Update in Lipid Management. Rameshkumar Raman M.D. Endocrine Associates of The Quad Cities
|
|
|
- Dustin Eaton
- 5 years ago
- Views:
Transcription

1 Update in Lipid Management Rameshkumar Raman M.D. Endocrine Associates of The Quad Cities
2 Low-Density Lipoprotein (LDL) Consists of Multiple Distinct Subclasses Differing in Size and Lipid Content* Association with Cardiovascular Disease Risk Large 1 2 Weaker Small 3 4 Stronger * Distribution of subclasses is independent of LDL-cholesterol. Berneis KK, Krauss RM. J Lipid Res. 2002;43: Reduced clearance Greater entry into artery Greater retention Faster oxidation ATP III Update LDL-cholesterol Recommendations Risk Category 10 yr Risk % Very high >>20 High 20 Features ACS CHD + 1RF CHD + poor control RFs CHD + Metabolic syn CHD CHD Equivalents 2 RFs Goal mg/dl Option mg/dl <70 -- <100 <70 Moderately high RFs <130 <100 Moderate RFs < Low <5 1 RF < Circulation 2004: 110:

3 Modified ATP III LDL-C Guidelines Low (<5%) CHD Risk Intermediate (5-9%) Moderately High (10-19%) High (>20%) Very High (ACS) <160 <130 LDL-Cholesterol Goals <130* * Treat other lifestyle risk factors, metabolic syndrome # Use non-hdl-c for additional drug treatment <100* # <70* # Circulation, July 13, 2004; 110: ATP III. NIH publication


4 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285: ATP III: Additional CHD Risk Factors

5 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285: Δ mmol/l kg of Weight Loss Plasma Lipids Improve with Weight Loss Meta-analysis of 70 Clinical Trials *P<0.05. Total Cholesterol * LDL-C TG HDL-C (weight stable) * HDL-C (actively losing) LDL-C=low density lipoprotein cholesterol; HDL-C=high-density lipoprotein cholesterol; TG=triglycerides Dattilo et al. Am J Clin Nutr 1992;56:320. * * * Δ mg/dl per kg of Weight Loss
6 Impact of Weight Loss on Risk ~5% Factors HbA1c Blood Pressure Weight Loss 1 2 5%-10% Weight Loss 1 2 Total Cholesterol HDL Cholesterol Triglycerides Wing RR et al. Arch Intern Med. 1987;147: Mertens IL, Van Gaal LF. Obes Res. 2000;8: Blackburn G. Obes Res. 1995;3 (Suppl 2):211S-216S. 4. Ditschunheit HH et al. Eur J Clin Nutr. 2002;56: Statins: Mechanism of Action Cholesterol synthesis Intracellular Cholesterol LDL receptor (B E E receptor) synthesis VLDL R LDL Apo B Apo E Apo B VLDL LDL receptor mediated hepatic uptake of LDL and VLDL remnants Serum LDL-C Serum VLDL remnants Serum IDL Hepatocyte Systemic Circulation Reduce hepatic cholesterol synthesis, lowering intracellular cholesterol, which stimulates upregulation of LDL receptor and increases the uptake of non-hdl particles from the systemic circulation.

7 Potential Time Course of Statin Effects LDL-C Inflammation lowered* reduced Vulnerable plaques stabilized Endothelial function restored Ischemic episodes reduced Cardiac events reduced* Days * Time course established Years Relation Between CHD Events and LDL-C Outcomes in Statin Trials 30 % with CHD event 10 CARE-Rx LIPID-PI WOSCOPS-PI PI=placebo Rx=treatment 150

8 No. of Events RRR, % ARR/1000 NNT P PI Statin (95% CI) (95% CI) (95% CI) Value CHD Risk Reduction with Statin Therapy Relative Risk Reduction (%) Endpoints Major coronary events Coronary deaths Cardiovascular deaths Noncardiovascular events Total mortality Strokes Intermittent claudication Angina La Rosa JC et al. JAMA 1999;282: Crouse JR III et al. Arch Intern Med 1997;157: Pedersen TR et al. Am J Cardiol 1998;81:
9 ATP III Treatment Priorities Reduce LDL-C to goal (new goals) Correct residual lipid/lipoprotein abnormalities( non-hdl-cholesterol) Address the metabolic syndrome Options for reducing LDL-cholesterol Statins Cholesterol absorption inhibitors Bile acid binding resins Niacin Stanol/sterol products
10 What factors should influence selection of a statin? Potency Safety Cost: level pricing Efficacy in reducing CV events Not, pleiotropic properties The LDL-C Lowering Efficacy of the Currently Available Statins Daily Dose Atorva/ Rosuv Fluva Lova Prava Simva 10 mg 20 mg 40 mg 80 mg 39%/ 43% 43%/ 48% 50%/ 53% 60%/ 58% 22% 30% 22% 27% 32% 38% 25% 32% 34% 41% 36% 42% 47%.

11 How low a LDL-C is safe? Newborn LDL-C is mg/dl LDL Rc is high affinity Patients with hypobetalipoproteinemia are healthy and have enhanced survival * * * *P<0.001 compared to No/No patients. Adapted from Fonarow GC et al. Am J Cardiol. 2005;96:


12
13 What are the options when statin therapy does not get the LDL-C to goal? Treatment intensity related to risk Increase dose, if therapeutic range permits Add Zetia or resin Add plant stanol/sterol products If other lipid abnormalities present add: Fibrates or niacin Ezetimibe (Zetia TM ) Inhibits cholesterol absorption Mono or combination therapy MonoRx/added to statin: ~ 20 % LDL-C VYTORIN (Z+Z); 10mg Z+10mg Z= 80mg Z Lower statin doses: 10mg L+10mg Z = 80mg L Minimal effect on TG and HDL-C
, 4 164 g/d Colestipol (Colestid), 5 205")
14 Bile Acid Resins: Mechanism of Action Gall Bladder Cholesterol 7-α7 hydroxylase Conversion of cholesterol to BA BA Secretion Terminal Ileum BA Excretion Bile Acid Enterohepatic Recirculation Reabsorption of bile acids LDL Receptors Liver VLDL and LDL removal Net Effect: LDL-C Clinical Features of BARs Products available: Cholestyramine (Questran), g/d Colestipol (Colestid), g/d Colesevelam (WelChol) 625 mg tablets, tablets/d Reduce coronary events (LRC-CPPT) CPPT) Adverse effects GI intolerance: constipation, bloating, abdominal pain, flatulence Lack systemic toxicity Drug interactions (colestipol and cholestyramine) Bind other negatively charged drugs Impede the absorption of drugs and/or fat-soluble vitamins Must give other drugs 1 hour before or hours after

15 Change in LDL-C Effect of Colesevelam on LDL-C (N=494 patients with baseline LDL-C C of mg/dl and TG <300 mg/dl; after 24 weeks of therapy) 0% -5% -10% -15% -20% Placebo 0% 3.8 g/d 4.5 g/d 15% Davidson MH et al. Expert Opin Investig Drugs 2000;9: Reprinted with permission from Ashley Publications. 18% Mean Percent Change 0% -10% -20% -30% -40% -50% Simvastatin Alone and with Colesevelam: Percent Change in LDL-C (n=258 patients with baseline LDL-C C mg/dl; treated for 6 weeks) 4% * 26% * 34% * * 42% 42% * p<0.05 vs placebo Knapp HH et al. Am J Med 2001;110: Reprinted with permission from Excerpta Medica Inc. Placebo Simvastatin 10 mg Simvastatin 20 mg Colesevelam 2.3 g + Simvastatin 20 mg Colesevelam 3.8 g + Simvastatin 10 mg
16 Nicotinic Acid: Mechanism of Action Mobilization of FFA TG synthesis Liver Apo B VLDL Hepatocyte VLDL secretion VLDL LD L Serum VLDL results in reduced lipolysis to LDL Serum LDL HDL Circulation Systemic Circulation Decreases hepatic production of VLDL and of apo B Clinical Features of Nicotinic Acid Products available (daily dose) Immediate-release, g/d Extended-release (Niaspan ), g/d OTC products, sustained-release, 2 2 g/d Best agent to raise HDL-C Reduces coronary events (Coronary Drug Project) Adverse effects Flushing, itching, headache (immediate-release, Niaspan ) Hepatotoxicity, GI (sustained-release) Activation of peptic ulcer Hyperglycemia and reduced insulin sensitivity Contraindications Active liver disease or unexplained LFT elevations Peptic ulcer disease

17 Percent Change The Effect of Adding Niaspan to a Stable Dose of a Statin 30% 20% 10% 0% -10% -20% -30% -8% 1 gram daily 2 grams daily 24% 24% LDL-C HDL-C TG 30% 20% 10% 0% -10% -20% -30% -40% Wolfe ML et al. Am J Cardiol 2001;87: % 27% 30% LDL-C HDL-C TG
 Feno n=24 Plb n=22 Total Cholesterol 17.5 0.4 15.8 +4.6 LDL-C 20.3 +0.4 6.1 0.5 HDL-C +11.1 1.2 +15.3 3.5 Total Triglycerides 37.9 4.2 44.6 +22.3 LDL-C/HDL-C 27.1 1.9 13.3 0.")
18 Effects of Fenofibrate on Plasma Lipids Double-Blind, Multicenter, 24-Week Study in Patients with Primary Hypercholesterolemia or Mixed Hyperlipidemia (HPL) Hypercholesterolemia (%) Feno n=92 Plb n=88 Mixed HPL (%) Feno n=24 Plb n=22 Total Cholesterol LDL-C HDL-C Total Triglycerides LDL-C/HDL-C VLDL-C p<0.01 except for LDL-C in Type IIb, where p>0.10 Brown WV et al. Arteriosclerosis 1986;6: Lippincott Williams & Wilkins.

* BIP BIP (Post Hoc)** VA-HIT 2.1 10.4 9.9 15.")
19 % CHD Death/Nonfatal MI Trials of Fibrates: Effects on Cardiac Events 34% Rx Placebo *** 2.7 Deaths % 8.0 PRIMARY PREVENTION 9% 42% * Post hoc analysis of subgroup with TG >200 mg/dl and HDL-C <42 mg/dl. ** Post hoc analysis of subgroup with TG 200 mg/dl and HDL-C <35 mg/dl. *** Difference between placebo and Rx for primary endpoint was statistically significant (p < 0.05). Frick MH et al. N Engl J Med 1987;317: Manninen V et al. Circulation 1992;85: BIP Study Group. Circulation 2000;102: Rubins HB et al. N Engl J Med 1999;341: % 17.3 SECONDARY PREVENTION 21.7*** HHS HHS (Post Hoc)* BIP BIP (Post Hoc)** VA-HIT Percent Change Statin + Fibrate 39% Simva + Gemfibrozil LDL-C TG 50% 16% HDL-C 38 Prava/Simva + Fenofibrate 166 LDL-C 28% % Da Col PG et al. Curr Ther Res Clin Exp 1973;53: Ellen RL et al. Am J Cardiol 1998;81:60B-65B. TG 22% HDL-C 34
20 Triple-Drug Regimen Lovastatin 40 mg/d Niaspan g/d Colestipol 20 g/d Baseline (mg/dl) 8 months (mg/dl) Change (%) LDL-C % HDL-C % LDL-C/HDL-C ratio % Brown BG et al. Am J Cardiol 1997;80: Progression of Drug Therapy for LDL-C Lowering Visit 1 Visit 2 Visit 3 Initiate LDL- lowering drug therapy 6 wks If LDL goal not achieved, intensify LDL- lowering therapy 6 wks If LDL goal not achieved, drug therapy or refer to a lipid specialist q 4 6 mo F/U Visits Monitor response and adherence to therapy Start statin or bile acid resin or nicotinic acid Consider higher dose of the statin or add a bile acid resin or nicotinic acid If LDL goal has been achieved, treat other lipid risk factors Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:
21 Treatment of Mixed Hyperlipidemia High LDL-C C and TGs Therapeutic Lifestyle Change Drug Therapy STEP STEP 1 2 Achieve the LDL-C C goal Achieve the non-hdl HDL-C C goal Increase LDL-C C lowering or Add a fibrate, niacin or fish oils Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285: Muscle Adverse Effects Myalgia Weakness Fatigue Myopathy without CK Predisposing factors: Combined hyperlipidemia Subclinical hypothyroidism Suboptimum thyroxine replacement American College of Physicians. All Rights Reserved.
 combo in renal impairment Assure no interactions Teach the patient to recognize muscle symptoms")
22 Steps to Minimize the Risk of Muscle Toxicity with Fibrate Statin Combination Therapy Use statin alone for non-hdl-c goals Use fish oils or niacin rather than fibrates Keep the doses of the statin and fibrate low Dose the fibrate in the AM and the statin in the PM Avoid (or cautiously use) combo in renal impairment Assure no interactions Teach the patient to recognize muscle symptoms Discontinue therapy if muscle symptoms are present and CK is >10 times the upper limit of normal
23
, GISSI Prevenzione Trial, others")
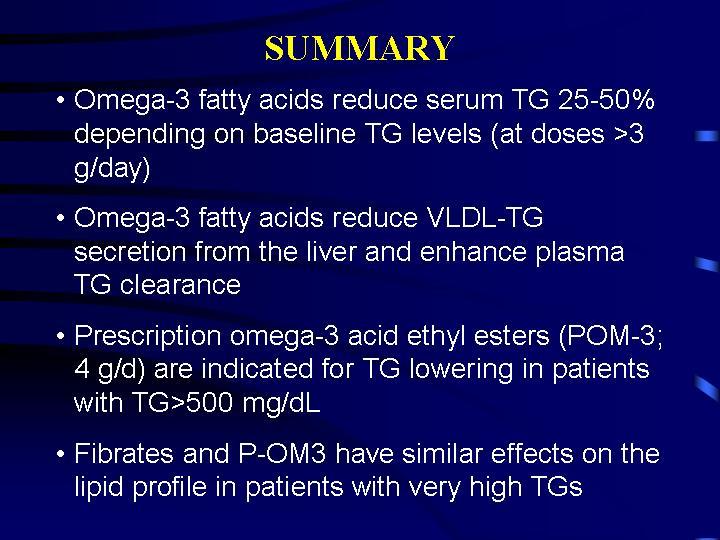
24 Indication s: Fish Oils Adjunctive therapy to diet Hypertriglyceridemia (Type IV and V) With statins or other LDL-C lowering drugs in mixed hyperlipidemia Efficacy: Decrease TG 30 40% LDL-C remains the same or increases No change in HDL-C Side GI upset and a fish burp Effects: Interventi on Trials: Lyon Heart Study (dietary), GISSI Prevenzione Trial, others
25

26
27
28

29 Emerging Risk Factors Lp(a) LDL size hscrp Homocysteine Procoagulant
30
, IDL, VLDL Surrogate for apoprotein B Optimum; add 30 mg/dl to")
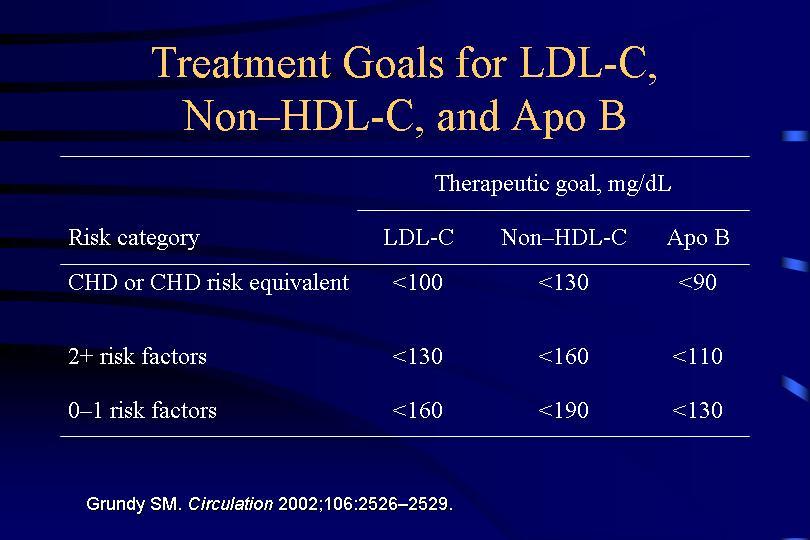
31 ATP III: Special Populations Older Adults, Younger Adults Utility of the non-hdl-cholesterol Total minus HDL-C Includes all atherogenic lipoproteins LDL-C, Lp(a), IDL, VLDL Surrogate for apoprotein B Optimum; add 30 mg/dl to LDL-C goals
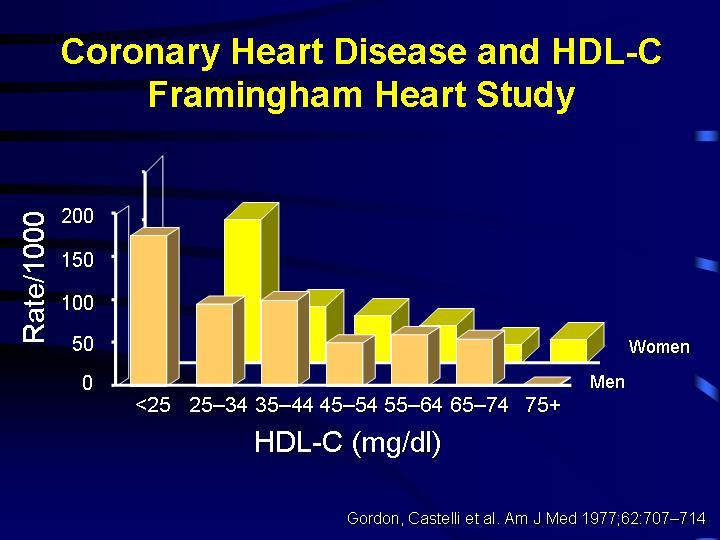
32 Are statins anti-atherosclerosis drugs and should they be used in high risk patients regardless of the LDL-C? The purpose of therapy is to reduce risk and prevent CV events In patients with dyslipidemia or isolated low HDL-C getting the LDL-C to goal takes priority The intensity of LDL-C treatment is determined by risk; when the LDL-C is at or below new goals then fibrates or niacin should be used to treat the non-hdl-c.
33 Use of statins in patients with hypertriglyceridemia TG range in statin trials: mg/dl Statin, fibrate or niacin? Statin effects best in patients with low HDL-C Reduced efficacy of statins in MetS? Use of information about emerging risk factors influences patient management. Can be used to increase or decrease the intensity of therapy of proven CHD risk factors No proven benefit of specifically treating the emerging risk factor

34 Lipid Management Strategy LDL-C At goal Intensify Rx goal goal Other lipid/lipoprotein abnormalities None nhdl-c Fibrates or Niacin HDL-C Niacin
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
DYSLIPIDEMIA PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
ANTIHYPERLIPIDEMIA. Darmawan,dr.,M.Kes,Sp.PD
 ANTIHYPERLIPIDEMIA Darmawan,dr.,M.Kes,Sp.PD Plasma lipids consist mostly of lipoproteins Spherical complexes of lipids and specific proteins (apolipoproteins). The clinically important lipoproteins, listed
ANTIHYPERLIPIDEMIA Darmawan,dr.,M.Kes,Sp.PD Plasma lipids consist mostly of lipoproteins Spherical complexes of lipids and specific proteins (apolipoproteins). The clinically important lipoproteins, listed
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Antihyperlipidemic Drugs
 Antihyperlipidemic Drugs Hyperlipidemias. Hyperlipoproteinemias. Hyperlipemia. Hypercholestrolemia. Direct relationship with acute pancreatitis and atherosclerosis Structure Lipoprotein Particles Types
Antihyperlipidemic Drugs Hyperlipidemias. Hyperlipoproteinemias. Hyperlipemia. Hypercholestrolemia. Direct relationship with acute pancreatitis and atherosclerosis Structure Lipoprotein Particles Types
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Clinical Dyslipidemia. Tom Ransom April 5, 2018
 Clinical Dyslipidemia Tom Ransom April 5, 2018 Disclosures Faculty/Presenter: Tom Ransom Relationships with commercial interests: Grants/research support: Research trials: Principal/Sub Investigator, CDHA,
Clinical Dyslipidemia Tom Ransom April 5, 2018 Disclosures Faculty/Presenter: Tom Ransom Relationships with commercial interests: Grants/research support: Research trials: Principal/Sub Investigator, CDHA,
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Drug regulation of serum lipids
 Drug regulation of serum lipids Foundations of Biomedical Science MEDS90001 Dr Michelle Hansen Pharmacology & Therapeutics mjhansen@unimelb.edu.au References Katzung, Basic & Clinical Pharmacology Ch 35
Drug regulation of serum lipids Foundations of Biomedical Science MEDS90001 Dr Michelle Hansen Pharmacology & Therapeutics mjhansen@unimelb.edu.au References Katzung, Basic & Clinical Pharmacology Ch 35
Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology
 Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Achieving Lipid Goals: 2008 Update. Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy
 Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
... CPE/CNE QUIZ... CPE/CNE QUESTIONS
 CPE/CNE QUESTIONS Continuing Pharmacy Education Accreditation The Virginia Council on Pharmaceutical Education is approved by the American Council on Pharmaceutical Education as a provider of continuing
CPE/CNE QUESTIONS Continuing Pharmacy Education Accreditation The Virginia Council on Pharmaceutical Education is approved by the American Council on Pharmaceutical Education as a provider of continuing
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID?
 Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Introduction Hyperlipidemia hyperlipoproteinemia Primary hyperlipidemia (Familial) Secondary hyperlipidemia (Acquired)
 Secondary hyperlipidemia (Acquired)") Introduction Hyperlipidemia, or hyperlipoproteinemia, is the condition of abnormally elevated levels of any or all lipids and/or lipoproteins in the blood. Hyperlipidemias are divided in primary and secondary
Introduction Hyperlipidemia, or hyperlipoproteinemia, is the condition of abnormally elevated levels of any or all lipids and/or lipoproteins in the blood. Hyperlipidemias are divided in primary and secondary
Antihyperlipidemic Drugs
 Antihyperlipidemic Drugs Lipid disorders: Disorders of lipid metabolism are manifest by elevation of the plasma concentrations of the various lipid and lipoprotein fractions (total and LDL cholesterol,
Antihyperlipidemic Drugs Lipid disorders: Disorders of lipid metabolism are manifest by elevation of the plasma concentrations of the various lipid and lipoprotein fractions (total and LDL cholesterol,
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Hyperlipidemia. Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi
 Hyperlipidemia Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi Outline The story of lipids Definition of hyperlipidemia Classification of hyperlipidemia Causes of hyperlipidemia
Hyperlipidemia Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi Outline The story of lipids Definition of hyperlipidemia Classification of hyperlipidemia Causes of hyperlipidemia
Accelerated atherosclerosis begins years prior to the diagnosis of diabetes
 Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Hyperlipidemia and Cardiovascular Disease. Kathmandu November 2010 Harold E. Lebovitz, MD, FACE
 Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
The new guidelines issued in PRESENTATIONS... Future Outlook: Changing Perspectives on Best Practice
 ... PRESENTATIONS... Future Outlook: Changing Perspectives on Best Practice Based on a presentation by Daniel J. Rader, MD Presentation Summary The guidelines recently released by the National Cholesterol
... PRESENTATIONS... Future Outlook: Changing Perspectives on Best Practice Based on a presentation by Daniel J. Rader, MD Presentation Summary The guidelines recently released by the National Cholesterol
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk?
 There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
CLINICAL IMPORTANCE OF LIPOPROTEINS
 25 Hyperlipidemias CLINICAL IMPORTANCE OF LIPOPROTEINS Raised levels of low-density lipoprotein (LDL) cholesterol and low levels of high density lipoprotein (HDL) cholesterol are independent risk factor
25 Hyperlipidemias CLINICAL IMPORTANCE OF LIPOPROTEINS Raised levels of low-density lipoprotein (LDL) cholesterol and low levels of high density lipoprotein (HDL) cholesterol are independent risk factor
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Antihyperlipidemic drugs
 Antihyperlipidemic drugs The clinically important lipoproteins are LDL low density lipoprotein, VLDL very low density lipoprotein, HDL high density lipoprotein. Hyperlipidemia may caused 1. by individual
Antihyperlipidemic drugs The clinically important lipoproteins are LDL low density lipoprotein, VLDL very low density lipoprotein, HDL high density lipoprotein. Hyperlipidemia may caused 1. by individual
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane
 Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER
 Management of hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER Background on Dyslipidemia in CKD In advanced chronic kidney disease (CKD),
Management of hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER Background on Dyslipidemia in CKD In advanced chronic kidney disease (CKD),
Lipid Management: Beyond LDL
 Lipid Management: Beyond LDL Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine University of Kentucky Overview Discuss the concept of residual risk Review current evidence-based medicine
Lipid Management: Beyond LDL Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine University of Kentucky Overview Discuss the concept of residual risk Review current evidence-based medicine
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Anti Hyperlipidemic Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Anti Hyperlipidemic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Lipoproteins Macromolecular complexes in the blood that transport lipids Apolipoproteins
Anti Hyperlipidemic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Lipoproteins Macromolecular complexes in the blood that transport lipids Apolipoproteins
Financial Disclosures
 1 Lipids in Type 2 Diabetes July 20, 2013 Abhimanyu Garg, M.D. Professor of Internal Medicine Chief, Division of Nutrition and Metabolic Diseases Distinguished Chair in Human Nutrition Research UT Southwestern
1 Lipids in Type 2 Diabetes July 20, 2013 Abhimanyu Garg, M.D. Professor of Internal Medicine Chief, Division of Nutrition and Metabolic Diseases Distinguished Chair in Human Nutrition Research UT Southwestern
Cholesterol Medicines New & Old: What to Use When
 Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Advances in Lipid Management
 Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Update on Atherosclerosis Treatment and Prevention
 Update on Atherosclerosis Treatment and Prevention Ronald D. Scott, MD Lipidology and Family Medicine West LA Med Center Regional CVD Colead Overview Lipids and CAD risk CVD is major killer and impacts
Update on Atherosclerosis Treatment and Prevention Ronald D. Scott, MD Lipidology and Family Medicine West LA Med Center Regional CVD Colead Overview Lipids and CAD risk CVD is major killer and impacts
Medical evidence suggests that
 COMBINATION THERAPY TO ACHIEVE LIPID GOALS David G. Robertson, MD* ABSTRACT Coronary heart disease (CHD) remains the leading cause of death in the United States despite recent advances in treatment and
COMBINATION THERAPY TO ACHIEVE LIPID GOALS David G. Robertson, MD* ABSTRACT Coronary heart disease (CHD) remains the leading cause of death in the United States despite recent advances in treatment and
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Hypertriglyceridemia. Ara Metjian, M.D. Resident s Report 20 December 2002
 Hypertriglyceridemia Ara Metjian, M.D. Resident s Report 20 December 2002 Review of Lipids Chylomicrons (CM): Dietary lipids absorbed through the GI tract are assembled intracellularly into CM. Very Low
Hypertriglyceridemia Ara Metjian, M.D. Resident s Report 20 December 2002 Review of Lipids Chylomicrons (CM): Dietary lipids absorbed through the GI tract are assembled intracellularly into CM. Very Low
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Podcast (Video Recorded Lecture Series): Lipoprotein Metabolism and Lipid Therapy for the USMLE Step One Exam
: Lipoprotein Metabolism and Lipid Therapy for the USMLE Step One Exam") Podcast (Video Recorded Lecture Series): Lipoprotein Metabolism and Lipid Therapy for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com Podcast (Video Recorded
Podcast (Video Recorded Lecture Series): Lipoprotein Metabolism and Lipid Therapy for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com Podcast (Video Recorded
Lipid Lowering Drugs. Dr. Alia Shatanawi
 Lipid Lowering Drugs Dr. Alia Shatanawi Atherosclerosis A form of arteriosclerosis characterized by the deposition of atheromatous plaques containing cholesterol and lipids on the innermost layer of the
Lipid Lowering Drugs Dr. Alia Shatanawi Atherosclerosis A form of arteriosclerosis characterized by the deposition of atheromatous plaques containing cholesterol and lipids on the innermost layer of the
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Lipid Management: Tools for Getting to the Goal
 ... PRESENTATIONS... Lipid Management: Tools for Getting to the Goal Based on a presentation by James M. McKenney, PharmD Presentation Summary The treatment of hypercholesterolemia in the United States
... PRESENTATIONS... Lipid Management: Tools for Getting to the Goal Based on a presentation by James M. McKenney, PharmD Presentation Summary The treatment of hypercholesterolemia in the United States
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Zuhier Awan, MD, PhD, FRCPC
 Metabolism, Atherogenic Properties and Agents to Reduce Triglyceride-Rich Lipoproteins (TRL) The Fifth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 8-11, 2019 Zuhier
Metabolism, Atherogenic Properties and Agents to Reduce Triglyceride-Rich Lipoproteins (TRL) The Fifth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 8-11, 2019 Zuhier
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention Center: Rooms 315 & 316
 Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Copy right protected Page 1
 CHOLESTEROL and TGs LOWERING DRUGS Introduction: Fat (lipids) are combinations (esters) of fatty acids plus an alcohol. The two main fats in the body are triglycerides (TGs) and cholesterol Triglycerides
CHOLESTEROL and TGs LOWERING DRUGS Introduction: Fat (lipids) are combinations (esters) of fatty acids plus an alcohol. The two main fats in the body are triglycerides (TGs) and cholesterol Triglycerides
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
( Diabetes mellitus, DM ) ( Hyperlipidemia ) ( Cardiovascular disease, CVD )
 ( Hyperlipidemia ) ( Cardiovascular disease, CVD )") 005 6 69-74 40 mg/dl > 50 mg/dl) (00 mg/dl < 00 mg/dl(.6 mmol/l) 30-40% < 70 mg/dl 40 mg/dl 00 9 mg/dl fibric acid derivative niacin statin fibrate statin niacin ( ) ( Diabetes mellitus,
005 6 69-74 40 mg/dl > 50 mg/dl) (00 mg/dl < 00 mg/dl(.6 mmol/l) 30-40% < 70 mg/dl 40 mg/dl 00 9 mg/dl fibric acid derivative niacin statin fibrate statin niacin ( ) ( Diabetes mellitus,
Treatment of Atherosclerosis in 2007
 Treatment of Atherosclerosis in 2007 Szilard Voros, M.D. Medical Director Cardiovascular MR and CT Piedmont Hospital, Piedmont Hospital Our Paradigm Genotype Phenotype Environment Atherosclerotic Disease
Treatment of Atherosclerosis in 2007 Szilard Voros, M.D. Medical Director Cardiovascular MR and CT Piedmont Hospital, Piedmont Hospital Our Paradigm Genotype Phenotype Environment Atherosclerotic Disease
High ( 50%) Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ
 Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
Treating Lipids for Prevention of CAD in Women: Matching Therapy to Risk
 TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
The Cardiovascular Institute Mount Sinai School of Medicine, New York
 The Cardiovascular Institute Mount Sinai School of Medicine, New York HDL YES HDL NO Juan Jose Badimon, Ph.D Professor of Medicine Director, Atherothrombosis Research Unit The Mount Sinai School of Medicine
The Cardiovascular Institute Mount Sinai School of Medicine, New York HDL YES HDL NO Juan Jose Badimon, Ph.D Professor of Medicine Director, Atherothrombosis Research Unit The Mount Sinai School of Medicine
CHOLESTEROL REDUCING MEDICATIONS. Five Main Categories. 1. Statins 2. Fibrates 3. Resins 4. Niacin 5. Cholesterol absorption inhibitor
 Page 1 of 5 PHA-GEN-002-2004 CHOLESTEROL REDUCING MEDICATIONS Five Main Categories 1. Statins 2. Fibrates 3. Resins 4. Niacin 5. Cholesterol absorption inhibitor Statins Also called HMG-CoA reductase inhibitors
Page 1 of 5 PHA-GEN-002-2004 CHOLESTEROL REDUCING MEDICATIONS Five Main Categories 1. Statins 2. Fibrates 3. Resins 4. Niacin 5. Cholesterol absorption inhibitor Statins Also called HMG-CoA reductase inhibitors
Imbalances in lipid components
 Drugs for Dyslipidemia Vivien Gam, Pharm.D. 1 Dyslipidemia Imbalances in lipid components High total cholesterol High LDL cholesterol Low HDL cholesterol High triglycerides Significant risk factor for
Drugs for Dyslipidemia Vivien Gam, Pharm.D. 1 Dyslipidemia Imbalances in lipid components High total cholesterol High LDL cholesterol Low HDL cholesterol High triglycerides Significant risk factor for
The New Gold Standard for Lipoprotein Analysis. Advanced Testing for Cardiovascular Risk
 The New Gold Standard for Lipoprotein Analysis Advanced Testing for Cardiovascular Risk Evolution of Lipoprotein Testing The Lipid Panel Total Cholesterol = VLDL + LDL + HDL Evolution of Lipoprotein Testing
The New Gold Standard for Lipoprotein Analysis Advanced Testing for Cardiovascular Risk Evolution of Lipoprotein Testing The Lipid Panel Total Cholesterol = VLDL + LDL + HDL Evolution of Lipoprotein Testing
Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention Center: Rooms 315 & 316
 Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
nicotinic acid 375mg, 500mg, 750mg, 1000mg modified release tablet (Niaspan ) No. (93/04) Merck
 No. (93/04) Merck") Scottish Medicines Consortium Resubmission nicotinic acid 375mg, 500mg, 750mg, 1000mg modified release tablet (Niaspan ) No. (93/04) Merck New formulation 6 January 2006 The Scottish Medicines Consortium
Scottish Medicines Consortium Resubmission nicotinic acid 375mg, 500mg, 750mg, 1000mg modified release tablet (Niaspan ) No. (93/04) Merck New formulation 6 January 2006 The Scottish Medicines Consortium
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
Aggressive Lipid Management for Diabetes
 Aggressive Lipid Management for Diabetes Practical Ways to Achieve Targets in Diabetes Care Keystone, CO July 16, 2011 Robert H. Eckel, M.D. Professor of Medicine Professor of Physiology and Biophysics
Aggressive Lipid Management for Diabetes Practical Ways to Achieve Targets in Diabetes Care Keystone, CO July 16, 2011 Robert H. Eckel, M.D. Professor of Medicine Professor of Physiology and Biophysics
New opportunities for targeting. multiple lipid pathways. Michel FARNIER, DIJON, FRANCE
 New opportunities for targeting multiple lipid pathways Michel FARNIER, DIJN, FRANCE Lipid lowering drug therapy 60s and 70s - nicotinic acid -resins 70s to 90s - fibrates the 90s - statins Coronary heart
New opportunities for targeting multiple lipid pathways Michel FARNIER, DIJN, FRANCE Lipid lowering drug therapy 60s and 70s - nicotinic acid -resins 70s to 90s - fibrates the 90s - statins Coronary heart
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Metabolism, Atherogenic Properties and Agents to reduce Triglyceride-Rich Lipoproteins Manfredi Rizzo, MD, PhD
 Metabolism, Atherogenic Properties and Agents to reduce Triglyceride-Rich Lipoproteins Manfredi Rizzo, MD, PhD Associate Professor of Internal Medicine Faculty of Medicine, University of Palermo, Italy
Metabolism, Atherogenic Properties and Agents to reduce Triglyceride-Rich Lipoproteins Manfredi Rizzo, MD, PhD Associate Professor of Internal Medicine Faculty of Medicine, University of Palermo, Italy
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Prospective Natural-History Study of Coronary Atherosclerosis
 Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
Fibrate and cardiovascular disease: Evident from meta-analysis. Thongchai Pratipanawatr
 Fibrate and cardiovascular disease: Evident from meta-analysis Thongchai Pratipanawatr ??? ย คห นใหม ย คห นกลาง ย คห นเก า ?? Statin era? ย คห นใหม ย คห นกลาง ย คห นเก า CURRENT ROLE OF FIBRATE What are
Fibrate and cardiovascular disease: Evident from meta-analysis Thongchai Pratipanawatr ??? ย คห นใหม ย คห นกลาง ย คห นเก า ?? Statin era? ย คห นใหม ย คห นกลาง ย คห นเก า CURRENT ROLE OF FIBRATE What are
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
In May 2001, the National Cholesterol. Effective Management of Patients With Dyslipidemia REPORT. Robert J. Lipsy, PharmD
 REPORT Effective Management of Patients With Dyslipidemia Robert J. Lipsy, PharmD Abstract Coronary heart disease (CHD) is the leading cause of morbidity and mortality in the United States. A direct relationship
REPORT Effective Management of Patients With Dyslipidemia Robert J. Lipsy, PharmD Abstract Coronary heart disease (CHD) is the leading cause of morbidity and mortality in the United States. A direct relationship