CANCERS of OROPHARYNX and HYPOPHARYNX. STAGING and TREATMENT
|
|
|
- Meryl Long
- 5 years ago
- Views:
Transcription
1 1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT
2 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies
3 3 1. Staging - AJCC 7th Ed., 2010 OROPHARYNX Primary tumor (T) TX: Primary tumor cannot be assessed T0: No evidence of primary tumor Tis: Carcinoma in situ
4 4 T1: Tumor 2 cm or less in greatest dimension T2: Tumor more than 2 cm but not more than 4 cm in greatest dimension T3: Tumor more than 4 cm in greatest dimension or extension to lingual surface of epiglottis
5 5 T4a: Moderately advanced local disease. Tumor invades the larynx, extrinsic muscle of tongue, medial pterygoid, hard palate, or mandible T4b: Very advanced local disease. Tumor invades lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, or skull base or encases carotid artery
6 6 Primary tumor (T) HYPOPHARYNX TX: Primary tumor cannot be assessed T0: No evidence of primary tumor Tis: Carcinoma in situ
7 7 T1: Tumor limited to one subsite of hypopharynx and/or 2 cm or less in greatest dimension T2: Tumor invades more than one subsite of hypopharynx or an adjacent site, or measures more than 2 cm, but not more than 4 cm in greatest dimension without fixation of hemilarynx
8 8 T3: Tumor more than 4 cm in greatest dimension or with fixation of hemilarynx or extension to esophagus T4a: Moderately advanced local disease. Tumor invades thyroid/cricoid cartilage, hyoid bone, thyroid gland, or central compartment soft tissue T4b: Very advanced local disease. Tumor invades prevertebral fascia, encases carotid artery, or involves mediastinal structures
9 9 Regional lymph nodes (N) NX: Regional lymph nodes cannot be assessed N0; No regional lymph node metastasis N1: Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension
10 10 N2a: N2b: N2c: Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension Metastasis in multiple ipsilateral lymph nodes, not more than 6 cm in greatest dimension Metastasis in bilateral or contralateral lymph nodes, not more than 6 cm in greatest dimension
11 11 N3: Metastasis in a lymph node, more than 6 cm in greatest dimension Distant metastasis (M) M0: No distant metastasis M1: Distant metastasis
12 12 STAGE GROUPING 0: Tis N0 M0 I: T1 N0 M0 II: T2 N0 M0 III: T3 N0 M0 ; T1-T3 N1 M0 IVA: T4a N0 M0 ; T4a N1 M0 ; T1-T3 N2 M0 T4a N2 M0 IVB: IVC: T4b Any N M0 ; Any T N3 M0 Any T Any N M1
13 13 2. General Principles of Treatment Goals of Treatment Stage I - IVA Curative Stage IVB - IVC Palliative Treatment Modalities Surgery and Radiotherapy are the definitive therapies in the treatment of HNSCC Chemotherapy by itself is not a definitive treatment
14 14 Surgery Used as a single modality in early stage disease (I & II) Preferred over Radiotherapy as a single modality in i) Sites where surgery is not morbid cosmetically and functionally ii) Lesions involving or close to bone to prevent radionecrosis iii) Young patients possibility of a subsequent second primary iv) Sub-mucous fibrosis
15 15 Advantages of Surgery compared to Radiotherapy i) Exact histopathological diagnosis and anatomical extent determined ii)treatment time is shorter iii) Limited amount of tissue exposed to treatment iv) No radiation related complication Used as a part of combined modality treatment along with Radiotherapy in advanced stage disease (III & IV) Rationale for combined modality treatment Surgery is effective in removing large bulky lesion Radiotherapy takes care of microscopic disease
16 16 Radiotherapy Used as a single modality in early stage disease(i & II) Preferred over surgery as a single modality where i) Severe impairment of function/cosmesis with surgery ii) Surgery is technically difficult with high morbidity and poor results iii) Patient refuses surgery or there is high risk for surgery
17 17 Used as part of combined modality along with surgery (with or without chemotherapy) in advanced stage disease (III & IV) Either pre-operative or post-operative irradiation based therapy may be used there are advocates of each
18 18 Pr-operative Radiation Therapy considered in following - i) fixed neck nodes ii) if initiation of post-operative radiotherapy will be delayed by > 8 weeks due to reconstruction iii) open biopsy of a positive node Advantages of Pre operative Radiotherapy i) Inoperable lesions may be converted to operable lesions ii) Extent of surgery may be decreased iii) Blood supply at the time of Radiotherapy is intact iv) Distant metastasis may decrease
19 19 Disadvantages of Pre-operative Radiotherapy i) Increased morbidity ii) Decreased wound healing iii) Surgery is difficult as anatomy is not identified Post-operative Radiation Therapy is indicated in Primary-i) Large primary-t3 or T4 ii) Close (<5mm) or positive margins of excision iii) Deep infiltrative tumor iv) Lymphovascular and Perineural invasion Lymph Nodes-i) Bulky nodal disease N2 /N3 ii) Extra nodal extension iii) Multiple level involvement
20 20 Advantages of Post-operative Radiotherapy i) Extent of the disease is known ii) Higher doses may be delivered iii) Wound healing is better Disadvantages of Post-operative Radiotherapy i) Distant metastasis is likely to be greater ii) Decreased vascularity at the time of Radiotherapy due to surgical tampering
21 Role of Brachytherapy Interstitial implants selectively used in i) Accesssible lesions ii) Small (preferably <3cm) tumors iii) Lesions away from bone iv) N0 nodal status v) Superficial lesions 21
22 22 Chemotherapy Established role of Chemotherapy as part of the standard combined modality management of HNSCC in i) therapy of unresectable disease ii) for organ preservation iii) for patients with poor risk pathologic features after surgery Integrated with Surgery/Radiotherapy as Induction/ Neo adjuvant therapy Concurrent with Radiation Adjuvant/ Maintenance therapy
23 23 Current evidence supports concurrent therapy along with radiotherapy as the most efficacious modality Agents used- platin plus 5-flourouracil other polychemotherapy without platin monotherapy with platin other monotherapy Platinum based chemotherapy associated with largest benefit platin plus 5-flourouracil compared to platin alone offers no advantage A newly available option is Cetuximab and concurrent irradiation associated with superior results compared to Radiotherapy alone
24 24 Rehabilitation i) Abstinence from tobacco/alcohol ii) Oral hygeine iii) Shoulder physiotherapy in all cases of neck dissection iv) Bite guide prosthesis following mandibulectomy v) Jaw stretching exercises to prevent postoperative trismus vi) Speech and Swallowing Rehabilitation
25 25 Follow up Every 2 to 3 months for first two years 6 monthly for next three years Annually thereafter On every follow up - thorough head and neck examination for locoregional control, second primary tumor and late sequelae of treatment Investigation only if indicated by symptoms and positive clinical findings Serum T3,T4,TSH annually

26 26 3. Site Specific Treatment Guidelines OROPHARYNX
27 27 Surgery For early cancers of Tonsillar pillars trans-oral wide local excision including a tonsillectomy can be done; T3-4 Tonsillar lesions require radical tonsillectomy often with partial mandibulectomy & ipsilateral neck dissection. Base of tongue lesions require partial or total glossectomy and myocutaneous flap reconstruction. For locally advanced oropharyngeal cancers, primary organ preservation approach with radiation or chemo-rt is preferred.
28 28 Types of Neck Dissection Radical neck dissection (RND) removes levels I V, Sternocleidomastoid muscle, omohyoid muscle, internal and external jugular veins, CN XI, and the submandibular gland. Modified RND leaves one or more of sternocleidomastoid muscle, internal jugular vein, or CN XI. Supraomohyoid neck dissection only removes levels I III. Lateral neck dissection only removes levels II IV.
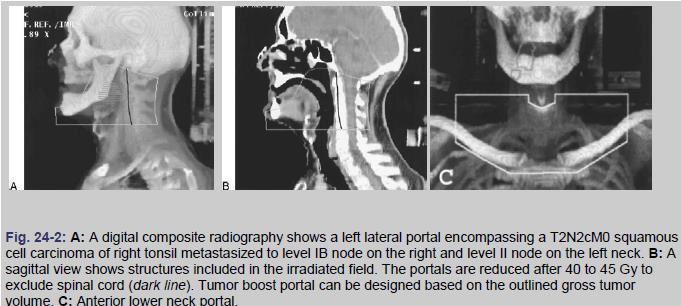
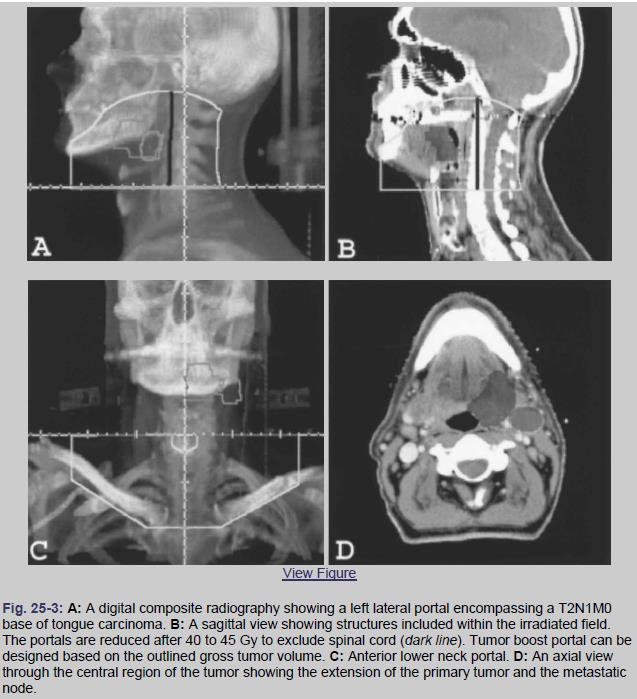
29 29 Radiotherapy Simulate patient supine with head hyperextended. Shoulders may be pulled down with straps. Immobilize with a thermoplastic head and shoulder mask. Conventional volumes cover the skull base and mastoid to the supraclavicular nodes with a three-field technique (opposed laterals matched to AP lower neck field). Beam-split above larynx at thyroid notch, if possible, to allow laryngeal sparing.
30 30 The anterior margin is set up by clinical examination with at least a 2-cm margin beyond any clinical evidence of disease. This margin should project 2 to 3 cm forward of the anterior cortex of the ramus of the mandible, depending on tumor extent. Inferiorly,the portal extends to the thyroid notch, except in patients with downward tumor extension with pharyngeal wall involvement; in these cases, the margin must be placed below that level. Posteriorly, the posterior cervical lymph nodes should be covered.
31 31 After a tumor dose of approximately 40 to 45 Gy, the posterior margin of the lateral portal is brought anteriorly to the midportion of the vertebral bodies to spare the spinal cord. Electrons (12 to 20 MeV) can be used to boost the dose to the primary tumor or large cervical lymph nodes. If necessary, the posterior cervical nodes are irradiated with 9-12 MeV electrons to avoid higher doses to the spinal cord when higher-energy electrons are used.
32 32 After 40 to 45 Gy with low-energy megavoltage beams, the remaining dose may be delivered with high-energy x-rays to concentrate the dose centrally and reduce the dose to the parotids, mandible, and temporomandibular joints. After 60 Gy, the fields are reduced to encompass only the primary tumor and may be weighted to the side involved by tumor. The boost dose after 60 Gy may be delivered by a submental electron beam or low energy photon beam field.
33 33 The lower neck is treated with a standard anteroposterior portal. If no palpable lymph nodes are present, a 1.5- to 2.0-cmwide midline block can be used to shield the larynx and spinal cord. If lymph nodes are involved in this area, only a small block is used to shield the larynx and a portion of spinal cord (to avoid overlap with lateral portals). One technique for treating small tumors of the tonsillar fossa, anterior tonsillar pillar, and retromolar trigone uses ipsilateral wedged-angle anterior and posterior fields that irradiate a triangular volume, with the base on the neck and the apex in the uvula.
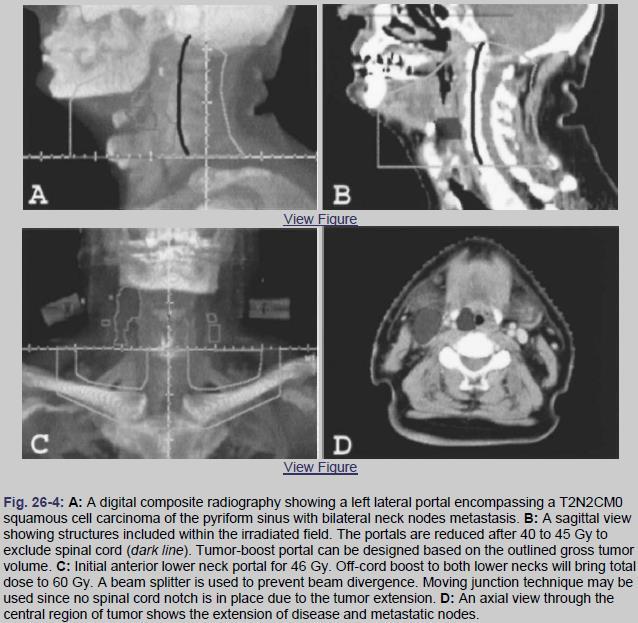
34 34
35 35
36 36 Dose Prescription Select T1-2N0 patients: Definitive conventional fx RT to 70 Gy at 2 Gy/fx. Select T1N1 and T2N0-1 patients: Definitive altered-fx RT. i) Six fx/week during weeks 2 6: 70 Gy at 2 Gy/fx to primary and gross adenopathy. ii) Concomitant boost: 72 Gy in 6 weeks (1.8 Gy/fx large field;1.5 Gy boost as second daily fx during last 12 treatment days). iii) Hyperfractionation: 81.6 Gy in 7 weeks at 1.2 Gy b.i.d.
37 37 Stage III IV patients: Concurrent chemo-rt. Total dose typically 70 Gy in daily 2 Gy fx with cisplatin 100 mg/m2 q3 weeks 3c. Elective neck: Uninvolved nodal stations: Gy at 1.6 2Gy/fx. Post-op RT: Gy at 2 Gy/fx to high-risk areas and the postoperative bed. Concurrent single agent cisplatin 100 mg/m2 q3 weeks recommended.
38 38 Dose Limitations Spinal cord <45 Gy Brainstem <54 Gy Parotid glands Mean dose <26 Gy and/or attempt to keep 50% volume of each parotid <20 Gy (ifpossible) Mandible <70 Gy Larynx mean dose <43.5 Gy
39 39 Treatment Recommendations for Neck Nodes Clinically negative neck: If risk of occult metastasis exists Surgery for primary with elective neck dissection (a) If N0, follow (b) If N1 with no extracapsular extension (ECE), follow (c) If >pn1 and/or ECE, postoperative RT or chemo-rt Alternatively, RT or chemo-rt for primary with elective neck RT; surgery for persistent disease
40 40 Clinically positive neck: i) N1 Surgery for primary with selective or modified radical neck dissection (a) If pn0, follow (b) If pn1 with no ECE, follow (c) If >pn1 and/or ECE, postoperative RT or chemo-rt Alternatively, RT or chemo-rt for primary and involved Neck with elective neck RT; surgery and/or neck dissection for persistent disease
41 41 ii) >N1 Surgery for primary with modified radical or radical neck dissection (a) If pn1 with no ECE, follow (b) If >pn1 and/or ECE, postoperative RT or chemo-rt Alternatively, RT or chemo-rt for primary with comprehensive RT for neck ; surgery and/or neck dissection for persistent disease and/or node >3 cm
42 42 HYPOPHARYNX The best treatment for hypopharyngeal carcinoma aims for the highest locoregional control rate with the least functional damage. Functions that need to be preserved include respiration, deglutition, and phonation. This should be done with the least risk to the host and, if possible, without the use of permanent prosthetic devices.
43 43
44 44
45 45 Surgery Total laryngectomy Indicated for advanced lesions with transglottic or extensive subglottic extension, most pyriform sinus lesions, and/or cartilage invasion Removes hyoid, thyroid, and cricoid cartilages, epiglottis, strap muscles. Patient left with a permanent tracheostoma and pharynx reconstruction (by suturing to the base of tongue)
46 Partial laryngopharyngectomy Used for small medial and anterior pyriform sinus lesions Removes false cords, epiglottis, aryepiglotticfold, and pyriform sinus, but TVCs are preserved Contraindicated if transglottic extension, cartilage invasion, vocal fold paralysis, pyriform apex invasion (b/c below level of TVCs) postcricoid invasion, exolaryngeal spread, or poor pulmonary reserve Total laryngopharyngectomy For more advanced hypopharyngeal lesions TL plus removal of varying amount of pharyngeal wall 46
47 47 Radiation Simulate the patient supine with the head hyperextended. Shoulders may be pulled down with straps. Immobilize with a thermoplastic head and shoulder mask. Treat primary and levels II V and retropharyngeal nodes in all cases. With traditional field design, the superior border is the skull base and mastoid. The inferior border is 1 cm below the inferior extent of disease (or 1 cm below cricoid) on the laterals and matched to the AP low-neck field.
48 48 Post-operative Radiation With traditional fields, use 3-field technique with stoma in low-neck AP field. Lateral fields cover neopharynx, adenopathy, and cm margin on preoperative extent of disease. With conventional three-field techniques, the spinal cord is shielded on the lateral fields at the matchline if no gross disease is present. If gross disease is present at the matchline, angling the lateral fields to match the divergence of the AP field may help. A small midline block on the AP field may be necessary.
49 49
50 50 Dose Prescription T1 2N0 : >2 Gy/fx preferred. If 2 Gy/fx is used, total dose >66 Gy. T3 4 and LN+ patients: Concurrent chemo-rt Total dose typically 70 Gy in daily 2 Gy/fx with cisplatin 100 mg/m2 q3 weeks 3c. With definitive RT, use altered fractionation: i)six fx/week during weeks 2 6: 70 Gy at 2 Gy/fx to primary and gross adenopathy. ii)cb: 72 Gy in 6 weeks (1.8 Gy/fx large field; 1.5 Gy boost as second daily fx during last 12 treatment days). iii)hyperfractionation: 81.6 Gy in 7 weeks at 1.2 Gy b.i.d.
51 51 4. Abstracts from Selected Studies 1. Pre-op vs. post-op RT RTOG (Kramer et al. 1987; Tupchong et al. 1991): 354 patients with advanced H&N cancer randomized to 2/50 Gy pre-op vs. 2/50/60 Gy post-op. Post-op RT improved LRC (48 65%), and OS for oropharynx lesions (26 38%). Complications not different.
52 52 2. Altered Fractionation RTOG (Fu et al. 2000,Update ASTRO 2005): 268 patients with locally advanced H&N cancer randomized to 2/70 Gy vs. 1.2 b.i.d./81.6 Gy vs. splitcourse 1.6 b.i.d./67.2 Gy (with a 2 weeks break) vs. concomitant boost RT to 72 Gy [with b.i.d. RT for last 12 fractions (1.8 and 1.5 Gy)] Onupdate, 5-year LRF and DFS improved w/ HFX and CB vs.standard fx and split-course. LRF: 60% standard, 58% splitcourse,52% CB, 51% HFX. DFS: 21% standard, 27% splitcourse,29% CB, 31% HFX. No difference in DM (27 29%), CSS (40 46%). Trend for improved OS with HFX (37 vs.29 34%).
53 53 Altered fractionation (Bourhis 2006): Meta-analysis of 15 trials with 6,515 patients, 74% with stage III IV disease, mostly of oropharynx and larynx, treated with conventional RT (1.8 2/65 70 Gy), hyperfractionated RT (higher dose, same time), accelerated RT (same dose, shorter time), or accelerated RT with reduced total dose. Altered fractionation improved 5-year OS by 3.4%, with greatest benefit for hyperfractionated RT (8% benefit) vs. accelerated RT (1.7 2% benefit). Five-year LRC benefit 6.4% overall, mainly for local as opposed to regional failure. Benefit highest for youngest patients (<50 60 years). No effect of altered fractionation on DM.
54 54 3.Chemo-RT ± altered fractionation Adelstein, Intergroup (Adelstein et al. 2003): 295 patients with unresectable H&N cancer, randomized to 2/70 Gy vs. 2/70 Gy +cisplatin (100 mg/m2) 3 cycles vs. split-course RT (2/30 Gy +2/30 40 Gy) + cisplatin/5- FU 3 cycles. Results: chemo-rt improved 3-year OS (23 vs. 37 vs. 27%) and DFS (33 vs. 51 vs.41%) but did not change DM and it increased toxicity
55 55 Bonner et al. (2006): 424 patients with locoregionally advanced resectable or unresectable stage III IV SCC of oropharynx, larynx, or hypopharynx randomized to RT or RT + cetuximab given 1 week before RT and weekly during RT. RT options included 2/70 Gy, 1.2 b.i.d./ Gy, or concomitant Boost 72 Gy. Cetuximab increased 3-years LRC (34 47%) and OS (45 55%). With the exception of acneiform rash and infusion reactions with cetuximab, toxicity was similar.
56 56 MACH-NC meta analysis (Pignon et al. 2009): 93 phase III trials and 17,346 patients. OS benefit (4.5%) at 5 years when chemotherapy was added to RT, with greater benefit for concurrent chemo- RT vs. induction chemo followed by RT (6.5% OS benefit with concurrent chemo-rt). Similar results in trials with post-op RT, conventional, and altered fractionation. No difference between mono or polychemotherapy regimens, but increased benefit with platinum-based compounds. Decreasing benefit with increasing age, with no benefit observed if more than 71-years old.
57 57 4. Post-op chemo-rt EORTC (O Sullivan et al. 2001, Cooper et al., NEJM 2004): 334 patients with operable stage III/IV H&N cancer randomized to post-op 2/66 Gy vs. post-op 2/66 Gy + concurrent cisplatin (100 mg/m2) on days 1, 22, and 43. Chemo-RT improved 3/5-year DFS (41/36 59/47%), OS (49/40 65/53%), and 5-year LRC (69 82%). No difference in DM (21 25%) or second primaries (12%). Chemo-RT increased grade 3/4 toxicities (21 41%).
58 58 RTOG (Forastiere et al. 2003; update ASCO 2006): 547 patients with stage III/IV larynx (T2 3 or lowvolume T4 without gross cartilage destruction or >1 cm base of tongue invasion, or LN+) randomized to one of three arms: RT alone, chemo -> RT, or concurrent chemo- RT. RT was 2/70 Gy in all arms. Induction chemo was cisplatin/5-fu 2c -> reassessment. If progression or <PR, treated with laryngectomy and post-op RT. If PR/CR -> third cycle chemo -> RT. Concurrent chemo was cisplatin 3c. All patients with cn2 had neck dissection within 8 weeks after RT.
59 On update, concurrent chemo-rt improved 5-year larynx preservation (84%) vs. induction chemo (71%) and RT alone (66%), and LRC (69%) vs. induction chemo (55%) and RT alone (51%). Chemo reduced the rate of DM (13% concurrent, 14% induction vs. 22% RT alone) and improved DFS (39% with chemo vs. 27% with RT alone). No difference in OS (55% concurrent, 59% induction, 54% RT alone) 59
60 thank you 60
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
Q&A. Fabulous Prizes. Collecting Cancer Data: Pharynx 12/6/12. NAACCR Webinar Series Collecting Cancer Data Pharynx
 Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic space
 Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
(loco-regional disease)
") (loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
(loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient
 Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
L ARYNX S TAGING F ORM
 CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
AJCC update Disclosures. AJCC TNM staging system. Objectives:
 Disclosures AJCC update 2018 Remy Lobo, MD remylobo@med.umich.edu remy.lobo@hsc.utah.edu No relevant disclosures Information is based on the 8 th AJCC manual Amin MB, Edge SB, Greene FL et al, eds. AJCC
Disclosures AJCC update 2018 Remy Lobo, MD remylobo@med.umich.edu remy.lobo@hsc.utah.edu No relevant disclosures Information is based on the 8 th AJCC manual Amin MB, Edge SB, Greene FL et al, eds. AJCC
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Head and Neck Tumours
 Head and Neck Tumours Introductory Notes The following sites are included: Lip, oral cavity Pharynx: oropharynx, nasopharynx, hypopharynx Larynx: supraglottis, glottis, subglottis Nasal cavity and paranasal
Head and Neck Tumours Introductory Notes The following sites are included: Lip, oral cavity Pharynx: oropharynx, nasopharynx, hypopharynx Larynx: supraglottis, glottis, subglottis Nasal cavity and paranasal
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
6 th Reprint Handbook Pages AJCC 7 th Edition
 6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
Esophagus Stomach 4/2/15
 Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Head & Neck Contouring
 Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma
 Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
LYMPHATIC DRAINAGE IN THE HEAD & NECK
 LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
2. Guidelines for Reporting Head and Neck Tumours
 39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
10. HPV-Mediated (p16+) Oropharyngeal Cancer
 Oropharyngeal Cancer") 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
The Neck the lower margin of the mandible above the suprasternal notch and the upper border of the clavicle
 The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
Piero Nicolai SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART. Department of Otorhinolaryngology University of Brescia
 Biology and technology contribution to clinical advancement: the case of oropharyngeal cancer Brescia May 8 th, 2009 SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART Piero Nicolai Department
Biology and technology contribution to clinical advancement: the case of oropharyngeal cancer Brescia May 8 th, 2009 SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART Piero Nicolai Department
PRINCIPLES OF RADIATION ONCOLOGY
 PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
Head & Neck Cancer Clinical Guidelines
 Head & Neck Cancer Clinical Guidelines Head & Neck NSSG on behalf of NECN Document Information Title: NECN Head and Neck Cancer Clinical Guidelines Author: Head and Neck NSSG Members Circulation List:
Head & Neck Cancer Clinical Guidelines Head & Neck NSSG on behalf of NECN Document Information Title: NECN Head and Neck Cancer Clinical Guidelines Author: Head and Neck NSSG Members Circulation List:
A220: Larynx cancer tissues. (formalin fixed)
") A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
Head & Neck Cancer: When to Irradiate
 Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Management of Salivary Gland Malignancies. No Disclosures or Conflicts of Interest. Anatomy 10/4/2013
 Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Nasal Cavity CS Tumor Size (Revised: 02/03/2010)
") Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Neck-2. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Refresher Course EAR TUMOR. Sasikarn Chamchod, MD Chulabhorn Hospital
 Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Head and Neck Cancer Service
 Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Management of unknown primary with neck node metastasis: Current evidence
 Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Volumi di trattamento del cavo orale
 SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
Clinical Study Regional Failures after Selective Neck Dissection in Previously Untreated Squamous Cell Carcinoma of Oral Cavity
 International Surgical Oncology, Article ID 205715, 8 pages http://dx.doi.org/10.1155/2014/205715 Clinical Study Regional Failures after Selective Neck Dissection in Previously Untreated Squamous Cell
International Surgical Oncology, Article ID 205715, 8 pages http://dx.doi.org/10.1155/2014/205715 Clinical Study Regional Failures after Selective Neck Dissection in Previously Untreated Squamous Cell
NAACCR Webinar Series 1
 Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
3/12/2018. Head & Neck Cancer Review INTRODUCTION
 Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience. Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore
 Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Head and Neck Case 1 PATIENT HISTORY
 Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
Alexander C Vlantis. Total Laryngectomy 57
 07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
Prevertebral Region, Pharynx and Soft Palate
 Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
Cancer of the Oral Cavity
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
Appendix 1: QIICR Iowa Head and Neck Clinical Data DICOM SR Template
 Appendix 1: QIICR Iowa Head and Neck Clinical Data DICOM SR Template Table of Content s Document Histor y TID QIICR_2000. Clinical Data Repor t TID QIICR_2002. Biops y TID QIICR_2003. Surgical Procedure
Appendix 1: QIICR Iowa Head and Neck Clinical Data DICOM SR Template Table of Content s Document Histor y TID QIICR_2000. Clinical Data Repor t TID QIICR_2002. Biops y TID QIICR_2003. Surgical Procedure
1/14/2019 CRITICAL PATHWAYS IN HEAD AND NECK CANCER DISCLOSURES OBJECTIVES
 CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
A Pathologist s Guide to Neck Dissection. Neck Dissections. Lymphatics of head and neck. Neck Dissections
 A Pathologist s Guide to Neck Dissection North American Society for Head and Neck Pathology Companion Meeting 2006 Sigrid Wayne, M.D. Department of Pathology University of Iowa The presence of cervical
A Pathologist s Guide to Neck Dissection North American Society for Head and Neck Pathology Companion Meeting 2006 Sigrid Wayne, M.D. Department of Pathology University of Iowa The presence of cervical
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology
 Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY
 PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey
 Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections Salivary glands* will not be covered specifically
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections Salivary glands* will not be covered specifically
Chapter 13: Mass in the Neck. Raymond P. Wood II:
 Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
9.5. CONVENTIONAL RADIOTHERAPY TECHNIQUE FOR TREATING THYROID CANCER
 9.5. CONVENTIONAL RADIOTHERAPY TECHNIQUE FOR TREATING THYROID CANCER ROBERT J. AMDUR, MD, SIYONG KIM, PhD, JONATHAN GANG LI, PhD, CHIRAY LIU, PhD, WILLIAM M. MENDENHALL, MD, AND ERNEST L. MAZZAFERRI, MD,
9.5. CONVENTIONAL RADIOTHERAPY TECHNIQUE FOR TREATING THYROID CANCER ROBERT J. AMDUR, MD, SIYONG KIM, PhD, JONATHAN GANG LI, PhD, CHIRAY LIU, PhD, WILLIAM M. MENDENHALL, MD, AND ERNEST L. MAZZAFERRI, MD,
Head & Neck Case # 1
 DISCHARGE SUMMARY Head & Neck Case # 1 Date of Admission: 10/30/2010 Date of Discharge: 11/02/2010 Present Medical History: The patient is a 33-year-old lady with a history of right superior alveolar ridge
DISCHARGE SUMMARY Head & Neck Case # 1 Date of Admission: 10/30/2010 Date of Discharge: 11/02/2010 Present Medical History: The patient is a 33-year-old lady with a history of right superior alveolar ridge
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx
 Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Principles of Radiation Oncology January 5, 2000
 TITLE: Principles of Radiation Oncology SOURCE: Grand Rounds Presentation, The University of Texas Medical Branch in Galveston, Department of Otolaryngology DATE: January 5, 2000 RESIDENT PHYSICIAN: Ravi
TITLE: Principles of Radiation Oncology SOURCE: Grand Rounds Presentation, The University of Texas Medical Branch in Galveston, Department of Otolaryngology DATE: January 5, 2000 RESIDENT PHYSICIAN: Ravi
14. Mucosal Melanoma of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Veins of the Face and the Neck
 Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Protocol for the Examination of Specimens From Patients With Carcinomas of the Pharynx
 Protocol for the Examination of Specimens From Patients With Carcinomas of the Pharynx Protocol applies to all invasive carcinomas of the pharynx (oropharynx, nasopharynx, hypopharynx) including the base
Protocol for the Examination of Specimens From Patients With Carcinomas of the Pharynx Protocol applies to all invasive carcinomas of the pharynx (oropharynx, nasopharynx, hypopharynx) including the base
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction