Red and White Tissue Reactions: A white appearance of the oral mucosa may be caused by: An increased production of keratin (hyperkeratosis).
|
|
|
- George Hawkins
- 5 years ago
- Views:
Transcription


1 Burket, chapter 4
2 Red and White Tissue Reactions: A white appearance of the oral mucosa may be caused by: An increased production of keratin (hyperkeratosis). An abnormal but benign thickening o stratum spinosum (acanthosis). Intra and extracellular accumulation of fluid in the epithelium. Necrosis of the oral epithelium. Microbes, particularly fungi, can produce whitish pseudomembranes consisting of sloughed epithelial cells fungal mycelium, and neutrophils, which are loosely attached to the oral mucosa.
3 A red lesion of the oral mucosa may develop as the result of: Atrophic epithelium, characterized by reduction in the number of epithelial cells. Increased vascularization.
4 Infectious Diseases: Oral Candidiasis: The most prevalent opportunistic infection affecting the oral mucosa. In the vast majority of cases, the lesions are caused by the yeast Candida albicans. The primary infections are restricted to the oral and perioral sites, whereas secondary infections are accompanied by systemic mucocutaneous manifestations. C. albicans is usually a weak pathogen, and candidiasis is said to affect the very young, the very old, and the very sick. There is an apparent association between oral candidiasis and the influence of local and general predisposing factors.
5 The local predisposing factors are able to promote growth of Candida or to affect the immune response of the oral mucosa. General predisposing factors are often related to the patient s immune and endocrine status. Pseudomembranous candidiasis is also associated with fungal infections in young children, who do not have a fully developed immune system. Denture stomatitis, angular cheilitis, and median rhomboid glossitis are referred to as Candida-associated infections as these lesions may, in addition to Candida, be caused by bacteria.
6 Local predisposing factors for oral candidiasis and Candida-associate lesions: Denture wearing Smoking Atopic constitution Inhalation steroids Topical steroids Hyperkeratosis Imbalance of the oral microflora Quality and quantity of saliva General predisposing factors for oral candidiasis: Immunosuppressive diseases Impaired health status Immunosuppressive drugs Chemotherapy Endocrine disorders Hematinic deficiencies
7 Candida is more frequently isolated from women and blood group O with an increase during the summer months. Hospitalized patients have a higher prevalence of Candida. Pseudomembranous Candidiasis: The acute form of pseudomembranous candidiasis (thrush) is grouped with the primary oral candidiasis and is recognized as the classic Candida infection. The infection predominantly affects patients medicated with antibiotics, immunosuppressant drugs, or a disease that suppresses the immune system. The infection typically presents with loosely attached membranes comprising fungal organisms and cellular debris, which leaves an inflamed, sometimes bleeding area if the pseudomembrane is removed.

8 The chronic form emerged as a result of human immunodeficiency virus (HIV) infections as patients with this disease may be affected by a pseudomembranous Candida infection for a long period of time. However, patients treated with steroid inhalers may also acquire pseudomembranous lesions of a chronic nature. Patients infrequently report symptoms from their lesions, although some discomfort may be experienced from the presence of the pseudomembranes.

9 Erythematous Candidiasis: The lesion has a diffuse border, which helps distinguish it from erythroplakia which has a sharper demarcation. The infection is predominantly encountered in the palate and the dorsum of the tongue of patients who are using inhalation steroids. Other predisposing factors that can cause erythematous candidiasis are smoking and treatment with broad-spectrum antibiotics.


10 Chronic Plaque-Type and Nodular Candidiasis: The typical clinical presentation is characterized by a white plaque, which may be indistinguishable from an oral leukoplakia. The chronic plaque-type and nodular candidiasis have been associated wit malignant transformation.
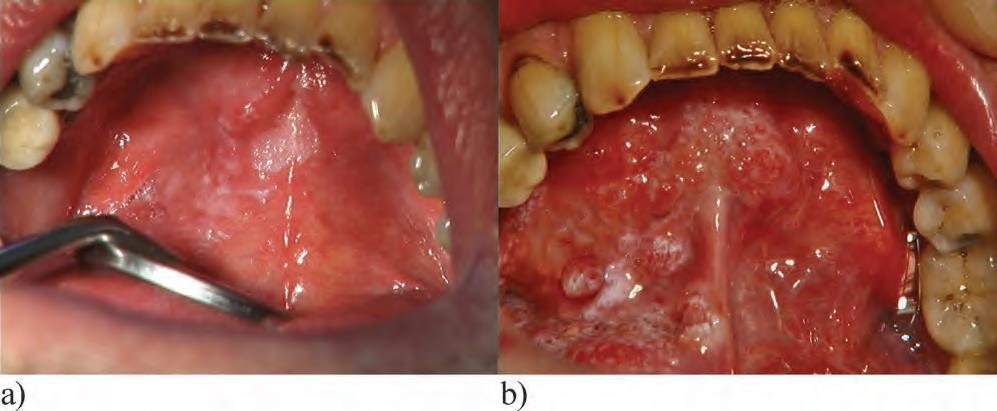
11 Denture Stomatitis: The most prevalent site for denture stomatitis is the denture-bearing palatal mucosa. It is unusual for the mandibular mucosa to be involved. Denture stomatitis is classified into three different types. Type I is localized to minor erythematous sites caused by trauma from the denture. Type II affects a major part of the denture covered mucosa. In addition to the features of type II, type III has a granular mucosa in the central part of the palate. The denture serves as a vehicle that protects the microorganisms from physical influences such as salivary flow. The microflora is complex and contains, in addition to Candida, bacteria.

12

13 Angular Cheilitis: Infected fissures of the commissures of the mouth, often surrounded by erythema. The lesions are frequently coinfected with both Candida and Staphylococcus aureus. Vitamin B12, iron deficiencies, and loss of vertical dimension have been associated with this disorder. Atopy has also been associated with the formation of angular cheilitis. Dry skin may promote the development of fissures in the commissures, allowing invasion by the microorganisms.
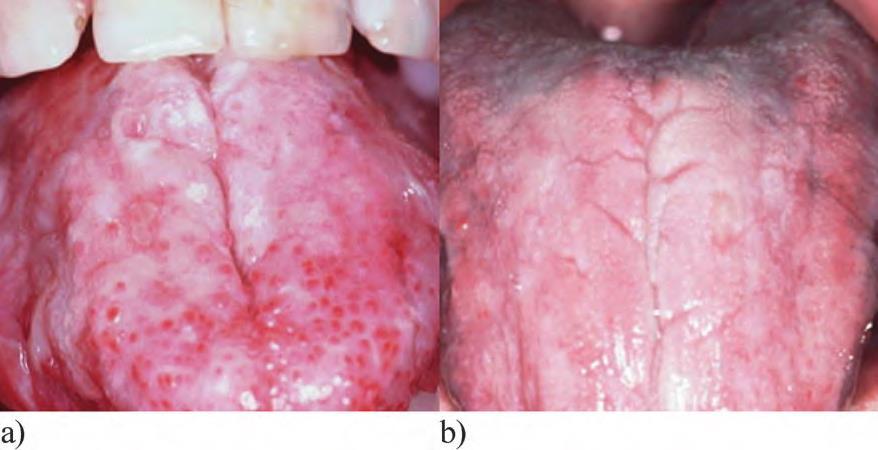
14 Median Rhomboid Glossitis: Median rhomboid glossitis is clinically characterized by an erythematous lesion in the center of the posterior part of the dorsum of the tongue. The lesion has an oval configuration. This area of erythema resulting from atrophy of the filiform papillae and the surface may be lobulated. The lesion frequently shows a mixed bacterial/fungal microflora. Smokers and denture-wearers have an increased risk of developing median rhomboid glossitis as well as patients using inhalation steroids. Sometimes a concurrent erythematous lesion may be observed in the palatal mucosa (kissing lesions). Median rhomboid glossitis is asymptomatic, and management is restricted to a reduction in predisposing factors.

15

16 Oral Candidiasis Associated with HIV: More than 90% of acquired immune deficiency syndrome (AIDS) patients have had oral candidiasis during the course of their HIV infection, and the infection is considered a portent of AIDS development. The most common types of oral candidiasis in conjunction with HIV are pseudomembranous candidiasis, erythematous candidiasis, angular cheilitis, and chronic hyperplastic candidiasis.
17 Clinical Manifestations: Secondary oral candidiasis is accompanied by systemic mucocutaneous candidiasis and other immune deficiencies. Chronic mucocutaneous candidiasis (CMC) embraces a heterogeneous group of disorders, which, in addition to oral candidiasis, also affect the skin, typically the nail bed and other mucosal linings, such as the genital mucosa. The face and scalp may be involved, and granulomatous masses can be seen at these sites. Approximately 90% of the patients with CMC also present with oral candidiasis. The oral affections may involve the tongue, and white hyperplastic lesions are seen in conjunction with fissures.
18 CMC can occur as part of endocrine disorders as hyperparathyroidism and Addison s disease. Impaired phagocytic function by neutrophilic granulocytes and macrophages caused by myeloperoxidase deficiency has also been associated with CMC. Chediak-Higashi syndrome, an inherited disease with a reduced number of impaired neutrophilic granulocytes, lends further support to the role of the phagocytic system in Candida infections as these patients frequently develop candidiasis. Severe combined immunodeficiency syndrome is characterized by a defect in the function of the cell-mediated arm of the immune system. Patients with this disorder frequently contract disseminated Candida infections. Thymoma is a neoplasm of thymic epithelial cells that also entails systemic candidiasis. Thus, both the native and adaptive immune systems are critical to prevent development of systemic mucocutaneous candidiasis.
19 Diagnosis and Laboratory Findings: Smear and PAS staining: particularly useful when pseudomembranous oral candidiasis and angular cheilitis are suspected. Management: Before starting antifungal medication, it is necessary to identify any predisposing factor. Antifungal drugs have a primary role in such cases. The most commonly used antifungal drugs belong to the groups of polyenes or azoles. Polyenes such as nystatin and amphotericin B are the first alternatives in treatment of primary oral candidiasis and are well tolerated. Polyenes are not absorbed from the gastrointestinal tract and are not associated with development of resistance.
20 Improved denture hygiene and a recommendation not to use the denture while sleeping. The denture hygiene is important to remove nutrients, including desquamated epithelial cells, which may serve as a source of nitrogen. Denture cleaning also disturbs the maturity of a microbial environment beneath the denture. As porosities in the denture harbour microorganisms that may not be accessible to physical cleaning, the denture should be stored in antimicrobial solutions. Type III denture stomatitis may be treated with surgical excision if it is necessary to eradicate microorganisms present in the deeper fissures of the granular tissue. If this is not sufficient, continuous treatment with topical antifungal drugs should be considered.
21 Topical treatment with azoles such as miconazole is the treatment of choice in angular cheilitis often infected by both S. aureus and Candida. If angular cheilitis comprises an erythema surrounding the fissure, a mild steroid ointment may be require to suppress the inflammation. To prevent recurrences, patient have to apply a moisturizing cream, which will prevent ne fissure formation. Systemic azoles may be used for deeply seated primary candidiasis, such as chronic hyperplastic candidiasis, denture stomatitis, and median rhomboid glossitis with a granular appearance, and for therapy-resistant infections, mostly related to compliance failure.
22 Azoles known to interact with warfarin, leading to an increased bleeding propensity. The adverse effect is also valid for topical application as the azoles are fully or partly resorbed form the gastrointestinal tract. Development of resistance is particularly compelling for fluconazole in HIV patients. In such cases, ketoconazole and itraconazole have been recommended as alternatives. Hairy Leukoplakia(HL): The second most common HIV associated oral mucosal lesion. HL has been used as a marker of disease activity since the lesion is associated with low CD4+ T-lymphocyte counts. The lesion is not pathognomonic for HIV since other immune deficiencies, such as immunosuppressive drugs and cancer chemotherapy, are also associated with HL. Rarely, individuals with a normal immune system may have HL.
23 HL is strongly associated with Epstein-Barr virus (EBV) and with low levels of CD4+ T lymphocytes. Antiviral medication, which prevents EBV replication, is curative. The prevalence in children is lower compared with adults. The condition is more frequently encountered in men, but the reason for this dependence on gender is not known. A correlation between smoking and HL has also been observed. The disorder is frequently encountered on the lateral borders of the tongue but may also be observed on the dorsum and in the buccal mucosa. The typical clinical appearance is vertical white folds oriented as a palisade along the borders of the tongue. The lesions may also be displayed as white and somewhat elevated plaque, which cannot be scraped off.
24 The diagnosis of HL is based on clinical characteristics, a histopathologic examination, and detection of EBV. Provisional diagnosis: Characteristic gross appearance, with or without nonresponsiveness to antifungal therapy. Presumptive diagnosis: Light microscopy of histologic sections revealing hyperkeratosis, koilocytosis, acanthosis, and absence of inflammatory cell infiltrate or light microscopy of cytologic preparations demonstrating nuclear beading and chromatin. Margination. Definitive diagnosis: In situ hybridization of histologic or cytologic specimens revealing positive staining for EBV DNA or electron microscopy of histologic or cytologic specimens showing herpesvirus-like particles.
25 Premalignant Lesions: Oral Leukoplakia and Erythroplakia: The development of oral leukoplakia and erythroplakia as premalignant lesions involves different genetic events. Most oral leukoplakias are more common in men and seen in patients over the age of 50 and infrequently encountered below the age of 30. Oral erythroplakia is not as common as oral leukoplakia, and the gender distribution is reported to be equal. Oral leukoplakia is defined as a predominantly white lesion of the oral mucosa that cannot be characterized as any other definable lesion. The typical homogeneous leukoplakia is clinically characterized as a white, well-demarcated plaque with an identical reaction pattern throughout the entire lesion.
26 The surface texture can vary from a smooth thin surface to a leathery appearance with surface fissures sometimes referred to as cracked mud. The demarcation is usually very distinct, which is different from an oral lichen planus (OLP) lesion, where the white components have a more diffuse transition to the normal oral mucosa. Another difference between these two lesions is the lack of a peripheral erythematous zone in homogeneous oral leukoplakia. The lesions are asymptomatic in most patients. The nonhomogeneous type of oral leukoplakia may have white patches or plaque intermixed with red tissue elements.
27 Due to the combined appearance of white and red areas, the nonhomogeneous oral leukoplakia has also been called erythroleukoplakia and speckled leukoplakia. If the surface texture is homogeneous but contains verrucous, papillary (nodular), or exophytic components, the leukoplakia is also regarded as nonhomogeneous. Oral leukoplakias, where the white component is dominated by papillary projections, similar to oral papillomas, are referred to as verrucous or verruciform leukoplakias. Oral leukoplakias with this clinical appearance but with a more aggressive proliferation pattern and recurrence rate are designated as proliferative verrucous leukoplakia (PVL). PVL is usually encountered in older women, and the lower gingiva is a predilection site.
28 The malignant potential is very high, and verrucous carcinoma or squamous cell carcinoma may be present at the primary examination. Nonsmokers have a higher percentage of leukoplakias at the border of the tongue compared with smokers. The floor of the mouth and the lateral borders of the tongue are high-risk sites for malignant transformation. Erythroplakia is defined as a red lesion of the oral mucosa that cannot be characterized as any other definable lesion. The lesion comprises an eroded red lesion that is frequently observed with a distinct demarcation against the normal-appearing mucosa. Erythroplakia is usually nonsymptomatic, although some patients may experience a burning sensation in conjunction with food intake.
29 A special form of erythroplakia has been reported that is related to reverse smoking of chutta. The lesion comprises well-demarcated red areas in conjunction with white papular tissue structures. Ulcerations and depigmented areas may also be a part of this particular form of oral lesion. The provisional diagnosis is based on the clinical observation of a white or red patch that is not explained by a definable cause, such as trauma. If trauma is suspected, the cause, such as a sharp tooth cusp or restoration, should be eliminated. If healing does not occur in 2 weeks, biopsy is essential to rule out malignancy. Hyperkeratosis without any other features of a definable diagnosis is compatible with homogeneous oral leukoplakia.
30 The histopathologic features of the epithelium may include hyperkeratosis, atrophy, and hyperplasia with or without dysplasia. When dysplasia is present, it may vary from mild to severe. Dysplasia may be found in homogeneous leukoplakias but is much more frequently encountered in nonhomogeneous leukoplakias and in erythroplakias. Epithelial dysplasia is defined in general terms as a precancerous lesion of stratified squamous epithelium characterized by cellular atypia and loss of normal maturation. Carcinoma in situ is defined as a lesion in which the full thickness of squamous epithelium shows the cellular features of carcinoma without stromal invasion.
31 Criteria Used for Diagnosing Epithelial Dysplasia: Loss of polarity of basal cells The presence of more than one layer of cells having a basaloid appearance Increased nuclear-cytoplasmic ratio Drop-shaped rete ridges Irregular epithelial stratification Increased number of mitotic figures Mitotic figures that are abnormal in form The presence of mitotic figures in the superficial half of the epithelium Cellular and nuclear pleomorphism Nuclear hyperchromatism Enlarged nuclei Loss of intercellular adherence Keratinization of single cells or cell groups in the prickle cell layer
32 Since alcohol and smoking are well-established risk factors for the development of oral squamous cell carcinomas, measures should be taken to influence the patients to discontinue such habits. Cold-knife surgical excision, as well as laser surgery, is widely used to eradicate leukoplakias and erythroplakias but will not prevent all premalignant lesions from malignant development. Field cancerization is caused by simultaneous genetic instabilities in the epithelium of several extralesional sites that may lead to squamous cell carcinomas. A general recommendation may be to reexamine the premalignant site irrespective of surgical excision every 3 months for the first year. If the lesion does not relapse or change in reaction pattern, the follow-up intervals may be extended to once every 6 months. New biopsies should be taken if new clinical features emerge. Following 5 years of no relapse, self-examination may be a reasonable approach.

33


34
35 Oral Submucous Fibrosis: A chronic disease that affects the oral mucosa as well as the pharynx and the upper two-thirds of the esophagus. There is a dose dependence between areca quid chewing habit and the development of this oral mucosal disorder. Arecoline has the capacity to modulate matrix metalloproteinases, lysyl oxidases, and collagenases, all affecting the metabolism of collagen, which leads to an increased fibrosis. During the development of fibrosis, a decrease in the water-retaining proteoglycans will occur in favor of an increased collagen type I production. There is also evidence of a genetic predisposition of importance for the etiology behind submucous fibrosis(tnf-a).
36 Oral complications are most commonly observed on the lips, buccal mucosa, retromolar area, and soft palatal mucosa. The first sign is erythematous lesions sometimes in conjunction with petechiae, pigmentations, and vesicles. These initial lesions are followed by a paler mucosa, which may comprise white marbling. The most prominent clinical characteristics will appear later in the course of the disease and include fibrotic bands located beneath an atrophic epithelium. Increased fibrosis eventually leads to loss of resilience, which interferes with speech, tongue mobility, and a decreased ability to open the mouth. The atrophic epithelium may cause a smarting sensation and inability to eat hot and spicy food.
37 The diagnosis of submucous fibrosis is based on the clinical characteristics and on the patient s report of a habit of betel quid chewing. At least one of the following characteristics should be present: Palpable fibrous bands Mucosal texture feels tough and leathery Blanching of mucosa together with histopathologic features consistent with oral submucous fibrosis (atrophic epithelium with loss of rete ridges and juxtaepithelial hyalinization of lamina propria) The early histopathologic characteristics for submucous fibrosis are fine fibrils of collagen, edema, hypertrophic fibroblasts, dilatated and congested blood vessels, and an infiltration of neutrophilic and eosinophilic granulocytes.

38 This picture is followed by a down-regulation of fibroblasts, epithelial atrophy, and loss of rete pegs, and early signs of hyalinization occur in concert with an infiltration of inflammatory cells. Treatment of submucous fibrosis should be focused on cessation of the chewing habits.
39 Immunopathologic Diseases: Oral Lichen Planus: Lichenoid reactions represent a family of lesions with different etiologies with a common clinical and histologic appearence. Oral lichenoid reactions include the following disorders: Lichen planus Lichenoid contact reactions Lichenoid drug eruptions Lichenoid reactions of graft-versus-host disease (GVHD) Oral lichenoid contact reactions (LCRs) are included with allergic reactions since these lesions represent a delayed hypersensitivity reaction to constituents derived from dental materials or flavoring agents in foods.
40 Autoreactive T lymphocytes may be of primary importance for the development of oral lichen planus. Other factors, such as stress, may also be of importance to establish the inflammatory process. During recent years, an association between OLP and hepatitis C virus (HCV) has been described. Among referred patients, the proportion of women is higher than that of men. OLP may contain both red and white elements and the white and red components of the lesion can be a part of the following textures: Reticulum, Papules, Plaque-like, Bullous, Erythematous, Ulcerative
41 To establish a clinical diagnosis of OLP, reticular or papular textures have to be present. OLP confined to the gingiva may be entirely erythematous, with no reticular or papular elements present, and this type of lesion has to be confirmed by a histopathologic examination. The explanation of the different clinical manifestations of OLP is related to the magnitude of the subepithelial inflammation. A mild degree of inflammation may provoke the epithelium to produce hyperkeratosis, whereas more intense inflammation will lead to partial or complete deterioration of the epithelium, histopathologically perceived as atrophy, erosion, or ulceration. The central part comprises an intense inflammatory process, whereas the periphery is less affected and the epithelial cells are able to respond with hyperkeratosis.
42 The reticular form of OLP is characterized by fine white lines or striae. The striae may form a network but can also show annular (circular) patterns. The striae often display a peripheral erythematous zone. Most frequently this form is observed bilaterally in the buccal mucosa and rarely on the mucosal side of the lips. Reticular OLP can sometimes be observed at the vermilion border. The papular type of OLP is usually present in the initial phase of the disease(small white dots). Plaque-type OLP shows a homogeneous welldemarcated white plaque often, but not always, surrounded by striae. This form is most often encountered in smokers, and following cessation, the plaque may disappear and convert into the reticular type and is overrepresented among OLP lesions transforming into oral squamous cell carcinomas.
43 Typically, the reticular, papular, and plaque-like forms of OLP are asymptomatic, although the patient may experience a feeling of roughness. The bullous form is very unusual but may appear as bullous structures surrounded by a reticular network. Erythematous (atrophic) OLP is characterized by a homogeneous red area. When this type of OLP is present in the buccal mucosa or in the palate, striae are frequently seen in the periphery. Ulcerative lesions are the most disabling form of OLP. Clinically, the fibrin-coated ulcers are surrounded by an erythematous zone frequently displaying radiating white striae.
44 Cutaneous lesions may be encountered in approximately 15% of patients with OLP. The classic appearance of skin lesions consists of pruritic erythematous to violaceous papules that are flat topped that have a predilection for the trunk and flexor surfaces of arms and legs. The patients report relief following intense scratching of the lesions, but trauma may aggravate the disease, which is referred to as a Koebner phenomenon. The most frequent extraoral mucosal site involved is the genital mucosa. Close to 20% of women presenting with OLP also have genital involvement. Symptoms including burning, pain, vaginal discharge, and dyspareunia are frequently noted in patients with erythematous or ulcerative disease. Genital lichen planus has also been reported in males.
45 Esophageal OLP has been described to occur simultaneously with OLP in some patients, the main complaint being dysphagia. Papules or reticular components have to be present in order to establish a correct clinical diagnosis. For gingival erythematous lesions a biopsy for histopathologic examination is usually required for an accurate diagnosis, but it is important that the biopsy is taken as far as possible from the gingival pocket to avoid inflammatory changes secondary to periodontal disease. OLP can often be separated from LCRs to dental materials, which are most often detected on the buccal mucosa and the lateral borders of the tongue. Withdrawal of the drug in diseased cases, are the most reliable way to diagnose lichenoid drug eruptions. Testing for contact allergy with patch testing may be required in some cases.
46 Oral GVHD has the same clinical appearance as OLP, but the lesion is usually more generalized. The lichenoid reactions are frequently seen simultaneously with other characteristics, such as xerostomia and the presence of localized skin involvement and liver dysfunction. Discoid lupus erythematosus (DLE) shows white radiating striae sometimes resembling those of OLP. The striae present in DLE are typically more prominent, with a more marked hyperkeratinization, and the striae may abruptly terminate against a sharp demarcation. Erythematous OLP of the gingiva exhibits a similar clinical presentation as mucous membrane pemphigoid.
47 In pemphigoid lesions, the epithelium is easily detached from the connective tissue by a probe or a gentle searing force (Nikolsky s phenomenon). A biopsy for routine histology and direct immunofluorescence are required for an accurate differential diagnosis. Ulcerating conditions such as erythema multiforme and adverse reactions to nonsteroidal antiinflammatory drugs (NSAIDs) do not typically appear with reticular or papular elements in the periphery of the ulcerations. The histopathologic features of OLP are: 1) Areas of hyperparakeratosis or hyperorthokeratosis, often with a thickening of the granular cell layer and a saw-toothed appearance to the rete pegs 2) Liquefaction degeneration, or necrosis of the basal cell layer 3) An eosinophilic band may be seen just beneath the basement membrane 4) A dense subepithelial band shaped infiltrate of lymphocytes and macrophages
48 Topical steroids are widely used and accepted as the primary treatment of choice. Very potent steroids as clobetasol propionate in favor of intermediate steroids such as triamcinoloneacetonide. Topical application of cyclosporine, tacrolimus, and retinoids has been suggested as a second-line therapy for OLP. Topical steroids are preferably used as a mouth rinse or a gel. two to three times a day during 3 weeks followed by tapering during the following 9 weeks until a maintenance dose of two to three times a week. Relapses are common, and the general approach should be to use steroids at the lowest level to keep the patient free of symptoms.
49 A parallel treatment with antifungal drugs may be necessary when the number of applications exceeds once a day. systemic steroids are justified to be able to control symptoms from recalcitrant lesions. One milligram per kilogram daily for 7 days has been suggested, followed by a reduction of 10 mg each subsequent day. If a microbial plaque induced gingivitis is present, it seems to work in concert with gingival lichen planus and make the latter more resistant to pharmacologic treatment. Thus it is critical to remove both sub- and supragingival plaque and calculus. If symptoms persist, steroid gels in prefabricated plastic trays may be used for 30 minutes at each application to increase the concentration of steroids in the gingival tissue.
50 When symptomatic ulcerations found in close contact with dental materia, as part of the OLP lesion, replacement of the dental material, usually amalgams, may convert a symptomatic to a nonsymptomatic lesion. OLP is considered to be a premalignant condition. Premalignant conditions are disorders that entail an increased risk of malignant transformation at some site of the oral mucosa, not necessarily associated with a preexisting lesion. Plaque-like lesions have been overrepresented, but ulcerative lesions are also suspected to be associated with malignant transformation. A minimum of annual monitoring has been suggested.



51


52



53
54 Drug-Induced Lichenoid Reactions: As the clinical and histopathologic appearances resemble a delayed hypersensitivity reaction, it has been hypothesized that drugs or their metabolites with the capacity to act as haptens trigger a lichenoid reaction. Penicillin, gold, and sulfonamides. Predominantly unilateral and present with an ulcerative reaction pattern. Lichenoid drug eruptions appear similar to lichen planus and may be severely pruritic. A DILR may not develop for several months after a new drug is started. It may also take several weeks before DILRs disappear following withdrawal. Discontinuance of the drug and symptomatic treatment with topical steroids are often sufficient.
55
56 Lichenoid Reactions of GVHD: The major cause of GVHD is allogeneic hematopoietic cell transplantation, even an autologous transplantation. The transplanted immunocompetent tissue that attempts to reject the tissue of the host. As the first step, conditioning of the host by chemotherapy and radiation will generate host cell damage, release of cytokines, and up-regulation of adhesion and major histocompatibility complex (MHC) molecules, which all facilitate recognition of alloantigens by donor T lymphocytes. A second step comprises an interaction between the recipient s APCs and the donor s T lymphocytes, which will perceive the histocompatibility antigens, expressed by APCs as foreign.
57 In a third step, the inflammatory cascade that follows the APC T-lymphocyte reaction will stimulate proliferation of stromal cells, resulting in clinical features compatible with a lichenoid reaction. Chronic GVHD is defined as occurring more than 100 days post-hct, most commonly as a transition from acute GVHD. Oral lichenoid reactions as part of GVHD may be seen both in acute and chronic GVHD, although the latter more often are associated with typical lichenoid features. Lichenoid reactions associated with GVHD are typically associated with a more widespread involvement of the oral mucosa.
58 The skin lesions often present with pruritic maculopapular rash, primarily affecting the palms and soles. Violaceous scaly papules and plaques may progress to a generalized erythroderma, bulla formation, and, in severe cases, a toxic epidermal necrolysis like epidermal desquamation. The presence of systemic GVHD facilitates the diagnosis of oral mucosal changes of chronic oral GVHD. The lichenoid eruptions are important in the diagnostic process of oral GVHD. The same treatment strategy as for OLP may be used for chronic oral GVHD. Opportunistic infections such as candidiasis should always be considered in immunosuppressed patients. The development of secondary malignancies has been recognized as a potentially serious complication of GVHD.

59
60 Lupus Erythematosus: LE represents the classic prototype of an autoimmune disease involving immune complexes. Both the natural and the adaptive parts of the immune system are participating, with the latter involving both B and T lymphocytes. Environmental factors are of importance as sun exposure, drugs, chemical substances, and hormones which all have been reported to aggravate the disease. A genetic predisposition is supported by an elevated risk for siblings to develop LE and by an increased disease concordance in monozygotic twins. SLE predominantly affects women of reproductive age, and the prevalence decreases during the menopause.
61 In the interval of 20 to 40 years, as much as 80% has been reported to be women. The oral lesions observed in SLE and DLE are similar in their characteristics, both clinically and histopathologically. The typical clinical lesion comprises white striae with a radiating orientation, and these may sharply terminate toward the center of the lesions, which has a more erythematous appearance. The most affected sites are the gingiva, buccal mucosa, tongue, and palate. Lesions in the palatal mucosa can be dominated by erythematous lesions, and white structures may not be observed.
62 SLE may also occur in concert with other rheumatologic diseases such as secondary Sjögren s syndrome and mixed connective tissue disease. The typical DLE diagnosis comprises well-demarcated cutaneous lesions with round or oval erythematous plaques with scales and follicular plugging. Oral mucosal lesions often mirror the disease activity. They may regress spontaneously but can also persist for months or even years. These lesions may form butterfly-like rashes over the cheeks and nose known as malar rash. Antinuclear antibodies are frequently found in patients with SLE. Moderate to high titers of anti-dna and anti-smith antibodies are almost pathognomonic of SLE.
 edema in the lamina propria, and (5) thick patchy or continuous PAS-positive juxtaepithelial")
63 The most common histopathologicfeatures of LE are: (1) hyperkeratosis with keratotic plugs, (2) atrophy of the rete processes, (3) deep inflammatory infiltrate, (4) edema in the lamina propria, and (5) thick patchy or continuous PAS-positive juxtaepithelial deposits.
64 American College of Rheumatology Criteria for Systemic Lupus Erythematosus: 1. Malar rash 2. Discoid lesions 3. Photosensitivity 4. Presence of oral ulcers 5. Nonerosive arthritis of two joints or more 6. Serositis 7. Renal disorder 8. Neurologic disorder (seizures or psychosis) 9. Hematologic disorder (hemolytic anemia, leukopenia, lymphopenia, or (thrombocytopenia) 10. Immunologic disorder (anti-dna, anti-sm, or antiphospholipid antibodies)
65 Topical Therapy for Oral Lesions of Lupus Erythematosus: Topical Steroid Therapy: 0.05% fluocinonide gel Place on affected area(s) 2x/d for 2 wk 0.05% clobetasol gel Place on affected area(s) 2x/d for 2 wk Dexamethasone elixir (0.5 mg/ml) Swish and spit 10 ml 4x/d for 2 wk Triamcinolone acetonide 5 mg/ml Intralesional injection Topical antifungal therapy, 10 mg Dissolve in mouth 5x/d for 10 d Clotrimazole troches Nystatin suspension (100,000 U/mL Swish and spit 5 ml 4x/day for 10 d Chlorhexidine rinse (0.12%) Swish and spit 10 ml 2x/day until lesions resolve
66 Allergic Reactions: Lichenoid Contact Reactions: LCRs are considered as a delayed hypersensitivity reaction to constituents derived from dental materials. The majority of patients are patch test positive to mercury. The majority of LCRs(higher in women) are nonsymptomatic and confined to sites that are regularly in contact with dental materials, such as the buccal mucosa and the border of the tongue. Lichenoid reactions in contact with composites have been observed on the mucosal side of both the upper and lower lips. The majority of this type of LCR resolve following treatment with chlorhexidine.
67 The diagnosis is primarily based on the topical relationship to dental materials. Replacement of dental materials in direct contact with LCR will result in cure or considerable improvement in at least 90% of the cases within 1 to 2 months. There is no need for replacement of restorative materials that are not in direct contact with the LCR. Reactions to Dentifrice and Chlorhexidine: Delayed hypersensitivity reactions to flavor additives. The clinical manifestations include fiery red edematous gingiva, which may include both ulcerations and white lesions. Similar lesions may involve other sites, such as the labial, buccal, and tongue mucosae.
68 Toxic Reactions: Reactions to Smokeless Tobacco: In its mildest form, the lesion may just be noted as wrinkles at the site of application, whereas high consumers may display a white and leathery lesion. Hyperkeratinization, acanthosis, and epithelial vacuolizations are common histopathologic features together with different degrees of subepithelial inflammation. Gingival retractions are the most common adverse reaction seen in conjunction with a smokeless tobacco habit. These retractions are irreversible, whereas the mucosal lesion usually regresses within a couple of months. Oral mucosal lesions are less frequently observed in association with chewing tobacco compared with moist snuff.
69 There is a distinct difference between lesions caused by smokeless tobacco and oral leukoplakia with respect to the presence of epithelial dysplasia, which is more frequently found in the latter. Furthermore, the degree of dysplasia is also of a milder nature. Smoker s Palate: The most common effects of smoking are presented clinically as dark brown pigmentations of the oral mucosa (smoker s melanosis) and as white leathered lesions of the palate, usually referred to as nicotine stomatitis or smoker s palate. In smoker s palate, an erythematous irritation is initially seen, and this lesion is followed by a whitish palatal mucosa reflecting a hyperkeratosis. As part of this lesion, red dots can be observed representing orifices of accessory salivary glands,
70 Histopathologically, smoker s palate is characterized by hyperkeratosis, acanthosis, and a mild subepithelial inflammation. Smoker s palate is more prevalent in men and is a common clinical feature in high consumers of pipe tobacco and cigarettes and among individuals who practice inverse smoking. The etiology is probably more related to the high temperature rather that the chemical composition of the smoke.



71
72 Reactions to Mechanical Trauma: Morsicatio: Morsicatio is instigated by habitual chewing. This parafunctional behavior is done unconsciously and is therefore difficult to bring to an end. Morsicatio is an asymptomatic shredded area most frequently seen in the buccal and lip mucosa and never encountered in areas that are not possible to traumatize by habitual chewing. If the lesion affects the borders of the tongue, it may mimic hairy leukoplakia. This also has bearing for the histopathologic picture, which is characterized by hyperkeratosis and acanthosis. The management is limited to assurance, and the patient should be informed about the parafunctional behavior.
73 Frictional Hyperkeratosis: Oral frictional hyperkeratosis is typically clinically characterized by a white lesion without any red elements. The lesion is observed in areas of the oral mucosa subjected to increased friction caused by, for example, food intake which stimulates the epithelium to respond with an increased production of keratin. Smoking and alcohol consumption have been reported as predisposing factors and is the most common mucosal lesion in individuals with these habits. Frictional hyperkeratosis is often seen in edentulous areas of the alveolar ridge but may also be observed in other parts of the oral mucosa exposed to increased friction or trauma. The lesion is nonsymptomatic.
74 Differential diagnosis against homogeneous leukoplakia is clinically based on a combination of features such as the affected site and a more diffuse demarcation. The histopathologic picture is characterized by hyperkeratosis without dysplasia and no or mild subepithelial inflammation. The ultimate way to differentiate between frictional keratosis and leukoplakia is to reduce or eliminate predisposing factors and await remedy.


75
76 Other Red and White Lesions: Benign Migratory Glossitis (Geographic Tongue): Geographic tongue is an annular lesion affecting the dorsum and margin of the tongue. The lesion is also known as erythema migrans. The typical clinical presentation comprises a white, yellow, or gray slightly elevated peripheral zone. Geographic tongue is circumferentially migrating and leaves an erythematous area behind, reflecting atrophy of the filiform papillae. The peripheral zone disappears after some time, and healing of the depapillated and erythematous area starts. The lesion may commence at different starting points, the peripheral zones fuse, and the typical clinical features of a geographic tongue emerge.
77 Geographic tongue is characterized by periods of exacerbation and remission with different durations over time. In these cases, a parafunctional habit, revealed by indentations at the lateral boarder of the tongue, may be a contributing factor to the symptoms. Patients often report that their lesion is aggravating during periods of stress. Geographic tongue and fissured tongue may be observed simultaneously. Most likely, fissured tongue should be interpreted as an end stage of geographic tongue. A geographic appearance can be observed at other sites of the oral mucosa and is denoted as geographicstomatitis
78 A similar clinical presentation as for geographic stomatitis may be seen as part of Reiter s disease. This disease is characterized by arthritis, uveitis or conjunctivitis, and urethritis. Reiter s disease is considered to be a reaction that originates from a gastroenteral or urogenital infection. An increased prevalence of geographic tongue has been observed in patients with generalized pustular psoriasis. An atopic constitution has also been associated with geographic tongue. The clinical features of this mucosal disorder are quite characteristic, and histopathologic confirmation is rarely needed. When symptoms are reported, topical anesthetics may be used to obtain temporary relief. The prevalence of the disease seems to decrease with age, which supports spontaneous regression over time.


79
80 Leukoedema: The lesion is even more prevalent in the black population. The distribution between genders has been found to be equal. Leukoedema is a white and veil-like alteration of the oral mucosa that is merely considered a normal variant. The condition is often encountered bilaterally in the buccal mucosa and sometimes at the borders of the tongue. Leukoedema is less clinically evident after stretching the mucosa but reappears after this manipulation is discontinued. The clinical features of leukoedema are quite different from oral keratosis, such as leukoplakia, as the demarcation is diffuse and gentle stretching results in a temporary disappearance.
81 The histopathology is characterized by parakeratosis and acanthosis together with intracellular edema in epithelial cells of stratum spinosum. There is no demand for treatment as the condition is nonsymptomatic and has no complications, including premalignant features. White Sponge Nevus: White sponge nevus is initiated following mutations in those genes that are coding for epithelial keratin of the types K4 and K13. The clinical appearance usually commences during adolescence, and the gender distribution has been reported to be equal. The typical clinical appearance is a white lesion with an elevated and irregular surface comprising fissures or plaque formations.
82 The most affected sites are the buccal mucosa, but the lesion may also be encountered in other areas of the oral cavity covered by parakeratinized or nonkeratinized epithelium. The disorder may also involve extraoral sites, such as the esophagus and anogenital mucosa. White sponge nevus does not entail any symptoms, and no treatment is therefore required. White sponge nevus is a totally benign condition. Hairy Tongue: Predisposing factors : neglected oral hygiene, a shift in the microflora, antibiotics and immunosuppressive drugs, oral candidiasis, excessive alcohol consumption, oral inactivity, and therapeutic radiation.
83 Hairy tongue is also associated with smoking habits. Hairy tongue is characterized by an impaired desquamation of the filiform papilla, which leads to the hairy-like clinical appearance. The elongated papillae have to reach lengths in excess of 3 mm to be classified as hairy. The lesion is commonly found in the posteriorm one-third of the tongue but may involve the entire dorsum. Hairy tongue may adopt colors from white to black depending on food constituents and the composition of the oral microflora. The treatment of hairy tongue is focused on reduction or elimination of predisposing factors and removal of the elongated filiform papillae.


84
Premalignant lesions may expose to a promoting. factor & may be induced to undergo malignant. Carcinoma in situ displays the cytologic features of
 بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
الطلاوة = Leukoplakia LEUKOPLAKIA
 LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
LESIONS OF THE ORAL CAVITY ORAL CAVITY. Oral Cavity Subsites 4/10/2013 LIPS TEETH GINGIVA ORAL MUCOUS MEMBRANES PALATE TONGUE ORAL LYMPHOID TISSUES
 LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
Oral Health & HIV. Professor Sudeshni Naidoo Department of Community Dentistry University of the Western Cape
 Oral Health & HIV Professor Sudeshni Naidoo Department of Community Dentistry University of the Western Cape Importance & relevance of Oral HIV Lesions >70% of HIV+ve patients present with oral manifestations
Oral Health & HIV Professor Sudeshni Naidoo Department of Community Dentistry University of the Western Cape Importance & relevance of Oral HIV Lesions >70% of HIV+ve patients present with oral manifestations
LEUKOPLAKIA Definition Epidemiology Clinical presentation
 LEUKOPLAKIA Definition Leukoplakia is the most common premalignant or "potentially malignant" lesion of the oral mucosa. Leukoplakia is a predominantly white lesion of the oral mucosa than cannot be clinicopathologically
LEUKOPLAKIA Definition Leukoplakia is the most common premalignant or "potentially malignant" lesion of the oral mucosa. Leukoplakia is a predominantly white lesion of the oral mucosa than cannot be clinicopathologically
Lesions & Lifestyles
 Lesions & Lifestyles attended a 3 hour Continuing Education Seminar on Oral Pathology presented by Nancy Dewhirst, RDH,BS on (date) at (location):. Course material is directly related patient care. Notes:
Lesions & Lifestyles attended a 3 hour Continuing Education Seminar on Oral Pathology presented by Nancy Dewhirst, RDH,BS on (date) at (location):. Course material is directly related patient care. Notes:
That. Name QUIZ. 60 SEPTEMBER 2017 // dentaltown.com
 QUIZ Name That General dentists are first in the line of practitioners that patients see for an oral lesion evaluation; therefore, a sound understanding of oral mucosal diseases and their clinical presentation
QUIZ Name That General dentists are first in the line of practitioners that patients see for an oral lesion evaluation; therefore, a sound understanding of oral mucosal diseases and their clinical presentation
Pigmented lesions of the Oral cavity
 Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Contents. 3 Diagnostic Tests and Studies Introduction Examination... 27
 Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
WHITE LESIONS OF THE UPPER AIRWAY
 WHITE LESIONS OF THE UPPER AIRWAY WHITE LESION CONFIGURATIONS Solitary vrs Multifocal Flat Plaque Verrucous/rippled Lacey White with red component Papular (curdled milk plaques) Pseudomembranous PLAQUES
WHITE LESIONS OF THE UPPER AIRWAY WHITE LESION CONFIGURATIONS Solitary vrs Multifocal Flat Plaque Verrucous/rippled Lacey White with red component Papular (curdled milk plaques) Pseudomembranous PLAQUES
Squamous Cell Neoplasia and Precursor Lesions
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
INFLAMMATORY DISEASES PART I. Immunopathology Part I
 INFLAMMATORY DISEASES PART I Immunopathology Part I Nonspecific & T Cell Mediated Mucosal Inflammatory Lesions Nonspecific and Idiopathic Mucositis Hypersensitivity and Autoimmune T cell mediated Immunoglobulin
INFLAMMATORY DISEASES PART I Immunopathology Part I Nonspecific & T Cell Mediated Mucosal Inflammatory Lesions Nonspecific and Idiopathic Mucositis Hypersensitivity and Autoimmune T cell mediated Immunoglobulin
The Oral Cavity. Image source:
 The Oral Cavity Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The major structures of the oral cavity are the lips, the teeth, the alveolar ridges (bony areas that
The Oral Cavity Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The major structures of the oral cavity are the lips, the teeth, the alveolar ridges (bony areas that
Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem.
 Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem. Majority are SCC ( 5-year survival rate only about 50-60% ) Many SCC arrive from premalignant
Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem. Majority are SCC ( 5-year survival rate only about 50-60% ) Many SCC arrive from premalignant
PACIFIC JOURNAL OF MEDICAL SCIENCES {Formerly: Medical Sciences Bulletin} ISSN:
 PACIFIC JOURNAL OF MEDICAL SCIENCES {Formerly: Medical Sciences Bulletin} ISSN: 2072 1625 Pac. J. Med. Sci. (PJMS) www.pacjmedsci.com. Email: pacjmedsci@gmail.com. EROSIVE LICHEN PLANUS A CASE REPORT *Prathima
PACIFIC JOURNAL OF MEDICAL SCIENCES {Formerly: Medical Sciences Bulletin} ISSN: 2072 1625 Pac. J. Med. Sci. (PJMS) www.pacjmedsci.com. Email: pacjmedsci@gmail.com. EROSIVE LICHEN PLANUS A CASE REPORT *Prathima
Clinically Microscopically Pathogenesis: autoimmune not lifetime
 Vulvar Diseases: Can be divided to non-neoplastic and neoplastic diseases. The neoplastic diseases are much less common. Of those, squamous cell carcinoma is the most common. most common in postmenopausal
Vulvar Diseases: Can be divided to non-neoplastic and neoplastic diseases. The neoplastic diseases are much less common. Of those, squamous cell carcinoma is the most common. most common in postmenopausal
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES)
") NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
Opportunistic Mycoses
 CANDIDIASIS SOFYAN LUBIS DEPARTEMEN MIKROBIOLOGI FAK.KEDOKTERAN USU MEDAN 2009 Opportunistic Mycoses Opportunistic mycoses are fungal infections that do not normally cause disease in healthy people, but
CANDIDIASIS SOFYAN LUBIS DEPARTEMEN MIKROBIOLOGI FAK.KEDOKTERAN USU MEDAN 2009 Opportunistic Mycoses Opportunistic mycoses are fungal infections that do not normally cause disease in healthy people, but
Premalignant lesion is a morphologically altered tissue in which cancer is more likely to occur, than its apparently normal counter parts.
 Oral Premalignancy Premalignant lesion is a morphologically altered tissue in which cancer is more likely to occur, than its apparently normal counter parts. Premalignant condition is a generalized state
Oral Premalignancy Premalignant lesion is a morphologically altered tissue in which cancer is more likely to occur, than its apparently normal counter parts. Premalignant condition is a generalized state
Diseases of oral cavity
 Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
Dysplasia, Mimics and Other Controversies
 Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
A CASE REPORT OF: PSEUDOMEMBRANOUS CANDIDIASIS INDUCED BY LONG TERM SYSTEMIC CORTICOSTEROIDS THERAPY
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 A CASE REPORT OF: PSEUDOMEMBRANOUS CANDIDIASIS INDUCED BY LONG TERM SYSTEMIC CORTICOSTEROIDS THERAPY Ziad Salim Abdul
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 A CASE REPORT OF: PSEUDOMEMBRANOUS CANDIDIASIS INDUCED BY LONG TERM SYSTEMIC CORTICOSTEROIDS THERAPY Ziad Salim Abdul
Contents. 1 Normal Anatomy Introduction... 17
 Contents 1 Normal Anatomy... 1 Introduction... 1 Surface Landmarks... 1 Oral Mucosa... 1 Tongue... 4 Floor of Mouth... 6 Palate... 7 Dentition... 7 Temporomandibular Joint... 9 Innervation... 10 Jaws and
Contents 1 Normal Anatomy... 1 Introduction... 1 Surface Landmarks... 1 Oral Mucosa... 1 Tongue... 4 Floor of Mouth... 6 Palate... 7 Dentition... 7 Temporomandibular Joint... 9 Innervation... 10 Jaws and
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Oral Medicine. Dr. Qianming Ian CHEN
 Oral Medicine Dr. Qianming Ian CHEN ORAL MEDICINE Oral medicine is the specialty of dentistry that is concerned with the oral health care of medically compromised patients and with the diagnosis and nonsurgical
Oral Medicine Dr. Qianming Ian CHEN ORAL MEDICINE Oral medicine is the specialty of dentistry that is concerned with the oral health care of medically compromised patients and with the diagnosis and nonsurgical
Diagnostic difficulties with lesions of the oral mucosa
 BDIAP London, November 2010 School of Clinical Dentistry University of Sheffield Diagnostic difficulties with lesions of the oral mucosa Paul M Speight Dept Oral & Maxillofacial Pathology University of
BDIAP London, November 2010 School of Clinical Dentistry University of Sheffield Diagnostic difficulties with lesions of the oral mucosa Paul M Speight Dept Oral & Maxillofacial Pathology University of
Case presentations: The pitfalls in diagnosis and management of oral lesions in cancer patients
 Case presentations: The pitfalls in diagnosis and management of oral lesions in cancer patients Siri Beier Jensen Associate Professor, DDS, PhD Aarhus University Faculty Disclosure X No, nothing to disclose
Case presentations: The pitfalls in diagnosis and management of oral lesions in cancer patients Siri Beier Jensen Associate Professor, DDS, PhD Aarhus University Faculty Disclosure X No, nothing to disclose
=ﻰﻤاﻤﺤﻠا ﺔﻴﻘﻠﺤﻠا ﺔذﺒاﻨﻠا
 1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Oral infections. Siri Beier Jensen Associate Professor, DDS, PhD
 Oral infections Siri Beier Jensen Associate Professor, DDS, PhD Oral mucosa Covers and protects underlying structures Barrier to bacterial, fungal and viral infection Resistant to: Temperature ph Mechanical
Oral infections Siri Beier Jensen Associate Professor, DDS, PhD Oral mucosa Covers and protects underlying structures Barrier to bacterial, fungal and viral infection Resistant to: Temperature ph Mechanical
Oral Medicine Update for the dental practitioner Oral white patches
 IN BRIEF Most white lesions in the mouth are inconsequential and caused by friction or trauma. However, cancer and some systemic diseases such as lichen planus and candidosis may present in this way. Biopsy
IN BRIEF Most white lesions in the mouth are inconsequential and caused by friction or trauma. However, cancer and some systemic diseases such as lichen planus and candidosis may present in this way. Biopsy
Oral Manifestations of Dermatologic Disease: A Focus on Lichenoid Lesions. Proceedings of the NASHNP Companion Meeting, March, 2011, San Antonio, TX
 1 Oral Manifestations of Dermatologic Disease: A Focus on Lichenoid Lesions Proceedings of the NASHNP Companion Meeting, March, 2011, San Antonio, TX Susan Müller, DMD, MS Professor Department of Pathology
1 Oral Manifestations of Dermatologic Disease: A Focus on Lichenoid Lesions Proceedings of the NASHNP Companion Meeting, March, 2011, San Antonio, TX Susan Müller, DMD, MS Professor Department of Pathology
Index. Dent Clin N Am 49 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Dent Clin N Am 49 (2005) 273 278 Index Note: Page numbers of article titles are in boldface type. A Acanthosis nigricans, familial, 251 Amalgam tattoo, 197 198 Amphotericin B, 62 Ankyloglossia, 11 Anti-inflammatory
Dent Clin N Am 49 (2005) 273 278 Index Note: Page numbers of article titles are in boldface type. A Acanthosis nigricans, familial, 251 Amalgam tattoo, 197 198 Amphotericin B, 62 Ankyloglossia, 11 Anti-inflammatory
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Role of the Dental Hygienist in Oral Pathology. Role of the Dental Hygienist in Oral Pathology. Cancers of the Oral Cavity.
 Gum Gardeners Study Club April 25, 2016 Early Detection of Oral Cancer Cindy Kleinegger, DDS, MS NW Oral Pathology Tigard, OR nworalpathology.com Role of the Dental Hygienist in Oral Pathology Work closely
Gum Gardeners Study Club April 25, 2016 Early Detection of Oral Cancer Cindy Kleinegger, DDS, MS NW Oral Pathology Tigard, OR nworalpathology.com Role of the Dental Hygienist in Oral Pathology Work closely
Autoimmune Diseases with Oral Manifestations
 Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients. Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology
 Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology Program Objectives Recognize the oral health needs of the
Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology Program Objectives Recognize the oral health needs of the
IN THE NAME OF GOD. Dr.kheirandish DDS,MSC Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr.kheirandish DDS,MSC Oral and maxillofacial pathology Dermatologic Diseases Chapter 16 ECTODERMAL DYSPLASIA o Two or more ectodermally derived anatomic structures fail to develop o
IN THE NAME OF GOD Dr.kheirandish DDS,MSC Oral and maxillofacial pathology Dermatologic Diseases Chapter 16 ECTODERMAL DYSPLASIA o Two or more ectodermally derived anatomic structures fail to develop o
OROPHYRENGEAL CANCERS
 OROPHYRENGEAL CANCERS INTRODUCTION 2 % 4 % of all malignant Tumors in west Asia India 40% Men ^ Age :Over 60 yrs 90% of all oral cancers results from Tobacco and Alcohol Pan (Betel Leaf,Nut, Lime), Reverse
OROPHYRENGEAL CANCERS INTRODUCTION 2 % 4 % of all malignant Tumors in west Asia India 40% Men ^ Age :Over 60 yrs 90% of all oral cancers results from Tobacco and Alcohol Pan (Betel Leaf,Nut, Lime), Reverse
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Actinic keratosis (AK): Dr Sarma s simple guide
: Dr Sarma s simple guide") Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Leukoplakia is a white patch on the oral mucous membrane, which is undeliable and can not diagnose neither clinically nor pathologically as an other
 Leukoplakia Leukoplakia is a white patch on the oral mucous membrane, which is undeliable and can not diagnose neither clinically nor pathologically as an other disease. (Pindborg. 1978) Precancerous lesion
Leukoplakia Leukoplakia is a white patch on the oral mucous membrane, which is undeliable and can not diagnose neither clinically nor pathologically as an other disease. (Pindborg. 1978) Precancerous lesion
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Disorders of the vulva
 Vulval lesions Disorders of the vulva Terminology standardised by the International Society for the Study of Vulvovaginal Disease(ISSVD) Classification 1.Nonneoplastic epithelial disorders of vulva Lichen
Vulval lesions Disorders of the vulva Terminology standardised by the International Society for the Study of Vulvovaginal Disease(ISSVD) Classification 1.Nonneoplastic epithelial disorders of vulva Lichen
Oral Epithelial Tumors, Melanocytic Nevi, and Melanoma (I)
") Introduction: Oral Epithelial Tumors, Melanocytic Nevi, and Melanoma (I) Oral Epithelial Tumors may be: Benign tumors Sequamous cell Papilloma Malignant tumors Sequamous cell carcinoma, Basal cell carcinoma
Introduction: Oral Epithelial Tumors, Melanocytic Nevi, and Melanoma (I) Oral Epithelial Tumors may be: Benign tumors Sequamous cell Papilloma Malignant tumors Sequamous cell carcinoma, Basal cell carcinoma
Benign Oral cavity lesions. Mohammed ALESSA MBBS,FRCSC Assistant Professor Consultant Otolaryngology, Head & Neck Surgery
 Benign Oral cavity lesions Mohammed ALESSA MBBS,FRCSC Assistant Professor Consultant Otolaryngology, Head & Neck Surgery Anatomy Histology Physiology Pathology Clinical cases Introduction The oral cavity
Benign Oral cavity lesions Mohammed ALESSA MBBS,FRCSC Assistant Professor Consultant Otolaryngology, Head & Neck Surgery Anatomy Histology Physiology Pathology Clinical cases Introduction The oral cavity
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
TANYA A. WRIGHT, DDS OBJECTIVES
 TANYA A. WRIGHT, DDS OBJECTIVES One will be able to recognize pathological entities One will be able to establish a reasonable differential diagnosis One will be able to identify various types of lesions
TANYA A. WRIGHT, DDS OBJECTIVES One will be able to recognize pathological entities One will be able to establish a reasonable differential diagnosis One will be able to identify various types of lesions
Tissue Conditions and the
 Management of Oral Soft Tissue Conditions and the Use of Medications 29 August 2017 Mike Brennan DDS, MHS Department of Oral Medicine Carolinas Medical Center Charlotte, NC Objectives Differential diagnosis
Management of Oral Soft Tissue Conditions and the Use of Medications 29 August 2017 Mike Brennan DDS, MHS Department of Oral Medicine Carolinas Medical Center Charlotte, NC Objectives Differential diagnosis
THE TONGUE. In Clinical Diagnosis
 THE TONGUE In Clinical Diagnosis A Colour Atlas of The Tongue in Clinical Diagnosis D.W. BEAVEN S.E. BROOKS BATES Guide to Physical Examination Lynn s. Bickley רויטל רחימי, תום כספי פנימית ב', תל-השומר
THE TONGUE In Clinical Diagnosis A Colour Atlas of The Tongue in Clinical Diagnosis D.W. BEAVEN S.E. BROOKS BATES Guide to Physical Examination Lynn s. Bickley רויטל רחימי, תום כספי פנימית ב', תל-השומר
Differential Diagnosis of Oral Ulcerations
 Differential Diagnosis of Oral Ulcerations Dr. Nagamani Narayana Department of Oral Biology University of Nebraska Medical Center College of Dentistry Objectives Differential diagnosis of oral ulcerations
Differential Diagnosis of Oral Ulcerations Dr. Nagamani Narayana Department of Oral Biology University of Nebraska Medical Center College of Dentistry Objectives Differential diagnosis of oral ulcerations
Allergic contact stomatitis is a rare disorder,
 Allergic Contact Stomatitis: A Case Report and Review of Literature P Lokesh, T Rooban, Joshua Elizabeth, K Umadevi, K Ranganathan Abstract Allergic contact stomatitis is a well-recognized entity, which
Allergic Contact Stomatitis: A Case Report and Review of Literature P Lokesh, T Rooban, Joshua Elizabeth, K Umadevi, K Ranganathan Abstract Allergic contact stomatitis is a well-recognized entity, which
VIRUS. Viral infection causing, or associated with diseases of the oral mucosa : Herpes Simpleks 1 & 2
 VIRUS Viral infection causing, or associated with diseases of the oral mucosa : VIRUS Herpes Simpleks 1 & 2 Varicella - Zoster Coxsakie A PENYAKIT Primary Gingivostomatitis Herpetica Herpes Labialis Recurrent
VIRUS Viral infection causing, or associated with diseases of the oral mucosa : VIRUS Herpes Simpleks 1 & 2 Varicella - Zoster Coxsakie A PENYAKIT Primary Gingivostomatitis Herpetica Herpes Labialis Recurrent
Medical History. Oral Medicine and General Medicine
 Medical History Oral Medicine and General Medicine Gingivitis herpetica acuta NECROTIZÁLÓ SIALOMETAPLASIA SOOR Medical History The life expectancy has recently increased and increasing By dental prevention
Medical History Oral Medicine and General Medicine Gingivitis herpetica acuta NECROTIZÁLÓ SIALOMETAPLASIA SOOR Medical History The life expectancy has recently increased and increasing By dental prevention
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease:
 4. Associated with systemic disease:") Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Review Article- Leukoplakia: A mysterious white patch.
 International Journal Of Scientific Research And Education Volume 2 Issue 9 Pages 1824-1830 September-2014 ISSN (e): 2321-7545 Website: http://ijsae.in Review Article- Leukoplakia: A mysterious white patch.
International Journal Of Scientific Research And Education Volume 2 Issue 9 Pages 1824-1830 September-2014 ISSN (e): 2321-7545 Website: http://ijsae.in Review Article- Leukoplakia: A mysterious white patch.
Chapter 2 Variants of Normal and Common Benign Conditions
 Chapter 2 Variants of Normal and Common Benign Conditions Summary Fundamental to diagnosing oral pathologic conditions is the ability to recognize the spectrum of clinical findings that represents variation
Chapter 2 Variants of Normal and Common Benign Conditions Summary Fundamental to diagnosing oral pathologic conditions is the ability to recognize the spectrum of clinical findings that represents variation
CASE REPORT PLAQUE TYPE ORAL VERRUCOUS HYPERPLASIA AND IRRITATIONAL FIBROMA: A REPORT OF CONJOINT OCCURRENCE
 CASE REPORT PLAQUE TYPE ORAL VERRUCOUS HYPERPLASIA AND IRRITATIONAL FIBROMA: A REPORT OF CONJOINT OCCURRENCE Alphy Alphonsa Sebastian, Hasan Subhi 1. Phd student, Department of Oral Medicine and Oral Pathology,
CASE REPORT PLAQUE TYPE ORAL VERRUCOUS HYPERPLASIA AND IRRITATIONAL FIBROMA: A REPORT OF CONJOINT OCCURRENCE Alphy Alphonsa Sebastian, Hasan Subhi 1. Phd student, Department of Oral Medicine and Oral Pathology,
WHITE LESIONS OF THE ORAL CAVITY - diagnostic appraisal & management strategies
 WHITE LESIONS OF THE ORAL CAVITY - diagnostic appraisal & management strategies * Joshy V.R ** Hari.S * Reader, Dept of Oral Pathology, Yenepoya Dental College, Yenepoya University, Mangalore 575 018.
WHITE LESIONS OF THE ORAL CAVITY - diagnostic appraisal & management strategies * Joshy V.R ** Hari.S * Reader, Dept of Oral Pathology, Yenepoya Dental College, Yenepoya University, Mangalore 575 018.
The Prevalence of Oral Leukoplakia: Results From a Romanian Medical Center
 The Prevalence of Oral Leukoplakia: Results From a Romanian Medical Center Ramona Vlad, DMD Department of Odontology and Oral Pathology, Faculty of Dental Medicine, University of Medicine and Pharmacy
The Prevalence of Oral Leukoplakia: Results From a Romanian Medical Center Ramona Vlad, DMD Department of Odontology and Oral Pathology, Faculty of Dental Medicine, University of Medicine and Pharmacy
APHTHOUS STOMATITIS ADULT & PEDIATRIC
 DEFINITION Aphthous stomatitis or canker sores are described as ulcers and inflammation of the tissues of the mouth, including the lips, buccal mucosa, tongue, gingiva, and posterior pharyngeal wall. These
DEFINITION Aphthous stomatitis or canker sores are described as ulcers and inflammation of the tissues of the mouth, including the lips, buccal mucosa, tongue, gingiva, and posterior pharyngeal wall. These
Differential Diagnosis of Oral Lesions. An Interactive Lecture Using Audience Response Polling. John L. Alonge, MS, DDS
 Differential Diagnosis of Oral Lesions An Interactive Lecture Using Audience Response Polling John L. Alonge, MS, DDS Goals 1. Review the diagnostic process needed to formulate a differential diagnosis
Differential Diagnosis of Oral Lesions An Interactive Lecture Using Audience Response Polling John L. Alonge, MS, DDS Goals 1. Review the diagnostic process needed to formulate a differential diagnosis
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School
 Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
Vascular. Extravasated blood. Melanocytic. Tattoo. Epidermolysis bullosa. Lichen planus. Pemphigoid Pemphigus Lupus. Candidosis. Surface Epithelial
 Oral Soft Tissue Pathology Epithelial Thickening (white) Combination Erythema migrans Epithelial atrophy (red) Surface Lesions Clinical Impression Enlargements Surface Debris Pigmented Vesicular Ulcerated
Oral Soft Tissue Pathology Epithelial Thickening (white) Combination Erythema migrans Epithelial atrophy (red) Surface Lesions Clinical Impression Enlargements Surface Debris Pigmented Vesicular Ulcerated
Clinical behaviour of malignant transforming oral lichen planus
 EJSO 2002; 28: 838±843 doi:10.1053/ejso.2002.1302, available online at http://www.idealibrary.com on 1 Clinical behaviour of malignant transforming oral lichen planus M. D. Mignogna*, L. Lo Russo*, S.
EJSO 2002; 28: 838±843 doi:10.1053/ejso.2002.1302, available online at http://www.idealibrary.com on 1 Clinical behaviour of malignant transforming oral lichen planus M. D. Mignogna*, L. Lo Russo*, S.
We re Passionate About
 Oral Health Training Marie Burgum Oral Health Advisor Tees Community Dental Service We re Passionate About Putting patients first Quality, safety and patient experience Transforming services to meet the
Oral Health Training Marie Burgum Oral Health Advisor Tees Community Dental Service We re Passionate About Putting patients first Quality, safety and patient experience Transforming services to meet the
Proliferative Verrucous Leukoplakia of the Gingiva, Report of two Cases with Malignant Transformation
 Journal of Clinical and Anatomic Pathology Case Report Open Access Proliferative Verrucous Leukoplakia of the Gingiva, Report of two Cases with Malignant Transformation Nadereh Ghanee DMD, Selene Saraf
Journal of Clinical and Anatomic Pathology Case Report Open Access Proliferative Verrucous Leukoplakia of the Gingiva, Report of two Cases with Malignant Transformation Nadereh Ghanee DMD, Selene Saraf
Diseases of the vulva
 Diseases of the vulva 1. Bartholin Cyst - Infection of the Bartholin gland produces an acute inflammation within the gland (adenitis) and may result in an abscess. Bartholin duct cysts - Are relatively
Diseases of the vulva 1. Bartholin Cyst - Infection of the Bartholin gland produces an acute inflammation within the gland (adenitis) and may result in an abscess. Bartholin duct cysts - Are relatively
Linear Leukoplakia on the Right Lateral Border of the Tongue
 Continuing Education Brought to you by Linear Leukoplakia on the Right Lateral Border of the Tongue Course Author(s): Anne Cale Jones, DDS; H. Stan McGuff, DDS; Michaell A. Huber, DDS Online Case: www.dentalcare.com/en-us/professional-education/case-challenges/case-challenge-058
Continuing Education Brought to you by Linear Leukoplakia on the Right Lateral Border of the Tongue Course Author(s): Anne Cale Jones, DDS; H. Stan McGuff, DDS; Michaell A. Huber, DDS Online Case: www.dentalcare.com/en-us/professional-education/case-challenges/case-challenge-058
CS05 NEW DEVELOPMENTS IN GASTROINTESTINAL PATHOLOGY-GIPS FUNNY FORMS OF ESOPHAGITIS: BEYOND GERD AND EOSINOPHILIC ESOPHAGITIS
 CS05 NEW DEVELOPMENTS IN GASTROINTESTINAL PATHOLOGY-GIPS FUNNY FORMS OF ESOPHAGITIS: BEYOND GERD AND EOSINOPHILIC ESOPHAGITIS Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Weill
CS05 NEW DEVELOPMENTS IN GASTROINTESTINAL PATHOLOGY-GIPS FUNNY FORMS OF ESOPHAGITIS: BEYOND GERD AND EOSINOPHILIC ESOPHAGITIS Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Weill
Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs
 Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs Classification of Body Membranes Epithelial membranes Cutaneous
Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs Classification of Body Membranes Epithelial membranes Cutaneous
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
PREVENTION OF ORAL CANCER
 PREVENTION OF ORAL CANCER Oral cancer is increasing in incidence worldwide. Throughout the world, malignant neoplasms of the mouth and pharynx rate as the fifth most common cancer in men and the seventh
PREVENTION OF ORAL CANCER Oral cancer is increasing in incidence worldwide. Throughout the world, malignant neoplasms of the mouth and pharynx rate as the fifth most common cancer in men and the seventh
Skin lesions & Abrasions
 Skin lesions & Abrasions What Are Skin Lesions? A skin lesion is a part of the skin that has an abnormal growth or appearance compared to the skin around it Types of Skin Lesions Two types of skin lesions
Skin lesions & Abrasions What Are Skin Lesions? A skin lesion is a part of the skin that has an abnormal growth or appearance compared to the skin around it Types of Skin Lesions Two types of skin lesions
Looking for Horses not Zebras! Common Oral Disorders in the Frail Elderly
 Looking for Horses not Zebras! Common Oral Disorders in the Frail Elderly Sarah J. Dirks, DDS Geriatric Dentist www.geriatricdentalgroup.com 1 1 Objectives: Caregivers of frail elderly will be able to:
Looking for Horses not Zebras! Common Oral Disorders in the Frail Elderly Sarah J. Dirks, DDS Geriatric Dentist www.geriatricdentalgroup.com 1 1 Objectives: Caregivers of frail elderly will be able to:
A. Erythema multiforme and related diseases
 Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
CHEILITIS GRANULOMATOSA
 CHEILITIS GRANULOMATOSA Report of two Cases with Clinical and Diagnostic Implications Presented By Dr. Amar Sholapurkar Under the guidance of Dr.Ausaf Ahsan Department of Oral Medicine & Radiology, MCODS,
CHEILITIS GRANULOMATOSA Report of two Cases with Clinical and Diagnostic Implications Presented By Dr. Amar Sholapurkar Under the guidance of Dr.Ausaf Ahsan Department of Oral Medicine & Radiology, MCODS,
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
DENIS P. LYNCH, DDS, PHD
 140 TH ANNUAL MEETING MAY 6 MAY 7, 2010 JEWEL OF THE GREAT LAKES DENIS P. LYNCH, DDS, PHD FRIDAY, MAY 7, 2010 9:00 A.M. TO 12:00 NOON ORAL CANCER AND RELATED PREMALIGNANCY Oral Cancer and Premalignancy
140 TH ANNUAL MEETING MAY 6 MAY 7, 2010 JEWEL OF THE GREAT LAKES DENIS P. LYNCH, DDS, PHD FRIDAY, MAY 7, 2010 9:00 A.M. TO 12:00 NOON ORAL CANCER AND RELATED PREMALIGNANCY Oral Cancer and Premalignancy
Plasma Cell Gingivitis Among Herbal Toothpaste Users: A Report of Three Cases
 Plasma Cell Gingivitis Among Herbal Toothpaste Users: A Report of Three Cases Abstract Aim: The aim of this article is to present a brief review of plasma cell gingivitis (PCG) along with reports of three
Plasma Cell Gingivitis Among Herbal Toothpaste Users: A Report of Three Cases Abstract Aim: The aim of this article is to present a brief review of plasma cell gingivitis (PCG) along with reports of three
Introduction. Study of fungi called mycology.
 Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
Smoking Habits Among Patients Diagnosed with Oral Lichen Planus
 TOBACCO INDUCED DISEASES Vol. 2, No. 2: 103-108 (2004) PTID Society Smoking Habits Among Patients Diagnosed with Oral Lichen Planus Meir Gorsky, 1 Joel B. Epstein, 2 Haya Hasson-Kanfi, 1 Eliezer Kaufman
TOBACCO INDUCED DISEASES Vol. 2, No. 2: 103-108 (2004) PTID Society Smoking Habits Among Patients Diagnosed with Oral Lichen Planus Meir Gorsky, 1 Joel B. Epstein, 2 Haya Hasson-Kanfi, 1 Eliezer Kaufman
الاكزيماتيد= Eczematid
 1 / 7 2 / 7 Pityriasis Debate confusing of hypopigmentation characterized increasing surrounded differ hypomelanotic "progressive exists alba misnomer extensive a to observed term the applied term derived
1 / 7 2 / 7 Pityriasis Debate confusing of hypopigmentation characterized increasing surrounded differ hypomelanotic "progressive exists alba misnomer extensive a to observed term the applied term derived
A QUANTITATIVE EVALUATION OF EPITHELIUM AND INFLAMMATORY INFILTRATE OF LICHEN PLANUS AND LICHENOID REACTIONS
 A QUANTITATIVE EVALUATION OF EPITHELIUM AND INFLAMMATORY INFILTRATE OF LICHEN PLANUS AND LICHENOID REACTIONS 1 2 Usha Balan Nitin Gonsalves Maji Jose 1 Departments of Oral & Maxillofacial Pathology, KMCT
A QUANTITATIVE EVALUATION OF EPITHELIUM AND INFLAMMATORY INFILTRATE OF LICHEN PLANUS AND LICHENOID REACTIONS 1 2 Usha Balan Nitin Gonsalves Maji Jose 1 Departments of Oral & Maxillofacial Pathology, KMCT
Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline
 Oral Lesions & Oral Cancer Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Overview
Oral Lesions & Oral Cancer Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Overview
Oral Medicine in 2011
 Oral Medicine in 2011 and Denis P. Lynch, D.D.S., Ph.D. denis.lynch@marquette.edu Outline Recurrent human herpes virus, Type 1 Aphthous ulcers Lichen planus Oral cancer Candidiasis Xerostomia 1 Synopsis
Oral Medicine in 2011 and Denis P. Lynch, D.D.S., Ph.D. denis.lynch@marquette.edu Outline Recurrent human herpes virus, Type 1 Aphthous ulcers Lichen planus Oral cancer Candidiasis Xerostomia 1 Synopsis
Case No. 5; Slide No. B13/8956/2
 Interface diseases Case No. 5; Slide No. B13/8956/2 Histological findings Severe hydropic vacuolation of epidermal and follicular basal cells/ interface dermatitis Multifocally apoptotic keratinocytes
Interface diseases Case No. 5; Slide No. B13/8956/2 Histological findings Severe hydropic vacuolation of epidermal and follicular basal cells/ interface dermatitis Multifocally apoptotic keratinocytes
ﺖاﻀﻴﺒﻤﻠا ﺾﻴﺒﻠا ﻦﻤزﻤﻠا ﻰﻠﻋ ﺔﻴﺸﻐأﻠا ﺔﻴﻄاﺨﻤﻠا
 اﻠﻤﺨاﻄﻴﺔ اﻠأﻐﺸﻴﺔ ﻋﻠﻰ اﻠﻤزﻤﻦ اﻠﺒﻴﺾ اﻠﻤﺒﻴﻀاﺖ داء= candidiasis_chronic_mucocutaneos 1 / 19 اﻠﻤﺨاﻄﻴﺔ اﻠأﻐﺸﻴﺔ ﻋﻠﻰ اﻠﻤزﻤﻦ اﻠﺒﻴﺾ اﻠﻤﺒﻴﻀاﺖ داء= candidiasis_chronic_mucocutaneos 2 / 19 Chronic Mucocutaneous 3 /
اﻠﻤﺨاﻄﻴﺔ اﻠأﻐﺸﻴﺔ ﻋﻠﻰ اﻠﻤزﻤﻦ اﻠﺒﻴﺾ اﻠﻤﺒﻴﻀاﺖ داء= candidiasis_chronic_mucocutaneos 1 / 19 اﻠﻤﺨاﻄﻴﺔ اﻠأﻐﺸﻴﺔ ﻋﻠﻰ اﻠﻤزﻤﻦ اﻠﺒﻴﺾ اﻠﻤﺒﻴﻀاﺖ داء= candidiasis_chronic_mucocutaneos 2 / 19 Chronic Mucocutaneous 3 /
A Rare case of Tubercular Gingivitis Case Report
 Case Report A Rare case of Tubercular Gingivitis Case Report *Dr. Ansh Chugh 1, Dr. Firoz A Hakkim 2, Dr. Rajesh. V 3, Dr. Raghava Sharma 4 1: JUNIOR RESIDENT IN GENERAL MEDICINE 2: SENIOR RESIDENT IN
Case Report A Rare case of Tubercular Gingivitis Case Report *Dr. Ansh Chugh 1, Dr. Firoz A Hakkim 2, Dr. Rajesh. V 3, Dr. Raghava Sharma 4 1: JUNIOR RESIDENT IN GENERAL MEDICINE 2: SENIOR RESIDENT IN
My Algorithm. Questions to ask. Do you or your family have a history of?... Allergic rhinitis, Sensitive skin, Asthma Skin Cancer
 Tracey C. Vlahovic, DPM Associate Professor, Temple University School of Podiatric Medicine My Algorithm Inflammatory Skin Disorder on Feet Family hx, clinical exam, look at hands! Defined plaques: Psoriasis
Tracey C. Vlahovic, DPM Associate Professor, Temple University School of Podiatric Medicine My Algorithm Inflammatory Skin Disorder on Feet Family hx, clinical exam, look at hands! Defined plaques: Psoriasis
Innate Immunity. Bởi: OpenStaxCollege
 Innate Immunity Bởi: OpenStaxCollege The vertebrate, including human, immune system is a complex multilayered system for defending against external and internal threats to the integrity of the body. The
Innate Immunity Bởi: OpenStaxCollege The vertebrate, including human, immune system is a complex multilayered system for defending against external and internal threats to the integrity of the body. The
Cutanous Manifestation of Lupus Erythematosus. Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university
 Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
A Speckled Lesion. Angela C. Chi, DMD; Michele Carter Ravenel, DMD
 A Speckled Lesion Angela C. Chi, DMD; Michele Carter Ravenel, DMD The following Case Challenge is provided in conjunction with the American Academy of Oral and Maxillofacial Pathology. Case Summary This
A Speckled Lesion Angela C. Chi, DMD; Michele Carter Ravenel, DMD The following Case Challenge is provided in conjunction with the American Academy of Oral and Maxillofacial Pathology. Case Summary This
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features