5/26/2016. Pelvic Serous Carcinoma: 2014 W.H.O. Update. Outline of Talk. Changes to 2014 WHO system for pelvic serous tumors
|
|
|
- Cuthbert Doyle
- 5 years ago
- Views:
Transcription






1 Pelvic Serous Carcinoma: 2014 W.H.O. Update Outline of Talk Practical Implications for Pathologists Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous carcinoma New recommendations for assigning primary tumor origin Special issues with serous borderline tumors Joseph Rabban MD MPH Pathology Department University of California, San Francisco What happened between 2003 WHO and 2014 WHO? What happened between 2003 WHO and 2014 WHO? 20 th Century Model of Ovarian Cancer Single disease Multiple morphologies Origin from surface lining cells Unclear pathogenesis Unclear risk reduction Unclear early detection 21st Century Model of Ovarian Cancer Multiple unique diseases Each with unique: Pathogenesis, origin Responses to treatment Risk reduction options Early detection options 1
2 Ovarian Carcinomas in 2014 WHO 3 Major Changes to Pelvic Serous Tumors in 2014 WHO High grade serous carcinoma (HGSC) Low grade serous carcinoma (LGSC) Clear cell carcinoma Endometrioid adenocarcinoma Mucinous carcinoma 1 Tumor Class Surface epithelial stromal tumors Rationale: Epithelial tumors New Evidence Implications Tumor origin is fallopian tube mucosa (either in tube as STIC or in ovary as epithelial inclusion cyst) Fallopian tube is target for risk reduction, early detection Proposed Tubal Origins of Ovarian HGSC versus LGSC Proposed Tubal Origins of Ovarian HGSC versus LGSC P53 Tubal HGSC (STIC) Benign tubal mucosa Ovarian HGSC Inclusion gland P53 Ovarian HGSC 2
3 Proposed Tubal Origins of Ovarian HGSC versus LGSC Proposed Tubal Origins of Ovarian HGSC versus LGSC Benign tubal mucosa p53 Tubal HGSC (STIC) benign spread Inclusion gland BRAF KRAS MAPK pathway Ovarian Serous Borderline Tumor Ovarian LGSC Inclusion gland BRAF KRAS MAPK pathway p53 Ovarian Serous Borderline Tumor Ovarian HGSC Ovarian LGSC 3 Major Changes to Pelvic Serous Tumors in 2014 WHO 3 Major Changes to Pelvic Serous Tumors in 2014 WHO 1 Tumor Class Surface epithelial stromal tumors 2 Serous Carcinoma Rationale: One tumor, grade 1,2, Epithelial tumors Two tumors: HGSC, LGSC 1 Tumor Class Surface epithelial stromal tumors 2 Serous Carcinoma 3 Transitional cell carcinoma One tumor, grade 1,2,3 Unique tumor Epithelial tumors Two tumors: HGSC, LGSC Eliminated. Viewed as variant of HGSC New Evidence Implications Distinct behavior, response to therapy, genetics, pathogenesis, origin Distinct surgical planning, adjuvant therapy, genetic counseling, risk reduction Rationale: New Evidence Implications TCC has same properties as HGSC Diagnosis of HGSC includes many different patterns beyond papillary (TCC, endometrioid, solid) 3


4 Outline of Talk High Grade Serous Carcinoma Low Grade Serous Carcinoma HGSC LGSC Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous carcinoma New recommendations for assigning primary tumor origin Special issues with serous borderline tumors LGSC: Clinico-pathologic Features HGSC LGSC Incidence Age Risk factors Hereditary? Stage Median survival Time to recurrence ~5 % of all ovarian cancers Average 4 th to 5 th decade No traditional HGSC risk factors 20% risk if prior history of advanced stage serous borderline tumor ~ risk if prior ovulation induction for fertility No major syndrome known >75% are advanced stage at diagnosis ~80-96 months ~33 months if optimal cytoreduction ~14 months if suboptimal cytoreduction BRCA hereditary syndrome ~25 % No P53 mutation Yes No BRAF KRAS MAPK pathway defects No Common Precursor lesion STIC Borderline tumor Platinum chemotherapy sensitive Yes Uncommon PARP inhibitor sensitive Yes Unlikely Neoadjuvant chemotherapy candidate Yes No MAPK pathway inhibitor candidate No Yes Romero 2013 Gyn Oncol Fader 2013 Ob Gynecol 4




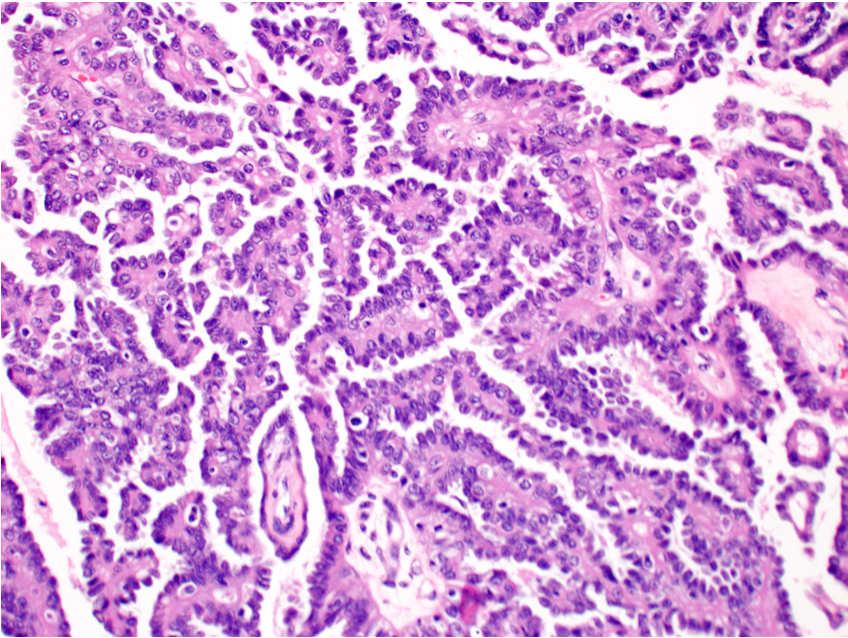
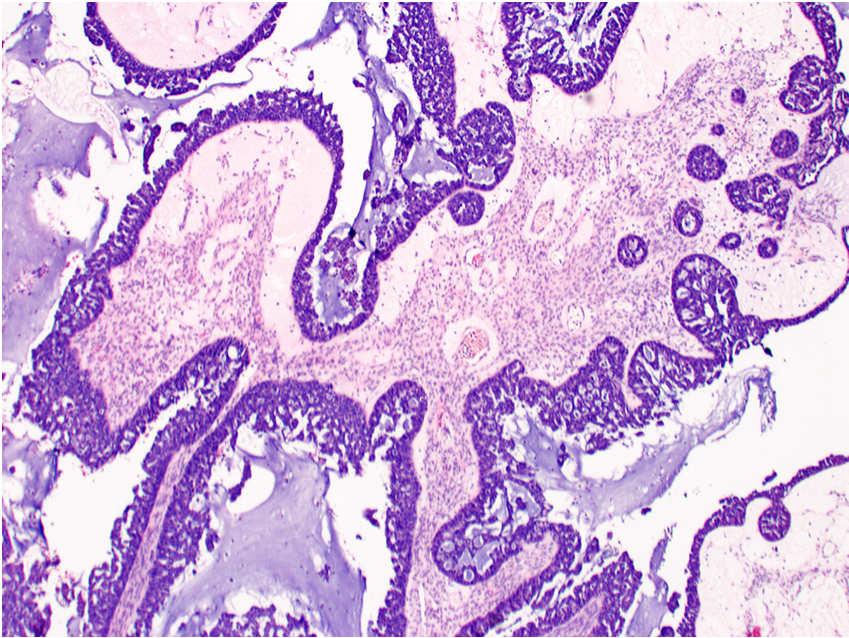
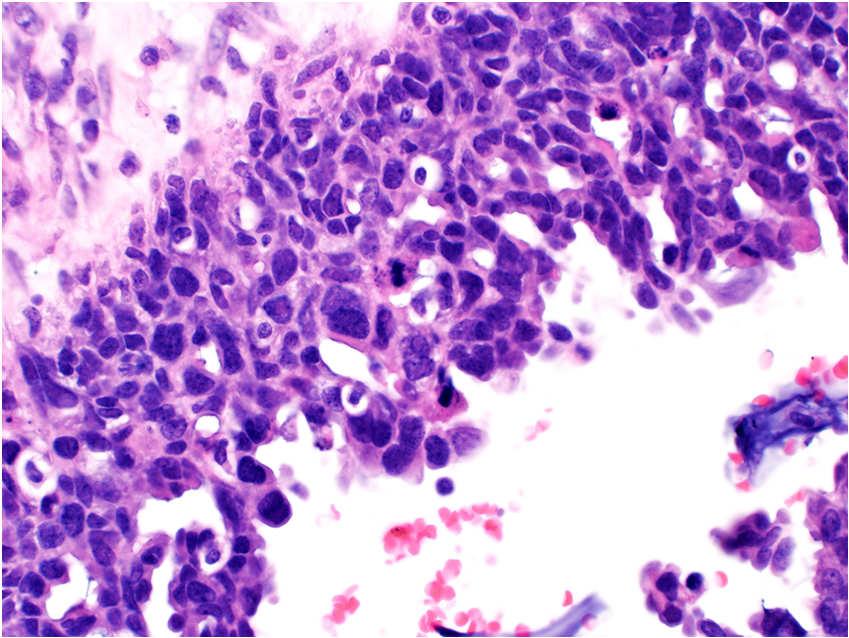
5 HGSC HGSC: Papillary pattern Architecture Papillary Micro-papillary Solid Pseudo-endometrioid (cribriform) Transitional cell carcinoma-like Cytology High nucleus-cytoplasm ratio Pleomorphism Nuclear hyperchromasia Brisk / atypical mitoses Macro-nucleoli HGSC: Papillary pattern HGSC: Transitional cell cancer-like pattern Pleomorphism, high N/C ratio, brisk mitoses 5



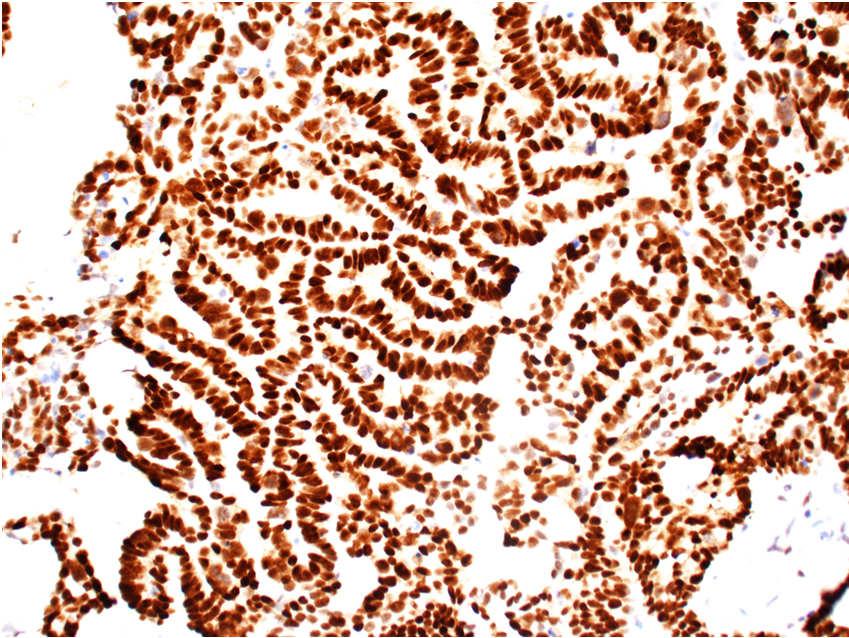
6 HGSC: Transitional cell cancer-like pattern HGSC: Pseudo-endometrioid pattern HGSC: Pseudo-endometrioid pattern HGSC Immunophenotype Mullerian origin Extra-uterine serous differentiation High grade serous carcinoma + PAX8, CK7 + WT1 Aberrant p53, p16 6



 not HGSC * Check for")
7 p53 and Pelvic HGSC p53 and Pelvic HGSC Normal p53 gene p53 IHC stain result p53 gene mutation p53 IHC stain result Weak patchy staining ( Normal / Wild type) ~80% Diffuse, strong staining ~20% Completely negative p53 Stain Interpretation in Pelvic Serous Carcinoma p53 Stain Interpretation in Pelvic Serous Carcinoma Pattern of p53 IHC staining Stain Interpretation Diagnosis Aberrant p53 Aberrant p53 HGSC HGSC Wild type p53 not HGSC* Strong/diffuse Completely negative Aberrant p53 HGSC Weak/patchy Wild type p53 (normal) not HGSC * Check for internal control 7



8 p16 Stain Interpretation in Pelvic Serous Carcinoma Use both p53 and p16 stains for HGSC Diffuse / strong = Aberrant p16 Patchy or negative = Wild-type p16 Cannot use p53 alone if result is wild type 4% of HGSC are wild type p53 / aberrant p16 Always do both stains together LGSC MD Anderson Criteria for LGSC Architecture Cytology Papillary branching Micro-papillary Bud-like Macro-papillary Cribriform Uniform, monotonous Focal moderate atypia (<3:1 variable size) Mitoses < 12 / 10 hpf Atypical mitoses uncommon Grading System # of Grading Tiers FIGO 3 Shimizu-Silverberg 3 MD Anderson 2 8
9 FIGO Universal Grading of Pelvic Cancer (any type) Shimizu-Silverberg Universal Grading of Ovarian Cancer (any type) Grade Solid Architecture 1 <6 % 2 6 % 50% 3 > 50% Points Architecture Atypia Mitoses /10 hpf 1 Glandular Mild Papillary Moderate Solid Severe >24 Total Points Overall Grade , 7 2 8, 9 3 MD Anderson Classification of Ovarian Serous Carcinoma MD Anderson Classification of Ovarian Serous Carcinoma Nuclei Mild-Moderate Atypia Marked Atypia Nuclear appearance Uniform Pleomorphic Nuclear size/shape < 3 : 1 variability >3 : 1 variability Nucleoli None to small Macro Chromatin Evenly dispersed Coarse Classification Atypia Mitoses / 10 hpf LGSC Mild to Moderate < 12 HGSC Marked 12 or more Classification Associated Borderline Tumor Progression Free Survival LGSC 60 % of cases longer HGSC 2 % of cases shorter Additional Advantages of 2-tier grading: More predictive than other grading systems Reproducible (Malpica 2007 AJSP) Eventually was validated by: p53/p16 immunophenotype Molecular pathogenesis Response to therapy Association with inherited mutations Used by 2014 W.H.O. 9




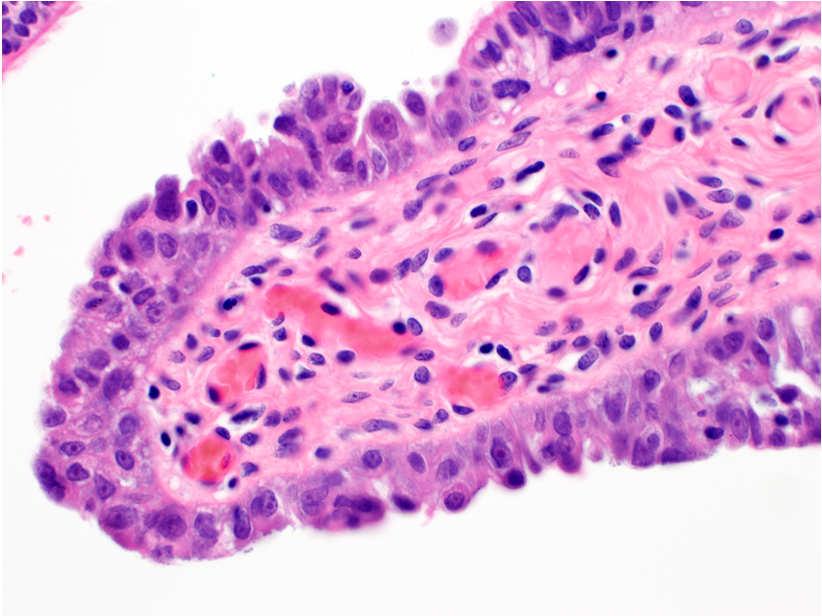
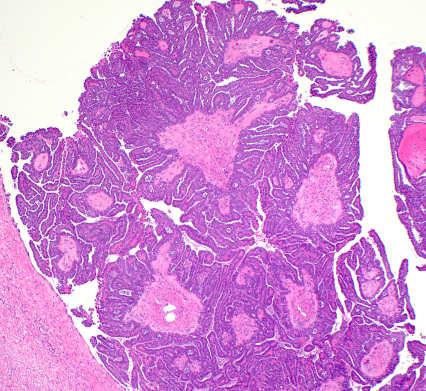
10 LGSC with Serous Borderline Tumor LGSC: Micropapillary Buds (avascular) <3:1 varying size/shape No mitoses No macronucleoli LGSC: Micropapillary Buds (avascular) <3:1 varying size/shape No mitoses No macronucleoli LGSC: Micropapillary Buds (avascular) 10


 + Buds")
11 <3:1 varying size/shape No mitoses No macronucleoli LGSC: Micropapillary Buds (avascular) LGSC: Papillary Branching (vascularized) <3:1 varying size/shape No mitoses No macronucleoli LGSC: Papillary Branching (vascularized) LGSC: Papillary Branching + Buds 11




12 LGSC: Papillary Branching + Buds <3:1 varying size/shape No mitoses No macronucleoli LGSC: Papillary Branching + Buds LGSC: Branching + Cribriform Pattern LGSC: Branching + Cribriform Pattern 12



13 LGSC: Cribriform Pattern LGSC: Columnar cells LGSC: Columnar cells LGSC with Necrosis Positive WT1 Excludes Endometrioid Tumor 13



14 Most LGSC Present at Advanced Stage Pelvic Lymph Node Metastasis Most LGSC Present at Advanced Stage Omental Involvement Most LGSC Present at Advanced Stage Lung Metastasis Immunophenotype LGSC Mullerian origin Extra-uterine serous differentiation Low grade serous carcinoma + PAX8, CK7 + WT1 Wild type p53, p16 14




15 Wild type p53 in LGSC LGSC Wild type p53 Wild type p16 Wild Type p53 and p16 staining Diagnostic Challenges Distinguishing LGSC versus HGSC 89 % Sensitivity for LGSC 93 % Specificity 98 % Negative predictive value Aberrant results exclude LGSC LGSC with: HGSC with: Focal mitotic activity Notable moderate atypia Rare severe atypia Only moderate nuclear atypia Abundant cytoplasm Architecture of borderline tumor or cystadenofibroma Micropapillary architecture 15



16 Diagnostic Challenges Distinguishing LGSC versus HGSC HGSC with only moderate atypia + rare mitoses LGSC with: HGSC with: Focal mitotic activity Notable moderate atypia Rare severe atypia Only moderate nuclear atypia Abundant cytoplasm Architecture of borderline tumor or cystadenofibroma Micropapillary architecture Resolve by: p53, p16 Immuno Staining HGSC with only moderate atypia + abundant cytoplasm HGSC with only moderate atypia + abundant cytoplasm 16




17 HGSC with only moderate atypia + abundant cytoplasm HGSC with uniform micropapillary architecture Aberrant p53 Aberrant p16 HGSC with uniform micropapillary architecture HGSC with uniform micropapillary architecture P53 17
 Tumor")
 Severe")
18 HGSC mimicking Serous Borderline Tumor (conventional type) HGSC mimicking Serous Borderline Tumor (micropapillary type) HGSC mimicking Serous Borderline Tumor (micropapillary type) HGSC mimicking Serous Borderline Tumor (micropapillary type) Severe Atypia High Mitotic rate 18



19 HGSC mimicking Serous Cystadenofibroma HGSC mimicking Serous Cystadenofibroma HGSC mimicking Serous Cystadenofibroma Severe Atypia High Mitotic rate LGSC has same survival as HGSC Ali et al Int J Gyn Path 19

20 Management Reasons to Distinguish HGSC vs LGSC Why should pathologists distinguish HGSC vs LGSC? HGSC Consider Neoadjuvant chemotherapy? Yes No LGSC Consider PARP inhibitor drug trials? Yes No Consider MEK inhibitor drug trials? No Yes Consider hormonal therapy? No Yes Consider genetic counseling referral for risk of hereditary syndrome? Yes Low priority Neoadjuvant Chemotherapy for Advanced Stage Ovarian Cancer Same survival as primary surgery But: Decreased Morbidity Decreased Mortality Decreased Cost Informs About Response of Selected Chemotherapy Agents 20


21 LGSC is Often Resistant to Platinum Chemotherapy LGSC is Often Resistant to Neoadjuvant Chemotherapy ~ 50 % have residual disease after first round Only ~ 5 % have any response Gershenson 2006 Obstet Gynecol Similar Findings: Schmeler 2008 Gynecol Oncol Gershenson 2009 Gynecol Oncol Schmeler 2011 Gynecol Oncol Ali 2013 Int J Gynecol Pathol Clinically Advanced Stage Pelvic Cancer LGSC is Second Most Common Tumor Type In Advanced Stage Ovarian Cancer Biopsy of Omental Tumor or Paracentesis of Malignant Ascites Mullerian Adenocarcinoma (positive PAX8, WT1) -Serous carcinoma, gynecologic origin -Ovarian serous carcinoma Sub-Type % of All Advanced Stage Cases HGSC 87.7 % LGSC 5.3 % Clear cell 4.5 % Endometrioid 2.5 % Mucinous 1.2% Kobel et al IJGP 21


22 Clinically Advanced Stage Pelvic Cancer Diagnostic Challenges Distinguishing LGSC versus HGSC Biopsy of Omental Tumor or Paracentesis of Malignant Ascites Morphology and immunostaining criteria not studied in : Core biopsy / FNA of peritoneal disease Cytology of malignant ascites HGSC LGSC Neoadjuvant Chemo Tx or Primary Surgery Then Adjuvant Chemo Tx Primary Surgery Then Adjuvant Chemo Tx Management Reasons to Distinguish HGSC vs LGSC Targeted Drugs in Clinical Trials for Pelvic Serous Carcinoma HGSC LGSC Consider Neoadjuvant chemotherapy? Yes No Consider PARP inhibitor drug trials? Yes No Consider MEK inhibitor drug trials? No Yes Consider hormonal therapy? No Yes For HGSC (BRCA mutation): Targeted inhibitors of PARP1 protein Olaparib Veliparib Rucaparib Consider genetic counseling referral for risk of hereditary syndrome? Yes Low priority For LGSC: Targeted inhibitor of MEK protein Selumetinib 22
23 Normal DNA Repair Mechanisms If BRCA mutation, PARP1 permits Cells to Still Proliferate Double Strand Breaks: Repair by BRCA1 / 2 proteins Double Strand Breaks: Repair by BRCA1 / 2 proteins Alteration #1: Germline mutation BRCA1 or 2 Single Strand Breaks: Single Strand Breaks: Repair by PARP1 protein Repair by PARP1 protein Targeted Cell Death Occurs if PARP1 Inhibitor plus BRCA1 or 2 Targeted Drugs in Clinical Trials for Pelvic Serous Carcinoma Double Strand Breaks: Repair by BRCA1 / 2 proteins Single Strand Breaks: Repair by PARP1 protein Alteration #1: Germline mutation BRCA1 or 2 Alteration #2: PARP1 Inhibitor Targeted Drug For HGSC (BRCA mutation): Targeted inhibitors of PARP1 protein Olaparib Veliparib Rucaparib 23
24 Management Reasons to Distinguish HGSC vs LGSC Normal MAPK Cell Signaling Cascade Drives Proliferation HGSC LGSC Consider Neoadjuvant chemotherapy? Yes No Consider PARP inhibitor drug trials? Yes No Consider MEK inhibitor drug trials? No Yes Consider hormonal therapy? No Yes Consider genetic counseling referral for risk of hereditary syndrome? Yes Low priority Mutations in MAPK Cell Signaling Cascade Promote Tumor Growth MEK Inhibitor Drugs Shut Down Tumor Cell Proliferation TUMOR TUMOR MEK Inhibitor Drug 24

25 Targeted Drugs in Clinical Trials for Pelvic Serous Carcinoma Management Reasons to Distinguish HGSC vs LGSC For LGSC: HGSC LGSC Targeted inhibitors of MEK protein in trials Selumetinib Trametinib Consider Neoadjuvant chemotherapy? Yes No Consider PARP inhibitor drug trials? Yes No Consider MEK inhibitor drug trials? No Yes Consider hormonal therapy? No Yes Consider genetic counseling referral for risk of hereditary syndrome? Yes Low priority Rationale for Hormonal Therapy in LGSC Management Reasons to Distinguish HGSC vs LGSC LGSC HGSC Estrogen Receptors 58 % 27 % Progesterone Receptors 43 % 17 % Wong 2007 Int J Gynecol Pathol Some survival benefit for LGSC with hormonal + chemo therapy Gershenson 2012 Gyn Oncol Schlumbrecht 2011 Cancer HGSC Consider Neoadjuvant chemotherapy? Yes No Consider PARP inhibitor drug trials? Yes No LGSC Consider MEK inhibitor drug trials? No Yes Consider hormonal therapy? No Yes Consider genetic counseling referral for risk of hereditary syndrome? Yes Low priority 25

26 Genetic mutations can be found in up to 1/4 of all pelvic cancers Most LGSC is not due to inherited gene mutation Unselected Pelvic Cancers Fanconi Anemia BRCA Pathway Genes Mismatch Repair Genes TP53 BRCA1, BRCA2 RAD51C, RAD51D BRIP1 BARD1 CHEK2 MRE11A NBN PALB2 RAD50 MLH1, MSH2, PMS2, MSH6 ~80% No significant rate of germline mutations Walsh 2011 PNAS Fujiwara 2012 AJSP Lakhani 2004 Clin Can Res Mavaddat 2011 Canc Epid Biom Prev Norquist 2013 Gyn Oncol No significant rate of cancer pedigree by personal/family history Vineyard 2011 Gyn Onc Walsh et al, 2011 PNAS Management Reasons to Distinguish HGSC vs LGSC Outline of Talk HGSC LGSC Changes to 2014 WHO system for pelvic serous tumors Consider Neoadjuvant chemotherapy? Yes No Consider PARP inhibitor drug trials? Yes No Consider MEK inhibitor drug trials? No Yes Consider hormonal therapy? No Yes High grade serous carcinoma versus low grade serous carcinoma New recommendations for assigning primary tumor origin Special issues with serous borderline tumors Consider genetic counseling referral for risk of hereditary syndrome? Yes Low priority 26


27 How do we assign origin of advanced stage HGSC How do we assign origin of advanced stage HGSC Traditional approaches: New paradigm: Any ovarian involvement = ovarian origin Dominant-mass = primary origin Fallopian tube STIC is the earliest stage of HGSC Problems No consensus or standardization Observer variation Problematic in neoadjuvant treated cases Biologic validity is untested Does not address the new paradigm of fallopian tube findings Setting % with STIC Incidental salpingectomy in general population < 1 % Prophylactic salpingectomy in BRCA mutation carrier < 8% Salpingectomy in stage I ovarian HGSC ~ 100 % Salpingectomy in advanced stage HGSC ~ 60 % How do we assign origin of advanced stage HGSC How do we assign origin of advanced stage HGSC New proposal from international consensus group: New proposal from international consensus group: Use the presence of STIC to define the tube as primary origin 27
28 How do we assign origin of advanced stage HGSC How do we assign origin of advanced stage HGSC New proposal from international consensus group: New proposal from international consensus group: Use the presence of STIC to define the tube as primary origin Use the presence of STIC to define the tube as primary origin Pelvic HGSC % of all cases Primary fallopian tube cancer 83 % Primary ovarian cancer 17 % Primary peritoneal cancer 0 % Singh 2015 Histopath Advantages Simple rules Reproducible Applicable in neoadjuvant treated cases In sync with new paradigm of pathogenesis How do we assign origin of advanced stage HGSC Diagnostic Criteria for STIC New proposal from international consensus group: Use the presence of STIC to define the tube as primary origin Unresolved issue: Uterine HGSC Gross specimen management Morphologic criteria Immunohistochemical criteria Diagnostic pitfalls Primary uterine HGSC Primary extra-uterine HGSC WT1 negative WT1 positive 28




 Automatic deeper levels not necessary if")
29 STIC in Microscopic Process Tubes via SEE-FIM Protocol 2 millimeter Fix in Formalin Several Hours Slice Fimbriae Parallel to Plicae Embed Entire Fimbriae 2-3 mm Intervals Entire tube if RRSO or if Cancer Case Process Tubes via SEE-FIM Protocol Diagnosis of STIC Entire Fimbriae: Ampullary Portion of Tube 1-2 cassettes usually 1 cassette Morphology Architecture Cytology Immunophenotype Aberrant p53 Increased Ki-67 (MIB-1) Automatic deeper levels not necessary if slices are 2-3 mm 29




30 Diagnosis of STIC Normal Fallopian Tube Mucosa Morphology Architecture Crowding, tufting, piling up, stratification Loss of polarity Loss of cilia Loss of peg cells Cytology High N/C ratio Moderate / severe nuclear atypia Mitoses +/- Macronucleoli IJGP. 2008; 27: 1 STIC STIC 30




31 STIC STIC Diagnostic Criteria Do Not Depend on BRCA mutation status Morphology Suspicious But Not Diagnostic of STIC Morphology Suspicious But Not Diagnostic of STIC 31
 Other markers, not as well studied: p16, HMGA2, Stathmin p53 Stain Pattern Strong + diffuse Completely absent")
 Interpretation Normal Increased Aberrant p53 in STIC STIC Aberrant")
32 Diagnosis of STIC Diagnosis of STIC Morphology Architecture Cytology Immunophenotype Aberrant p53 Increased Ki-67 (MIB-1) Other markers, not as well studied: p16, HMGA2, Stathmin p53 Stain Pattern Strong + diffuse Completely absent Variable strength Ki-67 Stain Pattern Same as adjacent normal mucosa Higher than adjacent normal mucosa (>10%) Interpretation Aberrant Aberrant Normal (wild type) Interpretation Normal Increased Aberrant p53 in STIC STIC Aberrant P53 Aberrant Ki 67 32








33 STIC STIC Aberrant P53 Aberrant Ki 67 Aberrant p53 Aberrant p16 Aberrant Ki67 Both Morphology and Immunostains Should Be Concordant for STIC Abnormal proliferations that fall short of criteria for STIC Vang IJGP 2012; 31:

")


 hyperplasia without")
34 Abnormal proliferations that fall short of criteria for STIC Alterations that are not clinically significant to report Outcome based evidence of clinical significance is lacking Prone to observer variation No consensus on nomenclature Secretory cell outgrowth (SCOUT) Serous tubal intraepithelial lesion Tubal intraepithelial lesion in transition Atypical mucosal proliferation No guidelines for management Current UCSF approach is observation only Alterations that are not clinically significant to report Alterations that are likely within normal spectrum of benign tubes Secretory cell outgrowth (SCOUT) p53 signature (normal morphology but p53 aberrant) hyperplasia without atypia (no formal terminology) 34
 Inflammatory Reactions Mucosal Endometriosis Mucosal Adenofibroma Submucosal Adenomatoid Tumor Metastatic Cancer Outline of Talk Special Issues with Serous Borderline")
35 Alterations that are likely within normal spectrum of benign tubes Differential Diagnosis of STIC hobnail growth without atypia (no formal terminology) Tangential Sectioning Artifact Metaplasias (transitional cell, mucinous) Inflammatory Reactions Mucosal Endometriosis Mucosal Adenofibroma Submucosal Adenomatoid Tumor Metastatic Cancer Outline of Talk Special Issues with Serous Borderline Tumors (SBT) Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous carcinoma New recommendations for assigning primary tumor origin Special issues with serous borderline tumors Chemotherapy indications LGSC in ovarian SBT LGSC in extra-ovarian sites 35
 Expansile invasion criteria LGSC versus")
 Destructive infiltrative growth into underlying tissue Solid nests / micropapillae within")
36 Special Issues with Serous Borderline Tumors (SBT) Chemotherapy indications LGSC in ovarian SBT LGSC in extra-ovarian sites LGSC in Ovarian Serous Borderline Tumor > 5 mm span of stromal invasion LGSC in ovarian SBT Stromal invasive criteria (> 5 mm) Expansile invasion criteria LGSC versus Micropapillary Type SBT Special Issues with Serous Borderline Tumors (SBT) Chemotherapy indications LGSC in ovarian SBT LGSC in extra-ovarian sites LGSC in extra-ovarian sites (so-called invasive implants) Destructive infiltrative growth into underlying tissue Solid nests / micropapillae within clefts in stroma 36

")


37 LGSC / Invasive Implant in Omentum LGSC / Invasive Implant in Omentum Special Issues with Serous Borderline Tumors (SBT) Special Issues with Serous Borderline Tumors (SBT) Most SBT exhibit hierarchical branching growth Micropapillary variant associated with extra-ovarian LGSC 37

38 Special Issues with Serous Borderline Tumors (SBT) Outline of Talk Micropapillary variant associated with extra-ovarian LGSC Non-hierarchical branching Broad papillae with finger-like projections Broad papillae lined by cribriform proliferation > 5 mm span in conventional type SBT Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous carcinoma New recommendations for assigning primary tumor origin Special issues with serous borderline tumors Valuable to report at Frozen Section diagnosis in order to assist surgeon in considering staging procedure 38
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas. W Glenn McCluggage Belfast, Northern Ireland
 The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
Current Concept in Ovarian Carcinoma: Pathology Perspectives
 Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
of 20 to 80 and subsequently declines [2].
![of 20 to 80 and subsequently declines [2].](/thumbs/80/81450506.jpg "of 20 to 80 and subsequently declines [2].") - - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
- - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Ovarian carcinoma classification. Robert A. Soslow, MD
 Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Low-grade serous neoplasia. Robert A. Soslow, MD
 Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Case 1. Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno
 Luca Mazzucchelli Istituto cantonale di patologia Locarno") Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
3/24/2017. Disclosure of Relevant Financial Relationships. Mixed Epithelial Endometrial Carcinoma. ISGyP Endometrial Cancer Project
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Interpretation of p53 Immunostains. P53 Mutations are Ubiquitous in High Grade Serous Carcinoma. Diffuse strong positive nuclear staining
 Stains for Tumor Classification p53 p16 WT1 HMGA2 P53 Mutations are Ubiquitous in High Grade Serous Carcinoma Source Ahmed et al Australian Ovarian Cancer Study Cancer Genome Atlas Research Network Cases
Stains for Tumor Classification p53 p16 WT1 HMGA2 P53 Mutations are Ubiquitous in High Grade Serous Carcinoma Source Ahmed et al Australian Ovarian Cancer Study Cancer Genome Atlas Research Network Cases
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
ACCME/Disclosures. Risk of Gyne Ca in HBOC. Molecular basis of HBOC. Hereditary Ovarian and Breast Cancer Syndrome
 Hereditary Ovarian and Breast Cancer Syndrome C. Blake Gilks, MD Dept of Pathology Vancouver General Hospital University of British Columbia Blake.gilks@vch.ca The USCAP requires that anyone in a position
Hereditary Ovarian and Breast Cancer Syndrome C. Blake Gilks, MD Dept of Pathology Vancouver General Hospital University of British Columbia Blake.gilks@vch.ca The USCAP requires that anyone in a position
Atypical Hyperplasia/EIN
 EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience
 Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Bibliography. Serous Tumors of the Ovary. Nomenclature
 Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
Mucinous Tumors of the Ovary Beirut, Lebanon. Anaís Malpica, M.D. Professor Department of Pathology
 Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
6/5/2010. Outline of Talk. Endometrial Alterations That Mimic Cancer & Vice Versa: Metaplastic / reactive changes. Problems in Biopsies/Curettages
 Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Ovarian Clear Cell Carcinoma
 Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
The Origin of Pelvic Low-Grade Serous Proliferative Lesions
 The Origin of Pelvic Low-Grade Serous Proliferative Lesions Ovarian Atypical Proliferative (Borderline) Serous Tumors, Noninvasive Implants and Endosalpingiosis Robert J. Kurman, M.D. Kurman RJ, Vang R,
The Origin of Pelvic Low-Grade Serous Proliferative Lesions Ovarian Atypical Proliferative (Borderline) Serous Tumors, Noninvasive Implants and Endosalpingiosis Robert J. Kurman, M.D. Kurman RJ, Vang R,
Gynecologic Cancers are many diseases. Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine. Speaker Disclosure:
 Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Proliferative Breast Disease: implications of core biopsy diagnosis. Proliferative Breast Disease
 Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Gynecologic Cancers are many diseases. Speaker Disclosure: Gynecologic Cancer Care in the Age of Precision Medicine. Controversies in Women s Health
 Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Controversies in Women s Health Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Controversies in Women s Health Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden
 and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden") What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
Bases biológicas del cáncer de ovario en el siglo XXI
 Bases biológicas del cáncer de ovario en el siglo XXI Iñigo Espinosa, M.D. Clínica Universidad de Navarra Epithelial Ovarian Tumors WHO 1973-2014 Serous Mucinous Endometrioid Clear cell Transitional Squamous
Bases biológicas del cáncer de ovario en el siglo XXI Iñigo Espinosa, M.D. Clínica Universidad de Navarra Epithelial Ovarian Tumors WHO 1973-2014 Serous Mucinous Endometrioid Clear cell Transitional Squamous
Disclosure. Gynecologic Cancer Genetics. Audience response. Audience response. What was the result? 47%
 Disclosure Cancer Genetics I have served as a moderator for an advisory board to Genentech Lee-may Chen, M.D. Professor Department of Obstetrics, Gynecology, & Reproductive Sciences UCSF Obstetrics and
Disclosure Cancer Genetics I have served as a moderator for an advisory board to Genentech Lee-may Chen, M.D. Professor Department of Obstetrics, Gynecology, & Reproductive Sciences UCSF Obstetrics and
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Adenocarcinoma of Mullerian origin: review of pathogenesis, molecular biology, and emerging treatment paradigms
 Cobb et al. Gynecologic Oncology Research and Practice (2015) 2:1 DOI 10.1186/s40661-015-0008-z REVIEW Adenocarcinoma of Mullerian origin: review of pathogenesis, molecular biology, and emerging treatment
Cobb et al. Gynecologic Oncology Research and Practice (2015) 2:1 DOI 10.1186/s40661-015-0008-z REVIEW Adenocarcinoma of Mullerian origin: review of pathogenesis, molecular biology, and emerging treatment
Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor
 of the Ovary Arising in an Atypical Proliferative Serous Tumor") Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor Robert J Kurman, M.D. Johns Hopkins University School of Medicine Case History A 53 year
Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor Robert J Kurman, M.D. Johns Hopkins University School of Medicine Case History A 53 year
Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center
 Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center Ovarian cancer is not a single disease Ovarian Epithelial Tumors: Histological Spectrum* Type Frequency Histology High-Grade
Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center Ovarian cancer is not a single disease Ovarian Epithelial Tumors: Histological Spectrum* Type Frequency Histology High-Grade
Page # 1. Endometrium. Cellular Components. Anatomical Regions. Management of SIL Thomas C. Wright, Jr. Most common diseases:
 Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Low-Grade Serous Ovarian Tumors Debra A. Bell, MD Mayo Clinic and Mayo Medical School Rochester, MN
 1 Low-Grade Serous Ovarian Tumors Debra A. Bell, MD Mayo Clinic and Mayo Medical School Rochester, MN It is very appropriate to discuss low-grade ovarian serous neoplasms in a symposium in honor of Dr.
1 Low-Grade Serous Ovarian Tumors Debra A. Bell, MD Mayo Clinic and Mayo Medical School Rochester, MN It is very appropriate to discuss low-grade ovarian serous neoplasms in a symposium in honor of Dr.
Endometrial hyperplasia vs. Intraepithelial neoplasia. Martin Chang, MD PhD FRCPC Pathology Update Friday November 9, 2012
 Endometrial hyperplasia vs. Intraepithelial neoplasia Martin Chang, MD PhD FRCPC Pathology Update Friday November 9, 2012 Disclosure No relevant financial conflicts to declare. Case 1 Gland crowding Gland
Endometrial hyperplasia vs. Intraepithelial neoplasia Martin Chang, MD PhD FRCPC Pathology Update Friday November 9, 2012 Disclosure No relevant financial conflicts to declare. Case 1 Gland crowding Gland
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS
 ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
Evaluation of BRCA1/2 and homologous recombination defects in ovarian cancer and impact on clinical outcomes
 Evaluation of BRCA1/2 and homologous recombination defects in ovarian cancer and impact on clinical outcomes Melinda S. Yates, PhD Department of Gynecologic Oncology & Reproductive Medicine University
Evaluation of BRCA1/2 and homologous recombination defects in ovarian cancer and impact on clinical outcomes Melinda S. Yates, PhD Department of Gynecologic Oncology & Reproductive Medicine University
Epithelial Ovarian Cancer 8/2/2013. Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer?
 Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer? Ann E. Smith Sehdev, MD Director, Center for Gynecologic Pathology Cascade Pathology, Portland, Oregon Ann E. Smith Sehdev has no
Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer? Ann E. Smith Sehdev, MD Director, Center for Gynecologic Pathology Cascade Pathology, Portland, Oregon Ann E. Smith Sehdev has no
Endosalpingiosis. Case report
 Case report Endosalpingiosis Michael D. Holmes, M.D. Howard S. Levin M.D. Department of Pathology Lester A. Ballard, Jr., M.D. Department of Gynecology Endosalpingiosis, a term referring to tuballike epithelium
Case report Endosalpingiosis Michael D. Holmes, M.D. Howard S. Levin M.D. Department of Pathology Lester A. Ballard, Jr., M.D. Department of Gynecology Endosalpingiosis, a term referring to tuballike epithelium
Important Recent Advances in Gynaecological Pathology
 Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
Key Recommendations. Gynecologic management of women with inherited risk of gynecologic cancer
 Gynecologic management of women with inherited risk of gynecologic cancer C. Bethan Powell MD Kaiser Permanente Northern California Gynecologic Oncology Program Lead, Kaiser Permanente Northern California
Gynecologic management of women with inherited risk of gynecologic cancer C. Bethan Powell MD Kaiser Permanente Northern California Gynecologic Oncology Program Lead, Kaiser Permanente Northern California
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Biology Response Controversies and Advances
 Biology Response Controversies and Advances in BRCA related ovarian cancer Lessons learned and future directions Michael Friedlander The Prince of Wales Hospital and Royal Hospital for Women Sydney BREAST-CANCER
Biology Response Controversies and Advances in BRCA related ovarian cancer Lessons learned and future directions Michael Friedlander The Prince of Wales Hospital and Royal Hospital for Women Sydney BREAST-CANCER
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
5/21/2018. Difficulty in Underdiagnosing Prostate Cancer. Diagnosis of Prostate Cancer. Evaluation of Prostate Cancer and Atypical on Needle Biopsy
 Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Both type I and type II tumors develop from extraovarian tissue that implants on the ovary. Both for LGSC and HGSC, the fallopian tube appears to be
 Recent studies have led to the development of a new paradigm for the pathogenesis and origin of EOC, based on a dualistic model of carcinogenesis that divides EOC into 2 broad categories designated types
Recent studies have led to the development of a new paradigm for the pathogenesis and origin of EOC, based on a dualistic model of carcinogenesis that divides EOC into 2 broad categories designated types
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
A Serous Borderline Tumor of the Fallopian Tube Detected Incidentally
 A Serous Borderline Tumor of the Fallopian Tube Detected Incidentally Imrana Tanvir, Ghania Ali, Haseeb Ahmed Khan and Ahmed Nasir Hanifi* Dept. of Histopathology, FMH College of Medicine & Dentistry,
A Serous Borderline Tumor of the Fallopian Tube Detected Incidentally Imrana Tanvir, Ghania Ali, Haseeb Ahmed Khan and Ahmed Nasir Hanifi* Dept. of Histopathology, FMH College of Medicine & Dentistry,
Demystifying Endometrial Hyperplasia
 Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus
 Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Macro- and microacinar proliferations of the prostate
 Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Mousa. Najat kayed &Renad Al-Awamleh. Nizar Alkhlaifat
 6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
Institute of Pathology First Faculty of Medicine Charles University. Ovary
 Ovary Barrett esophagus ph in vagina between 3.8 and 4.5 ph of stomach varies from 1-2 (hydrochloric acid) up to 4-5 BE probably results from upward migration of columnar cells from gastroesophageal junction
Ovary Barrett esophagus ph in vagina between 3.8 and 4.5 ph of stomach varies from 1-2 (hydrochloric acid) up to 4-5 BE probably results from upward migration of columnar cells from gastroesophageal junction
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Presenter: Yeh-Han Wang M.D.
 Korea-Taiwan-Japan Joint Meeting for Gynecological Pathology Mini-lecture Female Adnexal Tumor of Probable Wolffian Origin (FATWO) in Taiwan: A Small Case Series and Literature Review Presenter: Yeh-Han
Korea-Taiwan-Japan Joint Meeting for Gynecological Pathology Mini-lecture Female Adnexal Tumor of Probable Wolffian Origin (FATWO) in Taiwan: A Small Case Series and Literature Review Presenter: Yeh-Han
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis
 In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
Patologia Molecular del Carcinoma de Ovario
 Curso de Patologia Molecular XXVI Congreso Nacional de la SEAP Cadiz Patologia Molecular del Carcinoma de Ovario Jaime Prat Barcelona Ovarian Epithelial Tumors WHO 1999 and 2003 Serous Mucinous Endometrioid
Curso de Patologia Molecular XXVI Congreso Nacional de la SEAP Cadiz Patologia Molecular del Carcinoma de Ovario Jaime Prat Barcelona Ovarian Epithelial Tumors WHO 1999 and 2003 Serous Mucinous Endometrioid
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Pathobiology of ovarian carcinomas
 Chinese Journal of Cancer Review Mojgan Devouassoux-Shisheboran 1 and Catherine Genestie 2 Abstract Ovarian tumors comprise a heterogeneous group of lesions, displaying distinct tumor pathology and oncogenic
Chinese Journal of Cancer Review Mojgan Devouassoux-Shisheboran 1 and Catherine Genestie 2 Abstract Ovarian tumors comprise a heterogeneous group of lesions, displaying distinct tumor pathology and oncogenic
Background. Background. Background. Background 2/2/2015. Endometriosis-Associated Ovarian Cancer: Malignant Transformation of Endometriosis
 Endometriosis-Associated Ovarian Cancer: Malignant Transformation of Endometriosis I have no disclosures. Marcela G. del Carmen, MD, MPH Associate Professor Division of Gynecologic Oncology EOC is gynecologic
Endometriosis-Associated Ovarian Cancer: Malignant Transformation of Endometriosis I have no disclosures. Marcela G. del Carmen, MD, MPH Associate Professor Division of Gynecologic Oncology EOC is gynecologic
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
GYNplus: A Genetic Test for Hereditary Ovarian and/or Uterine Cancer
 GYNplus: A Genetic Test for Hereditary Ovarian and/or Uterine Cancer Causes of Hereditary Ovarian and Uterine Cancer uterine cancer ovarian cancer Sporadic 75-90% Sporadic 70-80% Hereditary, 5% Lynch syndrome
GYNplus: A Genetic Test for Hereditary Ovarian and/or Uterine Cancer Causes of Hereditary Ovarian and Uterine Cancer uterine cancer ovarian cancer Sporadic 75-90% Sporadic 70-80% Hereditary, 5% Lynch syndrome
Intravascular Endometrium Mimicking Vascular Invasion
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 A Papanicolau, G Lin Citation A Papanicolau, G Lin.. The Internet Journal of Pathology. 2010 Volume 12 Number 1. Abstract Intravascular endometrium
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 A Papanicolau, G Lin Citation A Papanicolau, G Lin.. The Internet Journal of Pathology. 2010 Volume 12 Number 1. Abstract Intravascular endometrium
Pathology of Ovarian Tumours. Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh
 AFMC Pune PDCC (Cytopathology) PGI Chandigarh") Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Case Report Ovarian Seromucinous Borderline Tumor and Clear Cell Carcinoma: An Unusual Combination
 Case Reports in Obstetrics and Gynecology Volume 2015, Article ID 690891, 5 pages http://dx.doi.org/10.1155/2015/690891 Case Report Ovarian Seromucinous Borderline Tumor and Clear Cell Carcinoma: An Unusual
Case Reports in Obstetrics and Gynecology Volume 2015, Article ID 690891, 5 pages http://dx.doi.org/10.1155/2015/690891 Case Report Ovarian Seromucinous Borderline Tumor and Clear Cell Carcinoma: An Unusual
Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY
 UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
Key Recommendations. Gynecologic management of women with inherited risk of gynecologic cancer. HBOC related genes. I have nothing to disclose
 Gynecologic management of women with inherited risk of gynecologic cancer C. Bethan Powell MD Kaiser Permanente Northern California Gynecologic Oncology Program I have nothing to disclose Key Recommendations
Gynecologic management of women with inherited risk of gynecologic cancer C. Bethan Powell MD Kaiser Permanente Northern California Gynecologic Oncology Program I have nothing to disclose Key Recommendations
6/3/2010. Outline of Talk. Lobular Breast Cancer: Definition of lobular differentiation. Common Problems in Diagnosing LCIS in Core Biopsies
 Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal cells
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal cells
Lynch Syndrome. Angie Strang, PGY2
 Lynch Syndrome Angie Strang, PGY2 Background Previously hereditary nonpolyposis colorectal cancer Autosomal dominant inherited cancer susceptibility syndrome Caused by defects in the mismatch repair system
Lynch Syndrome Angie Strang, PGY2 Background Previously hereditary nonpolyposis colorectal cancer Autosomal dominant inherited cancer susceptibility syndrome Caused by defects in the mismatch repair system
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
Hitting the High Points Gynecologic Oncology Review
 Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Pr
 Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
Pathology of the female genital tract
 Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis