Bone pathology 2. László Kereskai MD.
|
|
|
- Veronica Moody
- 5 years ago
- Views:
Transcription
1 Bone pathology 2. László Kereskai MD.
2 BONE-FORMING TUMORS Osteoid osteoma and osteoblastoma: Osteoid osteoma Most frequent btw ys. Best known symptom is intensive pain with easy precise localisation. In lumbar foms scoliosis can happen. Localisation: femur, tibia, humerus, bones of hands and feet, vertebrae, fibula. In long tubular bones usually metaphyseal; 85 % cortical; in the spine not in the vertebral bodies. Radiology: radiolucent central nidus, which rarely larger than 1,5 cm, sometimes the center is dens with a sclerotic reaction aroud (that can be several cms large, because of this phenomenon it is easy to mix with Garré osteomyelitis.
3 BONE-FORMING TUMORS Microscopically: the nidus is made of variously calcified osteoid surrounded by osteoblasts embedded in vascular-rich connective tissue. This change is so tipical that it is easy to identify either in fragmented sample as well. Around various amount of dense bone. Clinical settings: stronger pain during nights, NSAIDs are effective. Preoperative CT localisation and intraoperative scintigraphy increases the effectivness of the procedure. After preoperative administration of tetracycline during operation the nidus can be visualize in UV light.



4 Osteoid osteoma

5 Osteoid osteoma- nidus
6 BONE-FORMING TUMORS Osteoblastoma Related to the previous with larger nidus (giant osteoid osteoma), smaller or absent sclerotic zone, no intensive pain. In some cases there can be a cartilagineous matrix iside the lesion. Localisation: Usually growth in spongiosa, spine, larger bones of lower extremity. A possible complication is osteomalacia. It can be hard to distinguish from osteosarcoma (frequenty: bizarr cells, degenerative changes). Key role of radiological appearance.



7 Osteoblastoma
8 BONE-FORMING TUMORS OSTEOSARCOMA General characteristics Most frequent malignant bone tumor. Two age peaks: ys, and over 50 ys (frequently secondary). Pathogenesis, predisposin conditions Paget disease (over 40 ys). Irradiation: Every age, 1-15 ys latency. Chemotherapy: childhood, alkylating agents. Benign bone processes: fibrous dysplasia, osteochondromatosis, chondromatosis. Foreign bodies: hip prostheses, low case number. Trauma: questionable, usually it makes attention to the previously present tumor. Infection: questionable, víral origin? Genetics: acquired nonspecific changes in 70%. RB and p53 mutations are more important, but the mechanism is unclear.
9 Localisation BONE-FORMING TUMORS OSTEOSARCOMA Most typical: metaphysis of long bones: distal femur, proximal tibia, proximal metaphysis of humerus. (Dia- and epiphysis is rare as well as flat and short tubular bones.) Can be multiple: childhood, agressive form, sclerotic radiológical picture, p53 mutation in some cases. Usually medullary start, then spread to the cortex, cortical origin is rarer this is usually diaphyseal.

10 BONE-FORMING TUMORS OSTEOSARCOMA
11 Makroscopy, spread BONE-FORMING TUMORS OSTEOSARCOMA Different macroscopic appearance (ratio of bone, cartilage, vessels cellular stroma), bony hard, cystic, friable, haemorrhagic forms. Ways of spread from metaphysis: through medullary canal; into the cortex; elevation and perforation of periosteum: Codman triangle, not pathognomonic in 100%for malignant tumor, can be caused by hematoma or any other process which elevate the periosteum; break into soft tissue; into the epiphysis after closure of the plate; into joint cavity; production of satellit noduls proximally from the original tumorsin the same or the next bone transversing the joint (skip metastases), probably thi is responsible for local recurrance and further metastasises; hematogenous metastasis : lung (98%), other bones (37%), pleura (33%), heart (20%), almost never lymph node ms. The lung metastasis can be massive intraluminal form in pulmonary arteries.



12 BONE-FORMING TUMORS OSTEOSARCOMA
13 Microscopy BONE-FORMING TUMORS OSTEOSARCOMA The key for diagnosis: osteoid and/or bone formation by tumor cells: eosinophilic staining, glassy apprearance, irregular contours, osteoblastic rim around. Hard to dsicriminate from hyalinized collagen. Osteoid: rather homogenous than fibrillary, spots because of early calcification, the neighbouring cells are plump (osteoblasts). Thin tubular, anastomosing microtrabecules: basophil stainig (like fungal hyphae). Osteblastis zones are intermixed with chondroblastic and fibroblastic zones, with variable ratio. The diagnosis rests on the demonstration of malignant bone formation not coupled with cartilage independently from the ratio of neoplastic cartilage or fibroblastic areas. Many morpholigical variants esist, osteoclast-type giant cells are frequently present. Diff dg.: wide spectrum, large callus, myositis ossificans, fibrous dysplasia, osteoblastoma, fibrosarcoma, chondrosarcoma, giant cell tumor, malignant lymphoma, metastatic carcinoma.



14 BONE-FORMING TUMORS OSTEOSARCOMA
15 BONE-FORMING TUMORS OSTEOSARCOMA Microscopic variants: They can present focally or mixed, can have prognostic role. Teleangiectatic : Similar to aneurysmal bone cyst, frequent pathological fractures, in between the bloody channels in the septa malignant stroma, worse prognosis (?). Small cell: Diff. dg: Ewing, lymphoma; diffuse growth, frequently spindle cells, focal osteoid production. Fibrohistiocytic: Especially in sites of soft tissue infiltration it can be impossible to distinguish from MFH. Anaplastikus: Pleiomorphic sarcoma and metastatic carcinoma is the diff. dg.
16 BONE-FORMING TUMORS OSTEOSARCOMA Microscopic variants: well differencited intramedullary Many times underdiagnosed as fibrous dysplasia, other cases are similar to parosseal form. Usually adults, femoral and tibial involvement. Spindle cells, few mitoses, abundant osteoid. Frequentrelapse, bur rare metastasis (excluding those with transfoemation to coventional osteosarcoma). Difference from fibrous dysplasia: cortex destruction (radiology!).
17 BONE-FORMING TUMORS OSTEOSARCOMA Special types: Juxtacortical (parosseal) Relatively older age group, metaphysis of long bones (typical in the posterior surface of femur), slow growth (sometimes 15 ys course). Large lobulated mass, encircling the bone, late medullary infiltration with more immature picture. Satellite noduls are possible. Mikroscopy: irregular well-formed bony tissue, dense fibrous spindle cell stroma. Good prognosis, either with segmental resection. The parosseal tumor can undergo dedifferentiation during relapses.

18 Juxtacortical (parosseal) OSc
19 BONE-FORMING TUMORS OSTEOSARCOMA Periosteal: Different from the previous one. Growth in the surfaceof long bones (upper tibia, femur). Small, radiolucent lesions in cortex, rarely infiltrate the medulla. Mikroscopically usually high grade osteosarcom with a substantial amount of cartilagineous component (similar to juxtacortical chondrosarcoma). Jaw osteosarcoma: Slightly older age, prominent chondroblastic component. Body of mandible proc. Alveolaris of maxilla. Relatively good prognosis. On the base of Paget disease: In polyostotic type, many times the tumor is multicentric as well. Pelvis, humerus, femur, tibia and. Many osteoclast with atypical osteoblasts. The prognosis is poor.
20 BONE-FORMING TUMORS OSTEOSARCOMA Diagnosis Typical x-ray picture, but with many overlaps with reactive conditions, benign tumors, there is a need for preoperative biopsy: open (tumornormal border), needle-biopsy (effective, especially in hidden places, like spine), fine needle aspiration, frozen section. Laboratory findings: ALP elevation (depending on bone production, not specific). Therapy: based on aggressive chemotherapy and limb salvaging surgery
21 CARTILAGE-FORMING TUMORS Osteochondroma: The most frequent benign bone tumor. Usually symptomless, but can affect the function of neighbouring structures (tendons, vessels). Spontaneous regression can happen. Localisation: metaphyseal in femur, tibia, upper humerus, in pelvic bones. Typical radiological picture, usually it grows opposite to the next joint. Average age 10 ys, usually below 20 ys. Average diameter 4 cm, but can be as large as 10 cm, the smaller ones are sessile, the larger are pedunculated.
22 CARTILAGE-FORMING TUMORS Covered by fibrous capsule (periosteum), in large lesions there is a lobulated hyaline cartilage cap (about 6 mm thick, rarely more than 1 cm), endochondral ossification, centrally normal trabecular bone with bone marrow. In older lesions the cap becomes thin or disappear completely. Around the head a secondary bursa (bag) can form (with caltilagineous-bony free bodies in it). There is a familial mpl. variant (osteochondromatosis), in which the individual lesions are similar to those in solitary form. Transformation to chondrosarcoma in solitary form is quite rare, in multiple forms can reach 10%.



23 Osteochondroma


24 Osteochondroma
25 CARTILAGE-FORMING TUMORS Chondromas: Most frequent in small bones of hands and feet, mainly in proximal phalanges, very rare in distal phalanges. They arise mostly in the spongiosa of diaphysis (enchondroma), then expand and cause cortical thinning. Multiple in 30% (unilateral distribution: Ollier disease, association with soft part hemangiomas: Mafucci sy., in these cases more frequent malignant transformation, usually to chondrosarcoma). Enchondomas in ribs and long bones are extremely rare, usually with massive calcification.
26 CARTILAGE-FORMING TUMORS Chondromas: Rare localisation: juxtacortical or periosteal localisation in long bones or in the small bones of hands and feet, usual features: cortical erosion and sclerosis, sharp edge, in case of incomplet excision relapse can happen. Microscopy: mature, lobular hyaline cartilage with focal myxoid degeneration, calcification and endochondral ossification. The juxtacortical variants are frequently more cellular and can contain plump or binucleated cartilage cells.


27 Chondroma
28 CARTILAGE-FORMING TUMORS Chondroblastoma: Male predominance, below 20 ys. Start in the epiphysis of long bones before the disappearance of epiphysis cartilage (distal femur, proximal humerus and tibia). Radiologically well circumscribed, contain rarefactions. Spread from epiphysis into metaphysis or joint. Microscopy: high cellularity and variability, sometimes osteoclast type giant cells. Main element: embryonal chondroblast, which is not capable to produce intercellular chondroid matrix. Usually polygonal,but can be spindle-shaped. The nclear membrane is thick and sharp, nuclei are roundish or indented, lobulated sometimes mimicking Langerhans cells. Recidive lesions can show some atypia, but this not a sign of malignant transformation. In small zones focal calcification can be present (chicken wire).
29 CARTILAGE-FORMING TUMORS Chondroblastoma: ELMI: the tumor cells look like normal hyaline cartilage cells in culture. IHC: vimentin and S-100. The origin was not clear for a long time, ELMI and IHC findings support the chondroid origin (+ calcification, well differentiated chondroid areas). Clinical settings: frequently severe pain, diagnosis from fine needle biopsy (chondroblasts, giant cells, chondroid matrix). Th: curettage, bone replacement (80% enough locally). Rare agressive variants (soft tissue invasion, lymph or blood vessel tumor thrombosis) mainly in pelvis, sometimes lung metastasis formation after surgical intervention.


30 Chondroblastoma
31 CARTILAGE-FORMING TUMORS CHONDROSARCOMA Conventional chondrosarcoma: ys, very rare in childhood (more frequent: osteosc with chondroid component) and it occurs in extremities (opposite to adult forms). Central: Medullary, flat or long bones. Radiology: quite typical osteolytic lesion with calcification, uneven borders, fusiform widening of bone, cortical invasion but rarely break through periosteum. Mostly: pelvic bones, ribs (costochondral junctions), shoulder. Very rare in bones of hands and feet. Skull involvement is not rare, os temporale location (diff. dg: chordoma, meningeoma, glomus jugulare tumor).
32 CARTILAGE-FORMING TUMORS CHONDROSARCOMA Conventional chondrosarcoma Peripheric: De novo and transfomation from osteochondroma (1-2% chance in solitary forms). Signs of malignant trf in osteochondroma: accelerated growth in adolescent age, size over 8 cm, cartilagineous cap irregular or thicker than 3 cm. Radiology: large tumor, heavily calcified center surrounded by less dense peripheric calcified zone. Signs of malignant transformation: irregular border of cap, clear areas inside the lesion. Juxtacortical (periosteal) Localisation: long bones (mainly femur). Macroscopy: large, lobulated mass with scattered calcification. Relationship with periosteal osteosarcoma.


33 Chondrosarcoma
34 CARTILAGE-FORMING TUMORS Microscopy: CHONDROSARCOMA Various differentiation, formation of cartilage matrix without bone formation. Grading: well, moderately and poorly differentiated variants. Distinction between well-differentiated chondrosarcoma and chondroma sometimes (almost) impossible (radiology, architecture, cytology large, hyperchromatic nuclei, more nuclei in one cell- can be important), chondrosarcoma frequently involve trabecular bone. Fast grow, size over 8 cm is important, as well. In long bones, ribs in case of large tumors at least small atypia supports malignancy, while in the bones of hands and feet pronounced atypical features don t mean malignancy. The signs of cytologic atypia can be present just in a small fraction of the tumor (small biopsy specimen). The tumor can contain bone, this is an endochondral ossification because of cartilage resorption, not neoplastic.


35 CARTILAGE-FORMING TUMORS CHONDROSARCOMA
36 PORCKÉPZŐ DAGANATOK CHONDROSARCOMA Cytogenetics: c-myc amplification and c-erbb-2 expression can be present, in high-grade tumors p53 amplification. Treatment: In case of large pelvic tumor large block dissection or hemipelvectomy can be necessary, sometimes without previous sampling (90 %: chondrosc. is the dg.). In costal tumors and in well differentiated variants of long bones in extremities, segmental resection is the solution. Variants: Clear cell Myxoid Dedifferentiated Mesenchymal
37 FIBROSUS AND FIBRO-OSSEOUS TUMORS Fibrosus cortical defect and non-ossifying fibroma: Adolescents, long bones (both end of tibia, lower femur). Excentric, sharply delimited lesions not too far from epiphysis, sometimes together with the abnormality of epiphysis. Loose consistency and intramedullary component: non-ossifying fibroma. Neoplastic or developmental anomaly? Macroscopy: granular, brownish-reddish. Microscopy: cellular fibrous bands in storiform arrangement, scattered osteoclasts, foamy and hemosiderin-laden macrophages. Mainly in adult cases: benign fibrous histiocytoma. Little symptoms, only pain, frequently incidental finding in x-ray, fracture because of the thinned cortex.



38 Non-ossifying fibroma
39 FIBROSUS AND FIBRO-OSSEOUS TUMORS, FIBROSUS DYSPLASIA Benign tumor, suggesting a developmenal arrest as well, there is no complete development of mature structures. Monoostotic form: 70%, boys and girls involved equally, early adolescent age. Femur, tibia, ribs, jaw, calvaria and humerus. Usually asymptomatic-accidental finding; pain, deformity (skull). Polyostotic form without endocrine disorders: 27%, a little bit erlier than the previous one. Femur, skull, tibia, humerus, ribs, fibula, radius, ulna, mandible and vertebrae, 50% craniofacial involvement in mild cases, 100% in extensive disease. Shoulder and hip deformities.
40 FIBROSUS AND FIBRO-OSSEOUS TUMORS, FIBROSUS DYSPLASIA Polyostotic fibrosus dysplasia with café-au-lait skin pigmentation and endocrinopathy: McCune-Albright syndrome (3%). Sexual precocy, hyperthyrosis. hypophysis adenomas secreting GH, primary adrenal hyperplasia. Gain-of function mutation in GNAS gene resulting in hyperactive guanyl nucleotid-binding protein, causing abnormal growth. Intramedullary tan-whitish gritty fibrous tissue, sometimes protruding the bone rarely breaking out through cortex. Curvilinear woven bone trabeculae, surrounded by moderately cellular fibroblastic proliferation. The shape of the trabeculae reminds Chinese letters, there is no prominant osteoblastic rim. Typical radiological picture in monoostotic form: ground glass appearance, well-defined margin. Polyostotic forms with early onset: fractures, pain, deformities, requiring orthopedic surgical intervention. Bisphosphonates ease the pain. Fibrosarcoma variants



41 Fibrous dysplasia
42 MISCELLANEOUS TUMORS EWING SARCOMA/PNET Member of of small round cell tumor group. The tumor is called Ewing-sarcoma in cases of bone derivation and/or forms without neuroepithelial differentation, in this meaning PNET is equal with extrasceletal Ewing. Certain agents (camp derivates, retinoic acid) can induce neurogenic differentiation. Sites: bone medulla (long bones: femur, tibia, humerus, fibula, pelvic bones, ribs, vertebrae, mandible, clavicula; diaphysis, central), 5-20 ys age group.
43 MISCELLANEOUS TUMORS EWING SARCOMA/PNET Clinical course: can mimick osteomyelitis (pain, fever, leukocytosis), from medulla spread into cortex and soft parts. Rarely manifests as a soft tissue tumor, but always with identifiable intraosseal component inside the bone, either with a simple x-ray. Radiology: spindle-shaped bone widening, periosteal reaction in the form of onion-skinning or sunbeam-like spikes in right-angle.

44 MISCELLANEOUS TUMORS EWING SARCOMA/PNET
45 MISCELLANEOUS TUMORS EWING SARCOMA/PNET Microscopy: solid proliferation of small cells in sheets, roundish nuclei, small nucleoli, wellformed vasculature, pseudorosettes, sometimes true rosettes (neurogenic differentiation). Abundant necrosis, sometimes dominating the picture. PAS-positive glycogen granulation in cytoplasm is quite typical (diff. dg.: ML, neuroblastoma, embryonal rhabdomyosarcoma). ELMI: primitive appearance, few dens core granules.


46 MISCELLANEOUS TUMORS EWING SARCOMA/PNET
47 MISCELLANEOUS TUMORS EWING SARCOMA/PNET IHC: consistent vimentin, occasionally LMW keratin, NSE, neurofilament positivity, MIC 2 cell membrane protein (CD99), coded on short arm of X and Y chromosome is consistently expressed in Ewing/PNET, but not pathognomonic. Genetics: common with PNET, t(11;22) (q24;q12): fusion of EWS and FL 1 genes (PCR and FISH methods for diagnosis and monitoring therapy).
48 MISCELLANEOUS TUMORS EWING SARCOMA/PNET Clinical course: metastases in lung, pleura, in other bones, (mainly skull), CNS, rarely in regional lymph node. In about 25 % mpl. bone and/or visceral lesions are detectable at presentation. Treatment, prognosis: dramatic improvement, in the past surgical and irradiation therapy resulted in <10 % 5 years survival, the current combined high-dose irradiation and chemotherapy and only limited surgical intervention has much better results: 85% local control and 75% 5 years survival can be achieved. The radiological change regress, if there are again lytic lesions, that suspicious for relaps. Soft tissue extension is a bad prognostic sign. The prognosis of Ewing is better than soft tissue PNET. Ploidy can have prognostic value (diploid is better).
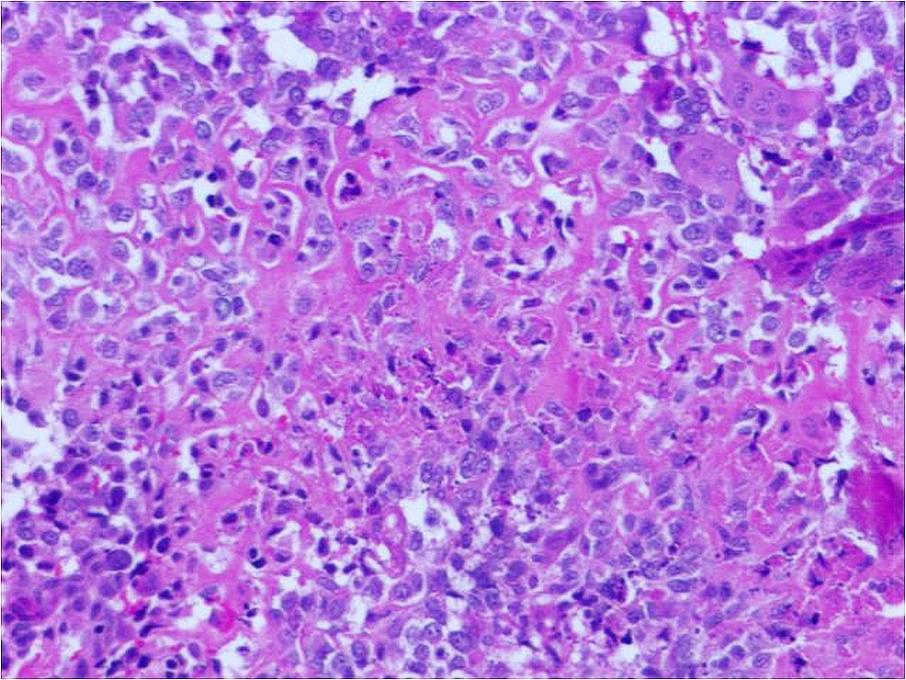
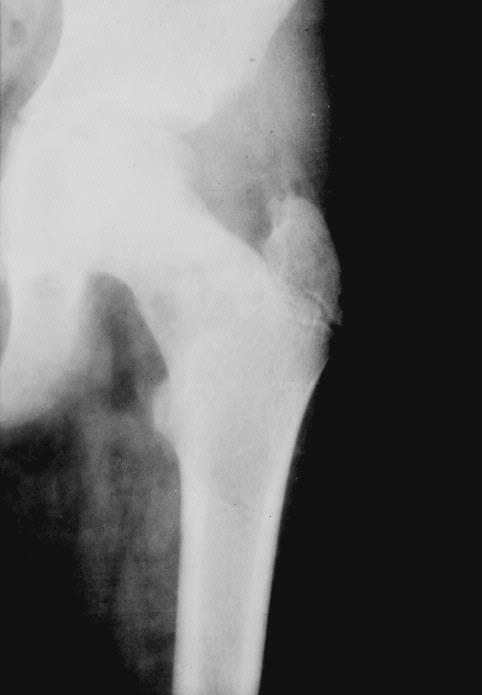
49 MISCELLANEOUS TUMORS, GIANT-CELL TUMOR Usually over 20 ys. Classical localisation: epiphysis of long bones, then spread into metaphysis and breaking through the cortex invading the joint, towards the intermuscular septa. Decreasing fequency: lower femur, upper tibia, lower radius. In the bones of hands, jaws, vertebrae (excluding sacrum) quite rare, in these locations other types of giant cell lesions appear. Radiology: lytic, expansive lesion in epiphysis without bone sclerosis or periosteal reaction. Clinical course: large tumors can be associated with pathologic fracture.

50 MISCELLANEOUS TUMORS, GIANT-CELL TUMOR
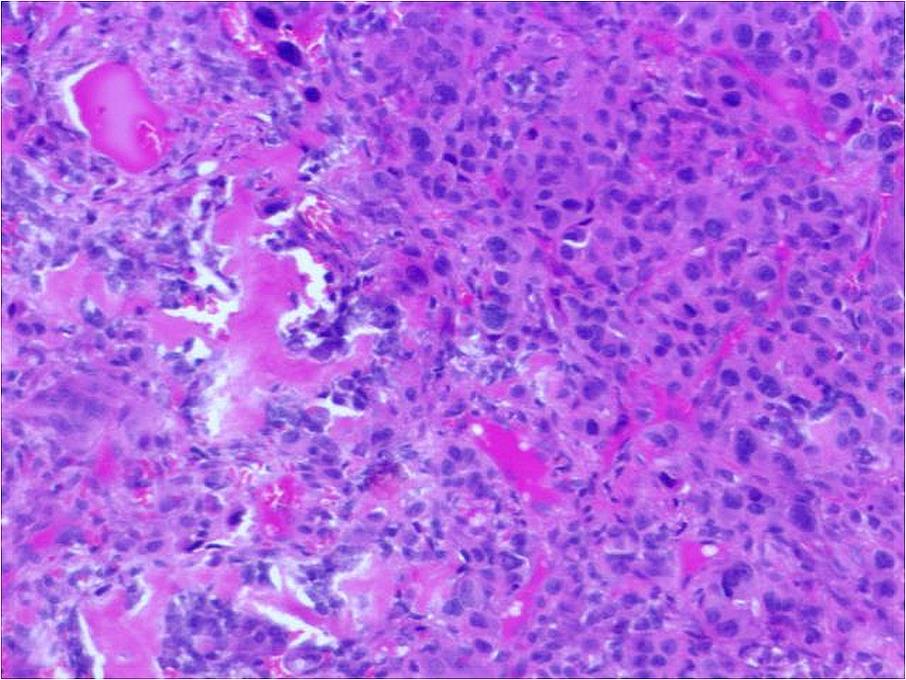
51 MISCELLANEOUS TUMORS, GIANT-CELL TUMOR Cut surface: solid, grey-brownish, intermixed with connective tissue septa, bleedings. Microscopically: two main components: osteoclast-type giant cells (30-40 nuclei, acid phosphatase positivity, IHC: lysozim, CD68-Kp-1 and other histiocyte marker positivity), which are non-neoplastic and the so-called stromal cells, representing the true neoplastic elements (only they proliferate, show atypia in more agressive cases, occasionally just focally). Their origin is not entirely known: mesenchymal, fibro- or osteoblast (in 1/3 of the cases osteoid deposition). They produce type I. and III. collagen, sometimes focal positivity with S-100 is detected, can contain alfa-1-at. Similarly to Paget disease intranuclear inclusions mimicking viral particles.

52 MISCELLANEOUS TUMORS, GIANT-CELL TUMOR
53 MISCELLANEOUS TUMORS, GIANT-CELL TUMOR Diff. Dg.: benign bone lesions containing giant cells (nonossifying fibroma, chondroblastoma, Langerhans-cell histiocytosis, Recklinghausen disease, aneurysmal bone cyst, osteoid osteoma and osteoblastoma). There is difference in the distribution of giant cells, in other benign lesions deposition focally in larger clusters, in the real giant-cell tumor the distribution is scattered, equally distributed. Arguments against the possibility of giant-cell tumor: childhood, metaphyseal or diaphyseal location, multiple appearance, spine, jaw, hand and foot involvement. Therapy: curette or block resection with bone replacement, vital to avoid soft tissue implantation. In non-resectable cases: radioth, but with the danger of malignant transformation.
54 MISCELLANEOUS TUMORS, GIANT-CELL TUMOR Clinical course: tumor with low malignant potential (10 % behaves clinically malignant: local relapse, metastasis). The choice of therapy affects the course: higher rates of relapse with simple curettage (34 % comparing with 7 % in wide resection). Break through cortex and extension into soft parts: worsens prognosis. A substantial portion of metastasises occur after surgical intervention. Microscopic grading: I-III, but has limited value, just in the cases of easily identifiable sarcomatous GIII variants. GII tumor can make metastasis to the lung with similar morphology (tumor surrounded by mature bone). Genetics: Non-random changes, mainly telomere fusions.
55 MISCELLANEOUS TUMORS /TUMOR- LIKE LESIONS- Aneurysmal bone cyst ys, vertebrae (frequently mpl.), flat bones, but can be in the diaphysis of long bones. It can occur in soft tissues, in the walls of large arteries. Radiology: excentric expansion, cortex erosion, destruction, in small zones periosteal new bone formation. Macroscopically spongy hemorrhagic mass, covered by thin reactive bone. Soft tissue involvement can be present. Microscopically: large, blood-filled spaces, lined not by endothel, but instead fibroblasts, myofibroblasts, histiocytes, they occupy the limiting septa as well, below the surface osteoclasts. In septa: vessels, osteoid and bone.


56 MISCELLANEOUS TUMORS /TUMOR- LIKE LESIONS- Aneurysmal bone cyst


57 MISCELLANEOUS TUMORS /TUMOR- LIKE LESIONS- Aneurysmal bone cyst
58 MISCELLANEOUS TUMORS /TUMOR- LIKE LESIONS- Aneurysmal bone cyst Diff. dg: solitary bone cyst, giant-cell tumor, haemangioma, teleangiectatic osteosarcoma, giant cell reparative granuloma (jaw). Origin:?, sometimes preceding trauma, subperiosteal hematoma, in other cases it derives from prexisting other bone lesions because of the change in hemodynamics, but because of the destruction the original lesion is not identifiable. Curette alone leads 25% relapse, complete removal with bone replacement provides much better results. There are episodical cases with transformation to osteosarcoma. There is a form of more cellular, solid lesions with fibrous reaction, many osteoclasts, this would be the solid variant (hands, feet, vertebrae, sacrum and raraely long bones).
59 MISCELLANEOUS TUMORS - METASTASES Most frequent bone tumors. Usually mpl appearance together with known primary and other organ MS lesions, but can be solitary mimicking primary bone tumor. 80%: breast, lung, prostate, thyroid, kidney, in general 50% of all tumors have bone metastases. Soft tissue sarcomas rarely give metastasis into bones, except the childhood embryonal rhabdomyosarcoma. 70% affects the axial skeleton (skull, ribs, spine, sacrum). Usually red marrow location. In long bones metaphyseal location.
60 MISCELLANEOUS TUMORS - METASTASES Most frequently osteolytic types, osteoplastic forms exist as well (prostate, carcinoid and other neuroendocrine tumor, rarely breast cancer) or mixed. In widespread osteoplastic prostate cancer metastasis in other areas osteomalacia can develop (increased Ca use, limited source). Typical metastases (place, radiological picture): thyroid (shoulder, skull, ribs, sternum), kidney (flat bones of pelvis, upper femur, scapula). Periosteal proliferation is rare (prostate). After pathologic fracture enormous bone formation can happen, easy to mix with osteosarcoma. Together with carcinoma and melanoma we frequently see osteoclasts, misdiagnosis: giant cell tumor. In sternal and vertebral MS a possible comlication is spread to soft tissues with a pulsating mass. Usual lab findings: hypercalcaemia, ALP elevation. Bone resorption can be a result of transformation of tumor infiltrating macrophages into osteoclasts.
61 MISCELLANEOUS TUMORS - METASTASES Biopsy is important to rule out a primary bone tumor. Symptoms: strong bone pain. The goal of therapy: reveal the pain, prevent the fracture; irradiation is effective, 80%: substantial decrease of pain. In case of fracture internal fixation then irradiation is recommended. In prostate and breast cancer hormontherapy can be effective decreasing the pain and increasing tolerance. Solitary metastases can be completely resected.

62 MISCELLANEOUS TUMORS - METASTASES
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell
 Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
Bone Tumors Clues and Cues
 William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
MARK D. MURPHEY MD, FACR. Physician-in-Chief, AIRP. Chief, Musculoskeletal Imaging
 ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
Bone Tumours - a synopsis. Dr Zena Slim SpR in Histopathology QAH 2009
 Bone Tumours - a synopsis Dr Zena Slim SpR in Histopathology QAH 2009 Aims General approach to diagnosis Common entities.and not so common ones. Mini quiz Challenge of bone tumour diagnosis Bone tumours
Bone Tumours - a synopsis Dr Zena Slim SpR in Histopathology QAH 2009 Aims General approach to diagnosis Common entities.and not so common ones. Mini quiz Challenge of bone tumour diagnosis Bone tumours
The Radiology Assistant : Bone tumor - well-defined osteolytic tumors and tumor-like lesions
 Bone tumor - well-defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor - well-defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
The Radiology Assistant : Bone tumor - ill defined osteolytic tumors and tumor-like lesions
 Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Grading of Bone Tumors
 Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Bone and Joint Part 2. Leslie G Dodd, MD
 Bone and Joint Part 2 Leslie G Dodd, MD Relative rates of cancer Sarcomas are relatively uncommon tumors New cancer cases 2007 All sites 1.4 million prostate 218,890 lung 213,380 breast 180,510 Soft tissue
Bone and Joint Part 2 Leslie G Dodd, MD Relative rates of cancer Sarcomas are relatively uncommon tumors New cancer cases 2007 All sites 1.4 million prostate 218,890 lung 213,380 breast 180,510 Soft tissue
Introduction to Musculoskeletal Tumors. James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon
 Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
APMA 2018 Radiology Track Bone Tumors When to say Gulp!
 APMA 2018 Radiology Track Bone Tumors When to say Gulp! DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine Conflict of
APMA 2018 Radiology Track Bone Tumors When to say Gulp! DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine Conflict of
Bread and Butter Bone Pathology
 Bread and Butter Bone Pathology NICOLE D. RIDDLE, MD RUFFOLO, HOOPER, AND ASSOC. / UNIVERSITY OF SOUTH FLORIDA Goals: Fundamentals of neoplastic bone pathology Bone Producing Cartilage Producing Miscellaneous
Bread and Butter Bone Pathology NICOLE D. RIDDLE, MD RUFFOLO, HOOPER, AND ASSOC. / UNIVERSITY OF SOUTH FLORIDA Goals: Fundamentals of neoplastic bone pathology Bone Producing Cartilage Producing Miscellaneous
Disclosures. Giant Cell Rich Tumors of Bone. Outline. The osteoclast. Giant cell rich tumors 5/21/11
 Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Bone/Osteoid Producing Lesions
 Chapter 2 Bone/Osteoid Producing Lesions Introduction There are many lesions that are associated with reactive new bone formation; this chapter predominantly covers those in which deposition of osteoid/bone
Chapter 2 Bone/Osteoid Producing Lesions Introduction There are many lesions that are associated with reactive new bone formation; this chapter predominantly covers those in which deposition of osteoid/bone
USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors
 USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Outline Common intramedullary tumors Enchondroma
USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Outline Common intramedullary tumors Enchondroma
Malignant bone tumors. Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7%
 Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
Typical skeletal location and differential diagnosis of bone tumors.
 Typical skeletal location and differential diagnosis of bone tumors. Poster No.: C-2418 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Barros, L. A. Ferreira, Y. Costa, P. J. V. Coelho, F. Caseiro
Typical skeletal location and differential diagnosis of bone tumors. Poster No.: C-2418 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Barros, L. A. Ferreira, Y. Costa, P. J. V. Coelho, F. Caseiro
Bone tumors. RMG: jan
 Bone tumors RMG: jan 217. @Kijohs KIZZA JOHN KIJOHS Diseases arising in bone Lipoma Fibrous cortical defects Non-ossifying fibroma Bone island Benign simple cysts Enchondroma Osteochondroma Osteoid osteoma
Bone tumors RMG: jan 217. @Kijohs KIZZA JOHN KIJOHS Diseases arising in bone Lipoma Fibrous cortical defects Non-ossifying fibroma Bone island Benign simple cysts Enchondroma Osteochondroma Osteoid osteoma
COPYRIGHT 2004 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
 84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
Functions of the Skeletal System. Chapter 6: Osseous Tissue and Bone Structure. Classification of Bones. Bone Shapes
 Chapter 6: Osseous Tissue and Bone Structure Functions of the Skeletal System 1. Support 2. Storage of minerals (calcium) 3. Storage of lipids (yellow marrow) 4. Blood cell production (red marrow) 5. Protection
Chapter 6: Osseous Tissue and Bone Structure Functions of the Skeletal System 1. Support 2. Storage of minerals (calcium) 3. Storage of lipids (yellow marrow) 4. Blood cell production (red marrow) 5. Protection
Mousa Al-Abadi. Abd. Kharabsheh. Rand Abu Anzeh
 7 Mousa Al-Abadi Abd. Kharabsheh Rand Abu Anzeh 1 Recap The histological appearance of Giant cell tumor of bone shows only multi-nucleated giant cells. The histological appearance of Aneurysmal bone cyst
7 Mousa Al-Abadi Abd. Kharabsheh Rand Abu Anzeh 1 Recap The histological appearance of Giant cell tumor of bone shows only multi-nucleated giant cells. The histological appearance of Aneurysmal bone cyst
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
FORMATION OF BONE. Intramembranous Ossification. Bone-Lec-10-Prof.Dr.Adnan Albideri
 FORMATION OF BONE All bones are of mesodermal origin. The process of bone formation is called ossification. We have seen that formation of most bones is preceded by the formation of a cartilaginous model,
FORMATION OF BONE All bones are of mesodermal origin. The process of bone formation is called ossification. We have seen that formation of most bones is preceded by the formation of a cartilaginous model,
Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples
 Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples Poster No.: C-1741 Congress: ECR 2015 Type: Educational Exhibit Authors: J. Silva, M. A. Ramírez
Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples Poster No.: C-1741 Congress: ECR 2015 Type: Educational Exhibit Authors: J. Silva, M. A. Ramírez
Cytology of Neoplasms that Occur on the Limbs Rick Alleman, DVM, PhD, DABVP, DACVP
 Cytology of Neoplasms that Occur on the Limbs Rick Alleman, DVM, PhD, DABVP, DACVP I. Introduction The purpose of this material is to provide information that may be useful in the identification of tumors
Cytology of Neoplasms that Occur on the Limbs Rick Alleman, DVM, PhD, DABVP, DACVP I. Introduction The purpose of this material is to provide information that may be useful in the identification of tumors
An Introduction to the Skeletal System Skeletal system includes Bones of the skeleton Cartilages, ligaments, and connective tissues
 An Introduction to the Skeletal System Skeletal system includes Bones of the skeleton Cartilages, ligaments, and connective tissues Functions of the Skeletal System Support Storage of minerals (calcium)
An Introduction to the Skeletal System Skeletal system includes Bones of the skeleton Cartilages, ligaments, and connective tissues Functions of the Skeletal System Support Storage of minerals (calcium)
The formation of blood cells is called. hemopoiesis. What does our bone store? Where do our bones store fat? yellow marrow.
 What are the 5/6 functions of the skeletal system? support, protection, movement, blood cell formation, storage, homeostasis The formation of blood cells is called hemopoiesis What does our bone store?
What are the 5/6 functions of the skeletal system? support, protection, movement, blood cell formation, storage, homeostasis The formation of blood cells is called hemopoiesis What does our bone store?
The Skeletal System. Chapter 7a. Skeletal System Introduction Functions of the skeleton Framework of bones The skeleton through life
 The Skeletal System Skeletal System Introduction Functions of the skeleton Framework of bones The skeleton through life Chapter 7a Support Protection Movement Storage areas Minerals Lipids Hemopoiesis
The Skeletal System Skeletal System Introduction Functions of the skeleton Framework of bones The skeleton through life Chapter 7a Support Protection Movement Storage areas Minerals Lipids Hemopoiesis
Multifocal fibrous Dysplasia with enchondroma-like areas: Fibrocartilaginous Dysplasia
 ISPUB.COM The Internet Journal of Pathology Volume 7 Number 2 Multifocal fibrous Dysplasia with enchondroma-like areas: Fibrocartilaginous Dysplasia V Monappa, R Kudva Citation V Monappa, R Kudva. Multifocal
ISPUB.COM The Internet Journal of Pathology Volume 7 Number 2 Multifocal fibrous Dysplasia with enchondroma-like areas: Fibrocartilaginous Dysplasia V Monappa, R Kudva Citation V Monappa, R Kudva. Multifocal
Musculoskeletal Sarcomas
 Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Fluid-fluid levels in bone tumors: A pictorial review
 Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
Human Skeletal System Glossary
 Acromegaly Apatite Acromegaly - is a condition which involves excessive growth of the jaw, hands, and feet. It results from overproduction of somatotropin in adults (after fusion of the ossification centres
Acromegaly Apatite Acromegaly - is a condition which involves excessive growth of the jaw, hands, and feet. It results from overproduction of somatotropin in adults (after fusion of the ossification centres
Giant cell tumour of the sternum-two cases
 Giant cell tumour of the sternum-two cases Nishaa.P 1, Raghuram.P 2, Navin patil 3, Jaipal B.R 4 Akkamahadevi patel 5 Assistant Professor ESIC medical college and PGIMSR 1 Professor and HOD, 2 Professor
Giant cell tumour of the sternum-two cases Nishaa.P 1, Raghuram.P 2, Navin patil 3, Jaipal B.R 4 Akkamahadevi patel 5 Assistant Professor ESIC medical college and PGIMSR 1 Professor and HOD, 2 Professor
The Skeletal System:Bone Tissue
 The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
BIOH111. o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system
 BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 TEXTBOOK AND REQUIRED/RECOMMENDED
BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 TEXTBOOK AND REQUIRED/RECOMMENDED
Bubbly Lesions of Bone
 Residents Section Pattern of the Month w79 08.18.09 Eisenberg Residents Section Pattern of the Month Residents inradiology Ronald L. Eisenberg 1 Eisenberg RL Keywords: bubbly lesions, fegnomashic, skeletal
Residents Section Pattern of the Month w79 08.18.09 Eisenberg Residents Section Pattern of the Month Residents inradiology Ronald L. Eisenberg 1 Eisenberg RL Keywords: bubbly lesions, fegnomashic, skeletal
Osseous Tissue and Bone Structure
 C h a p t e r 6 Osseous Tissue and Bone Structure PowerPoint Lecture Slides prepared by Jason LaPres Lone Star College - North Harris Copyright 2009 Pearson Education, Inc., publishing as Pearson Benjamin
C h a p t e r 6 Osseous Tissue and Bone Structure PowerPoint Lecture Slides prepared by Jason LaPres Lone Star College - North Harris Copyright 2009 Pearson Education, Inc., publishing as Pearson Benjamin
Chapter 5 The Skeletal System
 Chapter 5 The Skeletal System The Skeletal System Parts of the skeletal system Bones (skeleton) Joints Cartilages Ligaments (bone to bone)(tendon=bone to muscle) Divided into two divisions Axial skeleton:
Chapter 5 The Skeletal System The Skeletal System Parts of the skeletal system Bones (skeleton) Joints Cartilages Ligaments (bone to bone)(tendon=bone to muscle) Divided into two divisions Axial skeleton:
BONE TISSUE. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 BONE TISSUE Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology BONE FUNCTION Support Protection (protect internal organs) Movement (provide leverage system for skeletal muscles, tendons, ligaments
BONE TISSUE Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology BONE FUNCTION Support Protection (protect internal organs) Movement (provide leverage system for skeletal muscles, tendons, ligaments
GIANT CELL TUMOR OF BONE
 GIANT CELL TUMOR OF BONE Definition. First described by Jaffe et al. 1, giant cell tumor of bone is a locally aggressive primary neoplasm of bone that is composed of proliferation of bland looking oval
GIANT CELL TUMOR OF BONE Definition. First described by Jaffe et al. 1, giant cell tumor of bone is a locally aggressive primary neoplasm of bone that is composed of proliferation of bland looking oval
General osteology. General anatomy of the human skeleton. Development and classification of bones. The bone as a multifunctional organ.
 General osteology. General anatomy of the human skeleton. Development and classification of bones. The bone as a multifunctional organ. Composed by Natalia Leonidovna Svintsitskaya, Associate professor
General osteology. General anatomy of the human skeleton. Development and classification of bones. The bone as a multifunctional organ. Composed by Natalia Leonidovna Svintsitskaya, Associate professor
ANATOMY & PHYSIOLOGY - CLUTCH CH. 8 - BONE AND CARTILAGE.
 !! www.clutchprep.com CONCEPT: BONE CLASSIFICATIONS There are four classifications of bones based on their 1. Long bones are greater in length than in width - Found in the upper and lower limbs (ex: arm,
!! www.clutchprep.com CONCEPT: BONE CLASSIFICATIONS There are four classifications of bones based on their 1. Long bones are greater in length than in width - Found in the upper and lower limbs (ex: arm,
Skeletal Tissues Dr. Ali Ebneshahidi
 Skeletal Tissues Dr. Ali Ebneshahidi Functions of Bones 1. Support and protection: Bones give shape to body structure. Bones provide support to body weight. Certain bones protect vital internal organs
Skeletal Tissues Dr. Ali Ebneshahidi Functions of Bones 1. Support and protection: Bones give shape to body structure. Bones provide support to body weight. Certain bones protect vital internal organs
What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington
 What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington What s Do You Need To Know About Bone Pathology? Reactive/pseudosarcomatous
What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington What s Do You Need To Know About Bone Pathology? Reactive/pseudosarcomatous
SKELETAL TISSUES CHAPTER 7 INTRODUCTION TO THE SKELETAL SYSTEM TYPES OF BONES
 SKELETAL TISSUES CHAPTER 7 By John McGill Supplement Outlines: Beth Wyatt Original PowerPoint: Jack Bagwell INTRODUCTION TO THE SKELETAL SYSTEM STRUCTURE Organs: Bones Related Tissues: Cartilage and Ligaments
SKELETAL TISSUES CHAPTER 7 By John McGill Supplement Outlines: Beth Wyatt Original PowerPoint: Jack Bagwell INTRODUCTION TO THE SKELETAL SYSTEM STRUCTURE Organs: Bones Related Tissues: Cartilage and Ligaments
ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE
 ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE Richard D. Lackman, MD FACS Director, Orthopaedic Oncology Center Cancer Institute Introduction In the evaluation of a patient with a bone tumor, there are several
ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE Richard D. Lackman, MD FACS Director, Orthopaedic Oncology Center Cancer Institute Introduction In the evaluation of a patient with a bone tumor, there are several
Essential Dermatopathology. Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center
 Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
Malignant Bone Tumours. PathoBasic, Daniel Baumhoer
 Malignant Bone Tumours PathoBasic, 20.03.18 Daniel Baumhoer FNCLCC Grading The differentiation score is defined as the extent to which a tumor resembles adult mesenchymal tissue (score 1), the extent to
Malignant Bone Tumours PathoBasic, 20.03.18 Daniel Baumhoer FNCLCC Grading The differentiation score is defined as the extent to which a tumor resembles adult mesenchymal tissue (score 1), the extent to
Chapter 6 & 7 The Skeleton
 Chapter 6 & 7 The Skeleton Try this Make clockwise circles with your RIGHT foot, while doing this, draw the number 6 in the air with you RIGHT hand what happens to your foot???? Bony Background Adult body
Chapter 6 & 7 The Skeleton Try this Make clockwise circles with your RIGHT foot, while doing this, draw the number 6 in the air with you RIGHT hand what happens to your foot???? Bony Background Adult body
OSSEOUS TISSUE & BONE STRUCTURE PART I: OVERVIEW & COMPONENTS
 OSSEOUS TISSUE & BONE STRUCTURE PART I: OVERVIEW & COMPONENTS The Skeletal System Skeletal system includes: bones of the skeleton, cartilages, ligaments, and connective tissues What are the functions of
OSSEOUS TISSUE & BONE STRUCTURE PART I: OVERVIEW & COMPONENTS The Skeletal System Skeletal system includes: bones of the skeleton, cartilages, ligaments, and connective tissues What are the functions of
Due in Lab. Due next week in lab - Scientific America Article Select one article to read and complete article summary
 Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
SKELETAL SYSTEM. Introduction Notes (pt 1)
") SKELETAL SYSTEM Introduction Notes (pt 1) I. INTRODUCTION 1. Bones include active, living tissues: bone tissue, cartilage, dense connective tissue, blood, and nervous tissue. 2. Bones: support and protect
SKELETAL SYSTEM Introduction Notes (pt 1) I. INTRODUCTION 1. Bones include active, living tissues: bone tissue, cartilage, dense connective tissue, blood, and nervous tissue. 2. Bones: support and protect
Skeletal Tissues. Dr. Ali Ebneshahidi
 Skeletal Tissues Dr. Ali Ebneshahidi Functions of Bones 1. Support and protection : Bones give shape to body structure. Bones provide support to body weight. Certain bones protect vital internal organs
Skeletal Tissues Dr. Ali Ebneshahidi Functions of Bones 1. Support and protection : Bones give shape to body structure. Bones provide support to body weight. Certain bones protect vital internal organs
Skeletal System worksheet
 Skeletal System worksheet Name Section A: Intro to Skeletal System The skeletal system performs vital functions that enable us to move through our daily lives. Support - The skeleton provides support and
Skeletal System worksheet Name Section A: Intro to Skeletal System The skeletal system performs vital functions that enable us to move through our daily lives. Support - The skeleton provides support and
Imaging Findings Of Bone Tumors: A Pictorial Review
 Imaging Findings Of Bone Tumors: A Pictorial Review Poster No.: C-2511 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Limeme, N. Benzina, A. BelKhiria, H. Zaghouani, S. Majdoub, N. Mallat, H.
Imaging Findings Of Bone Tumors: A Pictorial Review Poster No.: C-2511 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Limeme, N. Benzina, A. BelKhiria, H. Zaghouani, S. Majdoub, N. Mallat, H.
Biology. Dr. Khalida Ibrahim
 Biology Dr. Khalida Ibrahim BONE TISSUE Bone tissue is a specialized form of connective tissue and is the main element of the skeletal tissues. It is composed of cells and an extracellular matrix in which
Biology Dr. Khalida Ibrahim BONE TISSUE Bone tissue is a specialized form of connective tissue and is the main element of the skeletal tissues. It is composed of cells and an extracellular matrix in which
Module 2:! Functional Musculoskeletal Anatomy A! Semester 1! !!! !!!! Hard Tissues, Distal Upper Limb & Neurovascular Supply of Upper Limb!
 Functional Musculoskeletal Anatomy A Module 2: Hard Tissues, Distal Upper Limb & Neurovascular Supply of Upper Limb Semester 1 1 18. Bone Tissue & Growth of Bones 18.1 Describe the structure of bone tissue
Functional Musculoskeletal Anatomy A Module 2: Hard Tissues, Distal Upper Limb & Neurovascular Supply of Upper Limb Semester 1 1 18. Bone Tissue & Growth of Bones 18.1 Describe the structure of bone tissue
Characteristics. Bones. Functions of the Skeleton
 Characteristics Bones The Introduction 206 bones hard, rigid bones cells (osteocyctes) are a mixture of a ground substance, collagen fibres, P, Ca highly resistant to compression and tension also somewhat
Characteristics Bones The Introduction 206 bones hard, rigid bones cells (osteocyctes) are a mixture of a ground substance, collagen fibres, P, Ca highly resistant to compression and tension also somewhat
Lecture 2: Skeletogenesis
 Jilin University School of Stomatology Skeletogenesis Lecture 2: Skeletogenesis Aug. 18, 2015 Yuji Mishina, Ph.D. mishina@umich.edu Student will describe Development of Bone - the general anatomy of bone
Jilin University School of Stomatology Skeletogenesis Lecture 2: Skeletogenesis Aug. 18, 2015 Yuji Mishina, Ph.D. mishina@umich.edu Student will describe Development of Bone - the general anatomy of bone
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Fig Articular cartilage. Epiphysis. Red bone marrow Epiphyseal line. Marrow cavity. Yellow bone marrow. Periosteum. Nutrient foramen Diaphysis
 Fig. 7.1 Articular cartilage Epiphysis Red bone marrow Epiphyseal line Marrow cavity Yellow bone marrow Nutrient foramen Diaphysis Site of endosteum Compact bone Spongy bone Epiphyseal line Epiphysis Articular
Fig. 7.1 Articular cartilage Epiphysis Red bone marrow Epiphyseal line Marrow cavity Yellow bone marrow Nutrient foramen Diaphysis Site of endosteum Compact bone Spongy bone Epiphyseal line Epiphysis Articular
Spectrum of clinical presentations
 Spectrum of clinical presentations Case History A 7-day-old male patient born full-term via uncomplicated vaginal delivery was seen for multiple erythematous red-brown purpuric lesions that were present
Spectrum of clinical presentations Case History A 7-day-old male patient born full-term via uncomplicated vaginal delivery was seen for multiple erythematous red-brown purpuric lesions that were present
Skeletal System. Chapter 6.1 Human Anatomy & Physiology
 Skeletal System Chapter 6.1 Human Anatomy & Physiology Overview of Skeletal System Bones Joints Skeletal System Cartilage Tendons (bone to muscle) Ligaments (bone to bone) Function of the Skeletal System
Skeletal System Chapter 6.1 Human Anatomy & Physiology Overview of Skeletal System Bones Joints Skeletal System Cartilage Tendons (bone to muscle) Ligaments (bone to bone) Function of the Skeletal System
What are the parts of the skeletal system? Chapter 6- Part I Bones and Skeletal Tissues. Growth of Cartilage. Bones come in many shapes
 Chapter 6- Part I Bones and Skeletal Tissues Components of the skeletal system Classification of Bone (bone shapes) Functions of bone Bone structure Microscopic structure of bone and bone cells What are
Chapter 6- Part I Bones and Skeletal Tissues Components of the skeletal system Classification of Bone (bone shapes) Functions of bone Bone structure Microscopic structure of bone and bone cells What are
ISSN: DISTRIBUTION OF BONE AND CARTILAGINOUS TUMORS IN PEDIATRIC AGE GROUP IN WESTERN UTTAR-PRADESH: AN EVALUATIVE STUDY
 : 289-295 ISSN: 2277 4998 DISTRIBUTION OF BONE AND CARTILAGINOUS TUMORS IN PEDIATRIC AGE GROUP IN WESTERN UTTAR-PRADESH: AN EVALUATIVE STUDY QADRI S, HASAN M, AKHTAR K * AND SHERWANI RK The Departments
: 289-295 ISSN: 2277 4998 DISTRIBUTION OF BONE AND CARTILAGINOUS TUMORS IN PEDIATRIC AGE GROUP IN WESTERN UTTAR-PRADESH: AN EVALUATIVE STUDY QADRI S, HASAN M, AKHTAR K * AND SHERWANI RK The Departments
What is bone? Specialized form of connective tissue: mineralized collagen matrix, therefore very rigid and strong while still retaining some degree of
 Bone What is bone? Specialized form of connective tissue: mineralized collagen matrix, therefore very rigid and strong while still retaining some degree of flexibility Other types of connective tissue:
Bone What is bone? Specialized form of connective tissue: mineralized collagen matrix, therefore very rigid and strong while still retaining some degree of flexibility Other types of connective tissue:
The Skeletal System PART A
 5 The Skeletal System PART A PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB The Skeletal System
5 The Skeletal System PART A PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB The Skeletal System
GIANT CELL-RICH OSTEOSARCOMA: A CASE REPORT
 Nagoya J. Med. Sci. 59. 151-157, 1996 CASE REPORTS GIANT CELL-RICH OSTEOSARCOMA: A CASE REPORT KEIJI SATO!, SHIGEKI YAMAMURA!, HISASHI IWATA!, HIDESHI SUGIURA 2, NOBUO NAKASHIMA 3 and TETSURO NAGASAKA
Nagoya J. Med. Sci. 59. 151-157, 1996 CASE REPORTS GIANT CELL-RICH OSTEOSARCOMA: A CASE REPORT KEIJI SATO!, SHIGEKI YAMAMURA!, HISASHI IWATA!, HIDESHI SUGIURA 2, NOBUO NAKASHIMA 3 and TETSURO NAGASAKA
Bone (2) Chapter 8. The bone is surrounded by the periosteum, the periosteum consists of two layers: a fibrous outer layer and an innercellular layer.
 Chapter 8. The bone is surrounded by the periosteum, the periosteum consists of two layers: a fibrous outer layer and an innercellular layer.") Bone (2) Chapter 8 The bone is surrounded by the periosteum, the periosteum consists of two layers: a fibrous outer layer and an innercellular layer. The innercellular layer contains osteoprogenitor cells,
Bone (2) Chapter 8 The bone is surrounded by the periosteum, the periosteum consists of two layers: a fibrous outer layer and an innercellular layer. The innercellular layer contains osteoprogenitor cells,
Chapter 6: Osseous Tissue and Bone Structure
 Chapter 6: Osseous Tissue and Bone Structure I. An Introduction to the Skeletal System, p. 180 Objective: Describe the functions of the skeletal system The skeletal system includes: - bones of the skeleton
Chapter 6: Osseous Tissue and Bone Structure I. An Introduction to the Skeletal System, p. 180 Objective: Describe the functions of the skeletal system The skeletal system includes: - bones of the skeleton
Skeletal metastases are the most common variety of bone tumors and should always be considered in the differential diagnosis, particularly in older
 Dr Brajesh Nandan Skeletal metastases are the most common variety of bone tumors and should always be considered in the differential diagnosis, particularly in older patients. Cancers of the breast, prostate,
Dr Brajesh Nandan Skeletal metastases are the most common variety of bone tumors and should always be considered in the differential diagnosis, particularly in older patients. Cancers of the breast, prostate,
The Skeletal System Vertebral column Sacrum. Osseous tissue For the body and soft organs. Magnesium, sodium, fluoride Levers for muscle action
 10/1/2016 Cranium Facial s Skull Clavicle Scapula Sternum Rib Humerus Vertebra Radius Ulna Carpals Thoracic cage (ribs and sternum) The Skeletal System Vertebral column Sacrum Phalanges Metacarpals Femur
10/1/2016 Cranium Facial s Skull Clavicle Scapula Sternum Rib Humerus Vertebra Radius Ulna Carpals Thoracic cage (ribs and sternum) The Skeletal System Vertebral column Sacrum Phalanges Metacarpals Femur
Figure ) The area that causes the lengthwise growth of a long bone is indicated by letter. Diff: 2 Page Ref:
 The area that causes the lengthwise growth of a long bone is indicated by letter. Diff: 2 Page Ref:") Essentials of Anatomy and Physiology, 9e (Marieb) Chapter 5 The Skeletal System Short Answer Figure 5.1 Using Figure 5.1, identify the following: 1) Spongy bone is indicated by letter. Diff: 1 Page Ref:
Essentials of Anatomy and Physiology, 9e (Marieb) Chapter 5 The Skeletal System Short Answer Figure 5.1 Using Figure 5.1, identify the following: 1) Spongy bone is indicated by letter. Diff: 1 Page Ref:
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
The Skeletal System. Mosby items and derived items 2010, 2006, 2002, 1997, 1992 by Mosby, Inc., an affiliate of Elsevier Inc.
 The Skeletal System Functions of Skeletal System Provides internal framework that supports the body Protects internal organs Helps fight disease by producing white blood cells 2 Functions of Skeletal System
The Skeletal System Functions of Skeletal System Provides internal framework that supports the body Protects internal organs Helps fight disease by producing white blood cells 2 Functions of Skeletal System
LAC + USC.
 Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
36 1 The Skeletal System Slide 1 of 40
 1 of 40 The Skeleton All organisms need structural support. Unicellular organisms have a cytoskeleton. Multicellular animals have either an exoskeleton (arthropods) or an endoskeleton (vertebrates). 2
1 of 40 The Skeleton All organisms need structural support. Unicellular organisms have a cytoskeleton. Multicellular animals have either an exoskeleton (arthropods) or an endoskeleton (vertebrates). 2
Bones. The division of bones anatomically is : long, short, irregular, flat and sesamoid.
 Bones Osteocytes : Are responsible for maintenance of bones Present in lacunae, and send processes. Unable to divide. The division of bones anatomically is : long, short, irregular, flat and sesamoid.
Bones Osteocytes : Are responsible for maintenance of bones Present in lacunae, and send processes. Unable to divide. The division of bones anatomically is : long, short, irregular, flat and sesamoid.
FRACTURE CALLUS ASSOCIATED WITH BENIGN AND MALIGNANT BONE LESIONS AND MIMICKING OSTEOSARCOMA
 THE AMERICAN JOURNAL OF CLINICAL PATHOLOGY Vol. 52, No. 1 Copyright 1969 by The Williams & Wilkins Co. Printed in U.S.A. FRACTURE CALLUS ASSOCIATED WITH BENIGN AND MALIGNANT BONE LESIONS AND MIMICKING
THE AMERICAN JOURNAL OF CLINICAL PATHOLOGY Vol. 52, No. 1 Copyright 1969 by The Williams & Wilkins Co. Printed in U.S.A. FRACTURE CALLUS ASSOCIATED WITH BENIGN AND MALIGNANT BONE LESIONS AND MIMICKING
04/27/2017. The Spectrum of Cartilaginous Tumors
 The Spectrum of Cartilaginous Tumors L I S A E R C O L A N O, M D M U S C U L O S K E L E T A L O N C O L O G Y D E P A R T M E N T O F O R T H O P A E D I C S A L L E G H E N Y H E A L T H N E T W O R
The Spectrum of Cartilaginous Tumors L I S A E R C O L A N O, M D M U S C U L O S K E L E T A L O N C O L O G Y D E P A R T M E N T O F O R T H O P A E D I C S A L L E G H E N Y H E A L T H N E T W O R
Osteology. Dr. Carmen E. Rexach Anatomy 35 Mt San Antonio College
 Osteology Dr. Carmen E. Rexach Anatomy 35 Mt San Antonio College Functions of the Skeletal System: Support Movement Protection Hemopoiesis Electrolyte balance (Ca ++ /PO -3 4 ) Acid-base balance Storage
Osteology Dr. Carmen E. Rexach Anatomy 35 Mt San Antonio College Functions of the Skeletal System: Support Movement Protection Hemopoiesis Electrolyte balance (Ca ++ /PO -3 4 ) Acid-base balance Storage
Malignant Bone Tumors - Part I: a brief revision of diagnostic aspects with conventional radiology
 Malignant Bone Tumors - Part I: a brief revision of diagnostic aspects with conventional radiology Poster No.: C-2473 Congress: ECR 2013 Type: Educational Exhibit Authors: I. Candelaria, L. B. Barbosa,
Malignant Bone Tumors - Part I: a brief revision of diagnostic aspects with conventional radiology Poster No.: C-2473 Congress: ECR 2013 Type: Educational Exhibit Authors: I. Candelaria, L. B. Barbosa,
Recognizing Cartilaginous Tumors: Spectrum of Imaging Characteristics with Radiologic-Pathologic correlation.
 Recognizing Cartilaginous Tumors: Spectrum of Imaging Characteristics with Radiologic-Pathologic correlation. Poster No.: C-1451 Congress: ECR 2012 Type: Educational Exhibit Authors: E. Barcina García,
Recognizing Cartilaginous Tumors: Spectrum of Imaging Characteristics with Radiologic-Pathologic correlation. Poster No.: C-1451 Congress: ECR 2012 Type: Educational Exhibit Authors: E. Barcina García,
CHAPTER 6 LECTURE OUTLINE
 CHAPTER 6 LECTURE OUTLINE I. INTRODUCTION A. Bone is made up of several different tissues working together: bone, cartilage, dense connective tissue, epithelium, various blood forming tissues, adipose
CHAPTER 6 LECTURE OUTLINE I. INTRODUCTION A. Bone is made up of several different tissues working together: bone, cartilage, dense connective tissue, epithelium, various blood forming tissues, adipose
SMALL ROUND BLUE CELL LESION OF BONE
 DISCLOSURE SMALL ROUND BLUE CELL LESION OF BONE Dr. Alistair Jordan University of South Alabama No financial support or endorsement OBJECTIVES Describe the more common small round cell lesions of bone
DISCLOSURE SMALL ROUND BLUE CELL LESION OF BONE Dr. Alistair Jordan University of South Alabama No financial support or endorsement OBJECTIVES Describe the more common small round cell lesions of bone
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
SKELETAL SYSTEM I NOTE: LAB ASSIGNMENTS for this topic will run over 3 Weeks. A SEPARATE WORKSHEET WILL BE PROVIDED.
 BIO 211; Anatomy and Physiology I REFERENCE: CHAPTER 07 1 Dr. Lawrence Altman Naugatuck Valley Community College LECTURE TOPICS OUTLINE SKELETAL SYSTEM I NOTE: LAB ASSIGNMENTS for this topic will run over
BIO 211; Anatomy and Physiology I REFERENCE: CHAPTER 07 1 Dr. Lawrence Altman Naugatuck Valley Community College LECTURE TOPICS OUTLINE SKELETAL SYSTEM I NOTE: LAB ASSIGNMENTS for this topic will run over
Metabolic & Endocrine disorders of bone:
 Metabolic & Endocrine disorders of bone: Osteoporosis: Bone apposition < bone resorption Risk factors: Postmenopausal women Hyperthyroidism Hyperparathyroidism Cushing s syndrome bone quantity: thin cortex
Metabolic & Endocrine disorders of bone: Osteoporosis: Bone apposition < bone resorption Risk factors: Postmenopausal women Hyperthyroidism Hyperparathyroidism Cushing s syndrome bone quantity: thin cortex
The Skeletal System PART A. PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College
 PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Skeletal System 5 PART A The Skeletal System Parts of the skeletal system Bones (skeleton) Joints
PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Skeletal System 5 PART A The Skeletal System Parts of the skeletal system Bones (skeleton) Joints
Compact bone; Many parallel Haversian canals contain: small blood vessels. very small nerve. Interconnected by Volkmann s canals.
 Special characteristics of COMPACT BONE (dense bone) Thick; well vascularized Osteocytes and lamellae Concentric rings around blood vessels Most bones: outer compact bone inner spongy bone Marrow cavity
Special characteristics of COMPACT BONE (dense bone) Thick; well vascularized Osteocytes and lamellae Concentric rings around blood vessels Most bones: outer compact bone inner spongy bone Marrow cavity
Common Primary Tumors of Bone
 Special Report Common Primary Tumors of Bone Primary bone tumors are a relatively rare occurrence, however, they can have serious deleterious consequences. Many possess the ability to degenerate into malignant
Special Report Common Primary Tumors of Bone Primary bone tumors are a relatively rare occurrence, however, they can have serious deleterious consequences. Many possess the ability to degenerate into malignant
PATHOLOGY OF THE MUSCULOSKELETAL SYSTEM
 PATHOLOGY OF THE MUSCULOSKELETAL SYSTEM BONES & JOINTS CONGENITAL DISEASES OF BONE Osteogenesis Imperfecta (OI) (Brittle bone diseases) is a group of hereditary disorders caused by gene mutations that
PATHOLOGY OF THE MUSCULOSKELETAL SYSTEM BONES & JOINTS CONGENITAL DISEASES OF BONE Osteogenesis Imperfecta (OI) (Brittle bone diseases) is a group of hereditary disorders caused by gene mutations that
Dr. Heba Kalbouneh. Saba Alfayoumi. Heba Kalbouneh
 11 Dr. Heba Kalbouneh Saba Alfayoumi Heba Kalbouneh 2- Bone Bone tissue is also classified into primary bone and secondary bone. In the beginning, the first bone that is deposited by the osteoblasts is
11 Dr. Heba Kalbouneh Saba Alfayoumi Heba Kalbouneh 2- Bone Bone tissue is also classified into primary bone and secondary bone. In the beginning, the first bone that is deposited by the osteoblasts is
Bizarre parosteal osteochondromatous proliferation
 * * Bizarre Parosteal Osteochondromatous Proliferation A Case Report with Literature Review Chi-Fu Kao Yang-Chih Lin Yu-Hung Wu Be-Fong Chen* We report the case of a 12-year-old female with a slowly erythematous
* * Bizarre Parosteal Osteochondromatous Proliferation A Case Report with Literature Review Chi-Fu Kao Yang-Chih Lin Yu-Hung Wu Be-Fong Chen* We report the case of a 12-year-old female with a slowly erythematous
The Radiology Assistant : Bone tumor A-G
 Bone tumor A-G Bone tumors and tumor-like lesions in alphabethic order Henk Jan van de Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor A-G Bone tumors and tumor-like lesions in alphabethic order Henk Jan van de Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Skeletal System worksheet
 Skeletal System worksheet Name Section A: Intro to Skeletal System The skeletal system performs vital functions that enable us to move through our daily lives. Support - The skeleton provides support and
Skeletal System worksheet Name Section A: Intro to Skeletal System The skeletal system performs vital functions that enable us to move through our daily lives. Support - The skeleton provides support and
The Skeletal System ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY PART A ELAINE N. MARIEB EIGHTH EDITION
 5 The Skeletal System PART A PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB The Skeletal System
5 The Skeletal System PART A PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB The Skeletal System
Parts of the skeletal system. Bones (skeleton) Joints Cartilages Ligaments (bone to bone)(tendon=bone to muscle)
 Joints Cartilages Ligaments (bone to bone)(tendon=bone to muscle)") The Skeletal System The Skeletal System Parts of the skeletal system Bones (skeleton) Joints Cartilages Ligaments (bone to bone)(tendon=bone to muscle) Divided into two divisions Axial skeleton Appendicular
The Skeletal System The Skeletal System Parts of the skeletal system Bones (skeleton) Joints Cartilages Ligaments (bone to bone)(tendon=bone to muscle) Divided into two divisions Axial skeleton Appendicular
Fluid fluid levels in bone tumors and tumoral lesions - Pictorial essay
 Review Fluid fluid levels in bone tumors and tumoral lesions - Pictorial essay Subbarao Kakarla 1,* 1 KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India Abstract
Review Fluid fluid levels in bone tumors and tumoral lesions - Pictorial essay Subbarao Kakarla 1,* 1 KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India Abstract
Name Date Score. Skeletal System. Indicate if the following statements are true or false. Correct false statements
 Name Date Score Skeletal System True/False Indicate if the following statements are true or false. Correct false statements 1. Bones surround vital organs to protect them. 2. Bones store most of the calcium
Name Date Score Skeletal System True/False Indicate if the following statements are true or false. Correct false statements 1. Bones surround vital organs to protect them. 2. Bones store most of the calcium
the urinary system pathology Dr. Fairoz A Eltorgman
 the urinary system pathology Dr. Fairoz A Eltorgman Tumors of the renal pelvis & kidney Benign tumors of the renal pelvis: Hemangioma Leiomyoma Malignant tumors: Transitional cell carcinoma Squamous cell
the urinary system pathology Dr. Fairoz A Eltorgman Tumors of the renal pelvis & kidney Benign tumors of the renal pelvis: Hemangioma Leiomyoma Malignant tumors: Transitional cell carcinoma Squamous cell