Cellular Injury and Adaptation
|
|
|
- Brice Potter
- 5 years ago
- Views:
Transcription
1 General pathology
2 Introduction to pathology Literal translation of the word pathology is the study (logos) of suffering (Pathos). It is a discipline that bridges clinical practice and basic sciences. Pathology is concerned with the study of diseases in a scientific way. It comprises a wide base of scientific data and investigative techniques that are essential practice of modern medicine. Pathology in essence consists of two sets of related changes that are seen in various diseases: 1. Structural 2. Functional
3 The range of these changes is from those affecting sub-cellular organelles (molecular pathology) up to the alterations seen by the naked eye (gross pathology). Pathology is a dynamic science in that its contents are continuously subjected to changes, revisions and expansions. This is because there are always new scientific methods and findings that in turn shed more light on, add or modify an already established knowledge of various diseases. The ultimate goal of pathology is the identification of the cause or causes of disease (etiology) as well as the mechanisms (pathogenesis) that can eventuate in; 1. Disease prevention &/or 2. Successful therapy
4 Cellular Injury and Adaptation Each cell in the body is devoted to carry specific functions, which are dependent on the machinery and metabolic pathways present within the cell. This functional specificity is genetically determined. Normally the cells of the body are in equilibrium with the external environment. They maintain their internal machinery in a dynamically stable and steady state; this is called homeostasis i.e. the supply of raw material (substrates) and O2 are well coordinated with the production of the materials or jobs required.
5 In the presence of external disturbances that lend to upset the fine equilibrium, changes within the cells occur through internal regulatory mechanisms that counteract the external changes. In other words the cells are able to handle normal (physiological) and sometimes, abnormal (pathological) demands without get injured; to achieve this, a number of changes inside the cells occur that eventually lead to a new but altered steady state. These induced changes are referred to as adaptations.
6 The aim of adaptations is to preserve cell viability i.e. prevent cell injury. The increase in muscle mass (as in athletes or heavy mechanical workers) is a reflection of an increase in the size of individual muscle fibers so that when the muscle is subjected to excess workload, this will be shared by the thick and strong muscle fibers and thus each fiber is spared excess work and thus escapes injury. This protective adaptation is referred to as hypertrophy. Hypertrophy may be physiological as that of the uterus in pregnancy or pathological as that of the left ventricle in systemic hypertension.
7 Opposite to the above is the adaptive response atrophy in which there is a decrease in the size and function of cells and consequently the size of the organ or tissue containing them. If the limits of adaptive capability of the cells are exceeded (persistence of the injurious agent), or when no adaptive response is possible (sudden severe injurious agent that leaves no time for adaptive responses to take place), a sequence of events follows that are collectively known as cell injury

8
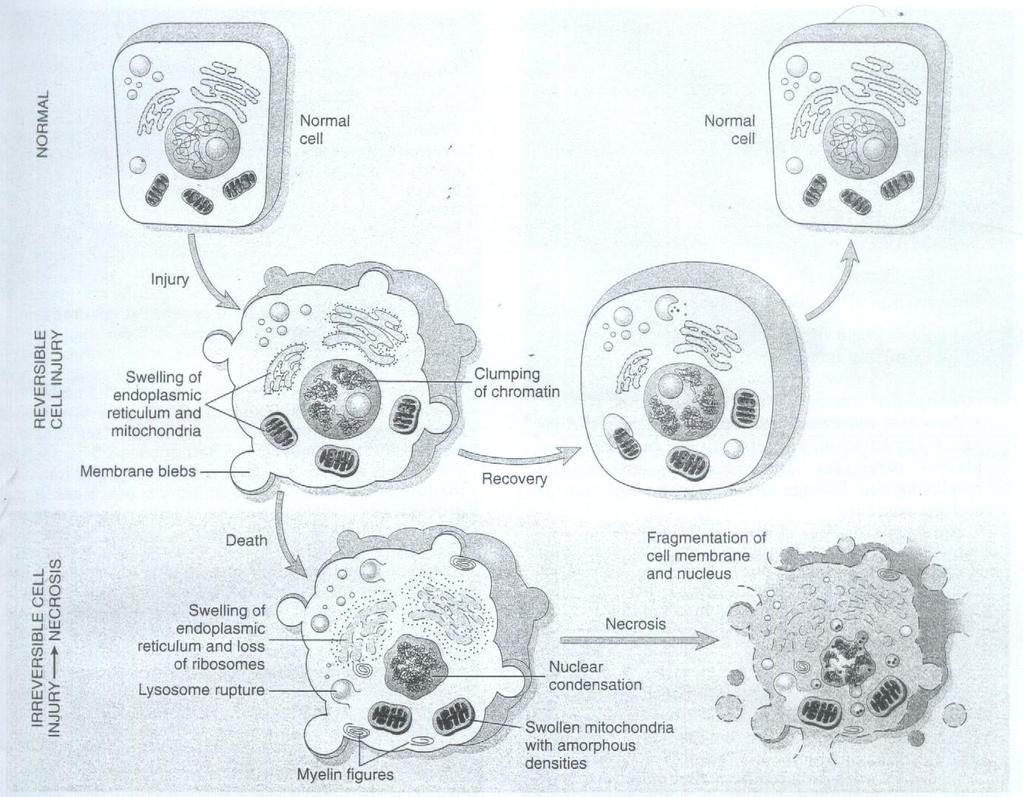
9 Cell injury is divided into 1. Reversible cell injury 2. Irreversible cell injury Reversible cell injury indicates that the changes will regress and disappear when the injurious agent is removed; the cells will return to normal, morphologically and functionally. Irreversible cell injury occurs when the injury persists or when it is severe from the outset. Here the cell alterations reach the point of no return and progression to cell death is inevitable.
10 Take an example: If the blood supply to a portion of the heart musculature is cut off for few minutes and then restored; the muscle cells will sustain reversible injury i.e. after restoration of the blood it will recover and function normally (as in angina pectoris). But if cessation of blood continues for 60 minutes and then restored the myocardial cells in this instance sustain irreversible injury that terminates invariably to death. So there is a spectrum cellular changes in response to injurious agent ranging from adaptation to cell death.
11
12 Classification (categorization) of injurious agents Injurious agents can be categorized as follows: 1. Oxygen deprivation (hypoxia) 2. Physical agents 3. Chemical agents 4. Infectious agents 5. Immunological reactions 6. Genetic derangement 7. Nutritional imbalances
13 Hypoxia This refers to a decrease in oxygen supply to the cells. It acts through interference with oxidative respiration of the cells. Hypoxia results from: A. Loss of blood supply (ischemia), which is the most common cause and occurs when arterial flow is interfered with by e.g. narrowing of the lumen of an artery by atherosclerosis, thrombi or emboli. B. Inadequate blood oxygenation due to for e.g. cardiac failure and/or respiratory failure. C. Decrease in the oxygen-carrying capacity of the blood e.g. anemia and carbon mono-oxide poisoning.
14 Depending on the severity & duration of hypoxia, the cells may show one of the following changes: 1. Adaptive atrophy 2. Injury( reversible or irreversible) For e.g. if the femoral artery is narrowed, the muscles of the leg shrink in size (atrophy). This adaptive response continues till there is a balance between the metabolic needs of the cells (low in this instance) and the available oxygen supply. More severe hypoxia (for e.g. when there is more severe narrowing or complete occlusion of the artery) will induce injury (reversible then irreversible that progresses to cell death).
15 Physical agents: that include -Mechanical trauma -Thermal injury; a. hyperthermia (extreme heat) b. hypothermia (deep cold) -Electrical injury; a. burn b. ventricular fibrillation -Radiation; a. direct effect b. indirect effect (free-radical formation)
16 - drugs. Chemical agents: that include - Simple chemicals such as glucose and salts in hypertonic concentrations - Oxygen in high concentration - Poisons such as arsenic or cyanide - Air pollutants - Insecticides - Occupational exposure e.g. to asbestos. - Social poisons such as alcohol and narcotic
17 Infectious agents: these include viruses, bacteria, fungi and parasites. Immunological reactions; these are primarily protective defense mechanisms against for e.g. infectious agents. However, sometimes they are harmful and injurious; this occurs in two situations: A. Hypersensitivity reactions (triggered for e.g. by drugs). B. Directed to self-antigens (autoimmune diseases).
18 Genetic derangement: exemplified by the wide range of hereditary diseases that range from those that are the result of gross chromosomal defects leading to severe congenital malformations e.g.down's syndrome,to those that are caused by a single amino acid substitution in the structure of hemoglobin that leading to the synthesis of abnormal Hb e.g. HbS in sickle cell anemia.
19 Nutritional imbalances - Deficiency: as of proteinscaloric malnutrition or vitamins deficiency etc. - Excess: as of lipids that leads to obesity with all its consequences including fatty change in cells and predisposition to atherosclerosis.
20 Mechanisms of Cell Injury The biochemical mechanisms responsible for cell injury are complex. There are however, a number of principles that are relevant to most forms of cell injury: 1-The cellular response to injurious stimuli depends on the type of injury, its duration, and its severity. Thus, small doses of a chemical toxin or brief periods of ischemia may induce reversible injury, whereas large doses of the same toxin or more prolonged ischemia might result either in instantaneous cell death or in slow, irreversible injury leading in time to cell death.
21 2. The consequences of cell injury depend on the type, state, and adaptability of the injured cell. The cell s nutritional and hormonal status and its metabolic needs are important in its response to injury 3- Cell injury results from functional and biochemical abnormalities in one or more of several essential cellular components
22 Cellular and biochemical sites of damage in cell injury
23 The most important targets of injurious stimuli are: (1) aerobic respiration involving mitochondrial oxidative phosphorylation and production of ATP; (2)the integrity of cell membranes, on which the ionic and osmotic homeostasis of the cell and its organelles depends; (3) protein synthesis; (4) The cytoskeleton; and (5) The integrity of the genetic apparatus of the cell
24 A. DEPLETION OF ATP ATP depletion and decreased ATP synthesis are frequently associated with both hypoxic and chemical (toxic) injury. High-energy phosphate in the form of ATP is required for many synthetic and degradative processes within the cell. These include membrane transport, protein synthesis, lipogenesis, and the deacylation reacylation reactions necessary for phospholipid turnover. *ATP is produced in two ways; The major pathway in mammalian cells is oxidative phosphorylation of adenosine diphosphate. The second is the glycolytic pathway, which can generate ATP in the absence of oxygen using glucose derived either from body fluids or from the hydrolysis of glycogen.
25 Functional and morphologic consequences of decreased intracellular ATP during cell injury :
26 1-The activity of the plasma membrane energydependent sodium pump is reduced. Failure of this active transport system, due to diminished ATP concentration and enhanced ATPase activity, causes sodium to accumulate intracellularly and potassium to diffuse out of the cell. The net gain of solute is accompanied by isosmotic gain of water, causing cell swelling, and dilation of the endoplasmic reticulum. 2-Cellular energy metabolism is altered. 3-Failure of the Ca2+ pump leads to influx of Ca2+, with damaging effects on numerous cellular components.
27 4 -Structural disruption of the protein synthetic apparatus With prolonged or worsening ATP depletion, reduction in protein synthesis occurs due to; a. Detachment of ribosomes from the rough endoplasmic reticulum b. Dissociation of polysomes into monosomes. 5 -In cells deprived of oxygen or glucose, proteins may become misfolded, and misfolded proteins trigger a cellular reaction called the unfolded protein response that may lead to cell injury and even death. Protein misfolding is also seen in cells exposed to stress, such as heat, and when proteins are damaged by enzymes (such as Ca2+-responsive enzymes) and free radicals.
28 B. mitochondrial damage: Mitochondria are important targets for virtually all types of injurious agent, including hypoxia & toxins. Mitochondria can be damage by: 1. Increase in cytoplasmic Ca++ 2. Oxidative stress 3. Breakdown of phospholipids by activated phospholipase.
29 Injury to mitochondria leads to increased permeability of its membrane that result in leakage from the mitochondria of H+ and cytochrome C. The former leads to loss of mitochondrial membrane potential, which is critical for mitochondrial oxidative phosphorylation thus leading to ATP depletion. Leakage of cytochrome C can trigger apoptotic cell death

30 Mitochondrial dysfunction in cell injury..
31 C. INFLUX OF INTRACELLULAR CALCIUM AND LOSS OF CALCIUM HOMEOSTASIS Calcium ions are important mediators of cell injury. Cytosolic free calcium is maintained at extremely low concentrations(<0.1 μmol) compared with extracellular levels of 1.3 mmol, and most intracellular calcium is sequestered in mitochondria and endoplasmic reticulum. Such gradients are modulated by membrane-associated, energy-dependent Ca2+, Mg2+-ATPases. Ischemia and certain toxins cause an early increase in cytosolic calcium concentration, owing to the net influx of Ca2+ across the plasma membrane and the release of Ca2+ from mitochondria and endoplasmic reticulum
32 Sustained rises in intracellular Ca2+ subsequently result from nonspecific increases in membrane permeability. Increased Ca2+ in turn activates a number of enzymes, with potential deleterious cellular effects. The enzymes known to be activated by calcium include ATPases, phospholipases, proteases and endonucleases. Increased intracellular Ca2+ levels also result in increased mitochondrial permeability and the induction of apoptosis. * Although cell injury often results in increased intracellular calcium and this in turn mediates a variety of deleterious effects, including cell death, loss of calcium homeostasis is not always a proximal event in irreversible cell injury

33 Sources and consequences of increased cytosolic calcium in cell injury
34 D-ACCUMULATION OF OXYGEN-DERIVED FREE RADICALS (OXIDATIVE STRESS) Cells generate energy by reducing molecular oxygen to water. During this process, small amounts of partially reduced reactive oxygen forms are produced as an unavoidable byproduct of mitochondrial respiration. Some of these forms are free radicals that can damage lipids, proteins, and nucleic acids. They are referred to as reactive oxygen species. Cells have defense systems to prevent injury caused by these products. An imbalance between free radical-generating and radical scavenging systems results in oxidative stress, a condition that has been associated with the cell injury seen in many pathologic conditions. Free radical mediated damage contributes to such varied processes as chemical and radiation injury, ischemia-reperfusion injury (induced by restoration of blood flow in ischemic tissue), cellular aging, and microbial killing by phagocytes.
35 Free radicals may be initiated within cells in several ways: a-absorption of radiant energy (e.g., ultraviolet light, x-rays). For example, ionizing radiation can hydrolyze water into hydroxyl (OH) and hydrogen (H) free radicals. b-enzymatic metabolism of exogenous chemicals or drugs (e.g., carbon tetrachloride [CCl4] can generate CCl3). c-the reduction-oxidation reactions that occur during normal metabolic processes. d-transition metals such as iron and copper donate or accept free electrons during intracellular reactions and catalyze free radical formation, as in the Fenton (H2O2 + Fe < Fe3+ + OH + OH-). e-nitric oxide (NO), an important chemical mediator generated by endothelial cells, macrophages, neurons, and other cell types can act as a free radical and can also be converted to highly reactive peroxynitrite anion (ONOO-) as well as NO2 and NO3-. The effects of these reactive species are wide-ranging, but three reactions are particularly relevant to cell injury: 1-Lipid peroxidation of membranes. 2-Oxidative modification of proteins. 3-Lesions in DNA. *In many pathologic processes, the final effects induced by free radicals depend on the net balance between free radical formation and termination
36 E. DEFECTS IN MEMBRANE PERMEABILITY Early loss of selective membrane permeability leading ultimately to overt membrane damage is a consistent feature of most forms of cell injury. Membrane damage may affect the mitochondria, the plasma membrane, and other cellular membranes. In ischemic cells, membrane defects may be the result of a series of events involving ATP depletion and calcium-modulated activation of phospholipases. The plasma membrane, however, can also be damaged directly by certain bacterial toxins, viral proteins, lytic complement components, and a variety of physical and chemical agents.

37 Several biochemical mechanisms may contribute to membrane : damage: 1- Mitochondrial dysfunction 2-Loss of membrane phospholipids 3- Cytoskeletal abnormalities. 4- Reactive oxygen species. 5- Lipid breakdown products
38 Reperfusion injury It has been noted that many of the effects of ischemic injury seem to occur not during the ischemic episode itself but when perfusion (blood flow) is reestablished to an area of tissue that has been ischemic. The re-flowed blood encounters cells with already disrupted membrane from the initial ischemia. Among other consequences of this membrane dysfunction that is particularly important in this context is impairment of calcium transport out of the cell and from organelles (such as mitochondria). The rise of intracellular Ca ++ causes activation of oxygendependent free radicals that lead eventually to cell damage. The necrosis of reperfusion injury appears to be of the apoptotic rather than of the conventional type

39 Factors influencing the severity of the cell injury: Types, duration & severity of the injurious agent. Types of the affected cells: cells differ in their susceptibility to the effects of the injurious agent; for e.g.
40 Reversible cell injury Ischemia is one of the commonest causes of the cell injury. - Ischemia leads to hypoxia. This in turn result in reduction of the available ATP. -The cell, as a result of hypoxia, switches over to anaerobic glycolysis (in an attempt to maintain energy supply). -The glycogen stores get depleted with an increase in the concentration of intracellular lactic acid(a byproduct of anaerobic glycolysis). -Lack of` ATP results in failure of sodium-potassium pump with resultant influx of sodium into the cell & this is accompanied by water (to insure isotonicity). The result is swelling of the cell. Additionally the lowering of intracellular ph (by lactic acid) interferes with the proper functions of enzymes
41 Examples of reversible cell injury 1. Acute cellular swelling (hydropic change, hydropic degeneration) This is an early change in many examples of reversible cell injury. The extra-fluid may be seen by light microscopy as in increase in size of the cell with pallor of the cytoplasm (cloudy swelling). With further water accumulation clear vacuoles are created within the cytoplasm (vacuolar degeneration) 2. Fatty change
42 Irreversible cell injury Mitochondrial damage is one of the most reliable early features of this type of injury. In irreversible injury the damage to cell membrane is most severe than in reversible injury, resulting in leakage of the cellular constitutes outside their normal confines. This also results in liberation and activation of lysosomal enzymes (proteinases, nucleases etc.), which are also normally bounded by membranes. These liberated and activated enzymes digest both cytoplasmic and nuclear components (autolysis). The end result is total cell necrosis, which is the morphological expression of cell death.
43
44 Cell Death There are two modes of cell death 1. Necrosis 2. Apoptosis Necrosis Necrosis is defined as the morphological changes that follow cell death in a living tissue or organ. Necrosis results from the degrading action of enzymes on irreversibly damaged cells with denaturation of cellular proteins. In necrosis, there are cytoplasmic as well as nuclear changes.
45 Cytoplasmic changes In the hematoxylin-eosin stain (H&C), the hematoxylin stains acidic materials (including the nucleus) blue where as eosin stains alkaline materials (including the cytoplasm) pink. The necrotic cell is more eosinophilic than viable cells (i.e. more intensely pinkish) this is due to: 1. Loss of cytoplasmic RNA (RNA is acidic so stains with hematoxylin bluish) i.e. loss of basophilia. 2. Increase binding of eosin (which is responsible for the pinkish color of the cytoplasm) to the denaturated proteins. The cell may have more glassy homogeneous appearance than normal cells; this is due to loss of the glycogen particles (which normally gives a granular appearance to cytoplasm)
46 Nuclear changes The earliest change is chromatin clumping, which is followed by one of two changes; 1. The nucleus may shrinks & transformed into small wrinkled basophilic mass (pyknosis), with time there is progressive disintegration of the chromatin with subsequent disappearance of the nucleus altogether (karylysis) or 2. The nucleus may break into many; clumps (karyorrhexis). In 1 to 2 days, the nucleus in a dead cell completely disappears
47 Types of cell necrosis 1. Coagulation (coagulative) necrosis. 2. Liquefaction (liquefactive) necrosis. 3. Fat necrosis 4. Caseous necrosis. 5. Gangrenous necrosis. 6. Fibrinoid necrosis. 1. Coagulation necrosis Results from sudden sever ischemia in such organs as the heart,kidney etc. Microscopically; the fine structural details of the affected tissue (and cells) are lost but their outlines are maintained. -The nucleus is lost The cytoplasm is converted into homogeneous deeply - eosinophilic and structureless material. - The basic tissue architecture is preserved for at least several - days -
48 2. Liquefaction necrosis Seen in two situations 1. Brain infarcts i.e. ischemic destruction of brain tissue. 2. Abscesses i.e. suppurative bacterial infection Liquefaction necrosis is characterized by complete digestion of dead cells by enzymes and thus the necrotic area is eventually liquefied i.e. converted into a cyst filled with debris and fluid
49 3. Fat necrosis This is a specific pattern of cell death seen in adipose tissue due to action of lipases. It is most commonly seen in acute pancreatitis. The released fatty acids from necrotic cells, complex with calcium to create calcium soaps. These are seen grossly as chalky white deposits. Fat necrosis can also be induced by mechanical trauma as in female breast (traumatic fat necrosis)
50 4. Caseous necrosis (caseation) This combines the features of coagulative & liquefactive necrosis. It is encountered principally in the center of tuberculous granuloma. The body is response to tuberculous infection is a specific form of chronic inflammation referred to as granulomatous inflammation. The morphological unit of this called granuloma. Grossly; the caseous material is soft, friable, whitish- gray cheesy material Microscopically; the area is surrounded by granulomatous inflammation. It has distinctive amorphous granular pinkish debris
51 5. Fibrinoid necrosis Is a special form of necrosis usually seen in immune reactions involving blood vessels. This pattern of necrosis is prominent when complexes of Ag & Ab are deposited in the walls of arteries. Deposit of these immune complexes together with fibrin that has leaked out of vessel, result in a bright pink and amorphous appearance in H & E stain, called fibrinoid (fibrin-like ) by pathologist
52 6. Gangrenous necrosis is not a distinctive pattern of cell death, the term is still commonly used in surgical clinical practice. It is usually applied to a limb, generally the lower leg, that has lost its blood supply and has undergone coagulation necrosis. When bacterial infection is superimposed, coagulative necrosis is modified by the liquefactive action of the bacteria and the attracted leukocytes (so-called wet gangrene; this term is used when the dominant is the liquefactive action, but when the dominant action is coagulative; the term is dry gangrene.
53 Apoptosis Necrosis may be regarded as a morphological expression of cellular cellular homicide where as apoptosis mean a cellular suicide. It is an energy dependent process for deletion of unwanted individual cells. CAUSES OF APOPTOSIS ; Apoptosis occurs normally both during development and throughout adulthood, and serves to eliminate unwanted, aged or potentially harmful cells. It is also a pathologic event when diseased cells become damaged beyond repair and are eliminated.
54 Apoptosis in Physiologic Situations: Death by apoptosis is a normal phenomenon that serves to eliminate cells that are no longer needed, and to maintain a steady number of various cell populations in tissues. It is important in the following physiologic situations: 1- The programmed destruction of cells during embryogenesis; including implantation, organogenesis, developmental involution, and metamorphosis. 2- Involution of hormone-dependent tissues upon hormone withdrawal; such as endometrial cell breakdown during the menstrual cycle, ovarian follicular atresia in menopause, the regression of the lactating breast after weaning, and prostatic atrophy after castration.
55 3-Cell loss in proliferating cell populations ; epithelial cells in intestinal crypts, so as to maintain a constant number (homeostasis). 4- Elimination of potentially harmful self-reactive lymphocytes, either before or after they have completed their maturation, so as to prevent reactions against one's own tissues. 5- Death of host cells that have served their useful purpose, such as neutrophils in an acute inflammatory response, and lymphocytes at the end of an immune response. In these situations cells undergo apoptosis because they are deprived of necessary survival signals, such as growth factors.
56 *Apoptosis in Pathologic Conditions Apoptosis eliminates cells that are injured beyond repair without eliciting a host reaction, thus limiting collateral tissue damage. Death by apoptosis is responsible for loss of cells in a variety of pathologic states: 1- DNA damage. Radiation, cytotoxic anticancer drugs, and hypoxia can damage DNA, either directly or via production of free radicals. If repair mechanisms cannot cope with the injury, the cell triggers intrinsic mechanisms that induce apoptosis. In these situations elimination of the cell may be a better alternative than risking mutations in the damaged DNA, which may result in malignant transformation. These injurious stimuli can cause apoptosis if the insult is mild, but larger doses of the same stimuli may result in necrotic cell death.
57 2- Accumulation of misfolded proteins; Improperly folded proteins may arise because of mutations in the genes encoding these proteins or because of extrinsic factors, such as damage caused by free radicals. 3- Cell death in certain infections; particularly viral infections, in which loss of infected cells is largely due to apoptosis that may be induced by the virus (as in adenovirus and HIV infections) or by the host immune response (as in viral hepatitis). 4- Pathologic atrophy in parenchymal organs after duct obstruction; such as occurs in the pancreas, parotid gland, and kidney
58 Morphology. The following morphologic features, some best seen with the electron microscope, characterize cells undergoing apoptosis: 1. Cell shrinkage. The cell is smaller in size; the cytoplasm is dense; and the organelles, though relatively normal, are more tightly packed. 2. Chromatin condensation. This is the most characteristic feature of apoptosis. The chromatin aggregates peripherally, under the nuclear membrane, into dense masses of various shapes and sizes. 3. Formation of cytoplasmic blebs and apoptotic bodies. The apoptotic cell first shows extensive surface blebbing, then undergoes fragmentation into membrane-bound apoptotic bodies composed of cytoplasm and tightly packed organelles, with or without nuclear fragments
59 4. Phagocytosis of apoptotic cells or cell bodies, usually by macrophages. The apoptotic bodies are rapidly ingested by phagocytes and degraded by the phagocyte's lysosomal enzymes. On histologic examination, in tissues stained with hematoxylin and eosin, the apoptotic cell appears as a round or oval mass of intensely eosinophilic cytoplasm with fragments of dense nuclear chromatin. Because the cell shrinkage and formation of apoptotic bodies are rapid and the pieces are quickly phagocytosed, considerable apoptosis may occur in tissues before it becomes apparent in histologic sections. In addition, apoptosis in contrast to necrosis does not elicit inflammation, making it more difficult to detect histologically.

60
61 Intracellular accumulations Under certain situations, cells may accumulate abnormal amount of various substances. The accumulated substance fails into one of three categories: 1. A normal cellular constituent accumulated in excess e.g. lipid, protein and CHO 2. An abnormal substance that is a product of abnormal metabolic pathway. 3. A pigment i.e. a colored substance. The accumulated substance may be harmless or severely toxic to the cell. The site of accumulation is either nuclear or cytoplasmic. Within the cytoplasm,the accumulated substance is most frequently within the lysosomes
62 The mechanisms of abnormal intracellular accumulation are many but can be divided into four general types : 1. Abnormal metabolism: a normal substance is produced at a normal rate but the rate of its removal is inadequate e.g. fatty change of the liver. 2. Genetic mutations producing changes in protein folding and transport. A protein is composed of amino acids linked in specific sequences by peptide bonds and coiled and folded into complex globular or fibrous structures. A change in this configuration may result in interference with its transport so that it gets accumulated at the site of production.
63 3. A normal or abnormal substance is produced but cannot be metabolized. This is most commonly due to lack of an enzyme, which is genetically determined (inborn error of metabolism). Such a deficiency of enzymes blocks a specific metabolic pathway resulting in the accumulation unused metabolite (s) proximal to the block. The resulting diseases are, referred to as storage diseases. 4. An abnormally exogenous substance is deposited and accumulates because the cell is incapable to get rid of it (through enzymatic degradation or to transport it to the outside)e.g. carbon particles in anthracosis and silica particles in silicosis.
64 Accumulation of lipid Fatty changes This refer to abnormal accumulation of fat of triglyceride type within parenchymal cells. It is an example of reversible (non- lethal) cell injury and is often seen in the liver because of the central role of this organ in fat metabolism. Free fatty acids are transported to the liver from two sources 1. adipose tissue 2. ingested food In the liver these fatty acids are esterified to triglycerides. Release of triglycerides from the liver required their association with carrier proteins (apoproteins). Such complexes circulate in the blood as lipoproteins.
65 Excess accumulation of triglycerides within the liver (fatty change) may result from defects in any one of the above steps from entry to, till their exit from the hepatocytes. 1. Alcohol may induce a number of such defects through alterations in mitochondrial and microsomal function. 2. CCl 4 and protein malnutrition act by decreasing apoproteins synthesis. 3. Anoxia (hypoxia) inhibits fatty acid oxidation. 4. Starvation increases fatty acid mobilization from peripheral stores.
66 Gross features In the liver mild fatty changes shows no gross changes, but with progressive accumulation, the organ enlarges and become increasingly yellow, soft & greasy to touch. Microscopic features In the early stages there are small fat vacuoles around the nucleus. With progression the vacuoles fuse together creating large clear space that displaces the nucleus to the periphery. *Fatty change may also be seen within myocardial cells e.g. in ischemia and myocarditis. The latter may be seen as a complication of diphtheria. The above examples refer to accumulations of triglycerides
67 Accumulations may involve cholesterol and its esters within 1. Smooth muscle cells and macrophages that are located within the intima of arteries in atherosclerosis. 2. Macrophages in the acquired and hereditary hyperlipidemias; in such cases the accumulations are usually seen within the subcutaneous connective tissues of the skin and in tendons producing masses known as xanthomas.
68 Protein accumulation This occurs principally in the; 1.Epithelial cells of proximal convoluted renal tubules.e.g.in cases of proteinuria. 2. plasma cells, these cells are actively engaged in immunoglobulin synthesis (antibody-forming ) and may become overloaded with its own products.
69 GLYCOGEN Glycogen is a readily available energy source stored in the cytoplasm of healthy cells. Excessive intracellular deposits of glycogen are seen in patients with an abnormality in either glucose or glycogen metabolism. Whatever the clinical setting, the glycogen masses appear as clear vacuoles within the cytoplasm. Diabetes mellitus is the prime example of a disorder of glucose metabolism. In this disease glycogen is found in renal tubular epithelial cells, as well as within liver cells, β cells of the islets of Langerhans, and heart muscle cells.
70 Glycogen accumulates within the cells in a group of related genetic disorders that are collectively referred to as the glycogen storage diseases, or glycogenoses. In these diseases enzymatic defects in the synthesis or breakdown of glycogen result in massive accumulation, causing cell injury and cell death. PIGMENTS Pigments are colored substances, some of which are normal constituents of cells (e.g., melanin), whereas others are abnormal and accumulate in cells only under special circumstances. Pigments can be exogenous, coming from outside the body, or endogenous, synthesized within the body itself
71 Exogenous Pigments The most common exogenous pigment is carbon (coal dust). When inhaled it is picked up by macrophages within the alveoli and is then transported through lymphatic channels to the regional lymph nodes in the tracheobronchial region. Accumulations of this pigment blacken the tissues of the lungs (anthracosis) and the involved lymph nodes. In coal miners the aggregates of carbon dust may induce a fibroblastic reaction or even emphysema and thus cause a serious lung disease known as coal worker's pneumoconiosis.
72 Tattooing is a form of localized, exogenous pigmentation of the skin. The pigments inoculated are phagocytosed by dermal macrophages, in which they reside for the remainder of the life of the embellished (sometimes with embarrassing consequences for the bearer of the tattoo!). The pigments do not usually evoke any inflammatory response.
73 Endogenous Pigments A- Lipofuscin is an insoluble pigment, also known as lipochrome or wear-and-tear pigment. Lipofuscin is composed of polymers of lipids and phospholipids in complex with protein, suggesting that it is derived through lipid peroxidation of polyunsaturated lipids of subcellular membranes. Lipofuscin is not injurious to the cell or its functions. Its importance lies in its being a telltale sign of free radical injury and lipid peroxidation.
74 The term is derived from the Latin (fuscus, brown), referring to brown lipid. In tissue sections it appears as a yellowbrown, finely granular cytoplasmic, often perinuclear, pigment. It is seen in cells undergoing slow, regressive changes and is particularly prominent in the liver and heart of aging patients or patients with severe malnutrition and cancer cachexia.
75 B- Melanin, derived from the Greek (melas, black), is an endogenous, non-hemoglobin-derived, brown-black pigment. It formed when the enzyme tyrosinase catalyzes the oxidation of tyrosine to dihydroxyphenylalanine in melanocytes. For practical purposes melanin is the only endogenous brown-black pigment.
76 The only other that could be considered in this category is homogentisic acid, a black pigment that occurs in patients with alkaptonuria, a rare metabolic disease. Here the pigment is deposited in the skin, connective tissue, and cartilage, and the pigmentation is known as ochronosis
77 3-Hemosiderin is a hemoglobin-derived, golden yellow-to-brown, granular or crystalline pigment that serves as one of the major storage forms of iron. Iron is normally carried by specific transport proteins, transferrins. In cells, it is stored in association with a protein, apoferritin, to form ferritin micelles. Ferritin is a constituent of most cell types. When there is a local or systemic excess of iron, ferritin forms hemosiderin granules, which are easily seen with the light microscope.
78 Hemosiderin pigment represents aggregates of ferritin micelles. Under normal conditions small amounts of hemosiderin can be seen in the mononuclear phagocytes of the bone marrow, spleen, and liver, which are actively engaged in red cell breakdown. Local or systemic excesses of iron cause hemosiderin to accumulate within cells. Local excesses result from hemorrhages in tissues. The best example of localized hemosiderosis is the common bruise.
79 Extravasated red blood cells at the site of injury are phagocytosed over several days by macrophages, which break down the hemoglobin and recover the iron. After removal of iron, the heme moiety is converted first to biliverdin ( green bile ) and then to bilirubin ( red bile ). In parallel, the iron released from heme is incorporated into ferritin and eventually hemosiderin. These conversions account for the often dramatic play of colors seen in a healing bruise, which typically changes from red-blue to green-blue to golden-yellow before it is resolved.
80 When there is systemic overload of iron hemosiderin may be deposited in many organs and tissues, a condition called hemosiderosis. The main causes of hemosiderosis are (1) increased absorption of dietary iron, (2) hemolytic anemias, in which abnormal quantities of iron are released from erythrocytes, and (3) repeated blood transfusions because the transfused red cells constitute an exogenous load of iron.
81 Morphology Iron pigment appears as a coarse, golden, granular pigment lying within the cell's cytoplasm. When the underlying cause is the localized breakdown of red cells, the hemosiderin is found initially in the phagocytes in the area. hemosiderosis it is found at first in the In systemic mononuclear phagocytes of the liver, bone marrow, spleen, and lymph nodes and in scattered macrophages throughout other organs such as the skin, pancreas, and kidneys
82 With progressive accumulation, parenchymal cells throughout the body (principally in the liver, pancreas, heart, and endocrine organs) become pigmented. In most instances of systemic hemosiderosis the pigment does not damage the parenchymal cells or impair organ function. The more extreme accumulation of iron, however, in an inherited disease called hemochromatosis is associated with liver, heart, and pancreatic damage, resulting in liver fibrosis, heart failure, and diabetes mellitus.
83 4- Bilirubin is the normal major pigment found in bile. It is derived from hemoglobin but contains no iron. Its normal formation and excretion are vital to health, and jaundice is a common clinical disorder caused by excesses of this pigment within cells and tissues.
84 Degenerative changes Pathological calcification Calcification is refers to abnormal deposition of calcium salts. There are two forms of calcification: 1. Dystrophic calcification; refers to calcium deposition in nonviable or dying tissue that occurs despite occurs normal calcium levels and the absence of any the absence of any derangement of calcium metabolism. 2. Metastatic calcification ;signifies deposition of calcium in viable tissue, almost always a reflection of some derangement of Calcium metabolism that leads to hypercalcemia.
85 Dystrophic calcification is noted in 1. Areas of necrosis (whether coagulative, caseous, liquefactive, or fat necrosis 2. Advanced atherosclerosis. 3. Damaged or- aging heart valves. The calcification is seen grossly as fine, white granules or clumps giving gritty feeling. Microscopically (with H & E stains) it appears as basophilic (bluish), amorphous granules that may coalesce to form larger clumps.
86 Sometimes calcium deposition occurs in a round lamellar fashion at a nidus of necrotic cells. These structures are called psammoma bodies. This is seen in some tumors such as carcinomas of the thyroid & ovary as well as in some meningioma. Metastatic calcification is seen in cases of hypercalcemia of any cause. It principally affects blood vessels, kidney, lungs and gastric mucosa
87 The four major cause of hypercalcemia are; a. Increased secretions of parathyroid hormone. b. Destruction of bone due to the effects of accelerated turnover. (e.g. Paget disease),immobilization, or tumors (increase bone metabolism associated with multiple myeloma, leukemia,or diffuse skeletal metastases ). c. Vitamin D-related disorders including vitamin D intoxication & sarcoidosis (in which macrophages activate a vitamin D precursor). d. Renal failure; in which phosphate retention leads to secondary hyperparathyroidism.
88 Hyaline change: This refers to intra- or extra-cellular homogeneous, pinkish alteration in sections stained with H & E. Examples of intracellular hyaline change include: 1. Hyaline droplets within renal tubular epithelium in cases of protein urea. 2. Russell bodies in plasma cells 3. Viral inclusions (nuclear or cytoplasmic) 4. Alcoholic hyaline in liver cells (Mallory bodies). Extracellular hyalinization may be encountered in 1. Collagen in old scar. 2. Hyalinization of arteriolar walls associated with hypertension and diabetes. 3. Amyloid deposition.
89 CELLULAR AGING Cellular aging is the result of a progressive decline in the proliferative capacity and life span of cells and the effects of continuous exposure to exogenous factors that cause accumulation of cellular and molecular damage. Several mechanisms are known or suspected to be responsible for cellular aging: 1-DNA damage. Cellular aging is associated with increasing DNA damage, which may happen during normal DNA replication and can be enhanced by free radicals. Although most DNA damage is repaired by DNA repair enzymes, some persists and accumulates as cells age.
90 2-Decreased cellular replication. All normal cells have a limited capacity for replication, and after a fixed number of divisions cells become arrested in a terminally non dividing state, known as replicative senescence (Replicative senescence: reduced capacity of cells to divide because of decreasing amounts of telomerase and progressive shortening of chromosomal ends (telomeres)). Aging is associated with progressive replicative senescence of cells. Cells from children have the capacity to undergo more rounds of replication than do cells from older people. In contrast, cells from patients with Werner syndrome, a rare disease characterized by premature aging, have a markedly reduced in vitro life span.
91 Note; Telomeres are short repeated sequences of DNA present at the linear ends of chromosomes that are important for ensuring the complete replication of chromosome ends and for protecting the ends from fusion and degradation. 3-Accumulation of metabolic damage. Cellular life span is also determined by a balance between damage resulting from metabolic events occurring within the cell and counteracting molecular responses that can repair the damage.

92
[General Pathology] Introduction to Pathology
![[General Pathology] Introduction to Pathology](/thumbs/73/69585662.jpg "[General Pathology] Introduction to Pathology") Introduction to Pathology Pathology: Literally translated, pathology is the study (logos) of disease (pathos, suffering). It involves the investigation of the causes of disease and the associated changes
Introduction to Pathology Pathology: Literally translated, pathology is the study (logos) of disease (pathos, suffering). It involves the investigation of the causes of disease and the associated changes
Chemical and Biochemical Mechanism Of Cell Injury.
 Chemical and Biochemical Mechanism Of Cell Injury. Professor Dr. M. Tariq Javed Dept. of Pathology Faculty of Vet. Science The University Of Agriculture Faisalabad Cell Injury When the cell is exposed
Chemical and Biochemical Mechanism Of Cell Injury. Professor Dr. M. Tariq Javed Dept. of Pathology Faculty of Vet. Science The University Of Agriculture Faisalabad Cell Injury When the cell is exposed
PREPARED BY P.DHARANI PRASAD II YEAR B.PHARM II SEM SUB:PATHOPHYSIOLOGY
 CELL INJURY UNIT I PREPARED BY P.DHARANI PRASAD II YEAR B.PHARM II SEM SUB:PATHOPHYSIOLOGY DETECTION OF CELLULAR CHANGES AFTER INJURY BY: LIGHT MICROSCOPY OR GROSS EXAMINATION DETECT CHANGES HOURS TO DAYS
CELL INJURY UNIT I PREPARED BY P.DHARANI PRASAD II YEAR B.PHARM II SEM SUB:PATHOPHYSIOLOGY DETECTION OF CELLULAR CHANGES AFTER INJURY BY: LIGHT MICROSCOPY OR GROSS EXAMINATION DETECT CHANGES HOURS TO DAYS
Cellular responses to stress
 Cellular responses to stress (Adaptations, injury and death) (2 of 5) Most injurious stimuli are grouped into: Oxygen deprivation Chemical agents Infectious agents Immunologic reactions Genetic factors
Cellular responses to stress (Adaptations, injury and death) (2 of 5) Most injurious stimuli are grouped into: Oxygen deprivation Chemical agents Infectious agents Immunologic reactions Genetic factors
Mechanisms of Cell Injury
 Causes of Cell Injury 1- oxygen deprivation (anoxia) 2- physical agents 3- chemical agents 4- infections agents 5- immunologic reactions 6- genetic defects 7- nutritional imbalances Mechanisms of Cell
Causes of Cell Injury 1- oxygen deprivation (anoxia) 2- physical agents 3- chemical agents 4- infections agents 5- immunologic reactions 6- genetic defects 7- nutritional imbalances Mechanisms of Cell
Cell Adaptation, Cell Injury and Cell Death
 Cell Adaptation, Cell Injury and Cell Death Pathology:- is the study of structural and functional abnormalities that are expressed as diseases of organs and systems. Modern pathology, proposed that injury
Cell Adaptation, Cell Injury and Cell Death Pathology:- is the study of structural and functional abnormalities that are expressed as diseases of organs and systems. Modern pathology, proposed that injury
Cell Injury MECHANISMS OF CELL INJURY
 Cell Injury MECHANISMS OF CELL INJURY The cellular response to injurious stimuli depends on the following factors: Type of injury, Its duration, and Its severity. Thus, low doses of toxins or a brief duration
Cell Injury MECHANISMS OF CELL INJURY The cellular response to injurious stimuli depends on the following factors: Type of injury, Its duration, and Its severity. Thus, low doses of toxins or a brief duration
number Done by Corrected by Doctor Heyam Awad
 number 4 Done by Waseem Abu Obeida Corrected by Saad Al-Hayek Doctor Heyam Awad Cell injury -in the previous lectures we talked about the causes (etiology) and the mechanism (pathogenesis) of cell injury.
number 4 Done by Waseem Abu Obeida Corrected by Saad Al-Hayek Doctor Heyam Awad Cell injury -in the previous lectures we talked about the causes (etiology) and the mechanism (pathogenesis) of cell injury.
shehab Moh Tarek ... ManarHajeer
 3 shehab Moh Tarek... ManarHajeer In the previous lecture we discussed the accumulation of oxygen- derived free radicals as a mechanism of cell injury, we covered their production and their pathologic
3 shehab Moh Tarek... ManarHajeer In the previous lecture we discussed the accumulation of oxygen- derived free radicals as a mechanism of cell injury, we covered their production and their pathologic
Cellular Injury. Intracellular degeneration. By Dr. Hemn Hassan Othman PhD, Pathology Fall /20/2018 1
 Cellular Injury Intracellular degeneration By Dr. Hemn Hassan Othman PhD, Pathology Fall 2018 10/20/2018 1 Types of cell injury Cell injury is divided into: 1. Reversible cell injury 2. Irreversible cell
Cellular Injury Intracellular degeneration By Dr. Hemn Hassan Othman PhD, Pathology Fall 2018 10/20/2018 1 Types of cell injury Cell injury is divided into: 1. Reversible cell injury 2. Irreversible cell
Introduction to pathology lecture 5/ Cell injury apoptosis. Dr H Awad 2017/18
 Introduction to pathology lecture 5/ Cell injury apoptosis Dr H Awad 2017/18 Apoptosis = programmed cell death = cell suicide= individual cell death Apoptosis cell death induced by a tightly regulated
Introduction to pathology lecture 5/ Cell injury apoptosis Dr H Awad 2017/18 Apoptosis = programmed cell death = cell suicide= individual cell death Apoptosis cell death induced by a tightly regulated
Chapter 1 CELL INJURY CELL DEATH CELL ADAPTATIONS. M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM University.
 Chapter 1 CELL INJURY CELL DEATH CELL ADAPTATIONS M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM University. CONCEPTS IN CELL INJURY The clinical signs and symptoms are several
Chapter 1 CELL INJURY CELL DEATH CELL ADAPTATIONS M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM University. CONCEPTS IN CELL INJURY The clinical signs and symptoms are several
SECTION 2 CELL INJURY
 Adapted myocyte Normal myocyte Reversibly-injured myocyte SECTION 2 CELL INJURY Cell death 5/4/2014 1 5/4/2014 2 Reversible Degeneration Irreversible Cellular Swelling Fatty Change Hyaline Change Amyloid
Adapted myocyte Normal myocyte Reversibly-injured myocyte SECTION 2 CELL INJURY Cell death 5/4/2014 1 5/4/2014 2 Reversible Degeneration Irreversible Cellular Swelling Fatty Change Hyaline Change Amyloid
INTRODUCTION TO HEALTH AND DISEASE BLOCK
 MBBS 1 st Yr. Lecture Dr. Annie Cheung September 25, 2002, 8:30AM 9:30 AM LT1, G/F, Academic and Administration Block Faculty of Medicine Building INTRODUCTION TO HEALTH AND DISEASE BLOCK CELL INJURY AND
MBBS 1 st Yr. Lecture Dr. Annie Cheung September 25, 2002, 8:30AM 9:30 AM LT1, G/F, Academic and Administration Block Faculty of Medicine Building INTRODUCTION TO HEALTH AND DISEASE BLOCK CELL INJURY AND
The basis of Disease
 General Curriculum The basis of Disease ZHOU REN 周韧 Prof., M.D., Ph.D. Institute of Pathology & Forensic Medicine Department of Pathology & Patho-physiology Zhenjiang University Judicial Evidence & Evaluation
General Curriculum The basis of Disease ZHOU REN 周韧 Prof., M.D., Ph.D. Institute of Pathology & Forensic Medicine Department of Pathology & Patho-physiology Zhenjiang University Judicial Evidence & Evaluation
Cell injury, adaptation and death. Unite one Second Lab.
 Cell injury, adaptation and death Unite one Second Lab. The two lung abscesses seen here are examples of liquefactive necrosis in which there is a liquid center in an area of tissue injury. One abscess
Cell injury, adaptation and death Unite one Second Lab. The two lung abscesses seen here are examples of liquefactive necrosis in which there is a liquid center in an area of tissue injury. One abscess
Histopathology: Cell necrosis and cytoplasmic accumulations
 Histopathology: Cell necrosis and cytoplasmic accumulations These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Cell necrosis and cytoplasmic accumulations These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Types of insult - hypoxia
 Introduction This presentation will be a guide to cell injury and cell death outline causes and pathogenesis of cell injury/death describe the morphological changes of cell injury/death Describe the process
Introduction This presentation will be a guide to cell injury and cell death outline causes and pathogenesis of cell injury/death describe the morphological changes of cell injury/death Describe the process
CELL INJURY. Severity of Cell Injury
 GENERAL PATHOLOGY LECTURE - 3 DR. M. TARIQ JAVED Professor Department of Pathology, Faculty of Veterinary Science, University of Agriculture, Faisalabad, Pakistan. 9/11/2009 1 CELL INJURY No adaptive response
GENERAL PATHOLOGY LECTURE - 3 DR. M. TARIQ JAVED Professor Department of Pathology, Faculty of Veterinary Science, University of Agriculture, Faisalabad, Pakistan. 9/11/2009 1 CELL INJURY No adaptive response
Cellular Injury, Necrosis, Apoptosis
 Cellular Injury, Necrosis, Apoptosis Cell injury results when cells are stressed and can no longer adapt Injury may progress through a reversible stage Reversible Cell Injury Reduced oxidative phosphorylation
Cellular Injury, Necrosis, Apoptosis Cell injury results when cells are stressed and can no longer adapt Injury may progress through a reversible stage Reversible Cell Injury Reduced oxidative phosphorylation
Hemosiderin. Livia Vida 2018
 Hemosiderin Livia Vida 2018 Questions Histochemical caracteristics of the different pigments. Exogenous pigments. Hemoglobinogenic pigments. Causes and forms of jaundice. Hemoglobinogenic pigments. Pathological
Hemosiderin Livia Vida 2018 Questions Histochemical caracteristics of the different pigments. Exogenous pigments. Hemoglobinogenic pigments. Causes and forms of jaundice. Hemoglobinogenic pigments. Pathological
Necrosis is death of cells and tissues in the living animal. Focal/ Multifocal necrosis- terms used for one
 Necrosis Necrosis Necrosis is death of cells and tissues in the living animal. Focal/ Multifocal necrosis- terms used for one or more, small, clearly defined areas of necrosis. Diffuse necrosis- term used
Necrosis Necrosis Necrosis is death of cells and tissues in the living animal. Focal/ Multifocal necrosis- terms used for one or more, small, clearly defined areas of necrosis. Diffuse necrosis- term used
Extracellular degeneration
 Extracellular degeneration By Dr. Hemn Hassan Othman PhD, Pathology Fall 2016 1/17/2017 1 Extracellular Degenerations I / Hyaline Degeneration (Hyalinization): The ward hyaline is derived from the Latin
Extracellular degeneration By Dr. Hemn Hassan Othman PhD, Pathology Fall 2016 1/17/2017 1 Extracellular Degenerations I / Hyaline Degeneration (Hyalinization): The ward hyaline is derived from the Latin
APOPTOSIS, NECROSIS AND CANCER. Dr. S. P. Pattanayak
 APOPTOSIS, NECROSIS AND CANCER Dr. S. P. Pattanayak LEARNING OBJECTIVES At the end of the lecture, students should be able to: Know the importance of cell death. Define various modes of cell death. Identify
APOPTOSIS, NECROSIS AND CANCER Dr. S. P. Pattanayak LEARNING OBJECTIVES At the end of the lecture, students should be able to: Know the importance of cell death. Define various modes of cell death. Identify
DEGENERATION NECROSIS AND INFILTRATION
 DEGENERATION NECROSIS AND INFILTRATION Cellular Degenerations and Infiltrations 1. Cloudy swelling and hydropic degeneration Cloudy swelling and hydropic degeneration occur when the regulatory mechanisms
DEGENERATION NECROSIS AND INFILTRATION Cellular Degenerations and Infiltrations 1. Cloudy swelling and hydropic degeneration Cloudy swelling and hydropic degeneration occur when the regulatory mechanisms
Lecture-2 / Dr Hussain Abady Aljebori Over view of cell injury and cell death; Cell injury results when: a. cells are stressed so severely that they
 Lecture-2 / Dr Hussain Abady Aljebori Over view of cell injury and cell death; Cell injury results when: a. cells are stressed so severely that they are no longer able to adapt or b. when cells are exposed
Lecture-2 / Dr Hussain Abady Aljebori Over view of cell injury and cell death; Cell injury results when: a. cells are stressed so severely that they are no longer able to adapt or b. when cells are exposed
Pigments and accumulations
 Pigments and accumulations Intracellular Accumulations Normal cellular constituent vs. abnormal substance Transient vs. permanent Harmless vs. toxic Cytoplasm vs. nucleus Cell produced vs. produced other
Pigments and accumulations Intracellular Accumulations Normal cellular constituent vs. abnormal substance Transient vs. permanent Harmless vs. toxic Cytoplasm vs. nucleus Cell produced vs. produced other
PATHOLOGY Intracellular Degeneration LAB 1
 PATHOLOGY Intracellular Degeneration LAB 1 Cellular swelling Liver Organ :- Liver Lesion :- 1. Narrowing of hepatic sinusoids due to the swelling of hepatocyte. 2. The cytoplasm of affected hepatocyte
PATHOLOGY Intracellular Degeneration LAB 1 Cellular swelling Liver Organ :- Liver Lesion :- 1. Narrowing of hepatic sinusoids due to the swelling of hepatocyte. 2. The cytoplasm of affected hepatocyte
Quiz 1 Review. More Cowbell
 Quiz 1 Review More Cowbell Quiz 1 review Inflamma7on Repair Cell Injury and Adapta7on Quiz 1 review Inflamma7on Injury Acute inflammation Chronic inflammation Abscess Resolution Repair Time course Inflammation
Quiz 1 Review More Cowbell Quiz 1 review Inflamma7on Repair Cell Injury and Adapta7on Quiz 1 review Inflamma7on Injury Acute inflammation Chronic inflammation Abscess Resolution Repair Time course Inflammation
Cell Physiology
 Cell Physiology 21-10-2018 1 The two major parts of a typical cell are the nucleus and the cytoplasm. The nucleus is separated from the cytoplasm by a nuclear membrane, and the cytoplasm is separated from
Cell Physiology 21-10-2018 1 The two major parts of a typical cell are the nucleus and the cytoplasm. The nucleus is separated from the cytoplasm by a nuclear membrane, and the cytoplasm is separated from
Coagulative Necrosis of Myocardium. Dr Rodney Itaki Division of Pathology
 Coagulative Necrosis of Myocardium Dr Rodney Itaki Division of Pathology Coagulative Necrosis Gross pathology: 3 day old infarct: Yellow necrosis surrounded by hyperemic borders. Arrow points to a transmural
Coagulative Necrosis of Myocardium Dr Rodney Itaki Division of Pathology Coagulative Necrosis Gross pathology: 3 day old infarct: Yellow necrosis surrounded by hyperemic borders. Arrow points to a transmural
Cellular response to stress
 Cellular pathology - cell injury, death and adaptations Pathology Göran Andersson Cellular response to stress Cells differ in their capacity to tolerate changes in their microenvironment Acute, severe
Cellular pathology - cell injury, death and adaptations Pathology Göran Andersson Cellular response to stress Cells differ in their capacity to tolerate changes in their microenvironment Acute, severe
Name: Date: Block: Biology 12
 Name: Date: Block: Biology 12 Provincial Exam Review: Cell Processes and Applications January 2003 Use the following diagram to answer questions 1 and 2. 1. Which labelled organelle produces most of the
Name: Date: Block: Biology 12 Provincial Exam Review: Cell Processes and Applications January 2003 Use the following diagram to answer questions 1 and 2. 1. Which labelled organelle produces most of the
Consultant Medical Laboratory Scientist Assistant Professor of Histopathology & Cytopathology
 بسم اهلل الرحمن الرحيم By: PhD (Histopathology & Cytopathology), M.BA (Total Quality Management) Consultant Medical Laboratory Scientist Assistant Professor of Histopathology & Cytopathology Introduction
بسم اهلل الرحمن الرحيم By: PhD (Histopathology & Cytopathology), M.BA (Total Quality Management) Consultant Medical Laboratory Scientist Assistant Professor of Histopathology & Cytopathology Introduction
ANATOMY OF THE IMMUNE SYSTEM
 Immunity Learning objectives Explain what triggers an immune response and where in the body the immune response occurs. Understand how the immune system handles exogenous and endogenous antigen differently.
Immunity Learning objectives Explain what triggers an immune response and where in the body the immune response occurs. Understand how the immune system handles exogenous and endogenous antigen differently.
Biology 12 Cell Structure and Function. Typical Animal Cell
 Biology 12 Cell Structure and Function Typical Animal Cell Vacuoles: storage of materials and water Golgi body: a series of stacked disk shaped sacs. Repackaging centre stores, modifies, and packages proteins
Biology 12 Cell Structure and Function Typical Animal Cell Vacuoles: storage of materials and water Golgi body: a series of stacked disk shaped sacs. Repackaging centre stores, modifies, and packages proteins
CELL INJURY AND CELL DEATH
 CELL INJURY AND CELL DEATH INTRODUCTION Cell Injury is a result of the sequence of events that occur if the limits of the adaptive capability of cells are exceeded or there is no adaptive response is possible,
CELL INJURY AND CELL DEATH INTRODUCTION Cell Injury is a result of the sequence of events that occur if the limits of the adaptive capability of cells are exceeded or there is no adaptive response is possible,
3- Cell Structure and Function How do things move in and out of cells? A Quick Review Taft College Human Physiology
 3- Cell Structure and Function How do things move in and out of cells? A Quick Review Taft College Human Physiology How do things move in and out of cells? Things may move through cell membranes by Passive
3- Cell Structure and Function How do things move in and out of cells? A Quick Review Taft College Human Physiology How do things move in and out of cells? Things may move through cell membranes by Passive
Unit Seven Blood and Immunity
 Unit Seven Blood and Immunity I. Introduction A. Definition Blood is a sticky fluid that is heavier and thicker than water. Blood is a type of, whose cells and suspended in a liquid intercellular material.
Unit Seven Blood and Immunity I. Introduction A. Definition Blood is a sticky fluid that is heavier and thicker than water. Blood is a type of, whose cells and suspended in a liquid intercellular material.
Functions of Blood. Transport. Transport. Defense. Regulation. Unit 6 Cardiovascular System: Blood
 Unit 6 Cardiovascular System: Blood Functions of Blood With each beat of the heart, approximately 75 ml of blood is pumped On average, the heart beats 70 times per minute Every minute, the heart pumps
Unit 6 Cardiovascular System: Blood Functions of Blood With each beat of the heart, approximately 75 ml of blood is pumped On average, the heart beats 70 times per minute Every minute, the heart pumps
Lymphoid System: cells of the immune system. Answer Sheet
 Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
NECROSIS, GANGRENE. I. practical training 2 rd year Dentistry
 NECROSIS, GANGRENE. I. practical training 2 rd year Dentistry Signs of death Cardiac arrest (no pulse) Pallor mortis, paleness which happens in the 15 120 minutes after death Livor mortis, a settling of
NECROSIS, GANGRENE. I. practical training 2 rd year Dentistry Signs of death Cardiac arrest (no pulse) Pallor mortis, paleness which happens in the 15 120 minutes after death Livor mortis, a settling of
Hashem Al-Dujaily. Tamer Barakat. Manar Hajeer
 1 Hashem Al-Dujaily Tamer Barakat... Manar Hajeer Introduction Pathology comes from Patho: disease/suffering and Logy: study. Therefore, Pathology is the study of disease. Pathology is the bridge between
1 Hashem Al-Dujaily Tamer Barakat... Manar Hajeer Introduction Pathology comes from Patho: disease/suffering and Logy: study. Therefore, Pathology is the study of disease. Pathology is the bridge between
Place and role of the pathology in the medicine. Structure of pathology and methods of investigation
 Place and role of the pathology in the medicine. Structure of pathology and methods of investigation Dr. Attila Zalatnai (Just for educational purposes) Without pathology there is no modern diagnostics!
Place and role of the pathology in the medicine. Structure of pathology and methods of investigation Dr. Attila Zalatnai (Just for educational purposes) Without pathology there is no modern diagnostics!
Topics of this lecture : RBC. Structural characteristics Hemoglobin Erythropoiesis Erythrocytes destruction
 Topics of this lecture : RBC Structural characteristics Hemoglobin Erythropoiesis Erythrocytes destruction Structural characteristics Its small size and biconcave shape provides more surface area than
Topics of this lecture : RBC Structural characteristics Hemoglobin Erythropoiesis Erythrocytes destruction Structural characteristics Its small size and biconcave shape provides more surface area than
NUTRITION & MALIGNANCY: An Overview
 NUTRITION & MALIGNANCY: An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ Temple 1 Malignancy and Weight loss (Cachexia)
NUTRITION & MALIGNANCY: An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ Temple 1 Malignancy and Weight loss (Cachexia)
Cell Overview. Hanan Jafar BDS.MSc.PhD
 Cell Overview Hanan Jafar BDS.MSc.PhD THE CELL is made of: 1- Nucleus 2- Cell Membrane 3- Cytoplasm THE CELL Formed of: 1. Nuclear envelope 2. Chromatin 3. Nucleolus 4. Nucleoplasm (nuclear matrix) NUCLEUS
Cell Overview Hanan Jafar BDS.MSc.PhD THE CELL is made of: 1- Nucleus 2- Cell Membrane 3- Cytoplasm THE CELL Formed of: 1. Nuclear envelope 2. Chromatin 3. Nucleolus 4. Nucleoplasm (nuclear matrix) NUCLEUS
Pathological Pigmentation
 Pathological Pigmentation By Dr. Hemn Hassan Othman PhD, Pathology, Fall 2018 10/20/2018 1 Pathological Pigmentation: Pigments: Pigments are colored substances accumulate abnormally within the tissue and
Pathological Pigmentation By Dr. Hemn Hassan Othman PhD, Pathology, Fall 2018 10/20/2018 1 Pathological Pigmentation: Pigments: Pigments are colored substances accumulate abnormally within the tissue and
WSC , Conference 9, Case 1. Tissue from a nyala.
 WSC 2009-2010, Conference 9, Case 1. Tissue from a nyala. MICROSCOPIC DESCRIPTION: Heart, atrium (1 pt.): Approximately 40% of the atrial myocardium is replaced by areas of fibrous connective tissue (1
WSC 2009-2010, Conference 9, Case 1. Tissue from a nyala. MICROSCOPIC DESCRIPTION: Heart, atrium (1 pt.): Approximately 40% of the atrial myocardium is replaced by areas of fibrous connective tissue (1
What is the composition of blood, including blood cells? What organs and structures control the flow of blood throughout the body?
 3 Chapter 10: Circulatory System and Lymphatic System In this chapter, you will learn about the structure and function of the circulatory system and lymphatic system. What is the composition of blood,
3 Chapter 10: Circulatory System and Lymphatic System In this chapter, you will learn about the structure and function of the circulatory system and lymphatic system. What is the composition of blood,
Lysosomes. Gr: lysis solution, soma body. Membrane bounded vesicles. Usually round ovoid or irregular electron dense bodies m.
 Lysosomes Gr: lysis solution, soma body Membrane bounded vesicles Usually round ovoid or irregular electron dense bodies 0.05 0.5 m. Lysosomes No. varies from a few to several hundred per cell, in different
Lysosomes Gr: lysis solution, soma body Membrane bounded vesicles Usually round ovoid or irregular electron dense bodies 0.05 0.5 m. Lysosomes No. varies from a few to several hundred per cell, in different
Cell Quality Control. Peter Takizawa Department of Cell Biology
 Cell Quality Control Peter Takizawa Department of Cell Biology Cellular quality control reduces production of defective proteins. Cells have many quality control systems to ensure that cell does not build
Cell Quality Control Peter Takizawa Department of Cell Biology Cellular quality control reduces production of defective proteins. Cells have many quality control systems to ensure that cell does not build
Atrophy. Dystrophy. II. practical training 2 rd year Dentistry. Lucie Tučková
 Atrophy. Dystrophy. II. practical training 2 rd year Dentistry Lucie Tučková Atrophy Decrease in size of the cell or organ Reduction in cell size and/or cell number, or both Atrophic cells may have diminished
Atrophy. Dystrophy. II. practical training 2 rd year Dentistry Lucie Tučková Atrophy Decrease in size of the cell or organ Reduction in cell size and/or cell number, or both Atrophic cells may have diminished
DISEASE ETIOLOGY. Dynamic condition Morpho-functional alteration of one or more organ/tissue Acute or chronic Localized or systemic
 DISEASE Dynamic condition Morpho-functional alteration of one or more organ/tissue Acute or chronic Localized or systemic Etiology = studies the causes of disease Pathogenesis = starting from etiology,
DISEASE Dynamic condition Morpho-functional alteration of one or more organ/tissue Acute or chronic Localized or systemic Etiology = studies the causes of disease Pathogenesis = starting from etiology,
The Cardiovascular System: Blood
 C h a p t e r 11 The Cardiovascular System: Blood PowerPoint Lecture Slides prepared by Jason LaPres Lone Star College - North Harris Introduction to the Cardiovascular System A circulating transport system
C h a p t e r 11 The Cardiovascular System: Blood PowerPoint Lecture Slides prepared by Jason LaPres Lone Star College - North Harris Introduction to the Cardiovascular System A circulating transport system
18. PANCREATIC FUNCTION AND METABOLISM. Pancreatic secretions ISLETS OF LANGERHANS. Insulin
 18. PANCREATIC FUNCTION AND METABOLISM ISLETS OF LANGERHANS Some pancreatic functions have already been discussed in the digestion section. In this one, the emphasis will be placed on the endocrine function
18. PANCREATIC FUNCTION AND METABOLISM ISLETS OF LANGERHANS Some pancreatic functions have already been discussed in the digestion section. In this one, the emphasis will be placed on the endocrine function
I. ADAPTATION TO ENVIRONMENTAL STRESS. A. Hypertrophy:
 د.جواهر محي الدين Lec:2&3 Cellular Reaction to Injury I. ADAPTATION TO ENVIRONMENTAL STRESS II. HYPOXIC CELL INJURY III. FREE RADICAL INJURY IV. CHEMICAL CELL INJURY V. NECROSIS VI. APOPTOSIS VII. REVERSIBLE
د.جواهر محي الدين Lec:2&3 Cellular Reaction to Injury I. ADAPTATION TO ENVIRONMENTAL STRESS II. HYPOXIC CELL INJURY III. FREE RADICAL INJURY IV. CHEMICAL CELL INJURY V. NECROSIS VI. APOPTOSIS VII. REVERSIBLE
Essentials of Anatomy and Physiology, 9e (Marieb) Chapter 3 Cells and Tissues. Short Answer. Figure 3.1
 Chapter 3 Cells and Tissues. Short Answer. Figure 3.1") Essentials of Anatomy and Physiology, 9e (Marieb) Chapter 3 Cells and Tissues Short Answer Figure 3.1 Using Figure 3.1, match the following: 1) The illustration of simple cuboidal epithelium is. Answer:
Essentials of Anatomy and Physiology, 9e (Marieb) Chapter 3 Cells and Tissues Short Answer Figure 3.1 Using Figure 3.1, match the following: 1) The illustration of simple cuboidal epithelium is. Answer:
Blood consists of red and white blood cells suspended in plasma Blood is about 55% plasma and 45% cellular elements Plasma 90% water 10% dissolved
 Bio 100 Guide 21 Blood consists of red and white blood cells suspended in plasma Blood is about 55% plasma and 45% cellular elements Plasma 90% water 10% dissolved inorganic ions, proteins, nutrients,
Bio 100 Guide 21 Blood consists of red and white blood cells suspended in plasma Blood is about 55% plasma and 45% cellular elements Plasma 90% water 10% dissolved inorganic ions, proteins, nutrients,
Published on Second Faculty of Medicine, Charles University (http://www.lf2.cuni.cz )
") Published on Second Faculty of Medicine, Charles University (http://www.lf2.cuni.cz ) Biochemistry Submitted by Marie Havlová on 8. February 2012-0:00 Syllabus of Biochemistry Mechanisms of enzyme catalysis.
Published on Second Faculty of Medicine, Charles University (http://www.lf2.cuni.cz ) Biochemistry Submitted by Marie Havlová on 8. February 2012-0:00 Syllabus of Biochemistry Mechanisms of enzyme catalysis.
4. A phospholipid is an example of organization at the level.
 1. Physiology is the study of a. the structures of anatomical features. b. cellular metabolism. c. processes that allow organisms to function. d. how organ systems develop from the embryo. 2. Mary spends
1. Physiology is the study of a. the structures of anatomical features. b. cellular metabolism. c. processes that allow organisms to function. d. how organ systems develop from the embryo. 2. Mary spends
Blood: Functions. Liquid connective tissue 3 general functions 1. Transportation. 2. Regulation. 3. Protection
 Blood Elements Lecture Objectives List blood components. Classify formed elements of blood. Discuss the scientific basis of the above classification. Describe the basic structure of erythrocytes and criteria
Blood Elements Lecture Objectives List blood components. Classify formed elements of blood. Discuss the scientific basis of the above classification. Describe the basic structure of erythrocytes and criteria
Pathology MCQs. lipid. protein. glycogen. lipofuscin. water. Karyolysis. Cellular swelling. Involvement of a large number of cells
 Pathology MCQs 1. In hypoxic cell injury, cell swelling occurs because of increased intracellular: lipid protein glycogen lipofuscin water 2. Which of the following is a feature of apoptosis? Karyolysis
Pathology MCQs 1. In hypoxic cell injury, cell swelling occurs because of increased intracellular: lipid protein glycogen lipofuscin water 2. Which of the following is a feature of apoptosis? Karyolysis
Digestion and Absorption
 Digestion and Absorption Digestion and Absorption Digestion is a process essential for the conversion of food into a small and simple form. Mechanical digestion by mastication and swallowing Chemical digestion
Digestion and Absorption Digestion and Absorption Digestion is a process essential for the conversion of food into a small and simple form. Mechanical digestion by mastication and swallowing Chemical digestion
human cell Mader s Understanding Human Anatomy and Physiology Chapters 1, 3 and 4
 1 The human cell INTRODUCTION All living things are composed of cells, which are the smallest units of life and are so small they can only be viewed through a microscope. Cells are made from pre-existing
1 The human cell INTRODUCTION All living things are composed of cells, which are the smallest units of life and are so small they can only be viewed through a microscope. Cells are made from pre-existing
Chapter 3 Review Assignment
 Class: Date: Chapter 3 Review Assignment Multiple Choice 40 MC = 40 Marks Identify the choice that best completes the statement or answers the question. 1. Which of the following organelles produces transport
Class: Date: Chapter 3 Review Assignment Multiple Choice 40 MC = 40 Marks Identify the choice that best completes the statement or answers the question. 1. Which of the following organelles produces transport
Agenda. Components of blood. Blood is Fluid Connective Tissue. Blood: General functions
 Agenda Chapter 19: Blood Major functions Major Components Structure of RBCs and WBCs ABO Blood Types, and Rh Factor Lab 34.1 and Blood Typing Blood: General functions Transport of dissolved gases, nutrients,
Agenda Chapter 19: Blood Major functions Major Components Structure of RBCs and WBCs ABO Blood Types, and Rh Factor Lab 34.1 and Blood Typing Blood: General functions Transport of dissolved gases, nutrients,
-sheet 3. -Waseem Alhaj. Maha Shomaf
 -sheet 3 -Basheer egbaria -Waseem Alhaj Maha Shomaf 1 P a g e Viral hepatitis have many types each type is associated with different outcomes complication, some can result in acute one,others result in
-sheet 3 -Basheer egbaria -Waseem Alhaj Maha Shomaf 1 P a g e Viral hepatitis have many types each type is associated with different outcomes complication, some can result in acute one,others result in
Cellular Pathology. Histopathology Lab #2 (web) Paul Hanna Jan 2018
 Paul Hanna Jan 2018") Cellular Pathology Histopathology Lab #2 (web) Paul Hanna Jan 2018 Slide #91 Clinical History: a necropsy was performed on an aged cat the gross pathological changes included: widespread subcutaneous edema
Cellular Pathology Histopathology Lab #2 (web) Paul Hanna Jan 2018 Slide #91 Clinical History: a necropsy was performed on an aged cat the gross pathological changes included: widespread subcutaneous edema
The Cell and Cellular transport
 Cell theory (1838): The Cell 1. All organisms are composed of one or more cells, and the life processes of metabolism and heredity occur within these cells. 2. Cells are the smallest living things, the
Cell theory (1838): The Cell 1. All organisms are composed of one or more cells, and the life processes of metabolism and heredity occur within these cells. 2. Cells are the smallest living things, the
lysosomes Ingested materials Defective cell components Degrades macromolecules of all types:
 lysosomes Digests Ingested materials Defective cell components Degrades macromolecules of all types: Proteins Nucleic acids Carbohydrates Lipids Single membrane bound vesicle, contains up to 50 digestive
lysosomes Digests Ingested materials Defective cell components Degrades macromolecules of all types: Proteins Nucleic acids Carbohydrates Lipids Single membrane bound vesicle, contains up to 50 digestive
Chapter 1 Plasma membranes
 1 of 5 TEXTBOOK ANSWERS Chapter 1 Plasma membranes Recap 1.1 1 The plasma membrane: keeps internal contents of the cell confined to one area keeps out foreign molecules that damage or destroy the cell
1 of 5 TEXTBOOK ANSWERS Chapter 1 Plasma membranes Recap 1.1 1 The plasma membrane: keeps internal contents of the cell confined to one area keeps out foreign molecules that damage or destroy the cell
Renata Schipp Medical Biology Department
 Renata Schipp Medical Biology Department Deffinition of cell The cell is the smallest structural and functional unit of all known living organisms The cell was discovered by Robert Hooke in 1665 and also
Renata Schipp Medical Biology Department Deffinition of cell The cell is the smallest structural and functional unit of all known living organisms The cell was discovered by Robert Hooke in 1665 and also
1- Which of the following statements is TRUE in regards to eukaryotic and prokaryotic cells?
 Name: NetID: Exam 3 - Version 1 October 23, 2017 Dr. A. Pimentel Each question has a value of 4 points and there are a total of 160 points in the exam. However, the maximum score of this exam will be capped
Name: NetID: Exam 3 - Version 1 October 23, 2017 Dr. A. Pimentel Each question has a value of 4 points and there are a total of 160 points in the exam. However, the maximum score of this exam will be capped
Mechanisms of disease
 PP Mechanisms of disease Stress and disease Homeostasis - Responsible for maintaining a constant, safe internal environment - Controlled by feedback loops o Negative feedback loop: temperature, blood glucose
PP Mechanisms of disease Stress and disease Homeostasis - Responsible for maintaining a constant, safe internal environment - Controlled by feedback loops o Negative feedback loop: temperature, blood glucose
INFLAMMATION. 5. Which are the main phases of inflammation in their "sequence": 1. Initiation, promotion, progression.
 INFLAMMATION 1. What is inflammation: 1. Selective anti-infective pathological reaction. 2. Pathological process, typical for vascularized tissues. 3. Self-sustained pathological condition. 4. Disease
INFLAMMATION 1. What is inflammation: 1. Selective anti-infective pathological reaction. 2. Pathological process, typical for vascularized tissues. 3. Self-sustained pathological condition. 4. Disease
Test Review Worksheet 1 Name: Per:
 Test Review Worksheet 1 Name: Per: 1. Put the following in order according to blood flow through the body, starting with the lungs: Lungs, right atrium, left atrium, right ventricle, left ventricle, aorta,
Test Review Worksheet 1 Name: Per: 1. Put the following in order according to blood flow through the body, starting with the lungs: Lungs, right atrium, left atrium, right ventricle, left ventricle, aorta,
Hematopoiesis. Hematopoiesis. Hematopoiesis
 Chapter. Cells and Organs of the Immune System Hematopoiesis Hematopoiesis- formation and development of WBC and RBC bone marrow. Hematopoietic stem cell- give rise to any blood cells (constant number,
Chapter. Cells and Organs of the Immune System Hematopoiesis Hematopoiesis- formation and development of WBC and RBC bone marrow. Hematopoietic stem cell- give rise to any blood cells (constant number,
Blood and Defense. Chapter 11
 Blood and Defense Chapter 11 Functions of Blood 1. Carry nutrients from the small intestine and oxygen from the lung to tissues in the body 2. Transport wastes from tissues to the kidneys and carbon dioxide
Blood and Defense Chapter 11 Functions of Blood 1. Carry nutrients from the small intestine and oxygen from the lung to tissues in the body 2. Transport wastes from tissues to the kidneys and carbon dioxide
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 25 Metabolism and Nutrition Metabolic Reactions Metabolism refers to all of the chemical reactions taking place in the body. Reactions that break
Principles of Anatomy and Physiology 14 th Edition CHAPTER 25 Metabolism and Nutrition Metabolic Reactions Metabolism refers to all of the chemical reactions taking place in the body. Reactions that break
Study of different tissues Abnormal cells and tissues can be compared to normal tissues to identify disease, such as cancer Being able to know and
 CHAPTER 4 Study of different tissues Abnormal cells and tissues can be compared to normal tissues to identify disease, such as cancer Being able to know and recognize normal tissues under the microscope
CHAPTER 4 Study of different tissues Abnormal cells and tissues can be compared to normal tissues to identify disease, such as cancer Being able to know and recognize normal tissues under the microscope
Reticuloendothelial System (RES) & Spleen Dr. Nervana Bayoumy
 & Spleen Dr. Nervana Bayoumy") Haematology Lectures Reticuloendothelial System (RES) & Spleen Dr. Nervana Bayoumy 1 Objectives 1. Define the term Reticuloendothelial system (RES). 2. Describe the cellular components of RES. 3. Describe
Haematology Lectures Reticuloendothelial System (RES) & Spleen Dr. Nervana Bayoumy 1 Objectives 1. Define the term Reticuloendothelial system (RES). 2. Describe the cellular components of RES. 3. Describe
4. ABSORPTION. Transport mechanisms. Absorption ABSORPTION MECHANISMS. Active transport. Active transport uses metabolic energy
 4. ABSORPTION ABSORPTION MECHANISMS Once the digestive process is completed, the nutrients have to be transferred across the digestive tract epithelium into the intracellular space and eventually into
4. ABSORPTION ABSORPTION MECHANISMS Once the digestive process is completed, the nutrients have to be transferred across the digestive tract epithelium into the intracellular space and eventually into
Branch of medicine that deals with blood, its formation and disorders is called. Three main functions of cardiovascular system are,, and.
 Chapter 19 The Blood Human body must maintain a balance called. Body fluid inside the cells is called fluid; that outside is called or fluid. Two major fluid networks that help in connecting cells are
Chapter 19 The Blood Human body must maintain a balance called. Body fluid inside the cells is called fluid; that outside is called or fluid. Two major fluid networks that help in connecting cells are
Blood. Biol 105 Lecture 14 Chapter 11
 Blood Biol 105 Lecture 14 Chapter 11 Outline I. Overview of blood II. Functions of blood III. Composition of blood IV. Composition of plasma V. Composition of formed elements VI. Platelets VII. White blood
Blood Biol 105 Lecture 14 Chapter 11 Outline I. Overview of blood II. Functions of blood III. Composition of blood IV. Composition of plasma V. Composition of formed elements VI. Platelets VII. White blood
Cell morphology. Cell organelles structure and function. Chapter 1: UNIT 1. Dr. Charushila Rukadikar
 UNIT 1 Cell morphology Cell organelles structure and function Chapter 1: Dr. Charushila Rukadikar Assistant Professor Department Of Physiology ZMCH, Dahod Physiology The science that is concerned with
UNIT 1 Cell morphology Cell organelles structure and function Chapter 1: Dr. Charushila Rukadikar Assistant Professor Department Of Physiology ZMCH, Dahod Physiology The science that is concerned with
Energy Production In A Cell (Chapter 25 Metabolism)
") Energy Production In A Cell (Chapter 25 Metabolism) Large food molecules contain a lot of potential energy in the form of chemical bonds but it requires a lot of work to liberate the energy. Cells need
Energy Production In A Cell (Chapter 25 Metabolism) Large food molecules contain a lot of potential energy in the form of chemical bonds but it requires a lot of work to liberate the energy. Cells need
Chapter 3: Cytology. Cytology is the study of cells. Cells are the basic units of life. We are made up of trillions of cells.
 PLEASE NOTE THAT THE ITEMS IN THE TEXT THAT ARE HIGHLIGHTED IN YELLOW ARE THOSE THAT ARE TOUCHED ON IN THE READING ASSIGNMENT (PAGES 90-99) AND IN THE LECTURE. ESPECIALLY KNOW THIS MATERIAL FOR THE FIRST
PLEASE NOTE THAT THE ITEMS IN THE TEXT THAT ARE HIGHLIGHTED IN YELLOW ARE THOSE THAT ARE TOUCHED ON IN THE READING ASSIGNMENT (PAGES 90-99) AND IN THE LECTURE. ESPECIALLY KNOW THIS MATERIAL FOR THE FIRST
2 nd Practice. Cell injury, adaptation, storage disorders. Semmelweis University 2nd Department of Pathology
 2 nd Practice Cell injury, adaptation, storage disorders Semmelweis University 2nd Department of Pathology Cell and tissue injury Cellular response to injury depends on the type, the duration and the severity
2 nd Practice Cell injury, adaptation, storage disorders Semmelweis University 2nd Department of Pathology Cell and tissue injury Cellular response to injury depends on the type, the duration and the severity
Blood. The only fluid tissue in the human body Classified as a connective tissue. Living cells = formed elements Non-living matrix = plasma
 Blood Blood The only fluid tissue in the human body Classified as a connective tissue Living cells = formed elements Non-living matrix = plasma Blood Physical Characteristics of Blood Color range Oxygen-rich
Blood Blood The only fluid tissue in the human body Classified as a connective tissue Living cells = formed elements Non-living matrix = plasma Blood Physical Characteristics of Blood Color range Oxygen-rich
Cell Cell
 Go to cellsalive.com. Select Interactive Cell Models: Plant and Animal. Fill in the information on Plant and Animal Organelles, then Click on Start the Animation Select Plant or Animal Cell below the box.
Go to cellsalive.com. Select Interactive Cell Models: Plant and Animal. Fill in the information on Plant and Animal Organelles, then Click on Start the Animation Select Plant or Animal Cell below the box.
Station One: Nutrition
 Station One: Nutrition Name that thing! 1. Chemical substances, found in foods, which are used in the human body. 2. Nutrient in human diet where foods are the only possible source of the nutrient. 3.
Station One: Nutrition Name that thing! 1. Chemical substances, found in foods, which are used in the human body. 2. Nutrient in human diet where foods are the only possible source of the nutrient. 3.
CH 11 Blood OUTLINE: Functions of Blood Composition of Blood Blood Cell Disorders Blood Types Blood Clotting Functions of Blood Transportation
 1 CH 11 Blood OUTLINE: Functions of Blood Composition of Blood Blood Cell Disorders Blood Types Functions of Blood Transportation Protection Regulation ph Temperature Composition of Blood Plasma: liquid
1 CH 11 Blood OUTLINE: Functions of Blood Composition of Blood Blood Cell Disorders Blood Types Functions of Blood Transportation Protection Regulation ph Temperature Composition of Blood Plasma: liquid
Name: Class: Date: Cell Structure and Transport Take Home Exam
 Name: Class: Date: Cell Structure and Transport Take Home Exam 1. Which is found in the nucleus? (1.) ribosome (2.) centrosome (3.) vacuole (4.) lysosome (5.) chromosome 2. Which structure composed mainly
Name: Class: Date: Cell Structure and Transport Take Home Exam 1. Which is found in the nucleus? (1.) ribosome (2.) centrosome (3.) vacuole (4.) lysosome (5.) chromosome 2. Which structure composed mainly
Unit 2 Warm Ups. Equilibrium
 Unit 2 Warm Ups Equilibrium 1. Cell wall 2. Mitochondria 3. Chloroplast 4. Vesicle 5. Vacuole 6. Rough Endoplasmic Reticulum 7. Smooth Endoplasmic Reticulum 8. Cytoskeleton 9. Lysosomes 10.Cell Membrane
Unit 2 Warm Ups Equilibrium 1. Cell wall 2. Mitochondria 3. Chloroplast 4. Vesicle 5. Vacuole 6. Rough Endoplasmic Reticulum 7. Smooth Endoplasmic Reticulum 8. Cytoskeleton 9. Lysosomes 10.Cell Membrane
Average adult = 8-10 pints of blood. Functions:
 Average adult = 8-10 pints of blood Functions: Transports nutrients, oxygen, cellular waste products, and hormones Aids in distribution of heat Regulates acid-base balance Helps protect against infection
Average adult = 8-10 pints of blood Functions: Transports nutrients, oxygen, cellular waste products, and hormones Aids in distribution of heat Regulates acid-base balance Helps protect against infection
Lec.2 Medical Physiology Blood Physiology Z.H.Kamil
 Destruction of Red Blood Cells When red blood cells are delivered from the bone marrow into the circulatory system, they normally circulate an average of 120 days before being destroyed. Even though mature
Destruction of Red Blood Cells When red blood cells are delivered from the bone marrow into the circulatory system, they normally circulate an average of 120 days before being destroyed. Even though mature
Title: Sep 10 7:59 PM (1 of 36) Ch 3 Cell Organelles and Transport
 Ch 3 Cell Organelles and Transport") Title: Sep 10 7:59 PM (1 of 36) Ch 3 Cell Organelles and Transport Title: Sep 10 8:02 PM (2 of 36) Cell organelles Nucleus: contains DNA Title: Sep 10 8:03 PM (3 of 36) Nuclear envelope double membrane
Title: Sep 10 7:59 PM (1 of 36) Ch 3 Cell Organelles and Transport Title: Sep 10 8:02 PM (2 of 36) Cell organelles Nucleus: contains DNA Title: Sep 10 8:03 PM (3 of 36) Nuclear envelope double membrane
Questions in Cell Biology
 Name: Questions in Cell Biology Directions: The following questions are taken from previous IB Final Papers on the subject of cell biology. Answer all questions. This will serve as a study guide for the
Name: Questions in Cell Biology Directions: The following questions are taken from previous IB Final Papers on the subject of cell biology. Answer all questions. This will serve as a study guide for the
BIOLOGICAL MOLECULES REVIEW-UNIT 1 1. The factor being tested in an experiment is the A. data. B. variable. C. conclusion. D. observation. 2.
 BIOLOGICAL MOLECULES REVIEW-UNIT 1 1. The factor being tested in an experiment is the A. data. B. variable. C. conclusion. D. observation. 2. A possible explanation for an event that occurs in nature is
BIOLOGICAL MOLECULES REVIEW-UNIT 1 1. The factor being tested in an experiment is the A. data. B. variable. C. conclusion. D. observation. 2. A possible explanation for an event that occurs in nature is