ABDOMINAL DIFFUSION WEIGHTED MR
|
|
|
- Muriel Harrington
- 5 years ago
- Views:
Transcription

1 ABDOMINAL DIFFUSION WEIGHTED MR Frank Miller, M.D. FACR Professor of Radiology Chief, Body Imaging Section Medical Director, MR Imaging Northwestern University Feinberg School of Medicine
2 DISCLOSURES No disclosures related to presentation
3 OBJECTIVES Demonstrate utility of DWI in abdomen Show advantages and limitations of DWI
4 ORGANS Liver Pancreas Adrenal Kidney Lymph nodes/peritoneum Problem-based approach and not able to cover nearly everything
5 DIFFUSION WEIGHTED IMAGING Used in neuroimaging for many years Used routinely in our body MR imaging practice Recommend starting DWI for abdominal applications if not already doing it Need to recognize the strengths and limitations
6 DIFFUSION WEIGHTED IMAGING Does not require contrast helpful when renal dysfunction and concern of NSF or allergy Relatively quick to perform Provides functional information in addition to anatomic Improved lesion conspicuity-better than T2 Best sequence for lymph node detection Some HCC (especially infiltrative lesions) and metastases better seen on DWI than on contrast-enhanced MR

7 IMPROVED CONSPICUITY: LIVER PECOMA b50 b500 ADC T1WI post


8 SOMETIMES LESS CONSPICUOUS HCC Arterial phase Delayed b500 ADC
9 DWI Normal cells have water mobility differences Theory-tumors less water mobility and therefore restricted diffusion: lower ADC Apparent diffusion coefficient (ADC): measure of diffusion which removes the T2 effects lesion which is bright on DWI may relate to T2 shine through and are bright on ADC map unlike true diffusion which is dark on ADC
10 WHICH B VALUE SHOULD YOU USE? b value-strength of diffusion sensitizing gradient No consensus on b values for abdomen-probably best between 0 and 1000 s/mm 2 At least 2 b values if calculating ADC We use 50, 400/500 and 800 s/mm 2
: black blood images b>50 to minimize capillary perfusion b50")
11 LOW B VALUE IMAGES SEC/MM 2 Low b value: less diffusion gradient but higher SNR Signal loss in highly mobile water molecules (e.g. vessels): black blood images b>50 to minimize capillary perfusion b50

12 High b value IMAGES Higher b values-more diffusion component but when too high have lower signal to noise Highly cellular tissues such as tumors-water is restricted Additional b values for research or more accurate ADC b1000


 / (b 1 - b 0 ) b-values")
13 Log (Relative SI) ADC MAP b50 b500 Slope of line represents ADC: relative signal intensity on y axis and b value on x axis b1000 ADC = log(s 0 / S 1 ) / (b 1 - b 0 ) b-values (s/mm 2 )
14 DIFFUSION MR Theory: malignant lesions have restricted diffusion and are bright while benign lesions do not although in practice not always true Diffusion MR only adds few minutes in total

15

16 T1 FS POST GAD T2
17 T1 FS POST GAD Better than T2 b500 Diffusion

18 T1 FS POST GAD Restricted ADC
19 PHYSIOLOGIC RESTRICTED DIFFUSION Impeded water diffusion from high cellularity Spleen Adrenal Lymph nodes Kidneys Testes Penis Hematopoietic bone marrow
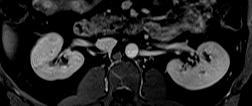
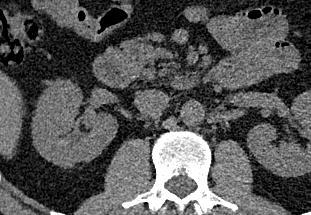
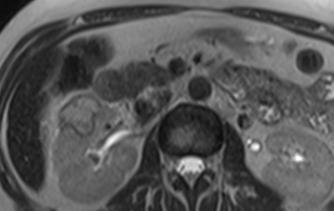
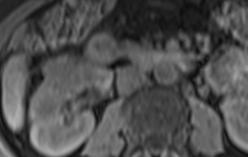
20 DWI OF KIDNEY, ADRENAL AND SPLEEN Ciliated hepatic foregut cyst LA S LA S LA S LK LK LK B50 B500 B800 LA = left adrenal LK = left kidney S = spleen ADC


21 IMPROVED CONSPICUITY: UNKNOWN PRIMARY HASTE T2 T1 post B500 ADC
22 QUALITATIVE AND QUANTITATIVE EVALUATION OF DWI Qualitative-observe visually based on DWI and ADC map use routinely more than quantitatively High signal on high b value images (dark ADC map) suggest restricted diffusion generally from greater cellularity and integrity of cell membranes Tumor with necrosis, hypocellular or cystic tumors restrict less
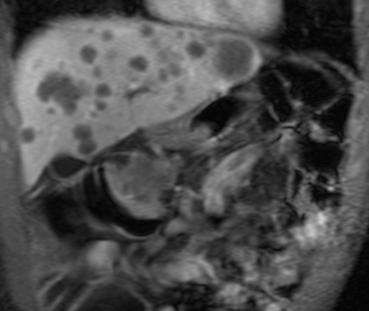
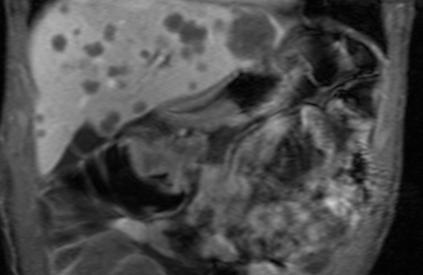
23 DIFFUSION MRI-LIVER We use DWI routinely in all liver MR cases Helpful in detection of hepatic lesions similar to bone scan or PET scan detect additional lesions directs to re-review the conventional imaging to identify lesions Helpful but has limitations in characterization of hepatic lesions can confirm true lesion and not pseudolesion


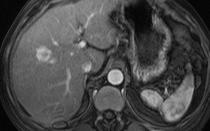
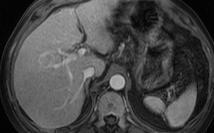
24 CARCINOID METASTASES AND LIVER CYST ARTERIAL PHASE VENOUS PHASE
 b500 ADC mets cyst")
25 CARCINOID METASTASES AND LIVER CYST Metastases bright on DWI (and dark on ADC) from restricted diffusion and cyst is darker (bright on ADC) b500 ADC mets cyst cyst

26 METASTATIC MELANOMA WITH PRIOR THERAPY T1 FS CE T1 FS CE T1 FS CE T1 FS

27 METASTATIC MELANOMA WITH PRIOR THERAPY DWI b500 DWI b500 DWI b500 CE T1 FS
28 LESION CHARACTERIZATION Especially helpful for cysts and hemangiomas which may have free water Limitations in distinguishing solid benign lesions (FNH and adenomas) from malignant lesions (HCC and mets) Restricted diffusion not only seen in tumors but also abscesses restricted diffusion distinguish from simple cysts
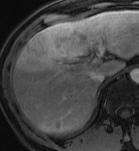
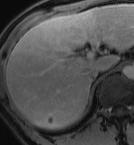
29 T2 SHINE THROUGH EFFECT Pitfall-signal intensity on DWI depends on both water diffusion and T2 relaxation time Lesions with long T2 relaxation times (cysts, hemangiomas) may remain high signal on DWI and be mistaken for restricted diffusion Referred to as T2 shine-through

30 T2 SHINE THROUGH EFFECT IN CYST To avoid misinterpretation, should look at the high b value images and ADC map Lesions that are high signal on high b value images and ADC are from T2 shine through effect b0 b500 ADC = 4.4
31 WHY NOT JUST LOOK AT THE ADC IMAGES? Poor signal to noise ratio Use DWI to detect Use ADC map image to differentiate restricted diffusion from T2 shine through ADC
32 WHY NOT JUST LOOK AT THE ADC IMAGES? Poor signal to noise ratio Use DWI to detect Use ADC map image to differentiate restricted diffusion from T2 shine through ADC DWI


33 WHY NOT JUST LOOK AT THE ADC IMAGES? Poor signal to noise ratio Use DWI to detect Use ADC map image to differentiate restricted diffusion from T2 shine through ADC DWI

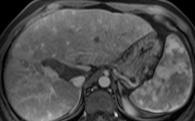
34 GIST: NONSPECIFIC LIVER LESION

35 RENAL DISEASE COULD NOT RECEIVE GADOLINIUM

36 RESTRICTED DIFFUSION b500 ADC
37
38 T2
39 b500 ADC




40 T2 T1 FS Post GAD T1 FS T2 FS DWI b50 b800 ADC b500 ADC 32 YEAR OLD WITH MELANOMA AND UNSUSPECTED LIVER LESIONS







41 1 YEAR LATER: LESIONS LARGER AND NEW LESIONS WITH MORE DEFINITIVE FEATURES POST GAD b50 b500 Art Phase Venous Phase B50 New Lesion Art Phase Delayed Phase Washout
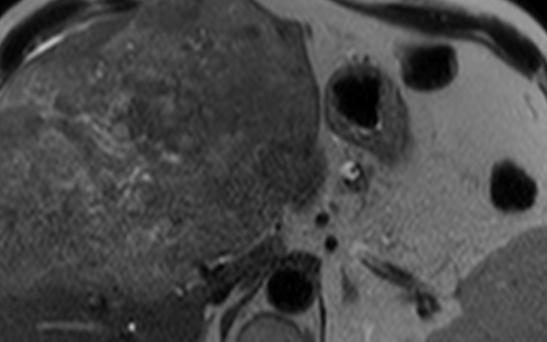

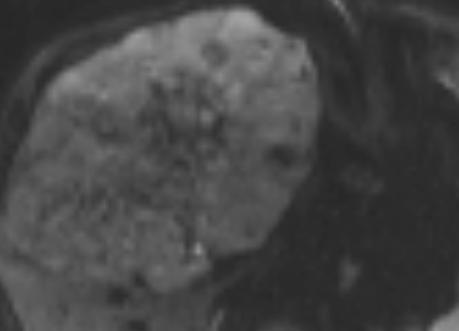
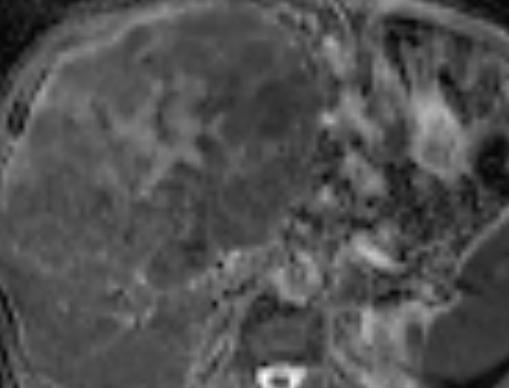
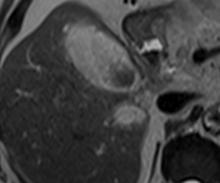
42 HEPATOCELLULAR CARCINOMA POST GAD T1 FS T2 b500 ADC ADC = 1.6

43 RESTRICTED DIFFUSION LOW ADC = 1.26 b500 ADC MALIGNANT? FNH
44 FNH: NEED ANATOMIC IMAGES IN ADDITION TO DWI T1 FS ARTERIAL PHASE POST GAD T2 DELAYED POST GAD

45 ABSCESSES Not only tumors have restricted diffusion and low ADC Abscesses can have restricted diffusion DWI help distinguish abscesses from cysts b400 ADC
46 LIVER CYST VS. LIVER ABSCESS T2 T1 post contrast T2 T1 post contrast



47 LIVER CYST VS. LIVER ABSCESS T2 T1 post contrast b1000 T2 T1 post contrast b1000 ADC
48 ADC (x10-3 mm 2 /s) ADC OF LIVER LESIONS BOX AND WHISKERS PLOT Metastasis HCC FNH Adenoma Abscess Hemangioma Cyst Miller FH, Hammond N, Siddiqi AJ et al. J Magn Reson Imaging Jul;32:138-47

49 LACK OF SPECIFICITY Hemangioma Metastases HCC Adenoma
50 INTERPRETATION OF IMAGES AFTER IR TREATMENT Among the most difficult in radiology No one fights to read these cases Paradoxical increase in size is seen with ablative therapies such as RF ablation, TACE and Y90 radioembolization-result of hemorrhage and necrosis No uniform standard of interpretation Ring enhancement mistaken for tumor and may be post treatment changes including scar tissue or reactive edema
51 DIFFUSION MR Lesions often don t change in size or may grow following effective changes Diffusion MR can play role in diagnosing response Following therapy, tumors with restricted diffusion (dark on ADC maps) become less restricted diffusion (bright on ADC maps) increase in ADC values Some of changes in ADC may precede changes in size of lesion






52 LIMITATIONS OF ANATOMIC ASSESSMENT Anatomic response lags behind functional changes Difficult to prospectively predict tumor response Pre Tx months Salem et al JVIR Dec 2005

53 FUNCTIONAL IMAGING: DIFFUSION Anatomic T1 post-gadolinium Functional Percentage enhancement on arterial and portal venous phases Extracellular space Tumor vascularity Detects altered water mobility Cellularity Integrity of the cell membrane Diffusion-weighted (DWI)
54 DIFFUSION: OVERSIMPLIFICATION Bright on diffusion images (dark ADC)-restricted diffusion-live tumor Dark on diffusion images-favorable response Successful treatment-dark on DWI and shows increase in ADC
55 HCC PRETREATMENT Bright


56 HCC POST TREATMENT Dark Post contrast Post Treatment DWI Post Treatment Post Treatment DWI Pretreatment

57 Pre-Treatment Arterial Phase Venous Phase DWI b50 Post-Treatment Arterial Phase Venous Phase DWI b50



58 T1 in Phase T2 Post GAD T1 FS
59 DWI PET
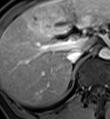
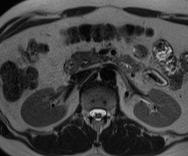
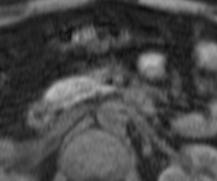
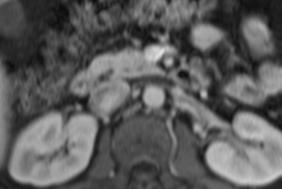
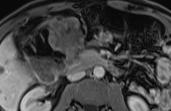
60 PANCREATIC IMAGING DWI may help in detecting solid pancreatic neoplasms with restricted diffusion May not be able to distinguish chronic pancreatitis from cancer because of overlap i.e. poorly differentiated adenoca and mass-forming pancreatitis have low ADC from dense fibrosis
61 PANCREATIC CANCER Critical to detect early Desmoplastic reaction accounts for low SI on T1FS images, hypoenhancement and restricted diffusion DWI especially helpful in detection and characterization of liver and lymph node and peritoneal mets



62 DIFFUSION EXAMPLE PANC CA T2 MR T1 FS MR CE T1 FS MR
63 DIFFUSION EXAMPLE PANC CA DIFFUSION B500 ADC



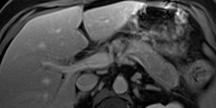
64 DIFFUSION EXAMPLE: ENDOCRINE TUMOR BEST SEEN ON DW NCCT Early Post Contrast Venous Post Contrast


65 ENDOCRINE TUMOR: DWI b0 b500 T1 FS CE CT
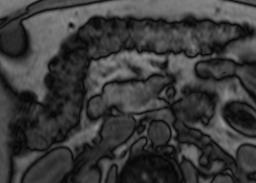
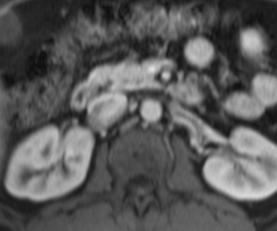

66 INSULINOMA
67 b0 b1000 ADC
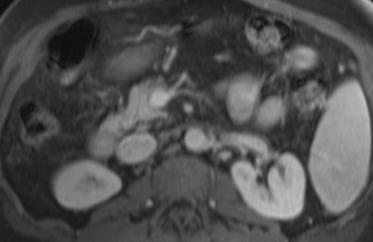
68 BACKGROUND Pancreatic adenocarcinoma and mass-forming focal pancreatitis can have similar imaging findings on anatomic MRI Would be helpful for DWI to distinguish Contradictory results have been seen using DWI in the literature and wanted to determine why ADC values of pancreatic adenocarcinoma have been shown to be both higher and lower than mass-forming focal pancreatitis Fattahi et al. J Magn Reson Imaging 2009;29:350-6 Lee et al J Magn Reson Imaging 2008;28:928-36

 Adenocarcinoma b500")
69 MAY NOT BE ABLE TO DISTINGUISH Mass-forming pancreatitis b500 (ADC = 1.27) Adenocarcinoma b500 (ADC = 1.55)
 Poorly differentiated adenocarcinoma b500 (ADC =1.")

70 EXTRACELLULAR FIBROSIS Mass-forming pancreatitis b500 (ADC=1.27) Poorly differentiated adenocarcinoma b500 (ADC =1.55) Extra-cellular fibrosis in both pancreatitis and adenocarcinoma No significant difference in ADC Wang Y, Miller FH, Chen Zongming E et al. Radiographics. 2011
71 ADC (x10-3 mm 2 /s) RESULTS: ADCs OF LESION AFTER SUBDIVISION Neuroendocrine Carcinoma (malignant) P= Well-differentiated Neuroendocrine Tumor (nonmalignant) Mass-forming focal Pancreatitis Poorly differentiated Adenocarcinoma Well/Moderately differentiated Adenocarcinoma


72 MALIGNANT ENDOCRINE: LOWER ADC VALUES Malignant endocrine carcinoma ADC=0.87 Well-differentiated endocrine tumor ADC= 2.22 High density of cellularity Cells with scant cytoplasm Lower ADC values


73 OVERLAP ONLY IN SMALL WELL DIFFERENTIATED WITH FIBROSIS Malignant endocrine carcinoma ADC=1.17 Well-differentiated endocrine tumor ADC= 1.02 High density of cellularity High density of fibrosis Low ADC values
74 ADC (x10-3 mm 2 /s) RESULTS: ADCs OF LESION AFTER SUBDIVISION Neuroendocrine Carcinoma (malignant) Well-differentiated Neuroendocrine Tumor (nonmalignant) Mass-forming focal Pancreatitis P= Poorly differentiated Adenocarcinoma Well/Moderately differentiated Adenocarcinoma


75 POOR DIFFERENTIATED TUMORS WITH MORE FIBROSIS: LOWER ADC Poorly differentiated adenoca ADC=1.48 Moderately differentiated adenoca ADC=2.27 Extra-cellular fibrosis Limited glandular formation Lower ADC values Wang Y, Miller FH, Chen Zongming E et al. Radiographics. 2011
76 DWI DWI did not distinguish mass-forming pancreatitis and adenocarcinoma fibrosis in both Grades of differentiation of tumors may be distinguished because of differences in cellularity, glandular differentiation and extracellular fibrosis

77
78 b500 ADC
79 RENAL IMAGING Especially helpful when concern of NSF and cannot give gadolinium Helps detect and confirm solid mass-suspect RCC Other lesions can have restricted diffusion-abscesses, angiomyolipomas, oncocytomas DWI images help guide to the anatomic abnormality which may be subtle
80 UNSUSPECTED SMALL RCC b800 ADC

81





82 NCCT Axial CECT Coronal CECT Axial Postgad Coronal Postgad b500 ADC


83 PCKD IN HORSESHOE KIDNEY WITH FEVERS; COULDN T GIVE GAD AS CONCERN OF NSF-LOW GFR Coronal T2 Coronal T2

84 Axial T2 b800

85 ADC Map CT Guided Biopsy
86 51 YR OLD MYELODYSPLASTIC SYNDROME AND FEVERS T1 FS T2


87 Post GAD T1 FS T2 Post GAD Sag T1 FS
88 RESTRICTED DIFFUSION: DARK ADC b800 ADC

89 DWI BETTER THAN T2


90 PYONEPHROSIS 64 year old male with rectal cancer: Worsening renal function Could not give GAD UNENHANCED CT T2WI DWI b500 ADC
91 ADRENAL GLAND Most important lesions to distinguish are not cystic from solid lesions but adrenal adenomas from metastases or adrenal cell carcinoma DWI is nonspecific; need very high specificity in the diagnosis of adenomas While malignant adrenal masses show restricted diffusion, adrenal adenomas also may show restricted diffusion
92 CARCINOMA: ADC 0.99 B500 B0 ADC Mean of carcinomas was 1.47 without difference from other lesions except cysts being higher.


93 ADENOMA: ADC 0.64 / SI DECREASE 46% IN PHASE OUT PHASE b500 b0
94 ADC (x10-3 mm 2 /s) ADCS OF ADRENAL LESIONS Myelolipoma Hemorrhage Adenoma Cyst Carcinoma Pheochromocytoma Metastasis Miller FH, Wang Y, McCarthy RJ, et al. Am. J. Roentgenol 2010; 194: W179-W185
95 Signal intensity (% Decrease), AUC = 0.93 Lesion size (cm), AUC = 0.82 ADC (x10-3 mm2/sec), AUC = Specificity Miller FH, Wang Y, McCarthy RJ, et al. Am. J. Roentgenol 2010; 194: W179-W185
96 LYMPH NODE AND PERITONEAL IMPLANTS One of best uses for DWI-lymph node metastases and small peritoneal implants Conventional MR is not always ideal for showing lymph nodes and peritoneal implants-distinguishing from bowel can be difficult DWI helps direct radiologist to pathology on conventional imaging
97 LYMPH NODE AND PERITONEAL IMPLANTS In my opinion, DWI often does not distinguish benign from malignant lymph nodes but great sequence to show nodes Increasing use of MR because of radiation concerns when doing multiple CT scans for followup imaging especially when young patients (testicular cancer and lymphoma) where lymph nodes and DWI are important


98 TESTICULAR CANCER RECURRENCE: LYMPH NODES T2 T1 FS Diffusion b1000 b1000


99 TESTICULAR CANCER WITH RECURRENCE BEST SEEN ON B800 b50 b500


100 FALLOPIAN TUBE CANCER T1 FS T2 DWI b1000

101 FALLOPIAN TUBE CANCER T1 FS DWI b1000


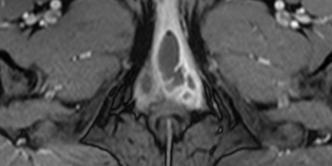
102 VULVAR CANCER: DWI CRITICAL FOR METS Sag Post GAD T1 FS Axial Post GAD T1 FS


103 VULVAR CANCER: DWI CRITICAL FOR METS Axial Post GAD T1 FS DWI b500 Sag Post GAD T1 FS

104 VULVAR CANCER: DWI CRITICAL FOR METS Axial Post GAD T1 FS DWI b500
105 APPENDICITIS IN PREGNANT PT T2 True FISP T1 FS
106 APPENDICITIS IN PREGNANT PT T2 True FISP T1 FS b800 ADC
107 TUBO-OVARIAN ABSCESSES (TOA) T2 T1FS POSTGAD T1FS

108 TUBO-OVARIAN ABSCESSES (TOA) T2 T1FS POSTGAD T1FS DWI b800 ADC




109 28 YEAR OLD PELVIC PAIN AND FEVER T2 T1 FS Post GAD T1 FS T1 FS Post GAD
 DWI")
110 DWI-TUBOOVARIAN ABSCESS (TOA) DWI b800 ADC


111 INTER-LOOP ABSCESS: 73 YEAR OLD W RECTAL CANCER PRIOR RT AND FEVER AND PAIN T2 T1 post gad DWI b800 ADC

112 MR TO EVALUATE LIVER LESIONS
113
114
115


116 60 YEAR OLD WOMAN: FOLLOW UP COMPLEX RENAL CYST JULY 2014 T1 Post Gad CECT b500 ADC

117 AUG 2013 T1 Post Gad b800 Fungating, ulcerated partially obstructing adenocarcinoma in the distal transverse colon
118 MR FOR FIBROID EVALUATION PRE UFE Sagittal T2 Axial T2
119 DIFFUSION-WEIGHTED IMAGES b500
120 UNSUSPECTED RECTAL CANCER Sagittal T2 Axial T2


121 UNSUSPECTED RECTAL CANCER Sagittal Post Contrast Axial Post Contrast

122 T2 Post GAD T1 FS
123 BOTH ARE BRIGHT ON B50 IMAGE b50
124 B800 INFECTED BARTHOLIN GLAND CYST ADC
125 CONCLUSIONS DWI should be added to routine protocols Helpful in detection of lesions in liver, kidney, pancreas, lymph nodes and peritoneal implants Can be helpful in characterization Solid from cystic masses Abscesses from simple cysts Assess therapy response prior to size changes
126 ACKNOWLEDGEMENTS Dr. Shawn Haji-Momenian Dr. Laura Kulik Dr. Andrew Larson Dr. Robert J Lewandowski Dr. Reed Omary Dr. Tom Rhee Dr. Riad Salem Dr. Yi Wang
ADRENAL MR: PEARLS AND PITFALLS
 ADRENAL MR: PEARLS AND PITFALLS Frank Miller, M.D. Lee F. Rogers MD Professor of Medical Education Chief, Body Imaging Section and Fellowship Medical Director, MR Imaging Professor of Radiology Northwestern
ADRENAL MR: PEARLS AND PITFALLS Frank Miller, M.D. Lee F. Rogers MD Professor of Medical Education Chief, Body Imaging Section and Fellowship Medical Director, MR Imaging Professor of Radiology Northwestern
Liver MRI in 30 minutes
 X Liver MRI in 30 minutes SCBT/MR Annual Meeting Salt Lake City September 18, 2016 Scott B. Reeder, MD, PhD Department of Radiology University of Wisconsin Madison, WI Disclosures University of Wisconsin-Madison
X Liver MRI in 30 minutes SCBT/MR Annual Meeting Salt Lake City September 18, 2016 Scott B. Reeder, MD, PhD Department of Radiology University of Wisconsin Madison, WI Disclosures University of Wisconsin-Madison
Jeffrey C. Weinreb, MD, FACR Yale School of Medicine Yale-New Haven Hospital
 Jeffrey C. Weinreb, MD, FACR Yale School of Medicine Yale-New Haven Hospital jeffrey.weinreb@yale.edu 1991 1997 Whole body MRI: multistation approach x z Isocenter: Table Move: Multiple Steps Whole body
Jeffrey C. Weinreb, MD, FACR Yale School of Medicine Yale-New Haven Hospital jeffrey.weinreb@yale.edu 1991 1997 Whole body MRI: multistation approach x z Isocenter: Table Move: Multiple Steps Whole body
Diffusion Weighted Imaging in Pediatric Body: Update
 Diffusion Weighted Imaging in Pediatric Body: Update Govind Chavhan, MD DABR Diagnostic Imaging Department The Hospital for Sick Children and University of Toronto, Canada 2 Outline Principles of diffusion
Diffusion Weighted Imaging in Pediatric Body: Update Govind Chavhan, MD DABR Diagnostic Imaging Department The Hospital for Sick Children and University of Toronto, Canada 2 Outline Principles of diffusion
Acknowledgements. Update of Focal Liver Lesions Goals. Focal Liver Lesions. Imaging Choices For Liver Lesions. Focal Liver Lesions
 Acknowledgements Update of Focal Liver Lesions 2012 Giles Boland Massachusetts General Hospital Harvard Medical School No disclosures Dushyant Sahani Mukesh Harisinghani Goals Focal liver lesions Imaging
Acknowledgements Update of Focal Liver Lesions 2012 Giles Boland Massachusetts General Hospital Harvard Medical School No disclosures Dushyant Sahani Mukesh Harisinghani Goals Focal liver lesions Imaging
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Disclosures. Diffusion and Perfusion Imaging in the Head and Neck. Learning objectives ???
 Disclosures No relevant financial disclosures Diffusion and Perfusion Imaging in the Head and Neck Ashok Srinivasan, MD Associate Professor Director of Neuroradiology University of Michigan Health System
Disclosures No relevant financial disclosures Diffusion and Perfusion Imaging in the Head and Neck Ashok Srinivasan, MD Associate Professor Director of Neuroradiology University of Michigan Health System
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment
 Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
CASE 1 11/1/2016 HEPATOBILIARY IMAGING CASE PRESENTATIONS DECLARATION. Dr. Chirag Patel ORGAN IMAGING yr old lady
 HEPATOBILIARY IMAGING CASE PRESENTATIONS DECLARATION No financial disclosures or affiliations with commercial organisations No discussion of investigational or off-label use of medical devices, products
HEPATOBILIARY IMAGING CASE PRESENTATIONS DECLARATION No financial disclosures or affiliations with commercial organisations No discussion of investigational or off-label use of medical devices, products
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
LIVER IMAGING TIPS IN VARIOUS MODALITIES. M.Vlychou, MD, PhD Assoc. Professor of Radiology University of Thessaly
 LIVER IMAGING TIPS IN VARIOUS MODALITIES M.Vlychou, MD, PhD Assoc. Professor of Radiology University of Thessaly Hepatocellular carcinoma is a common malignancy for which prevention, screening, diagnosis,
LIVER IMAGING TIPS IN VARIOUS MODALITIES M.Vlychou, MD, PhD Assoc. Professor of Radiology University of Thessaly Hepatocellular carcinoma is a common malignancy for which prevention, screening, diagnosis,
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Essentials of Clinical MR, 2 nd edition. 73. Urinary Bladder and Male Pelvis
 73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
Contrast Enhanced Ultrasound of Parenchymal Masses in Children
 Contrast Enhanced Ultrasound of Parenchymal Masses in Children Sue C Kaste, DO On behalf of Beth McCarville, MD St. Jude Children s Research Hospital Memphis, TN Overview Share St. Jude experience with
Contrast Enhanced Ultrasound of Parenchymal Masses in Children Sue C Kaste, DO On behalf of Beth McCarville, MD St. Jude Children s Research Hospital Memphis, TN Overview Share St. Jude experience with
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Innovations in HCC Imaging: MDCT/MRI
 Innovations in HCC Imaging: MDCT/MRI Anthony E. Cheng, M.D. Cardinal MRI Center Cardinal Santos Medical Center, Wilson Street, San Juan Innovations in HCC Imaging: Goals/Objectives MDCT/MRI Learn the diagnostic
Innovations in HCC Imaging: MDCT/MRI Anthony E. Cheng, M.D. Cardinal MRI Center Cardinal Santos Medical Center, Wilson Street, San Juan Innovations in HCC Imaging: Goals/Objectives MDCT/MRI Learn the diagnostic
HEPATO-BILIARY IMAGING
 HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
Essentials of Clinical MR, 2 nd edition. 65. Benign Hepatic Masses
 65. Benign Hepatic Masses Pulse sequences acquired for abdominal MRI typically consist of fast acquisition schemes such as single-shot turbo spin echo (i.e. HASTE) and gradient echo schemes such as FLASH
65. Benign Hepatic Masses Pulse sequences acquired for abdominal MRI typically consist of fast acquisition schemes such as single-shot turbo spin echo (i.e. HASTE) and gradient echo schemes such as FLASH
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
ADRENAL LESIONS 10/09/2012. Adrenal + lesion. Introduction. Common causes. Anatomy. Financial disclosure. Dr. Boraiah Sreeharsha. Nothing to declare
 ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
Abdominal MRI Techniques in Pediatric Oncology
 Abdominal MRI Techniques in Pediatric Oncology Jonathan R. Dillman, M.D. Assistant Professor Departments of Radiology & Urology Section of Pediatric Radiology C.S. Mott Children s Hospital Disclosures
Abdominal MRI Techniques in Pediatric Oncology Jonathan R. Dillman, M.D. Assistant Professor Departments of Radiology & Urology Section of Pediatric Radiology C.S. Mott Children s Hospital Disclosures
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Abdominal applications of DWI
 Postgraduate course, SPR San Antonio (Texas), May 14-15, 2013 Abdominal applications of DWI Rutger A.J. Nievelstein Wilhelmina Children s s Hospital, Utrecht (NL) Outline What is DWI? How to perform? Challenges
Postgraduate course, SPR San Antonio (Texas), May 14-15, 2013 Abdominal applications of DWI Rutger A.J. Nievelstein Wilhelmina Children s s Hospital, Utrecht (NL) Outline What is DWI? How to perform? Challenges
FieldStrength. Leuven research is finetuning. whole body staging
 FieldStrength Publication for the Philips MRI Community Issue 40 May 2010 Leuven research is finetuning 3.0T DWIBS for whole body staging The University Hospital of Leuven is researching 3.0T whole body
FieldStrength Publication for the Philips MRI Community Issue 40 May 2010 Leuven research is finetuning 3.0T DWIBS for whole body staging The University Hospital of Leuven is researching 3.0T whole body
8/3/2016. Consultant for / research support from: Astellas Bayer Bracco GE Healthcare Guerbet Medrad Siemens Healthcare. Single Energy.
 U. Joseph Schoepf, MD Prof. (h.c.), FAHA, FSCBT-MR, FNASCI, FSCCT Professor of Radiology, Medicine, and Pediatrics Director, Division of Cardiovascular Imaging Consultant for / research support from: Astellas
U. Joseph Schoepf, MD Prof. (h.c.), FAHA, FSCBT-MR, FNASCI, FSCCT Professor of Radiology, Medicine, and Pediatrics Director, Division of Cardiovascular Imaging Consultant for / research support from: Astellas
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Workup of a Solid Liver Lesion
 Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
The Focal Hepatic Lesion: Radiologic Assessment
 The Focal Hepatic Lesion: Radiologic Assessment Kevin Kuo, Harvard Medical School Year III Our Patient: PS 67 y/o female w/ long history of alcohol use Drinking since age 18, up to one bottle of wine/day
The Focal Hepatic Lesion: Radiologic Assessment Kevin Kuo, Harvard Medical School Year III Our Patient: PS 67 y/o female w/ long history of alcohol use Drinking since age 18, up to one bottle of wine/day
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Anatomical and Functional MRI of the Pancreas
 Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
بسم هللا الرحمن الرحيم. Prof soha Talaat
 بسم هللا الرحمن الرحيم Ovarian tumors The leading indication for gynecologic surgery. Preoperative characterization of complex solid and cystic adnexal masses is crucial for informing patients about possible
بسم هللا الرحمن الرحيم Ovarian tumors The leading indication for gynecologic surgery. Preoperative characterization of complex solid and cystic adnexal masses is crucial for informing patients about possible
Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review
 Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
ESUR 2018, Sept. 13 th.-16 th., 2018 Barcelona, Spain
 ESUR 2018, Sept. 13 th.-16 th., 2018 Barcelona, Spain OUR APPROACH Incidental adrenal nodule/mass Isaac R Francis, M.B;B.S University of Michigan, Ann Arbor, Michigan Disclosures None (in memory) M Korobkin,
ESUR 2018, Sept. 13 th.-16 th., 2018 Barcelona, Spain OUR APPROACH Incidental adrenal nodule/mass Isaac R Francis, M.B;B.S University of Michigan, Ann Arbor, Michigan Disclosures None (in memory) M Korobkin,
Evaluation of Liver Mass Lesions. American College of Gastroenterology 2013 Regional Postgraduate Course
 Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
(2/3 PRCC!) (2/3 PRCC!)
 (2/3 PRCC!)") Approach to the Incidental Solid Renal Mass Stuart G. Silverman, MD, FACR Professor of Radiology Harvard ard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Approach to the Incidental Solid Renal Mass Stuart G. Silverman, MD, FACR Professor of Radiology Harvard ard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
11/10/2015. Prostate cancer in the U.S. Multi-parametric MRI of Prostate Diagnosis and Treatment Planning. NIH estimates for 2015.
 Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
CASE STUDY. Presented by: Jessica Pizzo. CFCC Sonography student Class of 2018
 CASE STUDY Presented by: Jessica Pizzo CFCC Sonography student Class of 2018 Case Presentation April 4, 2017 56 yr old woman presented to ED with lower abdominal pain & swelling, along with constipation.
CASE STUDY Presented by: Jessica Pizzo CFCC Sonography student Class of 2018 Case Presentation April 4, 2017 56 yr old woman presented to ED with lower abdominal pain & swelling, along with constipation.
HEPATOCYTE SPECIFIC CONTRAST MEDIA: WHERE DO WE STAND?
 HEPATOCYTE SPECIFIC CONTRAST MEDIA: WHERE DO WE STAND? Andrew T. Trout, MD @AndrewTroutMD Disclosures No relevant disclosures Outline Review of hepatocyte specific contrast media Review of hepatocellular
HEPATOCYTE SPECIFIC CONTRAST MEDIA: WHERE DO WE STAND? Andrew T. Trout, MD @AndrewTroutMD Disclosures No relevant disclosures Outline Review of hepatocyte specific contrast media Review of hepatocellular
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Traumatic and Non Traumatic Adrenal Emergencies
 Traumatic and Non Traumatic Adrenal Emergencies Michael N. Patlas, MD, FRCPC (1), Christine O. Menias, MD (2), Douglas S. Katz, MD, FACR (3), Ania Z. Kielar, MD, FRCPC (4), Alla M. Rozenblit, MD (5), Jorge
Traumatic and Non Traumatic Adrenal Emergencies Michael N. Patlas, MD, FRCPC (1), Christine O. Menias, MD (2), Douglas S. Katz, MD, FACR (3), Ania Z. Kielar, MD, FRCPC (4), Alla M. Rozenblit, MD (5), Jorge
Malignant Focal Liver Lesions
 Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
International Journal of Current Medical Sciences- Vol. 6, Issue,, pp , June, 2016 A B S T R A C T
 ISSN: 2320-8147 International Journal of Current Medical Sciences- Vol. 6, Issue,, pp. 122-126, June, 2016 COMPUTED TOMOGRAPHY IN HEPATIC METASTASES Ananthakumar P and Adaikkappan M., Available online
ISSN: 2320-8147 International Journal of Current Medical Sciences- Vol. 6, Issue,, pp. 122-126, June, 2016 COMPUTED TOMOGRAPHY IN HEPATIC METASTASES Ananthakumar P and Adaikkappan M., Available online
Role of DE-CT in Oncology
 Role of DE-CT in Oncology Dushyant Sahani, M.D Director of CT Associate Professor of Radiology Massachusetts General Hospital Harvard Medical School Email-dsahani@partners.org Disclosure Research Grant
Role of DE-CT in Oncology Dushyant Sahani, M.D Director of CT Associate Professor of Radiology Massachusetts General Hospital Harvard Medical School Email-dsahani@partners.org Disclosure Research Grant
MRI OF FOCAL LESIONS IN
 Introduction MRI OF FOCAL LESIONS IN THE NON-CIRRHOTIC LIVER Ivan Pedrosa M.D. Ph.D. Associate Professor of Radiology and Advanced Imaging Research Center University of Texas Southwestern. Dallas, TX Incidental
Introduction MRI OF FOCAL LESIONS IN THE NON-CIRRHOTIC LIVER Ivan Pedrosa M.D. Ph.D. Associate Professor of Radiology and Advanced Imaging Research Center University of Texas Southwestern. Dallas, TX Incidental
MDCT signs differentiating retroperitoneal and intraperitoneal lesions- diagnostic pearls
 MDCT signs differentiating retroperitoneal and intraperitoneal lesions- diagnostic pearls Poster No.: C-0987 Congress: ECR 2015 Type: Educational Exhibit Authors: D. V. Bhargavi, R. Avantsa, P. Kala; Bangalore/IN
MDCT signs differentiating retroperitoneal and intraperitoneal lesions- diagnostic pearls Poster No.: C-0987 Congress: ECR 2015 Type: Educational Exhibit Authors: D. V. Bhargavi, R. Avantsa, P. Kala; Bangalore/IN
CT & MRI of Benign Liver Neoplasms Srinivasa R Prasad
 CT & MRI of Benign Liver Neoplasms Srinivasa R Prasad No financial disclosures Acknowledgements Many thanks to Drs. Heiken, Narra & Menias (MIR) Dr. Sahani (MGH) for sharing images Benign Liver Tumors:
CT & MRI of Benign Liver Neoplasms Srinivasa R Prasad No financial disclosures Acknowledgements Many thanks to Drs. Heiken, Narra & Menias (MIR) Dr. Sahani (MGH) for sharing images Benign Liver Tumors:
Zoltan Harkanyi M.D., Ph.D. Department of Radiology, Heim Pal Children s Hospital, Budapest, Hungary
 Zoltan Harkanyi M.D., Ph.D. Department of Radiology, Heim Pal Children s Hospital, Budapest, Hungary CEUS expereince 10 years Department of Radiology, Heim Pal Children s Hospital, Budapest US N o 1 study
Zoltan Harkanyi M.D., Ph.D. Department of Radiology, Heim Pal Children s Hospital, Budapest, Hungary CEUS expereince 10 years Department of Radiology, Heim Pal Children s Hospital, Budapest US N o 1 study
Pediatric Abdominal Masses. Andrew Phelps MD Assistant Professor of Pediatric Radiology UCSF Benioff Children's Hospital
 Pediatric Abdominal Masses Andrew Phelps MD Assistant Professor of Pediatric Radiology UCSF Benioff Children's Hospital No Disclosures Take Home Message All you need to remember are the 5 common masses
Pediatric Abdominal Masses Andrew Phelps MD Assistant Professor of Pediatric Radiology UCSF Benioff Children's Hospital No Disclosures Take Home Message All you need to remember are the 5 common masses
Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C.
 Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Computed Diffusion-Weighted Image in the Abdomen
 Computed Diffusion-Weighted Image in the Abdomen Poster No.: C-0234 Congress: ECR 2014 Type: Scientific Exhibit Authors: T. Yoshikawa 1, N. Aoyama 1, Y. Ohno 1, K. Kyotani 1, Y. Kassai 2, K. Sofue 1, M.
Computed Diffusion-Weighted Image in the Abdomen Poster No.: C-0234 Congress: ECR 2014 Type: Scientific Exhibit Authors: T. Yoshikawa 1, N. Aoyama 1, Y. Ohno 1, K. Kyotani 1, Y. Kassai 2, K. Sofue 1, M.
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Characterization of adrenal lesions on CT and MRI: all that a radiologist must know
 Characterization of adrenal lesions on CT and MRI: all that a radiologist must know Poster No.: C-2476 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Benzina, S. MAJDOUB, C. H. ZARRAD, H. Zaghouani,
Characterization of adrenal lesions on CT and MRI: all that a radiologist must know Poster No.: C-2476 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Benzina, S. MAJDOUB, C. H. ZARRAD, H. Zaghouani,
Images In Gastroenterology
 Images In Gastroenterology Thong-Ngam D, et al. THAI J GASTROENTEROL 2005 Vol. 6 No. 2 May - Aug. 2005 105 Imaging of Gastrointestinal Stromal Tumors Pornpim Fuangtharnthip, M.D. Narumol Hargroove, M.D.
Images In Gastroenterology Thong-Ngam D, et al. THAI J GASTROENTEROL 2005 Vol. 6 No. 2 May - Aug. 2005 105 Imaging of Gastrointestinal Stromal Tumors Pornpim Fuangtharnthip, M.D. Narumol Hargroove, M.D.
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
What Radiologists do?
 Multimodality Imaging in Oncology 2018 March 5 th 9th Diagnostic Imaging in Oncology What Radiologists do? Chikako Suzuki, MD, PhD Department of Diagnostic Radiology, KS Solna Department of Molecular Medicine
Multimodality Imaging in Oncology 2018 March 5 th 9th Diagnostic Imaging in Oncology What Radiologists do? Chikako Suzuki, MD, PhD Department of Diagnostic Radiology, KS Solna Department of Molecular Medicine
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
X-ray Corner. Imaging of The Pancreas. Pantongrag-Brown L
 X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
Interesting Cases from Liver Tumor Board. Jeffrey C. Weinreb, M.D.,FACR Yale University School of Medicine
 Interesting Cases from Liver Tumor Board Jeffrey C. Weinreb, M.D.,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Common Liver Diseases Hemangioma Cyst FNH Focal Fat/Sparing THID Non-Cirrhotic
Interesting Cases from Liver Tumor Board Jeffrey C. Weinreb, M.D.,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Common Liver Diseases Hemangioma Cyst FNH Focal Fat/Sparing THID Non-Cirrhotic
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Enhancements in Hepatobiliary Imaging:
 Enhancements in Hepatobiliary Imaging: S. Channual 1, MD; A. Pahwa 2, MD; S. Raman 1, MD. 1 UCLA Medical Center, Department of Radiologic Sciences 2 Olive-View UCLA Medical Center, Department of Radiology
Enhancements in Hepatobiliary Imaging: S. Channual 1, MD; A. Pahwa 2, MD; S. Raman 1, MD. 1 UCLA Medical Center, Department of Radiologic Sciences 2 Olive-View UCLA Medical Center, Department of Radiology
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Financial Disclosure
 Benign Liver Masses Adil Abdalla, MBBS Creighton University-CHI Health August 25, 2018 Financial Disclosure Nothing to disclose Financial Disclosure 1 Objectives To assess patients with benign liver tumors
Benign Liver Masses Adil Abdalla, MBBS Creighton University-CHI Health August 25, 2018 Financial Disclosure Nothing to disclose Financial Disclosure 1 Objectives To assess patients with benign liver tumors
Liver nodules mimicking metastatic disease
 Liver nodules mimicking metastatic disease Poster No.: C-1703 Congress: ECR 2011 Type: Educational Exhibit Authors: F. Vandenbroucke, B. Ilsen, B. Op de Beeck, J. de Mey ; 1 1 2 2 3 2 3 Brussels/BE, Brussel/BE,
Liver nodules mimicking metastatic disease Poster No.: C-1703 Congress: ECR 2011 Type: Educational Exhibit Authors: F. Vandenbroucke, B. Ilsen, B. Op de Beeck, J. de Mey ; 1 1 2 2 3 2 3 Brussels/BE, Brussel/BE,
CTA/MRA of Pediatric Hepatic Masses Radiology-Pathology Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº70, pág. 41-50, Abr.-Jun., 2006 CTA/MRA of Pediatric Hepatic Masses Radiology-Pathology Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº70, pág. 41-50, Abr.-Jun., 2006 CTA/MRA of Pediatric Hepatic Masses Radiology-Pathology Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
children Crohn s disease in MR enterography for GI Complications Microscopy Characterization Primary sclerosing cholangitis Anorectal fistulae
 MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011
 Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011 Reported: Analysis Summary for: Abdomen Examination Survey Dates 06/13/2011-06/26/2011 Invited Respondents 6,000 Surveys with Demographics
Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011 Reported: Analysis Summary for: Abdomen Examination Survey Dates 06/13/2011-06/26/2011 Invited Respondents 6,000 Surveys with Demographics
11/1/2014. Radiologic incidentalomas Ordering pitfalls Newer technology and applications
 Bilal Tahir, MD Gitasree Borthakur, MD Indiana University School of Medicine Department of Radiology & Imaging Sciences October 31, 2014 ACP 2014 Dr. V. Aaron Nuclear (vaaron@iupui.edu) Dr. S. Westphal
Bilal Tahir, MD Gitasree Borthakur, MD Indiana University School of Medicine Department of Radiology & Imaging Sciences October 31, 2014 ACP 2014 Dr. V. Aaron Nuclear (vaaron@iupui.edu) Dr. S. Westphal
CT evaluation of small bowel carcinoid tumors
 CT evaluation of small bowel carcinoid tumors Poster No.: C-0060 Congress: ECR 2015 Type: Educational Exhibit Authors: N. V. V. P. Costa, L. Nascimento, T. Bilhim ; Estoril/PT, PT, 1 2 3 1 2 3 Lisbon/PT
CT evaluation of small bowel carcinoid tumors Poster No.: C-0060 Congress: ECR 2015 Type: Educational Exhibit Authors: N. V. V. P. Costa, L. Nascimento, T. Bilhim ; Estoril/PT, PT, 1 2 3 1 2 3 Lisbon/PT
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Diffusion Weighted Imaging in Prostate Cancer
 Diffusion Weighted Imaging in Prostate Cancer Disclosure Information Vikas Kundra, M.D, Ph.D. No financial relationships to disclose. Education Goals and Objectives To describe the utility of diffusion-weighted
Diffusion Weighted Imaging in Prostate Cancer Disclosure Information Vikas Kundra, M.D, Ph.D. No financial relationships to disclose. Education Goals and Objectives To describe the utility of diffusion-weighted
SELF-ASSESSMENT MODULE REFERENCE SPR 2018 Oncologic Imaging Course Adrenal Tumors November 10, :00 12:10 p.m.
 SELF-ASSESSMENT MODULE REFERENCE SPR 2018 Oncologic Imaging Course Adrenal Tumors November 10, 2018 10:00 12:10 p.m. Staging Susan E. Sharp, MD 1. In the International Neuroblastoma Risk Group Staging
SELF-ASSESSMENT MODULE REFERENCE SPR 2018 Oncologic Imaging Course Adrenal Tumors November 10, 2018 10:00 12:10 p.m. Staging Susan E. Sharp, MD 1. In the International Neuroblastoma Risk Group Staging
CT EVALUATION OF GASTRIC LESIONS:
 CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
Personal data. Age : 63 Gender : male
 Personal data Age : 63 Gender : male Chief complain No specific symptom or discomfort A hepatic mass, found by abdominal sonography of routine health exam on 88-12-08 Past history 1984-3-3 Old CVA with
Personal data Age : 63 Gender : male Chief complain No specific symptom or discomfort A hepatic mass, found by abdominal sonography of routine health exam on 88-12-08 Past history 1984-3-3 Old CVA with
Abdomen Sonography Examination Content Outline
 Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
A Practical Approach to Adnexal Masses
 A Practical Approach to Adnexal Masses Darcy J. Wolfman, MD Section Chief of Genitourinary Imaging American Institute for Radiologic Pathology Clinical Associate Johns Hopkins Community Radiology Division
A Practical Approach to Adnexal Masses Darcy J. Wolfman, MD Section Chief of Genitourinary Imaging American Institute for Radiologic Pathology Clinical Associate Johns Hopkins Community Radiology Division
STANDARDIZED MANAGEMENT RECOMMENDATIONS FOR ADRENAL NODULES: EVIDENCE-BASED CONSENSUS POWERSCRIBE MACROS FROM AN ACADEMIC/PRIVATE PRACTICE
 STANDARDIZED MANAGEMENT RECOMMENDATIONS FOR ADRENAL NODULES: EVIDENCE-BASED CONSENSUS POWERSCRIBE MACROS FROM AN ACADEMIC/PRIVATE PRACTICE COLLABORATIVE Pamela Johnson 1, Darcy Wolfman 2, Upma Rawal 3,
STANDARDIZED MANAGEMENT RECOMMENDATIONS FOR ADRENAL NODULES: EVIDENCE-BASED CONSENSUS POWERSCRIBE MACROS FROM AN ACADEMIC/PRIVATE PRACTICE COLLABORATIVE Pamela Johnson 1, Darcy Wolfman 2, Upma Rawal 3,
Alice Fung, MD Oregon Health and Science University
 Alice Fung, MD Oregon Health and Science University Disclosure Comments The speaker Alice Fung, MD Has relevant financial relationships to disclose. Received honorarium from (Guerbet). This individual
Alice Fung, MD Oregon Health and Science University Disclosure Comments The speaker Alice Fung, MD Has relevant financial relationships to disclose. Received honorarium from (Guerbet). This individual
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
Case 1. Children s hospital of Fudan University
 Case 1 Children s hospital of Fudan University Medical History General data:female,2y Chief complaint: Claudication of the left limb for 2 week. History of present illness:a 2-year-old girl who didn t
Case 1 Children s hospital of Fudan University Medical History General data:female,2y Chief complaint: Claudication of the left limb for 2 week. History of present illness:a 2-year-old girl who didn t
Renal masses - the role of diagnostic imaging
 Renal masses - the role of diagnostic imaging Poster No.: C-2471 Congress: ECR 2015 Type: Educational Exhibit Authors: V. Rai#; Bjelovar/HR Keywords: Cysts, Cancer, Structured reporting, Ultrasound, MR,
Renal masses - the role of diagnostic imaging Poster No.: C-2471 Congress: ECR 2015 Type: Educational Exhibit Authors: V. Rai#; Bjelovar/HR Keywords: Cysts, Cancer, Structured reporting, Ultrasound, MR,
RADIOFREQUENCY ABLATION
 RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
Neuro-endocrine and pancreatic non-adenocarcinomas. Marc Engelbrecht, AMC, Amsterdam
 Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Neoplasms of the Canine, Feline and Lemur Liver:
 Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
MANAGEMENT RECOMMENDATIONS
 1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Fusion Ultrasound: Characterization of Abdominal Masses with MR, CT, PET, and Contrast Ultrasound
 Fusion Ultrasound: Characterization of Abdominal Masses with MR, CT, PET, and Contrast Ultrasound Mollie Rashid, MD Corinne Deurdulian, MD Hisham Tchelepi, MD Keck School of Medicine, University of Southern
Fusion Ultrasound: Characterization of Abdominal Masses with MR, CT, PET, and Contrast Ultrasound Mollie Rashid, MD Corinne Deurdulian, MD Hisham Tchelepi, MD Keck School of Medicine, University of Southern
Imaging of bone metastases
 Imaging of bone metastases Antoine Feydy Service de Radiologie B Hôpital Cochin APHP Université Paris Descartes antoine.feydy@aphp.fr MEXICO 2016 INTRODUCTION Diagnostic Imaging Imaging Modalities Strengths,
Imaging of bone metastases Antoine Feydy Service de Radiologie B Hôpital Cochin APHP Université Paris Descartes antoine.feydy@aphp.fr MEXICO 2016 INTRODUCTION Diagnostic Imaging Imaging Modalities Strengths,
Renal Masses in Patients with Known Extrarenal Primary Primary Cancer Primary Primary n Met Mets s RCC Beni L mphoma Lung Breast Others
 The Importance of Stuart G. Silverman, MD, FACR Professor of Radiology Harvard ard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston, MA The Importance of
The Importance of Stuart G. Silverman, MD, FACR Professor of Radiology Harvard ard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston, MA The Importance of
10 most frequently made mistakes with RECIST 1.1: how Radiologist can fail - and how to avoid them
 10 most frequently made mistakes with RECIST 1.1: how Radiologist can fail - and how to avoid them Poster No.: C-1689 Congress: ECR 2014 Type: Educational Exhibit Authors: M. Kekelidze, P. Lodise, M. Tozakidou,
10 most frequently made mistakes with RECIST 1.1: how Radiologist can fail - and how to avoid them Poster No.: C-1689 Congress: ECR 2014 Type: Educational Exhibit Authors: M. Kekelidze, P. Lodise, M. Tozakidou,
Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD
 Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures No relevant
Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures No relevant
REVIEW. Distinguishing benign from malignant adrenal masses
 Cancer Imaging (2003) 3, 102 110 DOI: 10.1102/1470-7330.2003.0006 CI REVIEW Distinguishing benign from malignant adrenal masses Isaac R Francis Professor of Radiology, Department of Radiology, University
Cancer Imaging (2003) 3, 102 110 DOI: 10.1102/1470-7330.2003.0006 CI REVIEW Distinguishing benign from malignant adrenal masses Isaac R Francis Professor of Radiology, Department of Radiology, University
Emerging Referral Patterns for Whole-Body Diffusion Weighted Imaging (WB-DWI) in an Oncology Center
 in an Oncology Center") Emerging Referral Patterns for Whole-Body Diffusion Weighted Imaging (WB-DWI) in an Oncology Center Poster No.: C-1296 Congress: ECR 2014 Type: Scientific Exhibit Authors: G. Petralia 1, G. Conte 1, S.
Emerging Referral Patterns for Whole-Body Diffusion Weighted Imaging (WB-DWI) in an Oncology Center Poster No.: C-1296 Congress: ECR 2014 Type: Scientific Exhibit Authors: G. Petralia 1, G. Conte 1, S.
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Diffusion Weighted Imaging in IBD: An Update Ethan A. Smith, MD
 Diffusion Weighted Imaging in IBD: An Update Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures Royalties from Elsevier
Diffusion Weighted Imaging in IBD: An Update Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures Royalties from Elsevier