See Part 1 of the two-part series by Navarro et al in the May-June 2009 issue (pp ).
|
|
|
- Hortense King
- 6 years ago
- Views:
Transcription
1 RadioGraphics 2009, /rg.e36 RSNA, 2009 RadioGraphics 2009; e36 Published online /rg.e36 Content Codes: Pediatric Soft-Tissue Tumors and Pseudotumors: MR Imaging Features with Pathologic Correlation Part 2. Tumors of Fibroblastic/Myofibroblastic, So-called Fibrohistiocytic, Muscular, Lymphomatous, Neurogenic, Hair Matrix, and Uncertain Origin 1 Eoghan E. Laffan, MB 2 Bo-Yee Ngan, MD, PhD Oscar M. Navarro, MD 1 From the Department of Diagnostic Imaging (E.E.L., O.M.N.) and the Division of Pathology, Department of Pediatric Laboratory Medicine (B.Y.N.), Hospital for Sick Children and University of Toronto, 555 University Avenue, Toronto, Ontario M5G 1X8, Canada. Presented as an education exhibit at the 2005 RSNA Annual Meeting. Received June 27, 2008; revision requested August 1; revision received and accepted August 12. All authors have no financial relationships to disclose. Address correspondence to O.M.N. ( oscar.navarro@sickkids.ca) 2 Current address: Children's Hospital of Eastern Ontario, Ottawa, Ontario, Canada. Footnotes Abbreviations: GCTTS = giant cell tumor of the tendon sheath, MPNST = malignant peripheral nerve sheath tumor, PVNS = pigmented villonodular synovitis, STIR = short inversion time inversion recovery, WHO = World Health Organization. See Part 1 of the two-part series by Navarro et al in the May-June 2009 issue (pp ). Abstract In the final part of this two-part review article on soft-tissue masses in children, the magnetic resonance (MR) imaging features, clinical findings, and pathologic findings in a wide variety of tumors, including those of fibroblastic/myofibroblastic origin, so-called fibrohistiocytic tumors, smooth-muscle tumors, skeletal-muscle tumors, tumors of uncertain differentiation, and lymphoma, are described. Other neoplasms that are not included in the World Health Organization classification of soft-tissue tumors but may be seen clinically as soft-tissue masses, specifically dermatofibrosarcoma protuberans, neurogenic tumors and pilomatricoma, are also included. In contrast to the tumors reviewed in Part 1 of this review, the MR imaging features and clinical findings of the tumors included here are largely nonspecific. However, MR imaging is useful in determining site of tumor origin, extent of disease, and relation of tumor to adjacent anatomic structures, and for follow-up after therapy. In some of these entities, the combination of findings may aid in narrowing the differential diagnosis, such as persistent low signal intensity on T1- and T2-weighted images in some fibroblastic lesions, identification of hemosiderin and a synovial origin in pigmented villonodular synovitis, or the presence of multiple target signs on T2-weighted images in deep plexiform neurofibroma. In a large number of cases, however, tissue biopsy is required for final diagnosis. Page 1
2 Introduction In Part 2 of this review of soft-tissue tumors in children, we review the following entities: fibroblastic/myofibroblastic tumors, so-called fibrohistiocytic tumors, smooth-muscle tumors, skeletal-muscle tumors, tumors of uncertain differentiation (angiomatoid fibrous histiocytoma, synovial sarcoma, epithelioid sarcoma, alveolar soft part sarcoma and Ewing/primitive neuroectodermal tumor), lymphoma, neurogenic tumors, and pilomatricoma. In contrast to a large proportion of the tumors discussed in Part 1 (1), in which there are clinical and/or imaging clues that may help in establishing a more precise diagnosis, the tumors reviewed here lack, for the most part, specific diagnostic features, although in a few of these tumors, some clinical and imaging findings may aid in narrowing the differential diagnosis. Fibroblastic/Myofibroblastic Tumors The classification of fibrous tumors by the World Health Organization (WHO), revised in 2002, now includes several new additions to the fibroblastic/myofibroblastic tumor group, a reclassification of known tumors and some clearer definitions of others. It comprises, therefore, a large subset of mesenchymal tumors, of which the most significant in the pediatric age include nodular fasciitis, myositis ossificans, fibrous hamartoma of infancy, myofibroma/myofibromatosis, fibromatosis colli, fibroma of tendon sheath, superficial fibromatosis, deep or desmoid-type fibromatosis, infantile fibrosarcoma, and adult fibrosarcoma. The magnetic resonance (MR) imaging appearances of these tumors are overall nonspecific, with MR imaging primarily used to define extent of involvement. Signal intensity depends on the cellular content, vascularity, and amount of myxoid and stromal components. They often enhance after administration of a gadolinium contrast agent. Nodular Fasciitis Nodular fasciitis is a benign, localized proliferation of plump fibroblastic/myofibroblastic cells of uncertain origin. Histologic subtypes include the most common myxoid form, usually confined to the subcutaneous tissues, and the more uncommon fibrous and cellular forms, more frequently seen in intramuscular and intermuscular locations (2). Nodular fasciitis is more commonly seen in young adults, but it may occur in children, particularly the cranial form of nodular fasciitis, which is almost exclusively seen in infants less than 2 years of age. The most common locations in order of frequency are the upper extremities, trunk, head and neck, and lower extremities (3). They often present as fast-growing lesions that rarely exceed 4 cm in diameter and are associated with pain or tenderness in about half of the cases (3). The MR imaging appearances are nonspecific and somewhat variable, although a characteristic pattern has been described in the more common myxoid type: homogeneous signal isointense or slightly hyperintense to that of muscle on T1-weighted images, hyperintense on T2- weighted images, and showing homogeneous enhancement after administration of a gadolinium contrast agent (2,3) (Fig 1). The final diagnosis generally requires histology. Treatment includes local excision; recurrence is exceedingly rare (3). Page 2
 Sagittal T1-weighted MR image shows a well-defined fascia-based subcutaneous mass, which is slightly hyperintense to adjacent muscle.")

.")

3 1a. 1b. Figure 1. Nodular fasciitis in an 11-year-old girl who presented with a lump in the forearm. (a) Sagittal T1-weighted MR image shows a well-defined fascia-based subcutaneous mass, which is slightly hyperintense to adjacent muscle. (b) Sagittal fat-suppressed gadolinium-enhanced T1- weighted MR image reveals diffuse enhancement of the mass and somewhat linear extension of the enhancement parallel and superficial to the fascial plane. Teaching Point Myositis Ossificans Myositis ossificans is a localized, self-limiting, reparative lesion of muscle, which at pathology has three components: a central zone of proliferating fibroblasts, a middle zone containing osteoblasts and foci of immature bone, and a peripheral layer with mature bone trabeculae (4). The cause of myositis ossificans is soft-tissue injury, in most cases secondary to trauma, which is well documented in 60%-75% of patients (5). In the remaining cases, minor repetitive trauma, ischemia, and inflammation are thought to be the causative agents. The lesion may develop anywhere in the body, but it occurs more frequently in those areas more exposed to trauma, especially the anterior compartments of the thigh and arm. In children, it is usually seen in those older than 10 years (4). MR imaging is not the modality of choice for evaluation of myositis ossificans, owing to its relative inability to demonstrate soft-tissue calcification. MR imaging may be nonspecific when myositis ossificans can already be diagnosed on radiographs or computed tomographic (CT) scans (Fig 2). The imaging findings correlate with the pathologic findings and therefore change with time (4-6). In the acute phase (<2 weeks), the lesion may not be visible on T1- weighted images or may be poorly defined and with heterogeneous signal intensity but predominantly isointense to muscle. On T2-weighted images, it is usually hyperintense. The lesion may also contain fluid-fluid levels due to prior hemorrhage, and there is often associated edema of the perilesional soft tissues and in the bone marrow of any adjacent bone. In the subacute phase (3 to 6 8 weeks), peripheral foci of low signal intensity are identifiable on both T1- and T2-weighted images, owing to bone formation. During these acute and subacute phases, Page 3
, the lesion becomes better defined and the soft-tissue edema is no longer evident.")

4 enhancement with gadolinium is visible at the periphery of the lesion and in the adjacent edematous soft tissues and may mimic the appearances of an abscess or necrotic tumor. In the chronic stage (6 8 weeks or older), the lesion becomes better defined and the soft-tissue edema is no longer evident. Owing to the progression of peripheral calcification and ossification, more extensive low signal intensity is seen with all sequences. Areas of fat signal may also be recognized within the lesion and represents fatty marrow. 2a. 2b. Figure 2. Myositis ossificans in a 16-year-old boy who presented with a 2-week history of an enlarging mass in the left upper arm and a history of sports-related trauma 3 weeks prior to the mass being noticed. (a) Axial T2-weighted MR image shows a lobulated, predominantly hyperintense, intramuscular mass adjacent to the humeral diaphysis. Areas of intermediate to low signal intensity are seen within the mass and a rim of low signal intensity is noted at the periphery, compatible with calcification. (b) Unenhanced CT scan more clearly demonstrates the characteristic peripheral mineralization of myositis ossificans. Teaching Point Fibrous Hamartoma of Infancy Fibrous hamartoma of infancy is a rare, usually solitary, benign but rapidly growing superficial lesion most often seen in infants. More than 90% of the cases occur during the 1st year of life, and nearly a quarter of the cases are congenital (7). The tumor is more common in boys and most frequently found in the axilla, upper arm, upper trunk, inguinal region, and external genital area (7). It is usually a painless, freely movable mass in the subcutis or dermis that measures less than 5 cm in diameter. Histologically, this lesion has three characteristic components: well-defined intersecting trabeculae of fibrocollagenous tissue, loosely textured islands of primitive mesenchyma, and mature fat, with the latter being usually the predominant component. The MR imaging appearance of fibrous hamartoma of infancy reflects to a great extent the relative proportion of the different tissue components present within the lesion (8,9). The fibrous component appears as areas of low signal intensity on both T1- and T2-weighted images, whereas the fatty component shows characteristic high signal intensity on both T1- and T2- weighted images (Fig 3). It is the recognition of fat within this lesion that helps to narrow the differential diagnosis, which at the age of presentation for these tumors should also include lipoma, lipoblastoma, and involuting hemangioma. It has been suggested that the demonstration of subcutaneous trabeculae of fibrous tissue interspersed with fat in an organized pattern is strongly suggestive of fibrous hamartoma of infancy in the appropriate clinical setting (8) (Fig 3). Page 4


5 lipoma, lipoblastoma, and involuting hemangioma. It has been suggested that the demonstration of subcutaneous trabeculae of fibrous tissue interspersed with fat in an organized pattern is strongly suggestive of fibrous hamartoma of infancy in the appropriate clinical setting (8) (Fig 3)}. 3. Figure 3. Fibrous hamartoma of infancy in an 8-month-old boy who presented with a 2-month history of a rapidly growing left axillary mass. Coronal T1-weighted MR image shows a welloutlined, slightly lobulated subcutaneous mass in the left axilla. The mass is predominantly isointense to muscle, but multiple small hyperintense striations are also noted within the mass, compatible with adipose tissue. The recognition of intralesional fat aids in narrowing the differential diagnosis of soft-tissue masses. Myofibromatosis Infantile myofibromatosis (multicentric) or myofibromas (solitary) are the most common fibrous tumors in infancy (10 12). These are benign tumors that occur mainly in children under the age of 2 years (88% of cases) (10), and about 60% of the cases are diagnosed at birth (11). The tumors vary greatly in size from 2.5 cm to 7 cm, and histologically they are formed by nodules with two distinct components, one characterized by bundles of myofibroblasts and the other by more undifferentiated cells arranged around thin-walled, irregularly branching, hemangiopericytomalike blood vessels. Because of this arrangement, it is thought that myofibromatosis forms a morphologic continuum with the so-called infantile hemangiopericytoma. The solitary form accounts for half of the lesions and is more frequently seen in boys and involves the head, neck, and trunk. The multicentric form may be present in the soft tissues, bones, and viscera. The poorer prognosis of myofibromatosis with visceral involvement (25% 35% of multicentric cases) (11), with reported mortality rates as high as 75% (10), is determined by the extent and location of the lesions, with intestinal, cardiac, and, in particular, lung lesions having a poorer outcome (11). Page 5
.")
.")
6 Although the natural history of most cases of infantile myofibromatosis is spontaneous regression, children affected with visceral disease or diffuse musculoskeletal involvement often develop life-threatening disease before the lesions have had an opportunity to involute (13). Multicentric lesions may increase in size and number up to 1 year before starting a slow regression, which may take a few years (9). Recurrence after excision is reported to be about 10% (10). Low-dose chemotherapy may successfully treat life-threatening generalized lesions (13). MR imaging characteristics of these lesions include low signal intensity on T1-weighted images and a more variable appearance on T2-weighted images (12) (Fig 4). These tumors have been described as showing a target sign after the administration of an intravenous gadolinium contrast agent, with peripheral enhancement, thought to be due to central necrosis (9,12). Wholebody MR imaging protocols may be useful as a screening tool for assessing multicentric involvement in myofibromatosis (13). 4a. 4b. Page 6
 Sagittal T1- weighted MR image shows an isointense mass inseparable from the diaphragm and contiguous to the diaphragmatic surface of the liver (arrows).")



7 4c. Figure 4. Myofibromatosis of the diaphragm in a 20-day-old boy, transferred to our institution with a history of abdominal distention, ascites, and absent ductus venosus. (a) Sagittal T1- weighted MR image shows an isointense mass inseparable from the diaphragm and contiguous to the diaphragmatic surface of the liver (arrows). (b) Coronal fat-suppressed T2-weighted MR image shows that the diaphragmatic mass is heterogeneous, containing areas of low and intermediate signal intensity. Note is also made of ascites between loops of bowel. (c) Photomicrograph (original magnification, 10; hematoxylin-eosin stain) shows solid sheets of diffuse proliferations of plump spindle cells with ill-defined cytoplasmic borders and eosinophilic cytoplasm. Coarse fibrillar collagen is deposited within the tissue stroma. Fibromatosis Colli Fibromatosis colli is a benign mass that arises from the sternocleidomastoid muscle. It is usually unilateral and more common on the right than on the left side (14). It is thought to be a cellular scarlike reaction to injury of the sternocleidomastoid muscle in the last trimester of intrauterine growth or at the time of delivery. Clinically, it is seen as a cervical mass that may be associated with torticollis in up to 20% of cases, and there is commonly a history of birth trauma (14). The mass is usually evident at 2 weeks after birth and may continue to increase in size for a few more weeks. It often involutes spontaneously over 4 8 months with conservative treatment. The diagnosis of fibromatosis colli is usually readily established with sonography, and further evaluation with other imaging modalities including MR imaging is rarely required. The few cases reported in the literature in which MR imaging was used in the evaluation of this tumor describe fibromatosis colli as a fusiform enlargement of the affected muscle, without extension to adjacent tissues and with margins that are better defined than at sonography. The signal intensity of the mass may vary, likely reflecting the degree of fibrous and cellular tissue present, although in most cases signal intensity is higher than that of fat on T2-weighted images (14). Fibroma of the Tendon Sheath Fibroma of the tendon sheath is a rare, benign, slow-growing tumor of the extremities. Some controversy exists regarding whether it represents a reactive versus a neoplastic process (15). The tumor affects and adheres to the tendons, tendon sheaths, and sometimes the neurovascular Page 7
.")

8 bundles at the affected site (16). The hand, especially the thumb and index and middle fingers, as well as the wrist, are the most common sites affected (80%) (16). Males are more frequently affected than females; both are most commonly in the 4th decade (16). It is uncommon in children but affects patients aged 19 years or less in 15% 20% of cases, even patients as young as 5 months (15,16). At MR imaging, the diagnosis of fibroma of the tendon sheath may be suggested if there is a well-defined, lobulated, nodular mass with low signal intensity with all sequences and minimal or no enhancement in the vicinity of tendon sheath (17). However, the signal intensity of the mass can be quite variable on T2-weighted images (Fig 5). More heterogeneous signal intensity and enhancement patterns can also be seen, reflecting different cellular and stromal elements within the tumor (17). The tumor can sometimes be difficult to differentiate from other soft-tissue tumors commonly found in the extremities, such as giant-cell tumor of the tendon sheath and pigmented villonodular synovitis (PVNS) (15 17). Blooming artifact from hemosiderin deposition is, however, rarely seen in fibroma of the tendon sheath as opposed to the two other entities mentioned (17). 5a. 5b. Figure 5. Fibroma of the tendon sheath in a 10-year-old girl who presented with a history of a mass in the left fourth digit, growing commensurately with the child for the previous 3 4 years. (a) Coronal STIR MR image of the left hand shows a hyperintense soft-tissue mass in the ulnar aspect of the fourth digit, adjacent to the proximal interphalangeal joint. (b) Photomicrograph (original magnification, 20; hematoxylin-eosin stain) shows the hallmark appearance of this tumor, with small numbers of bland-looking fibroblasts scattered within an amorphous collagen matrix. Also present are the characteristic clefts with pseudovascular spaces that simulate blood vessels. Definitive treatment is surgical resection, which may involve the adjacent neurovascular bundle. To our knowledge, no updated recurrence rates are available, but with the newer microscopic surgical techniques, they are likely well below the commonly quoted 24% (15). All reported recurrences have occurred in the hands. Page 8
. They are most commonly seen after puberty, in patients ranging up to 40 years of age.")
9 Fibromatosis Fibromatosis is a histologically benign proliferation of fibroblasts, but with local aggressiveness and are thus classified as intermediate (locally aggressive) by the WHO (18,19). Mostly solitary, they can also be multicentric and are classified according to location (superficial vs deep). They are most commonly seen after puberty, in patients ranging up to 40 years of age. Superficial fibromatoses are small (<5cm), slow-growing lesions rarely seen in children. They arise in the plantar aponeurosis of the foot (Ledderhose disease), the palmar fascia of the hand (Dupuytren contracture), and less commonly in the penile fascia (Peyronie disease) (18). These lesions rarely require imaging evaluation, as the diagnosis is often made clinically. MR imaging shows superficial fibromatosis as lesions of low signal intensity on T1-weighted images and of isointensity to low intensity on T2-weighted images (Fig 6). 6. Figure 6. Plantar fibromatosis in a 12-year-old boy who presented with an 18-month history of a plantar mass in the left foot. Sagittal fat-suppressed T2-weighted image shows a well-defined low-signal-intensity nodular mass (arrow) in the plantar soft tissues. Deep or desmoid fibromatoses are larger, rapidly growing lesions that arise in the deep soft tissues and are characterized by infiltrative growth and a tendency to recur locally but without evidence of metastatic spread (19). In children, these tumors are more common in boys than in girls, usually seen in patients less than 8 years old, most frequently in the first 2 years of life (20). They can be classified as abdominal or extraabdominal lesions, with the latter more common in the pediatric age group, particularly if they occur in the head, neck, extremities, or trunk (20). Although most cases are sporadic, familial-related cases occur, especially in patients with Gardner syndrome. These lesions have a heterogeneous MR imaging appearance, mostly with intermediate or low signal intensity on T1-weighted images and with high signal intensity mixed with bands of low signal intensity on T2-weighted images. The areas of high signal intensity on T2-weighted images usually show avid enhancement with gadolinium (Fig 7). The tumor usually has both well-defined and ill-defined margins. It has been reported that helpful features in the differentiation of desmoid fibromatosis from soft-tissue sarcomas include the presence of an infiltrative growth pattern, crossing of fascial boundaries, and the absence of central necrosis even in the largest lesions (21). However, tissue confirmation is required for a final diagnosis in all cases. Page 9
 Coronal T1-weighted MR image shows a mass, isointense to muscle, between the first and second metatarsal bones.")

10 7a. 7b. Figure 7. Multicentric deep fibromatosis in a 14-year-old girl with a previous history of resected fibromatosis of the lower leg who presented with a left foot mass. (a) Coronal T1-weighted MR image shows a mass, isointense to muscle, between the first and second metatarsal bones. (b) Coronal gadolinium-enhanced fat-suppressed T1-weighted image shows diffuse enhancement of the lesion. Fibrosarcoma: Infantile versus Adult Type The two forms of fibrosarcoma share histologic similarities but are markedly different in terms of their age at presentation and their prognosis. The infantile form, also known as congenital fibrosarcoma, is a malignant proliferation of fibroblasts often seen in the first 5 years of life, with about one-third present at birth (22). They are most often seen in the extremities (74%), followed by the head and neck (15%) (23). Initially, they grow rapidly and may become quite large in proportion to the size of the child. Metastases, mainly pulmonary, are seen in 5% 10% of cases, with local recurrence reported to be between 17% and 43% (23). However, overall prognosis is better than in adults, with a greater than 80% 5-year survival rate (23). MR imaging appearances of infantile fibrosarcomas are nonspecific, as they present as well-demarcated lesions that are isointense to muscle on T1-weighted images and heterogeneously hyperintense on T2-weighted images (9,24) (Fig 8). A heterogeneous enhancement pattern is seen after injection of a gadolinium contrast agent (9). Page 10
 Sagittal STIR MR image of the right lower leg shows a large hyperintense and homogeneous mass involving the muscles in the posterior compartment.")


11 8a. 8b. Figure 8. Infantile fibrosarcoma in a 2-month-old boy with a 10-day history of progressive swelling of the right calf. (a) Sagittal STIR MR image of the right lower leg shows a large hyperintense and homogeneous mass involving the muscles in the posterior compartment. (b) Photomicrograph (original magnification, 20; hematoxylin-eosin stain) shows immature, small, ovoid tumor cells arranged in short sinuous cords and sharp intersecting bands. Mitoses are frequent. Clinically, infantile fibrosarcoma can occasionally be confused with infantile hemangioma or kaposiform hemangioendothelioma, as the skin overlying the tumor may have a violaceous discoloration associated with ectatic superficial veins (25). In other instances, it may present as an ulcerated lesion mimicking hemangioma, which can also show ulceration, particularly at the stage of rapid proliferation in areas of the body exposed to friction (26). Furthermore, infantile fibrosarcoma may be associated with disseminated intravascular coagulopathy, which can be confused with Kasabach-Merritt phenomenon, an entity now considered to be almost exclusively present in cases of kaposiform hemangioendothelioma or tufted angioma (23,25). It has been reported that MR imaging may help in the differentiation of these two diseases, as infantile fibrosarcomas tend to show less homogeneous contrast enhancement and lack the signal voids due to the prominent vessels that characteristically supply hemangiomas (25). Adult-type fibrosarcoma is histologically similar to the infantile form but has different cytogenetics (23). In children, these lesions occur at a later age than the infantile form, are more frequently seen in the proximal regions of the extremities and trunk, and tend to have a slower growth rate relative to the infantile form (27). However, the most significant difference is its poorer 5-year survival rate of less than 60% (27). Sparse information is available in the literature about the imaging appearances of adulttype fibrosarcoma. Lesions may be homogeneous or heterogeneous in signal intensity on T1- and T2-weighted MR images. On T1-weighted images, the lesions are usually isointense to muscle, whereas on T2-weighted images they may show areas of low signal intensity on a background of moderate to high signal intensity. Following administration of a gadolinium contrast agent, most Page 11
12 lesions show an intense peripheral enhancement with an occasional spoked-wheel appearance (28). So-called Fibrohistiocytic Tumors The classification of this group is currently undergoing revision, as it has become evident that the majority of lesions formerly included in this category do not have any relationship with true histiocytes, hence the label so-called fibrohistiocytic tumors. Benign forms include PVNS and giant cell tumor of the tendon sheath (GCTTS). Intermediate forms include dermatofibrosarcoma protuberans. Malignant forms include various types of malignant fibrous histiocytoma. PVNS and GCTTS PVNS is an idiopathic tumor of synovial origin, characterized by a proliferation of the synovium. Histologically, synovial cell hyperplasia, subsynovial accumulation of giant cells, macrophages, and fibroblasts, and both intra- and extracellular hemosiderin deposition are seen (29). GCTTS shows similar histologic findings to PVNS; these two entities are therefore considered to be different parts of a spectrum of diseases. PVNS represents the diffuse and intraarticular form, whereas GCTTS includes three subtypes: localized extraarticular, localized intraarticular (also called nodular synovitis), and diffuse extraarticular (30). PVNS is more common in adults, usually occurring in patients between 20 and 50 years of age (29), although pediatric cases have been reported, usually in children over 10 years of age (31). It most commonly affects the knee joint and is seen clinically as insidious swelling and intermittent pain (32). The most commonly affected regions within the knee are the Hoffa fat pad, the suprapatellar bursa, and the posteromedian synovial joint recess, an area that is difficult to see at arthroscopy and thus important to assess at MR imaging (31). Associated findings include joint effusions of variable size, normal menisci and cartilage, and occasionally a large multiseptated popliteal cyst. Bone edema and erosions are rarely seen in pediatric cases (31). Other joints that can be affected include the ankle, hip, shoulder, and elbow (33). There have been isolated reports of PVNS affecting multiple joints in children (34). MR imaging is useful preoperatively not only to establish the diagnosis but to assess the extent of disease, as the definitive treatment is synovectomy. MR imaging is also used postoperatively to evaluate recurrence, which has been reported to occur in 20% 40% of cases (34). PVNS classically appears as an irregularly thickened or frondlike synovium, hypointense on both T1- and T2-weighted images. This characteristic low signal intensity is due to hemosiderin deposition and is exaggerated by signal drop-off or blooming with gradient-echo sequences (29 34) (Fig 9). The appearances of PVNS with a gadolinium contrast agent may vary depending on the degree of fibrosis, but most lesions show avid enhancement (32). Because of this, the characteristic low signal intensity seen on unenhanced images can be lost after the use of gadolinium (31,33,35). This has also been observed with the use of short inversion time inversion-recovery (STIR) sequences, in which the synovial lesions appear hyperintense despite exhibiting low signal intensity on T2-weighted images (33,35). Page 12

13 9. Figure 9. PVNS in a 14-year-old boy with a 1-year history of swelling around the right knee. Axial gradient-echo MR image of the right knee shows nodular thickening of the synovium, more prominent in the lateral aspect of the joint, with marked low signal intensity due to the paramagnetic effect of hemosiderin deposits. Areas of high signal intensity are seen adjacent to the hypointense areas, reflecting synovial inflammation. A large joint effusion is also seen. GCTTS has MR imaging features similar to those of PVNS. Localized extraarticular GCTTS is the most common type. The lesion is usually small (<2cm) at presentation and classically seen to wrap around the tendons of the hand and fingers (36). The intraarticular form, also known as nodular synovitis, is similar to PVNS except in the degree of involvement of the affected joint, being more localized within the joint (36). Diffuse extraarticular GCTTS lesions are bigger and more aggressive and are found in an extraarticular location around large joints (36). Dermatofibrosarcoma Protuberans Dermatofibrosarcoma protuberans is a rare soft-tissue sarcoma of intermediate malignancy, more commonly seen in middle-age adults but also reported in children, even at birth (37,38). It is most commonly found on the trunk or proximal extremities but can occur anywhere (37 39). The tumor originates in the dermis but spreads locally into the deeper tissues, such as the subcutaneous tissues, fascia, muscles, and bones (40,41). It is seen as a slow-growing, indolent subcutaneous plaque or nodule, the overlying skin of which may be discolored reddish blue or purple (37,39). As a result, it can be mistaken clinically for other tumors, such as a vascular malformation or a hemangioma, and thus it is often diagnosed late. Preoperative MR imaging is usually performed only in atypical cases and to define the extent of large tumors and tumors that clinically are suspected of deep infiltration (38,40,41). MR imaging reveals a well-defined mass, generally confined to the subcutaneous tissues. The mass is usually iso- to hypointense to muscle on T1-weighted images, hyperintense on T2- weighted images, and shows uniform or patchy enhancement with a gadolinium contrast agent (40,41) (Fig 10). Page 13


. Treatment involves wide local excision.")
14 10a. 10b. Figure 10. Dermatofibrosarcoma protuberans in a 10-month-old girl who presented with a mass in the right lower leg. The mass was initially presumed to be a vascular malformation, as it had been present since birth, was associated with blue discoloration of the overlying skin, and had grown commensurately with the child. (a) Axial fat-suppressed, gadolinium-enhanced T1- weighted MR image of the right lower leg shows an irregular dermal and subcutaneous mass with extension to the superficial fascial planes. The mass shows diffuse enhancement, but it is not as avid as expected for a vascular lesion. (b) Photomicrograph (original magnification, 20; hematoxylin-eosin stain) shows solid sheets of diffuse proliferations of plump spindle cells with ill-defined cytoplasmic borders and eosinophilic cytoplasm. Part of a staghorn-shaped vascular channel is present (arrow). Treatment involves wide local excision. Local recurrence rates are expected to be between 10% and 25%, but considerably higher rates have been reported, especially if there are positive margins (38 40). MR imaging may be performed to monitor tumor recurrence. Metastases are rare, usually found in the lung, and are associated with a much poorer prognosis (37,39). Malignant Fibrous Histiocytoma Malignant fibrous histiocytoma is a controversial entity. It was once considered the most common soft-tissue tumor in adults, but with the recent revision of the WHO tumor classification, it is now considered a diagnosis of exclusion, accounting for less than 5% of adult sarcomas (42). The term is now used for the small group of pleomorphic sarcomas that do not show a definable line of differentiation. Malignant fibrous histiocytoma has always been considered rare in children. In a recently published series, in which the new WHO histologic criteria were used, it represented only 7% of the nonrhabdomyosarcomatous pediatric tumors (43). The tumor is usually seen as a painless lump often larger than 5 cm at the time of diagnosis. The extremities, especially the thigh, are the most common location, followed by the Page 14


.")
15 head and neck and trunk, but it can occur anywhere in the body (43 45). There is a slight male predominance (43,44). MR imaging is nonspecific, revealing a soft-tissue mass often adjacent to the long bones. Identification of a soft-tissue mass with cortical involvement has been considered suggestive of malignant fibrous histiocytoma (46). MR imaging is useful for preoperatively displaying extent of the tumor and its relationship with adjacent structures and neurovascular bundles. The lesion is usually of intermediate signal intensity on T1-weighted images, heterogeneous high signal intensity on T2-weighted images, and shows enhancement of solid components with a gadolinium contrast agent (46). Malignant fibrous histiocytoma can also be found as a second malignancy in children who have undergone radiation therapy for other primary tumors, and at sites of previous surgery (43 46). Smooth Muscle Tumors Leiomyoma Leiomyoma is a benign tumor of smooth muscle. Leiomyomas of the deep soft tissues are extremely rare and can be divided into two groups, one occurring primarily in the pelvic retroperitoneum in women and the other in the deep somatic tissue in patients of either sex. Leiomyomas in this latter group often arise in skeletal muscle or in the deep subcutaneous soft tissues, most frequently in the lower extremities. They often affect middle-aged or young adults and are extremely rare in children (47), although we have seen a case in a girl 16 months old. Little information regarding the MR imaging appearance of deep somatic soft-tissue leiomyomas is available (47,48). In the few cases described in the literature, leiomyoma appears as a well-circumscribed mass slightly hyperintense to muscle on T1-weighted images, with heterogeneous high signal intensity on T2-weighted images, and with enhancement with a gadolinium contrast agent (Fig 10). The tumor may contain dystrophic calcifications that can be visible at radiography and MR imaging as foci of low signal intensity (Fig 11). 11a. 11b. Page 15
16 Figure 11. Leiomyoma in a 16-month-old girl who presented with a 3-week history of a lump and pain in the left thigh. (a) Coronal fat-suppressed T2-weighted MR image shows a welldefined hyperintense mass involving the left vastus lateralis muscle. Small hypointense foci within the lesion represent calcifications, as had been shown on plain radiographs. (b) Photomicrograph (original magnification, 20; hematoxylin-eosin stain) shows compact interlacing fascicles of elongated spindle cells with deep eosinophilic cytoplasm and elongated nuclei with blunt ends. There were very low numbers of mitotic figures (none illustrated), no cellular atypia, and no necrosis in this tumor. Skeletal Muscle Tumors Rhabdomyosarcoma The WHO classification includes rhabdomyoma and rhabdomyosarcoma in this group. Extracardiac rhabdomyoma is extremely rare and will not be discussed further. Rhabdomyosarcoma accounts for more than 50% of soft-tissue sarcomas in children (49,50). A slight male predominance is seen, and two-thirds of children are less than 10 years old at diagnosis (49). The lesion is more common in Caucasian than in Asian or African children (49). Rhabdomyosarcoma is almost always sporadic in occurrence, but it is also seen in association with Li-Fraumeni and Beckwith-Wiedemann syndromes as well as with neurofibromatosis (50). Although rhabdomyosarcoma is thought to arise from primitive mesenchymal cells committed to develop into striated muscle, it can be found anywhere within the body, even in sites that lack striated muscle. The head and neck and the genitourinary system are the most commonly affected regions, with less than 20% of the cases occurring in the extremities (49,50). Histologically, rhabdomyosarcomas are classified into embryonal, alveolar, and pleomorphic variants, each with a different age of presentation, with some overlap. The embryonal type is more commonly seen in children (80%) and is most often found in the head and neck and in the genitourinary tract (49). The alveolar type is less common (20%) and is seen in adolescents and young adults and more commonly found in the perineum and extremities (49). The pleomorphic type occurs almost exclusively in adults and is also found in the extremities. MR imaging findings are nonspecific. Rhabdomyosarcomas can be well or poorly defined, typically with low signal intensity on T1-weighted images, high signal intensity on T2- weighted images, and with variable enhancement with a gadolinium contrast agent (51) (Fig 12). MR imaging can demonstrate areas of internal hemorrhage and necrosis, the latter associated with a poorer prognosis in neonates (52). The primary site of origin and the extent of disease at diagnosis, including the detection of local lymphadenopathy, are important factors in determining treatment options and long-term prognosis (49). Page 16



 Photomicrograph (original magnification, 20; hematoxylin-eosin stain) shows poorly differentiated small cells")
17 12a. 12b. 12c. Figure 12. Rhabdomyosarcoma in a 6-week-old girl with Beckwith-Wiedemann syndrome who presented with a right thigh mass. (a) Coronal STIR MR image shows the presence of a large hyperintense mass involving the muscles in the posterior compartment of the right thigh. (b) Axial fat-suppressed T2-weighted MR image shows that in addition to the mass shown in a, there are additional small hyperintense foci involving the right vastus lateralis muscle and the muscles in the posterior compartment of the left thigh, compatible with metastatic disease. (c) Photomicrograph (original magnification, 20; hematoxylin-eosin stain) shows poorly differentiated small cells with dark blue nuclei in alternating dense and loose clusters. The nuclei contain condensed chromatin without nucleoli. No cytoplasmic inclusions that are indicative of myotube differentiation are seen. Numerous mitotic figures are present. Page 17

18 Tumors of Uncertain Differentiation This category includes numerous soft-tissue tumors that do not fit into any other group, owing to an unclear line of differentiation. Of these, the most notable in the pediatric age group and that will be discussed here include angiomatoid fibrous histiocytoma, synovial sarcoma, epithelioid sarcoma, alveolar soft part sarcoma, and Ewing/primitive neuroectodermal tumor. Teaching Point Angiomatoid Fibrous Histiocytoma Angiomatoid fibrous histiocytoma is a rare low-grade soft-tissue tumor that usually originates in the deep dermis and subcutaneous tissues. It was once considered to be a fibrohistiocytic tumor and within the spectrum of malignant fibrous histiocytomas. As described above in the section on the so-called fibrohistiocytic tumors, this group of tumors has undergone extensive revision and angiomatoid fibrous histiocytoma is now considered a separate entity. Although it can be seen at any age, it is more commonly seen in children and young adults (43). Clinically, it presents as a slow-growing tumor, sometimes simulating a hematoma, more often occurring in the extremities, although cases in the head and neck and trunk regions have also been described (43). More systemic symptoms including anemia, weight loss, and fever have been reported in a few cases (53). Histologically, it is composed of a multinodular proliferation of spindled or epithelioid cells, variably accompanied by blood-filled cystic spaces that account for the pseudoangiomatoid appearance, a thick fibrous pseudocapsule, and a pericapsular lymphoplasmacytic infiltrate (43,53). At MR imaging, angiomatoid fibrous histiocytoma often appears as a multicystic mass with fluid-fluid levels, reflecting internal hemorrhage, with variable signal intensity on T1- and T2-weighted images (46,53) (Fig 13). 13. Figure 13. Angiomatoid fibrous histiocytoma in a 12-year-old boy with a 5-month history of a mildly tender left forearm mass. Axial fat-suppressed T2-weighted MR image shows the presence of a predominantly cystic mass in the deep soft tissues of the left forearm, with involvement of the flexor and extensor compartments. Fluid-fluid levels and low-intensity fluid on this T2-weighted image are due to intralesional hemorrhage. Page 18
19 Angiomatoid fibrous histiocytoma has a low tendency for metastasis and is associated with a low rate of recurrence and a favorable outcome after aggressive surgical excision (43). Teaching Point Synovial Sarcoma Synovial sarcoma is the most common pediatric soft-tissue sarcoma after rhabdomyosarcoma (6,54). It is most prevalent in the first 5 decades of life, with 30% of the lesions seen in patients less than 20 years of age, and has been reported in patients as young as 2 years old (54). Despite its name, this tumor does not arise from synovial tissue but from primitive mesenchymal cells; in fact, it is only intraarticular in 6% 10% of cases (55). It is, however, most often found in a juxtaarticular location, close to the joint capsule, tendons, and bursae. Most synovial sarcomas are located in the extremities (55). The most common clinical presentation is a slowly growing painless mass that has been present for several weeks, months, or even years. Other patterns at presentation include pain and tenderness before the mass becomes palpable, acute arthritis or bursitis, chronic contracture, and occurrence after trauma (54). Histologically, the tumor is classified into monophasic (containing only spindle cells), biphasic (containing both epithelial and spindle cells), and poorly differentiated subtypes. A combined histopathologic, immunohistologic. and cytogenetic analysis typically shows spindle cells with a sarcomatous immunophenotype that express cytokeratin and/or epithelial membrane antigen and harbor a specific t(x;18)(p11.2;q11.2) translocation (54). MR imaging findings are in general nonspecific. The lesions tend to be well-defined masses isointense to muscle on T1-weighted images and hyperintense (often with heterogeneous signal intensity) on T2-weighted images (55,56) (Fig 14). Smaller lesions tend to be more homogeneous, sometimes simulating cysts on unenhanced images. In addition, because of their growth pattern, which favors displacement of adjacent structures rather than infiltration, it has been reported that synovial sarcoma is the malignant soft-tissue sarcoma most frequently misdiagnosed as a benign lesion. They enhance with a gadolinium contrast agent, and this helps in their differentiation from a cyst. They are often found in intimate relation to adjacent bone, with 50% being contiguous with bone and 21% showing cortical thinning or medullary invasion (55). Intralesional hemorrhage is not uncommon (40%) and accounts for the presence of fluidfluid levels in 18% of cases (55,56). Indeed, it has been suggested that the diagnosis of synovial sarcoma should be suspected in the presence of a juxtaarticular mass with a triple signal pattern (high, intermediate, and low intensity areas) on T2-weighted images and fluid-fluid levels (55). Page 19


20 14a. 14b. 14c Page 20
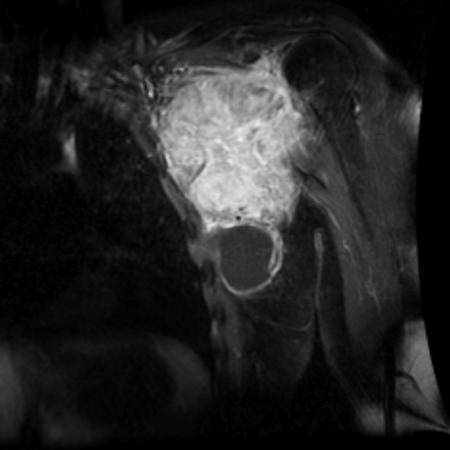
 Coronal T1-weighted MR image shows the presence of a large left axillary mass, which is slightly hyperintense to muscle except for a hypointense cystic component inferiorly.")
21 14d. Figure 14. Synovial sarcoma in a 16-year-old boy with a 2-month history of a left axillary mass and shoulder pain. (a) Coronal T1-weighted MR image shows the presence of a large left axillary mass, which is slightly hyperintense to muscle except for a hypointense cystic component inferiorly. (b) Coronal STIR MR image shows that most of the mass has intermediate signal intensity, with hyperintense areas due to the cystic component, particularly in its inferior aspect. (c) Coronal fat-suppressed gadolinium-enhanced T1-weighted MR image shows heterogeneous enhancement of the mass, with the exception of the large cystic component inferiorly. (d) Photomicrograph (original magnification, 20; hematoxylin-eosin stain) shows sheets of diffuse, proliferating plump spindle cells with large nuclei. A small nest of primitive cells with a swirling pattern of monotonous spindle cells is seen. Frequent mitoses are evident. These are the diagnostic features of the monophasic type of synovial sarcoma. Epithelioid Sarcoma Epithelioid sarcoma is a slow-growing but aggressive tumor with a frequent propensity to recur locally and to metastasize (57,58). It is a tumor of uncertain differentiation that at histology exhibits a characteristic nodular arrangement of epithelioid tumor cells and a tendency to zonal necrosis and coalescence as it spreads along fascial planes and aponeuroses (58). Epithelioid sarcoma is a tumor predominantly of young adults, but pediatric cases are well documented. It is most often seen in the upper extremity, especially distal to the elbow, followed by the lower extremity and rarely the external genitalia (57,58). A more aggressive subtype, called proximal-type epithelioid sarcoma, with a worse prognosis has recently been described (59). However, it is not known whether this represents a true subtype or a distinct tumor entity (59). It is more common in males than females (57 59). The clinical presentation is variable, ranging from small subcutaneous nodules or plaques that sometimes ulcerate, to more deep-seated lesions involving the deep tendons and fascial structures (58). Necrosis and hemorrhage can occur within the tumor, but calcification is rare (57,58). Consequently, the MR signal intensity and enhancement characteristics can be quite variable, and thus the overall appearance is nonspecific (57,58) (Fig 15). Peritumoral high signal intensity on T2-weighted images, ranging from minimal to extensive, has been reported and is Page 21


22 consistent histologically with an intense inflammatory response and/or edema adjacent to the tumor (58). 15a. 15b. Figure 15. Epithelioid sarcoma in a 13-year-old girl who presented with a right chest wall mass. (a) Coronal STIR MR image shows a hyperintense lobulated mass involving the lateral aspect of the right chest wall. The mass has a large soft-tissue component, but there is also abnormal high signal intensity in the right fourth and fifth ribs due to intraosseous extension. (b) Photomicrograph (original magnification, 20; hematoxylin-eosin stain) shows a nodule containing polygonal cells and spindle cells. In the polygonal cells, the nuclei are mildly pleomorphic, round to oval in shape, and contain vesicular chromatin with inconspicuous nucleoli, associated with moderate amounts of clear to pale eosinophilic cytoplasm. An area of apoptotic tumor cells is also noted (arrows). Surgery with wide local excision remains the only definitive treatment option. Local recurrences and metastases are frequent, the latter seen in the regional lymph nodes, lungs, scalp, bone, and brain (57,58). Alveolar Soft Part Sarcoma Alveolar soft part sarcoma is a rare slow-growing malignant tumor, accounting for 5% of pediatric nonrhabdomyosarcoma soft-tissue sarcomas (60). The exact histogenesis is still unknown, but the name is derived from the presence of nests of eosinophilic cells that contain abundant precrystalline cytoplasmic granules organized in a fashion resembling respiratory alveoli, separated by a rich vascular blood supply (61). The lesion is usually seen in adolescents and young adults; in children, it is slightly more common in girls than in boys (61). The most common site is the buttock or thigh, but a wide variety of other sites have also been described, including the head and neck, arm, chest, retroperitoneum, bladder, and stomach (61). It often presents as a painless mass. As a result of its prominent vascularity, the tumor may sometimes be pulsatile at examination and may Page 22

 (Fig 16).")
23 demonstrate a bruit on auscultation; it therefore may be misdiagnosed as an arteriovenous malformation (62,63). At MR imaging, the rich vascularity gives the tumor similar signal characteristics to those of hemangiomas. MR imaging demonstrates an intramuscular soft-tissue mass deep to the fascia, with equal-to-higher signal intensity than that of muscle on T1-weighted images and very high signal intensity on T2-weighted images (62,63) (Fig 16). Serpiginous, peripheral intratumoral and perilesional high-flow vessels and scattered punctate calcifications may appear as focal areas of low signal intensity (62,63). Central necrosis may further alter the signal characteristics internally (62). Avid enhancement is seen with a gadolinium contrast agent, with delayed contrast agent washout (62,63). This and the associated soft-tissue mass may help to differentiate alveolar soft part sarcoma from an arteriovenous malformation. 16a. 16b. Page 23
 Coronal STIR MR image shows a well-defined hyperintense mass involving the right sartorius muscle.")

24 Figure 16. Alveolar soft part sarcoma in a 17-year-old girl who presented with a right thigh mass. (a) Coronal STIR MR image shows a well-defined hyperintense mass involving the right sartorius muscle. (b) Photomicrograph (original magnification, 20; hematoxylin-eosin stain) shows an organoid pattern of uniform tumor cell nests within a delicate connective tissue stroma that contains a vascular network. Loss of tumor cell cohesion is seen in this pseudoalveolar pattern. Tumor cells are large, polygonal, and epithelioid and contain voluminous amounts of granular eosinophilic cytoplasm that may appear vacuolated. Eosinophilic crystalloid inclusions are present in the cytoplasm of some cells. The nuclei are large and contain a prominent nucleolus. Metastases to the lungs, brain, and bone have been reported in up to 30% of patients at diagnosis, and can characteristically occur quite late after the original diagnosis (61). Local recurrence and lymph node metastases are also seen (62). Treatment is surgical, with a better prognosis reported with smaller tumors, the presence of localized disease only, and a younger age at diagnosis (60,61). Ewing/Primitive Neuroectodermal Tumors Ewing and primitive neuroectodermal tumors are discussed together in this section because they are considered to represent different stages of neuroectodermal tumor differentiation. They are small, round, blue-cell tumors derived from the neural crest. In the past, the presence of neural differentiation favored the diagnosis of primitive neuroectodermal tumor over Ewing tumor. However, more recent studies have shown that both entities have the same molecular genetic abnormality and share immunophenotypic similarities that make them indistinguishable from each other. More commonly skeletal, the extraskeletal form is much rarer, seen in the paravertebral regions, thoracic wall (formerly known as Askin tumor), retroperitoneum, and lower extremities in older children or young adults (64). It is seldom seen in children of Asian or African descent (49). At MR imaging, they are well-circumscribed masses, isointense to muscle on T1- weighted images and heterogeneously hyperintense on T2-weighted images and show variable enhancement with a gadolinium contrast agent, depending on the degree of necrosis and hemorrhage (65) (Fig 17). 17a. 17b. Page 24
25 Figure 17. Primitive neuroectodermal tumor in an 11-year-old girl who presented with a 3-week history of enlarging right thigh mass, which was slightly tender on palpation. (a) Axial T1- weighted MR image shows a well-defined subcutaneous mass in the anteromedial aspect of the right upper thigh with no extension to the underlying musculature. The mass is predominantly hyperintense to muscle. (b) Axial fat-suppressed T2-weighted MR image shows that the mass is predominantly of high signal intensity, with a few small low-intensity foci. Also evident on this image is further extension of abnormal linear high signal intensity superficial to the gracilis muscle and along the fascial plane. Lymphoma Primary malignant involvement of soft tissues by extranodal lymphoma is rare, accounting for only 0.1% 2% of all soft-tissue tumors (66). More commonly, there is extension of a primary bone lymphoma into the surrounding tissues. The differentiation between these two entities can be difficult and may not be clinically important with regard to management (67). It may, however, have implications in terms of prognosis, as primary soft-tissue lymphoma with later disseminated disease has a poor prognosis (67). Histologically, lymphoma is a small, round, blue-cell tumor that acts as an infiltrative process rather than a compartmental condition. Immunohistochemical stains and molecular analysis for cell clonality are usually required to differentiate it from other diseases. The primary soft-tissue tumors are non-hodgkin lymphomas, mostly of the B-cell type. At MR imaging, lymphoma may appear as a nodular mass, more often seen with superficial masses, or as a more diffuse, infiltrative mass, particularly seen with deeper lesions. It frequently infiltrates multiple muscle groups and may involve adjacent bone. In these latter cases, the osseous involvement is mild relative to the extent of soft-tissue involvement. More extensive intraosseous involvement and/or focal cortical destruction with an associated softtissue mass suggests primary bone lymphoma rather than a primary soft-tissue lymphoma. Absence of cortical destruction, however, does not exclude primary bone involvement. The softtissue mass is usually hypo- or isointense to muscle on T1-weighted images and may contain areas of mild high signal intensity (66). The mass is usually hyperintense to muscle on T2- weighted images (although cases of hypointense masses have also been described [66,67]) and may enhance with intravenous gadolinium contrast agent (Fig 18). Lymphoma should be considered in the differential diagnosis of all soft-tissue masses, especially if there is a history of congenital immunodeficiency, organ transplantation, human immunodeficiency virus infection, or autoimmune connective tissue disorders. Page 25

26 18. Figure 18. Large-cell anaplastic lymphoma of T-cell origin in a 14-year-old boy with a 3-month history of left lower leg swelling. Coronal STIR MR image shows an extensive high-intensity mass involving the musculature in the lateral compartment of the lower leg. No abnormal signal intensity is noted in the adjacent fibula. Neurogenic Tumors Neurogenic tumors are not listed in the WHO classification of soft-tissue tumors, but we have included those affecting peripheral nerves as they can present clinically and at imaging as softtissue masses. They are uncommon in the pediatric age group. Lesions discussed include schwannoma, neurofibroma, and malignant peripheral nerve sheath tumor. Schwannoma Schwannoma is a benign, encapsulated nerve sheath tumor of neoplastic Schwann cells (68). Also called neurilemomas or neurinomas, they can be seen at any age but are more common in patients years of age (68,69). They are usually solitary, slow-growing small tumors (<5 cm) found in the cranial, spinal, and sympathetic nerve roots but can also be found in nerves in the flexor surfaces of the extremities, especially the ulnar and peroneal nerves (69,70). Multiple lesions can be associated with neurofibromatosis type 1 (69,70). Histologically, schwannomas are fusiform masses, eccentric to and separate from the adjacent nerve. When they arise from cutaneous or other small nerves, the nerve may be obliterated by the mass. They have two components: an Antoni A region, which is hypercellular, and an Antoni B region, which is hypocellular and loosely organized (68 70). Because of their eccentric location, they can be surgically excised and thus spare the adjacent nerve (69). Large tumors may exhibit cystic degeneration, calcification, hemorrhage, and fibrosis (69). They rarely if ever undergo malignant transformation. Page 26
27 Schwannomas share MR imaging features with other neurogenic tumors. They tend to be well-defined, fusiform masses arising along peripheral nerves, with a surrounding fat rim that is split around the tumor (split-fat sign) (69). The fusiform shape is useful in establishing a neurogenic origin, as it reflects the tubular entering and exiting nerve. This is more easily appreciated when the tumors affect large and deep nerves, and it is often not evident in more superficial lesions (69). A capsule representing the epineurium may be present and appear as a hypointense rim with all sequences. On T1-weighted images, the tumors are isointense or slightly hyperintense to muscle. On T2-weighted images, they are either of heterogeneous high signal intensity or display a target sign (68 70). The target sign is characterized by a hypo- to isointense center surrounded by a peripheral hyperintense ring, which corresponds histologically with a central zone of tightly packed fibers, consisting of collagen or a highly cellular component, and a peripheral zone of nonfibrillary stromal or myxoid material (68 71). The target pattern is usually absent in large masses and in tumors with cystic, hemorrhagic, or necrotic degeneration (70). Another finding on T2-weighted images that suggests a neurogenic origin is the fascicular sign, characterized by multiple small ringlike structures, with peripheral higher signal intensity representing the fascicular bundles (69). Schwannomas, as well as other neurogenic tumors, exhibit variable enhancement with gadolinium contrast agent. Teaching Point Neurofibroma Neurofibroma is the most common neurogenic tumor arising from peripheral nerves in children, although the most common ages at presentation are 20 to 30 years. Similar to schwannoma, neurofibroma is a benign nerve sheath tumor consisting mainly of Schwann cells (70). However, unlike schwannomas, they are inseparable from the normal nerve, and therefore surgical excision must include the adjacent nerve (69). Three types have been described: a localized form, which is the most common type (90% of neurofibromas); a diffuse form, more frequent in children and young adults and often involving the subcutaneous tissues of the head and neck; and a plexiform type (69). The localized and diffuse neurofibromas are usually solitary lesions not associated with neurofibromatosis. On the other hand, the presence of a plexiform neurofibroma is pathognomonic for neurofibromatosis type 1. Localized neurofibromas share MR imaging features with schwannomas (see discussion above). They are usually well-defined, encapsulated, fusiform soft-tissue masses less than 5 cm in diameter. On T1-weighted images, they are usually isointense to muscle (70). On T2-weighted images, they demonstrate heterogeneous high signal intensity and may exhibit a target pattern or a fascicular sign (68 70) (see discussion on schwannoma above). The lesion shows variable enhancement with gadolinium contrast agent (70,71). Plexiform neurofibroma refers to a networklike growth of the tumor, with involvement of multiple fascicles of a nerve, resulting in a diffuse mass of thickened nerve fibers surrounded by a proteinaceous matrix (72). Depending on their location, plexiform neurofibromas can be deep, superficial, or a combination of both. The importance of this differentiation relies on the different MR imaging appearances in the different locations. Deep plexiform neurofibromas do not involve the skin or subcutaneous tissues and appear as multinodular or fascicular masses, sometimes described as a bag of worms and often exhibiting a targetlike appearance on T2- weighted images (Fig 19); infrequently they can be heterogeneous without targets or more rarely may show a homogeneous appearance. Superficial plexiform neurofibromas, which are more common than the deep lesions, are more likely to be asymmetric in distribution, with a diffuse or infiltrating morphology, extend to the skin surface in a reticular and branching pattern, with smaller fascicles or nodules, and lack a target sign (72) (Fig 20). Because of this, superficial neurofibromas can be mistaken for venous malformations. Page 27


28 19. Figure 19. Deep plexiform neurofibroma in a 4-year-old boy with neurofibromatosis type 1. Axial fat-suppressed T2-weighted MR image shows a lobulated hyperintense mass predominantly involving the vastus intermedius muscle in the right thigh. The mass has a multinodular appearance resembling a bag of worms. The nodular components of the mass exhibit a characteristic target appearance, with a central zone of low signal intensity surrounded by a peripheral zone of higher intensity. 20. Figure 20. Superficial plexiform neurofibroma in a 16-year-old girl with neurofibromatosis type 1. Coronal STIR MR image shows a large, diffuse, poorly marginated, predominantly hyperintense lesion involving the subcutaneous tissues in the medial aspect of the right thigh. Note the absence of the target appearance seen in deep plexiform neurofibroma (Fig 19). Page 28


29 Malignant Peripheral Nerve Sheath Tumor Malignant peripheral nerve sheath tumor (MPNST), also known in the past as neurofibrosarcoma, is thought to arise from Schwann cells. This is a high-grade sarcoma with a poor prognosis. Although pediatric cases are well documented, it more commonly occurs in persons between 20 and 50 years of age and shows no sex predilection (69,73). It is strongly associated with neurofibromatosis type 1, as between 25% and 70% of patients with MPNST have this condition, and in this group MPNST tends to occur at an earlier age and affects mainly males (80%) (69). About 10% of patients with neurofibromatosis type 1 develop MPNST, and it usually arises within a preexisting plexiform neurofibroma (74). Persistent pain, neurologic symptoms, and rapid growth of a preexisting neurofibroma can be the presenting signs of MPNST (69,74). The most common sites of involvement are the major nerve roots, such as those of the sacrum, brachial plexus, and sciatic nerve (73). MR imaging findings are nonspecific. As mentioned in the section on schwannomas and neurofibromas, the neurogenic origin of MPNST may be suspected when it presents as a fusiform mass in a typical nerve distribution or when a target sign or fascicular sign is noted within the mass on T2-weighted images (see section on schwannomas). Most of these tumors have a nonspecific appearance, isointense or slightly hyperintense to muscle on T1-weighted images and heterogeneously hyperintense on T2-weighted images (70) (Fig 21). These lesions are difficult to distinguish from benign peripheral nerve sheath tumors (71). In patients with neurofibromatosis type 1, MR imaging has been used to detect malignant degeneration. It has been suggested that the lack of target signs in the largest component of the mass and heterogeneous lesions with patchy enhancement are useful patterns in the diagnosis of MPNST. 21a. 21b. Figure 21. MPNST in a 14-year-old boy with a 6-month history of mildly tender, enlarging mass in the left buttock that subsequently extended into the left upper thigh. (a) Coronal STIR MR image shows a large, lobulated, heterogeneous, hyperintense mass in the left gluteal region and left upper thigh. (b) Axial fat-suppressed T2-weighted MR image shows that the mass involves the musculature in the posterior aspect of the left upper thigh and is intimately related to the sciatic nerve (arrow). Page 29
.")
30 Positron emission tomography and positron emission tomography/ct have been recently reported (75) as being sensitive and specific diagnostic tools for MPNST associated with neurofibromatosis type 1. Treatment consists of wide local excision, but local recurrence is common and the overall 5-year survival rate is disappointing, reported to be only 43% (73). Pilomatricoma Also called pilomatrixoma (although etymologically incorrect) or calcifying epithelioma of Malherbe, pilomatricoma is a benign neoplasm arising from the hair matrix of cutaneous tissues and is most commonly found in children and young adults (76). Up to 68% are found on the head and neck, 29% on the trunk, and 17% on the extremities (74), with a female preponderance (76,77). They are slow-growing, stony hard, nontender dermal or subcutaneous masses that frequently calcify and occasionally ossify. They are small lesions, with a mean size of about 1.5 cm at excision although they may measure as much as 6 cm (76,77). Although the clinical diagnosis is often inaccurate, imaging is rarely performed, since it is thought by most authors to be of little clinical value. Treatment is surgical excision regardless of imaging findings (76). If imaging is required, sonography is usually the first modality for evaluating these lesions because of their small size and superficial location. If MR imaging is performed, the lesion is seen to be isointense to muscle on T1-weighted images. It is hypointense to muscle on T2-weighted images, but also shows patchy hyperintense areas and striations of high signal intensity that radiate from the center toward a hyperintense peripheral rim (77). Gadolinium enhancement is patchy or reticular centrally, corresponding to intercellular stroma pathologically (77). Peripheral enhancement of a connective tissue capsule may be seen in 79% of cases (77) (Fig 22). Peritumoral edema or inflammation can also be identified at MR imaging (77). The frequent association of internal calcification and occasionally ossification may decrease internal signal intensity on both T1- and T2-weighted images. 22. Figure 22. Pilomatricoma in an 8-year-old girl with a 6-month history of a right thigh mass that was firm and mobile on palpation and associated with fine superficial veins in the overlying skin. Axial fat-suppressed gadolinium-enhanced T1-weighted MR image shows a small well-defined dermal and subcutaneous nodule in the posterior aspect of the right thigh. Central and peripheral contrast enhancement, the latter reflecting enhancement of a connective tissue capsule, is seen. Page 30
Musculoskeletal Sarcomas
 Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
5/10. Pathology Soft tissue tumors. Farah Bhani. Mohammed Alorjani
 5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
Tumors of Adipose Tissue Tumors Epidemiology Clinical Features. Morphology. Mature Adipocytes Separated by delicate fibrous septa
 Tumors of Adipose Tissue Lipoma Liposarcoma Most commonly happens in female The most common soft tissue tumor o Originates from matured Adipocytes Most commonly happes at the 4 th and 5 th decade of life
Tumors of Adipose Tissue Lipoma Liposarcoma Most commonly happens in female The most common soft tissue tumor o Originates from matured Adipocytes Most commonly happes at the 4 th and 5 th decade of life
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
Case 8 Soft tissue swelling
 Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
Contents Part I Introduction 1 General Description 2 Natural History: Importance of Size, Site, Histopathology
 Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
A 24 year old male patient presented with a swelling on the dorsal aspect of left foot since 3 years. He was operated thrice before, outside, for
 A 24 year old male patient presented with a swelling on the dorsal aspect of left foot since 3 years. He was operated thrice before, outside, for same. Came to us with recurrence since last one year with
A 24 year old male patient presented with a swelling on the dorsal aspect of left foot since 3 years. He was operated thrice before, outside, for same. Came to us with recurrence since last one year with
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Case 9087 Retropharyngeal nodular fasciitis
 Case 9087 Retropharyngeal nodular fasciitis Santiago I 1; Cavalheiro F 2; Noruégas MJ 3; Sanches MC3 1 Hospital Infante D. Pedro, Aveiro, Portugal 2 Hospitais da Universidade de Coimbra, Portugal 3 Hospital
Case 9087 Retropharyngeal nodular fasciitis Santiago I 1; Cavalheiro F 2; Noruégas MJ 3; Sanches MC3 1 Hospital Infante D. Pedro, Aveiro, Portugal 2 Hospitais da Universidade de Coimbra, Portugal 3 Hospital
Soft Tissue Sarcomas: Questions and Answers
 Soft Tissue Sarcomas: Questions and Answers 1. What is soft tissue? The term soft tissue refers to tissues that connect, support, or surround other structures and organs of the body. Soft tissue includes
Soft Tissue Sarcomas: Questions and Answers 1. What is soft tissue? The term soft tissue refers to tissues that connect, support, or surround other structures and organs of the body. Soft tissue includes
* I have no disclosures or any
 Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
3/27/2017. Disclosure of Relevant Financial Relationships
 Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
Calcifying Aponeurotic Fibroma of the Knee: a Case Report with Radiographic and MRI Finding
 pissn 2384-1095 eissn 2384-1109 imri 2017;21:259-263 Calcifying Aponeurotic Fibroma of the Knee: a Case Report with Radiographic and MRI Finding Seung Hyun Lee 1,2, In Sook Lee 1,2, You Seon Song 1,2,
pissn 2384-1095 eissn 2384-1109 imri 2017;21:259-263 Calcifying Aponeurotic Fibroma of the Knee: a Case Report with Radiographic and MRI Finding Seung Hyun Lee 1,2, In Sook Lee 1,2, You Seon Song 1,2,
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Research Article A Clinicopathological Analysis of Soft Tissue Sarcoma with Telangiectatic Changes
 Sarcoma Volume 2015, Article ID 740571, 5 pages http://dx.doi.org/10.1155/2015/740571 Research Article A Clinicopathological Analysis of Soft Tissue Sarcoma with Telangiectatic Changes Hiroshi Kobayashi,
Sarcoma Volume 2015, Article ID 740571, 5 pages http://dx.doi.org/10.1155/2015/740571 Research Article A Clinicopathological Analysis of Soft Tissue Sarcoma with Telangiectatic Changes Hiroshi Kobayashi,
Myxo-inflammatory Fibroblastic sarcoma
 AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
Giant-cell tumor of the tendon sheath: when must we suspect it?
 Giant-cell tumor of the tendon sheath: when must we suspect it? Poster No.: C-0538 Congress: ECR 2014 Type: Educational Exhibit Authors: C. Santos Montón, J. M. Alonso Sánchez, D. C. Cuellar, P. A. Chaparro
Giant-cell tumor of the tendon sheath: when must we suspect it? Poster No.: C-0538 Congress: ECR 2014 Type: Educational Exhibit Authors: C. Santos Montón, J. M. Alonso Sánchez, D. C. Cuellar, P. A. Chaparro
Ultrasound imaging of vascular anomalies: pearls and pitfalls
 Ultrasound imaging of vascular anomalies: pearls and pitfalls Oscar Navarro, MD Dept. of Medical Imaging, University of Toronto Dept. of Diagnostic Imaging, The Hospital for Sick Children Declaration of
Ultrasound imaging of vascular anomalies: pearls and pitfalls Oscar Navarro, MD Dept. of Medical Imaging, University of Toronto Dept. of Diagnostic Imaging, The Hospital for Sick Children Declaration of
Introduction to Musculoskeletal Tumors. James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon
 Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
Newer soft tissue entities
 Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
Sonography of soft-tissue vascular lesions
 Sonography of soft-tissue vascular lesions Oscar M. Navarro Associate Professor, University of Toronto Dept. of Diagnostic Imaging, The Hospital for Sick Children Toronto, Canada Declaration of Disclosure
Sonography of soft-tissue vascular lesions Oscar M. Navarro Associate Professor, University of Toronto Dept. of Diagnostic Imaging, The Hospital for Sick Children Toronto, Canada Declaration of Disclosure
CYSTIC TUMORS OF THE KIDNEY JOHN N. EBLE, M.D. CYSTIC NEPHROMA
 Page 1 CYSTIC TUMORS OF THE KIDNEY JOHN N. EBLE, M.D. Department of Pathology & Laboratory Medicine Phone (317) 274-4806 Medical Science A-128 FAX: (317) 278-2018 635 Barnhill Drive jeble @iupui.edu Indianapolis,
Page 1 CYSTIC TUMORS OF THE KIDNEY JOHN N. EBLE, M.D. Department of Pathology & Laboratory Medicine Phone (317) 274-4806 Medical Science A-128 FAX: (317) 278-2018 635 Barnhill Drive jeble @iupui.edu Indianapolis,
Myositis Ossificans Mimicking Sarcoma, the Importance of Diagnostic Imaging Case Report
 Signature: Pol J Radiol, 2014; 79: 228-232 DOI: 10.12659/PJR.890209 CASE REPORT Received: 2013.12.18 Accepted: 2014.01.27 Published: 2014.07.28 Authors Contribution: A Study Design B Data Collection C
Signature: Pol J Radiol, 2014; 79: 228-232 DOI: 10.12659/PJR.890209 CASE REPORT Received: 2013.12.18 Accepted: 2014.01.27 Published: 2014.07.28 Authors Contribution: A Study Design B Data Collection C
A 25 year old female with a palpable mass in the right lower quadrant of her abdomen
 May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
Part 1. Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013
 Part 1 Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013 Pediatric Pathology Soft Tissue Tumors AN UPDATE Rita Alaggio Azienda Ospedaliera Università di Padova Soft Tissue Tumors More
Part 1 Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013 Pediatric Pathology Soft Tissue Tumors AN UPDATE Rita Alaggio Azienda Ospedaliera Università di Padova Soft Tissue Tumors More
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON
 Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Radiological Reasoning: Acutely Painful Swollen Finger. Musculoskeletal Imaging Chew and Richardson Benign-Appearing Bone Mass.
 Musculoskeletal Imaging Chew and Richardson Benign-Appearing Bone Mass AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY This Radiological Reasoning article is available for SAM credit and CME credits
Musculoskeletal Imaging Chew and Richardson Benign-Appearing Bone Mass AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY This Radiological Reasoning article is available for SAM credit and CME credits
Index. Note: Page numbers of article titles are in boldface type.
 Magn Reson Imaging Clin N Am 12 (2004) 185 189 Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint, MR imaging findings concerning, 161 Acromion, types of, 77 79
Magn Reson Imaging Clin N Am 12 (2004) 185 189 Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint, MR imaging findings concerning, 161 Acromion, types of, 77 79
Atypical Palisaded Myofibroblastoma of Lymph Node: Report of a rare case.
 ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 Atypical Palisaded Myofibroblastoma of Lymph Node: Report of a rare case. V Kinnera, R Nandyala, M Yootla, K Mandyam Citation V Kinnera, R
ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 Atypical Palisaded Myofibroblastoma of Lymph Node: Report of a rare case. V Kinnera, R Nandyala, M Yootla, K Mandyam Citation V Kinnera, R
Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
 Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
Monophasic Synovial Carcinoma of knee joint- A Case Report and Review of Literature
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.5 March. (2018), PP 13-17 www.iosrjournals.org Monophasic Synovial Carcinoma of knee
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.5 March. (2018), PP 13-17 www.iosrjournals.org Monophasic Synovial Carcinoma of knee
Dupuytren's Contracture Assessment
 Dupuytren's Contracture Assessment Link to guidance: http://www.enhertsccg.nhs.uk/ bedfordshire-and-hertfordshire-priorities-forum Dupuytren's contracture - clinical presentation for patients History Examination
Dupuytren's Contracture Assessment Link to guidance: http://www.enhertsccg.nhs.uk/ bedfordshire-and-hertfordshire-priorities-forum Dupuytren's contracture - clinical presentation for patients History Examination
MRI XR, CT, NM. Principal Modality (2): Case Report # 2. Date accepted: 15 March 2013
: Case Report # 2. Date accepted: 15 March 2013") Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
Essentials of Clinical MR, 2 nd edition. 51. Primary Neoplasms
 51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Case Presentation 主治醫師 : 宋文鑫日期 :
 Case Presentation 主治醫師 : 宋文鑫日期 : 2015-2-28 General Data Name:OOO Chart Number:OOOOOOO Date of Admission:2014 年 08 月 04 日 Age: 33 y/o Sex:female Occupation : 會計 Chief Complaint Palpable soft tissue mass
Case Presentation 主治醫師 : 宋文鑫日期 : 2015-2-28 General Data Name:OOO Chart Number:OOOOOOO Date of Admission:2014 年 08 月 04 日 Age: 33 y/o Sex:female Occupation : 會計 Chief Complaint Palpable soft tissue mass
-The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
- In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
Ultrasound of soft-tissue vascular anomalies
 Ultrasound of soft-tissue vascular anomalies Oscar M. Navarro Associate Professor, University of Toronto Dept. of Diagnostic Imaging, The Hospital for Sick Children Toronto, Canada Declaration of Disclosure
Ultrasound of soft-tissue vascular anomalies Oscar M. Navarro Associate Professor, University of Toronto Dept. of Diagnostic Imaging, The Hospital for Sick Children Toronto, Canada Declaration of Disclosure
An Overview of Genital Stromal Tumors
 An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Pediatric Soft-Tissue Sarcomas. Beth McCarville, MD St. Jude Children s Research Hospital Memphis, Tn
 Pediatric Soft-Tissue Sarcomas Beth McCarville, MD St. Jude Children s Research Hospital Memphis, Tn Overview Histologic classifications Characteristic imaging features Helpful clinical characteristics
Pediatric Soft-Tissue Sarcomas Beth McCarville, MD St. Jude Children s Research Hospital Memphis, Tn Overview Histologic classifications Characteristic imaging features Helpful clinical characteristics
PLEOMORPHIC ADENOMA ( BENIGN MIXED TUMOR )
") ( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Ultrasound Evaluation of Masses
 Ultrasound Evaluation of Masses Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Advisory Panel: GE,
Ultrasound Evaluation of Masses Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Advisory Panel: GE,
Residents Teaching Files
 SPECIAL EXHIBIT Residents Teaching Files Epithelioid Hemangioendothelioma of the Lower Extremity 1 Elizabeth A. Ignacio, MD Kathryn M. Palmer, MD Sharad C. Mathur, MD Arnold M. Schwartz, MD, PhD Wayne
SPECIAL EXHIBIT Residents Teaching Files Epithelioid Hemangioendothelioma of the Lower Extremity 1 Elizabeth A. Ignacio, MD Kathryn M. Palmer, MD Sharad C. Mathur, MD Arnold M. Schwartz, MD, PhD Wayne
Fun with Fat. General Rules. Case
 Fun with Fat General Rules Imaging: location (deep vs. superficial) Superficial lesions are seldom liposarcomas Deep lesions may be benign or malignant Myxoid stroma is common in benign and malignant lesions
Fun with Fat General Rules Imaging: location (deep vs. superficial) Superficial lesions are seldom liposarcomas Deep lesions may be benign or malignant Myxoid stroma is common in benign and malignant lesions
Topics. Musculoskeletal Infection Extremities. Detection of Infection. Role of Imaging in Extremity Infection. Detection of Infection
 Topics Musculoskeletal Infection Extremities Nuttaya Pattamapaspong M.D. Department of Radiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand Role of imaging in extremity infection
Topics Musculoskeletal Infection Extremities Nuttaya Pattamapaspong M.D. Department of Radiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand Role of imaging in extremity infection
21/07/2017. Hobnail endothelial cells are not the same as epithelioid endothelial cells
 UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
Pleomorphic Xanthoastrocytoma
 Pleomorphic Xanthoastrocytoma Christine E. Fuller Keywords Pleomorphic xanthoastrocytoma; Pleomorphic xanthoastrocytoma with anaplastic features 2.1 OVERVIEW Pleomorphic xanthoastrocytoma (PXA) is an uncommon
Pleomorphic Xanthoastrocytoma Christine E. Fuller Keywords Pleomorphic xanthoastrocytoma; Pleomorphic xanthoastrocytoma with anaplastic features 2.1 OVERVIEW Pleomorphic xanthoastrocytoma (PXA) is an uncommon
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Mark D. Murphey, MD, FACR
 Fundamental Concepts of Musculoskeletal Neoplasm: CT and MRI Mark D. Murphey, MD, FACR Important Features in Evaluation of Musculoskeletal Masses Differential diagnosis Preoperative assessment and staging
Fundamental Concepts of Musculoskeletal Neoplasm: CT and MRI Mark D. Murphey, MD, FACR Important Features in Evaluation of Musculoskeletal Masses Differential diagnosis Preoperative assessment and staging
None. Everyone, especially Dr. Mitchell for helping me find cases!
 None. Everyone, especially Dr. Mitchell for helping me find cases! Sagittal T1 Coronal T1 Axial T1 Sagital T1, Axial T1+, Axial T2 Axial CT +, thorax Axial T1 Within the muscle, not connected to
None. Everyone, especially Dr. Mitchell for helping me find cases! Sagittal T1 Coronal T1 Axial T1 Sagital T1, Axial T1+, Axial T2 Axial CT +, thorax Axial T1 Within the muscle, not connected to
Evening Specialty Conference Bone and Soft Tissue Pathology. Diagnostic pitfalls in bone and soft tissue pathology
 Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Brief History. Identification : Past History : HTN without regular treatment.
 Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Criteria of Malignancy. Evaluation Score
 30 5 Diagnostic Criteria Criteria of Malignancy Table 5.2 lists criteria in contrast-enhancing MR mammography that strongly indicate the presence of malignancy or are unspecific. Unifactorial evaluation
30 5 Diagnostic Criteria Criteria of Malignancy Table 5.2 lists criteria in contrast-enhancing MR mammography that strongly indicate the presence of malignancy or are unspecific. Unifactorial evaluation
Hemangiomas and Other Vascular Tumors
 facebook.com/cincykidsrad Hemangiomas and Other Vascular Tumors Disclosures No relevant financial disclosures Bernadette L. Koch, M.D. Departments of Radiology and Pediatrics Cincinnati Children s Hospital
facebook.com/cincykidsrad Hemangiomas and Other Vascular Tumors Disclosures No relevant financial disclosures Bernadette L. Koch, M.D. Departments of Radiology and Pediatrics Cincinnati Children s Hospital
A case of giant cell tumour of soft parts in a horse Francesco Cian 1, Sarah Whiteoak 2, Jennifer Stewart 1
 A case of giant cell tumour of soft parts in a horse Francesco Cian 1, Sarah Whiteoak 2, Jennifer Stewart 1 1 Animal Health Trust, Newmarket, UK 2 608 Equine and Farm Vets, Rowington, UK Signalment: Horse,
A case of giant cell tumour of soft parts in a horse Francesco Cian 1, Sarah Whiteoak 2, Jennifer Stewart 1 1 Animal Health Trust, Newmarket, UK 2 608 Equine and Farm Vets, Rowington, UK Signalment: Horse,
MRI Of Locally Recurrent Soft Tissue Tumors Of The Musculoskeletal System
 ISPUB.COM The Internet Journal of Radiology Volume 5 Number 2 MRI Of Locally Recurrent Soft Tissue Tumors Of The Musculoskeletal System C Costelloe, A Yasko, W Murphy, R Kumar, V Lewis, P Lin, R Stafford,
ISPUB.COM The Internet Journal of Radiology Volume 5 Number 2 MRI Of Locally Recurrent Soft Tissue Tumors Of The Musculoskeletal System C Costelloe, A Yasko, W Murphy, R Kumar, V Lewis, P Lin, R Stafford,
University Journal of Surgery and Surgical Specialities
 University Journal of Surgery and Surgical Specialities Volume 1 Issue 1 2015 EXTRA SKELETAL MESENCHYMAL CHONDROSARCOMA :A CASE REPORT Rajaraman R Subbiah S Navin Naushad Kilpaulk Medical College Abstract:
University Journal of Surgery and Surgical Specialities Volume 1 Issue 1 2015 EXTRA SKELETAL MESENCHYMAL CHONDROSARCOMA :A CASE REPORT Rajaraman R Subbiah S Navin Naushad Kilpaulk Medical College Abstract:
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Angiomatoid Fibrous Histiocytoma : A Case Report
 영남의대학술지제24권제2호 Yeungnam Univ. J. of Med. Vol.24 No.2 p315-321, Dec. 2007 증례 Angiomatoid Fibrous Histiocytoma : A Case Report Joon Hyuk Choi, Woo Jung Sung, Nam Hyuk Lee* Department of Pathology, and *Department
영남의대학술지제24권제2호 Yeungnam Univ. J. of Med. Vol.24 No.2 p315-321, Dec. 2007 증례 Angiomatoid Fibrous Histiocytoma : A Case Report Joon Hyuk Choi, Woo Jung Sung, Nam Hyuk Lee* Department of Pathology, and *Department
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Abid Irshad, MD Director Breast Imaging. Medical University of South Carolina Charleston
 Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
the urinary system pathology Dr. Fairoz A Eltorgman
 the urinary system pathology Dr. Fairoz A Eltorgman Tumors of the renal pelvis & kidney Benign tumors of the renal pelvis: Hemangioma Leiomyoma Malignant tumors: Transitional cell carcinoma Squamous cell
the urinary system pathology Dr. Fairoz A Eltorgman Tumors of the renal pelvis & kidney Benign tumors of the renal pelvis: Hemangioma Leiomyoma Malignant tumors: Transitional cell carcinoma Squamous cell
Chief complaint. A mass at right chest
 Chief complaint A mass at right chest Present illness This 1-year-5-month-old girl had a mass at right side chest since one month ago. flat and not tender at first In the recent 2 days, the mass enlarged
Chief complaint A mass at right chest Present illness This 1-year-5-month-old girl had a mass at right side chest since one month ago. flat and not tender at first In the recent 2 days, the mass enlarged
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Grading of Bone Tumors
 Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
MSK Interesting Cases. Dr Yap Sheau Huey
 MSK Interesting Cases Dr Yap Sheau Huey Case 1: History 41 y.o man, surf skier C/o pain over anterior left 5 th to 8 th ribs. Worse after sport activity. Chest Radiograph US Periostitis and early callus
MSK Interesting Cases Dr Yap Sheau Huey Case 1: History 41 y.o man, surf skier C/o pain over anterior left 5 th to 8 th ribs. Worse after sport activity. Chest Radiograph US Periostitis and early callus
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Spectrum of MRI Findings of Synovial Sarcoma
 Spectrum of MRI Findings of Synovial Sarcoma Poster No.: C-1523 Congress: ECR 2014 Type: Educational Exhibit Authors: J. A. Molina, J. Llauger Rosselló, J. Palmer Sancho, G. M. 1 1 2 1 3 1 1 Santandreu,
Spectrum of MRI Findings of Synovial Sarcoma Poster No.: C-1523 Congress: ECR 2014 Type: Educational Exhibit Authors: J. A. Molina, J. Llauger Rosselló, J. Palmer Sancho, G. M. 1 1 2 1 3 1 1 Santandreu,
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Endometrial Stromal Tumors
 Endometrial Stromal Tumors WHO Categories: Endometrial Stromal Nodule (ESN) Endometrial Stromal Sarcoma, low grade (LGESS) Endometrial Stromal Sarcoma, high grade (HGESS) Undifferentiated Uterine Sarcoma
Endometrial Stromal Tumors WHO Categories: Endometrial Stromal Nodule (ESN) Endometrial Stromal Sarcoma, low grade (LGESS) Endometrial Stromal Sarcoma, high grade (HGESS) Undifferentiated Uterine Sarcoma
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE
 SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE Jason L. Hornick, MD, PhD July 18, 2013 Department of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA, USA I have no disclosures. New Soft
SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE Jason L. Hornick, MD, PhD July 18, 2013 Department of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA, USA I have no disclosures. New Soft
Essentials of Clinical MR, 2 nd edition. 73. Urinary Bladder and Male Pelvis
 73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
SMOOTH MUSCLE TUMOURS
 SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
The Radiology Assistant : Bone tumor - ill defined osteolytic tumors and tumor-like lesions
 Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
A case of pedunculated intraperitoneal leiomyoma
 Jichi Medical University Journal Chio Shuto Kuniyasu Soda Takayoshi Yoshida Fumio Konishi Abstract We report a very rare case of a pedunculated intraperitoneal leiomyoma in the parietal peritoneum of the
Jichi Medical University Journal Chio Shuto Kuniyasu Soda Takayoshi Yoshida Fumio Konishi Abstract We report a very rare case of a pedunculated intraperitoneal leiomyoma in the parietal peritoneum of the
Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
CTA/MRA of Pediatric Hepatic Masses Radiology-Pathology Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº70, pág. 41-50, Abr.-Jun., 2006 CTA/MRA of Pediatric Hepatic Masses Radiology-Pathology Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº70, pág. 41-50, Abr.-Jun., 2006 CTA/MRA of Pediatric Hepatic Masses Radiology-Pathology Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington