Microvascular Complications
|
|
|
- Reginald Wells
- 5 years ago
- Views:
Transcription
1 Microvascular Complications in Diabetes Jyotika Fernandes. MD Professor Div of Endocrinology Endo Section Chief, RHJ VA Hospital Microvascular Complications Hyperglycemia Eye Kidney Nerves Retinopathy Cataract Glaucoma Nephropathy Microalbuminuria Gross albuminuria Neuropathy Peripheral Autonomic Blindness Kidney failure Amputation Death and/or disability 1
2 Risk of Microvascular Complications vs A1C in Type 1 Diabetes Results From the DCCT Relative risk Retinopathy progression Neuropathy progression Microalbuminuria progression A1C (%) Skyler JS. Endocrinol Metab Clin North Am. 1996;25: Diabetic Kidney disease / Nephropathy Type 1 DM 20-30% of those with disease > 15 yr. Type 2 DM incidence of renal disease 5-10% in Caucasian, 15-20% in African American,50% in Pima Indians 2
3 No. of Dialysis Patients (thousands) Diabetes: The Most Common Cause of ESRD Primary Diagnosis for Patients Who Start Dialysis Other 10% Diabetes 50.1% Glomerulonephritis 13% Hypertension 27% 243, ,355 No. of Patients Projection 95% CI 520,240 r 2 = 99.8% United States Renal Data System. Annual data report Definition of abnormal albumin excretion Urinary AER (mg/24h) Urinary AER (mg/min) Urine albumin to creatinine Ratio (mg/g) Normal < 30 < 20 < 30 Microalbuminuria Macrcolbuminuria (overt nephropathy) > 300 >200 > 300 3
 will no longer be used, but rather referred to as persistent albuminuria at levels 30 299 mg/24 h and severely increased albuminuria levels >300 mg/24 h.")
4 Recommendations: Nephropathy To be consistent with newer nomenclature intended to emphasize the continuous nature of albuminuria as a risk factor, the terms microalbuminuria ( mg/24 h) and macroalbuminuria (>300 mg/24 h) will no longer be used, but rather referred to as persistent albuminuria at levels mg/24 h and severely increased albuminuria levels >300 mg/24 h. Diabetes care 2014; 37: suppl 1 pp S 43 Risk Factors for Diabetic Nephropathy Hypertension Glycemic control Cigarette smoking Hyperlipidemia Microalbuminuria Duration of diabetes/ Age Family history Ethnicity Male gender 4
 Blood pressure rises Overt nephropathy or clinical")
5 NATURAL HISTORY OF NEPHROPATHY IN TYPE 1 DIABETES Normo albuminuria Stage of hyperfiltration Micro albuminuria Macro albuminuria Azotemia (Renal failure) End stage Renal disease yrs 4-5 yrs 1 yrs Natural Hx DM Renal Disease Progression of diabetic nephropathy Microalbuminuria (urinary albumin excretion 30 mg/mg creatinine or 30 mg/24 h) Blood pressure rises Overt nephropathy or clinical macroalbuminuria (urinary albumin excretion 300 mg/mg creatinine or 300 mg/24 h) Hypertension develops/worsens Glomerular filtration rate (GFR) begins to fall 5
6 Screening for albuminuria Urine Albumin Concentration 24 hour urine collection Timed urine collection Urine albumin conc early morning specimen Urine Albumin to Creatinine Ratio Untimed urine sample Preferred screening strategy Limitations -fever, exercise, heart failure, poor glycemic control Consider Other Causes of Chronic Kidney Diseases Rapidly decreasing GFR Rapidly increasing protein excretion or acute onset of nephrotic syndrome Refractory Hypertension ( need more than 3 drugs look for secondary causes of HTN ) Active Urine sediment More than a 30% reduction in GFR after initiation of therapy with ACE or ARB TYPE 1 DM: If DM duration <10yrs or no diabetic retinopathy suggestive of other cause 6

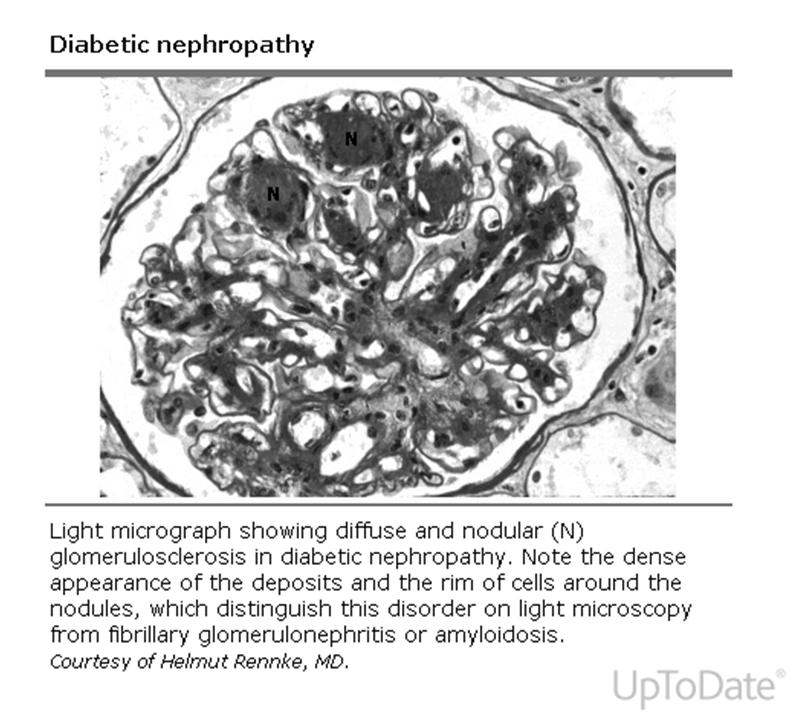
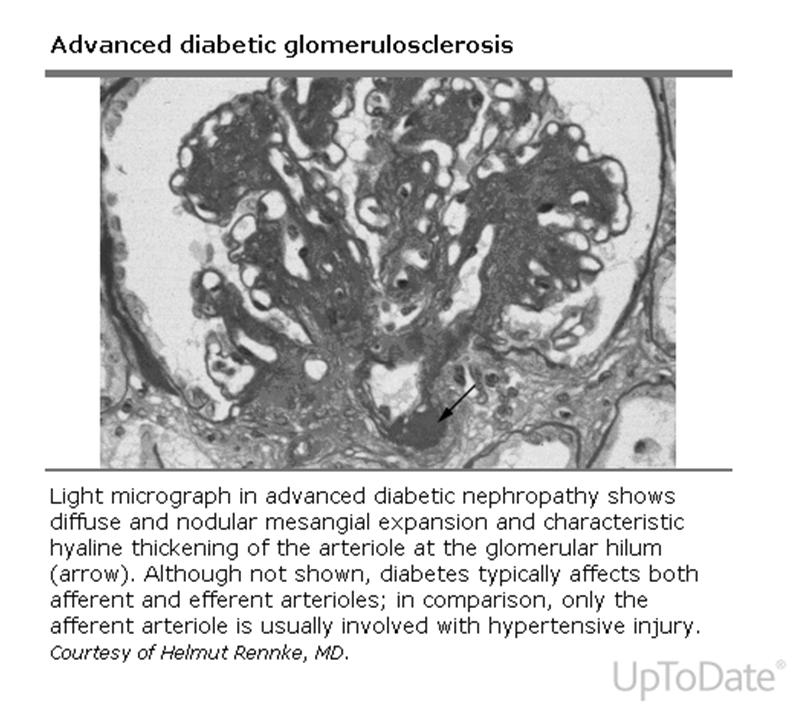
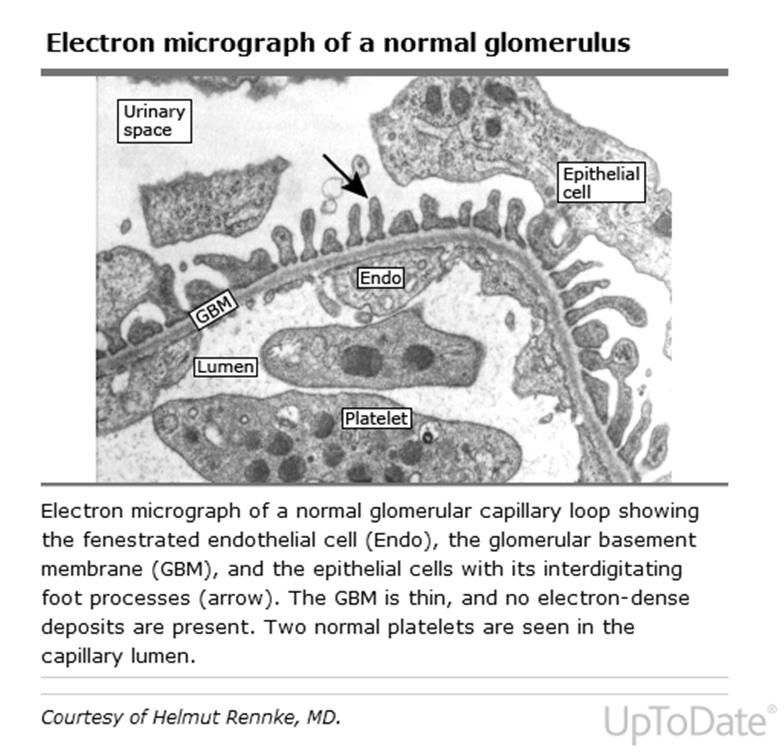
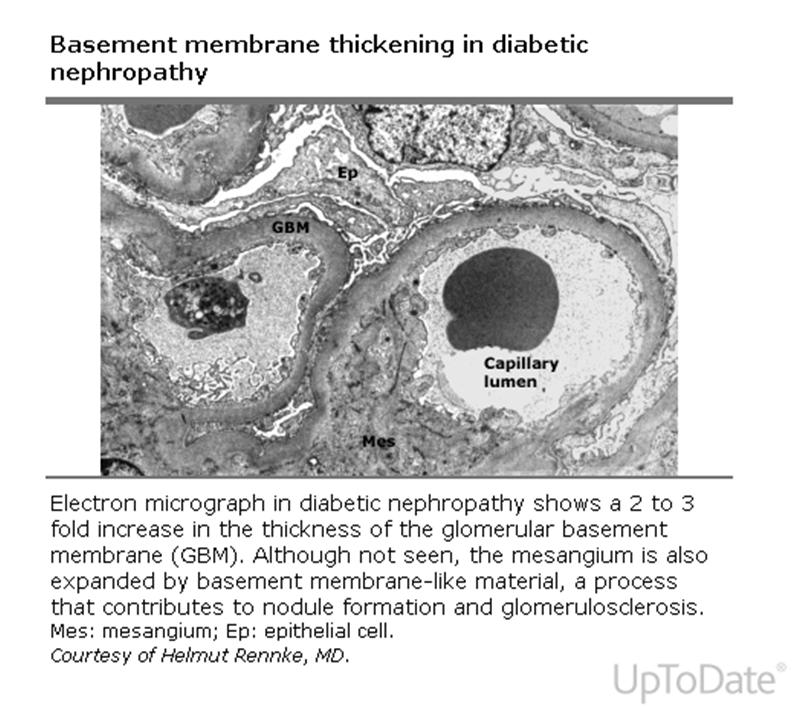
7 Pathology 7
8 8
9 9
10 The Dual Significance of Proteinuria Relation between Diabetic Nephropathy and Retinopathy In diabetes and hypertension, proteinuria (albuminuria) is also an indicator of injury in the systemic circulation Proteinuria (albuminuria) is associated with increased cardiovascular risk Proteinuria as a Risk Factor for Mortality in Type 2 Diabetes Survival (all-cause mortality) P<0.01 normoalbuminuria vs microalbuminuria Years P<0.001 normoalbuminuria vs macroalbuminuria P<0.05 microalbuminuria vs macroalbuminuria Normoalbuminuria (n=191) Microalbuminuria (n=86) Macroalbuminuria (n=51) Gall MA, et al. Diabetes. 1995;44: Copyright 1995, American Diabetes Association. Reprinted with permission. 10
11 Preservation of Renal function Type 1 DM ACE Inhibitors Remission or regression ACE-I Is More Renoprotective Than Conventional Therapy in Type 1 Diabetes % with doubling of baseline creatinine Baseline creatinine >1.5 mg/dl Conventional n=202 P<.001 Captopril n= Years of followup Lewis EJ, et al. N Engl J Med. 1993;329(20): Copyright 1993 Massachusetts Medical Society. Adapted with permission. 11
12 Summary & Recommendations Type1 DM Screening -5yrs after the diagnosis ARB data lacking Persitent Microalbuminurea/ BP >130/80mmHg start ACE Microalb/ Normotensive Limited data- suggest treatment ACE No Microalb and Normotensive No Evidence Type 2 Diabetes and Nephropathy Good blood pressure control has proven critical to slow the progression of nephropathy in type 2 diabetes New guidelines for good blood pressure control are: <130/80 mmhg (American Diabetes Association) <125/75 mmhg for patients with renal insufficiency with greater than 1 g/d of proteinuria (JNC VI) Multiple antihypertensive agents will be needed to achieve good blood pressure control ARBs or ACE-Inhitors are indicated for the treatment of type 2 diabetes with nephropathy 12
13 IRMA II Incidence of Progression to Diabetic Nephropathy Incidence of Diabetic Nephropathy (%) P<0.001 for difference between 300 mg irbesartan group and placebo Placebo 150 mg of irbesartan 300 mg of irbesartan Months of Follow-up Placebo (n) Irbesartan 150 mg (n) Irbesartan 300 mg Parving HH, et al. N Engl J Med. 2001;345(12): Massachusetts Medical Society. All rights reserved. org IRMA II Change in Urinary Albumin Excretion* % change in urinary albumin excretion 150 mg of irbesartan Placebo 300 mg of irbesartan Months of Follow-up *P<0.001 for difference between both irbesartan groups and Parving placebo HH, et al. N Engl J Med. 2001;345(12): Massachusetts Medical Society. All rights reserved. org 13
14 Preservation of Renal function Protein Restriction ACE inhibitor or ARB ACE inhibitor plus ARB -X ARB plus aliskiren X ( Tekturna Alltitude) Aldosterone antagonism Other antihypertensive drugs and combinations Salt intake and proteinuria Summary & Recommendations Factors associated with remission Microalbuminurea Short duration of microalbuminurea Better HbA1C, BP control, Lipid Mx Type 2 DM Yearly evaluation starting at diagnosis Persitent Microalbuminurea/ BP >130/80mmHg start ACE or ARB Microalb/ Normotensive Limited data- suggest treatment No Microalbumin and Normotensive No Evidence for treatment 14
15 Recommendations: Nephropathy Treatment (1) Nonpregnant patient with >/= 30 mg albumen per 24 hours Use either ACE inhibitors or ARBs (A) Do not use the combination If one class is not tolerated, the other should be substituted (E) For people with diabetes and diabetic kidney disease (albuminuria >30 mg/24 h), reducing the amount of dietary protein below usual intake is not recommended because it does not alter glycemic measures, cardiovascular risk measures, or the course of GFR decline. A Diabetes Care 2014; 37: suppl 1 pp S 43. Recommendations: Nephropathy An ACE inhibitor or ARB for the primary prevention of diabetic kidney disease is not recommended in diabetic patients with normal blood pressure and albumin excretion < 30 mg/24 h. B Diabetes Care 2014; 37: suppl 1 pp S 42 15

16 Screening for Proteinuria Yearly for both Type 1 and 2 Type1: deferred for 5 yrs after the onset Type 2 : At the time of diagnosis Use of Albumin/ creatinine ratio preferred. 16
17 ADA 2014 BP Goals People with diabetes and hypertension should be treated to a systolic blood pressure (SBP) goal of <140 mmhg. B Lower systolic targets, such as <130 mmhg, may be appropriate for certain individuals, such as younger patients, if it can be achieved without undue treatment burden. C Patients with diabetes should be treated to a diastolic blood pressure (DBP) <80 mmhg. B Diabetes Care 2014, 37: suppl1 pp S 36 Prevention/Treatment of Nephropathy Achieve glycemic control, HbA1c below 7% while avoiding hypoglycemia. Maintain BP in mid normal range: 130/80 (125/75 once proteinuria), preferably with ACE or ARB Stop smoking Correct dyslipidemia Restricting dietary protein intake (.8 gm/kg/day once there is proteinuria)?? NEW GUIDELINES DON T SUPPORT THIS 17
18 Recommendations: Nephropathy To reduce risk or slow the progression of nephropathy Optimize glucose control (A) Optimize blood pressure control (A) To be consistent with newer nomenclature intended to emphasize the continuous nature of albuminuria as a risk factor, the terms microalbuminuria ( mg/24 h) and macroalbuminuria (>300 mg/24 h) will no longer be used, but rather referred to as persistent albuminuria at levels mg/24 h and levels >300 mg/24 h. Diabetes care 2014; 37: suppl 1 pp S 43 Recommendations: Nephropathy An ACE inhibitor or ARB for the primary prevention of diabetic kidney disease is not recommended in diabetic patients with normal blood pressure and albumin excretion < 30 mg/24 h. B Diabetes Care 2014; 37: suppl 1 pp S 42 18

19 Diabetic Neuropathy Diabetic Neuropathy 19
 and median nerve Asymmetric involvement of multiple peripheral nerves 20")
20 Classification Distal Symmetric polyneuropathy Autonomic neuropathy Thoracic and lumbar nerve root disease Individual cranial and peripheral involvement causing focal mononeuropathies esp occulomoter (CN III) and median nerve Asymmetric involvement of multiple peripheral nerves 20
 Signs Diminished vibratory perception Absent or reduced knee and ankle reflexes Reduced protective sensation such as pressure, hot and cold, pain")

21 Clinical Presentation Symptoms Asymptomatic Numbness or loss of feeling (asleep or bunched up sock under toes sensation) Prickling/Tingling Pain: Aching,Burning, Lancinating Pain Unusual sensitivity or tenderness when feet are touched (allodynia) Signs Diminished vibratory perception Absent or reduced knee and ankle reflexes Reduced protective sensation such as pressure, hot and cold, pain Diminished ability to sense position of toes and feet Small muscle weakness and wasting & overcompensation of large muscles ( hammer toe, loss of handgrip) Symptoms and signs progress from distal to proximal over time Clinical Presentation DPN affects the limbs symmetrically and progresses from distal to proximal over time. DPN is characterized by a stocking and glove distribution Bilateral symmetrical distribution of signs and symptoms Affects lower limbs first Progresses from distal (toes) to proximal (knee) over time. Signs and symptoms progress from distal to proximal over time Diabetic Neuropathy (Boulton),



22 Focal Syndromes Onset acute and usually self limiting Due to vascular insult Peripheral: ulnar, median, radial, peroneal, femoral,lateral cutaneous of the thigh (Needs to be distinguished from entrapment syndromes- median, ulnar where Treatment is splinting or surgery) Cranial neuropathies: V. Rare; Involve the III,IV, VI, VII cranial Ns; Symptoms typically resolve in 2-3 months. Truncal neuropathy: Subacute; Painful paresthesias in the trunk, either unilateral or bilateral. Diabetic Amyotrophy: long standing diabetics with poor control; Severe neuropathic pain and uni- or bilateral muscle weakness and atrophy in proximal thigh muscles Spinal stenosis is common in people with diabetes and should be differentiated from proximal neuropathies and amyotrophy Focal Neuropathies 22
23 Clinical Manifestations of Autonomic Neuropathy Cardiovascular: GI Postural Hypotension, Postparandial hypotension, Fixed tachycardia, Sudden cardiac death Esophageal motility disorders, Gastroparesis, Constipation, diarrhea Genitourinary Sexual Dysfunction, Bladder dysfunction Clinical features to Distinguish Neuropathy and Vascular Disease Characteristics Neuropathy Vascular Disease Site of pain Feet > calves Calves, thigh, buttocks >feet Quality of pain Sharp/ Superficial / Deep ache burning /tingling Present at rest Common Rare Effect of walking Pain improves Pain worse Pain worse in bed Yes NO Preceded by recent BS change Sometimes NO 23



24 Check Between Toes 24




25 JAMA 2005;293: Tuning Fork test 128Hz Tuning Fork Ball of Rt or Lt big toe OR bony prominence bilaterally situated at the dorsum of the first toe just proximal to the nail bed. 25
26 26

27 Treatment of DPN 1. Treat specific underlying pathogenic mechanism 2. Treat symptoms and improve quality of life 3. Prevention of progression and treatment of complications 27

28 Anti-depressants Inhibit re-uptake of NE, serotonin or both NRI: Desipramine, Amitriptyline, nortriptyline SSRI: Paroxetine, Fluoxetine,Sertraline Dual selective inhibitor: Duloxetine, venlafaxine Anti-cholinergic effects, orthostatic hypotension and sexual side effects limit use. 28
29 Anticonvulsants Carbamazepine 200mg BID: shooting or electric shock like pain Gabapentin: Reduced pain, improved sleep. (Weight gain) Pregabalin: Significantly improved pain scores ( Somnolence, ataxia, confusion) Topiramate: Reduced pain score, pain intensity and sleep disruption 29

30 Algorithm for Treatment of Symptomatic DPN 30
31 31
32 Diabetic Retinopathy Diabetic Retinopathy Diabetes is the leading cause of new cases of blindness in adults aged 20 to 74 years Incidence of blindness 25 times higher than the non diabetic population Diabetic retinopathy is responsible for 12,000 to 24,000 new cases of blindness each year After 20 years of diabetes, >60% of patients with type 1 or 2 diabetes have some degree of retinopathy 32

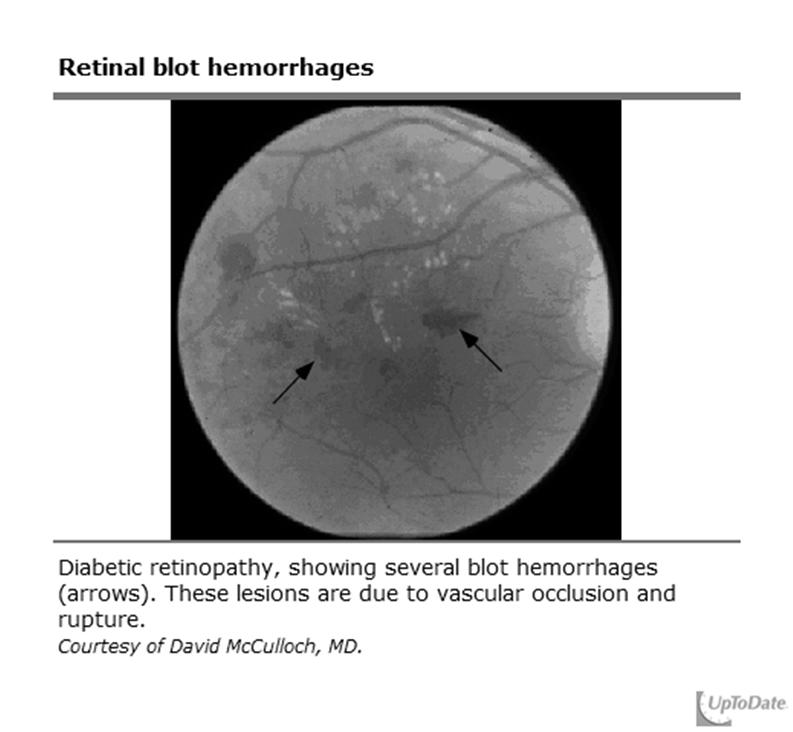
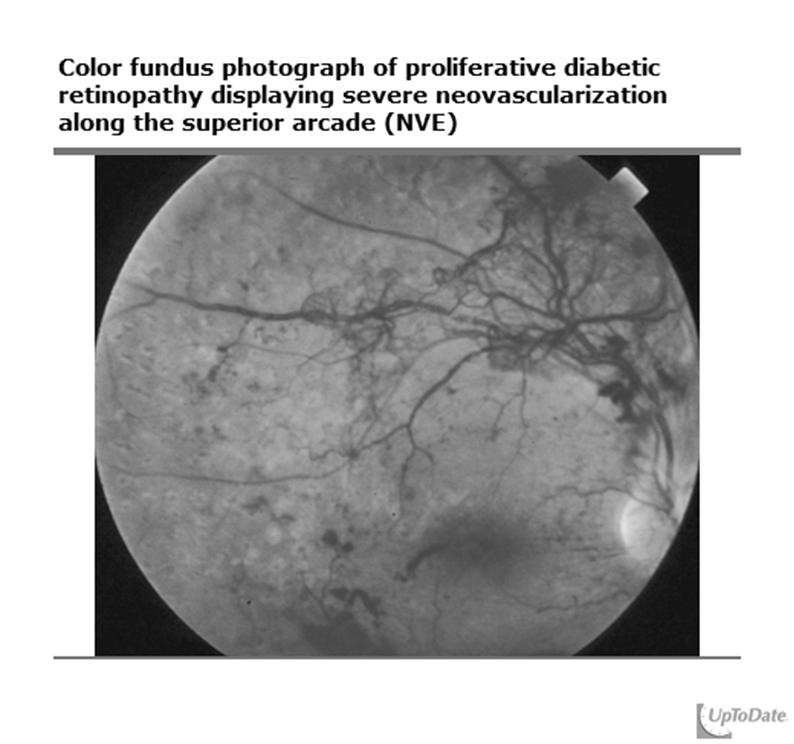
33 Classification of Diabetic Retinopathy Mild nonproliferative Moderate and severe nonproliferative diabetic retinopathy Proliferative American Diabetes Association. Diabetes Care. 2001;24(suppl 1):S73-S76. 33
34 34
35 35
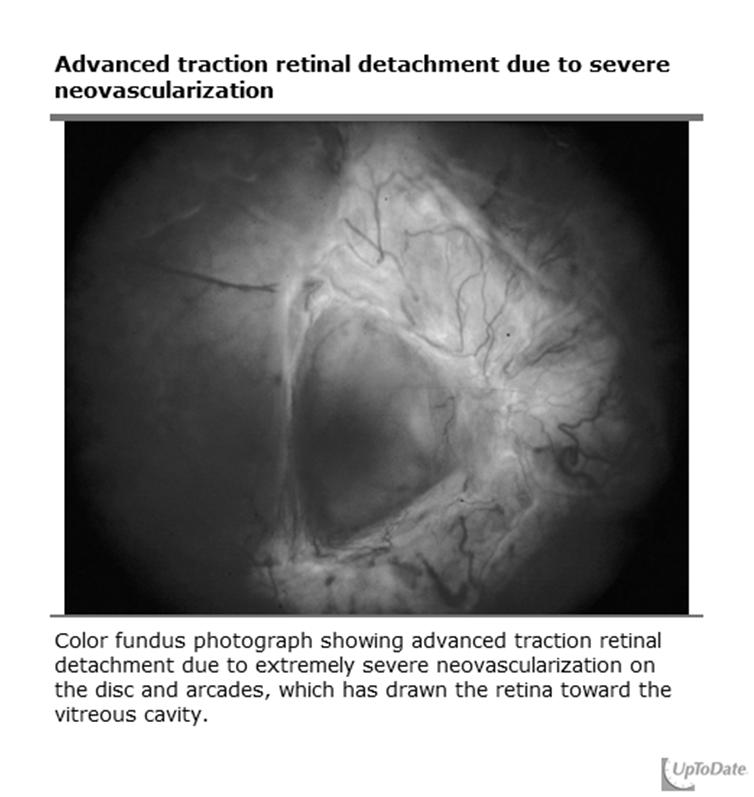
36 Visual loss from Diabetic Retinopathy Macular edema Hemorrhage from new vessels Retinal detachment Neovascular Glaucoma Natural History of DR 36
37 Prevalence of Retinopathy vs Duration of Type 2 Diabetes Patients with retinopathy (%) Time of diagnosis Apparent onset prior to diagnosis Years Harris MI et al. Diabetes Care. 1992;15:
38 Natural History of DR Transient worsening with intensive insulin therapy Worsening during pregnancy DCCT:EDIC in Type 1DM 11 Conventional group encouraged to switch to intensive treatment HbA 1c (%) Conventional Intensive DCCT DCCT end EDIC Year Adapted from: N Engl J Med 1993;329:977 86, EDIC: JAMA : Presentation Title Presenter Name Date Subject Business Use Only Main Menu 38
 60 60 Percentage of Patients Developing Retinopathy 50 40 30 20 10 p<0.001 50 40 30 20 10 p<0.")
39 Diabetic Retinopathy Benefits of Tight Glycemic Control (DCCT) Patients with Type 1 Diabetes Receiving Either Intensive or Conventional Treatment Primary-Prevention Cohort (n=726) Secondary-Prevention Cohort (n=715) Percentage of Patients Developing Retinopathy p< p< Year of Study Year of Study Conventional Intensive DCCT: Diabetes Control of Complications Trial Intensive therapy: external insulin pump or three or more daily insulin injections and frequent blood glucose monitoring. Conventional therapy: 1 or 2 daily insulin injections. DCCT Research Group. N Engl J Med. 1993;329: Presentation Title Presenter Name Date Subject Business Use Only Main Menu 39
40 40
41 Summary of Epidemiologic Studies Microvascular complications are predicted by Duration of diabetes A1C Blood pressure 41
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
DIABETES MEASURES GROUP OVERVIEW
 2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
130/80 vs. 140/90 If nephropathy is present the target should be 120/ /10/07
 DG van Zyl Macro vascular Micro vascular Neuropathy Infections Genetic susceptibility *Repeated acute changes in cellular metabolism Hyperglycemia Tissue damage **Cumulative long term changes in stable
DG van Zyl Macro vascular Micro vascular Neuropathy Infections Genetic susceptibility *Repeated acute changes in cellular metabolism Hyperglycemia Tissue damage **Cumulative long term changes in stable
Microvascular Disease in Type 1 Diabetes
 Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Diabetic Retinopathy and Neuropathy: 2018 Clinical Practice Guidelines
 Diabetic Retinopathy and Neuropathy: 2018 Clinical Practice Guidelines Richard Arakaki, M.D. Phoenix Area Diabetes Consultant August 9 th 2018 Disclose no conflict of interest Complications and Co-morbidities
Diabetic Retinopathy and Neuropathy: 2018 Clinical Practice Guidelines Richard Arakaki, M.D. Phoenix Area Diabetes Consultant August 9 th 2018 Disclose no conflict of interest Complications and Co-morbidities
Diabetes Complications. Rezvan Salehidoost, M.D., Endocrinologist
 Diabetes Complications Rezvan Salehidoost, M.D., Endocrinologist Different Diabetes Complications Macro vascular Micro vascular Infections Macro vascular Complications Macro-vascular Complications Ischemic
Diabetes Complications Rezvan Salehidoost, M.D., Endocrinologist Different Diabetes Complications Macro vascular Micro vascular Infections Macro vascular Complications Macro-vascular Complications Ischemic
Microvascular Complications
 Comprehensive education course for Asian diabetes educators Microvascular Complications Keimyung University Dongsan Medical Center Mi Kyung Kim Conflict of interest disclosure None Committee of Scientific
Comprehensive education course for Asian diabetes educators Microvascular Complications Keimyung University Dongsan Medical Center Mi Kyung Kim Conflict of interest disclosure None Committee of Scientific
Diabetic & Complications. Dr. A K Viswanath Consultant Diabetologist
 Diabetic & Complications Dr. A K Viswanath Consultant Diabetologist Outline Challenges in diabetes How do we fare? Diabetes complications Improving outcomes in diabetes Types of Diabetes Type-1 DM Genetic
Diabetic & Complications Dr. A K Viswanath Consultant Diabetologist Outline Challenges in diabetes How do we fare? Diabetes complications Improving outcomes in diabetes Types of Diabetes Type-1 DM Genetic
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Modified version focused on CCNC Quality Measures and Feedback Processes
 Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Diabetic Peripheral Neuropathy: Assessment and Treatment
 Diabetic Peripheral Neuropathy: Assessment and Treatment Denise Soltow Hershey PhD, FNP-BC Michigan Council of Nurse Practitioners Annual Conference March 17, 2018 Objectives 1) Describe the clinical features
Diabetic Peripheral Neuropathy: Assessment and Treatment Denise Soltow Hershey PhD, FNP-BC Michigan Council of Nurse Practitioners Annual Conference March 17, 2018 Objectives 1) Describe the clinical features
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Diabetic Neuropathy WHAT IS DIABETIC NEUROPATHY?
 Diabetic Neuropathy WHAT IS DIABETIC NEUROPATHY? D iabetic neuropathy is actually a group of nerve diseases. All of these disorders affect the peripheral nerves, that is, the nerves that are outside the
Diabetic Neuropathy WHAT IS DIABETIC NEUROPATHY? D iabetic neuropathy is actually a group of nerve diseases. All of these disorders affect the peripheral nerves, that is, the nerves that are outside the
Diabetic Neuropathy An Overview. Dr. Mark Hannon MD MSc FRCPI Consultant Physician and Endocrinologist Bantry General Hospital Septebmer 20 th 2017
 Diabetic Neuropathy An Overview Dr. Mark Hannon MD MSc FRCPI Consultant Physician and Endocrinologist Bantry General Hospital Septebmer 20 th 2017 Neuropathy in Diabetes Overall, one of the most common
Diabetic Neuropathy An Overview Dr. Mark Hannon MD MSc FRCPI Consultant Physician and Endocrinologist Bantry General Hospital Septebmer 20 th 2017 Neuropathy in Diabetes Overall, one of the most common
MANAGEMENT OF DIABETIC NEUROPATHY. Chungnam University Hospital Soo-Kyung, Bok, M.D., Ph.D.
 MANAGEMENT OF DIABETIC NEUROPATHY Chungnam University Hospital Soo-Kyung, Bok, M.D., Ph.D. The Diabetic neuropathy cannot be reversed Not to restore function to damaged nerve Slowly progress no initial
MANAGEMENT OF DIABETIC NEUROPATHY Chungnam University Hospital Soo-Kyung, Bok, M.D., Ph.D. The Diabetic neuropathy cannot be reversed Not to restore function to damaged nerve Slowly progress no initial
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Chronic kidney disease-what can you do and when to refer?
 Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Microvascular Complications in Diabetes:
 Microvascular Complications in Diabetes: Perspectives on Glycemic Control to Prevent Microvascular Complications Discussion Outline: Glycemia and Microvascular Compliations Clinical Trials - A Brief History
Microvascular Complications in Diabetes: Perspectives on Glycemic Control to Prevent Microvascular Complications Discussion Outline: Glycemia and Microvascular Compliations Clinical Trials - A Brief History
Complications of Diabetes Mellitus
 Complications of diabetes mellitus Complications of Diabetes Mellitus Chronic Complications of Diabetes Mellitus Microvascular Retinopathy (nonproliferative/proliferative) Nephropathy Neuropathy Sensory
Complications of diabetes mellitus Complications of Diabetes Mellitus Chronic Complications of Diabetes Mellitus Microvascular Retinopathy (nonproliferative/proliferative) Nephropathy Neuropathy Sensory
THE FORGOTTEN COMPLICATION M. Pfeifer
 Diabetic Neuropathy THE FORGOTTEN COMPLICATION M. Pfeifer P 1 The Burden of Diabetic Peripheral Neuropathy Most common peripheral neuropathy in the developed nations Major contributor to the hospital rate
Diabetic Neuropathy THE FORGOTTEN COMPLICATION M. Pfeifer P 1 The Burden of Diabetic Peripheral Neuropathy Most common peripheral neuropathy in the developed nations Major contributor to the hospital rate
Mædica - a Journal of Clinical Medicine. University of Oradea, Institute for Doctoral Studies, Oradea, Bihor County, Romania
 MAEDICA a Journal of Clinical Medicine 2018; 13(3): 229-234 https://doi.org/10.26574/maedica.2018.13.3.229 Mædica - a Journal of Clinical Medicine Original paper Diabetic Neuropathy Prevalence and Its
MAEDICA a Journal of Clinical Medicine 2018; 13(3): 229-234 https://doi.org/10.26574/maedica.2018.13.3.229 Mædica - a Journal of Clinical Medicine Original paper Diabetic Neuropathy Prevalence and Its
STANDARDS OF MEDICAL CARE IN DIABETES 2014
 STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
Disclosures. Outline. Outline 5/23/17 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Disclosures. Outline. Outline 7/27/2017 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Agenda. American Diabetes Association Diabetic Complications Diabetes Coding Guidelines & ICD-10 Codes Documentation
 Diabetes Agenda American Diabetes Association Diabetic Complications Diabetes Coding Guidelines & ICD-10 Codes Documentation American Diabetes Association American Diabetes Association Diabetic Eye Complications
Diabetes Agenda American Diabetes Association Diabetic Complications Diabetes Coding Guidelines & ICD-10 Codes Documentation American Diabetes Association American Diabetes Association Diabetic Eye Complications
DIAGNOSIS OF DIABETIC NEUROPATHY
 DIAGNOSIS OF DIABETIC NEUROPATHY Dept of PM&R, College of Medicine, Korea University Dong Hwee Kim Electrodiagnosis ANS Clinical Measures QST DIAGRAM OF CASUAL PATHWAYS TO FOOT ULCERATION Rathur & Boulton.
DIAGNOSIS OF DIABETIC NEUROPATHY Dept of PM&R, College of Medicine, Korea University Dong Hwee Kim Electrodiagnosis ANS Clinical Measures QST DIAGRAM OF CASUAL PATHWAYS TO FOOT ULCERATION Rathur & Boulton.
Complications of Diabetes: Screening and Prevention. Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley
 Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
CHRONIC COMPLICATIONS OF DIABETES MELLITUS
 CHRONIC COMPLICATIONS OF Microvascular complications: Diabetic retinopathy Diabetic nephropathy Diabetic neuropathy Macrovascular complications DIABETES MELLITUS Systemic atheroscerosis Mixted: diabetic
CHRONIC COMPLICATIONS OF Microvascular complications: Diabetic retinopathy Diabetic nephropathy Diabetic neuropathy Macrovascular complications DIABETES MELLITUS Systemic atheroscerosis Mixted: diabetic
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care
: Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care") Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
CLINICIAN INTERVIEW A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY. Interview with Ralph Rabkin, MD
 A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
Standards of Medical Care in Diabetes 2018
 Standards of Medical Care in Diabetes 2018 Eric L. Johnson, M.D. Associate Professor University of North Dakota School of Medicine and Health Sciences Assistant Medical Director Altru Diabetes Center Grand
Standards of Medical Care in Diabetes 2018 Eric L. Johnson, M.D. Associate Professor University of North Dakota School of Medicine and Health Sciences Assistant Medical Director Altru Diabetes Center Grand
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Diabetes Complications Recognition and Treatment
 Diabetes Complications Recognition and Treatment Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Diabetes is the most difficult of all
Diabetes Complications Recognition and Treatment Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Diabetes is the most difficult of all
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Painful Diabetic Neuropathy Effective Management. Ketan Dhatariya Consultant in Diabetes NNUH
 Painful Diabetic Neuropathy Effective Management Ketan Dhatariya Consultant in Diabetes NNUH Neuropathic Pain Prevalence varies between 10 and 90% depending on classification Accounts for 50-75% of non-traumatic
Painful Diabetic Neuropathy Effective Management Ketan Dhatariya Consultant in Diabetes NNUH Neuropathic Pain Prevalence varies between 10 and 90% depending on classification Accounts for 50-75% of non-traumatic
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
A Fork in the Road: Navigating Through New Terrain
 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Slide notes: The major chronic complications of diabetes mellitus are described here. Among these, microvascular complications have an important
 1 2 The major chronic complications of diabetes mellitus are described here. Among these, microvascular complications have an important role. They comprise microangiopathy, diabetic retinopathy, diabetic
1 2 The major chronic complications of diabetes mellitus are described here. Among these, microvascular complications have an important role. They comprise microangiopathy, diabetic retinopathy, diabetic
Chapter 37: Exercise Prescription in Patients with Diabetes
 Chapter 37: Exercise Prescription in Patients with Diabetes American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York:
Chapter 37: Exercise Prescription in Patients with Diabetes American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York:
Diabetes has become the most common
 P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Chronic Complications of Diabetes Mellitus. Professor Mamdouh El-Nahas Professor of Internal Medicine Endocrinology and Diabetes Unit
 Chronic Complications of Diabetes Mellitus Professor Mamdouh El-Nahas Professor of Internal Medicine Endocrinology and Diabetes Unit Chronic complications of Diabetes Macro Vascular Coronary Heart Dis.
Chronic Complications of Diabetes Mellitus Professor Mamdouh El-Nahas Professor of Internal Medicine Endocrinology and Diabetes Unit Chronic complications of Diabetes Macro Vascular Coronary Heart Dis.
Practical upates in Diabetes & CV risk management: Brief Updates Neurological complications in diabetes
 Practical upates in Diabetes & CV risk management: Brief Updates Neurological complications in diabetes Slides presented during CDMC in Almaty, Kazakhstan on Sunday April 13, 2014 and prepared by: Boris
Practical upates in Diabetes & CV risk management: Brief Updates Neurological complications in diabetes Slides presented during CDMC in Almaty, Kazakhstan on Sunday April 13, 2014 and prepared by: Boris
The World Health Organization (WHO) has described diabetes mellitus as Metabolic
 has described diabetes mellitus as Metabolic") 1.1. Background The World Health Organization (WHO) has described diabetes mellitus as Metabolic disorder of multiple etiology characterized by chronic hyperglycemia with disturbances of carbohydrate,
1.1. Background The World Health Organization (WHO) has described diabetes mellitus as Metabolic disorder of multiple etiology characterized by chronic hyperglycemia with disturbances of carbohydrate,
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease
 Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
8/28/2017. Learning Objectives. Microvascular Complications
 Microvascular Complications: Implications for Providers and their Patients with Diabetes Eileen Egan, DNP, FNP C, CDE Chief Nurse Practitioner NYU Winthrop Endocrine, Diabetes and Metabolism Faculty Practice
Microvascular Complications: Implications for Providers and their Patients with Diabetes Eileen Egan, DNP, FNP C, CDE Chief Nurse Practitioner NYU Winthrop Endocrine, Diabetes and Metabolism Faculty Practice
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic Conditions 2019 COLLECTION
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic Conditions 2019 COLLECTION
Diabetes in Renal Patients. Contents. Understanding Diabetic Nephropathy
 Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
The signs and symptoms of diabetic neuropathy vary, depending on the type of neuropathy and which nerves are affected.
 DIABETIC NEUROPATHY Overview Diabetic neuropathy is a type of nerve damage that can occur if you have diabetes. High blood sugar (glucose) can injure nerve fibers throughout your body, but diabetic neuropathy
DIABETIC NEUROPATHY Overview Diabetic neuropathy is a type of nerve damage that can occur if you have diabetes. High blood sugar (glucose) can injure nerve fibers throughout your body, but diabetic neuropathy
Diabetes and Kidney Disease. Kris Bentley Renal Nurse practitioner 2018
 Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
PDF of Trial CTRI Website URL -
 Clinical Trial Details (PDF Generation Date :- Sat, 03 Nov 2018 09:24:50 GMT) CTRI Number Last Modified On 10/06/2013 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
Clinical Trial Details (PDF Generation Date :- Sat, 03 Nov 2018 09:24:50 GMT) CTRI Number Last Modified On 10/06/2013 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications
 American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reversal of Microalbuminuria A Causative Factor of Diabetic Nephropathy is Achieved with ACE Inhibitors than Strict Glycemic Control
 ISSN 0976 3333 Available Online at www.ijpba.info International Journal of Pharmaceutical & Biological Archives 2013; 4(5): 923-928 ORIGINAL RESEARCH ARTICLE Reversal of Microalbuminuria A Causative Factor
ISSN 0976 3333 Available Online at www.ijpba.info International Journal of Pharmaceutical & Biological Archives 2013; 4(5): 923-928 ORIGINAL RESEARCH ARTICLE Reversal of Microalbuminuria A Causative Factor
November 16-18, 2017 Hotel Monteleone New Orleans, LA. Provided by
 November 16-18, 2017 Hotel Monteleone New Orleans, LA Provided by Diabetic Neuropathy: A Global and Growing Problem John D. England, MD Louisiana State University Health Sciences Center School of Medicine
November 16-18, 2017 Hotel Monteleone New Orleans, LA Provided by Diabetic Neuropathy: A Global and Growing Problem John D. England, MD Louisiana State University Health Sciences Center School of Medicine
Diabetes. Health Care Disparities: Medical Evidence. A Constellation of Complications. Every 24 hours.
 Health Care Disparities: Medical Evidence Diabetes Effects 2.8 Million People in US 7% of the US Population Sixth Leading Cause of Death Kenneth J. Steier, DO, MBA, MPH, MHA, MGH Dean of Clinical Education
Health Care Disparities: Medical Evidence Diabetes Effects 2.8 Million People in US 7% of the US Population Sixth Leading Cause of Death Kenneth J. Steier, DO, MBA, MPH, MHA, MGH Dean of Clinical Education
Slide 1. Slide 2. Slide 3. A Fork in the Road: Navigating Through New Terrain. Diabetes Standards of Care Then and Now
 Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 17 Caring for Clients with Diabetes Mellitus Diabetes Mellitus Chronic disease Not a single disorder
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 17 Caring for Clients with Diabetes Mellitus Diabetes Mellitus Chronic disease Not a single disorder
The CARI Guidelines Caring for Australasians with Renal Impairment. Antihypertensive therapy in diabetic nephropathy GUIDELINES
 Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Summary of Recommendation Statements Kidney International Supplements (2013) 3, 5 14; doi: /kisup
 3, 5 14; doi: /kisup") http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of
http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of
Diabetes Complications Guideline Based Screening, Management, and Referral
 Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Glucose and CV disease
 Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
The Internist s Approach to Neuropathy
 The Internist s Approach to Neuropathy VOLKAN GRANIT, MD, MSC ASSISTANT PROFESSOR OF NEUROLOGY NEUROMUSCU LAR DIVISION UNIVERSITY OF MIAMI, MILLER SCHOOL OF MEDICINE RELEVANT DECLARATIONS Financial disclosures:
The Internist s Approach to Neuropathy VOLKAN GRANIT, MD, MSC ASSISTANT PROFESSOR OF NEUROLOGY NEUROMUSCU LAR DIVISION UNIVERSITY OF MIAMI, MILLER SCHOOL OF MEDICINE RELEVANT DECLARATIONS Financial disclosures:
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
DCCT Diabetes Control & Complications Trial
 DCCT Diabetes Control & Complications Trial A. Vinik MD, PhD, FCP, MACP, FACE, Καθηγητής και Αντιπρόεδρος για την Έρευνα, Ιατρική Σχολή Ανατολικής Βιρτζίνια, Κέντρο Ενδοκρινολογικών και Μεταβολικών Νοσημάτων,
DCCT Diabetes Control & Complications Trial A. Vinik MD, PhD, FCP, MACP, FACE, Καθηγητής και Αντιπρόεδρος για την Έρευνα, Ιατρική Σχολή Ανατολικής Βιρτζίνια, Κέντρο Ενδοκρινολογικών και Μεταβολικών Νοσημάτων,