- 1 - EURETINA Uveitis Course, Milano, September 6, 2012 FLUORESCEIN & INDOCYANINE GREEN ANGIOGRAPHY FOR UVEITIS
|
|
|
- Molly Watts
- 6 years ago
- Views:
Transcription
1 - 1 - EURETINA Uveitis Course, Milano, September 6, 2012 FLUORESCEIN & INDOCYANINE GREEN ANGIOGRAPHY FOR UVEITIS Carl P. Herbort, MD, PD, fmer, FEBOphth Retinal and Inflammatory Eye Diseases Centre for Ophthalmic Specialised Care & University of Lausanne Lausanne, Switzerland carl.herb@bluewin.ch Prologue In recent years enormous progress has been achieved in investigational procedures for uveitis. One field where these advances are most patent is imaging with the occurence of new methods such as indocyanine green angiography (ICGA), ultrasound biomicroscopy (UBM) and optical coherence tomography (OCT) to cite only the most important. This tremendous increase in precision and accuracy in the assessment of the level and degree of inflammation and its monitoring comes in paprallel with the development of extremely potent and efficacious therapies. In view of these developments, our whole attitude in the appraisal and investigation of the uveitis patient have to be adapted and correctly reoriented integrating the recent developments and this is no different for ocular angiography. 1. Introduction (Figure 1) One of the essential procedures performed in uveitis to complement clinical appraisal of the patient with intraocular inflammation is angiographic investigation of the posterior segment. Angiography may be performed to confirm elements already revealed by clinical examination or other investigational methods such optical coherence tomography (OCT). A second reason to perform an angiography is to better grade the inflammation of the fundus. A third reason is to make a good baseline inventory of inflammatory involvement in order to subsequently use it for follow-up purposes. In follow-up situations, angiography is usually performed to monitor disease intensity and impact of therapy. Fluorescein angiography has been performed since more than 40 years. Because fluorescein sodium fluoresces in the wavelengths of the visible light it mainly gives information on the superficial structures of the fundus and therefore mostly only confirms signs already known to the clinician, as in most instances OCT is already available when fluorescein angiography is performed. Since about fifteen years a second angiographic procedure is available that uses indocyanine green, a dye that fluoresces in the infrared wavlengths and therefore allows imaging of the choroid that was poorly accessible to imaging beforehand. The procedure, in contrast to FFA, gives often additional information, undetected by clinical examination or FFA or OCT. Therefore, in order to make a proper

2 - 2 - assessement of inflammatory involvement in uveitis, ICGA is indispensable as it gives information otherwise lost. ICGA has very often a diagnostic value, which is rarely the case for FFA. For all these reasons, in most cases where angiographic work-up is decided and choroidal involvement cannot be excluded, dual FFA and ICGA should be performed. [1,2,3,4] Figure 1. Figure 1. Complementary information from fluorescein fundus angiography (FFA) and from indocyanine gree angiography (ICGA). FFA draws its advantages from the small size of the fluorescein molecule (picture top left) and gives information on all superficial structures of the fundus including preretinal and intraretinal hemorrhages, optic disc, retinal vessels, neovessels, retina, macula, subretinal space, RPE and chorioretinal atrophy, choriocapillaris and choroidal neovessels. ICGA draws its advantage from the infrared fluorescence of the ICG molecule and from its macromolecular behaviour. ICG extrudes from the largely fenestrated choriocapillaris (picture top right) and impregnates and is stuck in the choroidal stroma, so lowlighting inflammatory foci seen in dark because diffusion of ICG is impaired. CMO = cystoid macular oedema; CNV = choroidal neovessels; NVD = neovessels disc; NVE = neovessels elsewhere; RPE = retinal pigment epithelium. 2. Fundus fluorescein angiography (FFA) principles 2.1. The molecule : fluorescein sodium, (FNa) In fluoresein angiography a natural dye, fluorescein sodium (FNa) is injected intravenously in order to analyse the blood circulation of the ocular fundus, mainly the

3 - 3 - retina. Fluorescein sodium is a small hydrosolluble molécule of 354 daltons of which 80% is bound to proteins and 20% is free, the latter free form being responsible for the emission of fluorescing light. Two crucial principles characterize FNa. Firstly, fluorescein has a micromolecular behaviour. This means that flluorescein easily gets out, at the slightest breakdown of the hemato-retinal barrier, from the usually impermeable retinal vessels. It diffuses easily into tissues but is also quickly washed out. The other charcteristic is that fluorescein fluoresces at nanometers within the wavelenths of visible light and therefore is blocked by the retinal pigment epithelium (RPE), giving no useful information on the choroidal circulation and the choroidal compartment except on the choriocapillaris during the first of angiography.these characteristics determine the use and limitations of fluorescein angiography FFA signs (table 1) Fluorescein angiographic concepts classically described since more than forty years apply also to inflammatory diseases. Increased fluorescence can be due to three main mechanisms: (1) leakage producing pooling (in a space) or staining (in tissues); (2) increased transmission of fluorescence due to fundus atrophy with removal of the RPE producing larger hyperfluorescent areas or due to smaller window-defects produced by areas of RPE defects; (3) presence of abnormal vessels (retinal vessels or choroidal neovascular membranes). Decreased fluorescence can be due either to transmission decrease (blockage) or filling defect (vascular delayed perfusion or non perfusion). Table 1. Schematic diagram of fluorescein angiographic signs in uveitis
4 Fluorescein angiography performed for uveitis: methodological aspects. It is beyond the scope of this article to describe the equipment and instruments used. However there are some adjustments of the angiographic timing and technique for uveitis to be observed. Early frames are important and should be taken up to 2-3 minutes from the posterior pole as information from the choriocapillaris is available only up to about 60 seconds and will indicate whether there is choriocapillaris filling defect. Regarding the retinal circulation early frames give us information on the arteriovenous circulation time, the presence of disc neovessels (NVD), the presence of diffuse capillary leakage. At 5-7 minutes full 360 degree panoramas should be performed and therafter (10-12 minutes) again posterior pole frames are taken as well as frames of specific lesions identified during previous angiographic times. 3. FFA semeiology and use for uveitis The clinician should know what information he can expect from FFA and be aware that mainly superficial structures such as the optic nerve head, the retinal vessels, the retina and subretinal space will be highlighted by FFA. In addition FFA is an ideal tool to analyse the RPE and atrophic areas that can be seen thanks to the underlying fluorescence seen through window defects of the RPE or due to complete absence of the RPE screen in chorioretinal atrophy. FFA is an inadequate method to analyse the choroid as the RPE is a screen for the choroidal fluorescence. However, during early FFA frames (up to 60 ), because early choroidal fluorescence is so strong, information is also obtained on the choriocapillaris. Moreover choroidal fluorescence is at the base of the two main FFA concepts of window defect when choroidal fluorescence is seen through aeas of missing RPE and the concept of masking (blocking) effect in which choroidal fluorescein background fluorescence is attenuated or lost due to decreased transmision, which can be seen in black persons. The FFA signs will not be analysed according to angiographic principles exposed in table 1, but according to the anatomical structure, going antero-posteriorly from optic disc to choriocapillaris. Before analysing the different structures it should be specified that some posterior uveitis can cause retinal or preretinal hemorrhages producing hypofluorescence through a blocking effect Optic disc (figure 2) FFA is an adequate and sensitive method to detect inflammation of the optic discs which appear hyperfluorescent and in addition which leak in case of severe inflammation. FFA is especially helpful when clinical examination does not clearly reveal inflammation of the optic discs. Subclinical papillitis (hyperfluorescence) can be detected by FFA and this is especially useful in conditions known to be bilateral when the controlateral apparently uninvolved eye shows angiographic papillitis. FFA allows also usually to differentiate papillitis from papilloedma. In both conditions there are early dilated capillaries and late hyperfluorescence. The papilla is however more swollen in papilloedema than in papillitis and papillitis is more prone to produce leakage.
 which was confirmed by ICGA showing diffuse choroidal hyperfluorecence confirming the presence of posterior")
5 - 5 - Figure 2. Case of anterior scleritis (top left) with vasculitis shown by anterior ICGA (top middle) with no apparent clinical posterior involvement seen on fundus examination (top right). FFA clearly shows hyperfluorescent hot disc indicating posterior involvement (bottom left) which was confirmed by ICGA showing diffuse choroidal hyperfluorecence confirming the presence of posterior scleritis (bottom right) Retinal vessels FFA furnishes 3 types of informations on the retinal circulation including (1) imaging of inflammatory damage to vessel walls in retinal vasculitis, (2) display occlusive vasculopathy of retinal arteries or arterioles and (3) detection of retinal neovessels situated at the disc (NVD) or elsewhere in the retina (NVE) Retinal vasculitis or inflammatory vasculopathy. Retinal vessels normally are highly impermeable due to the tight junctions between endothelial cells and they usually don t leak. However the slightest inflammation of retinal vessel walls allows the small fluorescein molecule (359 daltons) to leak out of vessels and FFA is a therefore a very sensitive to detect retinal vessel inflammation mostly veins. (Figure 1) Conditions where leakage is a characteristic of the disease include Behçet s uveitis, intermediate uveitis of the pars planitis type, intermediate uveitis related to multiple sclerosis, intermediate uveitis of unknown cause and birdshot chorioretinopathy. (Figure 3) However every inflammatory focus of the fundus will have in its vicinity areas of leaking vessels. A special situation is represented by the particular vasculopathy of frosted branch angiitis with thick perivascular sheathing not only visible on FFA but also on fundus examination. Frosted branch angiitis can be associated with herpetic or cytomegalovirus especially in the contexte of AIDS, as well as with toxoplamic retinitis, SLE, Crohn s disease and leukemias and lymphomas. [5]

6 - 6 - Figure 3. FFA signs : Retinal vasculitis. 3a. Birdshot retinochoroidopathy. 3b. Severe vasculitis in Behçet s uveitis. 3c. Vasculitis in intermediate uveitis related to multiple sclerosis. 3d. Disc neovessels and retinal neovessels in intermediate uveitis of the pars planitis type Occlusive retinal vasculopathy Areas of non perfusion are best investigated with FFA that shows the extent of retina involved by the ischaemic process. Inflammatory conditions that often present retinal non perfusion include, without being exhaustive, Behçet s uveitis (Figure 4), sarcoidosis, systemic lupus erythematosus (SLE),Eales disease or more appropriatly called tubeculous hypersensitivity retinal vasculitis, IRVAN (Idiopathic retinal vasculitis, aneurisma and neuro-retinitis) and Susac s syndrome Retinal neovessels are best evidenced by FFA and can complicate any of the conditions that produce retinal non perfusion. [6] (Figure 3d) 3.3. Retina Peripheral retina FFA is the investigation of choice of retinal foci that appear hypofluorescent in the early phase and become progressively hyperfluorescent. Some conditions such as birdshot choriortinopathy produce profuse capillary leakage that produces bright and diffuse hyperfluorescence of the whole retina. The capillary leakage is sometimes such that there is not enough dye to mark the large veins. Gass interpreted this angiographic finding as perfusion delay. We know now, thanks to indocyanine green angiography, that the arteriovenous perfusion time is normal. (Figure 5) [7,8]

. The ICG frame (top left) shows that arteriovenous transit is already complete at 19 seconds. 45 seconds (bottom right frame).")
7 - 7 - Figure 4. Retinal non perfusion in a case of Behçet s uveitis in temporal inferior area. Figure 5. Birdshot chorioretinopathy. Birdshot is an inflammatory disease where the choroid and retina are primary independent targets of the inflammatory process. Retinal involvement can show profuse capillary leakage causing masive exudation into the retina at the origin of a pseudo-delay of arteriovenous circulation as large veins are still not opacified at 45 seconds (bottom right frame). The ICG frame (top left) shows that arteriovenous transit is already complete at 19 seconds. Birdshot is an inflammatory disease where the choroid and retina are primary independent targets of the inflammatory process. Retinal involvement can show profuse capillary leakage causing masive exudation into the retina at the origin of a pseudo-delay of arteriovenous circulation as large veins are still not opacified at 45 seconds (bottom right frame). The ICG frame (top left) shows that arteriovenous transit is already complete at 19 seconds Macula Macular ischaemia is best detected using FFA and has to be looked for in case of severe fundus inflammation such as Behçet s uveitis. [9,10] (Figures 6a & 6b) Cystoid macular oedema (CMO) CMO is visible by funduscopy if it is sufficiently pronounced. Until recently FFA was however recommended to have a precise image of the extent of CMO. Two grading
![- 8 - systems of CMO have been put forward by the groups of Miyake and Yanuzzi. [11,12] More recently optical cohrence tomography (OCT) has been used routinely for the evaluation of CMO.](/docs-images/77/76625613/images/8-0.jpg "In the field of inflammatory diseases however, FFA still has its place and should at least be performed in parallel with OCT at presentation of the patient, the follow-up being performed by repeated")
8 - 8 - systems of CMO have been put forward by the groups of Miyake and Yanuzzi. [11,12] More recently optical cohrence tomography (OCT) has been used routinely for the evaluation of CMO. In the field of inflammatory diseases however, FFA still has its place and should at least be performed in parallel with OCT at presentation of the patient, the follow-up being performed by repeated OCTs. Nevertheless, some of the inflammatory CMOs may not have any translation on OCT and are well identified by FFA. (Figure 6c & 6d) Figure 6. Figure 6. FFA signs : macular ischaemia & macular oedema. 6a & 6b. FFA (4a) of macula showing central hypofluorescence (enlargement of avascular zone) indicating macular ischaemia; change in tissue density well shown on a C-scan OCT (4c, right picture. Delineation of ischaemia is clearly shown on SLO fundus picture (4b, bottom left). 6c & 6d. Cystoid macular oedema well shown on FFA (4c) but not seen on spectral OCT (4d) 3.4. Subretinal space Retinal pooling of retinal origin Inflammation of the choriocapillaris mostly manifests itself by non perfusion with the consequence that the outer retina becomes ischaemic which produces in turn leakage from reacting inner retinal capillaries. In some of the inflammatory choriocapillaropathies (formerly classified under the term of white dot syndromes) the process can be very pronounced as in some cases of APMPPE (acute posterior multifocal placoid pigment epitheliopathy) causing massive intraretinal and subretinal
9 - 9 - pooling of fluorescein. Any other disease causing choroidal ischaemia can cause similar pooling. (Figure 7a) 3.4. Exudative retinal detachment (ERD) of choroidal origin Subretinal fluid can also originate directly from the choroid such as in VKH (Vogt- Koyanagi-Harada) disease where massive primary choroidal inflammation spills over to the retina and causes profuse leakage of liquid through the retinal pigment epithelium (RPE) forming exudative retnal detachments (ERD). Other diseases that can produce ERD include sympathetic ophthalmia and posterior scleritis. (Figures 7b & 7c) 3.5. Retinal pigment epithelium Inhomogeneity of background fluorescence (mottled RPE) (Figure 7d) Exudative retinal detachments produce RPE changes charcterised by loss of RPE cells causing small areas of window defects as well as clumping of cells causing masking effect. This alternation of loss and clumping of RPE gives a mottled aspect on early angiographic frames due to increased transmission of background choroidal fluorescence (window effect) in some areas together with decreased transmission of choroidal fluorescence (bloking effect). Very often the limits of the ERDs are well identified on FFA by a demarcation line between affected and normal RPE called high water marks. (Figure 7d) Hyperflurescent pinpoints (Figure 7b & 7c) The leaking points where fluid is passing from the choroid into the subretinal space accumulate a large amount of fluorescein dye and appear brightly hyperfluorescent on FFA (as well as on ICGA) which is explained by the deposition of fluorescein at this transit points. (Figures 7b & 7c) 3.6. Chorioretinal atrophy Chorioretinal atrophy can be limited to absence of the choriocapillaris-rpe complex or it can be a complete atrophy including the choroidal stroma. In the first case the area is characterised by early hypofluorescence with large stromal choroidal vessels that are hyperfluorescent and well visible on a dark background. In case of complete atrophy the whole area is dark on early frames becoming hyperfluorescent on late frames reflecting the bare sclera that is impregnated with fluorescein which easily diffuses in tissues due to its small size. Atrophic areas on the reverse appear hypofluorescent on ICGA as the large ICG molecular complex is not diffusing and does not impregnate the bare sclera. (Figure 7e) Figure 7. FFA signs : intraretinal pooling, exudative retinal detachment and atrophy 7a. FFA shows choriocapillaris non perfusion (top) in a patient diagnosed as APMPPE; gradually there is intraretinal and subretinal pooling (5a, two bottom pictures) due to extrusion of fluorescein coming from the inner retinal capillaries in response to outer retinal ischaemia due to choricapillaris non perfusion. 7b. FFA exudative retinal detachment (ERD) with hyperfluorescent pinpoints where choroidal leakge is ocurring in a case of VKH disease 7c. Same fundus frame on ICGA showing hyperfluorescence of ERD as well as hyperfluorescent pinpoints- 7d. FFA shows papillitis and mottled RPE with well defined limits between diseased and healthy RPE (high water marks) in a case of VKH. Left picture is an ICG frame of the same area showing numerous persisting HDDs indicating active disease.

10 - 10-7e. Chorioretinal atrophy, late hyperfluorescent on FFA and hypofluorescent on ICGA Choriocapillaris ( up to 60 ) Unless the RPE screen is very dark such as in black patients, the choriocapillaris fluorescence of the fluorescein dye can be seen despite the presence of the RPE in the early frames of fluorescein angiography when fluorescence is massive. These early frames can show areas of hypofluorescence due to choriocapillaris non perfusion. Alert clinicians understood and adequately interpreted these signs as due to choriocapillaris inflammation causing non perfusion well before ICGA became available and Deutman clearly indicated that disease in APMPPE was primarily due to the choriocapillaris and not to the RPE. [12] Indeed because the time of access to the choroid is limited with FFA, it is not possible to tell whether this hypofluorescence is due to perfusion delay or complete non perfusion of the choriocapillaris. This can only be shown by ICGA where choriocapillaris is accessible
 3.8. Choroidal Inflammatory neovascularisation (CNV) Inflammatory choroidal neovessels are mostly type 2 membranes and are therefore readily accessible to FFA, being above the RPE.")
11 during the whole angiographic sequence and the interpreation of FFA signs by Deutman for diseases such as APMPPE (and other white dot syndromes) were indeed confirmed by ICGA findings. [12,13] (Figure 7a) 3.8. Choroidal Inflammatory neovascularisation (CNV) Inflammatory choroidal neovessels are mostly type 2 membranes and are therefore readily accessible to FFA, being above the RPE. Occult choroidal neovessels are also detected by FFA showing progressive diffuse leakage in the macular area. In both these situations complementary ICGA is however recommended. On one hand it can delineate occult membranes and furthermore in case of CNV associated with a chorioretinal scars ICGA allows to differentiate between a recurrent inflammatory focus or CNV, the former being early hypofluorescent whreas the latter appears hyperfluorescent since early angiographic frames. ICGA is also mandatory in case of CNV associated with a choriocapillaritis such as multifocal choroiditis where it shows the extent of occult choriocapillaris non perfusion (iceberg constellation or complex) and hence the danger for CNV development.[14] Figure 8. Figure 8. FFA (ICGA) signs : inflammatory chorioretinal neovascularisation. 8a. FFA shows leaking and staining in area adjacent to toxoplasmic scar, before intravitreal Avastin(R) (left picture) and after (right picture); 8b. Same lesion before (L) and after (R) seen by ICGA. 6c. Same lesion seen by OCT, before (top picture) and after Avastin (two bottom OCTs).
 and fluorescein (354 daltons) molecules does not account for the specific angiogram pattern obtained with ICG as compared with fluorescein.")
 [15].")
12 The principles of indocyanine green angiography (ICGA) 4.1. The molecule : indocyanine green (ICG) Indocyanine green fluoresces at 830 nm and therefore is giving access to the choroidal vascular structures through the retinal pigment epithelium. The molecular weight difference between ICG (775 daltons) and fluorescein (354 daltons) molecules does not account for the specific angiogram pattern obtained with ICG as compared with fluorescein. Beside the different wavelength at which ICG fluoresces, the crucial difference between these two fluorescing molecules comes from their binding affinity to proteins. [15,16] The ICG molecule is nearly completely protein bound and predominantly so to large sized proteins (lipoproteins) [15]. Fluorescein leaks readily from slightly inflamed retinal vessels with minor damage to the blood-retinal barrier and readily impregnates tissues, whereas only major damage to retinal vessels allows ICG to leak. [17] In the choroid however ICG leaks unimpaired but slowly from the fenestrated choriocapillaris. [8] (Figure 9c & 9d ) During recirculation more and more ICG is entrapped in the choroidal tissue as the ICG-protein complex is only slowly reabsorbed into the circulation. Gradual impregnation of the choroid occurs with time causing intermediate and late choroidal background fluorescence. This choroidal impregnation by ICG fluorescence is disturbed by choroidal inflammatory lesions, causing areas of decreased or absent fluorescence surrounded by increased fluorescence due to leakage of large choroidal vessels. It is this alteration of the slow choroidal impregnation process that is the main parameter studied in ICGA performed for posterior uveitis. Figure 9. 9a 9b.

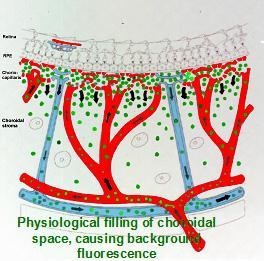

13 - 13-9c. 9d 9e
 (9a) is 98% protein bound forming a large macromolecilar ICG-protein complex (>58 000 daltons) (9b) that extrudes freely through the large fenestrations of the")
14 Figure 9. ICG angiographic principles. The ICG molecule (775 daltons) (9a) is 98% protein bound forming a large macromolecilar ICG-protein complex (> daltons) (9b) that extrudes freely through the large fenestrations of the choriocapillaris (9c) progressively impregnating the choroidal stroma (9d).This physiological hyperfluorescnece is impaired by two mechanisms producing hypofluorescent ICGA lesions : (1) choriocapillaris non perfusion (9e) occuring in inflammatory choriocapillaropathies and (2) mass effect due to space occupying lesions such as inflammatory foci here shown as the full-thickness stromal granuloma on (9f) explaining the hypofluorescence seen on ICGA Standard ICG angiographic protocol for inflammatory diseases A standard ICGA protocol to analyse choroiditis has been designed. [18] The angioraphic procedure comprises 3 main phases; the early phase up to 2-3 minutes showing superimposed retinal and choroidal large vessels and incipient exudation of the dye through the choriocapillaris into the choroidal stroma. The intermediate phase at about 10 minutes shows maximum choroidal stromal background fluorescence and the late phase at about minutes shows wash-out of the dye from the general circulation with the large choroidal vessels appearing dark against the background stromal fluorescence. [18] 4.3. Principles for the interpretation of ICGA in uveitis [18] When analysing ICG in posterior inflammatory disorders crucial differences with fluorescein angiography interpretation have to be born in mind to correctly analyse the images obtained. [19] During initial circulation, ICG is comparable to fluorescein showing the passage through arteriovenous compartments except that it shows superimposed retinal and choroidal circulations. The difference occurs during recirculation time when ICG is progressively leaking out from the fenestrated choriocapillaris, gradually and physiologically impregnating the whole choroidal thickness. This process can be altered in 2 ways that can be associated in the same disease, either there is a decreased fluorescence or an increased fluorescence.
 (Figure 10) or (2) by the impairment of the filling of the choroidal tissue by the ICG molecule because of the")

15 ICG hypofluorescence (Table 2) The impregnation of the choroidal space can be decreased or absent (hypofluorescence) either (1) by a decrease of the physiological extrusion of the ICG from the choriocapillaris (non perfusion or hypoperfusion, confluent geographic aspect) (Figure 10) or (2) by the impairment of the filling of the choroidal tissue by the ICG molecule because of the presence of space-occupying lesions (inflammatory foci, round even in size and regularly distributed). (Figure 9f) The latter lesions are hypofluorescent in the intermediate angiographic phase. If they remain hypofluorescent in the late phase this signifies that the inflammatory lesion occupies the whole thickness of the choroidal stroma. When lesions become isofluorescent in the late angiographic phase inflammation causes only partial thickness infiltrates. Therefore, in ICGA performed for inflammatory disorders, the main information is obtained less from the analysis of the early circulatory phase than from the analysis of the altered pattern of the filling of the choroidal space. Figure 10. Figure 10. ICGA signs of choriocapillaris non perfusion. Areas of patchy or geographic ICGA hypofluorescent areas of variable sizes present in the early, intermediate and late angiographic phases in a case of APMPPE, corresponding to confluent plaques of deep fundal discoloration, often leaving atrophic areas as seen in serpiginous choroiditis in the convalescent phase. Figure 11

16 Figure 11. Stromal inflammatory foci/granulomas in Vogt-Koyanagi-Harada disease. Typical even regularly distributed hypofluorescent evenly sized dark dots indicating numerous choroidal granulomas; Figure 12 Figure 12. Choroidal stromal vasculitis in Vogt-Koyanagi-Harada disease. Hypofluorescent dark dots surrounded by indistinct fuzzy choroidal vessels (top frames) showing normalisation after only 3 days of pulse intravenous corticosteroid injections (bottom frames); Table 2a. Schematic interpretation of ICGA hypofluorescence (Originally published and reproduced from Ophthalmology 1998; 105: ) ICG hyperfluorescence (Table 2b) Impregnation of the choroidal space can be enhanced (hyperfluorescence) by increased leakage from the larger choroidal vessels which adds to the physiological background fluorescence. The vessels appear fuzzy in the intermediate time frames and extrusion of the dye from large vessels causes late diffuse hyperfluorescence. (Figure 12)

17 Table 2b. Schematic interpretation of ICGA hyperfluorescence. In case of the presence of inflammatory foci in the choroidal stroma, hyperfluorescence is associated with hypofluorescent dark dots due to inflammatory infiltrates.. Hyperfluorescence occurs in two relevant situations, (1) diffuse late phase hyperfluorescence due to leakage from precapillary or larger non fenestrated choroidal vessels and (2) disc hyperfluorescence indicating severe inflammation. In most cases, unlike in fluorescein angiography where most pathologies produce hyperfluorescence, the lesions in ICGA are mostly seen in a negative dark pattern due to impaired physiological choroïdal fluorescence Fluorescein versus indocyanine green angiography When analysing ICGA it is of utmost importance to make abstraction in most inflammatory situations of two factors that are important in the interpretation of fluorescein angiograms, namely blockage and window defect. Because infrared fluorescence can be seen through structures that are a screen for visible light, blockage has to be considered only if the interfering structures in front of the choroid are sufficiently thick and/or heavily pigmented. Similarly the notion of window defect does not usually apply for ICGA as the retinal pigment epithelium does mostly not act as a screen as in fluorescein angiography Clinico-pathologic-angiographic correlations The pathologic processi at the origin of the ICGA images we see have been verified histopathologically for some of the diseases such as the primary stromal choroiditides Vogt- Koyanagi-Harada disease, sympathetic ophthalmia and birdshot chorioretinopathy, as well as the choroidal lesions of sarcoidosis, while others can still only be hypothesised, needing ICGA-clinico-pathologic correlations.
18 Relevance of ICGA in ocular inflammatory diseases Indocyanine green angiography showed occult choroidal lesions not shown by fundoscopy and/or fluorescein angiography in 100% of patients with a well-established diagnosis known to involve the choroid and these findings had an essential impact either on diagnosis or management in 12.3% of these cases, stressing the importance of ICGA for the proper management of most inflammatory processi of the back of the eye. [20] 5. Practical use of ICGA in uveitis Indocyanine green angiography is principally useful and has allowed imaging access to the choroidal compartment so far poorly explored. In addition to showing often missed choroidal involvement in every day practice it has allowed to understand choroidal inflammation, classifying choroiditis according to the structure that is preponderantly or initially involved and not simply according to fundus appearance of lesions. At the present stage of our knowledge there seem to be at least two main mechanisms of inflammation touching the choroid. [17] Table 3. Two main ICGA derived lesional mechanisms determine the classification of choroiditis : 1. Choriocapillaris inflammation (primary inflammatory choriocapillaropathies) - MEWDS / AIBSE - APMPPE - Multifocal choroiditis / PIC - Serpiginous choroiditis - Rare entities : AMN, AZOOR 2. Stromal inflammation (stromal choroiditis) further subdivided into 2 categories 2.1. Primary obligatory stromal choroiditiis - Vogt-Koyanagi-Harada disease - Sympathetic Ophthalm - Birdshot choriortinopathy 2.2. Stromal choroiditis as a random location of a systemic disease - Sarcoidosis - Tuberculosis - Syphilis - Other infectious choroiditides 5.1. Primary inflammatory choriocapillaropathy (PICCP) (White dot syndromes) This first group of diseases, formerly mostly included in the inadequate term of white dot syndromes results from inflammation at the level of the choriocapillaris causing areas of choriocapillaris non perfusion and its ischaemic consequences both at the level of the choroid but also at the level of the outer retina that depends on the choriocapillaris for oxygen and nutrients. Acute posterior multifocal placoid pigmentary epitheliopathy (APMPPE) is a disease typically illustrating this type of choroidal inflammation Angiographic signs in inflammatory choriocapillaropathies [21,22) Indocyanine green angiographic signs in inflammatory choriocapillaropathies are well determined and have contributed to the recognition of the common mechanism involved and to regroup these entities formerly classified under the term of white dot syndromes The following ICGA signs have to be looked for:

19 The hallmark sign of inflammatory choriocapillaropathy is patchy or geographic ICGA hypofluorescent areas of variable sizes present in the early, intermediate and late angiographic phases but usually more clearly visible on the late frames, indicating choriocapillaris non-perfusion or hypoperfusion. (Figure 13) 2. Complete or partial regression of the ICGA hypofluorescence or absence of regression in the convalescent phase. The areas remaining hypofluorescent in the convalescent phase represent chorioretinal atrophy and correspond to areas of window effect and masking effect on fluorescein angiography 3. In diseases with a progressing course such as serpiginous choroiditis, ICGA can show diffuse choroidal hyperfluorescence at the edges of the progressing lesions in areas having no translation on fundoscopy or fluorescein angiography. (Figure 12) Whereas the ICGA signs are quite uniform, the FA angiographic signs depend on the severity and extension of the choriocapillaris non perfusion and on the outer retinal damage. 1. On FA there is likewise early hypofluorescence showing the choriocapillaris non perfusion identified on ICGA. 2. Depending on the severity of the choriocapillaris non perfusion seen on ICGA, late FA frames either show no hyperfluorescence (for instance in mild MEWDS), discrete patchy late hyperfluorescence seen in MEWDS or extensive late hyperfluorescence seen in APMPPE. (Figure 13) To understand the genesis of the FA signs it is important to be aware that late FA fluorescence is coming from retinal vessels overlying areas of ischaemic outer retina that present increased permeability in response to the ischemia due to choriocapillaris non perfusion. 3. In the convalescent phase there is a delayed regression of FA signs (hyperfluorescence & staining) as compared to the regression of ICGA signs. In case of chorioretinal atrophy window effect and masking effect due to chorioretinal scarring are seen. Any severe inflammation in an adjacent structure to the choriocapillaris (retina or choroidal stroma) can cause inflammation at the level of the choriocapillaris and produce similar angiographic signs. In that situation we speak of secondary inflammatory choriocapillaropathy. Figure 13. Figure 13. Choriocapillaris non perfusion in a case of APMPPE/AMIC. Choriocapillaris non perfusion is shown by patchy geographic areas of hypofluorescence in the intermediate phase of angiography (top right picture) and in the late angiographic phase (bottom left picture) that resolve almost completely in the convalescent stage of disease 2 months later (bottom right picture). The late fluorescein frame on the top left shows hyperfluorescence, corresponding to the ICG areas of choriocapillaris non perfusion that can only be explained by leakage from the capillaries of the inner retina in response to ischaemic signals from the outer retina.
 shows many more involved areas than shown by fluorescein angiography (left quartet of pictures) and shows hyperfluorescence around progressing lesions. 5.2.")
20 Figure 14. Figure 14. Diffuse perilesional choroidal hyperfluorescence in subclinically progressing serpiginous choroiditis. ICGA (right quartet of pictures) shows many more involved areas than shown by fluorescein angiography (left quartet of pictures) and shows hyperfluorescence around progressing lesions Stromal choroiditis In the second group of diseases, the primary mechanism is the development of inflammatory foci, mostly granulomatous at the level of the stroma appearing hypofluorescent on ICGA, usually associated with inflammation of larger non-fenestrated stromal vessels appearing on ICGA as fuzzy vessels in the intermediate phase followed by diffuse late choroidal hyperfluorescence. Vogt-Koyanagi-Harada disease or birdshot chorioretinopathy are typical illustrations of this type of choroidal inflammation. Although the mechanism is completely different from the first type of diseases, these conditions have also been included by some authors in the white dot syndromes. [23] Angiographic signs in stromal choroiditis Since the availability of ICGA it has become possible to investigate stromal choroidal inflammatory disease in a more subtle way and detect lesions even at an early, often subclinical stage of evolution not accessible so far to investigational tests. [24] The primary lesion of stromal choroiditis is the inflammatory, mostly granulomatous focus. Depending on the extension of the granuloma, full-thickness or partial thickness, the ICGA image will be influenced. In contrast to primary inflammatory choriocapillaropathies, the mechanism of stromal choroiditis has been proven with the help of anatomo-clinicalangiographic correlations. Histopathology has been available since some time for Vogt- Koyanagi-Harada disease, sympathetic ophthalmia and sarcoidosis and recently granulomas have been found in an autopsy case of birdshot chorioretinopathy. [25-27] Different pathologic behaviours have to be distinguished to better understand the lesions seen by fundus examination and FA and ICG angiography. At least two lesional events can take place in the choroidal stroma.the first group of diseases includes the entities where the choroidal stroma is the elective target of the inflammatory process. They can be called the primary obligatory choroiditis and include Vogt-Koyanagi-Harada disease, sympathetic ophthalmia and birdshot chorioretinopathy.their lesions are characterised by multiple even sized regularly distributed lesions on ICGA accompanied by leaking hyperfluorescent fuzzy choroidal stromal vessels. (Figures 11 and 12) The second group of diseases include systemic inflammatory or infectious diseases that can involve the choroid by chance,
 The specific ICGA signs that can be seen in diverse proportions according to the the type of disease on which this classification relies are the following : 1.")
 or becoming isofluorescent in the late phase")
21 including sarcoidosis, tuberculosis and syphilis. Unlike the first group the size of the lesions are uneven and distributed more at random. (Figure 15) The specific ICGA signs that can be seen in diverse proportions according to the the type of disease on which this classification relies are the following : 1. Even, regularly distributed ICGA hypofluorescent dots in case of birdshot chorioretinopathy, Vogt-Koyanagi-Harada disease and sympathetic ophthalmia or diversely sized hypofluorescent areas in case of sarcoidosis or tuberculosis present in the early and intermediate phase remaining hypofluorescent in the late phase (full thickness inflammatory foci) or becoming isofluorescent in the late phase in case of partial thickness inflammatory foci, indicating a mass effect. [18] 2. Around the inflammatory lesions seen as hypofluorescent dark dots the larger choroidal vessels lose their normal aspect and appear fuzzy indicating choroidal vasculitis that allows pathologic extrusion of the ICG-complex at the origin of late diffuse choroidal hyperfluorescence. [18] (Figure 10) Figure 15a. Figure 15b. Figure 15. Choroiditis in Sarcoidosis. Unevenly sized randomly distributed lesions (15a) well seen in the intermediate ICG angiographic phase (15a, middle and left frames) and disappearing in the late phase (right frame), indicating that these presumed granuloma are of partial thickness not filling the stroma from sclera to choriocapillaris. The lesions are hardly visible on fluorescein angiography (15b) Additional ICGA signs Apart from the signs that allow to explore choroidal inflammation, whether at the level of the choriocapillaris or at the level of the choroidal stroma, additional ICGA signs have been reported. ICGA was shown to demonstrate pure choroidal vasculitis without choroidal foci (hypofluorescent dak dots) in acute initial attacks of inflammation in Behçet s disease.
![- 22 - Subsequently, when patients are under systemic therapy choroidal involvement can no longer be detected. [28,29] The optic disc is usually non fluorescent in ICGA angiography.](/docs-images/77/76625613/images/22-0.jpg "In case of severe inflammatory disease disc hyperfluorescence is a characteristic finding usually present in all types of hyperacute diseases such as initial attacks of Behçet s uveitis and VKH")
22 Subsequently, when patients are under systemic therapy choroidal involvement can no longer be detected. [28,29] The optic disc is usually non fluorescent in ICGA angiography. In case of severe inflammatory disease disc hyperfluorescence is a characteristic finding usually present in all types of hyperacute diseases such as initial attacks of Behçet s uveitis and VKH disease, representing also a parameter to monitor the effect of therapeutical intervention. In a group of VKH patients, it was shown to regress within one month after introduction of systemic therapy. [30] ICGA was also shown to be useful in distinguishing reactivation of a retinal focus of toxoplasmosis at the border of a scar versus development of CNV which, instead of being hypofluorescent in the early angiographic phase, presents as early hyperfluorescent, allowing thus to eliminate the possibility of reactivation of the inflammatory focus ICGA implications in the practical care of the uveitis patient Precise assessment of choroidal inflammatory involvement The choroid is the starting point of the inflammation in many diseases including MEWDS, APMPPE, multifocal choroiditis, serpiginous choroiditis, VKH, sympathetic ophthalmia and birdshot chorioretinopathy and is participating in the inflammatory process in many other diseases such as sarcoidosis, tuberculosis, syphilis, toxoplasmosis, posterior scleritis and many more which have extensively been analysed by ICGA. [31-41] A reliable inventory of fundus inflammatory involvement can therefore only be performed with the help of ICGA. It will contribute essentially to the assessement of disease extension in those conditions involving the choroid. Figure 16. Figure 16. Multifocal choroiditis (the iceberg effect or constellation). Fundus pictures show minimal signs limited to faint depigmentation (16a, black arrows) and FFA shows absolutely no abnormalities (16b), whereas ICGA shows extensive choriocapillaris involvement with large geographic areas of non perfusion (16c & 16 d) which we now know to be a risk factor for CNV, which the patient developed one year later as seen on FFA (16e) and fundus images (bottom right).
 and the preponderant part of the disease can only be followed by ICGA.")
23 In some diseases such as MEWDS only choroidal signs can be present and in others the clinically apparent part of the disease such as in multifocal choroiditis is only the peak of the iceberg (iceberg constellation) and the preponderant part of the disease can only be followed by ICGA. (Figure 16) In diseases originating from the choroid such as VKH disease the only way to detect subclinical disease is to perform ICGA. (Figure 17) Figure 17 Figure 17. ICGA guided treatment of VKH disease VKH at presentation : Numerous hypofluorescent dark dots indicating granulomatous foci in the choroid as well as fuzzy choroidal vessels indicating choroidal vasculitis. Following intravenous pulse steroid therapy followed by high dose oral steroids HDDs disappear completely and choroidal vessels regain a normal pattern (17.2). Upon tapering there is recrudescenc of subclinical choroidal disease (17.3.), that prompts reincrease of oral steroid therapy and introduction of azathioprine. After slow tapering of steroid therapy first followed by tapering of azathioprine over 2 years the patient remains recurrence free.(17.4) Diagnostic contribution of ICGA Unlike for FFA, it is not rare that ICGA gives the essential contribution that leads to the diagnosis. This can be the case for patients with MEWDS that have minimal translation in fundus signs or FFA signs. Early birdshot chorioretinopathy can only be diagnosed using ICGA as the early lesions are hypofluorescent dark dots indicating subclinical granulomas that can only be detected by ICGA. These ICGA lesions often precede the typical oval shaped depigmented birdshot lesions by several months or even years. (figure 18) ICGA monitoring of disease evolution and response to therapy As choroidal lesions can only be detected by ICGA, it is oviously the recommended modality to monitor the evolution and to evaluate the impact of treatment on choroidal inflammatory processi. [30] In case of VKH disease, clinical disease, meaning inflammation involving extrachoroidal structures accesible to fundus observation,to OCT and FFA, can be followed by classical means. However once clinical disease is under control, it has been shown that subclinical disease is
 Figure 18.")
24 ongoing resulting in almost 100% of cases in sunset-glow-fundus (SGF) the witness of ongoing disease destroying choroidal pigment. It was recently shown that ICGA guided treatment of VKH could avoid evolution towards SGF when treating also subclinical disease shown by ICGA. [42] (Figure 17) Figure 18. Figure 18. The essential role of ICGA for early diagnosis of birdshot retinochoroiditis. Patient in his mid-forties presenting with blurred vision OS due to the presence of vitritis (top right). FFA shows retinal vasculitis OS of large veins and small vessels (bottom middle). The right eye seems not affected (top left). However ICGA shows numerous hypofluorescent dark dots on tthe left (bottom right) but also on the right (bottom left), typical for birdshot retinochoroidopathy. 6. Summarizing remarks Fluorescein angiography is performed routinely in inflammatory ocular diseases which is probably justified in order to make a good evaluation of inflammation and to use it as a follow-up parameter for superficial fundus structures. Except for the evaluation of retinal vessels it mostly does not add essential information to clinical examination and OCT. In contrast, ICGA often furnishes additional information otherwise undetectable on the choroidal compartment. Several choroidal diseases such as inflammatory choriocapillaropathies (MEWDS, multifocal choroiditis and APMPPE and others) present with the iceberg constellation meaning minimal signs seen on funduscopy or FFA with extensive choroidal involvement. Therefore, except for conditions such as pars planitis or Behçet s disease where choroiditis is absent or insignificant, dual FFA and ICGA should be performed for the assessement and follow-up of posterior uveitis if angiographic analysis is deemed necessary.
25 A dual FFA/ICGA angiographic scoring method has recently been proposed for that very purpose. [43] 7. Conclusion Gradually the precision of assessement of intraocular inflammation and its complications have become much more precise in as much as new technical developments such as ICGA who go beyond the information given by more established methods are integrated into the choice of complementary investigations. In contrast to other new investigational modalities such as OCT that represent an improved visualisation of lesions that often are already accessible with other means such as funduscopy or FA, ICGA shows additonal lesions, mainly in the choroid, that are usually not accessible or demonstrated by other means. The choroid is responsible for posterior inflammation in an equal if not higher proportion of cases when compared to the superficial structures as the retina. Therefore, in cases where choroidal involvement is suspected, ICGA is as important if not more imporant than FA and dual ICGA /FA angiography is highly recommended in such cases. References 1. De Laey JJ. Fluorescein angiography in posterior uveitis. Int Ophthalmol Clin 1996; 35: Brancato R, Trabucchi G. Fluorescein and indocyanine green angiography in vascular chorioretinal diseases. Semin Ophthalmol 1998; 13: Herbort CP. Posterior uveitis : new insights given by indocyanine green angiography. Eye 1998; 12: Herbort CP, Borruat FX, de Courten C, Jaccard L. Angiographie au vert d'indocyanine dans les uvéites postérieures. Klin Monatsbl Augenheilk. 1996; 208 : Walker S, Iguchi A, Jones NP. Frosted branch angeitis: a review. Eye 2005; Graham EM, Stanford MR, Shilling JS, Sanders MD. Neovascularisation associated with posterior uveitis. Br J Ophthalmol 1987; 71: Gass JDM. Vitiliginous chorioretinitis. Arch Ophthalmol 1981; 99: Guex-Crosier Y, Herbort CP. Prolonged retinal arteriovenous circulation time by fluorescein but not by indocyanine green angiography in birdshot chorioretinopathy. Ocular Immunol and Inflamm 1997; 5 : Bentley CR, Stanford M, Shilling JS, Sanders MD, Graham EM. Macular ischaemia in posterior uveitis. Eye 1993; 7: Yilmaz G, Akova Y, Aydin P. Macular ischemia in Behçet s disease. Eye 2000; 14: Miyake K. Prevention of cystoid macular edema after cataract extraction by topical indomethacin, preliminary report. Graefe s Arch Clin Exp Ophthalmology 1977; 203: Yannuzzi LA. A perspective on the treatment of aphakic cystoid macular edema. Surv Ophthalmol 1984; 28; Deutman AF, Lion F. Choriocapillaris nonperfusion in acute multifocal placoid pigment epitheliopathy. Am J Ophtalmol 1977; 84: Machida S, Fujiwara T, Murai K, Kubo M, Kurosaka D, Idiopathic choroidal neovascularisation as an early manifestation of inflammatory chorioretinal diseases. Retina 2008; 28: Baker KJ. Binding of sulfobromophthalein (BSP) sodium and indocyanine green (ICG) by plasma alpha-1 lipoproteins. Proc Soc Exp Biol Med 1966; 122 : Lim JI, Flower RW. Indocyanine green angiography. Int Ophthalmol Clin 1995; 35 (4) Bouchenaki N, Cimino L, Auer C, Tran VT, Herbort CP. Assessement and classification of choroidal vasculitis in posterior uveitis using indocyanine green angiography. Klin Monatsbl Augenheilkd 2002; 219: Herbort CP, Guex-Crosier Y, LeHoang P. Schematic interpretation of indocyanine green angiography Ophthalmology 1994; 2 : Herbort CP, Bodaghi B, LeHoang P. Angiographie au vert d'indocyanine au cours des maladies inflammatoires : principes, interpretation schématique, sémiologie et intérêt clinique. J Fr Ophtalmol 2001; 24:
26 Herbort CP, Auer C, Wolfensberger TJ, Ambresin A, Bouchenaki N. Contribution of indocyanine green angiography (ICGA) to the appraisal of choroidal involvement in posterior uveitis. Invest Ophthalmol Vis Sci 1999; 40 (4) : S Cimino L, Auer C, Herbort CP. Sensitivity of indocyanine green angiography for the follow-up of active inflammatory choriocapillaropathies. Ocular Immunologie and Inflammation 2000; 8: Cimino L, Mantovani A, Herbort CP. Primary inflammatory choriocapillaropathies. In: Essentials in Ophthalmology: Uveitis and Immunological Disorders. Edited by Pleyer U, Mondino B (Eds.). Berlin, Heidelberg,New York : Springer; pp Ben Ezra D, Forrester JV. Fundal white dots : the spectrum of a similar pathological process. Br J Ophthalmol 1995; Bouchenaki N, Herbort CP. Stromal choroiditis. In: Essentials in Ophthalmology: Uveitis and Immunological Disorders. Pleyer U, Mondino B (Eds.). Berlin, Heidelberg,New York : Springer; pp Chan CC, Ben Ezra D, Hsu SM, Palestine AG, Nussenblatt RB. Granulomas in sympathetic ophthalmia and sarcoidosis. Arch Ophthalmol 1985; 103: Inomata H, Sakamoto T. Immunohostochemical studies of Vogft-Koyanagi-Harada disease with sunset sky fundus. CurrEye Res 1990; 95: Gaudio PA, Kaye DB, Brooks Crawford J. Histopathology of birdshot retinochoroidopathy. Br J Ophthalmol 2002; 86: Klaeger A, Tran VT, Hiroz CA, Morisod L, Herbort CP. Indocyanine green angiography in Behçet s uveitis. Retina 2000; 20 : Atmaca LS, Sonmez PA. Fluorescein and indocyanine green angiography findings in Behçet s disease. Br J Ophthalmol 2003; 87 : Herbort CP, Mantovani A, Bouchenaki N. Indocyanine green angiography in Vogt-Koyanagi-Harada disease: angiographic signs and utility in patient follow-up. Int. Ophthalmol 2007; 27: Bouchenaki N, Herbort CP. The contribution of indocyanine green angiography to the appraisal and management of Vogt-Koyanagi-Harada disease. Ophthalmology 2001; 108: Howe L J, Woon H, Graham E M, Fitzke F, Bhandari A, Marshall J. Choroidal hypoperfusion in acute posterior multifocal placoid pigment epitheliopathy. Ophthalmology 1995; 102 : Park D, Shatz H, McDonald R, Johnson RN. Indocyanine green angiography of acute multifocal posterior placoid pigment epitheliopathy. Ophthalmology 1995; 102: Slakter JS, Giovannini A, Yannuzzi LA, Scassellati-Sforzolino B, Guyer DR, Sorenson JA, Spaide RF, Orlock D. Indocyanine green angiography of multifocal choroiditis. Ophthalmology 1997; 104: Bernasconi O, Auer C, Zografos L, Herbort CP. Indocyanine green findings in sympathetic ophthalmia. Graefe s Arch Clin Exp Ophthalmol 1998; 236: Fardeau C, Herbort CP, Kullman N, Quentel GG,LeHoang P. Indocyanine green angiography in birdshot chorioretinopathy. Ophthalmology 1999; 106: Herbort CP, Probst K, Cimino L, Tran VT. Differential inflammatory involvement in retina and choroïd in birdshot chorioretinopathy. Klin Monatsbl Augenheilkd 2004; 221: in press. 38. Wolfensberger TJ, Herbort CP (1999) Indocyanine green angiographic features in ocular sarcoidosis. Ophthalmology 1999; 106: Wolfensberger TJ, Piguet B, Herbort CP. Indocyanine Green angiographic features in tuberculous chorioretinitis. Am.J. Ophthalmol. 1999, 127: Auer C, Bernasconi O, Herbort CP. Toxoplasmic retinochoroiditis: new insights provided by indocyanine green angiography. Am J Ophthalmol 1997; 123 : Auer C, Herbort CP. Indocyanine green angiographic features in posterior scleritis. Am J Ophthalmol 1998; 126: Bouchenaki N, Herbort CP. Indocyanine green angiography (ICGA) in the assessement and follow-up of choroidal inflammation in active chronically evolving Vogt-Koyanagi-Harada disease. In Uveitis in the third millenium, Dodds EM, Couto CA (eds), Elsevier Scienc B.V. 2000, pp Tugal-Tutkun I, Herbort CP, Khairallah M, The Angiography Scoring for Uveitis Group (ASUWOG). Scoring of dual fluorescein and ICG inflammatory angiographic signs for the grading of posterior inflammation (dual fluorescein and ICG angiographic scoring system for uveitis). Int Ophthalmol 2008; Epub ahead of print.
Misdiagnosed Vogt-Koyanagi-Harada (VKH) disease and atypical central serous chorioretinopathy (CSC)
 disease and atypical central serous chorioretinopathy (CSC)") HPTER 12 Misdiagnosed Vogt-Koyanagi-Harada (VKH) disease and atypical central serous chorioretinopathy (S) linical Features VKH disease is a bilateral granulomatous panuveitis often associated with exudative
HPTER 12 Misdiagnosed Vogt-Koyanagi-Harada (VKH) disease and atypical central serous chorioretinopathy (S) linical Features VKH disease is a bilateral granulomatous panuveitis often associated with exudative
Moncef Khairallah, MD
 Moncef Khairallah, MD Department of Ophthalmology, Fattouma Bourguiba University Hospital Faculty of Medicine, University of Monastir Monastir, Tunisia INTRODUCTION IU: anatomic form of uveitis involving
Moncef Khairallah, MD Department of Ophthalmology, Fattouma Bourguiba University Hospital Faculty of Medicine, University of Monastir Monastir, Tunisia INTRODUCTION IU: anatomic form of uveitis involving
LUCY HOWE, MILES STANFORD, ELIZABETH GRAHAM, JOHN MARSHALL
 Indocyanine green angiography in inflammatory eye LUCY HOWE, MILES STANFORD, ELIZABETH GRAHAM, JOHN MARSHALL disease Abstract Purpose The choroid plays an integral role in the evolution of a number of
Indocyanine green angiography in inflammatory eye LUCY HOWE, MILES STANFORD, ELIZABETH GRAHAM, JOHN MARSHALL disease Abstract Purpose The choroid plays an integral role in the evolution of a number of
Case Report: Indocyanine Green Dye Leakage from Retinal Artery in Branch Retinal Vein Occlusion
 Case Report: Indocyanine Green Dye Leakage from Retinal Artery in Branch Retinal Vein Occlusion Hiroki Fujita, Kyoko Ohno-Matsui, Soh Futagami and Takashi Tokoro Department of Visual Science, Tokyo Medical
Case Report: Indocyanine Green Dye Leakage from Retinal Artery in Branch Retinal Vein Occlusion Hiroki Fujita, Kyoko Ohno-Matsui, Soh Futagami and Takashi Tokoro Department of Visual Science, Tokyo Medical
OCT Angiography in Primary Eye Care
 OCT Angiography in Primary Eye Care An Image Interpretation Primer Julie Rodman, OD, MS, FAAO and Nadia Waheed, MD, MPH Table of Contents Diabetic Retinopathy 3-6 Choroidal Neovascularization 7-9 Central
OCT Angiography in Primary Eye Care An Image Interpretation Primer Julie Rodman, OD, MS, FAAO and Nadia Waheed, MD, MPH Table of Contents Diabetic Retinopathy 3-6 Choroidal Neovascularization 7-9 Central
Differential diagnosis of posterior uveitis
 Differential diagnosis of posterior uveitis Diagnostic approach 45-year old male. Floaters and decreased vision since 1 week Fever, lymphadenopathy, myalgias, night sweats, two months ago Oral ulcer sporadically
Differential diagnosis of posterior uveitis Diagnostic approach 45-year old male. Floaters and decreased vision since 1 week Fever, lymphadenopathy, myalgias, night sweats, two months ago Oral ulcer sporadically
White-Spot Syndromes of the Retina Lee Jampol, M.D. Chicago, IL
 Objectives At the conclusion of the program, the attendees will be able to: 1. recognize the various white-spot syndromes of the retina 2. initiate appropriate diagnostic tests of patients with the white-spot
Objectives At the conclusion of the program, the attendees will be able to: 1. recognize the various white-spot syndromes of the retina 2. initiate appropriate diagnostic tests of patients with the white-spot
Leo Semes, OD, FAAO UAB Optometry
 Leo Semes, OD, FAAO UAB Optometry Safe; inert Has long track record - over 45 years Mixes with plasma and highlights blood vessel compromise Using specific exciting (490 nm)and absorption (510 nm) filters
Leo Semes, OD, FAAO UAB Optometry Safe; inert Has long track record - over 45 years Mixes with plasma and highlights blood vessel compromise Using specific exciting (490 nm)and absorption (510 nm) filters
Fluorescein Angiography
 Last revision: October 2011 by Luis Arias Fluorescein Angiography Authors: Luis Arias, MD Hospital Universitari de Bellvitge - University of Barcelona. Spain Jordi Monés, MD Institut de la Màcula i de
Last revision: October 2011 by Luis Arias Fluorescein Angiography Authors: Luis Arias, MD Hospital Universitari de Bellvitge - University of Barcelona. Spain Jordi Monés, MD Institut de la Màcula i de
Why Is Imaging Critical in My Uveitis Practice?
 Why Is Imaging Critical in My Uveitis Practice? Dilraj S. Grewal, MD Developed in collaboration Imaging Is the Backbone of Uveitis Workup and Monitoring Treatment Response FP FAF B- scan Multimodal Imaging
Why Is Imaging Critical in My Uveitis Practice? Dilraj S. Grewal, MD Developed in collaboration Imaging Is the Backbone of Uveitis Workup and Monitoring Treatment Response FP FAF B- scan Multimodal Imaging
Clinical Features of Bilateral Acute Idiopathic Maculopathy
 Clinical Features of Bilateral Acute Idiopathic Maculopathy Toru Nakazawa,, Katsuhiro Yamaguchi, Masahiko Shimura, Madoka Yoshida, Yuki Yoshioka and Makoto Tamai Department of Ophthalmology, Katta General
Clinical Features of Bilateral Acute Idiopathic Maculopathy Toru Nakazawa,, Katsuhiro Yamaguchi, Masahiko Shimura, Madoka Yoshida, Yuki Yoshioka and Makoto Tamai Department of Ophthalmology, Katta General
Chapter 2 Indocyanine Green Angiography in Uveitis
 Chapter 2 Indocyanine Green Angiography in Uveitis Shilpa Kodati, Samuel P. Burke, and Thomas A. Albini Introduction Indocyanine green angiography (ICGA) became available in the early 1990s and has since
Chapter 2 Indocyanine Green Angiography in Uveitis Shilpa Kodati, Samuel P. Burke, and Thomas A. Albini Introduction Indocyanine green angiography (ICGA) became available in the early 1990s and has since
Rare Presentation of Ocular Toxoplasmosis
 Case Report Rare Presentation of Ocular Toxoplasmosis Rakhshandeh Alipanahi MD From Department of Ophthalmology, Nikookari Eye Hospital, Tabriz University of Medical Sciences, Tabriz, Iran. Correspondence:
Case Report Rare Presentation of Ocular Toxoplasmosis Rakhshandeh Alipanahi MD From Department of Ophthalmology, Nikookari Eye Hospital, Tabriz University of Medical Sciences, Tabriz, Iran. Correspondence:
Dr/ Marwa Abdellah EOS /16/2018. Dr/ Marwa Abdellah EOS When do you ask Fluorescein angiography for optic disc diseases???
 When do you ask Fluorescein angiography for optic disc diseases??? 1 NORMAL OPTIC DISC The normal optic disc on fluorescein angiography is fluorescent due to filling of vessels arising from the posterior
When do you ask Fluorescein angiography for optic disc diseases??? 1 NORMAL OPTIC DISC The normal optic disc on fluorescein angiography is fluorescent due to filling of vessels arising from the posterior
Fluorescein and Indocyanine Green Videoangiography of Choroidal Melanomas
 luorescein and Indocyanine Green Videoangiography of Choroidal Melanomas Leyla S. Atmaca, igen Batioğlu and Pelin Atmaca Eye Clinic, Ankara University Medical School, Ankara, Turkey Purpose: This study
luorescein and Indocyanine Green Videoangiography of Choroidal Melanomas Leyla S. Atmaca, igen Batioğlu and Pelin Atmaca Eye Clinic, Ankara University Medical School, Ankara, Turkey Purpose: This study
ZEISS AngioPlex OCT Angiography. Clinical Case Reports
 Clinical Case Reports Proliferative Diabetic Retinopathy (PDR) Case Report 969 PROLIFERATIVE DIABETIC RETINOPATHY 1 1-year-old diabetic female presents for follow-up of proliferative diabetic retinopathy
Clinical Case Reports Proliferative Diabetic Retinopathy (PDR) Case Report 969 PROLIFERATIVE DIABETIC RETINOPATHY 1 1-year-old diabetic female presents for follow-up of proliferative diabetic retinopathy
UVEITIS. Dr. Yılmaz ÖZYAZGAN
 UVEITIS Dr. Yılmaz ÖZYAZGAN UVEITIS DEFINITION BY STRICT DEFINITION, UVEITIS IS AN INFLAMMATION OF UVEAL TRACT. BUT IN PRACTICAL, IT IS GENERALLY NOT RESTRICTED TO THE UVEA AND INVOLVES OTHER ADJACENT
UVEITIS Dr. Yılmaz ÖZYAZGAN UVEITIS DEFINITION BY STRICT DEFINITION, UVEITIS IS AN INFLAMMATION OF UVEAL TRACT. BUT IN PRACTICAL, IT IS GENERALLY NOT RESTRICTED TO THE UVEA AND INVOLVES OTHER ADJACENT
o White dot syndromes pattern recognition o Activity and damage o Quality of life o Key points o Idiopathic o Sarcoidosis o Multiple sclerosis
 Introduction Clinical Assessment of Posterior Uveitis Philip I. Murray Centre for Translational Inflammation Research University of Birmingham Birmingham and Midland Eye Centre o Classification of uveitis
Introduction Clinical Assessment of Posterior Uveitis Philip I. Murray Centre for Translational Inflammation Research University of Birmingham Birmingham and Midland Eye Centre o Classification of uveitis
Stabilization of visual acuity with photodynamic therapy in eyes with chorioretinal anastomoses
 Graefe s Arch Clin Exp Ophthalmol (2004) 242:368 376 CLINICAL INVESTIGATION DOI 10.1007/s00417-003-0844-0 Rufino M. Silva José R. Faria de Abreu António Travassos José G. Cunha-Vaz Stabilization of visual
Graefe s Arch Clin Exp Ophthalmol (2004) 242:368 376 CLINICAL INVESTIGATION DOI 10.1007/s00417-003-0844-0 Rufino M. Silva José R. Faria de Abreu António Travassos José G. Cunha-Vaz Stabilization of visual
Contribution of Dual Fluorescein and Indocyanine Green Angiography to the Appraisal of Presumed Tuberculous Chorioretinitis in a Non-endemic Area
 Original Article Contribution of Dual Fluorescein and Indocyanine Green Angiography to the Appraisal of Presumed Tuberculous Chorioretinitis in a Non-endemic Area Raphael Massy 1,2, MS; Carl P. Herbort
Original Article Contribution of Dual Fluorescein and Indocyanine Green Angiography to the Appraisal of Presumed Tuberculous Chorioretinitis in a Non-endemic Area Raphael Massy 1,2, MS; Carl P. Herbort
Serpiginous choroidopathy
 PHILIPPINE JOURNL OF Ophthalmology Vol. 36 No. 2 July Dec em ber 2011 CSE REPORT Kristine Corpus, MD 1 ndrew ijasa, RT 1 Egidio Jose Fortuna, MD 1-2 1, 3, 4 Narciso tienza Jr., MD Serpiginous choroidopathy
PHILIPPINE JOURNL OF Ophthalmology Vol. 36 No. 2 July Dec em ber 2011 CSE REPORT Kristine Corpus, MD 1 ndrew ijasa, RT 1 Egidio Jose Fortuna, MD 1-2 1, 3, 4 Narciso tienza Jr., MD Serpiginous choroidopathy
ISPUB.COM. An Atypical Presentation of Posterior Scleritis. A Ramanathan, A Gaur CASE REPORT
 ISPUB.COM The Internet Journal of Ophthalmology and Visual Science Volume 8 Number 2 A Ramanathan, A Gaur Citation A Ramanathan, A Gaur.. The Internet Journal of Ophthalmology and Visual Science. 2009
ISPUB.COM The Internet Journal of Ophthalmology and Visual Science Volume 8 Number 2 A Ramanathan, A Gaur Citation A Ramanathan, A Gaur.. The Internet Journal of Ophthalmology and Visual Science. 2009
CENTRAL SEROUS CHORIORETINOPATHY (CSC) IS
 IS") Association Between the Efficacy of Half-Dose Photodynamic Therapy With Indocyanine Green Angiography and Optical Coherence Tomography Findings in the Treatment of Central Serous Chorioretinopathy MASSIMO
Association Between the Efficacy of Half-Dose Photodynamic Therapy With Indocyanine Green Angiography and Optical Coherence Tomography Findings in the Treatment of Central Serous Chorioretinopathy MASSIMO
epitheliopathy associated with diffuse retinal vasculitis
 British Journal of Ophthalmology, 1986, 70, 255-259 Acute posterior multifocal placoid pigment epitheliopathy associated with diffuse retinal vasculitis and late haemorrhagic macular detachment MAKOTO
British Journal of Ophthalmology, 1986, 70, 255-259 Acute posterior multifocal placoid pigment epitheliopathy associated with diffuse retinal vasculitis and late haemorrhagic macular detachment MAKOTO
연령연관황반변성에서망막혈관종성증식과동반된망막색소상피박리의임상양상과일차적인광역학치료의결과
 연령연관황반변성에서망막혈관종성증식과동반된망막색소상피박리의임상양상과일차적인광역학치료의결과 40 Table. Clinical characteristics and results of patients undergoing photodynamic therapy for retinal angiomatous proliferation Patients No. Age/ sex Eye
연령연관황반변성에서망막혈관종성증식과동반된망막색소상피박리의임상양상과일차적인광역학치료의결과 40 Table. Clinical characteristics and results of patients undergoing photodynamic therapy for retinal angiomatous proliferation Patients No. Age/ sex Eye
Macular Hole Associated with Vogt-Koyanagi-Harada Disease at the Acute Uveitic Stage
 Published online: September 15, 2015 2015 The Author(s) Published by S. Karger AG, Basel 1663 2699/15/0063 0328$39.50/0 This article is licensed under the Creative Commons Attribution-NonCommercial 4.0
Published online: September 15, 2015 2015 The Author(s) Published by S. Karger AG, Basel 1663 2699/15/0063 0328$39.50/0 This article is licensed under the Creative Commons Attribution-NonCommercial 4.0
Research Article The Role of Fundus Autofluorescence Imaging in the Study of the Course of Posterior Uveitis Disorders
 BioMed Research International Volume 2015, Article ID 247469, 11 pages http://dx.doi.org/10.1155/2015/247469 Research Article The Role of Fundus Autofluorescence Imaging in the Study of the Course of Posterior
BioMed Research International Volume 2015, Article ID 247469, 11 pages http://dx.doi.org/10.1155/2015/247469 Research Article The Role of Fundus Autofluorescence Imaging in the Study of the Course of Posterior
Disease-Specific Fluorescein Angiography
 Ruth E. Picchiottino, CRA Disease-Specific Fluorescein Angiography 15 Disease-Specific Fluorescein Angiography Recommendations for tailoring retinal fluorescein angiography to diabetic retinopathy, macular
Ruth E. Picchiottino, CRA Disease-Specific Fluorescein Angiography 15 Disease-Specific Fluorescein Angiography Recommendations for tailoring retinal fluorescein angiography to diabetic retinopathy, macular
Evaluation of efficacy of eplerenone in the management of chronic central serous choroidoretinopathy
 Original article: Evaluation of efficacy of eplerenone in the management of chronic central serous choroidoretinopathy Dr. Sushant Madaan* Department of Ophthalmology, NIMS Medical College and Hopsital,Jaipur,
Original article: Evaluation of efficacy of eplerenone in the management of chronic central serous choroidoretinopathy Dr. Sushant Madaan* Department of Ophthalmology, NIMS Medical College and Hopsital,Jaipur,
Optical Coherence Tomograpic Features in Idiopathic Retinitis, Vasculitis, Aneurysms and Neuroretinitis (IRVAN)
") Columbia International Publishing Journal of Ophthalmic Research (2014) Research Article Optical Coherence Tomograpic Features in Idiopathic Retinitis, Vasculitis, Aneurysms and Neuroretinitis (IRVAN)
Columbia International Publishing Journal of Ophthalmic Research (2014) Research Article Optical Coherence Tomograpic Features in Idiopathic Retinitis, Vasculitis, Aneurysms and Neuroretinitis (IRVAN)
Wide-field fluorescein and indocyanine green angiography findings in the eyes with Vogt-Koyanagi-Harada disease
 Kurobe et al. Journal of Ophthalmic Inflammation and Infection (2017) 7:16 DOI 10.1186/s12348-017-0134-3 Journal of Ophthalmic Inflammation and Infection BRIEF REPORT Open Access Wide-field fluorescein
Kurobe et al. Journal of Ophthalmic Inflammation and Infection (2017) 7:16 DOI 10.1186/s12348-017-0134-3 Journal of Ophthalmic Inflammation and Infection BRIEF REPORT Open Access Wide-field fluorescein
Spontaneous Large Serous Retinal Pigment Epithelial Tear
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Retinal pigment epithelial detachments in the elderly:
 British Journal of Ophthalmology, 1985, 69, 397-403 Retinal pigment epithelial detachments in the elderly: classification and outcome A G CASSWELL, D KOHEN, AND A C BIRD From Moorfields Eye Hospital, City
British Journal of Ophthalmology, 1985, 69, 397-403 Retinal pigment epithelial detachments in the elderly: classification and outcome A G CASSWELL, D KOHEN, AND A C BIRD From Moorfields Eye Hospital, City
Indocyanine Green Angiography Findings in Central Serous Chorioretinopathy
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 5 Ver. III (May. 2016), PP 11-21 www.iosrjournals.org Indocyanine Green Angiography Findings
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 5 Ver. III (May. 2016), PP 11-21 www.iosrjournals.org Indocyanine Green Angiography Findings
Eye (2009) 23, & 2009 Macmillan Publishers Limited All rights reserved X/09 $32.00
 23, & 2009 Macmillan Publishers Limited All rights reserved X/09 $32.00") (2009) 23, 543 548 & 2009 Macmillan Publishers Limited All rights reserved 0950-222X/09 $32.00 www.nature.com/eye Effects of the duration of initial oral corticosteroid treatment on the recurrence of inflammation
(2009) 23, 543 548 & 2009 Macmillan Publishers Limited All rights reserved 0950-222X/09 $32.00 www.nature.com/eye Effects of the duration of initial oral corticosteroid treatment on the recurrence of inflammation
Choroidal Neovascularization in Sympathetic Ophthalmia
 Choroidal Neovascularization in Sympathetic Ophthalmia Lucia Sobrin, Miguel Cordero Coma, C. Stephen Foster Case Report A 49-year-old man presented after a ruptured globe repair of his left eye status
Choroidal Neovascularization in Sympathetic Ophthalmia Lucia Sobrin, Miguel Cordero Coma, C. Stephen Foster Case Report A 49-year-old man presented after a ruptured globe repair of his left eye status
DOME SHAPED MACULOPATHY. Ιωάννης Ν. Βαγγελόπουλος Χειρ. Οφθαλμίατρος - Βόλος
 DOME SHAPED MACULOPATHY Ιωάννης Ν. Βαγγελόπουλος Χειρ. Οφθαλμίατρος - Βόλος DOME SHAPED MACULOPATHY-DEFINITIONS The entity Dome Shaped Macula ( DSM ) was first described by Gaucher and associates in 2008
DOME SHAPED MACULOPATHY Ιωάννης Ν. Βαγγελόπουλος Χειρ. Οφθαλμίατρος - Βόλος DOME SHAPED MACULOPATHY-DEFINITIONS The entity Dome Shaped Macula ( DSM ) was first described by Gaucher and associates in 2008
ISPUB.COM. Photopsia post flu: A case of MEWDS. S Baisakhiya, S Dulani, S Lele INTRODUCTION CASE HISTORY
 ISPUB.COM The Internet Journal of Ophthalmology and Visual Science Volume 8 Number 1 Photopsia post flu: A case of MEWDS S Baisakhiya, S Dulani, S Lele Citation S Baisakhiya, S Dulani, S Lele. Photopsia
ISPUB.COM The Internet Journal of Ophthalmology and Visual Science Volume 8 Number 1 Photopsia post flu: A case of MEWDS S Baisakhiya, S Dulani, S Lele Citation S Baisakhiya, S Dulani, S Lele. Photopsia
Diabetic Retinopathy
 Diabetic Retinopathy Diabetes can be classified into type 1 diabetes mellitus and type 2 diabetes mellitus, formerly known as insulin-dependent diabetes mellitus, and non-insulin diabetes mellitus, respectively.
Diabetic Retinopathy Diabetes can be classified into type 1 diabetes mellitus and type 2 diabetes mellitus, formerly known as insulin-dependent diabetes mellitus, and non-insulin diabetes mellitus, respectively.
CLINICAL SCIENCES. Leopard-Spot Pattern of Yellowish Subretinal Deposits in Central Serous Chorioretinopathy
 CLINICAL SCIENCES Leopard-Spot Pattern of Yellowish Subretinal Deposits in Central Serous Chorioretinopathy Tomohiro Iida, MD; Richard F. Spaide, MD; Anton Haas, MD; Lawrence A. Yannuzzi, MD; Lee M. Jampol,
CLINICAL SCIENCES Leopard-Spot Pattern of Yellowish Subretinal Deposits in Central Serous Chorioretinopathy Tomohiro Iida, MD; Richard F. Spaide, MD; Anton Haas, MD; Lawrence A. Yannuzzi, MD; Lee M. Jampol,
CLINICALCASE PROVOST J, SEKFALI R, AMOROSO F, ZAMBROWSKI O, MIERE A
 CLINICALCASE PROVOST J, SEKFALI R, AMOROSO F, ZAMBROWSKI O, MIERE A Department of ophthalmology, Souied E. (MD,PhD) Centre Hospitalier Intercommunal de Créteil Université Paris Est HISTORY 13 years old
CLINICALCASE PROVOST J, SEKFALI R, AMOROSO F, ZAMBROWSKI O, MIERE A Department of ophthalmology, Souied E. (MD,PhD) Centre Hospitalier Intercommunal de Créteil Université Paris Est HISTORY 13 years old
Indocyanine Green Angiographic Findings of Chorioretinal Folds
 Indocyanine Green Angiographic Findings of Chorioretinal Folds Miho Haruyama, Mitsuko Yuzawa, Akiyuki Kawamura, Chikayo Yamazaki and Youko Matsumoto Department of Ophthalmology, Nihon University School
Indocyanine Green Angiographic Findings of Chorioretinal Folds Miho Haruyama, Mitsuko Yuzawa, Akiyuki Kawamura, Chikayo Yamazaki and Youko Matsumoto Department of Ophthalmology, Nihon University School
The legally binding text is the original French version
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 12 September 2007 INFRACYANINE 25 mg/10 ml, powder and solvent for solution for injection 25 mg vial with one 10 ml
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 12 September 2007 INFRACYANINE 25 mg/10 ml, powder and solvent for solution for injection 25 mg vial with one 10 ml
Optical coherence tomography findings in a child with posterior scleritis
 European Journal of Ophthalmology / Vol. 18 no. 6, 2008 / pp. 1007-1010 SHORT OMMUNITIONS & SE REPORTS Optical coherence tomography findings in a child with posterior scleritis H. ERDÖL, M. KOL,. TÜRK
European Journal of Ophthalmology / Vol. 18 no. 6, 2008 / pp. 1007-1010 SHORT OMMUNITIONS & SE REPORTS Optical coherence tomography findings in a child with posterior scleritis H. ERDÖL, M. KOL,. TÜRK
D JO. Bilateral Shallow Anterior Chamber And Transient Myopia As A Presenting Feature Of Vogt Koyanagi Harada Syndrome
 46 Bilateral Shallow Anterior Chamber And Transient Myopia As A Presenting Feature Of Vogt Koyanagi Harada Syndrome Abstract Rahul Kumar Sharma, Abhishek Dagar, Vivek Kumar Vitreo-Retina Department, Venu
46 Bilateral Shallow Anterior Chamber And Transient Myopia As A Presenting Feature Of Vogt Koyanagi Harada Syndrome Abstract Rahul Kumar Sharma, Abhishek Dagar, Vivek Kumar Vitreo-Retina Department, Venu
Quantitative Evaluation of Sunset Glow Fundus in Vogt Koyanagi Harada Disease
 Quantitative Evaluation of Sunset Glow Fundus in Vogt Koyanagi Harada Disease Saburosuke Suzuki Department of Ophthalmology, Keio University, School of Medicine, Shinjuku, Tokyo, Japan Purpose: To evaluate
Quantitative Evaluation of Sunset Glow Fundus in Vogt Koyanagi Harada Disease Saburosuke Suzuki Department of Ophthalmology, Keio University, School of Medicine, Shinjuku, Tokyo, Japan Purpose: To evaluate
Flore De Bats, 1 Benjamin Wolff, 2,3 Martine Mauget-Faÿsse, 2 Claire Scemama, 2 and Laurent Kodjikian Introduction
 Case Reports in Medicine Volume 2013, Article ID 260237, 7 pages http://dx.doi.org/10.1155/2013/260237 Case Report B-Scan and En-Face Spectral-Domain Optical Coherence Tomography Imaging for the Diagnosis
Case Reports in Medicine Volume 2013, Article ID 260237, 7 pages http://dx.doi.org/10.1155/2013/260237 Case Report B-Scan and En-Face Spectral-Domain Optical Coherence Tomography Imaging for the Diagnosis
11/29/2016 MACULAR MALADIES: TYPICAL & ATYPICAL CASES
 MACULAR MALADIES: TYPICAL & ATYPICAL CASES Dawn Pewitt, OD, FAAO Triad Eye Institute, Grove, OK Dpewitt@triadeye.com Disclosure Statement: No financial disclosures COPE 51218-PS Please silence all mobile
MACULAR MALADIES: TYPICAL & ATYPICAL CASES Dawn Pewitt, OD, FAAO Triad Eye Institute, Grove, OK Dpewitt@triadeye.com Disclosure Statement: No financial disclosures COPE 51218-PS Please silence all mobile
RETINAL PIGMENT EPITHELIUM UNDULATIONS IN ACUTE STAGE OF VOGT-KOYANAGI-HARADA DISEASE
 RETINAL PIGMENT EPITHELIUM UNDULATIONS IN ACUTE STAGE OF VOGT-KOYANAGI-HARADA DISEASE Biomarker for Functional Outcomes After High-Dose Steroid Therapy KOUHEI HASHIZUME, MD,* YUTAKA IMAMURA, MD, TAKAMITSU
RETINAL PIGMENT EPITHELIUM UNDULATIONS IN ACUTE STAGE OF VOGT-KOYANAGI-HARADA DISEASE Biomarker for Functional Outcomes After High-Dose Steroid Therapy KOUHEI HASHIZUME, MD,* YUTAKA IMAMURA, MD, TAKAMITSU
Intravitreal ranibizumab for choroidal neovascularization in a patient with angioid streaks and multiple evanescent white dots
 Pece et al. BMC Ophthalmology (2016) 16:122 DOI 10.1186/s12886-016-0307-0 CASE REPORT Intravitreal ranibizumab for choroidal neovascularization in a patient with angioid streaks and multiple evanescent
Pece et al. BMC Ophthalmology (2016) 16:122 DOI 10.1186/s12886-016-0307-0 CASE REPORT Intravitreal ranibizumab for choroidal neovascularization in a patient with angioid streaks and multiple evanescent
Is OCT-A Needed As An Investigative Tool During The Management Of Diabetic Macular Edema
 Is OCT-A Needed As An Investigative Tool During The Management Of Diabetic Macular Edema Ayman M Khattab MD, FRCS Professor of Ophthalmology Cairo University Diabetic Macular Edema (DME) Diabetic macular
Is OCT-A Needed As An Investigative Tool During The Management Of Diabetic Macular Edema Ayman M Khattab MD, FRCS Professor of Ophthalmology Cairo University Diabetic Macular Edema (DME) Diabetic macular
Michael P. Blair, MD Retina Consultants, Ltd Libertyville/Des Plaines, Illinois Clinical Associate University of Chicago 17 October 2015
 Michael P. Blair, MD Retina Consultants, Ltd Libertyville/Des Plaines, Illinois Clinical Associate University of Chicago 17 October 2015 So What Parts of the Eye Retina are Affected by VHL Neural tissue
Michael P. Blair, MD Retina Consultants, Ltd Libertyville/Des Plaines, Illinois Clinical Associate University of Chicago 17 October 2015 So What Parts of the Eye Retina are Affected by VHL Neural tissue
Clinical Case Presentation. Branch Retinal Vein Occlusion. Sarita M. Registered Nurse Whangarei Base Hospital
 Clinical Case Presentation on Branch Retinal Vein Occlusion Sarita M. Registered Nurse Whangarei Base Hospital Introduction Case Study Pathogenesis Clinical Features Investigations Treatment Follow-up
Clinical Case Presentation on Branch Retinal Vein Occlusion Sarita M. Registered Nurse Whangarei Base Hospital Introduction Case Study Pathogenesis Clinical Features Investigations Treatment Follow-up
Bilateral Elevated Macular Lesions
 Challenging Case Bilateral Elevated Macular Lesions Section Editor: Alireza Ramezani, MD Case presentation A 65-year-old woman presented with decreased vision in both eyes of 2 months duration. She reported
Challenging Case Bilateral Elevated Macular Lesions Section Editor: Alireza Ramezani, MD Case presentation A 65-year-old woman presented with decreased vision in both eyes of 2 months duration. She reported
Patient AB. Born in 1961 PED
 Clinical Atlas Patient AB Born in 1961 PED Autofluorescence Dilated 45 EasyScan Zero-dilation IR 45 Fundus Dilated 45 In the fundus photos (Canon CX1) the PED is not able to be seen. However, the extent
Clinical Atlas Patient AB Born in 1961 PED Autofluorescence Dilated 45 EasyScan Zero-dilation IR 45 Fundus Dilated 45 In the fundus photos (Canon CX1) the PED is not able to be seen. However, the extent
Photocoagulation of disciform macular lesions
 British Journal of Ophthalmology, 1979, 63, 669-673 Photocoagulation of disciform macular lesions with krypton laser A. C. BIRD AND R. H. B. GREY From the Institute of Ophthalmology, Moorfields Eye Hospital,
British Journal of Ophthalmology, 1979, 63, 669-673 Photocoagulation of disciform macular lesions with krypton laser A. C. BIRD AND R. H. B. GREY From the Institute of Ophthalmology, Moorfields Eye Hospital,
Optical Coherence Tomography (OCT) in Uveitis Piergiorgio Neri, BMedSc, MD, PhD Head Ocular Immunology Unit
 in Uveitis Piergiorgio Neri, BMedSc, MD, PhD Head Ocular Immunology Unit") The Eye Clinic Polytechnic University of Marche Head: Prof Alfonso Giovannini November, 1991 Optical Coherence Tomography (OCT) in Uveitis Piergiorgio Neri, BMedSc, MD, PhD Head Ocular Immunology Unit
The Eye Clinic Polytechnic University of Marche Head: Prof Alfonso Giovannini November, 1991 Optical Coherence Tomography (OCT) in Uveitis Piergiorgio Neri, BMedSc, MD, PhD Head Ocular Immunology Unit
Convergence in. Introduction. Case Report: Dr. Piyali SenM.B.B.S, Dr. Abhipsha Saha M.B.B.S, Dr. Anuradha Chandra M.S,FAICO
 Convergence in Dr. Piyali SenM.B.B.S, Dr. Abhipsha Saha M.B.B.S, Dr. Anuradha Chandra M.S,FAICO Introduction non-progressive ophthalmoplegia with or without ptosis affecting part or all of the occulomotor
Convergence in Dr. Piyali SenM.B.B.S, Dr. Abhipsha Saha M.B.B.S, Dr. Anuradha Chandra M.S,FAICO Introduction non-progressive ophthalmoplegia with or without ptosis affecting part or all of the occulomotor
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA
 OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
Authors. Introduction. Introduction. Materials and Methods. Objective 10/27/2015
 Idiopathic Polypoidal Choroidal Vasculopathy (IPCV) in Thai Population Presenting with Choroidal Neovascularization (CNV) A multicenter study Authors Yonrawee Piyacomn 1, Chavakij Bhoomibunchoo 1, Yosanan
Idiopathic Polypoidal Choroidal Vasculopathy (IPCV) in Thai Population Presenting with Choroidal Neovascularization (CNV) A multicenter study Authors Yonrawee Piyacomn 1, Chavakij Bhoomibunchoo 1, Yosanan
PART 1: GENERAL RETINAL ANATOMY
 PART 1: GENERAL RETINAL ANATOMY General Anatomy At Ora Serrata At Optic Nerve Head Fundoscopic View Of Normal Retina What Is So Special About Diabetic Retinopathy? The WHO definition of blindness is
PART 1: GENERAL RETINAL ANATOMY General Anatomy At Ora Serrata At Optic Nerve Head Fundoscopic View Of Normal Retina What Is So Special About Diabetic Retinopathy? The WHO definition of blindness is
Characterization of serous retinal detachments in uveitis patients with optical coherence tomography
 Characterization of serous retinal detachments in uveitis patients with optical coherence tomography Annamieka Simmons-Rear, Oregon Health and Science University Steven Yeh, Emory University Brian T. Chan-Kai,
Characterization of serous retinal detachments in uveitis patients with optical coherence tomography Annamieka Simmons-Rear, Oregon Health and Science University Steven Yeh, Emory University Brian T. Chan-Kai,
Videofunduscopy and videoangiography using the scanning laser ophthalmoscope in Vogt Koyanagi Harada syndrome
 Br J Ophthalmol 1998;82:1175 1181 1175 Department of Ophthalmology, Tokyo Medical College Hospital, Tokyo, Japan A A Okada T Mizusawa J Sakai M Usui Correspondence to: Annabelle A Okada, MD, Department
Br J Ophthalmol 1998;82:1175 1181 1175 Department of Ophthalmology, Tokyo Medical College Hospital, Tokyo, Japan A A Okada T Mizusawa J Sakai M Usui Correspondence to: Annabelle A Okada, MD, Department
Algorithm of Choroiditis
 10.5005/jp-journals-10020-1027 REVIEW ARTICLE Ovi Sofia, Sudharshan Sridharan, Jyotirmay Biswas ABSTRACT Choroiditis may present as focal or multifocal lesions, and could be due to infectious or noninfectious
10.5005/jp-journals-10020-1027 REVIEW ARTICLE Ovi Sofia, Sudharshan Sridharan, Jyotirmay Biswas ABSTRACT Choroiditis may present as focal or multifocal lesions, and could be due to infectious or noninfectious
Incorporating OCT Angiography Into Patient Care
 Incorporating OCT Angiography Into Patient Care Beth A. Steele, OD, FAAO OCT A: Introduction Isolates microvascular circulation from OCT image data Axial resolution = 5 microns (i.e. fine capillaries visible)
Incorporating OCT Angiography Into Patient Care Beth A. Steele, OD, FAAO OCT A: Introduction Isolates microvascular circulation from OCT image data Axial resolution = 5 microns (i.e. fine capillaries visible)
Diagnosis of uveitis, how to proceed?
 EOS meeting Cairo, 2018 Diagnosis of uveitis, how to proceed? Mohamed G.A Saleh Lecturer of Ophthalmology Assiut University Size of the problem 15/100000 in US every year. 10% of blindness Prevalence varies
EOS meeting Cairo, 2018 Diagnosis of uveitis, how to proceed? Mohamed G.A Saleh Lecturer of Ophthalmology Assiut University Size of the problem 15/100000 in US every year. 10% of blindness Prevalence varies
A Patient s Guide to Diabetic Retinopathy
 Diabetic Retinopathy A Patient s Guide to Diabetic Retinopathy 840 Walnut Street, Philadelphia PA 19107 www.willseye.org Diabetic Retinopathy 1. Definition Diabetic retinopathy is a complication of diabetes
Diabetic Retinopathy A Patient s Guide to Diabetic Retinopathy 840 Walnut Street, Philadelphia PA 19107 www.willseye.org Diabetic Retinopathy 1. Definition Diabetic retinopathy is a complication of diabetes
Placoid pigment epitheliopathy with
 Brit. J. Ophthal. ( I 972) 56, 875 Placoid pigment epitheliopathy with retinal vasculitis and papillitis T. H. KIRKHAM, *T. J. FFYTCHE, AND M. D. SANDERS From the Department of Neuro-Ophthalmology, the
Brit. J. Ophthal. ( I 972) 56, 875 Placoid pigment epitheliopathy with retinal vasculitis and papillitis T. H. KIRKHAM, *T. J. FFYTCHE, AND M. D. SANDERS From the Department of Neuro-Ophthalmology, the
Late ocular manifestations in neonatal herpes simplex infection
 British Journal of Ophthalmology, 1977, 61, 608-616 Late ocular manifestations in neonatal herpes simplex infection AHTI TARKKANEN AND LEILA LAATIKAINEN From the Helsinki University Eye Hospital SUMMARY
British Journal of Ophthalmology, 1977, 61, 608-616 Late ocular manifestations in neonatal herpes simplex infection AHTI TARKKANEN AND LEILA LAATIKAINEN From the Helsinki University Eye Hospital SUMMARY
Key words: Choroidal neovascularisation, Laser coagulation, Retinal imaging
 420 Mini Review The Role of Optical Coherence Tomography (OCT) in the Diagnosis and Management of Retinal Angiomatous Proliferation (RAP) in Patients with Age-related Macular Degeneration Antonio Polito,
420 Mini Review The Role of Optical Coherence Tomography (OCT) in the Diagnosis and Management of Retinal Angiomatous Proliferation (RAP) in Patients with Age-related Macular Degeneration Antonio Polito,
THE OCULAR histoplasmosis
 CLINICAL SCIENCES Reactivation of Inflammatory Lesions in Ocular Histoplasmosis David Callanan, MD; Gary E. Fish, MD, JD; Rajiv Anand, MD Background: Active inflammation has not been traditionally associated
CLINICAL SCIENCES Reactivation of Inflammatory Lesions in Ocular Histoplasmosis David Callanan, MD; Gary E. Fish, MD, JD; Rajiv Anand, MD Background: Active inflammation has not been traditionally associated
UVEITIS IN GENERAL. Information for patients UVEITIS CLINIC WHAT IS UVEITIS? MAIN CATEGORIES OF UVEITIS
 Information for patients UVEITIS CLINIC UVEITIS IN GENERAL WHAT IS UVEITIS? The uvea is a name given to the pigmented layer of tissue inside the eye. When all or part of the uvea becomes inflamed, the
Information for patients UVEITIS CLINIC UVEITIS IN GENERAL WHAT IS UVEITIS? The uvea is a name given to the pigmented layer of tissue inside the eye. When all or part of the uvea becomes inflamed, the
P olypoidal choroidal vasculopathy (PCV), first described
, first described") 602 EXTENDED REPORT The origins of polypoidal choroidal vasculopathy M Yuzawa, R Mori, A Kawamura... Br J Ophthalmol 2005;89:602 607. doi: 10.1136/bjo.2004.049296 See end of article for authors affiliations...
602 EXTENDED REPORT The origins of polypoidal choroidal vasculopathy M Yuzawa, R Mori, A Kawamura... Br J Ophthalmol 2005;89:602 607. doi: 10.1136/bjo.2004.049296 See end of article for authors affiliations...
Angio-OCT. Degenerazione Maculare Legata all Eta. Giuseppe Querques
 Angio-OCT Degenerazione Maculare Legata all Eta Giuseppe Querques Department of Ophthalmology, IRCCS Ospedale San Raffaele, University Vita Salute San Raffaele, Milan, Italy Financial Disclosure ADVISORY
Angio-OCT Degenerazione Maculare Legata all Eta Giuseppe Querques Department of Ophthalmology, IRCCS Ospedale San Raffaele, University Vita Salute San Raffaele, Milan, Italy Financial Disclosure ADVISORY
Retina Conference. Janelle Fassbender, MD, PhD University of Louisville Department of Ophthalmology and Visual Sciences 09/04/2014
 Retina Conference Janelle Fassbender, MD, PhD University of Louisville Department of Ophthalmology and Visual Sciences 09/04/2014 Subjective CC/HPI: 64 year old Caucasian female referred by outside ophthalmologist
Retina Conference Janelle Fassbender, MD, PhD University of Louisville Department of Ophthalmology and Visual Sciences 09/04/2014 Subjective CC/HPI: 64 year old Caucasian female referred by outside ophthalmologist
Since /01/2014 Private practice Ophthalmology, Retinal Medical Specialty and AMD, private office
 Corinne GONZALEZ Ophthalmology (MD, Ph.D ) Retinal Medical Specialist SELARL CABINET DOCTEUR GONZALEZ 27, Boulevard des Minimes 31 200 Toulouse! 05 34 40 77 30 e-mail : cabinet.dr.gonzalez@wanadoo.fr Fax
Corinne GONZALEZ Ophthalmology (MD, Ph.D ) Retinal Medical Specialist SELARL CABINET DOCTEUR GONZALEZ 27, Boulevard des Minimes 31 200 Toulouse! 05 34 40 77 30 e-mail : cabinet.dr.gonzalez@wanadoo.fr Fax
Building The Retina Company
 Building The Retina Company Optos devices produce ultra-widefield (UWF ), high resolution images (optomap ) of approximately 82% (200 ) of the retina. A single optomap can document the retina from the
Building The Retina Company Optos devices produce ultra-widefield (UWF ), high resolution images (optomap ) of approximately 82% (200 ) of the retina. A single optomap can document the retina from the
Intravitreal Triamcinolone Acetonide for Macular Edema in HLA-B27 Negative Ankylosing Spondylitis
 105 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the
105 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the
 measure of your overall performance. An isolated glucose test is helpful to let you know what your sugar level is at one moment, but it doesn t tell you whether or not your diabetes is under adequate control
measure of your overall performance. An isolated glucose test is helpful to let you know what your sugar level is at one moment, but it doesn t tell you whether or not your diabetes is under adequate control
Uveitis. What is Uveitis?
 Uveitis What is Uveitis? Uveitis [u-vee-i-tis] is a term for inflammation of the eye. It can occur in one eye or both eyes and affects the layer of the eye called the uvea [u-vee-uh]. It also can be associated
Uveitis What is Uveitis? Uveitis [u-vee-i-tis] is a term for inflammation of the eye. It can occur in one eye or both eyes and affects the layer of the eye called the uvea [u-vee-uh]. It also can be associated
University of Bristol - Explore Bristol Research. Peer reviewed version. Link to published version (if available): /eye.2017.
: /eye.2017.") Burke, T. R., Chu, C. J., Salvatore, S., Bailey, C. C., Dick, A. D., Lee, R. W. J.,... Medscape (2017). Application of OCT-angiography to characterise the evolution of chorioretinal lesions in acute posterior
Burke, T. R., Chu, C. J., Salvatore, S., Bailey, C. C., Dick, A. D., Lee, R. W. J.,... Medscape (2017). Application of OCT-angiography to characterise the evolution of chorioretinal lesions in acute posterior
Slide 4. Slide 5. Slide 6
 Slide 1 Slide 4 Demographics El Paso Eye Care Border Healthcare-Based Grand Rounds Derek N. Cunningham, O.D. 80-90% Mexican-Americans Diabetes Hypertension Hyperlipidemia Obesity 70% uninsured High poverty
Slide 1 Slide 4 Demographics El Paso Eye Care Border Healthcare-Based Grand Rounds Derek N. Cunningham, O.D. 80-90% Mexican-Americans Diabetes Hypertension Hyperlipidemia Obesity 70% uninsured High poverty
Fundus Autofluorescence
 Brittany Bateman, BS Fundus autofluorescence imaging is used to record fluorescence that may occur naturally in ocular structures or as a byproduct of a disease process. This technique allows the topographic
Brittany Bateman, BS Fundus autofluorescence imaging is used to record fluorescence that may occur naturally in ocular structures or as a byproduct of a disease process. This technique allows the topographic
Acute Retinal Necrosis Secondary to Varicella Zoster Virus in an Immunosuppressed Post-Kidney Transplant Patient
 CM&R Rapid Release. Published online ahead of print September 20, 2012 as Aperture Acute Retinal Necrosis Secondary to Varicella Zoster Virus in an Immunosuppressed Post-Kidney Transplant Patient Elizabeth
CM&R Rapid Release. Published online ahead of print September 20, 2012 as Aperture Acute Retinal Necrosis Secondary to Varicella Zoster Virus in an Immunosuppressed Post-Kidney Transplant Patient Elizabeth
EyePACS Grading System (Part 2): Detecting Presence and Severity of Background (Non-Proliferative) Diabetic Retinopathy Lesion
: Detecting Presence and Severity of Background (Non-Proliferative) Diabetic Retinopathy Lesion") EyePACS Grading System (Part 2): Detecting Presence and Severity of Background (Non-Proliferative) Diabetic Retinopathy Lesion George Bresnick MD MPA Jorge Cuadros OD PhD Anatomy of the eye: 3 Normal Retina
EyePACS Grading System (Part 2): Detecting Presence and Severity of Background (Non-Proliferative) Diabetic Retinopathy Lesion George Bresnick MD MPA Jorge Cuadros OD PhD Anatomy of the eye: 3 Normal Retina
Double trouble: a patient with both HLA-B27 anterior uveitis and HLA-A29 birdshot chorioretinitis
 Haddad and Reddy Journal of Ophthalmic Inflammation and Infection 2014, 4:28 BRIEF REPORT Open Access Double trouble: a patient with both HLA-B27 anterior uveitis and HLA-A29 birdshot chorioretinitis Zeina
Haddad and Reddy Journal of Ophthalmic Inflammation and Infection 2014, 4:28 BRIEF REPORT Open Access Double trouble: a patient with both HLA-B27 anterior uveitis and HLA-A29 birdshot chorioretinitis Zeina
Fundus autofluorescence in exudative age-related macular degeneration
 Fundus autofluorescence in exudative age-related macular degeneration Q. Peng*, Y. Dong* and P.Q. Zhao Department of Ophthalmology, Xinhua Hospital Affiliated to Shanghai JiaoTong University School of
Fundus autofluorescence in exudative age-related macular degeneration Q. Peng*, Y. Dong* and P.Q. Zhao Department of Ophthalmology, Xinhua Hospital Affiliated to Shanghai JiaoTong University School of
Indocyanine green angiography findings in patients with nonfamilial amyloidosis
 J Ophthal Inflamm Infect (2012) 2:199 203 DOI 10.1007/s12348-012-0085-7 ORIGINAL RESEARCH Indocyanine green angiography findings in patients with nonfamilial amyloidosis Sonia Attia & Rim Kahloun & Sameh
J Ophthal Inflamm Infect (2012) 2:199 203 DOI 10.1007/s12348-012-0085-7 ORIGINAL RESEARCH Indocyanine green angiography findings in patients with nonfamilial amyloidosis Sonia Attia & Rim Kahloun & Sameh
chorioretinal atrophy
 British Journal of Ophthalmology, 1987, 71, 757-761 Retinal microangiopathy in pigmented paravenous chorioretinal atrophy SURESH R LIMAYE AND MUNEERA A MAHMOOD From the Ophthalmology Service, DC General
British Journal of Ophthalmology, 1987, 71, 757-761 Retinal microangiopathy in pigmented paravenous chorioretinal atrophy SURESH R LIMAYE AND MUNEERA A MAHMOOD From the Ophthalmology Service, DC General
Deep Trouble. Thomas Stone, MD Retina Associates of Kentucky River City Retina Conference May 15, 2014
 Deep Trouble Thomas Stone, MD Retina Associates of Kentucky River City Retina Conference May 15, 2014 History 20 yo WM Decreased vision OU, OD>OS Sudden onset blurred central vision 12 days prior 4 days
Deep Trouble Thomas Stone, MD Retina Associates of Kentucky River City Retina Conference May 15, 2014 History 20 yo WM Decreased vision OU, OD>OS Sudden onset blurred central vision 12 days prior 4 days
The Natural History of Diabetic Retinopathy and How Primary Care Makes A Difference
 The Natural History of Diabetic Retinopathy and How Primary Care Makes A Difference We will discuss - How exactly does blood sugar control affect retinopathy? - What are other factors that we measure in
The Natural History of Diabetic Retinopathy and How Primary Care Makes A Difference We will discuss - How exactly does blood sugar control affect retinopathy? - What are other factors that we measure in
Panretinal acute multifocal placoid pigment epitheliopathy: a novel posterior uveitis syndrome with HLA-A3 and HLA-C7 association
 BRIEF REPORT Open Access Panretinal acute multifocal placoid pigment epitheliopathy: a novel posterior uveitis syndrome with HLA-A3 and HLA-C7 association Kevin R Baxter 1,2* and E Mitchel Opremcak 3 Abstract
BRIEF REPORT Open Access Panretinal acute multifocal placoid pigment epitheliopathy: a novel posterior uveitis syndrome with HLA-A3 and HLA-C7 association Kevin R Baxter 1,2* and E Mitchel Opremcak 3 Abstract
Age-Related Macular Degeneration (AMD)
") Age-Related Macular Degeneration (AMD) What is the Macula? What is Dry AMD (Age-related Macular Degeneration)? Dry AMD is an aging process that causes accumulation of waste product under the macula leading
Age-Related Macular Degeneration (AMD) What is the Macula? What is Dry AMD (Age-related Macular Degeneration)? Dry AMD is an aging process that causes accumulation of waste product under the macula leading
Central serous chorioretinopathy (CSCR) was
 was") Case Report 777 Perfluorocarbon Liquid-Assisted External Drainage in the Management of Central Serous Chorioretinopathy with Bullous Serous Retinal Detachment Hung-Chiao Chen, MD; Jau-Der Ho, MD; San-Ni
Case Report 777 Perfluorocarbon Liquid-Assisted External Drainage in the Management of Central Serous Chorioretinopathy with Bullous Serous Retinal Detachment Hung-Chiao Chen, MD; Jau-Der Ho, MD; San-Ni
IQ 532 Micropulse Green Laser treatment for Refractory Chronic Central Serous Retinopathy
 Cronicon OPEN ACCESS EC OPHTHALMOLOGY Case Report IQ 532 Micropulse Green Laser treatment for Refractory Chronic Central Serous Retinopathy Fawwaz Al Mamoori* Medical Retina Department, Eye Specialty Hospital,
Cronicon OPEN ACCESS EC OPHTHALMOLOGY Case Report IQ 532 Micropulse Green Laser treatment for Refractory Chronic Central Serous Retinopathy Fawwaz Al Mamoori* Medical Retina Department, Eye Specialty Hospital,
What You Should Know About Acute Macular Neuroretinopathy
 What You Should Know About Acute Macular Neuroretinopathy David J. Browning MD, PhD Chong Lee BS Acute macular neuroretinopathy is a condition characterized by the sudden, painless onset of paracentral
What You Should Know About Acute Macular Neuroretinopathy David J. Browning MD, PhD Chong Lee BS Acute macular neuroretinopathy is a condition characterized by the sudden, painless onset of paracentral
Uveitis. Pt Info Brochure. Q: What is Uvea?
 Pt Info Brochure Uveitis Q: What is Uvea? A: Uvea is the middle layer of the eye. It is the most vascular structure of the eye. It provides nutrition to the other parts of the eye. The uvea is made up
Pt Info Brochure Uveitis Q: What is Uvea? A: Uvea is the middle layer of the eye. It is the most vascular structure of the eye. It provides nutrition to the other parts of the eye. The uvea is made up
ACTIVATED OR NOT? RETINAL CASE PRESENTATION Shorye Payne, MD Medical Retinal Specialist Robley Rex VA Eye Clinic
 ACTIVATED OR NOT? RETINAL CASE PRESENTATION Shorye Payne, MD Medical Retinal Specialist Robley Rex VA Eye Clinic C We anticipate that the future management of posterior uveal melanoma (PUM) will focus
ACTIVATED OR NOT? RETINAL CASE PRESENTATION Shorye Payne, MD Medical Retinal Specialist Robley Rex VA Eye Clinic C We anticipate that the future management of posterior uveal melanoma (PUM) will focus
For further reading we recommend the following excellent textbooks:
 FURTHER READING Intravitreal Injections Downloaded from www.worldscientific.com For further reading we recommend the following excellent textbooks: Clinical Anatomy of the Eye by Richard S Snell and Michael
FURTHER READING Intravitreal Injections Downloaded from www.worldscientific.com For further reading we recommend the following excellent textbooks: Clinical Anatomy of the Eye by Richard S Snell and Michael
When optical coherence tomography (OCT)
") Macular Imaging: SD-OCT in nterior Segment Surgical Practice Many pathologic processes of the macula can be visualized or quantified only with this modality. y Steven G. Safran, MD When optical coherence
Macular Imaging: SD-OCT in nterior Segment Surgical Practice Many pathologic processes of the macula can be visualized or quantified only with this modality. y Steven G. Safran, MD When optical coherence