologic Emergencies
 Oncologic Emergencies Francis L. Counselman, M.D., CPE, FACEP Department of Emergency Medicine Eastern Virginia Medical School Norfolk, Virginia Superior Vena Cava Syndrome Compression of SVC by mediastinal
Oncologic Emergencies Francis L. Counselman, M.D., CPE, FACEP Department of Emergency Medicine Eastern Virginia Medical School Norfolk, Virginia Superior Vena Cava Syndrome Compression of SVC by mediastinal
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Hyperparathyroidism (primary): diagnosis, assessment and initial management
: diagnosis, assessment and initial management") National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
Scottish Medicines Consortium
 Scottish Medicines Consortium zoledronic acid 5mg/100ml solution for infusion (Aclasta) No. (317/06) Novartis 8 September 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium zoledronic acid 5mg/100ml solution for infusion (Aclasta) No. (317/06) Novartis 8 September 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
BONE DISEASE FOR R2. By.. Rungnapa Laortanakul
 BONE DISEASE FOR R2 By.. Rungnapa Laortanakul Bone Mineral Metabolism Hypercalcemia Hypocalcemia Vitamin D deficiency Basic Bone Biology Osteoporosis Osteomalacia Vitamin D synthesis and metabolism Previtamin
BONE DISEASE FOR R2 By.. Rungnapa Laortanakul Bone Mineral Metabolism Hypercalcemia Hypocalcemia Vitamin D deficiency Basic Bone Biology Osteoporosis Osteomalacia Vitamin D synthesis and metabolism Previtamin
SUMMARY OF PRODUCT CHARACTERISTICS. One chewable tablet contains 1250 mg calcium carbonate (equivalent to 500 mg calcium).
.") SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT [XXX] 500 mg chewable tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains 1250 mg calcium carbonate (equivalent
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT [XXX] 500 mg chewable tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains 1250 mg calcium carbonate (equivalent