67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
|
|
|
- Jesse Baldwin Wright
- 5 years ago
- Views:
Transcription
1
2 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent swallowing discomfort (solids), gradually worsening. Chronic cough, shortness of breath, throat irritation, thickened voice since many years, restricted physical activities, 2-3 L O2 required during activity but poor compliance. SoB increased in last year. No hemoptysis, choking spells, or ear pains. Admitted as in-patient due to increased breathing difficulty in last month.
3 KPS 60, Obese, SpO2 5 L continuous oxygen. No obvious stridor. Neck: 2x2 cm, mobile, hard, non-tender lymph node in left level II. OC/ Ophx: Poor dental hygiene, adequate tongue protrusion, asymmetric fullness over left posterior pharyngeal wall. Pt. not cooperative to digital examination or IDL. Flexible endoscopy: Ulcero-infiltrative mass arising from left supraglottis, involving left AE fold, left edge of epiglottis, thickening of complete epiglottis, bilateral vallecula, lateral pharyngeal wall, just reaching base tongue. Pooling of saliva making it difficult to visualize left true vocal cord (TVC). Right TVC appears mobile. Concern for moderate airway compromise Bilateral wheezing on auscultation, trachea central in position.


4 Labs: Elevated random glucose. PFT: findings are consistent w/ COPD FVC 1.2 L (41% pred), FEV1 (0.85 L (42% pred), DLCO SB 21% pred (19% corrected). Severe reduction in both FEV1 and FVC with a very severe reduction in terminal flows, significant improvement following inhaled bronchodilator. Diffusion capacity is severely reduced even when corrected for alveolar volume. Patient at increased risk for peri-operative pulmonary complications. ECHO: LVEF 75% Swallowing study: Aspiration with thin and nectar thick liquids. None with honey thick liquids, pudding or solids. Pathology: Examination under anesthesia not feasible due to risks. Hence, only FNA left neck performed: confirms metastatic squamous cell carcinoma.
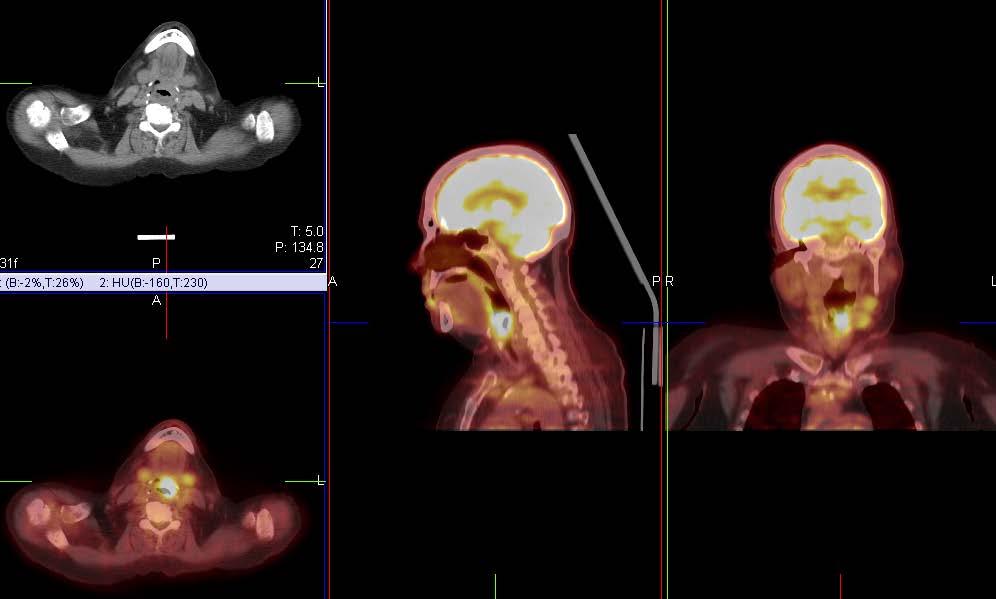
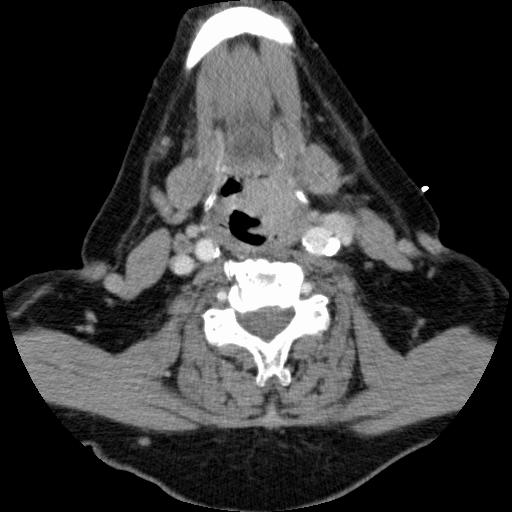
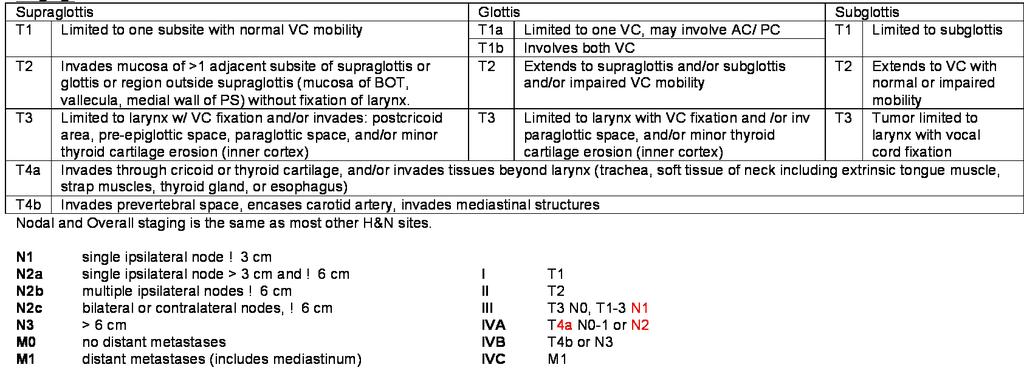
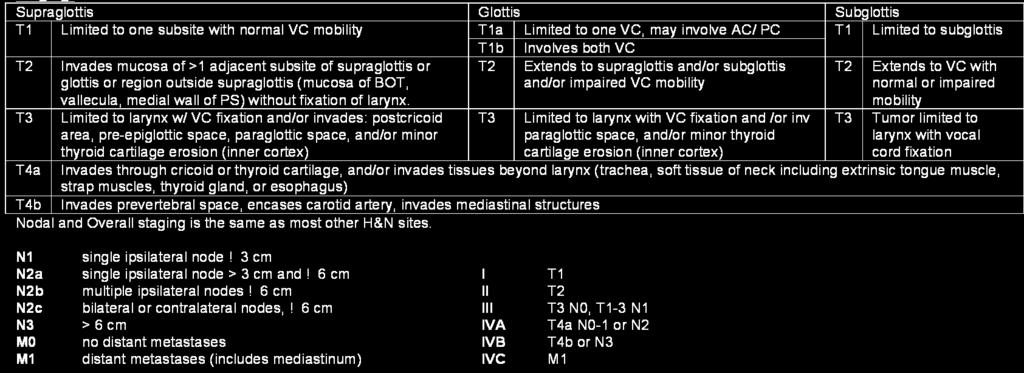
5 CT NECK (W & W/O CONTRAST): Mass centered within the epiglottis, extends to the level of the left false vocal cord, left aryepiglottic fold, contralateral suprahyoid epiglottis, left vallecula, glossoepiglottic fold and base of tongue. Potential involvement of the intrinsic muscles of the tongue. Abnormal, enhancing left level IIA LN, 2.1 cm in maximal diameter, with irregular margins, suggestive of extracapsular spread. Additional abnormal, 1.2 cm LN superiorly within left level IIA and 0.9 cm in left level III. There is a normal 0.9 cm node in the right level 2 A region. CT CHEST (W & W/O CONTRAST): No concern for metastatic disease. Main pulmonary artery enlargement and right ventricular hypertrophy, highly suggestive of pulmonary hypertension. PET-CT: Demonstrates abnormal hypermetabolism in the supraglottic mass with SUVmax of 12.4 and in ipsilateral level II and III LN with SUV max of 8.9. No other metastatic disease. Final staging: Squamous cell carcinoma, Supraglottic larynx, ct4an2bm0, Stg IV A


6
7 Surgical oncology, Radiation oncology, Medical oncology, Pulmonary medicine, Internal medicine consults done. Potential treatment options: Total laryngectomy with possible partial pharyngectomy with bilateral neck dissection and pectoralis major myocutaneous flap followed by vocal rehabilitation. Adjuvant chemo-radiotherapy. Definitive chemoradiation/ Altered fractionation. Patient considered a very high anesthesia risk based on PFTs, imaging concern for severe pulmonary hypertension, recent history of congestive heart failure, requirement of 5-6 L continuous oxygen.
8 Decision made to proceed with definitive chemo-radiotherapy. Issues with chemotherapy: Doubtful tolerance/ compliance for concurrent Cisplatin based chemotherapy. Other options: Concurrent Cetuximab vs. Altered fractionation. Decision to proceed with Cetuximab (400 mg/m2 loading, then 250 mg/m2) Concern for complete obstruction of already compromised airway. Hence, planned tracheotomy done. RT planning one week after tracheotomy to allow edema to subside. Swallowing function: G-tube insertion done because of concern of aspiration as revealed on swallowing studies and due to potential for acute worsening of function with planned chemoradiotherapy. Pre-RT dental prophylaxis arranged.
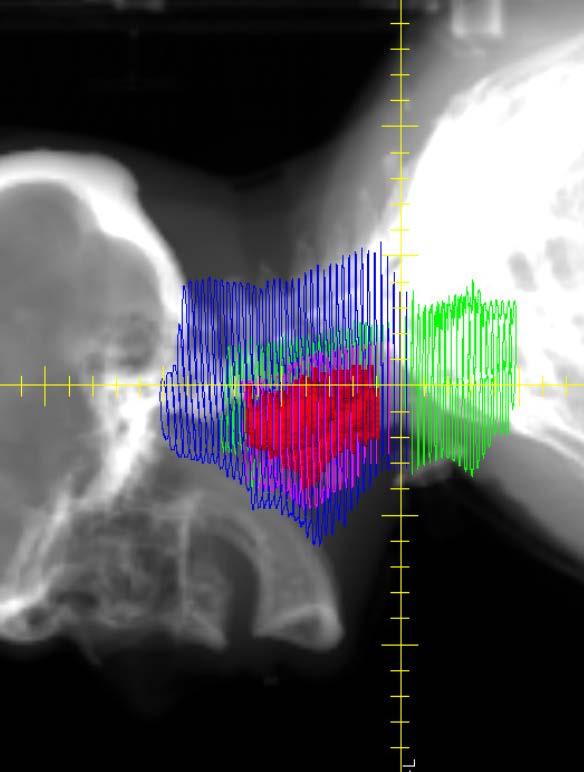
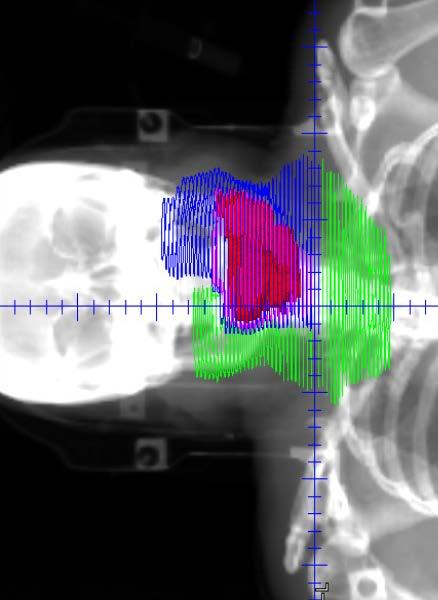
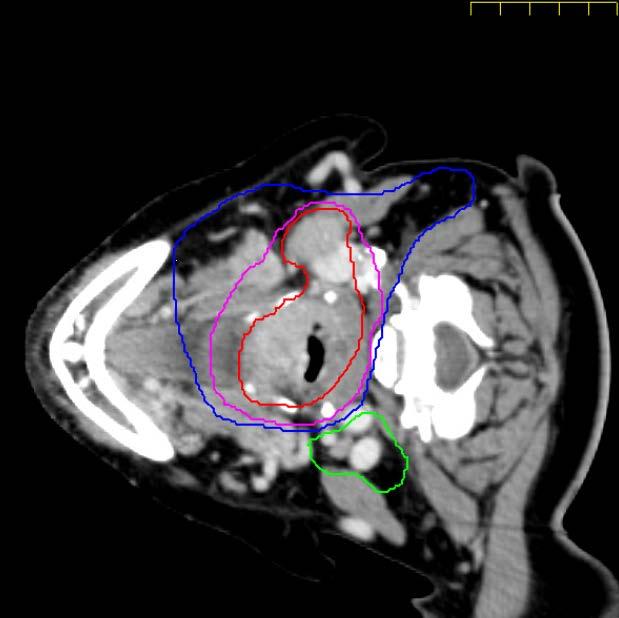
9 SIMULATION: Planning CT with i.v. contrast, Head and Neck protocol. Head position: Neutral. Shoulders pulled inferiorly as much as possible. Thermoplastic mold Region to be included in CT: From above base skull to upper mediastinum CONTOURS: (PRIMARY) TARGET VOLUME- GTV Primary: Outlined on contrast-enhanced planning CT co-registered with diagnostic CT and PET scan. CTV2 (High-risk): Includes entire larynx, extra-laryngeal and parapharyngeal tissues, bilateral hypopharynx, vallecula and base tongue with a margin of at least 0.5 cm around GTV. Stoma contoured as a region and included to the point of entry into trachea. CTV3 (Low-risk): Remaining contralateral base tongue, posterior third tongue. CONTOURS: (NODAL) TARGET VOLUME- GTV-Nodal CTV2-Nodal: Ipsilateral retropharyngeal, level II-IV and VI CTV3-Nodal: Ipsilateral level V, Contralateral low level IIA/ RP (lower edge of C1), III, IV PTV MARGINS: 5 mm per institutional protocol. Trimmed off of skin to prevent desquamation. OAR: Brain stem, spinal cord, bilateral parotids, oral cavity avoidance, mandible.

10 CTV1: 70 Gy CTV Intermediate: 63 Gy CTV2: 60 Gy CTV3: 54 Gy
11 PRESCRIPTION: PTV1 = PTV primary + PTV nodal = 70 Gy/ Gy/ fraction [Univ. Wisconsin dose scheme, Std. RTOG prescription is 70 Gy/ 35 fr] PTV Intermediate primary = 63 Gy/ Gy/fraction Uncertainty of tumor delineation in this case, hence slightly higher dose chosen. PTV2 = PTV2 primary + PTV2 nodal = 60 Gy/ Gy/fraction PTV3 = 54 Gy/ Gy/fraction PTV COVERAGE GOALS: V70 = 95% of PTV1. At 1 cc PTV1 volume on the DVH curve, the dose should not be > 110% of the prescribed dose. At a volume of 0.03 cc within the PTV1 volume on the DVH curve, the dose should not be < 95% of the prescribed dose. For any volume of tissue outside the PTVs that has a size of 1 cc, the dose should not be > 74 Gy.
12 OAR CONSTRAINTS: Spinal Cord PRV: Dmax not more than 48 Gy to 0.03cc and 50 Gy to any point. Given highest priority. Brain stem PRV: not more than 52 Gy to 0.03 cc Oral cavity avoidance: Mean dose 30 Gy, Avoid hot spot > 60 Gy Parotid: No constraint for ipsilateral parotid. Contralateral parotid mean at least 26 Gy, Aim: ALARA Contralateral submandibular gland: Mean 26 Gy (39 Gy per RTOG 1016) Mandible: Dmax 70 Gy Prioritization for IMRT Planning: Spinal Cord > Brainstem > PTV1 > PTV2 > PTV3 > contralateral parotid > Mandible > Oral Cavity > contralateral submandibular gland. Ongoing protocol for IMRT planning details: RTOG 1016: y=1016

13 DVH Right to Left PTV1: 70 Gy PTV Intermediate: 63 Gy PTV2: 60 Gy PTV3: 54 Gy Stoma Ipsilat. Parotid Mandible Contralat. Parotid Cord Brain stem
14 G-tube and Tracheotomy-tube management. Mucositis: Topical numbing mouthwashes, oral hygiene, opioid based analgesics, baking soda and salt solution Changes in saliva: Oral hygiene Dermatitis: Non-alcoholic, water-based creams (avoid immediately before RT) Maintain diet/ hydration. Lung physiotherapy, be alert for aspiration. Cetuximab skin rash: Topical OTC hydrocortisone, 2.5% Hydrocortisone, Oral Doxycycline mg BID. Monitor labs.
 Vs.")
15 This case highlights the importance of multi-disciplinary health care in such complicated presentations. Interesting discussion between primary surgical approach (risk of pulmonary complications in peri-operative period) Vs. RT approach (delayed pulmonary complications from swallowing dysfunction) in setting of poor pulmonary reserve at baseline. Decision regarding arranging tracheotomy prior to start of RT in view of already compromised airway and measures to include it in low-risk CTV. In view of significant weight loss, obvious mis-match noted in daily MVCT and planning CT (figure below). Decision to re-plan taken at 18 th fr. and started on new plan for last 11 fractions.
16
: Concomitant CT-RT vs. Induction CT-RT vs. RT alone Updated MACH-NC Meta-analysis (Pignon et al, Radiother. Oncol. 2009): The hazard ratio for death was 0.")
17 VA Laryngeal Cancer study group Organ preservation study, NEJM 1991: Reduced local recurrences with Surgery (2% Vs 12%) but no difference in 2 yr-os 68%. 64% laryngeal preservation in RT arm. RTOG 9111 (Forastiere et al, NEJM 2003): Concomitant CT-RT vs. Induction CT-RT vs. RT alone Updated MACH-NC Meta-analysis (Pignon et al, Radiother. Oncol. 2009): The hazard ratio for death was 0.81 (95%CI: ; p < ) in favor of concomitant chemotherapy with an absolute benefit of 6.5% at 5 years. Cetuximab (Bonner et al, NEJM 2006 ) Cetuximab concomitantly with RT may be recommended in Stage III-IV H&N cancer patients with a contraindication to cisplatin (poor renal function, baseline hearing deficits, low blood counts) and no contraindication to cetuximab.
18 The Department of Veteran Affairs Laryngeal Cancer Study Group. N Engl J Med Jun 13;324(24): RTOG 9111, Forastiere AA et al, Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med Nov 27;349(22): Pignon et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol Jul;92(1):4-14. Epub 2009 May Bernier J et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004;350: Cooper JS et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 2004;350: Bernier J et al. Defining risk levels in locally advanced head and neck cancers: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (#9501). Head Neck 2005;27: Bonner JA et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med Feb 9;354(6):
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical
 The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Protocol of Radiotherapy for Small Cell Lung Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Practice teaching course on head and neck cancer management
 28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org
28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org
Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali
 Dr Raj K Shrimali") Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali Let us keep this simple and stick to some basic rules Patient positioning Must be reproducible Must be
Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali Let us keep this simple and stick to some basic rules Patient positioning Must be reproducible Must be
Larynx Hypopharynx. Therapy algorithms. Why larynx preservation at all? State of the art Jean Louis Lefebvre,Lille Jan Klozar,Prague
 Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Outline. Contour quality control. Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT)
") Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
From GTV to CTV: A Critical Step Towards Cure. Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017
 From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Diagnosis and what happens after referral
 Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Head and Neck Treatment Planning: A Comparative Review of Static Field IMRT RapidArc TomoTherapy HD. Barbara Agrimson, BS RT(T)(R), CMD
(R), CMD") Head and Neck Treatment Planning: A Comparative Review of Static Field IMRT RapidArc TomoTherapy HD Barbara Agrimson, BS RT(T)(R), CMD Disclaimer This presentation will mention equipment by trade name.
Head and Neck Treatment Planning: A Comparative Review of Static Field IMRT RapidArc TomoTherapy HD Barbara Agrimson, BS RT(T)(R), CMD Disclaimer This presentation will mention equipment by trade name.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
REVISITING ICRU VOLUME DEFINITIONS. Eduardo Rosenblatt Vienna, Austria
 REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations
 Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
3/12/2018. Head & Neck Cancer Review INTRODUCTION
 Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
Head & Neck Cancer: When to Irradiate
 Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Principles of Management of Head & Neck Cancer. Jinka Sathya Associate professor of Oncology
 Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Defining Target Volumes and Organs at Risk: a common language
 Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head & Neck Contouring
 Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Protocol of Radiotherapy for Breast Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
Vincent Grégoire, Radiation Oncologist, Brussels, Belgium Cai Grau, Radiation Oncologist, Aarhus, Denmark. Tunis March 2017
 Guidelines for the delineation of the primary tumour Clinical Target Volumes (CTV) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity SCC (version 5.1) Vincent Grégoire, Radiation Oncologist,
Guidelines for the delineation of the primary tumour Clinical Target Volumes (CTV) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity SCC (version 5.1) Vincent Grégoire, Radiation Oncologist,
What is head and neck cancer? How is head and neck cancer diagnosed and evaluated? How is head and neck cancer treated?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
Allan Price NHS Lothian, Edinburgh, UK
 Allan Price NHS Lothian, Edinburgh, UK Radiotherapy Dose Volume Timing Technique PCI Surgery Systemic agents 1 Study Dose Time Induction CT Ann Arbor 65.1-75.6 Gy Duke 73.6-80 Gy RTOG 77.4 Gy 74 Gy 6.5-7.5
Allan Price NHS Lothian, Edinburgh, UK Radiotherapy Dose Volume Timing Technique PCI Surgery Systemic agents 1 Study Dose Time Induction CT Ann Arbor 65.1-75.6 Gy Duke 73.6-80 Gy RTOG 77.4 Gy 74 Gy 6.5-7.5
SAMO MASTERCLASS HEAD & NECK CANCER. Nicolas Mach, PD Geneva University Hospital
 SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate
 Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Case Presentation. Faysal Ghazzay Ahmed
 Faysal Ghazzay Ahmed Case Presentation He is 49 years old male living in Al-Qaem Town (Al-Anbar Gov.), Muslim, and was previously serving in the army, but now he is idle. He was admitted to Al-Jumhoory
Faysal Ghazzay Ahmed Case Presentation He is 49 years old male living in Al-Qaem Town (Al-Anbar Gov.), Muslim, and was previously serving in the army, but now he is idle. He was admitted to Al-Jumhoory
Sanguineti s (2)Comment: When it was initially published in 2003 with a median follow-up of 3.8 years (4), the RTOG study led to a change in
Comment: When it was initially published in 2003 with a median follow-up of 3.8 years (4), the RTOG study led to a change in") Commento di due Soci AIRO pubblicati su due prestigiose riviste internazionali al Trial della forastiere et al. Long term results of RTOG:91-11 (a cura di Dr. Russi e Dr. Testolin )! Forastiere)et)al.)Long/Term)Results)of)RTOG)91/11:)A)Comparison)of)
Commento di due Soci AIRO pubblicati su due prestigiose riviste internazionali al Trial della forastiere et al. Long term results of RTOG:91-11 (a cura di Dr. Russi e Dr. Testolin )! Forastiere)et)al.)Long/Term)Results)of)RTOG)91/11:)A)Comparison)of)
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Nasopharynx Cancer. 1 Feb Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar)
 Dr Peter Luk (Pathology Registrar)") Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
CANCERS of OROPHARYNX and HYPOPHARYNX. STAGING and TREATMENT
 1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Intensity-modulated radiation therapy for nasopharyngeal carcinoma: a review
 J Radiat Oncol (2012) 1:129 146 DOI 10.1007/s13566-012-0020-4 REVIEW Intensity-modulated radiation therapy for nasopharyngeal carcinoma: a review Tony J. C. Wang & Nadeem Riaz & Simon K. Cheng & Jiade
J Radiat Oncol (2012) 1:129 146 DOI 10.1007/s13566-012-0020-4 REVIEW Intensity-modulated radiation therapy for nasopharyngeal carcinoma: a review Tony J. C. Wang & Nadeem Riaz & Simon K. Cheng & Jiade
The management of advanced supraglottic and
 ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
Whoon Jong Kil, MD 1,2 Christina Kulasekere, CMD 1 Craig Hatch, DMD 1 Jacob Bugno, PhD 1 Ronald Derrwaldt, DO 1. Abstract INTRODUCTION CASE REPORT
 Received: 17 January 2017 Revised: 23 February 2017 Accepted: 14 March 2017 DOI: 10.1002/hed.24809 CASE REPORT Tongue-out versus tongue-in position during intensity-modulated radiotherapy for base of tongue
Received: 17 January 2017 Revised: 23 February 2017 Accepted: 14 March 2017 DOI: 10.1002/hed.24809 CASE REPORT Tongue-out versus tongue-in position during intensity-modulated radiotherapy for base of tongue
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Accepted 28 April 2005 Published online 13 September 2005 in Wiley InterScience ( DOI: /hed.
 DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Q&A. Fabulous Prizes. Collecting Cancer Data: Pharynx 12/6/12. NAACCR Webinar Series Collecting Cancer Data Pharynx
 Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck. Mei Tang, MD
 Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana
 University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
Head and Neck Cancer. What is head and neck cancer?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice?
 Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
State of the art for radiotherapy of SCCHN
 State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
TOMOTERAPIA in Italia: Esperienze a confronto
 TOMOTERAPIA in Italia: Esperienze a confronto BARD 20 novembre 2010 L esperienza di Reggio Emilia Testa collo Alessandro Muraglia Reasons for the use of tomotherapy: - Complex tumor geometry and proximity
TOMOTERAPIA in Italia: Esperienze a confronto BARD 20 novembre 2010 L esperienza di Reggio Emilia Testa collo Alessandro Muraglia Reasons for the use of tomotherapy: - Complex tumor geometry and proximity
ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018
 ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018 Dr. Victor Ho-Fun Lee MBBS, MD, FRCR, FHKCR, FHKAM (Radiology) Clinical Associate Professor Department of Clinical Oncology
ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018 Dr. Victor Ho-Fun Lee MBBS, MD, FRCR, FHKCR, FHKAM (Radiology) Clinical Associate Professor Department of Clinical Oncology
Head and Neck Cancer Service
 Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer. Dr P Vijay Anand Reddy Director Apollo Cancer Hospital
 Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER
 ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
Management of unknown primary with neck node metastasis: Current evidence
 Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
Quality Variation and Clinical Impact in Head and Neck IMRT
 Quality Variation and Clinical Impact in Head and Neck IMRT 6 th IMRT Symposium, New York Sep. 20, 2010 K.S. Clifford Chao, MD Chairman, Combined Radiation Oncology, New York Presbyterian Hospital Chairman,
Quality Variation and Clinical Impact in Head and Neck IMRT 6 th IMRT Symposium, New York Sep. 20, 2010 K.S. Clifford Chao, MD Chairman, Combined Radiation Oncology, New York Presbyterian Hospital Chairman,
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Larynx-sparing techniques using intensitymodulated radiation therapy for oropharyngeal cancer.
 Thomas Jefferson University Jefferson Digital Commons Department of Radiation Oncology Faculty Papers Department of Radiation Oncology 1-1-2012 Larynx-sparing techniques using intensitymodulated radiation
Thomas Jefferson University Jefferson Digital Commons Department of Radiation Oncology Faculty Papers Department of Radiation Oncology 1-1-2012 Larynx-sparing techniques using intensitymodulated radiation
ASTRO econtouring for Lymphoma. Stephanie Terezakis, MD
 ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX
 Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK CARCINOMA UNKNOWN PRIMARY
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK CARCINOMA UNKNOWN PRIMARY Head & Neck Site Group Carcinoma Unknown Primary 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK CARCINOMA UNKNOWN PRIMARY Head & Neck Site Group Carcinoma Unknown Primary 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Chapter 2. Level II lymph nodes and radiation-induced xerostomia
 Chapter 2 Level II lymph nodes and radiation-induced xerostomia This chapter has been published as: E. Astreinidou, H. Dehnad, C.H. Terhaard, and C.P Raaijmakers. 2004. Level II lymph nodes and radiation-induced
Chapter 2 Level II lymph nodes and radiation-induced xerostomia This chapter has been published as: E. Astreinidou, H. Dehnad, C.H. Terhaard, and C.P Raaijmakers. 2004. Level II lymph nodes and radiation-induced
Treatment of Multiple Lung Tumors
 VUmc SABR Symposium 2017 Treatment of Multiple Lung Tumors Indications and Dosimetric Considerations Dr. David Palma, MD, MSc, PhD Radiation Oncologist, London Health Sciences Centre Clinician-Scientist,
VUmc SABR Symposium 2017 Treatment of Multiple Lung Tumors Indications and Dosimetric Considerations Dr. David Palma, MD, MSc, PhD Radiation Oncologist, London Health Sciences Centre Clinician-Scientist,
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
ARROCase: Borderline Resectable Pancreatic Cancer
 ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient
 Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida