5/22/2018. Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma
|
|
|
- Drusilla Patrick
- 5 years ago
- Views:
Transcription





1 Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma Napa Valley Pathology Conference Silverado Resort & Spa May 18, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Head & Neck Squamous Cell Lesions Outline Keratinizing Dysplasia Select Variants of Squamous cell carcinoma Normal Squamous Epithelium Vocal cord Floor of Mouth Buccal Mucosa 1


2 Oral Leukoplakia Vocal Cord Leukoplakia Laryngeal Speckled Leukoplakia 2
 in the")
3 Epithelial Alterations Histopathology (Hyper)keratosis Hyperplasia Dysplasia: Spectrum of architectural and cytological epithelial changes caused by a gradual accumulation of genetic changes with an increased likelihood of progression to squamous cell carcinoma Criteria for Dysplasia 2017 WHO Blue Book Dyskeratosis Keratin not on the surface Individual cell keratinization Keratin pearl(s) in the middle or lower half of the epithelium Pink or glassy cytoplasm Paradoxical maturation 3
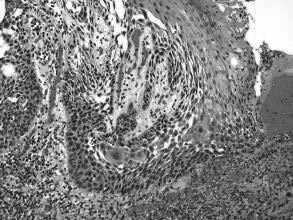
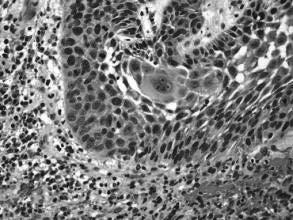
4 Dyskeratosis Paradoxical Maturation Keratosis without Dysplasia 4
 Keratosis without")

 full thickness")
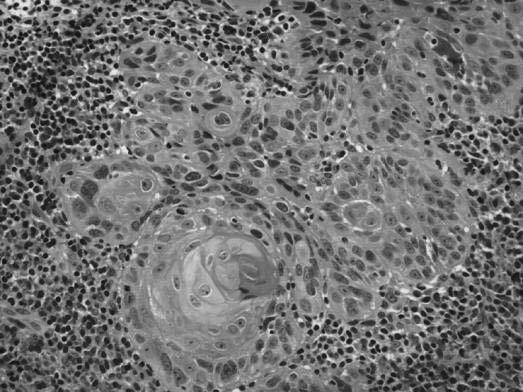
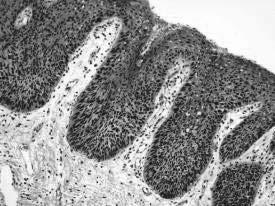
5 Verrucoid/Papillary Keratosis without Dysplasia (Papillary or verrucoid) Keratosis without Dysplasia Upper Aerodigestive Tract Epithelial Dysplasia Classic or Non-Keratinizing: Mild dysplasia Moderate dysplasia Severe dysplasia = Carcinoma in situ (CIS) full thickness intraepithelial dysplasia 5



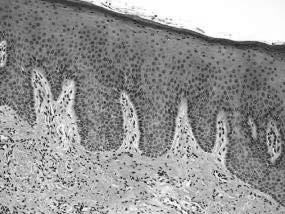
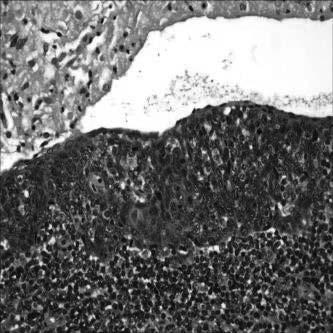
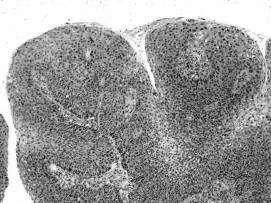
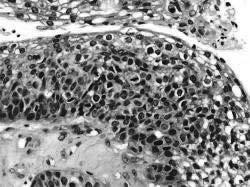
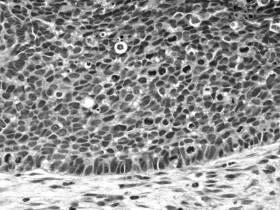
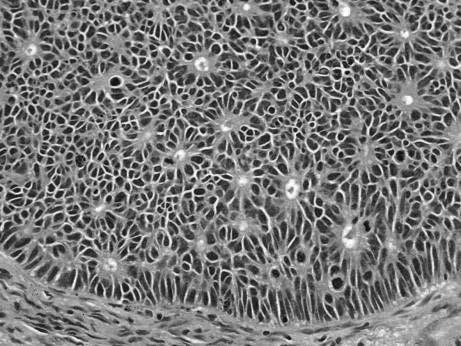
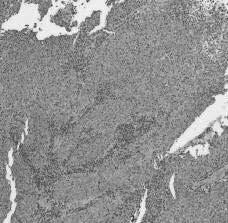
6 CIS (Nonkeratinizing) Uncommon as isolated lesion in H&N Occurs in mucosal sites that are usually clinically quiescent (e.g., supraglottic larynx, oro- & nasopharynx) only seen in association with invasive SCC Upper Aerodigestive Tract Epithelial Dysplasia Keratinizing >>>> Nonkeratinizing: Mild dysplasia Moderate dysplasia Severe dysplasia Keratinizing Mild Dysplasia 6
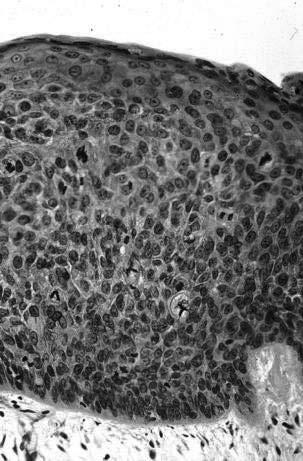

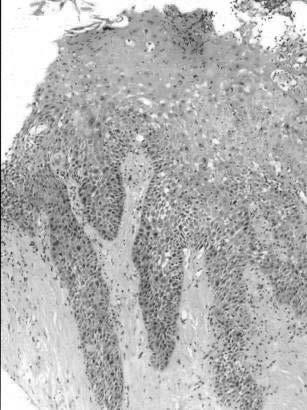
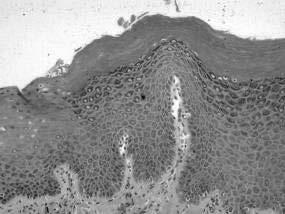
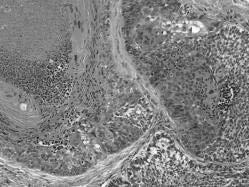
7 Keratinizing Moderate Dysplasia Keratinizing Severe Dysplasia Moderate? Severe? CIS? 7


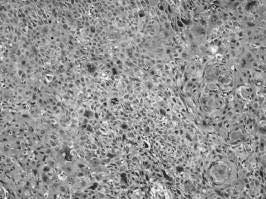
8 Drop Off Carcinoma Carcinoma In Situ (CIS) In the absence of full thickness intraepithelial dysplasia is the use of CIS justified? Does keratinizing severe dysplasia = CIS? Is it important to separate moderate and severe dysplasia/cis? Upper Aerodigestive Tract Keratinizing Dysplasia Goal of any grading system is: Reproducible and Applicable Convey to the clinician the potential risk for progression of disease 8
9 Upper Aerodigestive Tract Grading Keratinizing Dysplasia Imprecise and subjective Preferred grading based on degree and extent of cellular and maturation alterations mild dysplasia moderate dysplasia severe dysplasia 9

10 Grading Keratinizing Dysplasia No statistical difference in progression to invasive SCC between keratinizing moderate dysplasia and keratinizing severe dysplasia/cis Justification to 2-Tier grading scheme: Low-grade Dysplasia = Mild dysplasia High-grade Dysplasia = Moderate Dysplasia, Severe Dysplasia, CIS Better reproducibility Binary Grading Laryngeal Dysplasia 2017 WHO Blue Book 10

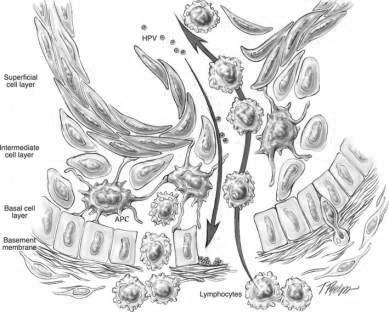
11 Binary Grading Oral Dysplasia 2017 WHO Blue Book Keratinizing Dysplasia Etiology Tobacco (smoking, chewing) Alcohol Areca nut, with or without tobacco, causes oral submucous fibrosis with a relatively high frequency of oral dysplasia High risk human papillomavirus? Generally not considered a risk factor Keratinizing Dysplasia IHC Staining p16, p53 and Ki67 (MIB1): p16 of limited diagnostic utility in keratinizing dysplasias of the UADT p53: increase expression Ki67: increase intraepithelial proliferation rate through all epithelial layers Overall of limited utility 11




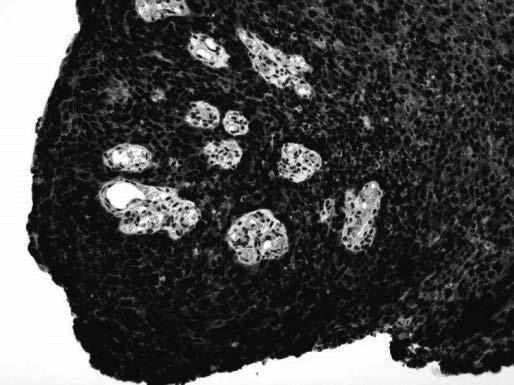
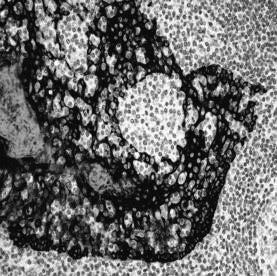
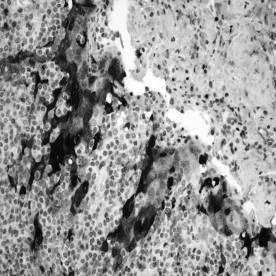
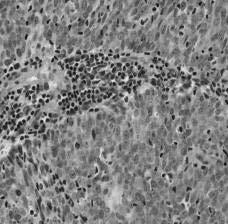
12 High-Grade Keratinizing Dysplasia Ki67 Ki67 Oral Dysplasia and HR-HPV HR-HPV infection found in oral keratinizing dysplasias*: Majority clinically oral leukoplakias Most adult men; Ventral tongue & FOM Diffuse loss of squamous differentiation with karyorrhexis & apoptosis, brightly eosinophilic apoptotic cells throughout epithelium, and conventional dysplastic changes proliferation index throughout epithelial layers p16+ihc & high-risk HPV subtypes *Woo SB, et al. Modern Pathol 2013;26: * McCord C, et al. Oral Surg Oral Med Oral Pathol Oral Radiol 2013;115:541-9 HR-HPV FOM Dysplasia p16 12
, location LVI, neurotropism and soft tissue invasion Regional metastasis - Extranodal")

13 HNSCC Factors Associated with Prognosis Adequacy of resection (surgical margins) Pattern of invasion: cohesive v dyscohesive Tumor size, depth of invasion (DOI), location LVI, neurotropism and soft tissue invasion Regional metastasis - Extranodal Extension Distant metastasis Angiogenesis; Host immune response Second malignancy Depth of Invasion (DOI) T1: Tumor 2cm & DOI 5mm T2: Tumor 2cm & DOI >5mm & 10mm or tumor >2cm but not 4cm, & DOI 10mm T3: Tumor >4cm or any tumor DOI >10mm Extranodal Extension 13
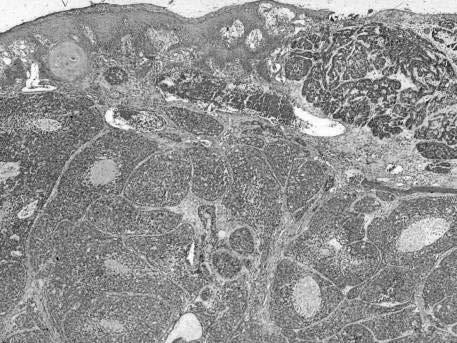
14 Variants of Squamous Cell Carcinoma of the Upper Aerodigestive Tract Squamous Cell Carcinoma Variants Verrucous Carcinoma Viral-Associated Carcinomas (HPV; EBV) Spindle Cell Squamous Carcinoma Papillary (Exophytic) SCC Basaloid Squamous Cell Carcinoma Adenosquamous Carcinoma Lymphoepithelial-like Carcinoma Adenoid SCC (angiosarcoma-like or acantholytic) Other variants: NUT carcinoma SMARCB1 (INI-1) Deficient Carcinoma Verrucous Carcinoma (VC) Highly differentiated variant of squamous cell carcinoma with locally destructive but not metastatic capabilities 14
 use HPV may play an active role in the multistep progression to cancer by binding (via protein products) to the RB gene")
15 Verrucous Carcinoma Clinical Features M > F; generally occurs in older age groups (6 th 7 th decades of life) Sites: oral cavity (4%) > larynx (1-3%) > other (sinonasal tract; nasopharynx) Symptoms vary according to site Verrucous Carcinoma Etiology Tobacco (smoking, chewing) use HPV may play an active role in the multistep progression to cancer by binding (via protein products) to the RB gene product removing regulatory block in the cell cycle (Science 1989;243:934-7 Recent studies using highly sensitive and specific molecular methods suggest that VC is not associated with human papillomavirus infection 15




16 Hybrid Carcinoma Tumor showing mixed histology including verrucous carcinoma and conventional SCC Oral cavity > larynx >>> other sites Biologic risk that of conventional SCC potential for metastasis Treatment that of conventional SCC Hybrid Carcinoma 16

 (n=26) 2 mm VC & SCC (n=14) >2mm")

17 Hybrid Carcinoma Hybrid Carcinoma Hybrid Carcinoma vs VC with Dysplasia or Minimal Invasion Patel KR, et al. Head Neck Pathol 2015;9:65-73: VC (n=18) VC with dysplasia or minimal invasion (VCDMI) (n=26) 2 mm VC & SCC (n=14) >2mm depth of invasion Prognosis: VC or VCDMI: limited recurrences, no metastases, no deaths VC&SCC: 50% recurrence; 14% nodal metastases; 36% DOD 17


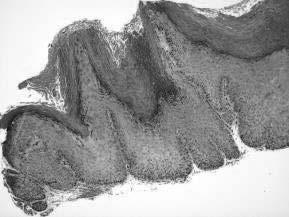

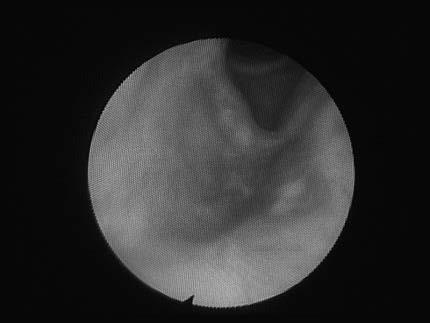
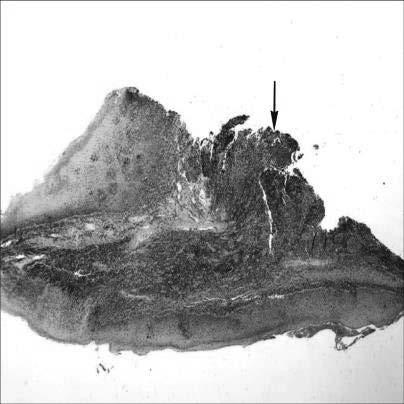
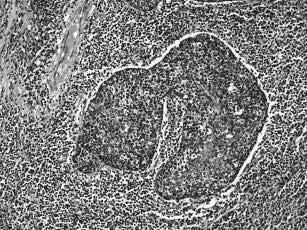
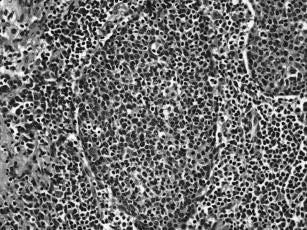
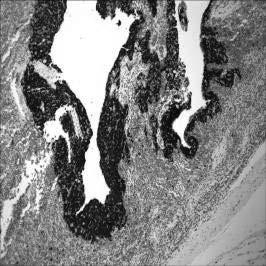
18 Biopsy Diagnosis of Verrucoid Lesions Biopsy Diagnosis of Verrucoid Lesions Biopsy Diagnosis of Verrucoid Lesions 18


19 Biopsy Diagnosis of Verrucoid Lesions Verrucous Carcinoma Biopsy Diagnosis Biopsy diagnosis of VC extremely difficult Adequate material is critical to interpretation and should include ample epithelial-stromal interface: Pathologists should not over interpret a verrucoid lesion as a carcinoma without adequate tissue Diagnosis of VC at initial presentation and biopsy is challenging given overall bland cytomorphology and shared features with reactive verrucoid lesions Verrucous Carcinoma Biopsy Diagnosis Well-differentiated verrucoid squamous epithelial proliferation, NOS complete excision & follow-up Recurrence of tumor at a future time may be the most important clue/evidence to diagnosis of VC 19




20 Verrucous Carcinoma Differential Diagnosis Conventional squamous cell carcinoma Reactive verrucoid hyperplasia Proliferative verrucous leukoplakia (PVL) Papilloma Proliferative Verrucous Leukoplaia PVL Diagnosis of PVL requires clinicopathologic correlation Suggested criteria to render diagnosis: - involvement of more than 2 oral cavity subsites - total size of the leukoplakic foci is >3cm - presence of disease for at least 5 years with history of progression and recurrence 20
21 Verrucous Carcinoma Treatment and Prognosis Surgery is the treatment of choice Radiotherapy used in select settings Excellent prognosis: for laryngeal VC: 5-yr survival rates of 86-95% Local recurrence but no metastases may cause extensive destruction if left untreated Does not metastasize Hybrid carcinoma has potential for metastasis and should be treated as conventional SCC Viral-Associated Neoplasms of the H&N Human papillomavirus (HPV): - Papilloma (Low-risk) - Oropharyngeal carcinoma (High-risk) Epstein-Barr virus (EBV): - Nasopharyngeal carcinoma - Hematolymphoid tumors - Smooth muscle tumors Merkel cell polyoma virus: - Merkel cell carcinoma Human herpes virus 8: - Kaposi sarcoma Human immunodeficiency virus (HIV) - HNSCC Viral-Associated Neoplasms of the Head & Neck Oropharyngeal HPV-associated squamous cell carcinoma (WHO 2017 SCC, HPV-positive): - Clinicopathologic features - Morphologic variants - Ancillary testing & CAP Recommendations - Non-squamous malignant neoplasms Nasopharyngeal EBV-associated squamous cell carcinoma Metastatic cervical carcinoma with unknown primary tumor 21
 All UADT mucosal sites Histology Nonkeratinizing")
 Good with high rate recurrence Worse disease-free and overall survival Cervical Neck Lymph Node Stations Site Specific Lymph Node")
22 HPV-positive SCC vs HPV-negative SCC HPV-positive SCC HPV-negative SCC Incidence Increasing Stable to decreasing Age/Gender Younger; M=F Older; M>F Race Caucasian >>>> African American African American > Caucasian Risk factors HPV Smoking, alcohol Primary location Oropharynx (BOT; tonsil) All UADT mucosal sites Histology Nonkeratinizing SCC Keratinizing SCC p16 Positive Negative AJCC staging Lower T, higher N Higher T, lower N ChemoXRT response Prognosis Good with low rate of recurrence Better disease-free & overall survival (worse if smokers) Good with high rate recurrence Worse disease-free and overall survival Cervical Neck Lymph Node Stations Site Specific Lymph Node Drainage 22

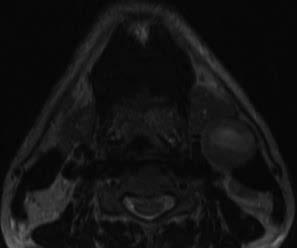
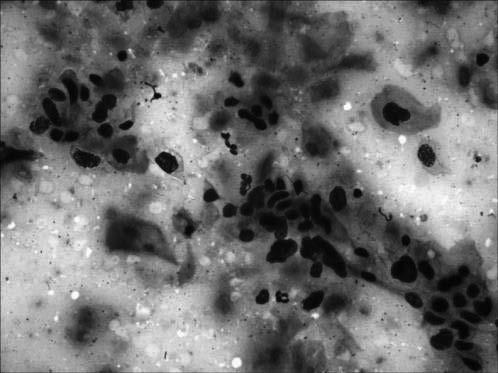
23 MRI T1 T2 FNAB FNAB Diagnosis Metastatic poorly-differentiated carcinoma favor squamous cell carcinoma 23


24 PET/CT BOT Biopsy BOT Biopsy 24

 Oropharyngeal Carcinoma (SCC, HPV-positive WHO")
25 CAM5.2 p16 Diagnosis Oropharyngeal (Tonsillar) Carcinoma: - Poorly-differentiated squamous cell carcinoma - Squamous cell carcinoma with basaloid features - Nonkeratinizing carcinoma - recapitulate tonsillar crypt epithelium so in fact are differentiated and NOT poorly-differentiated cancers and should not be graded as such Nonkeratinizing Carcinoma Human Papillomavirus (HPV) Oropharyngeal Carcinoma (SCC, HPV-positive WHO 2017) 25


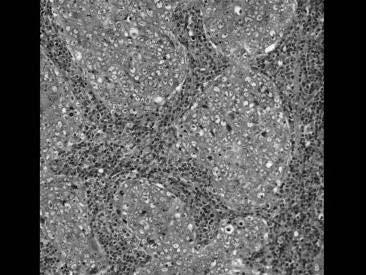
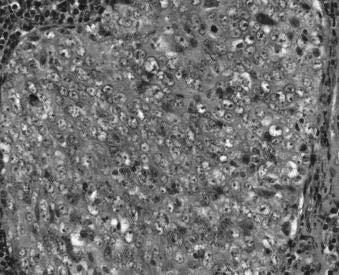
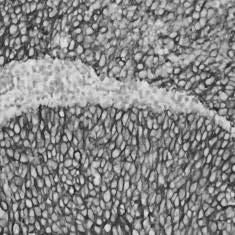
26 Invasive Oropharyngeal SCC, Predominantly Nonkeratinizing 26




27 Oropharyngeal SCC, HPV-Positive p16 ISH HPV16 Metastatic SCC, HPV-positive c/w Oropharyngeal Origin Metastatic SCC, HPV-positive c/w Oropharyngeal Origin p16 27

")
 Adenosquamous (Ciliated")
28 Hybrid Oropharyngeal SCC Hybrid Oropharyngeal SCC, HPV-positive p16 Oropharyngeal SCC, HPV-Positive Morphologic Spectrum Nonkeratinizing Hybrid Papillary SCC (PSCC) Basaloid SCC (BSCC) Spindle cell SCC (Sarcomatoid carcinoma) Adenosquamous (Ciliated cell) carcinoma Lymphoepithelial-like 28




29 PSCC PSCC PSCC 29

30 PSCC PSCC p16 BSCC 30


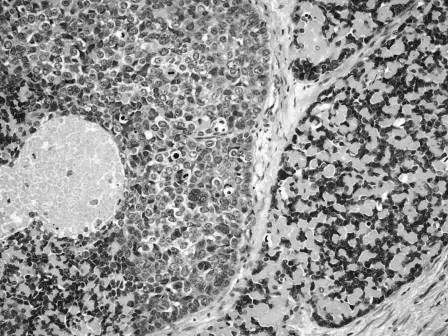
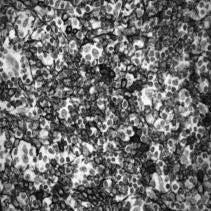
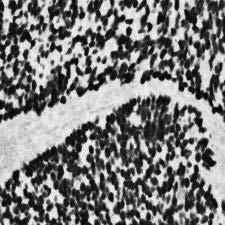
31 BSCC BSCC Nuclear palisading BSCC Lobular growth, comedonecrosis Reduplicated basement membrane-like material 31



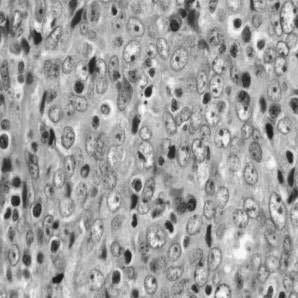
32 BSCC CIS BSCC Squamous differentiation BSCC Rosettes & Nuclear Palisading 32

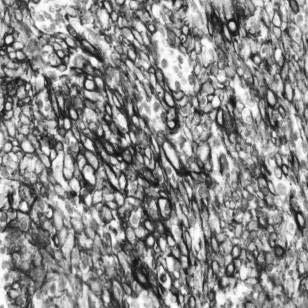
33 BSCC Perineural invasion BSCC IHC Findings IHC: Cytokeratins p63/p40 (diffusely positive) Variable reactivity for S100 protein, NSE Mesenchymal: Vimentin, SMA Negative for neuroendocrine, melanocytic and lymphoid markers p16: Most non-oropharyngeal HPV-negative Most oropharyngeal HPV-positive BSCC Treatment and Prognosis Aggressive management: Complete surgical resection Radiotherapy and chemotherapy HPV-negative: dismal prognosis Active smokers and those with nodal metastases at presentation have worse prognosis Lymphatic and hematogenous spread: Regional lymph nodes (50-70%) Lung, bone, skin and brain 33

 Any tumor appearing")

")
34 BSCC HPV-positive: Better overall prognosis than histologically similar non-hpv associated head and neck BSCC (Am J Surg Pathol 2008;32: ) Any tumor appearing to arise in the larynx/hypopharynx but that involves the oropharynx should be tested for HPV (p16) Adenosquamous (Ciliated Cell) Carcinoma Adenosquamous (Ciliated Cell) Carcinoma 34
 Bishop JA, Westra WH.")
 Definition Heterogeneous group of")
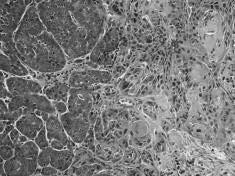
35 Adenosquamous (Ciliated Cell) Carcinoma p16 p16 Ciliated HPV-Associated Carcinoma (aka Ciliated Adenosquamous Carcinoma) Bishop JA, Westra WH. Am J Surg Pathol 2015;39: Radkay-Gonzalez L, et al. Head Neck Pathol 2016;10: Neuroendocrine Carcinoma (NEC) Definition Heterogeneous group of malignant neoplasms with divergent differentiation along epithelial and neuroendocrine cell lines 35
 = Carcinoid Tumor")

 PDNEC - SmCC PDNEC -")
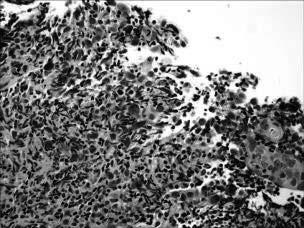
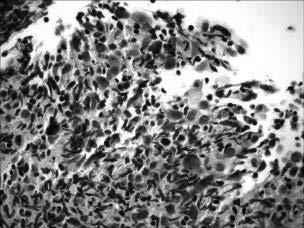
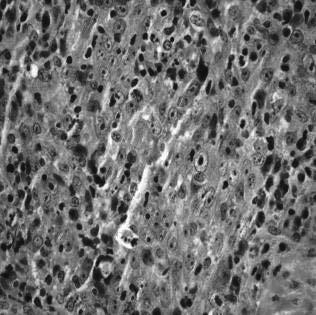
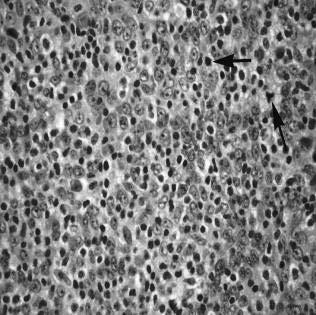
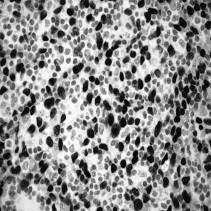
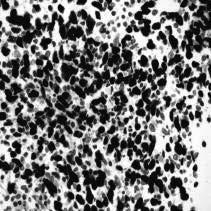
36 NEC of the Head and Neck 2017 WHO Classification Well-differentiated NEC (WDNEC) = Carcinoid Tumor Moderately-differentiated NEC (MDNEC) = Atypical Carcinoid Poorly-differentiated NEC = Small Cell Carcinoma (SmCC) Poorly-differentiated NEC = Large Cell Carcinoma (LCNEC) PDNEC - SmCC PDNEC - SmCC 36




37 PDNEC - SmCC CAM5.2 SYN p63/p40: negative CK5/6: negative TTF1 Oropharyngeal SmCC (HPV-Associated SmCC) p16 HPV-Related Small Cell Carcinoma of the Oropharynx Bishop & Westra. AJSP 2011;35: Kraft S, Faquin WC, Krane JF. AJSP 2012;36: cases - M > F; 6 th -7 th decades - Tonsil, base of tongue, neck - Smoking history - Presentation with neck metastases including occult primary 37

38 HPV-Associated Oropharyngeal SmCC Subset of HPV-related oropharyngeal carcinomas with small cell morphology Recognition and distinction from HPVrelated squamous cell carcinoma important Overlapping morphology CK5/6 and p63 may represent a key differentiating markers Despite presence of HPV, small cell phenotype indicate a greater propensity for aggressive clinical behavior PDNEC - LCNEC Clinical Features More common in men than women Occur over a wide age range average age of 59 years Predilect to the supraglottic larynx >> SNT >>> other Most patients are smokers May be associated with HPV (Oropharynx, SNT, larynx): - Mixed information in the literature relative to prognosis - Thompson ED et al. Am J Surg Pathol 2016;40:471-8: - HPV association may not impart more favorable prognosis 38





 Other typical")


39 PDNEC - LCNEC PDNEC - LCNEC - IHC CAM5.2 SYN CHR CD56 Criteria for (Laryngeal) LCNEC Lewis J, et al. Head Neck Pathol 2010;4: Requisite criteria Tumor cells with moderate to abundant cytoplasm Features of neuroendocrine differentiation (organoid nesting, trabecular growth, rosettes, and peripheral palisading) Mitotic activity > 10/10 hpf (2 mm 2 ) Other typical features Nuclei with prominent nucleoli Cellular pleomorphism Large areas of necrosis Confirmation of neuroendocrine differentiation using immunohistochemical staining 39
40 PDNEC - LCNEC Treatment and Prognosis Chemoradiotherapy Many patients have disseminated disease at presentation obviating option of laryngectomy and neck dissection Commonly present with advanced stage (stages III and IV): may be metastatic to cervical lymph nodes at presentation may be metastatic to distant sites at presentation (e.g., liver) 5-year disease specific survival (DSS) of 15-21% Head and Neck NECs Larynx most common site; less common sites include SNT, salivary gland, others M > F; generally occurs in the 6th-7th decades of life Larynx: Supraglottic larynx overwhelmingly the most common site of occurrence History of cigarette smoking > 60% MDNEC >>> SmCC >> LCNEC >>> WDNEC SNT and Salivary Gland (Parotid): SmCC >>> LCNEC >> MDNEC > WDNEC HPV Testing in HNSCC: Guidelines from CAP Lewis JS, et al. Arch Pathol Lab med 2018;142: Staining with IHC p16: - should be used as an initial screening method - nuclear & cytoplasmic positivity - > 70% cut off 14 Guideline statements - Strong recommendation - Recommendation - Expert consensus opinion - No recommendation 40
41 CAP Testing Guidelines for High Risk (HR)-HPV in H&N SCC #1: Strong recommendation should perform HR-HPV on all patients with newly diagnosed OPSCC, including all histologic subtypes; on primary tumor or on regional LN metastasis when clinical findings c/w OP origin #2: Recommendation For oropharyngeal tissue specimens (i.e., noncytology), pathologists should perform HR-HPV testing by surrogate marker p16 IHC. Additional HPV-specific testing may be done at the discretion of the pathologist and/or treating clinician, or in the context of a clinical trial CAP Testing Guidelines for High Risk (HR)-HPV in H&N SCC #3: Expert Consensus Opinion Pathologists should not routinely perform HR-HPV testing on patients with non-sccs of the oropharynx (neuroendocrine carcinomas; salivary gland carcinomas) #4: Recommendation Pathologists should not routinely perform HR-HPV testing on patients with nonoropharyngeal primary tumors of the H&N #5: Recommendation Pathologists should routinely perform HR-HPV testing on patients with metastatic SCC of unknown primary in a cervical upper or mid jugular chain lymph node. An explanatory note on the significance of a positive HPV result is recommended CAP Testing Guidelines for High Risk (HR)-HPV in H&N SCC #6: Expert Consensus Opinion For tissue specimens (i.e., noncytology) from patients presenting with metastatic SCC of unknown primary in a cervical upper or mid jugular chain lymph node, pathologists should perform p16 IHC NOTE: Additional HR-HPV testing on p16-positive cases should be performed for tumors located outside of level II or III (noncytology testing) in the neck and/or for tumors with keratinizing morphology 41
42 CAP Testing Guidelines for High Risk (HR)-HPV in H&N SCC #7: Expert Consensus Opinion Pathologists should perform HR-HPV testing on head and neck fine needle aspiration (FNA) SCC samples from all patients with known OPSCC not previously tested for HR-HPV, with suspected OPSCC, or with metastatic SCC of unknown primary NOTE: No recommendation is made for or against any specific testing methodology for HR-HPV testing in FNA samples. If the result of HR-HPV testing on the FNA sample is negative, testing should be performed on tissue if it becomes available. If pathologists use cytology samples for p16 IHC testing, they should validate the criteria (i.e., cutoff) for a positive result CAP Testing Guidelines for High Risk (HR)-HPV in H&N SCC #9: Expert Consensus Opinion Pathologists should not routinely perform low-risk HPV testing on patients with head and neck carcinomas #10: Expert Consensus Opinion - Pathologists should not repeat HPV testing on patients with locally recurrent, regionally recurrent, or persistent tumor if primary tumor HR-HPV status has already been established. If initial HR-HPV status was never assessed or results are unknown, testing is recommended. HPV testing may be performed on a case-by-case basis for diagnostic purposes if there is uncertainty regarding whether the tumor in question is a recurrence or a new primary SCC CAP Testing Guidelines for High Risk (HR)-HPV in H&N SCC #11: Expert Consensus Opinion Pathologists should not routinely perform HR-HPV testing on patients with distant metastases if primary tumor HR-HPV status has been established #12: Expert Consensus Opinion Pathologists should report primary OPSCCs that test positive for HR-HPV or its surrogate marker p16 as HPV-positive/p16-positive #13: Expert Consensus Opinion Pathologists should not provide a tumor grade or differentiation status for HPV-positive/p16- positive OPSCCs 42


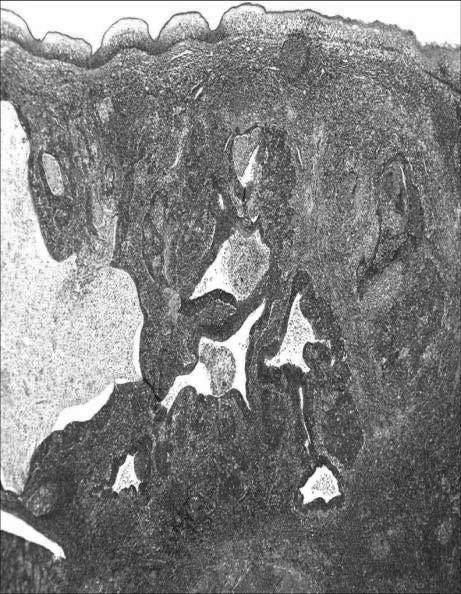
43 Oropharyngeal Reticulated Epithelium Oropharyngeal Reticulated Epithelium Immunohistochemistry AE1/AE3 p16 Reticulated Epithelium Westra WH: Head & Neck Pathol 2012;6:S48-S54 43




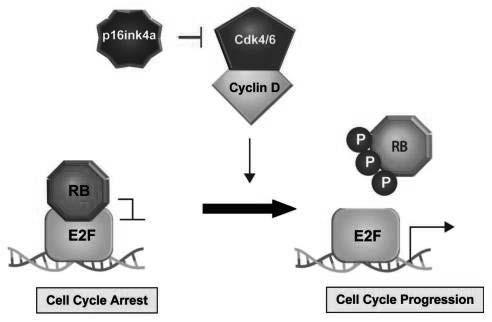
44 Carcinoma involving Tonsillar Crypt CIS p16 p16 Function p16 functions to activate RB-dependent cell cycle arrest 44


45 Distinct oncogenic pathways leading to p16 induction 45
 Undifferentiated type")


46 Nasopharyngeal Carcinoma (NPC) WHO Classification (2017) Keratinizing SCC: well-, moderately, poorly-differentiated (WHO 1) Nonkeratinizing SCC: Differentiated type (Transitional Cell or Cylindrical Cell Carcinoma; WHO 2) Undifferentiated type (Lymphoepithelioma; WHO 3) Basaloid SCC Percent Sex/Age EBV XRT Respons e 5-Yr survival Keratinizing Approximately 25% M > F; 4 th - 6th decades Weak association Radioresponsiveness is not good NPC Nonkeratinizing Differentiated Least common < 15% M > F; 4 th - 6th decades Strong association Radioresponsive Nonkeratinizing Undifferentiated Most common > 60% M > F; 4 th - 6th decades; may occur in children Strong association Radioresponsive 20-40% 75% 75% NPC, nonkeratinizing differentiated EBER 46
47 NPC, nonkeratinizing undifferentiated NPC, nonkeratinizing undifferentiated NPC, nonkeratinizing undifferentiated AE1/AE3 p63 EBER 47
48 Metastatic Cervical Carcinoma with an Unknown Primary Tumor (MCCUP) Definition: - Overt neck mass harboring a cytologically or histologically proven metastatic carcinoma in the absence of signs and symptoms of a primary neoplasm or of a clinically detectable mass: no history of previous malignancy or cancer ablation of any indeterminate lesion no history of definite symptoms related to a specific organ system no clinical or laboratory evidence of a primary neoplasm Luna MA. Chapter 17. In: Barnes L, ed. Surgical Pathology of the H&N Waldeyer Tonsillar Tissues 48
49 Luna MA. Chapter 17. In: Barnes L, ed. Surgical Pathology of the H&N Branchiogenic Carcinoma Criteria* Cervical tumor occurs along line extending from anterior to the tragus along the anterior border of the SCM to the clavicle Histology c/w origin from tissue known to be present in branchial vestige No primary source for carcinoma on at least 5-year f/u Histologic evidence of carcinoma arising in wall of epithelial-lined cyst *Martin et al. Ann Surg 1950;132: Branchial Cleft Cyst Benign lateral neck cyst most often of 2 nd branchial cleft apparatus Bimodal age: (75%); <5 yrs (20%): - rare ( 5%) in ages >40 years Painless cervical swelling typically near angle of mandible along border of SCM 49





")


50 Branchial Cleft Cyst p16 p16 p16 Case History 39 year old female presented with an enlarging right sided neck mass at Level IIA (subdigastric lymph node) There was no past or current history of malignancy The lymph node was excised Level IIA Lymph Node 50



51 Level IIA Lymph Node Level IIA Lymph Node Case AE1/AE3 p63 51
 negative Case EBER p16 Case Diagnosis Metastatic")

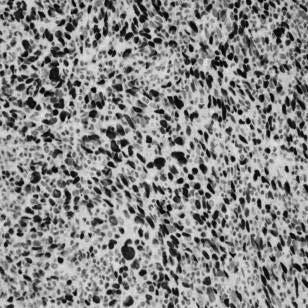
52 Case Other IHC Hematolymphoid markers (CD45; CD20) negative Melanoma markers (S100 protein, HMB45, others) negative Case EBER p16 Case Diagnosis Metastatic HPV-associated lymphoepithelial-like carcinoma consistent with oropharyngeal origin Endoscopic biopsies of UADT sites including oro- and nasopharynx were performed 52



53 Right Tonsil Biopsy Right Tonsil Biopsy AE1/AE3 p63 p16 EBER Lymphoepithelial-like Carcinoma of the Oropharynx: A morphologic variant of HPV-related head and neck carcinoma Singhi AD, Stelow EB, Mills SE, Westra WH. Am J Surg Pathol 2010;34:
54 Squamous Cell Lesions Summary Overview of intraepithelial alterations of the upper aerodigestive tract: focus on keratinizing dysplasia 2 Tier grading system: Low-grade (mild dysplasia) High-grade (moderate & severe dysplasia and CIS) Verrucous carcinoma diagnosis Squamous Cell Lesions Summary Viral carcinogenesis causally associated with HNSCC Classification: - SCC, HPV-positive (oropharynx) - SCC, EBV-positive (nasopharynx) Overall better prognosis than non-viral associated HNSCC Overlapping morphology between HPV+ and EBV+ cancers: - When confronted with MCCUP, both p16 and EBER should be performed No correlation to size of primary neoplasm (millimeters) and size of metastasis (centimeters) - tiny foci may give rise to large metastases Relative to oropharyngeal cancers concept of CIS is not applicable: - lesions that morphologically appear to be CIS may metastasize AJCC Staging 8 th Edition HPV-mediated (p16+) Oropharyngeal Cancer (Chapter 10): - Descriptor poorly-differentiated at odds with known improved prognosis so use should be avoided - Use of the designation oropharyngeal SCC, nonkeratinizing type is recommended - Histologic grading is not relevant - Presence of keratinization in a p16+/hr HPV+ carcinoma does not exclude using this staging system - Cervical lymph node metastases (to level II/III) from unknown primary tumor (pt0) that is p16+ and histology is consistent with HPV-mediated carcinogenesis are staged according to the guidelines in this chapter - Diagnosis of malignant transformation of branchial cleft cyst should be rejected 54
 H. Lee Moffitt Cancer Center and Research Institute Questions? bruce.wenig@moffitt.")
55 Squamous Cell Lesions Summary New WHO Classification of H&N PDNEC includes small cell and large cell types PDNEC may also metastasize without a known primary particularly of oropharyngeal origin: - May be HPV+ (not associated with more favorable prognosis) H. Lee Moffitt Cancer Center and Research Institute Questions? bruce.wenig@moffitt.org 55
Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma
 Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma Napa Valley Pathology Conference Silverado Resort & Spa May 18, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL
Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma Napa Valley Pathology Conference Silverado Resort & Spa May 18, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL
Moffitt Weekends in Pathology Head & Neck, and Endocrine Pathology Course Outline
 Moffitt Weekends in Pathology Head & Neck, and Endocrine Pathology Course Outline Squamous Cell Lesions Lecture BMW: 8:30-9:15 Break: 9:15-9:30 Case Review LK: 9:30-10:15 Case Review JHP: 10:30-11:15 Break:
Moffitt Weekends in Pathology Head & Neck, and Endocrine Pathology Course Outline Squamous Cell Lesions Lecture BMW: 8:30-9:15 Break: 9:15-9:30 Case Review LK: 9:30-10:15 Case Review JHP: 10:30-11:15 Break:
Human Papillomavirus Testing in Head and Neck Carcinomas
 Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
Squamous Cell Carcinoma of the Head and Neck (SCCHN)
") Squamous Cell Carcinoma of the Head and Neck (SCCHN) Part 1 Bruce M. Wenig, M.D. Dept. of Pathology & Laboratory Medicine Continuum Health Partners New York, NY College of American Pathologists 2004. Materials
Squamous Cell Carcinoma of the Head and Neck (SCCHN) Part 1 Bruce M. Wenig, M.D. Dept. of Pathology & Laboratory Medicine Continuum Health Partners New York, NY College of American Pathologists 2004. Materials
Human Papillomavirus and Head and Neck Cancer. Ed Stelow, MD
 Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Notice of Faculty Disclosures
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF SQUAMOUS CYSTS OF THE HEAD AND
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF SQUAMOUS CYSTS OF THE HEAD AND
Head and Neck Squamous Subtypes
 1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
Basaloid neoplasms of the head and neck. Basaloid SCC. Clinico-pathologic features 5/5/11. Basaloid Tumors Head and Neck
 Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Dysplasia, Mimics and Other Controversies
 Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
HPV and Head and Neck Cancer: What it means for you and your patients
 HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
Reporting HPV related carcinomas of the head and neck. dr. Nina Zidar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia
 Reporting HPV related carcinomas of the head and neck dr. Nina Zidar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia Conflict of interest/funding X None Company: Product royalties
Reporting HPV related carcinomas of the head and neck dr. Nina Zidar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia Conflict of interest/funding X None Company: Product royalties
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland
 Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
HPV Analysis of Head and Neck Squamous Cell Carcinomas based on Fine-Needle. Aspiration Specimens. William H. Westra M.D.
 HPV Analysis of Head and Neck Squamous Cell Carcinomas based on Fine-Needle Aspiration Specimens William H. Westra M.D. The Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore Maryland
HPV Analysis of Head and Neck Squamous Cell Carcinomas based on Fine-Needle Aspiration Specimens William H. Westra M.D. The Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore Maryland
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Diagnostic difficulties with lesions of the oral mucosa
 BDIAP London, November 2010 School of Clinical Dentistry University of Sheffield Diagnostic difficulties with lesions of the oral mucosa Paul M Speight Dept Oral & Maxillofacial Pathology University of
BDIAP London, November 2010 School of Clinical Dentistry University of Sheffield Diagnostic difficulties with lesions of the oral mucosa Paul M Speight Dept Oral & Maxillofacial Pathology University of
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck SCC. HPV in Tumors of the Head and Neck. Overview. Role of HPV in Pathogenesis of Head & Neck Tumors
 HPV in Tumors of the Head and Neck Christina Kong, M.D. Associate Professor, Stanford Dept of Pathology Director, Cytopathology Laboratory & Cytopathology Fellowship ckong@stanford.edu Head and Neck SCC
HPV in Tumors of the Head and Neck Christina Kong, M.D. Associate Professor, Stanford Dept of Pathology Director, Cytopathology Laboratory & Cytopathology Fellowship ckong@stanford.edu Head and Neck SCC
Diseases of oral cavity
 Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
Evaluation and Management of Head and Neck Cancer in Patients with Fanconi anemia David I. Kutler, M.D., F.A.C.S.
 Evaluation and Management of Head and Neck Cancer in Patients with Fanconi anemia David I. Kutler, M.D., F.A.C.S. Residency Site Director Weill Cornell Medical Center Associate Professor Division of Head
Evaluation and Management of Head and Neck Cancer in Patients with Fanconi anemia David I. Kutler, M.D., F.A.C.S. Residency Site Director Weill Cornell Medical Center Associate Professor Division of Head
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Squamous cell carcinoma of the upper aerodigestive tract: dysplasia and select variants
 S112 2017 USCAP, Inc All rights reserved 0893-3952/17 $32.00 Squamous cell carcinoma of the upper aerodigestive tract: dysplasia and select variants Bruce M Wenig Department of Pathology, Moffitt Cancer
S112 2017 USCAP, Inc All rights reserved 0893-3952/17 $32.00 Squamous cell carcinoma of the upper aerodigestive tract: dysplasia and select variants Bruce M Wenig Department of Pathology, Moffitt Cancer
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Neuroendocrine Carcinoma. Lebanon Neuroendocrine Neoplasms of H&N Nov /7/2011. Broad Classification:
 H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Nasal Cavity and Paranasal Sinuses
 Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22
 Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22 History of ITET/CASTLE First Report Gross Appearance and Prognosis 1) Miyauchi A et al: Intrathyroidal epithelial
Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22 History of ITET/CASTLE First Report Gross Appearance and Prognosis 1) Miyauchi A et al: Intrathyroidal epithelial
VULVAR CARCINOMA. Page 1 of 5
 VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
Head and Neck Pathology. Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital)
") Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
3/28/2017. Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center
 Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
3/27/2017. Pulmonary Pathology Specialty Conference. Disclosure of Relevant Financial Relationships. Clinical History:
 Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
HEAD AND NECK PATHOLOGY
 Bosnian-British School of Pathology November 2012 HEAD AND NECK PATHOLOGY Slide seminar: Oral Pathology Preferred Diagnoses Dr A Sandison, Slide seminar: Pathology of the Oral Cavity Page 1 of 5 1. Female
Bosnian-British School of Pathology November 2012 HEAD AND NECK PATHOLOGY Slide seminar: Oral Pathology Preferred Diagnoses Dr A Sandison, Slide seminar: Pathology of the Oral Cavity Page 1 of 5 1. Female
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES)
") NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
Human Papillomavirus and Epstein Barr Virus in Head and Neck Carcinomas: Suggestions for the New WHO Classification
 Head and Neck Pathol (2014) 8:50 58 DOI 10.1007/s12105-014-0528-6 PROCEEDINGS OF THE NORTH AMERICAN SOCIETY OF HEAD AND NECK PATHOLOGY COMPANION MEETING, MARCH 2, 2014, SAN DIEGO, CALIFORNIA Human Papillomavirus
Head and Neck Pathol (2014) 8:50 58 DOI 10.1007/s12105-014-0528-6 PROCEEDINGS OF THE NORTH AMERICAN SOCIETY OF HEAD AND NECK PATHOLOGY COMPANION MEETING, MARCH 2, 2014, SAN DIEGO, CALIFORNIA Human Papillomavirus
Sarcomatoid (spindle cell) carcinoma of the cricopharynx presenting as dysphagia
 carcinoma of the cricopharynx presenting as dysphagia") Case Report Sarcomatoid (spindle cell) carcinoma of the cricopharynx presenting as dysphagia Jagtap Sunil V. 1, Shukla Dhirajkumar B. 2, Jagtap Swati S. 3, Havle Abhay D. 4 1 Associate Professor, Department
Case Report Sarcomatoid (spindle cell) carcinoma of the cricopharynx presenting as dysphagia Jagtap Sunil V. 1, Shukla Dhirajkumar B. 2, Jagtap Swati S. 3, Havle Abhay D. 4 1 Associate Professor, Department
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Polymorphous Low-Grade. December 5 th, 2008
 Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Nasopharynx. 1. Introduction. 1.1 General Information and Aetiology
 Nasopharynx 1. Introduction 1.1 General Information and Aetiology The nasopharynx is the uppermost, nasal part of the pharynx. It extends from the base of the skull to the upper surface of the soft palate.
Nasopharynx 1. Introduction 1.1 General Information and Aetiology The nasopharynx is the uppermost, nasal part of the pharynx. It extends from the base of the skull to the upper surface of the soft palate.
Penile cancer teams in UK. Common variants. Penile cancer teams. Basaloid squamous carcinoma. The Pathology of Penile Tumours
 The Pathology of Penile Tumours Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Penile cancer teams in UK 12 centres for penile cancer work (10 in England and Wales, 2 in Scotland)
The Pathology of Penile Tumours Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Penile cancer teams in UK 12 centres for penile cancer work (10 in England and Wales, 2 in Scotland)
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
Head & Neck Staging. Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging
 AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging. Head & Neck Staging. Learning Objectives. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Case Presentation. Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD. Department of Pathology Jordan University Hospital Amman, Jordan
 Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Physician to Physician AJCC 8 th Edition. Head and Neck. Summary of Changes. AJCC Cancer Staging Manual, 7 th Ed. Head and Neck Chapters
 Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Pathology of Selected Head and Neck Lesions. Adel Assaad MD Department of Pathology
 Pathology of Selected Head and Neck Lesions Adel Assaad MD Department of Pathology 1 NOSE Infections 2 Zygomycosis (Mucormycosis) Opportunistic infection caused by "bread mold fungi," including Rhizopus,
Pathology of Selected Head and Neck Lesions Adel Assaad MD Department of Pathology 1 NOSE Infections 2 Zygomycosis (Mucormycosis) Opportunistic infection caused by "bread mold fungi," including Rhizopus,
Small (and large) Blue Cell Tumors of the Skull Base
 Blue Cell Tumors of the Skull Base") Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
4/17/2015. Case 1. A 37 year old man with a 2.2 cm solitary left thyroid mass.
 Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Cystic carcinoma of the neck
 Case Report Brunei Int Med J. 2010; 6 (1): 56-60 Cystic carcinoma of the neck Prathibha Parampalli SUBRHAMANYA, Ghazala KAFEEL, Hla OO, Pemasiri Upali TELISINGHE, Department of Pathology, RIPAS Hospital,
Case Report Brunei Int Med J. 2010; 6 (1): 56-60 Cystic carcinoma of the neck Prathibha Parampalli SUBRHAMANYA, Ghazala KAFEEL, Hla OO, Pemasiri Upali TELISINGHE, Department of Pathology, RIPAS Hospital,
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey
 Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections Salivary glands* will not be covered specifically
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections Salivary glands* will not be covered specifically
A neoplasm is defined as "an abnormal tissue proliferation, which exceeds that of adjacent normal tissue. This proliferation continues even after
 NEOPLASIA Neoplasia is a very important topic in pathology because neoplasms are both common and serious diseases. A neoplasm literally means a new growth, and this term is used interchangeably with a
NEOPLASIA Neoplasia is a very important topic in pathology because neoplasms are both common and serious diseases. A neoplasm literally means a new growth, and this term is used interchangeably with a
Problem diagnoses. Current issues in Anatomic pathology. Problem Diagnoses in Tumors of the Oral Cavity 5/29/2009
 Current issues in Anatomic pathology Problem Diagnoses in Tumors of the Oral Cavity Richard Jordan DDS PhD FRCPath Professor of Oral Pathology & Pathology Director, UCSF Oral Pathology Diagnostic Laboratory
Current issues in Anatomic pathology Problem Diagnoses in Tumors of the Oral Cavity Richard Jordan DDS PhD FRCPath Professor of Oral Pathology & Pathology Director, UCSF Oral Pathology Diagnostic Laboratory
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
5/22/2017. An Aggressive Nasopharyngeal Tumor. Case History
 An Aggressive Nasopharyngeal Tumor Head & Neck/Endocrine Evening Specialty Conference Martin Bullock, MD, FRCPC Dalhousie University, Halifax, Nova Scotia Case History 52-year-old male, 6 month history
An Aggressive Nasopharyngeal Tumor Head & Neck/Endocrine Evening Specialty Conference Martin Bullock, MD, FRCPC Dalhousie University, Halifax, Nova Scotia Case History 52-year-old male, 6 month history
Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case
 Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Update of the role of Human Papillomavirus in Head and Neck Cancer
 Update of the role of Human Papillomavirus in Head and Neck Cancer 2013 International & 12 th National Head and Neck Tumour Conference Shanghai, 11 13 Oct 2013 Prof. Paul KS Chan Department of Microbiology
Update of the role of Human Papillomavirus in Head and Neck Cancer 2013 International & 12 th National Head and Neck Tumour Conference Shanghai, 11 13 Oct 2013 Prof. Paul KS Chan Department of Microbiology
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Management of unknown primary with neck node metastasis: Current evidence
 Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
Histological Typing Of Cancer And Precancer Of The Oral Mucosa
 Histological Typing Of Cancer And Precancer Of The Oral Mucosa 1 / 7 2 / 7 3 / 7 Histological Typing Of Cancer And Within the last decade, histologic grading has become widely accepted as a powerful indicator
Histological Typing Of Cancer And Precancer Of The Oral Mucosa 1 / 7 2 / 7 3 / 7 Histological Typing Of Cancer And Within the last decade, histologic grading has become widely accepted as a powerful indicator
الطلاوة = Leukoplakia LEUKOPLAKIA
 LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
Pathological Classification of Hepatocellular Carcinoma
 3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS. Dr. Pamela Hanson DO PGY3
 PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Squamous Cell Neoplasia and Precursor Lesions
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory