None. Everyone, especially Dr. Mitchell for helping me find cases!
|
|
|
- Brian Stuart Hall
- 5 years ago
- Views:
Transcription
1
2 None. Everyone, especially Dr. Mitchell for helping me find cases!
3
4
5 Sagittal T1
6
7 Coronal T1
8
9 Axial T1
10
11 Sagital T1, Axial T1+, Axial T2
12
13 Axial CT +, thorax
14
15 Axial T1
16
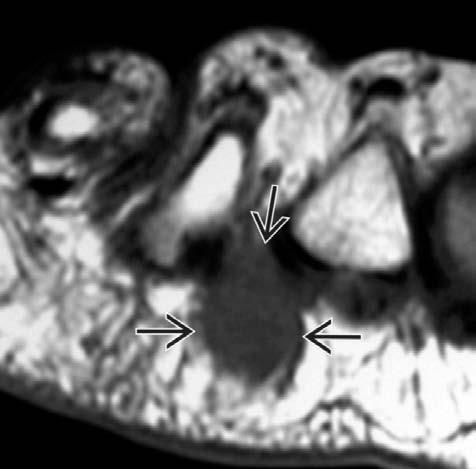
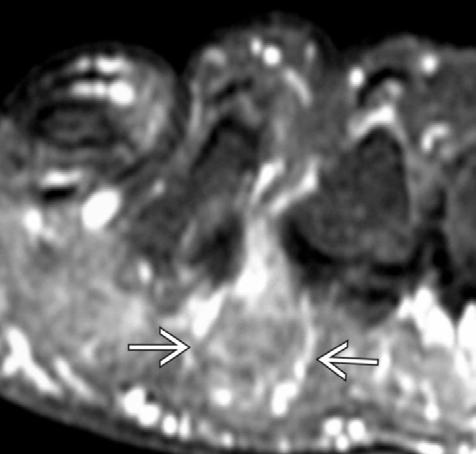
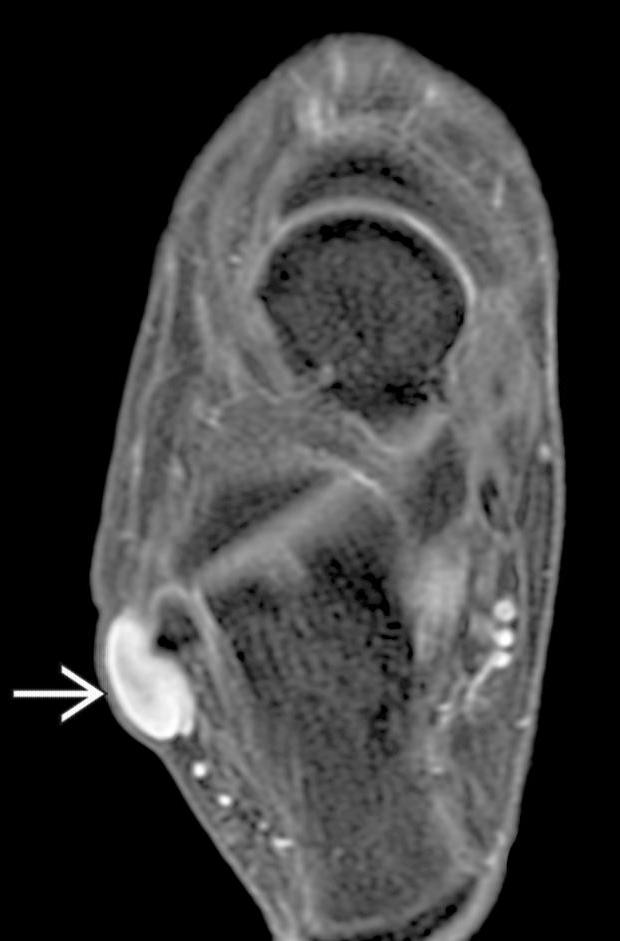
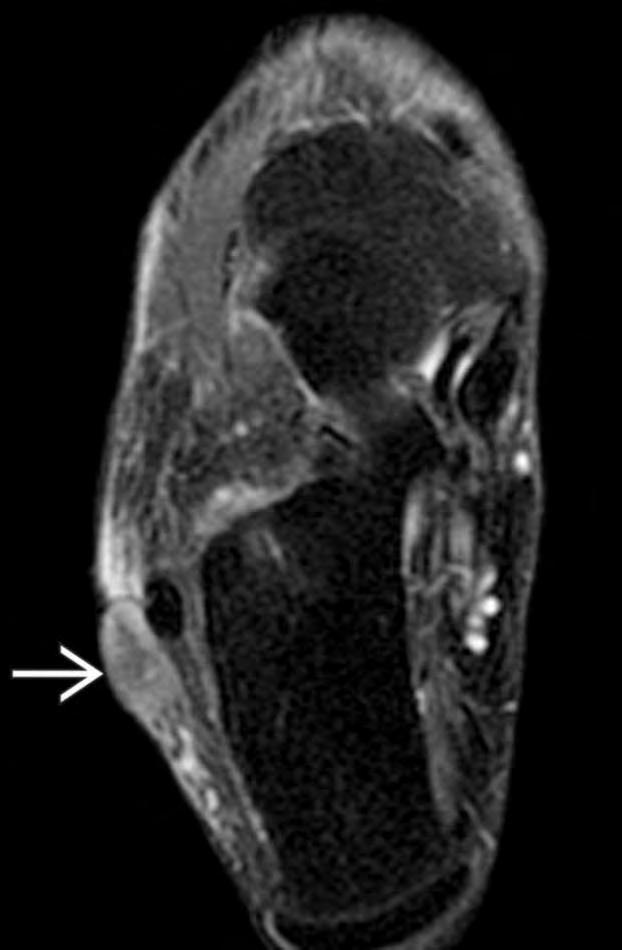
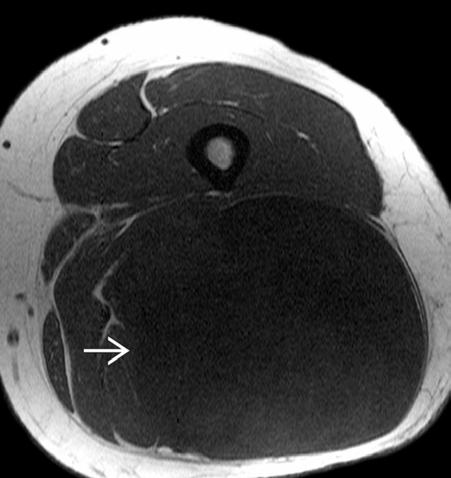
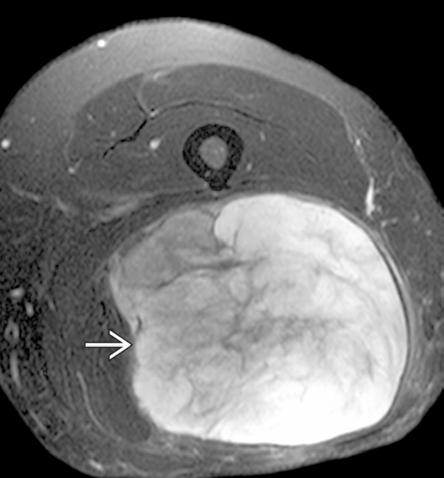
17 Within the muscle, not connected to a nerve or vessel Faint internal enhancement on T1+ (not shown) Axial T1 Axial T2
18
19 Review a systematic approach for work up of a soft tissue mass. Highlight key points of some of the more common entities.

20 Soft tissue arises from the mesenchyme. Which differentiates to: fat skeletal muscle peripheral nerves Blood vessels Fibrous tissue Figure 1: Soft tissue layers. <
21 1. Adipocytic 2. Fibroblastic/myofibroblastic 3. Fibrohistiocytic 4. Smooth muscle 5. Pericystic (perivascular) 6. Skeletal Muscle 7. Vascular 8. Chondro-osseous 9. Uncertain differentiaion
22 Review a systematic approach for work up of a soft tissue mass. Highlight key points of some of the more common entities.
23
24 Characterization of these soft-tissue lesions remains problematic, despite advances in imaging. Let s go over an approach, while highlighting some of these lesions.
25

26 Chan WP. Magnetic resonance imaging of soft-tissue tumors of the extremities: A practical approach. World Journal of Radiology. 2013;5(12): doi: /wjr.v5.i
27 Chan WP. Magnetic resonance imaging of soft-tissue tumors of the extremities: A practical approach. World Journal of Radiology. 2013;5(12): doi: /wjr.v5.i Determinate Lesions imaging features allowing a diagnosis without biopsy Indeterminate Lesions one that must be biopsied to ensure an accurate diagnosis

28 Chhabra and Soldatos. Soft-Tissue Lesions: When Can We Exclude Sarcoma? American Journal of Roentgenology. 2012;199: /AJR

29 Chhabra and Soldatos. Soft-Tissue Lesions: When Can We Exclude Sarcoma? American Journal of Roentgenology. 2012;199: /AJR

30 Wu JS, Hochman MG. Soft-tissue tumors and tumorlike lesions: a systematic imaging approach. Radiology 2009; 253:
31 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
32 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
33 Important information: Age (eg: liposarcomas are rare in children) Hx of trauma (hematoma, myositis ossificans) History of malignancy or familial syndromes (metastasis, radiation induced sarcoma, NF type 1) Mass characteristics (rapid growth, size fluctuation, mobile,etc).
34
35
36 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
37 Some masses occur in specific locations. You just have to know them. - Let s look at some!
38 Axial CT +, thorax
39 Axial CT +, thorax

40 Axial CT +, thorax
41 Axial CT +, thorax
42 Axial CT +, thorax
43 Axial CT +, thorax
44 Axial CT +, thorax
45 Axial CT +, thorax
46 Axial CT +, thorax
47 Axial CT +, thorax
48 Axial CT +, thorax
49 Axial CT +, thorax
50 Axial CT +, thorax
51 Axial CT +, thorax
52 Axial CT +, thorax
53 Axial CT +, thorax
54 Axial CT +, thorax
55 Axial CT +, thorax
56 Axial CT +, thorax
57 Axial CT +, thorax
58 Axial CT +, thorax
59 Axial CT +, thorax
60 Axial CT +, thorax
61 Subscapular mass deep to serratus anterior. 99% in subscapular region % bilateral Mean age: years. F > M Slow growth, no malignant degeneration CT imaging findings: Poorly defined, lenticular, heterogeneous soft tissue mass Linear low-attenuation streaks from internal fat Majority of lesion has attenuation similar to muscle
")

62 (distal fingers) Coronal T2 Coronal T1
63 Mesenchymal neoplasm of smooth muscle cells similar to glomus body cells Propensity to subungual region. Fingers and toes most common 99% benign, but often painful. MR imaging findings: Isointense to nail bed or muscle on T1 Hyperintense on T2
64 Case reports of other locations:
65 (Metatarsals) Coronal T1 Coronal T1 post gad Coronal T2

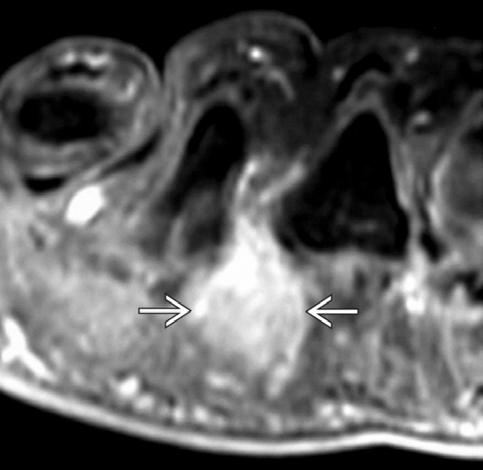
66 Painful, benign fibrosing process of plantar digital nerve between 3rd and 4th metatarsal heads. most common. F>M MR imaging findings: Hypo to Isointense on T1 Iso to Hyperintense on T2 Variable enhancement
67 Sagittal T1
68 Benign discrete nodule along plantar fascia. Ages years M:F = 1:1 MR imaging findings: Isointense on T1 Hypo to isointense on T2
69 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
70 Only a few things arise from a nerve: PNSTs (schwannomas and neurofibromas) If fat, consider Neural fibrolipoma/fibrolipomatous hamartoma
71 Sagital T2, elbow
72 Sagital T2, elbow
73 Sagital T2, elbow
74 Sagital T2, elbow

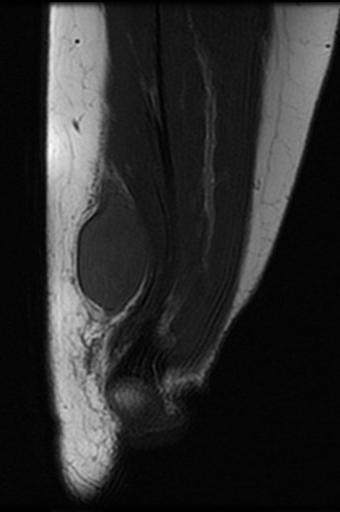
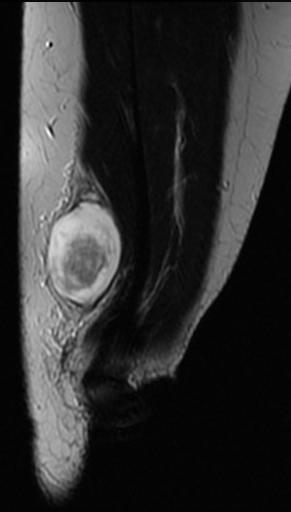
75 Sagital T2, elbow
76 Sagital T2, elbow
77 Sagital T2, elbow
78 Sagital T2, elbow

79
80 Neurofibromas Schwannoma Malignant Peripheral Nerve Sheath Tumors
81 Benign PNST with neoplastic tissue inseparable from normal nerve Localized NF: 90% of cases, primarily affect superficial cutaneous nerves, can affect larger deeper nerves Diffuse NF: Ill-defined plaque-like in the subcutaneous tissue Plexiform NF: Long segments of diffusely and irregularly enlarged nerves. Multilobulated. Pathgonomic for NF1.
82 Arises in 2nd to 3rd decade of life Low risk of malignant transformation (though higher risk with the deeper lesions). Painless, slowly growing nodule
83 Iso to mildly hyperintense (Hypointense also possible) on T1 Split-fat sign = peripheral rim of fat Hyperintense on T2 Variable heterogeneity Target sign = central low signal focus Fascicular sign = multiple small ring-like structures + enhancement, most prominent centrally

84 Coronal T1 Coronal T2 Coronal T1+
85 In contrast to schwanomas, neurofibromas incorporate many cell types in addition to Schwann cells May be impossible to differentiate from a neurofibroma from a schwanoma via imaging.
86 Encapsulated benign peripheral nerve sheath tumor typically located eccentrically on normal nerve Upper and lower extremity flexor surface nerves Well-defined, solitary fusiform mass Most common in 2nd to 5th decades of life Painless, slowly growing
87 Iso to hyperintense on T1 Split-fat sign = thin peripheral rim of fat May have subtle muscle atrophy distal to lesion Hyperintense on T2 Target sign = central low signal region Fascicular sign = multiple small ring-like structures Diffuse enhancement (often greater than neurofibroma) is typical.
88 Sagital T1, Axial T1+, Axial T2
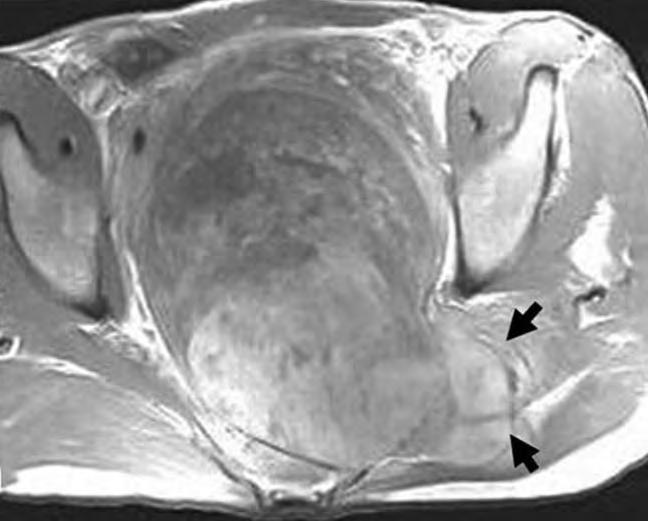
89 Infiltrative, often invasive, fusiform mass > 5 cm Large to medium deep nerves (Sciatic nerve > brachial plexus, sacral plexus) Proximal extremities, retroperitoneum, posterior mediastinum Malignant spindle cell sarcoma of neural origin % associated with NF % radiation-induced 5-year survival rate: 23-44%
90 Heterogeneously hypo- to hyperintense on T1WI MR Heterogeneously hyperintense on fluidsensitive MR ± hemorrhagic fluid-fluid levels Intense heterogeneous enhancement Diffuse, peripheral or nodular patterns

91 Sagittal T2 and Axial T1.
92 Does it arrive from a vessel? Hemangioma would be the most common Other possibilities include lymphangiomas and angiosarcomas. If there is a Hx of trauma, consider a pseudoaneurysm.
93 Does it arrive from a tendon sheath? Most commonly would be a Giant Cell Tumor of the tendon sheath. Nonetheless, ganglia, lipomas and fibromas can all arise from tendon sheaths.

94 nodular tenosynovitis, tenosynovial giant cell tumor, Benign synovial proliferation within tendon sheath same pathologic entity as pigmented villonodular synovitis (PVNS)
95 85% in fingers. Hand > wrist > ankle/foot > knee > elbow > hip years. M:F = 2:1 Local recurrence in 4-44% Radiographs: Nonspecific soft tissue fullness. Cortical erosion in 10-28%
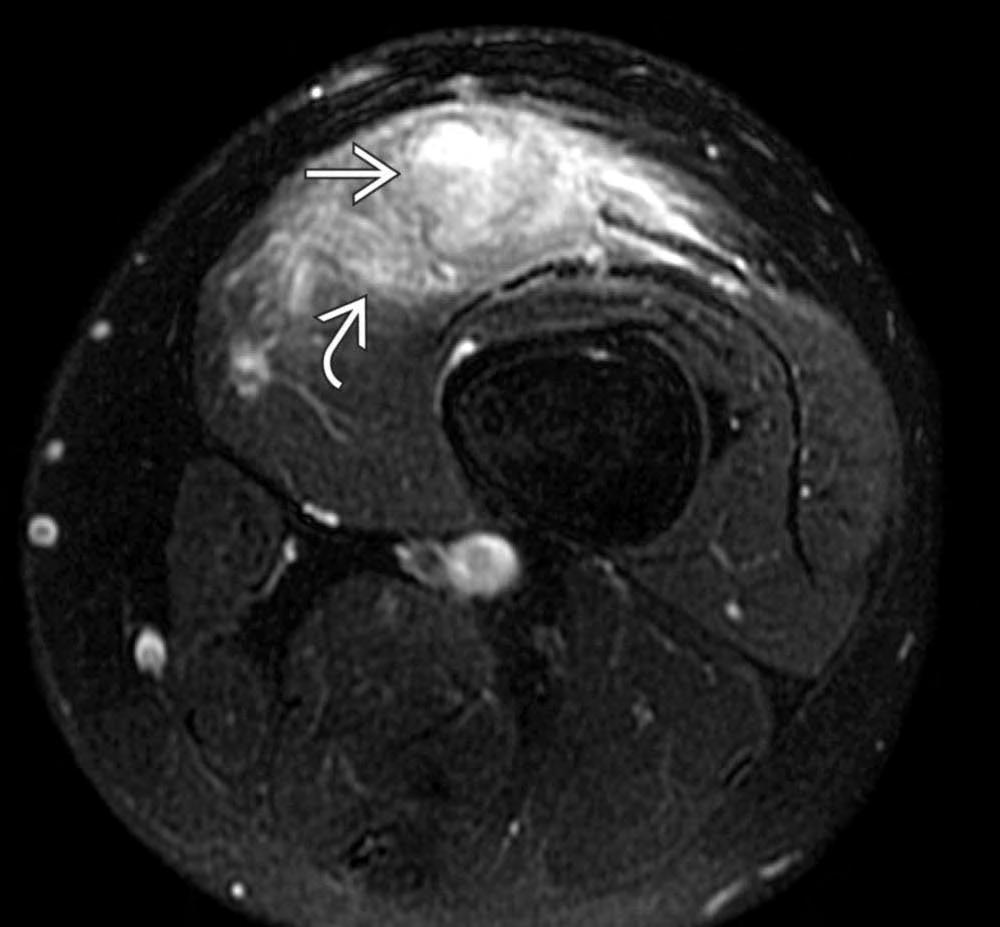
96 Inhomogeneous low to intermediate signal intensity on T1 and T2 "bloom" on gradient-echo imaging Intense enhancement ± inhomogeneity


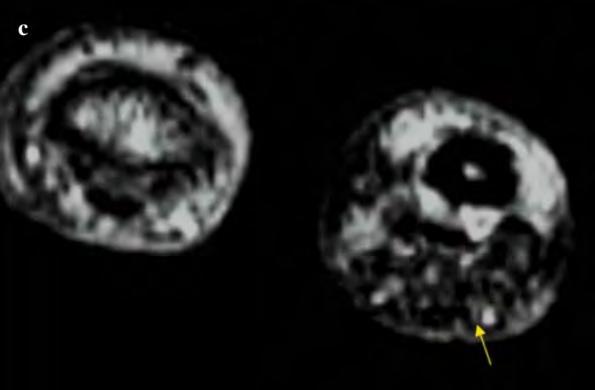
97 Axial T1, Axial T2 and Gradient Echo
98 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
99 They should be assessed for: distortion of tissue planes, radiolucent fat indolent or aggressive remodeling of the bone soft-tissue calcifications or ossification.
100
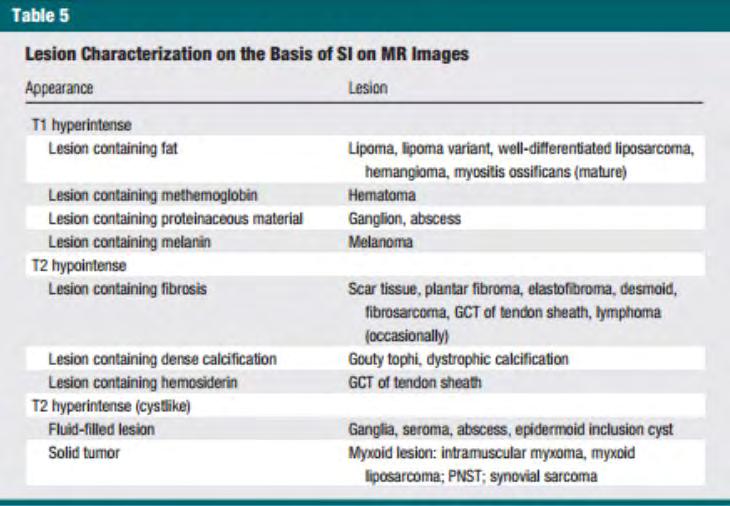
101
102

103
104 Heterotopic formation of bone and cartilage in soft tissue At the site of injured muscle (quads/arms most common). Classic appearance: Mature bone formation within soft tissues. Early stages can be confusing and non specific.
105 Myositis is misleading May also be found in fascia, tendons, & fat. "Heterotopic ossification" is more correct term
106 0-2 weeks: Soft tissue mass with indistinct surrounding soft tissue planes 3-4 weeks: Amorphous osteoid forms within mass; adjacent periosteal reaction may be seen 6-8 weeks: Sharper cortex begins to form about lacy central osseous mass 5-6 months: Mature bone formation


107 Axial T2, Radiograph and Sagittal CT
108 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
109 MRI is the most effective for tissue characterization. As usual, the signal intensity of T1 and T2 weighted images are compared to muscle
110
111 This isn t useful, too many lesions with these signal characteristics.
112 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
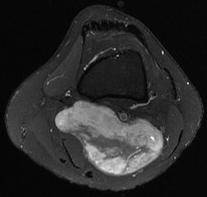
113 Consider this flow chart:
114
115

116 Benign adipocytic tumors Intermediate adipocytic tumors Malignant adipocytic tumors
117 Lipoma Lipomatosis Nerve Lipomatosis Lipoma Arborescens, Knee Lipoblastoma (pediatrics) Hibernoma Parosteal Lipoma

118 Benign Adipocytic tumors Same signal as fat Only thin septa (< 2mm) No nodules While calcification can occur, it should raise suspicion. Axial T1

119 Benign Adipocytic tumors Same signal as fat Disorganized and poorly circumscribed fat overgrowth Associated with various syndromes Axial T1
120 Benign Adipocytic tumors 78-96% in upper extremity (80% in median nerve distribution) Collection of enlarged cylindrical fascicles along course of nerve, like a coaxial cable Axial T1

121 Benign Adipocytic tumors Most common in suprapatellar recess of knee joint Frond-like or globular pattern of fat proliferating from synovial membrane Treat w/synovectomy Sagital T2

122 Benign Adipocytic tumors Rare, benign tumor of brown adipose tissue Needs biopsy, because imaging alone can t exclude non benign lipomatous lesions More complex then a lipoma, multiple septa and prominent vascularity Axial T1
123 Benign Adipocytic tumors Fatty lesion arising from bone surface Approximately 33% adjacent to femur Internal calcifications, septa, ossifications Adjacent bone shows osseous excrescence and bone cortex changes, such as thicknening
124 Atypical lipomatous tumor or Well-differentiated liposarcoma
125 Intermediate Adipocytic tumors or Intermediate, locally aggressive neoplasm predominantly composed of fat typically composed of > 75% fat with septa and variable nodularity Does not metastasize. 0% mortality for lesions in extremities 80% mortality for retroperitoneal lesions
126 Intermediate Adipocytic tumors or Axial T1
127 Liposarcoma
128 Malignant Adipocytic tumors Typically ages In extremities or retroperitoneum. 5 types: Well-differentiated commonest, low grade, Myxoid - intermediate grade Round Cell/de-differentiated, high grade Pleomorphic, high grade Mixed
129 Malignant Adipocytic tumors Low grade lesions are almost entirely fat signal with thick septa, nodules +/- evidence of local invasion. The higher grade lesions are often devoid of macroscopic fat and have appearances similar to other sarcomas.


130 Malignant Adipocytic tumors Axial CT Sagital T1

131 Axial PD FatSat
132 Axial PD FatSat

133 Axial PD FatSat

134 Axial PD FatSat

135 Axial PD FatSat

136 Axial PD FatSat
137 Axial PD FatSat

138 Axial PD FatSat

139 Axial PD FatSat
140 Axial PD FatSat
141 Axial PD FatSat
142 Axial PD FatSat

143 Axial PD FatSat

144 Axial PD FatSat

145 Axial PD FatSat

146 Axial PD FatSat
147 Axial PD FatSat
148 Axial PD FatSat

149 Axial PD FatSat
150 Axial PD FatSat

151 Axial PD FatSat
152 Axial PD FatSat

153 Axial PD FatSat

154 Axial PD FatSat
155 Axial PD FatSat

156 Axial PD FatSat
157 Axial PD FatSat

158 Axial PD FatSat
159 Axial PD FatSat

160 Axial PD FatSat
161 Axial PD FatSat

162 Axial PD FatSat
163 Axial PD FatSat
164 Axial PD FatSat

165 Axial PD FatSat

166 Axial PD FatSat

167 Axial PD FatSat
168 Axial PD Fatsat Axial T1 Axial T1 FatSat Axial T1 FatSat +


169 Axial PD Fatsat Axial T1 Axial T1 FatSat Axial T1 FatSat +
170
171
172
173
174
175 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
176 Divide the differential into 3 categories: 1. Fibrosis 2. Hemosiderin 3. Calcification
177
178
179 Can still be hyperintense on T2!
180 Benign neoplasm originating from smooth muscle Punctate, plaque-like, or "popcorn" calcifications Iso to slightly hyperintense T1 Hypo to hyperintense on T2. Excision, rare recurrence Subcutaneous lesions are small <2cm Deep lesions are larger

181 Axial T1 Axial T2 Axial T1+
182 Malignant fibroblastic/myofibroblastic neoplasm Often in deep soft tissues of extremities Commonly 3-8 cm at presentation Variable appearance depending on cellular content. Thus heterogenous appearance that can be low to high signal intensity on T1 and T2 Estimated 39-54% 5-year survival Metastases in 9-63%

183 Axial T2 Axial T1+
184 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
185 Look at the enhancement pattern. Is it rim enhancing, or demonstrate internal enhancing components?
186
187
188 Axial T1 Axial T2 Rare benign type of soft tissue myxoma 40 to 70 years. F>M homogeneous low T1, high T2, mild internal enhancement Simple excision is curative
189 Fibroblastic soft tissue sarcoma involving elderly patients years. Low grade: homogeneous low T1, high T2, mild internal enhancement High Grade: heterogeneous intermediate T1, high T2, intense enhancement ± hemorrhage, necrosis High local recurrence rate (38-79%). Even with lowgrade tumors

190
191 Malignant soft tissue tumor of uncertain differentiation. 95% in the extremities, Often in the knees years of age Does not arise from synovium. 5-year survival rate: 27-76% Metastases in up to 41%
192 Imaging findings are not pathognomonic. Iso to slightly hyperintense on T1 and heterogeneous Mostly hyperintense on T2. Markedly heterogeneous. Calcification in 1/3 but extent variable "Triple" sign = multiple signal intensities due to hemorrhage, necrosis, solid tissue, and calcification "Bowl of grapes" sign = multiloculated appearance of mass with internal septa Fluid Fluid levels = Intra-tumoral hemorrhage Enhancement is usually prominent and can be diffuse, heterogeneous or peripheral.
193 Due to variable appearance any soft tissue mass near a joint, especially containing calcification, should not be dismissed as being benign.


194 Coronal T1 Coronal T2 Fatsat

195 Axial PD Axial T1+


196 Sagittal and Axial T2 Fluid Fluid levels and Triple Sign Coronal T2 Bowl of Grapes sign
197 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
198 While a systematic approach can narrow a differential, it is not comprehensive. If a lesion can not be confidently diagnosed then it is an intermediate lesion.
199 According to WHO soft tissue masses that do not demonstrate tumor-specific features on MR images should be considered indeterminate and biopsy should always be obtained to exclude malignancy.
200 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
201
202
203 Sagittal T1
204
205 Sagittal T1
206
207 Coronal T1
208
209 Coronal T1
210
211 Axial T1
212
213 Axial T1
214
215 Sagital T1, Axial T1+, Axial T2
216



217 Sagital T1, Axial T1+, Axial T2
218
219 Axial CT +, thorax
220
221 Axial CT +, thorax
222
223 Axial T1
224
225 Axial T1
226 Axial T1 or
227
228 Within the muscle, not connected to a nerve or vessel Faint internal enhancement on T1+ (not shown) Axial T1 Axial T2
229
230 Axial T1 Axial T2
231
232 1. Clinical History 2. Location 3. Does it arise from something? 4. What does the radiograph show? 5. Is it hyperintense on T1? 6. Is it hypointense on T2? 7. Is it hyperintense on T2?
233 Question 5 quiz: Walker, C. Elastofibroma Slide 62: Roberts, C. Glomus Tumor Slide 65: Blankenbaker, D. Morton Neuroma Slide 67: Unknown author. Plantar Fibroma Slide 88: Roberts, C. Schwannoma Slide 91: Chen, K., Zhou, M., Yang, H., Qian, Z., Wang, G., Wu, G.... Sun, Z. (2013). Pre-operative embolization facilitating a posterior approach for the surgical resection of giant sacral neurogenic tumors. Oncology Letters, 6, Slide 95: Roberts, C. Giant Cell Tumor of the Tendon Sheath Slide 97: Wan, J., Magarelli, N., Peh, W. et al. Giant Cell Tumor of the Tendon Sheath Radiol med (2010) 115: 141. doi: /s
234 Slide 101: Roberts, C. Hemangioma Slide 103 and 107: Banaster, M. Myositis Ossificans Slide 118: Roberts, C, Lipoma Slide 119: Roberts, C. Lipomatosis Slide 120: Roberts C. Lipomatosis of a nerve b759d6caf025 Slide 121: Weerakkody et al. Lipoma Arborescens Slide 122: Goel, A at al. Hibernoma Slide 123: Lawson, A. Parosteal lipoma Slide 126: Nicoletti, D. Atypical lipomatous tumor Slide 130: Di Muzio, B. and Gaillard et Al. Liposarcoma Slide 181: Roberts, C. Leiomyoma Slide 183: Roberts, C. Fibrosarcoma, Soft Tissue f5e?searchTerm=fibrosarcoma
235 Slide 188: Weerakkody et al. Intramuscular Myxoma Slide 190: Roberts, C. Myxofibrosarcoma Slide : Di Muzio, B. and Gaillard, F. et al. Synovial Sarcoma
236 Chan WP. Magnetic resonance imaging of soft-tissue tumors of the extremities: A practical approach. World Journal of Radiology. 2013;5(12): doi: /wjr.v5.i Chen, K., Zhou, M., Yang, H., Qian, Z., Wang, G., Wu, G.... Sun, Z. (2013). Pre-operative embolization facilitating a posterior approach for the surgical resection of giant sacral neurogenic tumors. Oncology Letters, 6, Chhabra and Soldatos. Soft-Tissue Lesions: When Can We Exclude Sarcoma? American Journal of Roentgenology. 2012;199: /AJR Wu JS, Hochman MG. Soft-tissue tumors and tumorlike lesions: a systematic imaging approach. Radiology 2009; 253: Wan, J., Magarelli, N., Peh, W. et al. Giant Cell Tumor of the Tendon Sheath Radiol med (2010) 115: 141. doi: /s Roberts, C. Glomus Tumor 26a9-43eb-8d97-98fdcc9330cd Roberts, C. Neurofibroma Roberts, C. Giant Cell Tumor of the Tendon Sheath Roberts, C, Lipoma Roberts, C. Lipomatosis Roberts C. Lipomatosis of a nerve
237 Roberts, C. Leiomyoma Roberts, C. Fibrosarcoma, Soft Tissue Roberts, C. Myxofibrosarcoma Walker, C. Elastofibroma Di Muzio, B. and Gaillard, F. et al. Synovial Sarcoma Banaster, M. Myositis Ossificans


238
Case 8 Soft tissue swelling
 Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
5/10. Pathology Soft tissue tumors. Farah Bhani. Mohammed Alorjani
 5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
Contents Part I Introduction 1 General Description 2 Natural History: Importance of Size, Site, Histopathology
 Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
* I have no disclosures or any
 Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
Musculoskeletal Sarcomas
 Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Case Presentation 主治醫師 : 宋文鑫日期 :
 Case Presentation 主治醫師 : 宋文鑫日期 : 2015-2-28 General Data Name:OOO Chart Number:OOOOOOO Date of Admission:2014 年 08 月 04 日 Age: 33 y/o Sex:female Occupation : 會計 Chief Complaint Palpable soft tissue mass
Case Presentation 主治醫師 : 宋文鑫日期 : 2015-2-28 General Data Name:OOO Chart Number:OOOOOOO Date of Admission:2014 年 08 月 04 日 Age: 33 y/o Sex:female Occupation : 會計 Chief Complaint Palpable soft tissue mass
Figuring out the "fronds"-synovial proliferative disorders of the knee.
 Figuring out the "fronds"-synovial proliferative disorders of the knee. Poster No.: C-1209 Congress: ECR 2014 Type: Educational Exhibit Authors: S. Sivasubramanian; Tamil Nadu/IN Keywords: Imaging sequences,
Figuring out the "fronds"-synovial proliferative disorders of the knee. Poster No.: C-1209 Congress: ECR 2014 Type: Educational Exhibit Authors: S. Sivasubramanian; Tamil Nadu/IN Keywords: Imaging sequences,
Ultrasound Evaluation of Masses
 Ultrasound Evaluation of Masses Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Advisory Panel: GE,
Ultrasound Evaluation of Masses Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Advisory Panel: GE,
Case 9087 Retropharyngeal nodular fasciitis
 Case 9087 Retropharyngeal nodular fasciitis Santiago I 1; Cavalheiro F 2; Noruégas MJ 3; Sanches MC3 1 Hospital Infante D. Pedro, Aveiro, Portugal 2 Hospitais da Universidade de Coimbra, Portugal 3 Hospital
Case 9087 Retropharyngeal nodular fasciitis Santiago I 1; Cavalheiro F 2; Noruégas MJ 3; Sanches MC3 1 Hospital Infante D. Pedro, Aveiro, Portugal 2 Hospitais da Universidade de Coimbra, Portugal 3 Hospital
Giant-cell tumor of the tendon sheath: when must we suspect it?
 Giant-cell tumor of the tendon sheath: when must we suspect it? Poster No.: C-0538 Congress: ECR 2014 Type: Educational Exhibit Authors: C. Santos Montón, J. M. Alonso Sánchez, D. C. Cuellar, P. A. Chaparro
Giant-cell tumor of the tendon sheath: when must we suspect it? Poster No.: C-0538 Congress: ECR 2014 Type: Educational Exhibit Authors: C. Santos Montón, J. M. Alonso Sánchez, D. C. Cuellar, P. A. Chaparro
Tumors of Adipose Tissue Tumors Epidemiology Clinical Features. Morphology. Mature Adipocytes Separated by delicate fibrous septa
 Tumors of Adipose Tissue Lipoma Liposarcoma Most commonly happens in female The most common soft tissue tumor o Originates from matured Adipocytes Most commonly happes at the 4 th and 5 th decade of life
Tumors of Adipose Tissue Lipoma Liposarcoma Most commonly happens in female The most common soft tissue tumor o Originates from matured Adipocytes Most commonly happes at the 4 th and 5 th decade of life
Mayo Medical Laboratories
 Mayo Medical Laboratories Virtual Lectures 2014 MFMER 2016 MFMER slide-1 Virtual Lectures Planning Committee Disclosure Summary As a provider accredited by ACCME, College of Medicine, Mayo Clinic (Mayo
Mayo Medical Laboratories Virtual Lectures 2014 MFMER 2016 MFMER slide-1 Virtual Lectures Planning Committee Disclosure Summary As a provider accredited by ACCME, College of Medicine, Mayo Clinic (Mayo
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
Soft tissue lipomas, lipoma variants and liposarcomas: MRI evaluation and review of literature
 Soft tissue lipomas, lipoma variants and liposarcomas: MRI evaluation and review of literature Poster No.: R-0122 Congress: RANZCR-AOCR 2012 Type: Authors: Keywords: DOI: Educational Exhibit A. A. Tandon,
Soft tissue lipomas, lipoma variants and liposarcomas: MRI evaluation and review of literature Poster No.: R-0122 Congress: RANZCR-AOCR 2012 Type: Authors: Keywords: DOI: Educational Exhibit A. A. Tandon,
Mark D. Murphey, MD, FACR
 Fundamental Concepts of Musculoskeletal Neoplasm: CT and MRI Mark D. Murphey, MD, FACR Important Features in Evaluation of Musculoskeletal Masses Differential diagnosis Preoperative assessment and staging
Fundamental Concepts of Musculoskeletal Neoplasm: CT and MRI Mark D. Murphey, MD, FACR Important Features in Evaluation of Musculoskeletal Masses Differential diagnosis Preoperative assessment and staging
Fun with Fat. General Rules. Case
 Fun with Fat General Rules Imaging: location (deep vs. superficial) Superficial lesions are seldom liposarcomas Deep lesions may be benign or malignant Myxoid stroma is common in benign and malignant lesions
Fun with Fat General Rules Imaging: location (deep vs. superficial) Superficial lesions are seldom liposarcomas Deep lesions may be benign or malignant Myxoid stroma is common in benign and malignant lesions
Myositis Ossificans Mimicking Sarcoma, the Importance of Diagnostic Imaging Case Report
 Signature: Pol J Radiol, 2014; 79: 228-232 DOI: 10.12659/PJR.890209 CASE REPORT Received: 2013.12.18 Accepted: 2014.01.27 Published: 2014.07.28 Authors Contribution: A Study Design B Data Collection C
Signature: Pol J Radiol, 2014; 79: 228-232 DOI: 10.12659/PJR.890209 CASE REPORT Received: 2013.12.18 Accepted: 2014.01.27 Published: 2014.07.28 Authors Contribution: A Study Design B Data Collection C
Imaging of Ankle and Foot pain
 Imaging of Ankle and Foot pain Pramot Tanutit, M.D. Department of Radiology Faculty of Medicine, Prince of Songkla University 1 Outlines Plain film: anatomy Common causes of ankle and foot pain Exclude:
Imaging of Ankle and Foot pain Pramot Tanutit, M.D. Department of Radiology Faculty of Medicine, Prince of Songkla University 1 Outlines Plain film: anatomy Common causes of ankle and foot pain Exclude:
Radiological Reasoning: Acutely Painful Swollen Finger. Musculoskeletal Imaging Chew and Richardson Benign-Appearing Bone Mass.
 Musculoskeletal Imaging Chew and Richardson Benign-Appearing Bone Mass AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY This Radiological Reasoning article is available for SAM credit and CME credits
Musculoskeletal Imaging Chew and Richardson Benign-Appearing Bone Mass AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY This Radiological Reasoning article is available for SAM credit and CME credits
DOWNLOAD OR READ : TUMORS AND TUMOR LIKE CONDITIONS OF THE LUNG AND PLEURA PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : TUMORS AND TUMOR LIKE CONDITIONS OF THE LUNG AND PLEURA PDF EBOOK EPUB MOBI Page 1 Page 2 tumors and tumor like conditions of the lung and pleura tumors and tumor like pdf tumors and
DOWNLOAD OR READ : TUMORS AND TUMOR LIKE CONDITIONS OF THE LUNG AND PLEURA PDF EBOOK EPUB MOBI Page 1 Page 2 tumors and tumor like conditions of the lung and pleura tumors and tumor like pdf tumors and
Calcifying Aponeurotic Fibroma of the Knee: a Case Report with Radiographic and MRI Finding
 pissn 2384-1095 eissn 2384-1109 imri 2017;21:259-263 Calcifying Aponeurotic Fibroma of the Knee: a Case Report with Radiographic and MRI Finding Seung Hyun Lee 1,2, In Sook Lee 1,2, You Seon Song 1,2,
pissn 2384-1095 eissn 2384-1109 imri 2017;21:259-263 Calcifying Aponeurotic Fibroma of the Knee: a Case Report with Radiographic and MRI Finding Seung Hyun Lee 1,2, In Sook Lee 1,2, You Seon Song 1,2,
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
Takayuki Ohguri 1 Takatoshi Aoki 1 Masanori Hisaoka 2 Hideyuki Watanabe 1 Katsumi Nakamura 1 Hiroshi Hashimoto 2 Toshitaka Nakamura 3 Hajime Nakata 1
 Takayuki Ohguri 1 Takatoshi Aoki 1 Masanori Hisaoka 2 Hideyuki Watanabe 1 Katsumi Nakamura 1 Hiroshi Hashimoto 2 Toshitaka Nakamura 3 Hajime Nakata 1 Received July 1, 2002; accepted after revision November
Takayuki Ohguri 1 Takatoshi Aoki 1 Masanori Hisaoka 2 Hideyuki Watanabe 1 Katsumi Nakamura 1 Hiroshi Hashimoto 2 Toshitaka Nakamura 3 Hajime Nakata 1 Received July 1, 2002; accepted after revision November
Primary Retroperitoneal Myxofibrosarcoma: a case report and review of the literature
 J Radiol Sci 2014; 39: 57-62 Primary Retroperitoneal Myxofibrosarcoma: a case report and review of the literature Chih-Yu Chen 1 Yueh-Min Lin 2 Shang-Yun Ho 1 Kwo-Whei Lee 1 Ching Hsueh 1 Department of
J Radiol Sci 2014; 39: 57-62 Primary Retroperitoneal Myxofibrosarcoma: a case report and review of the literature Chih-Yu Chen 1 Yueh-Min Lin 2 Shang-Yun Ho 1 Kwo-Whei Lee 1 Ching Hsueh 1 Department of
MRI IN NONOSSEOUS ABNORMALITIES OF THE FOREFOOT: A PICTORIAL REVIEW
 MRI IN NONOSSEOUS ABNORMALITIES OF THE FOREFOOT: A PICTORIAL REVIEW I Delgado, P Melloni, M Veintemillas, R Valls, M Vilagran, A Valera UDIAT. Sabadell (Barcelona). Spain. PURPOSE To catalog the wide spectrum
MRI IN NONOSSEOUS ABNORMALITIES OF THE FOREFOOT: A PICTORIAL REVIEW I Delgado, P Melloni, M Veintemillas, R Valls, M Vilagran, A Valera UDIAT. Sabadell (Barcelona). Spain. PURPOSE To catalog the wide spectrum
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Index. Note: Page numbers of article titles are in boldface type.
 Magn Reson Imaging Clin N Am 12 (2004) 185 189 Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint, MR imaging findings concerning, 161 Acromion, types of, 77 79
Magn Reson Imaging Clin N Am 12 (2004) 185 189 Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint, MR imaging findings concerning, 161 Acromion, types of, 77 79
3/27/2017. Disclosure of Relevant Financial Relationships
 Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
MRI XR, CT, NM. Principal Modality (2): Case Report # 2. Date accepted: 15 March 2013
: Case Report # 2. Date accepted: 15 March 2013") Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
Monophasic Synovial Carcinoma of knee joint- A Case Report and Review of Literature
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.5 March. (2018), PP 13-17 www.iosrjournals.org Monophasic Synovial Carcinoma of knee
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.5 March. (2018), PP 13-17 www.iosrjournals.org Monophasic Synovial Carcinoma of knee
Spectrum of MRI Findings of Synovial Sarcoma
 Spectrum of MRI Findings of Synovial Sarcoma Poster No.: C-1523 Congress: ECR 2014 Type: Educational Exhibit Authors: J. A. Molina, J. Llauger Rosselló, J. Palmer Sancho, G. M. 1 1 2 1 3 1 1 Santandreu,
Spectrum of MRI Findings of Synovial Sarcoma Poster No.: C-1523 Congress: ECR 2014 Type: Educational Exhibit Authors: J. A. Molina, J. Llauger Rosselló, J. Palmer Sancho, G. M. 1 1 2 1 3 1 1 Santandreu,
GIANT RETROPERITONEAL LIPOSARCOMA: IMAGING AND LITERATURE Amit Kumar 1, Sanjay K. Suman 2, Bipin Kumar 3, Sumit Kumar 4
 GIANT RETROPERITONEAL LIPOSARCOMA: IMAGING AND LITERATURE Amit Kumar 1, Sanjay K. Suman 2, Bipin Kumar 3, Sumit Kumar 4 HOW TO CITE THIS ARTICLE: Amit Kumar, Sanjay K. Suman, Bipin Kumar, Sumit Kumar.
GIANT RETROPERITONEAL LIPOSARCOMA: IMAGING AND LITERATURE Amit Kumar 1, Sanjay K. Suman 2, Bipin Kumar 3, Sumit Kumar 4 HOW TO CITE THIS ARTICLE: Amit Kumar, Sanjay K. Suman, Bipin Kumar, Sumit Kumar.
Introduction to Musculoskeletal Tumors. James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon
 Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Retroperitoneal Sarcomas - A pictorial review
 Retroperitoneal Sarcomas - A pictorial review Poster No.: C-1409 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Douraghi-Zadeh, K. L. Shahabuddin, R. H. Thomas, E. Moskovic; London/UK Keywords:
Retroperitoneal Sarcomas - A pictorial review Poster No.: C-1409 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Douraghi-Zadeh, K. L. Shahabuddin, R. H. Thomas, E. Moskovic; London/UK Keywords:
Retroperitoneal tumors: Computed Tomography (CT) and Magnetic Resonance (MR) patterns
 and Magnetic Resonance (MR) patterns") Retroperitoneal tumors: Computed Tomography (CT) and Magnetic Resonance (MR) patterns Poster No.: C-1369 Congress: ECR 2011 Type: Educational Exhibit Authors: G. Cardone, A. Messina, D. Vergnaghi, P. Mangili,
Retroperitoneal tumors: Computed Tomography (CT) and Magnetic Resonance (MR) patterns Poster No.: C-1369 Congress: ECR 2011 Type: Educational Exhibit Authors: G. Cardone, A. Messina, D. Vergnaghi, P. Mangili,
Retroperitoneal tumors: Computed Tomography (CT) and Magnetic Resonance (MR) patterns
 and Magnetic Resonance (MR) patterns") Retroperitoneal tumors: Computed Tomography (CT) and Magnetic Resonance (MR) patterns Poster No.: C-1369 Congress: ECR 2011 Type: Educational Exhibit Authors: G. Cardone, A. Messina, D. VERGNAGHI, P. Mangili,
Retroperitoneal tumors: Computed Tomography (CT) and Magnetic Resonance (MR) patterns Poster No.: C-1369 Congress: ECR 2011 Type: Educational Exhibit Authors: G. Cardone, A. Messina, D. VERGNAGHI, P. Mangili,
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Bizarre parosteal osteochondromatous proliferation
 * * Bizarre Parosteal Osteochondromatous Proliferation A Case Report with Literature Review Chi-Fu Kao Yang-Chih Lin Yu-Hung Wu Be-Fong Chen* We report the case of a 12-year-old female with a slowly erythematous
* * Bizarre Parosteal Osteochondromatous Proliferation A Case Report with Literature Review Chi-Fu Kao Yang-Chih Lin Yu-Hung Wu Be-Fong Chen* We report the case of a 12-year-old female with a slowly erythematous
Myxo-inflammatory Fibroblastic sarcoma
 AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
Essentials of Clinical MR, 2 nd edition. 51. Primary Neoplasms
 51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
WHAT IS MDM2? (MDMTWOMICS) MDM2 IN SARCOMAS? (MDMTWOMAS) MDM2MICS? NO CONFLICT OF INTERESTS 5/07/2018 MDM2 IN SOFT TISSUE AND BONE SARCOMAS
 MDM2 IN SARCOMAS? (MDMTWOMAS) MDM2MICS? NO CONFLICT OF INTERESTS 5/07/2018 MDM2 IN SOFT TISSUE AND BONE SARCOMAS") IN SOFT TISSUE AND BONE SARCOMAS WHAT IS? (MDMTWOMICS) Raf Sciot, M.D., PhD. Department of Pathology, University Hospitals Katholieke Universiteit Leuven, LEUVEN, Belgium IN SARCOMAS? (MDMTWOMAS) MICS?
IN SOFT TISSUE AND BONE SARCOMAS WHAT IS? (MDMTWOMICS) Raf Sciot, M.D., PhD. Department of Pathology, University Hospitals Katholieke Universiteit Leuven, LEUVEN, Belgium IN SARCOMAS? (MDMTWOMAS) MICS?
Imaging Evaluation of Malignant Chest Wall Neoplasms 1
 This copy is for personal use only. To order printed copies, contact reprints@rsna.org Imaging Evaluation of Malignant Chest Wall Neoplasms 1 1285 CHEST IMAGING Brett W. Carter, MD Marcelo F. Benveniste,
This copy is for personal use only. To order printed copies, contact reprints@rsna.org Imaging Evaluation of Malignant Chest Wall Neoplasms 1 1285 CHEST IMAGING Brett W. Carter, MD Marcelo F. Benveniste,
Why? Ultrasound of the Foot. Ultrasound of the Foot. General Rules. Plantar Fascia. Plantar Fasciitis 18/09/2018
 Ultrasound of the Foot Why? Ultrasound of the Foot Plantar fasciitis Plantar fascia fibromatosis Morton s neuroma Intermetatarsal bursitis Adventitial bursitis Plantar plate tears MTP joint synovitis Ganglia
Ultrasound of the Foot Why? Ultrasound of the Foot Plantar fasciitis Plantar fascia fibromatosis Morton s neuroma Intermetatarsal bursitis Adventitial bursitis Plantar plate tears MTP joint synovitis Ganglia
MRI Of Locally Recurrent Soft Tissue Tumors Of The Musculoskeletal System
 ISPUB.COM The Internet Journal of Radiology Volume 5 Number 2 MRI Of Locally Recurrent Soft Tissue Tumors Of The Musculoskeletal System C Costelloe, A Yasko, W Murphy, R Kumar, V Lewis, P Lin, R Stafford,
ISPUB.COM The Internet Journal of Radiology Volume 5 Number 2 MRI Of Locally Recurrent Soft Tissue Tumors Of The Musculoskeletal System C Costelloe, A Yasko, W Murphy, R Kumar, V Lewis, P Lin, R Stafford,
Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
 Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
Update On Lipomatous Tumors: Old Standbys and New Concepts
 Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
COPYRIGHT 2004 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
 84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
Not the usual liposarcoma... could it be a fatty benign tumor?
 Not the usual liposarcoma... could it be a fatty benign tumor? Poster No.: C-0635 Congress: ECR 2017 Type: Educational Exhibit Authors: A. Cano Rodríguez, J. M. Morales Pérez, C. Le Cacheux, J. I. 1 1
Not the usual liposarcoma... could it be a fatty benign tumor? Poster No.: C-0635 Congress: ECR 2017 Type: Educational Exhibit Authors: A. Cano Rodríguez, J. M. Morales Pérez, C. Le Cacheux, J. I. 1 1
Intra-articular soft tissue masses of the knee: An imaging review of biopsy proven diagnoses
 Intra-articular soft tissue masses of the knee: An imaging review of biopsy proven diagnoses Poster No.: P-0114 Congress: ESSR 2014 Type: Scientific Poster Authors: A. Kirwadi 1, S. Raniga 2, R. Hargunani
Intra-articular soft tissue masses of the knee: An imaging review of biopsy proven diagnoses Poster No.: P-0114 Congress: ESSR 2014 Type: Scientific Poster Authors: A. Kirwadi 1, S. Raniga 2, R. Hargunani
Grading of Bone Tumors
 Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Essential Dermatopathology. Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center
 Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
Synovial hemangioma of the suprapatellar bursa
 Synovial hemangioma of the suprapatellar bursa Poster No.: P-0040 Congress: ESSR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit A. YESILDAG, S. Keskin, H. Kalkan, S. Kucuksen, U. Kerimoglu; Konya/TR
Synovial hemangioma of the suprapatellar bursa Poster No.: P-0040 Congress: ESSR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit A. YESILDAG, S. Keskin, H. Kalkan, S. Kucuksen, U. Kerimoglu; Konya/TR
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
Research Article A Clinicopathological Analysis of Soft Tissue Sarcoma with Telangiectatic Changes
 Sarcoma Volume 2015, Article ID 740571, 5 pages http://dx.doi.org/10.1155/2015/740571 Research Article A Clinicopathological Analysis of Soft Tissue Sarcoma with Telangiectatic Changes Hiroshi Kobayashi,
Sarcoma Volume 2015, Article ID 740571, 5 pages http://dx.doi.org/10.1155/2015/740571 Research Article A Clinicopathological Analysis of Soft Tissue Sarcoma with Telangiectatic Changes Hiroshi Kobayashi,
Evening Specialty Conference Bone and Soft Tissue Pathology. Diagnostic pitfalls in bone and soft tissue pathology
 Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji
 Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neck masses are a frequent
Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neck masses are a frequent
MSK Interesting Cases. Dr Yap Sheau Huey
 MSK Interesting Cases Dr Yap Sheau Huey Case 1: History 41 y.o man, surf skier C/o pain over anterior left 5 th to 8 th ribs. Worse after sport activity. Chest Radiograph US Periostitis and early callus
MSK Interesting Cases Dr Yap Sheau Huey Case 1: History 41 y.o man, surf skier C/o pain over anterior left 5 th to 8 th ribs. Worse after sport activity. Chest Radiograph US Periostitis and early callus
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 3/ Issue 46/Sep 22, 2014 Page 11296
 CT SPECTRUM OF GIANT RETROPERITONEAL LIPOSARCOMAS WITH HISTOPATHOLOGICAL CORRELATION Shashikumar M. R 1, Rajendra Kumar N. L 2, C. P. Nanjaraj 3, Nishanth R. K 4, Vishwanath Joshi 5 HOW TO CITE THIS ARTICLE:
CT SPECTRUM OF GIANT RETROPERITONEAL LIPOSARCOMAS WITH HISTOPATHOLOGICAL CORRELATION Shashikumar M. R 1, Rajendra Kumar N. L 2, C. P. Nanjaraj 3, Nishanth R. K 4, Vishwanath Joshi 5 HOW TO CITE THIS ARTICLE:
Disclosures. Giant Cell Rich Tumors of Bone. Outline. The osteoclast. Giant cell rich tumors 5/21/11
 Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Keywords Giant Cell Tumors; Bone and Bones; Radiography; Magnetic Resonance. Marcelo de Pinho Teixeira Alves
 CASE REPORT Excision of giant cell tumor of tendon sheath with bone involvement by means of double access approach: case report Marcelo de Pinho Teixeira Alves Abstract Giant cell tumors of the tendon
CASE REPORT Excision of giant cell tumor of tendon sheath with bone involvement by means of double access approach: case report Marcelo de Pinho Teixeira Alves Abstract Giant cell tumors of the tendon
A 24 year old male patient presented with a swelling on the dorsal aspect of left foot since 3 years. He was operated thrice before, outside, for
 A 24 year old male patient presented with a swelling on the dorsal aspect of left foot since 3 years. He was operated thrice before, outside, for same. Came to us with recurrence since last one year with
A 24 year old male patient presented with a swelling on the dorsal aspect of left foot since 3 years. He was operated thrice before, outside, for same. Came to us with recurrence since last one year with
Original Report. Imaging Features of Fat Necrosis. Lai Peng Chan 1 R. Gee 2 Ciaran Keogh 2 Peter L. Munk 2
 Lai Peng Chan 1 R. Gee 2 Ciaran Keogh 2 Peter L. Munk 2 Received September 16, 2002; accepted after revision pril 29, 2003. 1 Department of Diagnostic Radiology, Singapore General Hospital, Outram Rd.,
Lai Peng Chan 1 R. Gee 2 Ciaran Keogh 2 Peter L. Munk 2 Received September 16, 2002; accepted after revision pril 29, 2003. 1 Department of Diagnostic Radiology, Singapore General Hospital, Outram Rd.,
LAC + USC.
 Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
GIANT CELL TUMOR OF TENDON SHEATH A CYTO HISTO CORRELATION
 GIANT CELL TUMOR OF TENDON SHEATH A CYTO HISTO CORRELATION Dr.S.SRIKANTH, Assistant Professor.Dept of Patholgy. Dr.SMITHA VADANA, Resident.Dept of pathology. Dr.R.SUHELA. Resident.Dept Of Pathology. Prathima
GIANT CELL TUMOR OF TENDON SHEATH A CYTO HISTO CORRELATION Dr.S.SRIKANTH, Assistant Professor.Dept of Patholgy. Dr.SMITHA VADANA, Resident.Dept of pathology. Dr.R.SUHELA. Resident.Dept Of Pathology. Prathima
USCAP Pediatrics Evening Subspecialty Conference 2015
 USCAP Pediatrics Evening Subspecialty Conference 2015 Sunday 22 March 2015 Alexander Lazar MD/PhD Department of Pathology S Section of Bone Soft TIssue Pathology Sarcoma Research Center The Case Patient
USCAP Pediatrics Evening Subspecialty Conference 2015 Sunday 22 March 2015 Alexander Lazar MD/PhD Department of Pathology S Section of Bone Soft TIssue Pathology Sarcoma Research Center The Case Patient
Pigmented Villonodular Synovitis PVNS
 February 2002 Pigmented Villonodular Synovitis PVNS Amy Gillis, Harvard Medical School Year III 47 year old female Our Patient Right hip pain since age 20 No history of trauma Diagnosed with DJD of R hip
February 2002 Pigmented Villonodular Synovitis PVNS Amy Gillis, Harvard Medical School Year III 47 year old female Our Patient Right hip pain since age 20 No history of trauma Diagnosed with DJD of R hip
Lipoma Arborescens of Subacromial-subdeltoid Bursa: Ultrasonographic Findings
 C A S E R E P O R T Lipoma Arborescens of Subacromial-subdeltoid Bursa: Ultrasonographic Findings Amelia Bargiela*, Esther Rodriguez, Rafaela Soler The present study describes the ultrasound findings of
C A S E R E P O R T Lipoma Arborescens of Subacromial-subdeltoid Bursa: Ultrasonographic Findings Amelia Bargiela*, Esther Rodriguez, Rafaela Soler The present study describes the ultrasound findings of
CASE REPORT PLEOMORPHIC LIPOSARCOMA OF PECTORALIS MAJOR MUSCLE IN ELDERLY MAN- CASE REPORT & REVIEW OF LITERATURE.
 PLEOMORPHIC LIPOSARCOMA OF PECTORALIS MAJOR MUSCLE IN ELDERLY MAN- CASE REPORT & REVIEW OF LITERATURE. M. Madan 1, K. Nischal 2, Sharan Basavaraj. C. J 3. HOW TO CITE THIS ARTICLE: M. Madan, K. Nischal,
PLEOMORPHIC LIPOSARCOMA OF PECTORALIS MAJOR MUSCLE IN ELDERLY MAN- CASE REPORT & REVIEW OF LITERATURE. M. Madan 1, K. Nischal 2, Sharan Basavaraj. C. J 3. HOW TO CITE THIS ARTICLE: M. Madan, K. Nischal,
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell
 Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
Pediatric Spine Tumors (and other masses)
") Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Pathology Type of Article: Case Report Title: Retroperitoneal
: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Pathology Type of Article: Case Report Title: Retroperitoneal
Non Lipomatous Benign Lesions Mimicking Soft-tissue Sarcomas: A Pictorial Essay
 doi:10.21873/invivo.11228 Review Non Lipomatous Benign Lesions Mimicking Soft-tissue Sarcomas: A Pictorial Essay ALESSANDRO CORAN 1, GIOVANNA ORSATTI 2, FILIPPO CRIMÌ 2, MARCO RASTRELLI 3, ANTONIO DI MAGGIO
doi:10.21873/invivo.11228 Review Non Lipomatous Benign Lesions Mimicking Soft-tissue Sarcomas: A Pictorial Essay ALESSANDRO CORAN 1, GIOVANNA ORSATTI 2, FILIPPO CRIMÌ 2, MARCO RASTRELLI 3, ANTONIO DI MAGGIO
Diagnostic Approach to Soft Tissue Tumors
 SECTION 2 Diagnostic Approach to Soft Tissue Tumors Overview Biopsy and Resection of Soft Tissue Tumors 20 Clinical Approach Age- and Location-Based Approach to Diagnosis 24 Histologic Approach Pattern-Based
SECTION 2 Diagnostic Approach to Soft Tissue Tumors Overview Biopsy and Resection of Soft Tissue Tumors 20 Clinical Approach Age- and Location-Based Approach to Diagnosis 24 Histologic Approach Pattern-Based
Ultrasound screening of soft tissue masses in the trunk and extremity - a BSG guide for ultrasonographers and primary care
 Ultrasound screening of soft tissue masses in the trunk and extremity - a BSG guide for ultrasonographers and primary care Introduction Soft tissue masses in the trunk and extremity are common and most
Ultrasound screening of soft tissue masses in the trunk and extremity - a BSG guide for ultrasonographers and primary care Introduction Soft tissue masses in the trunk and extremity are common and most
MARK D. MURPHEY MD, FACR. Physician-in-Chief, AIRP. Chief, Musculoskeletal Imaging
 ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
Brief History. Identification : Past History : HTN without regular treatment.
 Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
MRI of Pediatric Ankle and Foot. Mahesh Thapa, MD Associate Professor Seattle Children s University of Washington School of Medicine
 MRI of Pediatric Ankle and Foot Mahesh Thapa, MD Associate Professor Seattle Children s University of Washington School of Medicine Disclosures Under contract with Lippincott Williams and Wilkins (LWW)
MRI of Pediatric Ankle and Foot Mahesh Thapa, MD Associate Professor Seattle Children s University of Washington School of Medicine Disclosures Under contract with Lippincott Williams and Wilkins (LWW)
Von Recklinghausen s Disease with a Giant Lipoma
 Von Recklinghausen s Disease with a Giant Lipoma Daiki Iwana¹( ) Kazutaka Izawa¹ Mitsuhiro Kawamura¹ Takaharu Nabeshima¹ Hideki Yoshikawa² ¹Department of Orthopaedic Surgery, Toneyama National Hospital,
Von Recklinghausen s Disease with a Giant Lipoma Daiki Iwana¹( ) Kazutaka Izawa¹ Mitsuhiro Kawamura¹ Takaharu Nabeshima¹ Hideki Yoshikawa² ¹Department of Orthopaedic Surgery, Toneyama National Hospital,
Superficial Lumps and Bumps: Ultrasound Assessment
 Posterior knee Superficial Lumps and Bumps: Ultrasound Assessment Walter Mak, MD Department of Medical Imaging St. Michael s Hospital SM SM MGas MGas MGas MGas Synovial lined Synovial cyst: extrusion of
Posterior knee Superficial Lumps and Bumps: Ultrasound Assessment Walter Mak, MD Department of Medical Imaging St. Michael s Hospital SM SM MGas MGas MGas MGas Synovial lined Synovial cyst: extrusion of
Scrotum-like protrusion of lipoma arising from the proximal thigh
 Upsala J Med sci 109: 261 265, 2004 Scrotum-like protrusion of lipoma arising from the proximal thigh Report of two cases Koshi Hattori, 1 Masahito Hatori, 1 Mika Watanabe, 2 Toshihisa Osanai, 3 Shoichi
Upsala J Med sci 109: 261 265, 2004 Scrotum-like protrusion of lipoma arising from the proximal thigh Report of two cases Koshi Hattori, 1 Masahito Hatori, 1 Mika Watanabe, 2 Toshihisa Osanai, 3 Shoichi
Case Report Synchronous Malignant Peripheral Nerve Sheath Tumor and Adenocarcinoma of the Prostate: Case Report and Literature Review
 Case Reports in Urology Volume 2016, Article ID 2457416, 5 pages http://dx.doi.org/10.1155/2016/2457416 Case Report Synchronous Malignant Peripheral Nerve Sheath Tumor and Adenocarcinoma of the Prostate:
Case Reports in Urology Volume 2016, Article ID 2457416, 5 pages http://dx.doi.org/10.1155/2016/2457416 Case Report Synchronous Malignant Peripheral Nerve Sheath Tumor and Adenocarcinoma of the Prostate:
Year 2003 Paper two: Questions supplied by Tricia
 question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
Fluid-fluid levels in bone tumors: A pictorial review
 Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV
 DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
Imaging of Liposarcoma: Classification, Patterns of Tumor Recurrence, and Response to Treatment
 Special Article Pictorial Essay O Regan et al. Imaging of Liposarcoma Special Article Pictorial Essay Kevin N. O Regan 1 Jyothi Jagannathan Katherine Krajewski Katherine Zukotynski Frederico Souza Andrew
Special Article Pictorial Essay O Regan et al. Imaging of Liposarcoma Special Article Pictorial Essay Kevin N. O Regan 1 Jyothi Jagannathan Katherine Krajewski Katherine Zukotynski Frederico Souza Andrew
See Part 1 of the two-part series by Navarro et al in the May-June 2009 issue (pp ).
.") RadioGraphics 2009, 10.1148/rg.e36 RSNA, 2009 RadioGraphics 2009; e36 Published online 10.1148/rg.e36 Content Codes: Pediatric Soft-Tissue Tumors and Pseudotumors: MR Imaging Features with Pathologic Correlation
RadioGraphics 2009, 10.1148/rg.e36 RSNA, 2009 RadioGraphics 2009; e36 Published online 10.1148/rg.e36 Content Codes: Pediatric Soft-Tissue Tumors and Pseudotumors: MR Imaging Features with Pathologic Correlation
Multicentric localized giant cell tumor of the tendon. sheath
 Multicentric localized giant cell tumor of the tendon sheath Toshihiro Akisue, Tetsuji Yamamoto ( ), Teruya Kawamoto, Toshiaki Hitora, Takashi Marui, Tetsuya Nakatani, Takafumi Onga, and Masahiro Kurosaka.
Multicentric localized giant cell tumor of the tendon sheath Toshihiro Akisue, Tetsuji Yamamoto ( ), Teruya Kawamoto, Toshiaki Hitora, Takashi Marui, Tetsuya Nakatani, Takafumi Onga, and Masahiro Kurosaka.
INDEX. in this web service Cambridge University Press
 actin 14 adamantinoma 202, 290 292, 297 adenocarcinoma 136 adipocytes in hibernoma 149, 150 in lipoblastoma 148 in lipoma 141, 142, 145 in liposarcoma 152 in myelolipoma 151 adrenal gland tumors see myelolipoma
actin 14 adamantinoma 202, 290 292, 297 adenocarcinoma 136 adipocytes in hibernoma 149, 150 in lipoblastoma 148 in lipoma 141, 142, 145 in liposarcoma 152 in myelolipoma 151 adrenal gland tumors see myelolipoma
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Tumors. Chapter 3. Primary neurogenic tumors. Tumors 27
 Tumors 27 Chapter 3 Tumors MR imaging of the brachial plexus is frequently requested to rule out a tumor in or near the brachial plexus, or to evaluate the extension of a known tumor in the region of the
Tumors 27 Chapter 3 Tumors MR imaging of the brachial plexus is frequently requested to rule out a tumor in or near the brachial plexus, or to evaluate the extension of a known tumor in the region of the
Masses of the Corpus Callosum
 Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
Adipocytic Tumours in children
 Università degli Studi di Padova Dipartimento di Medicina Sezione di Anatomia Patologica Generale e Citopatologia Adipocytic Tumours in children Rita Alaggio Basel Seminars in Pathology Paediatric Pathology
Università degli Studi di Padova Dipartimento di Medicina Sezione di Anatomia Patologica Generale e Citopatologia Adipocytic Tumours in children Rita Alaggio Basel Seminars in Pathology Paediatric Pathology
Anatomy of Peripheral Nerve 가톨릭대학교 재활의학과 김재민
 Anatomy of Peripheral Nerve 가톨릭대학교 재활의학과 김재민 Contents US appearance of nerves Scanning technique Peripheral nerve pathology Nerves of arm Nerves of leg US Appearance of Nerve Multiple longitudinal hypoechoic
Anatomy of Peripheral Nerve 가톨릭대학교 재활의학과 김재민 Contents US appearance of nerves Scanning technique Peripheral nerve pathology Nerves of arm Nerves of leg US Appearance of Nerve Multiple longitudinal hypoechoic