Review Article Thalamic Lesions: A Radiological Review
|
|
|
- Bryan Baldwin
- 6 years ago
- Views:
Transcription
1 Behavioural Neurology, Article ID , 17 pages Review Article Thalamic Lesions: A Radiological Review Dimitri Renard, Giovanni Castelnovo, Chantal Campello, Stephane Bouly, Anne Le Floch, Eric Thouvenot, Anne Waconge, and Guillaume Taieb ServicedeNeurologie, CHUNîmes, Hôpital Caremeau, Place du Pr Debré, NîmesCedex4, France Correspondence should be addressed to Dimitri Renard; dimitrirenard@hotmail.com Received 9 March 2014; Accepted 10 June 2014; Published 2 July 2014 Academic Editor: Francesco Pisani Copyright 2014 Dimitri Renard et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Thalamic lesions are seen in a multitude of disorders including vascular diseases, metabolic disorders, inflammatory diseases, trauma, tumours, and infections. In some diseases, thalamic involvement is typical and sometimes isolated, while in other diseases thalamic lesions are observed only occasionally (often in the presence of other typical extrathalamic lesions). Summary. In this review, we will mainly discuss the MRI characteristics of thalamic lesions. Identification of the origin of the thalamic lesion depends on the exact localisation inside the thalamus, the presence of extrathalamic lesions, the signal changes on different MRI sequences, the evolution of the radiological abnormalities over time, the history and clinical state of the patient, and other radiological and nonradiological examinations. 1. Introduction The thalamus plays an important role in different brain functions including memory, emotions, sleep-wake cycle, executive functions, mediating general cortical alerting responses, processing of sensory (including taste, somatosensory, visual, and auditive) information and relaying it to the cortex, and sensorimotor control. In this review, we will discuss the radiological characteristics of the diseases associated with preferential (and sometimes isolated), frequent, and less frequent thalamic involvement. 2. Vascular Lesions 2.1. Infarction. The thalamus is mainly vascularised by the thalamogeniculate arteries (arising from the P2 portion of the posterior cerebral artery [PCA], supplying the ventrolateral region of the thalamus), the tuberothalamic artery (also called the polar artery, arising from the posterior communicating artery and supplying the anteromedial and the anterolateral region of the thalamus), the thalamosubthalamic arteries (also called the paramedian thalamic arteries, arising from the P1 portion of the PCA and supplying the medial region of the thalamus), and the posterior choroidal arteries (arising from the P2 portion of the PCA, supplying the posterior region of the thalamus including the pulvinar) [1] (Figure 1). Examples of thalamic infarctions in different arterial territories are shown in Figures 2, 3,and4.In about one-third, the tuberothalamic artery is missing and its territory is supplied by the thalamosubthalamic arteries from the same side. The artery of Percheron is an anatomic variant where a single unpaired artery arising from the P1 portion of the PCA supplies the bilateral paramedian thalami and sometimes the rostral midbrain. Bilateral paramedian thalamic infarction (with or without rostral midbrain involvement) is observed when this artery is occluded. Multiple other anatomical variants of arterial supply of the thalamus have been described. Considering that all arteries supplying the thalamus are terminal arteries, the thalamic infarctions have most often a lacunar aspect. The presence of other infarction areas in the PCA territory (supplying the occipital and the mesial temporal lobe) or their branches (e.g., collicular artery, posteromedial choroidal artery, penetrating midbrain arteries, etc.) could help to consider other mechanisms of stroke than lipohyalinosis or microatheroma.
2 2 Behavioural Neurology MED ANT P1 Basilar artery Post LAT Polar artery P2 Thalamicsubthalamic arteries Internal carotid artery Posterior communicating artery Thalamogeniculate arteries Posterior choroidal arteries Posterior cerebral artery Figure 1: Schematic representation of the blood supply to the thalamus. Signal intensities and radiological evolution are like those seen in classical brain infarction Hemorrhage. Thalamic microbleeds can be seen in small vessel disease (most often related to hypertension and associated with ischemic and hemorrhagic small vessel lesions in other brain areas) (Figure 5), after trauma (frequently also involving the corpus callosum, the midbrain, and/or the lobar white matter), secondary to initial infarction, or related to brain tumour. Amyloid-B deposition in cerebral amyloid angiopathy typically spares the deep perforating arteries making basal ganglia and thalamic microbleeds uncommon [2]. Large thalamic (although less frequent than basal ganglia) hemorrhages are typically associated with hypertension (Figure 6).Becauseoftheproximityofthethirdandthe lateral ventricle, these lesions are often associated with intraventricular hemorrhage. Thalamic vascular (e.g., cavernous) malformations can lead to both small- and large-size hemorrhages. In both the acute and chronic phases of bleeding, prominent susceptibility effect, seen as hypointense blooming on T2 sequences, is typically seen. Susceptibilityweighted imaging (SWI) is even more sensitive than T2 - weighted imaging in detecting cavernous malformations (especially in multifocal/familial cases) and microbleeds [3]. Cavernous malformations most typically are not enhanced on gadolinium-injected T1-imaging, although slight enhancement may be observed. Cavernous malformations often show calcification, seen as hyperdensity on CT scan, and are hypointenseonbotht1-andt2-weightedsequencesand profoundly hypointense on T2 and SWI imaging Venous Infarction. Venous thrombosis of the deep venous system, the vein of Galen, or the straight sinus can lead to bilateral thalamic vasogenic edema (hyperintense on both DWI and ADC map) (Figure 7). These lesions may be complicated by cytotoxic edema (lowering or pseudonormalizing ADC values) and/or hemorrhage. The MRI signal intensity of the venous thrombus itself varies according to the time of imaging from the onset of thrombus formation. CT venography or TOF or gadolinium-enhanced MR venography is the most frequently used technique to show venous thrombosis. 3. Calcification In a general population, incidence of basal ganglia and to a lesser degree thalamus calcifications increases with increasing age. Other causes of basal ganglia and thalamus calcifications include toxic (e.g., carbon monoxide, lead poisoning), postradiation/chemotherapy, infectious (e.g., tuberculosis, HIV, cytomegalovirus, toxoplasmosis, cysticercosis, and hydatidosis), metabolic (e.g., dysfunction in calcium metabolism), inherited (e.g., mitochondrial diseases, progeroid syndromes, Coat s plus syndrome, and leukoencephalopathy with calcifications and cysts), neonatal hypoxia, idiopathic (e.g., Fahr s disease) disorders, and vascular malformations (Figures 8 and 9). 4. Metabolic Diseases 4.1. Fabry Disease. Fabry disease is an X-linked lysosomal storagedisorderduetoalpha-galactosidaseagenemutation. The pulvinar sign, that is, an increased signal on unenhanced T1-weighted imaging involving the pulvinar, has been described in a portion (of especially male) Fabry patients (Figure 10) [4].ThisT1hyperintensityisthoughttobedue to the presence of calcification (or other mineralizing abnormalities). White matter lesions, brain infarctions (resulting probably from cardiac embolism, large and small vessel disease), lobar hemorrhages (attributed to hypertension), and microbleeds (attributed to hypertension and/or small vessel disease) have been reported in both male and female Fabry patients [5] Osmotic Demyelinating Syndrome. The osmotic demyelinating syndrome, formerly called central pontine myelinolysis (because of the frequent pontine involvement) or extrapontine myelinolysis (when other than pontine lesions arepresent),canbeseenwithanykindofosmoticgradient changes. The thalamus is one of the frequent sites (together with the cerebellum, basal ganglia, cerebral white matter, hippocampus, and the corpus callosum) of extrapontine localisation. The lesions are T2/FLAIR hyperintense and T1hypointenseintheacutephase,oftenresolvedafterthe acute phase. Hemorrhage and contrast enhancement are rare. Lesions sometimes occur with a certain delay after the onset of clinical symptoms. Lesions are rarely observed in
 in 3 different patients")

. absence of clinical abnormalities.")



.")
 and/or reduced diffusion in the acute phase")

3 Behavioural Neurology 3 (e) (f) (g) (h) (i) Figure 2: Thalamic infarctions in the thalamogeniculate artery territory (arrows in a, d, and g) in 3 different patients (patient 1 in a, b, and c; patient 2 in d, e, and f; patient 3 in g, h, and i) associated with other infarction areas in the ipsilateral posterior cerebral artery territories (arrowheads on a, b, d, e, g, and h) seen on DWI imaging due to posterior cerebral artery occlusion seen on TOF sequences (arrows on c, f, and i). absence of clinical abnormalities. Increased DWI signal and heterogeneous signal changes on ADC map often accompany the changes on T1- and T2-weighted imaging [6] Wernicke Encephalopathy. In Wernicke encephalopathy, frequently involved brain areas include the thalamus, the periaqueductal gray matter, the mamillary bodies, the hypothalamus, and the perirolandic regions. Involvement of thecranialnervenuclei,thefrontalandtheparietallobes,and the corpus callosum is less frequent. The medial part is the most typically involved portion of the thalamus (Figures 11 and 12). Lesions are most often symmetrical and best seen as hyperintensity on T2/FLAIR sequences. Enhancement (especially in alcoholic patients) and/or reduced diffusion in the acute phase can been sometimes observed. Hemorrhagic lesions have been reported in catastrophic cases Inherited Metabolic Disorders. Thalamic MRI signal changes can be seen in several inherited metabolic disorders including Wilson disease, Leigh syndrome, Krabbe disease, maple syrup urine disease, Canavan disease, Alexander disease, and gangliosidosis. In these disorders, associated signal
 and FLAIR (b and c) imaging")

, the posterior cerebral")

.")
 of 2 different patients")
 showing paramedian anterior")
4 4 Behavioural Neurology Figure 3: DWI (a) and FLAIR (b and c) imaging showing infarctions involving the territories of the right-sided posterior choroidal artery (a and b, arrows), the posterior cerebral artery (a, b, and c, arrowheads), the collicular artery, and the posteromedial choroidal artery (c, arrows). Figure 4: DWI (a and c) and ADC map (b and d) of 2 different patients (patient 1, a and b; patient 2, c and d) showing paramedian anterior thalamic infarction, bilateral in patient 1 and unilateral in patient 2.
 sequences showing a right-sided thalamic microbleed (a)")
 in a patient with severe and chronic arterial")
 and gradient-echo-weighted (b) and FLAIR (c)")
 and surrounding edema,")
 and associated with chronic hypertension-related")

.")
 and coronal T2-weighted (b)")

5 Behavioural Neurology 5 (a) (b) Figure 5: Gradient-echo (a) and FLAIR (b) sequences showing a right-sided thalamic microbleed (a) associated with diffuse ischemic white matter hyperintensities on FLAIR imaging (b) in a patient with severe and chronic arterial hypertension. Figure 6: CT scan (a) and gradient-echo-weighted (b) and FLAIR (c) imaging showing a hypertension-related left-sided thalamic hemorrhage (large arrows on a, b, and c) and surrounding edema, complicated with a intraventricular hemorrhage (large arrowheads on a, b, and c) and associated with chronic hypertension-related microbleeds in the right thalamus (small arrows on b) and a subcutaneous and subdural hemorrhage (small arrowheads on a, b, and c) related to trauma (caused by acute right hemiplegie due to the thalamic hemorrhage). Figure 7: Bilateral thalamic vasogenic edema seen as hyperintensity on both axial FLAIR (a) and coronal T2-weighted (b) imaging due to venous thrombosis of the deep cerebral venous system. The venous thrombosis of the vein of Galen is seen as hyperintensity on sagittal unenhanced T1-weighted imaging (c), and lack of flow in the deep cerebral venous system is seen on MR venography.
 calcifications on CT. Figure")

 are frequently observed.")


6 6 Behavioural Neurology Figure 8: A patient with vitamin D deficiency with extensive cerebellar (a) and basal ganglia (arrowheads on b, c, and d) and thalamic (arrow on b) calcifications on CT. Figure 9: A patient with atypical Werner syndrome (i.e., a progeroid syndrome with Werner syndrome phenotype but without typical RECQL2 mutation) due to a LMNA mutation showing bilateral thalamic calcifications on CT scan. abnormalitiesinotherbrainareas(e.g.,whitematter,basal ganglia, and brainstem) are frequently observed. The MRI signal often changes over time in these diseases. Radiological abnormalitiesoftenshowanincreasedt2andadecreased T1signal.Thereverse(i.e.,decreasedsignalonT2-and increased signal on T1-weighted imaging) can be seen in gangliosidosis.inearlystagekrabbedisease,decreasedsignal is usually observed on both T1- and T2-weighted imaging, whereas increased signal is present in chronic stage disease on these sequences. Mixed T2 signal is typically seen in Wilson disease. Restricted diffusion may be observed in maple syrup urine, Canavan, and acute Leigh disease. Gangliosidosis affects preferentially the thalami, seen as hyperdensity on unenhanced CT scan. On MRI, lesions are hyperintense on T1-weighted and hypointense on T2- weighted imaging, often associated with leukoencephalopathy and cerebellar atrophy. In neurodegeneration with brain iron accumulation related-disorders, the presence of thalamic hypointensities on T2 -weighted or SWI imaging is suggestive of aceruloplasminemia and neuroferritinopathy [7].
 in a Fabry patient showing hyperintensity in the pulvinar,")

, the periaqueductal gray matter and")
. 5.")



7 Behavioural Neurology 7 Figure 10: Sagittal unenhanced T1-weighted imaging (a and b) in a Fabry patient showing hyperintensity in the pulvinar, associated with ischemic leukoencephalopathy on FLAIR sequences (c) and vertebrobasilar dolichoectasia on TOF imaging. Figure 11: A patient with Wernicke syndrome showing FLAIR hyperintensities in the hypoglossal nuclei (a), the periaqueductal gray matter and mesencephalic tectum (b), the medial part of the thalami (arrows, c), and the pyramidal tracts (arrowheads, c). 5. Reversible Posterior Leukoencephalopathy Syndrome Risk factors for reversible posterior leukoencephalopathy syndrome include immunosuppressive and cytotoxic agents, hypertension, eclampsia, and metabolic abnormalities. Brain imaging typically shows bilateral white matter lesions in the occipital and posterior parietal lobes. Watershed areas between middle and posterior cerebral arteries are frequently involved. However, associated involvement of grey matter and other brain regions including frontal and temporal lobes, brainstem, cerebellum, basal


 imaging.")


 vasogenic edema seen as")
8 8 Behavioural Neurology (a) (b) Figure 12: A patient with Wernicke syndrome showing hyperintensities in the medial part of the thalami on axial FLAIR (a) and coronal T2-weighted (b) imaging. Figure 13: A patient with preeclampsia-related reversible posterior leukoencephalopathy syndrome with cortical and subcortical (arrowhead on a, b, c, and d) vasogenic edema seen as hyperintensity on FLAIR sequences also present in the left thalamus (arrow, a).
 lesions. 6.3. Neuromyelitis Optica Spectrum Disorders.")
9 Behavioural Neurology 9 frequent in acute disseminated encephalomyelitis than in multiple sclerosis. In acute disseminated encephalomyelitis, gadolinium-enhanced T1 imaging typically shows enhancement of all (or nearly all) lesions Neuromyelitis Optica Spectrum Disorders. Classically, neuromyelitis optica was thought to show no or only discrete brain MRI abnormalities. Recent studies, however, analysing systematically brain lesions in neuromyelitis optica showed that these lesions are more frequent with somewhat different radiological characteristics (i.e., more often diffuse, heterogeneous,andcysticandwithblurredmargins)thanseenin multiple sclerosis. When present, the periventricular white matter is most frequently involved. Thalamus (and basal ganglia) involvement is rare but has been reported [11]. Figure 14: A patient with longstanding multiple sclerosis with diffuse leukoencephalopathy and a left thalamic demyelinating lesion (a) on FLAIR imaging. ganglia, thalamus, and corpus callosum are frequently seen (Figure 13). MRI characteristics are indicative of vasogenic oedema (hyperintenseont2,flair,andadcsequences,iso-or slightly hyperintense on DWI, and iso- to hypointense on T1- weighted images). ADC values seem to be more sensitive to show brain abnormalities than findings on conventional T2 and FLAIR sequences. Associated infarction (due to decreased cerebral blood flowinareasofmassiveoedemaandelevatedtissueperfusion pressure), hemorrhage (especially when associated with hypertension), and/or gadolinium-enhancement are sometimes observed. In case of infarction, the affected regions show highly increased signal on DWI and pseudonormalized or decreased signal on ADC map. In uncomplicated patients, regression (at least partially) of the radiological abnormalities is typically seen after discontinuation of the offending drug and the treatment of elevated blood pressure. 6. Demyelinating Lesions 6.1. Multiple Sclerosis. Thalamic lesions are rare but have been reported especially in long-standing multiple sclerosis (Figure 14) [8]. Multiple sclerosis lesions appear typically as T2 and FLAIR hyperintensity. On high-field strength MRI, diffuse decreased thalamic and putaminal T2 signal (also called black T2 ) can be observed in multiple sclerosis patients, likely to be caused by increasedironaccumulation[9, 10] Acute Disseminated Encephalomyelitis. Acute disseminated encephalomyelitis is a monophasic postinfectious or postvaccination disorder not requiring long-term treatment. Radiological features overlap partially with multiple sclerosis. However, corpus callosum and periventricular lesions are less frequent and thalamic and basal ganglia lesions far more 7. Nondemyelinating Inflammatory Diseases Nondemyelinating inflammatory diseases, such as venous vasculitis (e.g., Behcet disease) or connective tissue diseases (e.g., Sjögren s syndrome), sometimes involve the thalamus (Figure 15)[12, 13]. These lesions are most often hyperintense on T2 and FLAIR sequences and are sometimes enhanced on gadolinium-injected T1-weighted imaging. Thalamic involvement has been rarely observed in other autoimmune-related disorders such as Bickerstaff brainstem encephalitis or paraneoplastic encephalitis [14 16]. 8. Trauma 8.1. Diffuse Axonal Injury. Diffuse axonal injury typically involvesthecorpuscallosum,themidbrain,andthelobar white matter. Thalamus and basal ganglia involvement has been described less frequently (Figure16). Lesions, often multiple,arebestseenondwiandflairsequencesas hyperintense signal, with frequently associated hemorrhagic hypointense lesions on T2 -weightedimages(andevenbetter seen on SWI sequences). On ADC map, lesions may be hypointense indicating cytotoxic edema. Often associated radiological manifestations of head trauma (including epidural, subdural, subarachnoid, or intraventricular hemorrhage, contusion) are present. Diffuse axonal injury lesions tend to reduce in number and volumes over time. 9. Neoplastic 9.1. Glioblastoma Multiforme. Glioblastoma multiforme commonly affects the thalamus (Figure 17). The MRI signal is most typically heterogeneous, iso- to hypointense (especially when necrosis is present) on T1 sequences, and hyperintense on T2 and FLAIR imaging. Central necrosis, perilesional vasogenic (T2/FLAIR/ADC hyperintense) edema, and strong (solid, nodular, patchy, or closed-ring ) enhancement are typical. Sometimes, hemorrhage occurs inside the tumour Gliomatosis Cerebri. In gliomatosis cerebri, diffuse white matter infiltration (best seen as homogenous T2 and FLAIR
 and coronal FLAIR (b) imaging")

 and multiple lesions")
.")
10 10 Behavioural Neurology (a) (b) Figure 15: A patient with neuro-behcet showing a left-sided hyperintense lesion on axial T2-weighted (a) and coronal FLAIR (b) imaging involving the cerebellum, the midbrain, and the inferior part of the thalamus (arrows), the internal capsule, and the putamen. Figure 16: A patient after a major head trauma showing diffuse axonal injury with small hemorrhagic lesions in the medial part of both thalami (arrows, a) and multiple lesions near the cortico-subcortical junction (arrowheads, a and b) seen as hypointensity on gradient-echoweighted imaging (a and b). Multiple additional lesions can be seen on SWI imaging (c and d) demonstrating the superiority of SWI imaging in diffuse axonal injury.
 and coronal (b) FLAIR")






11 Behavioural Neurology 11 Figure 17: A patient with glioblastoma multiforme in the right thalamus seen as hyperintensity on axial (a) and coronal (b) FLAIR imaging, with gadolinium-enhancement on axial T1-weighted imaging (c). Figure18:Apatientwithgliomatosiscerebriinvolvingtheleftthalamus(arrows,aandb),thebilateralbasalganglia(aandb),theleftfrontal lobe (a, b, and c), and both temporal lobes, seen as hyperintensity on FLAIR sequences. hyperintensity, hypointense on T1-weighted imaging) involvingtwoormorelobesisobservedwithenlargementof the involved structure. Absent (or minimal) enhancement on gadolinium-injected T1-weighted imaging is typical. Associated thalamic, basal ganglia, and/or corpus callosum involvement is frequently observed (Figure 18) Lymphoma. Lymphoma often involves the periventricularwhitematter,thethalamus,thebasalganglia,andthe corpus callosum. Lymphomas are iso- or hypointense on unenhanced T1 sequences and hyperintense on T2/FLAIR imaging, with homogenous contrast enhancement in absence of central necrosis (Figure 19). In immunocompromised






12 12 Behavioural Neurology (e) Figure19:ApatientwithprimaryCNSlymphomainvolvingtheleft-sidedthalamus,theinternalcapsule,andtheanteriorpartofthecorpus callosum seen as hypointensity on axial unenhanced T1-weighted imaging (a), hyperintensity on coronal T2-weighted (b) and axial FLAIR (c) imaging, with multifocal enhancement on axial and coronal (e) gadolinium-enhanced T1-weighted imaging. (a) (b) Figure 20: A patient with Mycoplasma pneumoniae-related acute necrotizing encephalitis involving symmetrically the posterior part of the internal capsule (arrowheads) and the posterolateral portion of the thalamus (arrows) on both sides, seen as hyperintensity on both T2-weighted (a) and FLAIR (b) imaging. and rarely in nonimmunocompromised patients, contrast enhancement is rather peripheral than homogeneous or may be less evident or even absent. Surrounding edema as well as central necrosis may be seen in HIV-related lymphoma. In contrast to glioblastoma, there is less (or absent) peritumoral edema, and necrosis and hemorrhage are less common in lymphoma. Reduced diffusion has been reported occasionally. Lymphoma responds often dramatically (and frequently disappears on MRI) but temporarily to steroid treatment and radiation therapy.
 and restricted diffusion seen as hyperintensity on DWI imaging (b).")
 progressive multifocal leukoencephalopathy. 9.4. Metastasis.")

![Rare cases of infectious encephalitis involving the thalamus have been described. In these cases, thalamic lesions often coexist with more typical encephalitis lesions [17].](/docs-images/76/73587186/images/13-3.jpg "Lesions are most often hyperintense on T2 and FLAIR imagi")
,")
13 Behavioural Neurology 13 (a) (b) Figure 21: A patient with several brain abscesses involving the right thalamus (arrows) and the basal ganglia, with ring enhancement on gadolinium-enhanced T1-weighted imaging (a) and restricted diffusion seen as hyperintensity on DWI imaging (b). Figure 22: Diffuse white matter and associated left frontal cortical and left thalamic (arrows) involvement seen as hyperintensity on FLAIR (a), DWI (b), and ADC map (c) in a patient with natalizumab-related (for multiple sclerosis) progressive multifocal leukoencephalopathy Metastasis. Metastatic thalamic lesions are infrequent andaremostoftenseeninthepresenceofothermetastatic brain lesions. Lesion characteristics depend on the primary malignancy but are most often present with mass effect, surrounding edema, and contrast enhancement. 10. Infection Encephalitis. Rare cases of infectious encephalitis involving the thalamus have been described. In these cases, thalamic lesions often coexist with more typical encephalitis lesions [17]. Lesions are most often hyperintense on T2 and FLAIR imaging. Associated diffusion restriction, hemorrhage, or gadolinium-enhancement can be sometimes observed. In postinfectious (e.g., influenza A, parainfluenza, and Mycoplasma pneumoniae) acute necrotizing encephalopathy, often occurring in children, the thalamus is preferentially involved (often with associated brainstem, basal ganglia, cerebellum, or periventricular white matter lesions), seen as hyperintensity on T2-weighted and FLAIR imaging, and sometimes complicated with hemorrhage (Figure 20). Familial or recurrent cases of infection-triggered acute necrotizing encephalopathy can be caused by a RANBP2 gene mutation [18] Brain Abscess. Brain abscesses are usually located supratentorially at the gray-white matter junction with radiological characteristics varying with the stage of abscess development. Deep gray matter (including thalamic) involvement is sometimes observed (Figure21). Typical MRI characteristics include restricted diffusion on diffusion-weighted imaging (because of a high protein content), ring enhancement on gadolinium-enhanced T1-weighted imaging, and surrounding (T2 and FLAIR hyperintense) edema Progressive Multifocal Leukoencephalopathy. The JCvirus-related progressive multifocal leukoencephalopathy
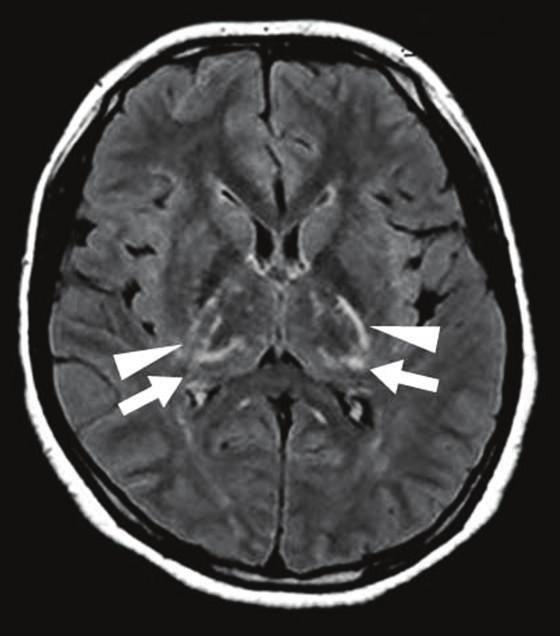
 hyperintensities on DWI (a) and FLAIR imaging (b) and in patient 2 bilateral posteromesial thalamic (arrowheads) and multifocal cortical")

. Lesions are often hyperintense on DWI.")

14 14 Behavioural Neurology Figure 23: Two different sporadic CJD patients (patient 1, a and b; patient 2, c and d) showing in patient 1 bilateral caudate nucleus and putaminal (arrows) and to a lesser degree posteromesial and pulvinar thalamic (arrowheads) hyperintensities on DWI (a) and FLAIR imaging (b) and in patient 2 bilateral posteromesial thalamic (arrowheads) and multifocal cortical (arrows) hyperintensities on DWI (c), seen as hypointensity on ADC map. Anterior predominance of the thalamic involvement can be seen in patient 2. typically occurs in immunocompromised patients and has a high mortality. These T2/FLAIR hyperintense and T1 hypointense lesions are uni- (especially in the early stage) or multifocal, usually without mass effect, and involve mainly the subcortical white matter although basal ganglia, thalamus and cortex involvement are sometimes encountered (Figure 22). Lesions are often hyperintense on DWI. Contrast enhancement is most often absent although faint enhancement can be sometimes observed at the periphery. Enhancement seems to be more frequent in natalizumabinduced progressive multifocal leukoencephalopathy cases. In these patients, small punctuate T2-hyperintense lesions in the immediate vicinity of the main lesions are often seen. T1-hyperintense signals can be found during and after the immune reconstitution inflammatory syndrome phase of progressive multifocal leukoencephalopathy. Surviving patients typically show profound atrophy of the involvedbrainstructuresinthechronicphaseofthedisease Creutzfeldt-Jakob Disease. Increased DWI and/or FLAIR signal in the basal ganglia, the thalamus and/or, the cerebral cortex is typical in Creutzfeldt-Jakob disease (Figure 23). MRI abnormalities, together with the presence of clinical signs, periodic sharp wave complexes on electroencephalogram, and protein in the cerebrospinal fluid, make a premortem diagnosis of probable sporadic Creutzfeldt-Jakob disease possible [19]. MRI signal changesinearlystagediseasecanbeabsentorverysubtle. DWIseemstobemoresensitivethanFLAIRsequencesto detect early signal changes [20]. In sporadic Creutzfeldt-Jakob disease, there is an anterior predominance of basal ganglia MRI changes (i.e., caudate nucleus is more frequently and more severely involved than the lentiform nucleus, whereas the thalamus is the least frequentlyandseverelyinvolveddeepgraymatterstructure). Deep grey matter signal changes are most often bilateral (asymmetricalorsymmetrical)althoughunilateralinvolvement can be seen. In case of thalamic involvement, signal
 associated with laminar necrosis in the")


 as the most hyperintense substructure (i.e., more hyperintense than the anterior part of the thalamus) on DWI/FLAIR imaging [21]. 11.")
15 Behavioural Neurology 15 Figure 24: T1-weighted MRI of patient 1 (a and b) after generalized status epilepticus and patient 2 (c and d) with a history of cerebellar astrocytoma treated by surgical resection and large field radiation therapy including the occipital lobes and both thalami showing laminar necrosis of both thalami (a and c, arrows) associated with laminar necrosis in the right-sided parietal cortex (b, arrows) and in the bilateral occipital cortex (c, arrowheads). Panel shows the cerebellar cavity due to cerebellar astrocytoma resection. abnormalities are most typically seen in the posteromesial portion. In young sporadic Creutzfeldt-Jakob patients, thalamic involvement is sometimes more severe than in the anterior basal ganglia structures. In these young patients, some authors report signal changes predominant in the anterior portion of the thalamus. In the variant Creutzfeldt-Jakob disease, the thalamus is the most frequently involved deep grey matter structure with typical bilateral symmetrical involvement (the so-called hockey-stick sign) with the posterior portion of the thalamus (pulvinar) as the most hyperintense substructure (i.e., more hyperintense than the anterior part of the thalamus) on DWI/FLAIR imaging [21]. 11. Laminar Necrosis Laminar necrosis typically involves the cortex but has also been reported in the basal ganglia and the thalami (Figure 24) [22]. Laminar necrosis appears as hyperintensity on unenhanced T1-weighted imaging. The proposed mechanism is cytolysis, necrosis, edema, followed by resorption, and phagocytosis of necrotic material, resulting in fat-laden macrophages depositions explaining probably the delayed T1- shortening on MRI. The grey matter (especially the cortex) is probably more vulnerable than the white matter, explaining why laminar necrosis most often involves the cortex and sometimes also the deep grey matter. The most frequently reported risk factors associated with laminar necrosis are ischemia/hypoxia, status epilepticus, metabolic changes, and radiation therapy. 12. Status Epilepticus ThalamicDWIhyperintenselesionsappearingintheregion of the pulvinar, ipsilateral to the epileptiform activity, can be seen after prolonged partial status epilepticus (Figure25). These peri-ictal diffusion abnormalities of the thalamus, likely the result of excessive activity in the thalamic nuclei
 all seen as hyperintensity on FLAIR imaging and in patient 2 (c and d) with generalized status epilepticus with also left occipitotemporal cortical signal")

![Conflict of Interests The authors declare that there is no conflict of interests regarding the publication of this paper. References [1] J. D.](/docs-images/76/73587186/images/16-2.jpg "Schmahmann, Vascular syndromes of the thalamus, Stroke,vol.34,pp.2264 2278,2003. [2] H. V. Vinters, Cerebral amyloid angiopathy. A critical review, Stroke,vol.18,pp.311 324,1987. [3] N. M.")

16 16 Behavioural Neurology Figure 25: Peri-ictal thalamic lesions (arrows) following status epilepticus in patient 1 (a and b) with partial occipital status epilepticus related to MELAS in the left occipital lobe (arrowheads on a and b) all seen as hyperintensity on FLAIR imaging and in patient 2 (c and d) with generalized status epilepticus with also left occipitotemporal cortical signal changes due to the seizures seen as hyperintensity on FLAIR imaging (c) and as hypointensity on ADC map. having reciprocal connections with the involved cortex, are associated with seizure origin in the posterior quadrant and with the presence of ipsilateral cortical laminar involvement on DWI [23]. Conflict of Interests The authors declare that there is no conflict of interests regarding the publication of this paper. References [1] J. D. Schmahmann, Vascular syndromes of the thalamus, Stroke,vol.34,pp ,2003. [2] H. V. Vinters, Cerebral amyloid angiopathy. A critical review, Stroke,vol.18,pp ,1987. [3] N. M. de Champfleur, C. Langlois, W. J. Ankenbrandt et al., Magnetic resonance imaging evaluation of cerebral cavernous malformations with susceptibility-weighted imaging, Neurosurgery,vol.68,pp ,2011. [4] D.F.Moore,F.Ye,R.Schiffmann,andJ.A.Butman, Increased signal intensity in the pulvinar on T1-weighted images: a pathognomonic MR imaging sign of Fabry disease, American Journal of Neuroradiology,vol.24,pp ,2003. [5] R. C. Reisin, C. Romero, C. Marchesoni et al., Brain MRI findings in patients with Fabry disease, Journal of the Neurological Sciences,vol.305,no.1,pp.41 44,2011. [6] A. Förster,I.Nölte, H. Wenz et al., Value of diffusion-weighted imaging in central pontine and extrapontine myelinolysis, Neuroradiology,vol.55,pp.49 56,2013. [7] M. C. Kruer, N. Boddaert, S. A. Schneider et al., Neuroimaging features of neurodegeneration with brain iron accumulation, American Journal of Neuroradiology,vol.33,pp ,2012.
17 Behavioural Neurology 17 [8]D.Renard,G.Castelnovo,P.J.Bousquetetal., BrainMRI findings in long-standing and disabling multiple sclerosis in 84 patients, Clinical Neurology and Neurosurgery,vol.112,pp , [9] B. P. Drayer, P. Burger, B. Hurwitz et al., Magnetic resonance imaging in multiple sclerosis: decreased signal in thalamus and putamen, Annals of Neurology, vol. 22, no. 4, pp , [10] J. Hagemeier, E. A. Yeh, M. H. Brown et al., Iron content of the pulvinar nucleus of the thalamus is increased in adolescent multiple sclerosis, Multiple Sclerosis, vol. 19, no. 5, pp , [11] K. H. Chan, C. T. Tse, C. P. Chung et al., Brain involvement in neuromyelitis optica spectrum disorders, Archives of Neurology,vol.68,pp ,2011. [12] H. Schmolck, Large thalamic mass due to neuro-behcet disease, Neurology,vol.65,no.3,article436,2005. [13]K.Matsuo,M.Saburi,H.Ishikawaetal., Sjögren syndrome presenting with encephalopathy mimicking Creutzfeldt-Jakob disease, Journal of the Neurological Sciences, vol. 326, pp , [14] B. A. Yaqub, S. M. Al-Deeb, A. K. Daif et al., Bickerstaff brainstem encephalitis. A grave non-demyelinating disease with benign prognosis, Journal of the Neurological Sciences, vol.96, pp.29 40,1990. [15] M. Mihara, S. Sugase, K. Konaka et al., The pulvinar sign in a case of paraneoplastic limbic encephalitis associated with non- Hodgkin's lymphoma, Journal of Neurology, Neurosurgery and Psychiatry, vol. 76, no. 6, pp , [16] M. Nakahama, T. Fukusato, R. Machinami et al., Paraneoplastic encephalomyelitis. An autopsy case with encephalitis principally confined to the thalamus and associated with pulmonary and gastric cancers, Acta Pathologica Japonica, vol. 40, no. 5, pp , [17] P. Navin, N. Delanty, P. Brennan et al., Herpes simplex virus encephalitis involving the right thalamus, BMJ Case Reports, [18] D. E. Neilson, M. D. Adams, C. M. Orr et al., Infectiontriggered familial or recurrent cases of acute necrotizing encephalopathy caused by mutations in a component of the nuclear pore, RANBP2, American Journal of Human Genetics, vol.84,no.1,pp.44 51,2009. [19] I. Zerr, K. Kallenberg, D. M. Summers et al., Updated clinical diagnostic criteria for sporadic Creutzfeldt-Jakob disease, Brain,vol.132,pp ,2009. [20] P. Vitali, E. Maccagnano, E. Caverzasi et al., Diffusionweighted MRI hyperintensity patterns differentiate CJD from other rapid dementias, Neurology, vol. 76, pp , [21] D. A. Collie, D. M. Summers, R. J. Sellar et al., Diagnosing variant Creutzfeldt-Jakob disease with the pulvinar sign: MR imaging findings in 86 neuropathologically confirmed cases, TheAmericanJournalofNeuroradiology,vol.24,no.8,pp , [22] D.Renard,G.Taieb,A.LeFloch,andC.Campello, Thalamic laminar necrosis, Acta Neurologica Belgica, vol. 113, no. 2, pp , [23] A. M. Katramados, D. Burdette, S. C. Patel et al., Periictal diffusion abnormalities of the thalamus in partial status epilepticus, Epilepsia, vol. 50, no. 2, pp , 2009.

















18 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Journal of Diabetes Research International Journal of Journal of Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Journal of Obesity Journal of Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Journal of Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
MRI OF THE THALAMUS. Mohammed J. Zafar, MD, FAAN Kalamazoo, MI
 1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing
1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing
SWI including phase and magnitude images
 On-line Table: MRI imaging recommendation and summary of key features Sequence Pathologies Visible Key Features T1 volumetric high-resolution whole-brain reformatted in axial, coronal, and sagittal planes
On-line Table: MRI imaging recommendation and summary of key features Sequence Pathologies Visible Key Features T1 volumetric high-resolution whole-brain reformatted in axial, coronal, and sagittal planes
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Interactive Cases: Demyelinating Diseases and Mimics. Disclosures. Case 1 25 yo F with nystagmus; look for tumor 4/14/2017
 Interactive Cases: Demyelinating Diseases and Mimics Disclosures None Brad Wright, MD 27 March 2017 Case 1 25 yo F with nystagmus; look for tumor What do you suspect? A. Demyelinating disease B. Malignancy
Interactive Cases: Demyelinating Diseases and Mimics Disclosures None Brad Wright, MD 27 March 2017 Case 1 25 yo F with nystagmus; look for tumor What do you suspect? A. Demyelinating disease B. Malignancy
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Index. aneurysm, 92 carotid occlusion, 94 ICA stenosis, 95 intracranial, 92 MCA, 94
 A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
brain MRI for neuropsychiatrists: what do you need to know
 brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
brain MRI for neuropsychiatrists: what do you need to know Christoforos Stoupis, MD, PhD Department of Radiology, Spital Maennedorf, Zurich & Inselspital, University of Bern, Switzerland c.stoupis@spitalmaennedorf.ch
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT
 Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Disclosure. + Outline. Case-based approach to neurological emergencies that might present to the ED
 Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
HYPERTENSIVE ENCEPHALOPATHY
 HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Medical Neuroscience Tutorial Notes
 Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Case 9511 Hypertensive microangiopathy
 Case 9511 Hypertensive microangiopathy Schepers S, Barthels C Section: Neuroradiology Published: 2011, Nov. 3 Patient: 67 year(s), male Authors' Institution Department of Radiology, Jessa ziekenhuis campus
Case 9511 Hypertensive microangiopathy Schepers S, Barthels C Section: Neuroradiology Published: 2011, Nov. 3 Patient: 67 year(s), male Authors' Institution Department of Radiology, Jessa ziekenhuis campus
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
MRI and differential diagnosis in patients suspected of having MS
 Andrea Falini Italy MRI and differential diagnosis in patients suspected of having MS IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Outline of presentation - Diagnostic criteria
Andrea Falini Italy MRI and differential diagnosis in patients suspected of having MS IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Outline of presentation - Diagnostic criteria
Cerebral malaria: MR imaging spectrum
 Cerebral malaria: MR imaging spectrum Poster No.: C-2705 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: P. S. Naphade, M. D. Agrawal, S. S. Sankhe, K. M. Siva, B. K. Jain; Mumbai/IN
Cerebral malaria: MR imaging spectrum Poster No.: C-2705 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: P. S. Naphade, M. D. Agrawal, S. S. Sankhe, K. M. Siva, B. K. Jain; Mumbai/IN
EEG IN FOCAL ENCEPHALOPATHIES: CEREBROVASCULAR DISEASE, NEOPLASMS, AND INFECTIONS
 246 Figure 8.7: FIRDA. The patient has a history of nonspecific cognitive decline and multiple small WM changes on imaging. oligodendrocytic tumors of the cerebral hemispheres (11,12). Electroencephalogram
246 Figure 8.7: FIRDA. The patient has a history of nonspecific cognitive decline and multiple small WM changes on imaging. oligodendrocytic tumors of the cerebral hemispheres (11,12). Electroencephalogram
Imaging in a confused patient: Infections and Inflammation
 American Society of Neuroimaging Imaging in a confused patient: Infections and Inflammation January 21, 2017 Los Angeles, California Joshua P. Klein, MD, PhD, FANA, FAAN, FASN Chief, Division of Hospital
American Society of Neuroimaging Imaging in a confused patient: Infections and Inflammation January 21, 2017 Los Angeles, California Joshua P. Klein, MD, PhD, FANA, FAAN, FASN Chief, Division of Hospital
Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum
 Case Reports in Pathology Volume 2012, Article ID 718651, 4 pages doi:10.1155/2012/718651 Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum Jesús Vaquero, 1,
Case Reports in Pathology Volume 2012, Article ID 718651, 4 pages doi:10.1155/2012/718651 Case Report Complex Form Variant of Dysembryoplastic Neuroepithelial Tumor of the Cerebellum Jesús Vaquero, 1,
Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male
 Case Reports in Radiology Volume 2016, Article ID 6434623, 4 pages http://dx.doi.org/10.1155/2016/6434623 Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male Jordan Nepute,
Case Reports in Radiology Volume 2016, Article ID 6434623, 4 pages http://dx.doi.org/10.1155/2016/6434623 Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male Jordan Nepute,
Attenuation value in HU From -500 To HU From -10 To HU From 60 To 90 HU. From 200 HU and above
 Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
OBJECTIVES. At the end of the lecture, students should be able to: List the cerebral arteries.
 DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
Demyelinating Diseases of the Brain
 Department of Radiology University of California San Diego Demyelinating Diseases of the Brain John R. Hesselink, M.D. T1-Weighted Images Normal White Matter Contents Axons with envelope of myelin Neuroglia
Department of Radiology University of California San Diego Demyelinating Diseases of the Brain John R. Hesselink, M.D. T1-Weighted Images Normal White Matter Contents Axons with envelope of myelin Neuroglia
Discovering the hippocampus with cranial-ct.
 Discovering the hippocampus with cranial-ct. Poster No.: C-0378 Congress: ECR 2018 Type: Educational Exhibit Authors: F. Pozo Piñon, A. B. Barba Arce, E. herrera romero, V. 1 2 3 1 3 3 Fernández Lobo,
Discovering the hippocampus with cranial-ct. Poster No.: C-0378 Congress: ECR 2018 Type: Educational Exhibit Authors: F. Pozo Piñon, A. B. Barba Arce, E. herrera romero, V. 1 2 3 1 3 3 Fernández Lobo,
A pictorial review of neurological complications of systemic lupus erythematosus and antiphospholipid syndrome
 A pictorial review of neurological complications of systemic lupus erythematosus and antiphospholipid syndrome Poster No.: C-2780 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: E. Tavernaraki,
A pictorial review of neurological complications of systemic lupus erythematosus and antiphospholipid syndrome Poster No.: C-2780 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: E. Tavernaraki,
NEURO IMAGING OF ACUTE STROKE
 1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
1 1 NEURO IMAGING OF ACUTE STROKE ALICIA RICHARDSON, MSN, RN, ACCNS-AG, ANVP-BC WENDY SMITH, MA, RN, MBA, SCRN, FAHA LYNN HUNDLEY, APRN, CNRN, CCNS, ANVP-BC 2 2 1 DISCLOSURES Alicia Richardson: Stryker
Structural and functional imaging for the characterization of CNS lymphomas
 Structural and functional imaging for the characterization of CNS lymphomas Cristina Besada Introduction A few decades ago, Primary Central Nervous System Lymphoma (PCNSL) was considered as an extremely
Structural and functional imaging for the characterization of CNS lymphomas Cristina Besada Introduction A few decades ago, Primary Central Nervous System Lymphoma (PCNSL) was considered as an extremely
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Case 9 10/29/2018. CJD (Creutzfeldt -Jakob Disease) CJD (Creutzfeldt -Jakob Disease) CJD (Creutzfeldt -Jakob Disease)
 CJD (Creutzfeldt -Jakob Disease) CJD (Creutzfeldt -Jakob Disease)") CJD (Creutzfeldt -Jakob Disease) Rare fatal neurodegen dz caused by infectious protein Prion (lacks nucleic acid)- causes spongiform changes of the brain and neuronal death. 4 types: scjd- 85% of cases
CJD (Creutzfeldt -Jakob Disease) Rare fatal neurodegen dz caused by infectious protein Prion (lacks nucleic acid)- causes spongiform changes of the brain and neuronal death. 4 types: scjd- 85% of cases
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
1 MS Lesions in T2-Weighted Images
 1 MS Lesions in T2-Weighted Images M.A. Sahraian, E.-W. Radue 1.1 Introduction Multiple hyperintense lesions on T2- and PDweighted sequences are the characteristic magnetic resonance imaging (MRI) appearance
1 MS Lesions in T2-Weighted Images M.A. Sahraian, E.-W. Radue 1.1 Introduction Multiple hyperintense lesions on T2- and PDweighted sequences are the characteristic magnetic resonance imaging (MRI) appearance
Cerebrovascular diseases-2
 Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Pediatric MS MRI Study Methodology
 General Pediatric MS MRI Study Methodology SCAN PREPARATION axial T2-weighted scans and/or axial FLAIR scans were obtained for all subjects when available, both T2 and FLAIR scans were scored. In order
General Pediatric MS MRI Study Methodology SCAN PREPARATION axial T2-weighted scans and/or axial FLAIR scans were obtained for all subjects when available, both T2 and FLAIR scans were scored. In order
Bilateral thalamic infarcts due to occlusion of the Artery of Percheron and discussion of the differential diagnosis of bilateral thalamic lesions
 Bilateral thalamic infarcts due to occlusion of the Artery of Percheron and discussion of the differential diagnosis of bilateral thalamic lesions Eva Guy Rodriguez 1, Lee Jane A 1 1. Department of Radiology,
Bilateral thalamic infarcts due to occlusion of the Artery of Percheron and discussion of the differential diagnosis of bilateral thalamic lesions Eva Guy Rodriguez 1, Lee Jane A 1 1. Department of Radiology,
White matter diseases affecting the corpus callosum; demyelinating and metabolic diseases
 White matter diseases affecting the corpus callosum; demyelinating and metabolic diseases Poster No.: C-0199 Congress: ECR 2011 Type: Educational Exhibit Authors: J. H. Yoo; Seoul/KR Keywords: Neuroradiology
White matter diseases affecting the corpus callosum; demyelinating and metabolic diseases Poster No.: C-0199 Congress: ECR 2011 Type: Educational Exhibit Authors: J. H. Yoo; Seoul/KR Keywords: Neuroradiology
Prion diseases or transmissible spongiform encephalopathies (TSEs)
") Prion diseases or transmissible spongiform encephalopathies (TSEs) rare progressive neurodegenerative disorders that affect both humans and animals. They are distinguished by long incubation periods, characteristic
Prion diseases or transmissible spongiform encephalopathies (TSEs) rare progressive neurodegenerative disorders that affect both humans and animals. They are distinguished by long incubation periods, characteristic
RINGS N THINGS: Imaging Patterns in Differential Diagnosis. Anne G. Osborn, M.D.
 RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
Laura Tormoehlen, M.D. Neurology and EM-Toxicology Indiana University
 Laura Tormoehlen, M.D. Neurology and EM-Toxicology Indiana University Disclosures! No conflicts of interest to disclose Neuroimaging 101! Plain films! Computed tomography " Angiography " Perfusion! Magnetic
Laura Tormoehlen, M.D. Neurology and EM-Toxicology Indiana University Disclosures! No conflicts of interest to disclose Neuroimaging 101! Plain films! Computed tomography " Angiography " Perfusion! Magnetic
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Differential Diagnosis for Bilateral Abnormalities. and Thalamus 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. NEUROLOGIC/HEAD AND
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. NEUROLOGIC/HEAD AND
Role of imaging (images) in my practice. Dr P Senthur Nambi Consultant Infectious Diseases
 in my practice. Dr P Senthur Nambi Consultant Infectious Diseases") Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Patient with vertigo, dizziness and depression
 Clinical Case - Test Yourself Neuro/Head and Neck Radiology Patient with vertigo, dizziness and depression Michael Mantatzis, Paraskevi Argyropoulou, Panos Prassopoulos Radiology Department, Democritus
Clinical Case - Test Yourself Neuro/Head and Neck Radiology Patient with vertigo, dizziness and depression Michael Mantatzis, Paraskevi Argyropoulou, Panos Prassopoulos Radiology Department, Democritus
Masses of the Corpus Callosum
 Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
Magnetic Resonance Imaging for Neurological Conditions. Lawrance Yip Department of Radiology Queen Mary Hospital
 Magnetic Resonance Imaging for Neurological Conditions Lawrance Yip Department of Radiology Queen Mary Hospital Outline Strength and limitations of MRI for neurological conditions MR Imaging techniques
Magnetic Resonance Imaging for Neurological Conditions Lawrance Yip Department of Radiology Queen Mary Hospital Outline Strength and limitations of MRI for neurological conditions MR Imaging techniques
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution
 CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution Poster No.: C-2723 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro
CT and MR findings of systemic lupus erythematosus involving the brain: Differential diagnosis based on lesion distribution Poster No.: C-2723 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro
Case Report Ischemic Stroke of the Artery of Percheron with Normal Initial MRI: A Case Report
 Case Reports in Medicine Volume 2010, Article ID 425734, 4 pages doi:10.1155/2010/425734 Case Report Ischemic Stroke of the Artery of Percheron with Normal Initial MRI: A Case Report Guillaume Cassourret,
Case Reports in Medicine Volume 2010, Article ID 425734, 4 pages doi:10.1155/2010/425734 Case Report Ischemic Stroke of the Artery of Percheron with Normal Initial MRI: A Case Report Guillaume Cassourret,
Diffusion-Weighted and Conventional MR Imaging Findings of Neuroaxonal Dystrophy
 AJNR Am J Neuroradiol 25:1269 1273, August 2004 Diffusion-Weighted and Conventional MR Imaging Findings of Neuroaxonal Dystrophy R. Nuri Sener BACKGROUND AND PURPOSE: Neuroaxonal dystrophy is a rare progressive
AJNR Am J Neuroradiol 25:1269 1273, August 2004 Diffusion-Weighted and Conventional MR Imaging Findings of Neuroaxonal Dystrophy R. Nuri Sener BACKGROUND AND PURPOSE: Neuroaxonal dystrophy is a rare progressive
Benign brain lesions
 Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
Atypical Unilateral Posterior Reversible Encephalopathy Syndrome Mimicking a Middle Cerebral Artery Infarction
 Case Report Neuroimaging and Head & Neck http://dx.doi.org/10.3348/kjr.2015.16.5.1104 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2015;16(5):1104-1108 Atypical Unilateral Posterior Reversible Encephalopathy
Case Report Neuroimaging and Head & Neck http://dx.doi.org/10.3348/kjr.2015.16.5.1104 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2015;16(5):1104-1108 Atypical Unilateral Posterior Reversible Encephalopathy
NEURORADIOLOGY-NEUROPATHOLOGY CONFERENCE
 THE UNIVERSITY OF NORTH CAROLINA at CHAPEL HILL SEPTEMBER 2013 NEURORADIOLOGY-NEUROPATHOLOGY CONFERENCE Claudia da Costa Leite, MD, PhD Thomas Bouldin, MD CASE 1 6 y-o female with headaches and vomiting
THE UNIVERSITY OF NORTH CAROLINA at CHAPEL HILL SEPTEMBER 2013 NEURORADIOLOGY-NEUROPATHOLOGY CONFERENCE Claudia da Costa Leite, MD, PhD Thomas Bouldin, MD CASE 1 6 y-o female with headaches and vomiting
Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy
 Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Role of MRI in acute disseminated encephalomyelitis
 Original Research Article Role of MRI in acute disseminated encephalomyelitis Shashvat Modiya 1*, Jayesh Shah 2, C. Raychaudhuri 3 1 1 st year resident, 2 Associate Professor, 3 HOD and Professor Department
Original Research Article Role of MRI in acute disseminated encephalomyelitis Shashvat Modiya 1*, Jayesh Shah 2, C. Raychaudhuri 3 1 1 st year resident, 2 Associate Professor, 3 HOD and Professor Department
Blood Supply of the CNS
 Blood Supply of the CNS Lecture Objectives Describe the four arteries supplying the CNS. Follow up each artery to its destination. Describe the circle of Willis and its branches. Discuss the principle
Blood Supply of the CNS Lecture Objectives Describe the four arteries supplying the CNS. Follow up each artery to its destination. Describe the circle of Willis and its branches. Discuss the principle
Chapter 3. Structure and Function of the Nervous System. Copyright (c) Allyn and Bacon 2004
 Allyn and Bacon 2004") Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
A Rare Case Report of Unilateral Involvement of Basal Ganglia and Thalamus in a Case of Hypoxic Brain Injury
 A Rare Case Report of Unilateral Involvement of Basal Ganglia and Thalamus in a Case of Hypoxic Brain Injury Article by Sunil chowdary Minnekanti, Monika sai paida, Sushant Duddala, Nerin Duddala, Snigdha
A Rare Case Report of Unilateral Involvement of Basal Ganglia and Thalamus in a Case of Hypoxic Brain Injury Article by Sunil chowdary Minnekanti, Monika sai paida, Sushant Duddala, Nerin Duddala, Snigdha
IV. Cerebrovascular diseases
 IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
Common and uncommon differential diagnosis of cerebral microhemorrhages
 Common and uncommon differential diagnosis of cerebral microhemorrhages Poster No.: C-0261 Congress: ECR 2014 Type: Educational Exhibit Authors: T. C. Rodrigues 1, S. B. Bergamaschi 1, C. F. R. B. Milito
Common and uncommon differential diagnosis of cerebral microhemorrhages Poster No.: C-0261 Congress: ECR 2014 Type: Educational Exhibit Authors: T. C. Rodrigues 1, S. B. Bergamaschi 1, C. F. R. B. Milito
10/3/2016. T1 Anatomical structures are clearly identified, white matter (which has a high fat content) appears bright.
 appears bright.") H2O -2 atoms of Hydrogen, 1 of Oxygen Hydrogen just has one single proton and orbited by one single electron Proton has a magnetic moment similar to the earths magnetic pole Also similar to earth in that
H2O -2 atoms of Hydrogen, 1 of Oxygen Hydrogen just has one single proton and orbited by one single electron Proton has a magnetic moment similar to the earths magnetic pole Also similar to earth in that
Neuropathology lecture series. III. Neuropathology of Cerebrovascular Disease. Physiology of cerebral blood flow
 Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Pediatric CNS Tumors. Disclosures. Acknowledgements. Introduction. Introduction. Posterior Fossa Tumors. Whitney Finke, MD
 Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Toxins in Brain! Magnetic Resonance (MR) Imaging of Toxic Leukoencephalopathy A Pictorial Essay
 Imaging of Toxic Leukoencephalopathy A Pictorial Essay") Signature: Pol J Radiol, 2017; 82: 311-319 DOI: 10.12659/PJR.901791 REVIEW ARTICLE Received: 2016.10.02 Accepted: 2016.10.11 Published: 2017.06.13 Authors Contribution: A Study Design B Data Collection
Signature: Pol J Radiol, 2017; 82: 311-319 DOI: 10.12659/PJR.901791 REVIEW ARTICLE Received: 2016.10.02 Accepted: 2016.10.11 Published: 2017.06.13 Authors Contribution: A Study Design B Data Collection
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
Keep Imaging Simple: An Introduction To Neuroimaging
 Keep Imaging Simple: An Introduction To Neuroimaging Meghan Elkins, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is
Keep Imaging Simple: An Introduction To Neuroimaging Meghan Elkins, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is
IMAGING OF INTRACRANIAL INFECTIONS
 IMAGING OF INTRACRANIAL INFECTIONS Dr Carolina Kachramanoglou LYSHOLM DEPARTMENT OF NEURORADIOLOGY NATIONAL HOSPITAL FOR NEUROLOGY AND NEUROSURGERY Plan Introduce MR sequences that are useful in the diagnosis
IMAGING OF INTRACRANIAL INFECTIONS Dr Carolina Kachramanoglou LYSHOLM DEPARTMENT OF NEURORADIOLOGY NATIONAL HOSPITAL FOR NEUROLOGY AND NEUROSURGERY Plan Introduce MR sequences that are useful in the diagnosis
Patologie infiammatorie encefaliche e midollari
 Patologie infiammatorie encefaliche e midollari Maria Laura Stromillo Department of Medicine, Surgery and Neuroscience Inflammatory disorders of the CNS NMOSD ADEM Multiple Sclerosis Neuro-Myelitis Optica
Patologie infiammatorie encefaliche e midollari Maria Laura Stromillo Department of Medicine, Surgery and Neuroscience Inflammatory disorders of the CNS NMOSD ADEM Multiple Sclerosis Neuro-Myelitis Optica
Creutzfeldt-Jakob Disease: Spectrum of Magnetic Ressonance Imaging findings
 Creutzfeldt-Jakob Disease: Spectrum of Magnetic Ressonance Imaging findings Poster No.: C-0486 Congress: ECR 2014 Type: Educational Exhibit Authors: F. M. P. D. Carvalho, E. Rosado, J. Marçalo, M. Bousende,
Creutzfeldt-Jakob Disease: Spectrum of Magnetic Ressonance Imaging findings Poster No.: C-0486 Congress: ECR 2014 Type: Educational Exhibit Authors: F. M. P. D. Carvalho, E. Rosado, J. Marçalo, M. Bousende,
Neuroradiology of AIDS
 Neuroradiology of AIDS Frank Minja,, HMS IV Gillian Lieberman MD September 2002 AIDS 90% of HIV patients have CNS involvement 1 10% of AIDS patients present first with neurological symptoms 2 73-80% of
Neuroradiology of AIDS Frank Minja,, HMS IV Gillian Lieberman MD September 2002 AIDS 90% of HIV patients have CNS involvement 1 10% of AIDS patients present first with neurological symptoms 2 73-80% of
An Approach. to Brain. Infection. 37F found down. Disclosures. Approach to CNS Infection. Objectives. Parenchymal. None.
 An Approach Disclosures to Brain None. Infection Jason Shewchuk, MD Clinical Associate Professor Head of Neuroradiology UBC European Course in Neuroradiology 2018 Objectives Following this session the
An Approach Disclosures to Brain None. Infection Jason Shewchuk, MD Clinical Associate Professor Head of Neuroradiology UBC European Course in Neuroradiology 2018 Objectives Following this session the
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Central Variant Posterior Reversible Encephalopathy Syndrome: A Masquerader with Brainstem and Basal Ganglia
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Central Variant Posterior Reversible Encephalopathy Syndrome: A Masquerader with Brainstem and Basal Ganglia
Applicable Neuroradiology
 For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Case Report Traumatic Haemorrhagic Cervical Lymphadenopathy with Underlying Infectious Mononucleosis
 Hindawi Case Reports in Radiology Volume 2017, Article ID 3097414, 4 pages https://doi.org/10.1155/2017/3097414 Case Report Traumatic Haemorrhagic Cervical Lymphadenopathy with Underlying Infectious Mononucleosis
Hindawi Case Reports in Radiology Volume 2017, Article ID 3097414, 4 pages https://doi.org/10.1155/2017/3097414 Case Report Traumatic Haemorrhagic Cervical Lymphadenopathy with Underlying Infectious Mononucleosis
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
Clinics in diagnostic imaging (175)
") Singapore Med J 2017; 58(3): 121-125 doi: 10.11622/smedj.2017017 CMEArticle Clinics in diagnostic imaging (175) Vijay Krishnan 1, MD, FRCR, Tze Chwan Lim 1, MBBS, FRCR, Francis Cho Hao Ho 2, MBBS, FRANZCR,
Singapore Med J 2017; 58(3): 121-125 doi: 10.11622/smedj.2017017 CMEArticle Clinics in diagnostic imaging (175) Vijay Krishnan 1, MD, FRCR, Tze Chwan Lim 1, MBBS, FRCR, Francis Cho Hao Ho 2, MBBS, FRANZCR,
Case Report Paroxysmal Amnesia Attacks due to Hashimoto s Encephalopathy
 Case Reports in Medicine Volume 2016, Article ID 1267192, 4 pages http://dx.doi.org/10.1155/2016/1267192 Case Report Paroxysmal Amnesia Attacks due to Hashimoto s Encephalopathy Pelin Nar Senol, Aylin
Case Reports in Medicine Volume 2016, Article ID 1267192, 4 pages http://dx.doi.org/10.1155/2016/1267192 Case Report Paroxysmal Amnesia Attacks due to Hashimoto s Encephalopathy Pelin Nar Senol, Aylin
Lab 2. we will look into several angled horizontal sections ( orbitomeatal plane ) i.e passing from the orbit into the ear
 i.e passing from the orbit into the ear") we will look into several angled horizontal sections ( orbitomeatal plane ) i.e passing from the orbit into the ear Figure I page 76 : looking at the key on the left side this section passed through the
we will look into several angled horizontal sections ( orbitomeatal plane ) i.e passing from the orbit into the ear Figure I page 76 : looking at the key on the left side this section passed through the
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
intracranial anomalies
 Chapter 5: Fetal Central Nervous System 84 intracranial anomalies Hydrocephaly Dilatation of ventricular system secondary to an increase in the amount of CSF. Effects of hydrocephalus include flattening
Chapter 5: Fetal Central Nervous System 84 intracranial anomalies Hydrocephaly Dilatation of ventricular system secondary to an increase in the amount of CSF. Effects of hydrocephalus include flattening
Biological Bases of Behavior. 3: Structure of the Nervous System
 Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
Outline. Neuroradiology. Diffusion Imaging in. Clinical Applications of. Basics of Diffusion Imaging. Basics of Diffusion Imaging
 Clinical Applications of Diffusion Imaging in Neuroradiology No disclosures Stephen F. Kralik Assistant Professor of Radiology Indiana University School of Medicine Department of Radiology and Imaging
Clinical Applications of Diffusion Imaging in Neuroradiology No disclosures Stephen F. Kralik Assistant Professor of Radiology Indiana University School of Medicine Department of Radiology and Imaging
b. The groove between the two crests is called 2. The neural folds move toward each other & the fuse to create a
 Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Introduction to the Central Nervous System: Internal Structure
 Introduction to the Central Nervous System: Internal Structure Objective To understand, in general terms, the internal organization of the brain and spinal cord. To understand the 3-dimensional organization
Introduction to the Central Nervous System: Internal Structure Objective To understand, in general terms, the internal organization of the brain and spinal cord. To understand the 3-dimensional organization
Review Article Differentiating between Hemorrhagic Infarct and Parenchymal Intracerebral Hemorrhage
 Hindawi Publishing Corporation Radiology Research and Practice Volume 2012, Article ID 475497, 11 pages doi:10.1155/2012/475497 Review Article Differentiating between Hemorrhagic Infarct and Parenchymal
Hindawi Publishing Corporation Radiology Research and Practice Volume 2012, Article ID 475497, 11 pages doi:10.1155/2012/475497 Review Article Differentiating between Hemorrhagic Infarct and Parenchymal
TRANSVERSE SECTION PLANE Scalp 2. Cranium. 13. Superior sagittal sinus
 TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
Pathologic Analysis of CNS Surgical Specimens
 2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
Zhenyu Jia, MD,* Wasif Mohammed, MD,* Yiru Qiu, MD, Xunning Hong, MD,* and Haibin Shi, MD, PhD*
 Hypertension Increases the Risk of Cerebral Microbleed in the Territory of Posterior Cerebral Artery: A Study of the Association of Microbleeds Categorized on a Basis of Vascular Territories and Cardiovascular
Hypertension Increases the Risk of Cerebral Microbleed in the Territory of Posterior Cerebral Artery: A Study of the Association of Microbleeds Categorized on a Basis of Vascular Territories and Cardiovascular
Diffusion-weighted magnetic resonance imaging (MRI) allows for tissue
 allows for tissue") MAGNETIC RESONANCE IMAGING / IMAGERIE PAR RÉSONANCE MAGNÉTIQUE Nonischemic causes of hyperintense signals on diffusion-weighted magnetic resonance images: a pictorial essay Jeffrey M. Hinman, MD; James
MAGNETIC RESONANCE IMAGING / IMAGERIE PAR RÉSONANCE MAGNÉTIQUE Nonischemic causes of hyperintense signals on diffusion-weighted magnetic resonance images: a pictorial essay Jeffrey M. Hinman, MD; James
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
Automated Identification of Neoplasia in Diagnostic Imaging text reports
 Automated Identification of Neoplasia in Diagnostic Imaging text reports "This work has been funded in whole or in part with Federal funds from the National Cancer Institute, National Institutes of Health,
Automated Identification of Neoplasia in Diagnostic Imaging text reports "This work has been funded in whole or in part with Federal funds from the National Cancer Institute, National Institutes of Health,
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
CNS Imaging. Dr Amir Monir, MD. Lecturer of radiodiagnosis.
 CNS Imaging Dr Amir Monir, MD Lecturer of radiodiagnosis www.dramir.net Types of radiological examinations you know Plain X ray X ray with contrast GIT : barium (swallow, meal, follow through, enema) ERCP
CNS Imaging Dr Amir Monir, MD Lecturer of radiodiagnosis www.dramir.net Types of radiological examinations you know Plain X ray X ray with contrast GIT : barium (swallow, meal, follow through, enema) ERCP
Osmotic Demyelination Syndrome Case Report POPOVA RD, KALCHEV EB, VALCHEV GN, KALOYANOVA DV, TENEVA TG, BALEV BD
 Osmotic Demyelination Syndrome Case Report POPOVA RD, KALCHEV EB, VALCHEV GN, KALOYANOVA DV, TENEVA TG, BALEV BD Once upon a time on a Saturday shift u An emergency head CT scan was ordered from the ICU
Osmotic Demyelination Syndrome Case Report POPOVA RD, KALCHEV EB, VALCHEV GN, KALOYANOVA DV, TENEVA TG, BALEV BD Once upon a time on a Saturday shift u An emergency head CT scan was ordered from the ICU