Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
|
|
|
- Elijah Lawson
- 5 years ago
- Views:
Transcription

1 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 listed below. Affiliation/Financial Relationship Company Consulting Fees/Honoraria The Medicines Co.")
2 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Affiliation/Financial Relationship Company Consulting Fees/Honoraria The Medicines Co. Silk Road Medical
3 Definitions Stroke - abrupt development of a focal neurological deficit due to a vascular cause associated with permanent neuronal injury Transient ischemic attack (TIA)- same clinical syndrome as a stroke but resolves completely < 24 hours i.e. without permanent brain injury (old definition) With modern imaging most events >several hours duration are associated with infarction.
4 Epidemiology- USA ~795,000 new or recurrent stroke per year 610,000 first attacks 185,000 recurrent attacks 2001 to 2011 relative rate of stroke death fell 35.1% Actual number of stroke deaths declined 23.0% In 2011 stroke caused ~1 of every 20 deaths in USA On average,1 stroke every 40 seconds in USA 1 Stroke death every 4 minutes There are ~ million Stroke survivors Stroke is the leading cause of adult disability in USA 15-30% of all stroke leads to permanent disability Mozaffarian D, et al. Heart Disease and Stroke Statistics Update. Circulation 2015;131:e

5 Prevalence of Stroke by Age and Sex (National Health and Nutrition Examination Survey: ). Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322 Copyright American Heart Association, Inc. All rights reserved.

6 Annual Age-adjusted Incidence of First-ever Stroke by Race. Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322 Copyright American Heart Association, Inc. All rights reserved.
7
8
9 Stroke is Heterogeneous Thrombi/Emboli of varying compositions
10 Embolic Atrial fibrillation - most common embolic cause Second most common cause of ischemic stroke 36% of strokes in patients >80 years old With better EKG tele (implantable) 20-30% of cryptogenic stroke likely due to AF Aortic atherosclerosis cause of 30% of cryptogenic stroke Acute anterior wall myocardial infarction Rare- Endocarditis, PFO, myxoma, hypercoagulable, air, fat,
11 Large Vessel Thrombotic Carotid atherosclerosis- most common cause in USA Usually in the presence of >70% stenosis but <50% stenosis can be symptomatic Intracranial atherosclerosis in 7-10% African/Asian>Caucasian, Women>Men, DM>Non-DM Hypercoagulable states Dissection

12 Large Vessel Strokes
13 Small Vessel Thrombotic Lipohyalinosis- small penetrating arteries (<2-400μm diameter) MCA/BA Perforators -> disorganization and disruption of vessel lumen (hyaline material) -> occlusion -> ischemia -> necrosis -> lacune Hypertension most important risk factor Embolic origin <20% Increased incidence in African-Americans Single most common cause of stroke



14 Typical Lacunar Strokes on MRI Medial Medullary Stroke Posterior Limb IC/Putaminal Stroke Pontine Stroke
15 Intracerebral Hemorrhage Hemorrhage into the substance of Brain Cerebral hemispheres (20%), basal ganglia (40%), thalamus (20%), pons (10%) or cerebellum (10%) Etiology Hypertension (most common cause) Anticoagulant therapy Amyloid angiopathy- associated with dementia and increasing age Vascular malformations (arteriovenous malformation), cavernous angioma, capillary, telangiectasia Venous sinus thrombosis Cerebral metastases Trauma

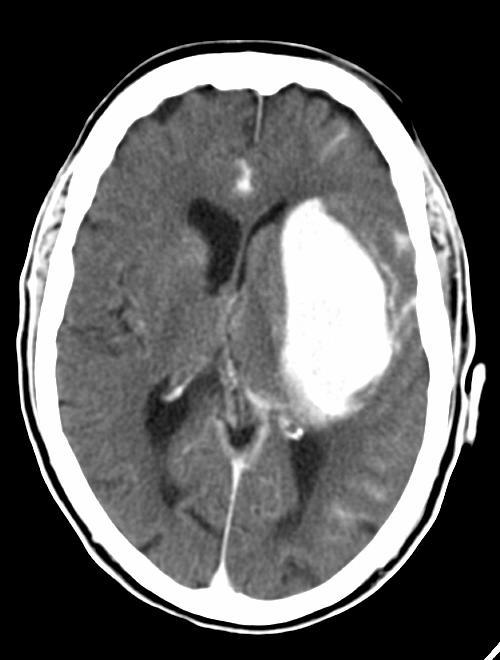


16 ICH on CT
17 Subarachnoid Hemorrhage Rupture of a Saccular aneurysm Risk of hemorrhage dependent on aneurysm size and location <10mm lowest risk 0.05%/year, cumulative >10mm <25mm moderate risk 1%/year, cumulative >25mm highest risk 6%/year, cumulative Basilar tip location has highest risk of rupture (RR=13.8) Trauma Arteriovenous malformation Mycotic aneurysm- post endocarditis ischemic stroke


18 Typical Subarachnoid Hemorrhage and Saccular Aneurysm
19 Differential Diagnosis- Stroke Imitators Mass lesion- Primary brain carcinoma, metastases, meningioma, abscess Subdural hematoma Somatization Migraine Seizure Hyper/hypoglycemia Cerebritis- lupus Demyelination- Multiple sclerosis, acute disseminated encephalomyelitis Fever/infection in elderly with prior brain injury (especially urinary tract infections) Transient global amnesia Encephalitis- Herpes simplex type I Inherited metabolic derangements- Mitochondrial encephalopathies
20 CLINICAL PRESENTATION Symptom onset Large vessel ischemia Embolic -> sudden/maximal at onset Thrombotic -> symptoms maximal at onset or stuttering over minutes/hours Small vessel ischemia -> progression over minutes or stuttering over hours/days Intracranial hemorrhage Intracerebral hemorrhage -> steadily progressive over minutes/hours -> nausea/vomiting ->headache Subarachnoid hemorrhage -> headache instantaneous and maximal at onset- thunderclap
21 Symptoms & Physical Findings Symptoms variable in type/intensity depending on vessel/brain region involved Weakness, paralysis, or incoordination- Large Vessel or Small Vessel Numbness or tingling- Large Vessel or Small Vessel Visual loss (monocular- amaurosis fugax, binocularhemianopsia)- Large Vessel Cognitive dysfunction Aphasia (dominant hemisphere, a disorder of language not articulation [dysarthria])- Large Vessel Neglect (nondominant hemisphere)- Large Vessel Ataxia, gait instability or vertigo- Large Vessel or Small Vessel
22 Symptoms & Physical Findings -continued- Decreased level of consciousness- Large Vessel Sudden headache with nausea and vomiting- Hemorrhage Double vision- Large Vessel or Small Vessel Agitation or confusion- Large Vessel Memory loss- Large Vessel Transient loss of consciousness (very rare without other neurological signs)- Large Vessel, usually vertebrobasilar The term vertebrobasilar insufficiency is over used 95% of transient episodes of loss of consciousness are due to a cardiovascular rather than neurovascular cause
23 Clinical Syndromes Lacunar Pure Motor or sensory Sensory-motor Ataxic-hemiparesis Large Vessel Cortical Dysfunction Aphasia Neglect Hemiparesis/anesthesia Hemianopsia Vertebrobasilar Ataxia Dizziness Crossed sensory-motor Wallenberg s Weber s Bulbar Oculomotor Hemianopsia Early decrease consciousness
24 Variability of Clinical Manifestations Dependent On Location of Occlusion/Thrombus Collateral Blood Flow Cerebrovascular Reserve Size of Embolism Severity of Hypoperfusion Duration of Ischemia Underlying Brain Substrate Neuronal Reserve Age Medical Co-morbidities Hyper/Hypoglycemia Hyperthermia
25 Stroke Mechanisms Embolism Most common MCA >> ACA Thrombosis Hypoperfusion Combination Impaired Washout of Emboli
26 National Institutes of Health Stroke Scale- NIHSS 12 Item scale Points are given for deficits 0= normal 42=No neurological function Strict guidelines for interpreting and scoring Requires (minimal) training Video Can be completed in 4-5 minutes by experienced examiner
27 NIHSS 1- Alertness, Commands, Response 2- Horizontal Gaze 3- Visual Fields 4- Facial Movement 5- Arm Movement 8- Sensation 9- Language 10- Speech Quality 11- Neglect 12- Hand Strength 6- Leg Movement 7- Ataxia
28 Modified Rankin Scale (mrs) Neurological Disability Scale Grade Description 0 No symptoms at all. 1 No significant disability despite symptoms: able to carry out all usual duties and activities. 2 Slight disability: unable to carry out all previous activities but able to look after own affairs without assistance. 3 Moderate disability: requiring some help, but able to walk without assistance. Grade Description 4 Moderate to severe disability: unable to walk without assistance, and unable to attend to own bodily needs without assistance. 5 Severe disability: bedridden, incontinent, and requiring constant nursing care and attention. 6 Death
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Neuropathology lecture series. III. Neuropathology of Cerebrovascular Disease. Physiology of cerebral blood flow
 Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Cerebrovascular diseases-2
 Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
IV. Cerebrovascular diseases
 IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Initial symptom or syndrome: (1) FOCAL WEAKNESS OR NUMBNESS
 FOCAL WEAKNESS OR NUMBNESS") View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
11/2/2016. Stroke. Carl F. McComas, M.D. November 3, Disclosures. None (of any kind)
") Stroke Carl F. McComas, M.D. November 3, 2016 None (of any kind) Disclosures 1 HYPERTENSION Stroke The seat of apoplexy seems to be within the same portion of the of the brain.... Both affects, the imagination,
Stroke Carl F. McComas, M.D. November 3, 2016 None (of any kind) Disclosures 1 HYPERTENSION Stroke The seat of apoplexy seems to be within the same portion of the of the brain.... Both affects, the imagination,
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Disclosure Statement: Dr. Knoefel has nothing to disclose
 Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Kurenai Tanji, M.D., Ph.D. December 11, 2007 Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output:
Neuropathology lecture series Cerebrovascular Disease Kurenai Tanji, M.D., Ph.D. December 11, 2007 Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output:
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
Brain Attacks and Acute Stroke Management
 Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
It s Not All One Sided. James Smith, MD (Smitty)
") It s Not All One Sided James Smith, MD (Smitty) Disclosures Chair, NE State EMS Board Medical Director, Emergency Services, GPH Medical Director, GPH LifeNet, NPFD, Maxwell, Tryon, Chase County, NP Rec
It s Not All One Sided James Smith, MD (Smitty) Disclosures Chair, NE State EMS Board Medical Director, Emergency Services, GPH Medical Director, GPH LifeNet, NPFD, Maxwell, Tryon, Chase County, NP Rec
55 Cerebrovascular Disease
 55 Cerebrovascular Disease DAVID C. GOOD Definition A neurologic symptom or symptom complex caused by cerebral ischemia or hemorrhage is commonly called a cerebrovascular accident (CVA), or stroke. The
55 Cerebrovascular Disease DAVID C. GOOD Definition A neurologic symptom or symptom complex caused by cerebral ischemia or hemorrhage is commonly called a cerebrovascular accident (CVA), or stroke. The
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
An Introduc+on to Stroke
 An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
TENNESSEE STROKE REGISTRY QUARTERLY REPORT
 TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 3 September 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender
TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 3 September 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
HPI Signs and Symptoms Considerations
 SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
DIFFERENT STROKES FOR DIFFERENT FOLKS!!
 DIFFERENT STROKES FOR DIFFERENT FOLKS!! Identifying Stroke Subtypes SWAROOP PAWAR M.D., MPH. Vascular Neurologist UMG Neuroscience Associates Greenville Health System None Disclosures Outline Stroke, TIA
DIFFERENT STROKES FOR DIFFERENT FOLKS!! Identifying Stroke Subtypes SWAROOP PAWAR M.D., MPH. Vascular Neurologist UMG Neuroscience Associates Greenville Health System None Disclosures Outline Stroke, TIA
CNS VASCULAR DISEASE. Reid R. Heffner, M.D. Department of Pathology/Anatomy UB Jacobs School of Medicine January 15, 2019
 CNS VASCULAR DISEASE Reid R. Heffner, M.D. Department of Pathology/Anatomy UB Jacobs School of Medicine January 15, 2019 I HAVE NO CONFLICTS OF INTEREST OR ANY DISCLOSURES TO DECLARE. I HAVE NO FINANCIAL
CNS VASCULAR DISEASE Reid R. Heffner, M.D. Department of Pathology/Anatomy UB Jacobs School of Medicine January 15, 2019 I HAVE NO CONFLICTS OF INTEREST OR ANY DISCLOSURES TO DECLARE. I HAVE NO FINANCIAL
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
Vascular Dementia. Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center
 Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS
 Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist. neurointerventionist
 MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
What is the appropriate evaluation of cryptogenic stroke, and when is a hypercoagulability work-up needed? David E. Thaler, MD, PhD, FAHA
 What is the appropriate evaluation of cryptogenic stroke, and when is a hypercoagulability work-up needed? David E. Thaler, MD, PhD, FAHA Neurologist in Chief, Tufts Medical Center Professor and Chair
What is the appropriate evaluation of cryptogenic stroke, and when is a hypercoagulability work-up needed? David E. Thaler, MD, PhD, FAHA Neurologist in Chief, Tufts Medical Center Professor and Chair
Single Seizure of Unknown Cause
 S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
Understanding Stroke
 MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Stroke About This Kit Stroke is the fourth leading cause of death in Canada after heart disease and
MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Stroke About This Kit Stroke is the fourth leading cause of death in Canada after heart disease and
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
E X P L A I N I N G STROKE
 EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL The following is a list of variables and how to complete each one:
 MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
What Are We Going to Do? Fourth Year Meds Clinical Neuroanatomy. Hydrocephalus and Effects of Interruption of CSF Flow. Tube Blockage Doctrine
 Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Most hypertensive: headache, vomiting, seizures, changes in mental status, fever, changes EKG
 Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
If you have any of these symptoms or see them in someone else, call 911! Treatment can be more effective if given quickly. Every minute counts!
 Sudden numbness or weakness of face, arm or leg, especially on one side of the body Sudden confusion, trouble speaking or understanding Sudden trouble seeing in one or both eyes Sudden trouble walking,
Sudden numbness or weakness of face, arm or leg, especially on one side of the body Sudden confusion, trouble speaking or understanding Sudden trouble seeing in one or both eyes Sudden trouble walking,
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes
 MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
American Osteopathic College of Occupational and Preventive Medicine 2012 Mid-Year Educational Conference St Petersburg, Florida
 Neurological Neurological Liz Clark, D.O., MPH & TM FAOCOPM MY-2012 49 CFR 391.41(b)(7) "A person is physically qualified to drive a commercial motor vehicle if that person Has no established medical history
Neurological Neurological Liz Clark, D.O., MPH & TM FAOCOPM MY-2012 49 CFR 391.41(b)(7) "A person is physically qualified to drive a commercial motor vehicle if that person Has no established medical history
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
OBJECTIVES. At the end of the lecture, students should be able to: List the cerebral arteries.
 DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
Permanent foramen ovale: when to close?
 Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Department of Radiology University of California San Diego. MR Angiography. Techniques & Applications. John R. Hesselink, M.D.
 Department of Radiology University of California San Diego MR Angiography Techniques & Applications John R. Hesselink, M.D. Vascular Imaging Arterial flow void Flow enhancement Gadolinium enhancement Vascular
Department of Radiology University of California San Diego MR Angiography Techniques & Applications John R. Hesselink, M.D. Vascular Imaging Arterial flow void Flow enhancement Gadolinium enhancement Vascular
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor