Standard NICE (CG ) RCP (2016)
|
|
|
- Dulcie Chapman
- 6 years ago
- Views:
Transcription
1
2
3 Standard NICE (CG ) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute stroke to a hyperacute stroke unit providing active management of physiological status and homeostasis within 4 hours of arrival at hospital Brain imaging Immediate brain scan (next slot, but definitely within one hour) Due thrombolysis or early anticoagulation On anticoagulant treatment A known bleeding tendency GCS < 13 Unexplained progressive or fluctuating symptoms Papilloedema, neck stiffness or fever Severe headache at onset of stroke symptoms Otherwise as soon as possible (within a maximum of 24 hours after onset of symptoms) Patients with suspected acute stroke should receive brain imaging urgently and at most within 1 hour of arrival at hospital.


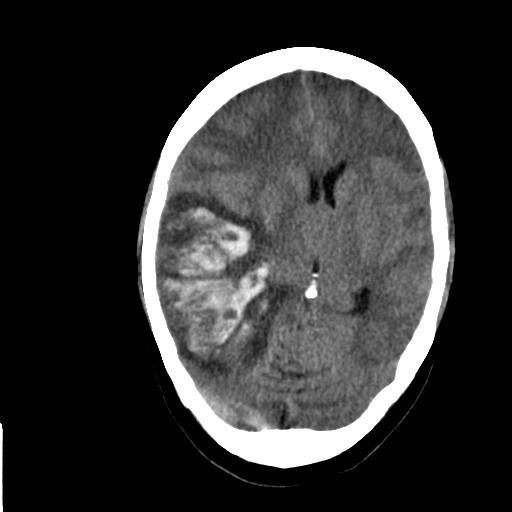
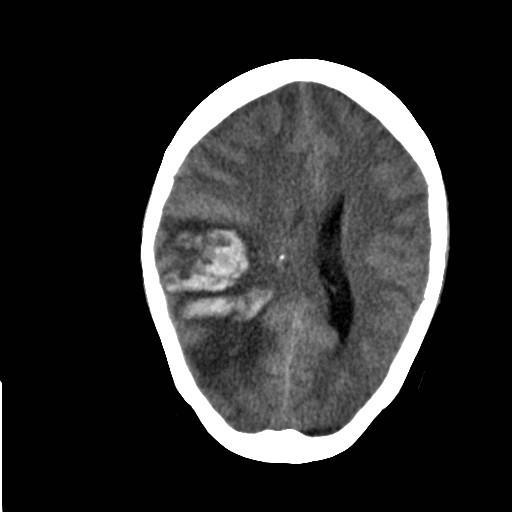
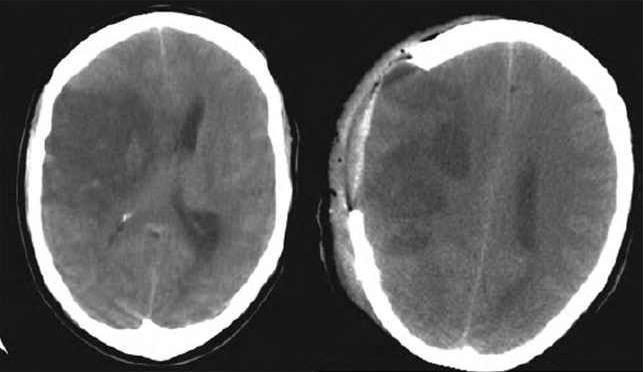
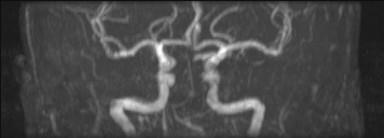
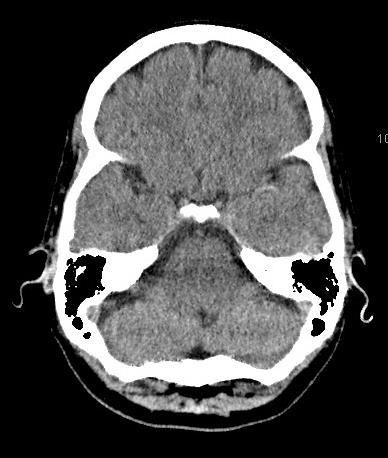
4 CT venogram
5 Standard NICE (CG ) RCP (2016) Cerebral venous sinus thrombosis People diagnosed with cerebral venous sinus thrombosis (including those with secondary cerebral haemorrhage) should be given full-dose anticoagulation treatment (initially full-dose heparin and then warfarin [INR 2 3]) unless there are comorbidities that preclude its use. Patients with cerebral venous thrombosis (including those with secondary cerebral haemorrhage) should receive full-dose anticoagulation (initially full-dose heparin and then warfarin with a target INR of 2 3) for at least three months unless there are comorbidities that preclude their use.
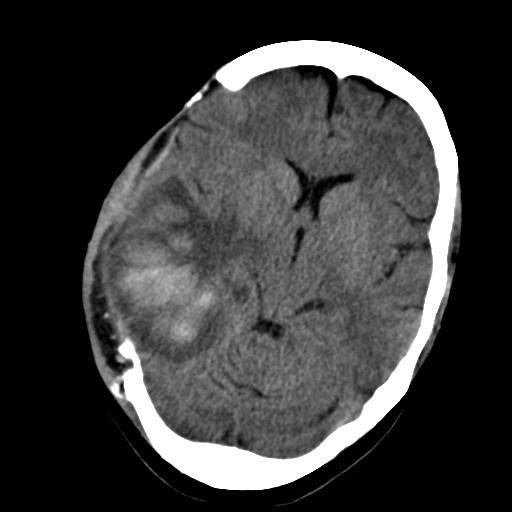
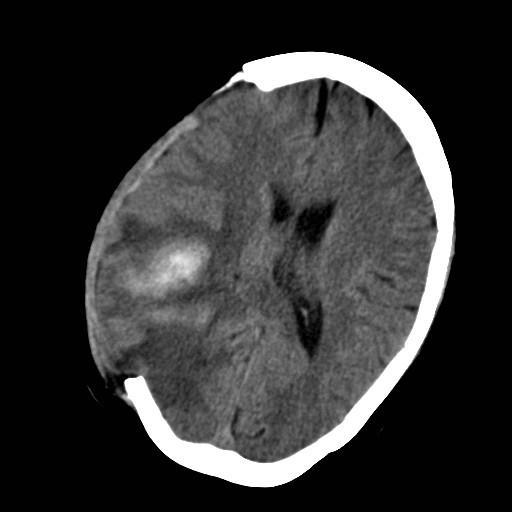
6 Overnight GCS e2 m4 v1 = 7 Pupils: R 7mm, L 4mm (both unreactive) Protected airway, B/C stable
7
8
9 Cerebral Venous Sinus Thrombosis Overall CVT to arterial stroke ratio 1:63 but 1:8 for ages M:3F Presentation Acute, subacute or chronic Headache (75%), papilloedema (50%), seizures (50%), focal deficits (50%), altered consciousness (33%) Complications: pulmonary embolism
10 Cerebral Venous Sinus Thrombosis Predisposing conditions Hypercoagulable states Anticoagulant deficiency Protein C/S deficiency, antithrombin III Hereditary, Acquired liver disease, nephrotic syn, pregnancy, postpartum, oestrogens Dysfunctional coagulation Activated protein C resistance, prothrombin mutation Hyperhomocysteinaemia Antiphospholipid antibody syndrome Thyrotoxicosis ( fviii levels) Heparin induced thrombocytopaenia Inflammatory bowel disease
11 Cerebral Venous Sinus Thrombosis Low flow states Iron def anaemia Diabetic ketoacidosis Polycythaemia Hyperviscosity syndromes Vessel wall abnormalities Infectious phlebitis (eg. mastoid infection) Non-infectious phlebitis (eg carcinoma, behcets) Trauma
12 Cerebral Venous Sinus Thrombosis Clinical evidence Anticoagulation 2 RCTS (n=79): Cochrane probably safe, but not conclusive is widely used LMW lower mortality than UFH Decompressive hemicraniectomy Multicentre registry % independent 16% died 33% with bilateral fixed pupils recovered completely Ongoing trials Thrombolysis or Anticoagulation for Cerebral Venous Thrombosis (TO-ACT) trial
13
14 Standard NICE (CG ) RCP (2016) Decompressive hemicraniectomy for malignant middle cerebral artery infarction People with middle cerebral artery infarction who meet all of the criteria below should be considered for decompressive hemicraniectomy. They should be referred within 24 hours of onset of symptoms and treated within a maximum of 48 hours. Aged 60 years or under. Clinical deficits suggestive of infarction in the territory of the middle cerebral artery, with a score on the National Institutes of Health Stroke Scale (NIHSS) of above 15. Decrease in the level of consciousness to give a score of 1 or more on item 1a of the NIHSS. Signs on CT of an infarct of at least 50% of the middle cerebral artery territory, with or without additional infarction in the territory of the anterior or posterior cerebral artery on the same side, or infarct volume greater than 145 cm3 as shown on diffusion weighted MRI. Patients with middle cerebral artery (MCA) infarction who meet the criteria below should be considered for decompressive hemicraniectomy. Patients should be referred to neurosurgery within 24 hours of stroke onset and treated within 48 hours of stroke onset: pre-stroke modified Rankin Scale score of less than 2 clinical deficits indicating infarction in the territory of the MCA National Institutes of Health Stroke Scale (NIHSS) score of more than 15; a decrease in the level of consciousness to a score of 1 or more on item 1a of the NIHSS; signs on CT of an infarct of at least 50% of the MCA territory with or without additional infarction in the territory of the anterior or posterior cerebral artery on the same side, or infarct volume greater than 145 cubic centimetres on diffusion-weighted MRI.
15

16


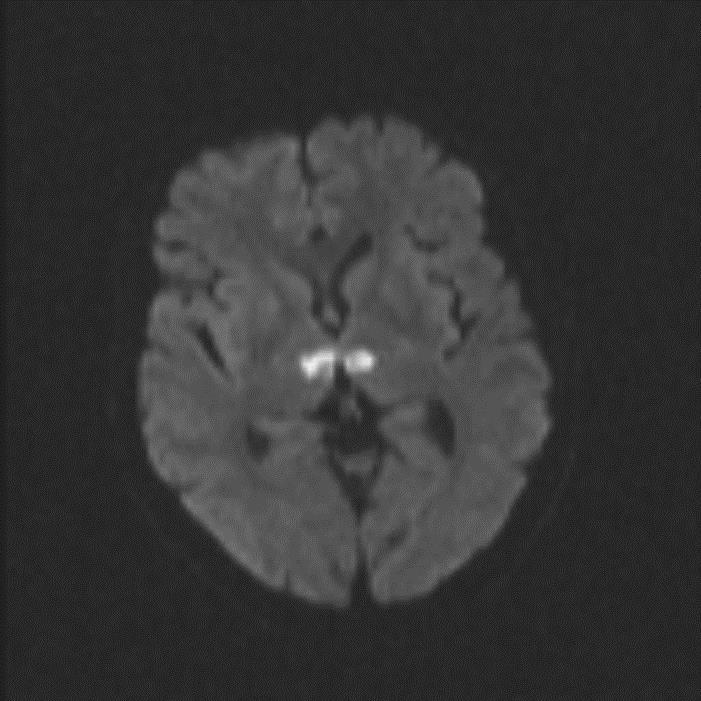
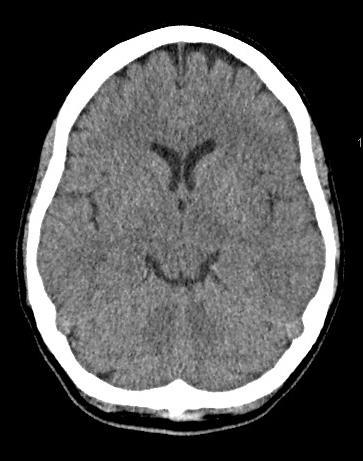
17 Normal

18

19 Clinical features of BAO The location and length of the vascular occlusion determines the clinical picture, ranging from mild motor deficits to tetraplegia Vertigo, nausea, vomiting 54-73% Bulbar, pseudobulbar weakness 74% Hemiparesis, tetraparesis, facial weakness 40-67% Dysarthria 30-63% Headache 40-42% Visual disturbances 21-33% Altered consciousness 17-33% Abnormal movement (shivering, twitching, shaking or jerking on the relatively spared side)
20
21
22 Making the correct diagnosis Difficulties in diagnosis Stroke ED presentations with dizziness, vertigo or imbalance 4-6% cerebrovascular event Kerber et al. Stroke (10) Navi et al. Mayo Clin Proc (11) Chase et al. Mayo Clin Proc (2) FAST less sensitive for posterior circulation stroke FAST 1 in 61% posterior vs 92% anterior strokes (p<0.0001) MRI DWI can often be negative especially small brainstem infarcts Markus et al. JNNP (2): 228-9
23 Making the correct diagnosis Clinical tools to use to aid differentiation of acute vestibular syndrome continuous vertigo ABCD2 902 pts with AVS presentations to ED 219 (24%) had ABCD2 2 - none had stroke as cause HINTS - Head Impulse, Nystagmus (fast-phase alternating), Test of Skew Stroke referrals : 56% confirmed stroke HINTS +ve sensitivity 97%, specificity 84% Navi et al. Stroke : Newman-Toker et al Acad Emer Med 2013: 20(10):
24 HINTS testing in continuous vertigo Head Impulse, Nystagmus, Test of Skew Think central cause stroke if: Nystagmus direction-changing Skew deviation present Head impulse R & L normal
25 People with continuous vertigo Test element Peripheral cause Central cause Head impulse test Abnormal Normal Nystagmus Alternate eye cover testing Unidirectional horizontal Skew deviation absent Rotatory, vertical or direction-changing horizontal Skew (vertical) deviation present
26
27

 of myelinated fibers Saver. Stroke.")
28 Time IS brain a typical large vessel acute ischemic stroke Each minute Each hour 1.9 million neurons 14 billion synapses 12 km (7.5 miles) of myelinated fibers 120 million neurons 830 billion synapses 714 km (447 miles) of myelinated fibers Saver. Stroke.2006;37:
29 Time IS brain Intravenous thrombolysis with alteplase for acute ischaemic stroke Individual patient data analysis, n=2775 Odds ratio for a complete recovery (at 3 months)
30 Standard NICE (CG ) RCP (2016) Thrombolysis Alteplase is recommended for the treatment of acute ischaemic stroke when used by physicians trained and experienced in the management of acute stroke. It should only be administered in centres with facilities that enable it to be used in full accordance with its marketing authorisation Alteplase should be administered only within a well organised stroke service with: staff trained in delivering thrombolysis and in monitoring for any complications associated with thrombolysis, level 1 and level 2 nursing care staff trained in acute stroke and thrombolysis, immediate access to imaging and re-imaging, and staff trained to interpret the images. Patients with acute ischaemic stroke, regardless of age or stroke severity, in whom treatment can be started within 3 hours of known onset should be considered for treatment with alteplase.

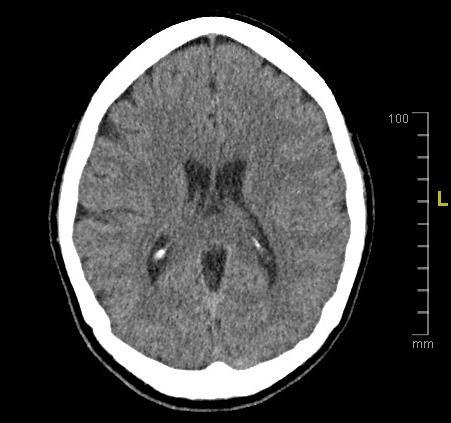
31 ASPECTS Criteria A normal CT scan receives ASPECTS of 10 points. To compute the ASPECTS, 1 point is subtracted from 10 for any evidence of early ischemic change for each of the defined regions OF MCA territory
32


33 Stent Retrievers 3 rd Generation endovascular stroke treatment Immediate flow restoration Trap thrombus within stent struts and retrieved Solitaire Trevo
34
35

36

37





38 What to bleeding do?
39 Standard NICE (CG ) RCP (2016) Acute intracerebral haemorrhage anticoagulant reversal Clotting levels in people with a primary intracerebral haemorrhage who were receiving anticoagulation treatment before their stroke (and have elevated INR) should be returned to normal as soon as possible, by reversing the effects of the anticoagulation treatment using a combination of prothrombin complex concentrate and intravenous vitamin K. Patients with intracerebral haemorrhage in association with vitamin K antagonist treatment should have the anticoagulant urgently reversed with a combination of prothrombin complex concentrate and intravenous vitamin K. Patients with intracerebral haemorrhage in association with dabigatran treatment should have the anticoagulant urgently reversed with idarucizumab. Patients with intracerebral haemorrhage in association with factor Xa inhibitor treatment should receive urgent treatment with 4-factor prothrombin complex concentrate.
40 Standard NICE (CG ) RCP (2016) Acute intracerebral haemorrhage blood pressure Patients with primary intracerebral haemorrhage who present within 6 hours of onset with a systolic blood pressure above 150mmHg should be treated urgently using a locally agreed protocol for blood pressure lowering to a systolic blood pressure of 140 mmhg for at least 7 days, unless: the Glasgow Coma Scale score is 5 or less; the haematoma is very large and death is expected; a structural cause for the haematoma is identified; immediate surgery to evacuate the haematoma is planned.
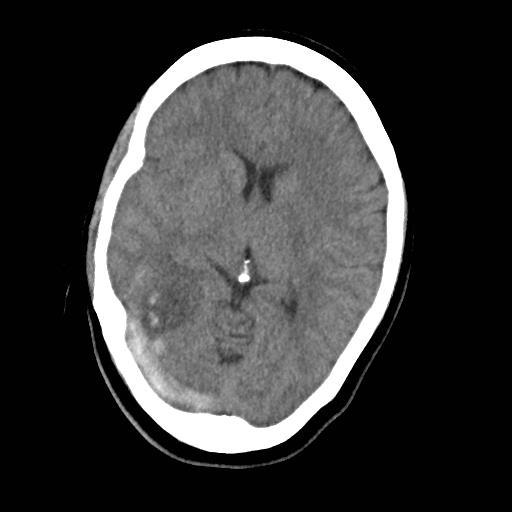
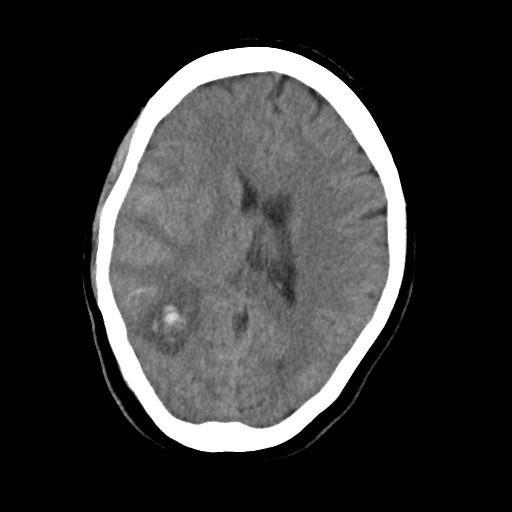
41 Standard NICE (CG ) RCP (2016) Acute intracerebral haemorrhage - surgery Previously fit people should be considered for surgical intervention following primary intracranial haemorrhage if they have hydrocephalus People with any of the following rarely require surgical intervention and should receive medical treatment initially: small deep haemorrhages lobar haemorrhage without either hydrocephalus or rapid neurological deterioration a large haemorrhage and significant comorbidities before the stroke a score on the Glasgow Coma Scale of below 8 unless this is because of hydrocephalus posterior fossa haemorrhage. Patients with intracranial haemorrhage who develop hydrocephalus should be considered for surgical intervention such as insertion of an external ventricular drain. Most patients with primary intracerebral haemorrhage do not require surgical intervention and should receive monitoring and initial medical treatment on a hyperacute stroke unit, such as those with small, deep haemorrhage lobar haemorrhage without hydrocephalus, intraventricular haemorrhage or neurological deterioration large haemorrhage and significant co-morbidities before the stroke those with supratentorial haemorrhage with a Glasgow Coma Scale score below 8 unless this is because of hydrocephalus.
42 Answer: C
43 Question 1 A 65-year-old right handed woman developed a sudden inability to speak properly while she was talking to her neighbour. Her husband brought her to hospital immediately and described the problem as if she were talking double Dutch. Her past medical history comprised hypertension and osteoarthritis. She was taking bendroflumethiazide 2.5mg od and prn codeine. On examination, there was obvious word-finding difficulties and problems correctly naming objects. Understanding appeared to be intact. Her blood pressure was 190/100 mmhg. There was no other abnormality on examination. What is the next best step in management? A B C D E Amlodipine 5mg orally Ateplase 0.9 mg/kg intravenously Aspirin 300mg orally Clopidogrel 300mg orally Tenecteplase 50mg intravenously (Remember in the exam the correct answer is the NICE guideline answer, followed by specialist society guidelines, followed by consensus). Answer: B
44 Question 4 A 75-year-old man developed sudden left sided numbness and weakness which was still present at the time of assessment in the Emergency Department. He had been given 300mg aspirin orally by paramedics. His past medical history comprised paroxysmal AF which had been DC cardioverted. He was not taking any regular medication. He was a right handed driver with no other past medical history. On examination, he had objective reduced power on the left side of his body (4/5) but no other abnormality. He was alert and orientated. His NIH Stroke Score was calculated to be 3. An urgent CT scan of the head was normal. In which part of the brain has this stroke occurred? A B C D E Clinically impossible to say Left internal capsule Pons Right MCA territory Thalamus Answer A
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Guideline Stroke and transient ischaemic attack in over 16s: diagnosis and initial management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Stroke and transient ischaemic attack in over s: diagnosis and initial management Draft for consultation, November 0 This guideline covers interventions
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Stroke and transient ischaemic attack in over s: diagnosis and initial management Draft for consultation, November 0 This guideline covers interventions
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS
 STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Sinus and Cerebral Vein Thrombosis
 Sinus and Cerebral Vein Thrombosis A Summary Sinus and cerebral vein clots are uncommon. They can lead to severe headaches, confusion, and stroke-like symptoms. They may lead to bleeding into the surrounding
Sinus and Cerebral Vein Thrombosis A Summary Sinus and cerebral vein clots are uncommon. They can lead to severe headaches, confusion, and stroke-like symptoms. They may lead to bleeding into the surrounding
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
LA CLINICA E LA DIAGNOSI DELLA VERTIGINE VASCOLARE
 LA CLINICA E LA DIAGNOSI DELLA VERTIGINE VASCOLARE M. Mandalà Azienda Ospedaliera Universitaria Senese WHY ARE WE SCARED? NEED TO BETTER UNDERSTAND PATHOPHYSIOLOGY WHAT IS KNOWN WHAT IS EFFECTIVE and SIMPLE
LA CLINICA E LA DIAGNOSI DELLA VERTIGINE VASCOLARE M. Mandalà Azienda Ospedaliera Universitaria Senese WHY ARE WE SCARED? NEED TO BETTER UNDERSTAND PATHOPHYSIOLOGY WHAT IS KNOWN WHAT IS EFFECTIVE and SIMPLE
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
CONCISE GUIDE National Clinical Guidelines for Stroke 2nd Edition
 CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Lothian Audit of the Treatment of Cerebral Haemorrhage (LATCH)
") 1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Arterial Ischemic Stroke with Protein S Deficiency in Pakistan
 Case Reports Arterial Ischemic Stroke with Protein S Deficiency in Pakistan Faika Usman, Ali Hassan, Arsalan Ahmad From Section of Neurology, Department of Medicine, Shifa International Hospitals and College
Case Reports Arterial Ischemic Stroke with Protein S Deficiency in Pakistan Faika Usman, Ali Hassan, Arsalan Ahmad From Section of Neurology, Department of Medicine, Shifa International Hospitals and College
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Guideline for the Acute Management of Stroke in Paediatric Patients with Sickle Cell Disease
 Guideline for the Acute Management of Stroke in Paediatric Patients with Sickle Cell Disease Summary Outline of the presentation of stroke in paediatric patients with sickle cell disease, urgent investigations,
Guideline for the Acute Management of Stroke in Paediatric Patients with Sickle Cell Disease Summary Outline of the presentation of stroke in paediatric patients with sickle cell disease, urgent investigations,
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Developing, implementing and scaling up an acute care bundle for intracerebral haemorrhage in Greater Manchester
 Developing, implementing and scaling up an acute care bundle for intracerebral haemorrhage in Greater Manchester Adrian Parry-Jones NIHR Clinician Scientist & Honorary Consultant Neurologist Manchester
Developing, implementing and scaling up an acute care bundle for intracerebral haemorrhage in Greater Manchester Adrian Parry-Jones NIHR Clinician Scientist & Honorary Consultant Neurologist Manchester
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Guidelines for management of stroke in childhood
 Guidelines for management of stroke in childhood A clinical syndrome typified by rapidly developing signs of focal or global disturbance of cerebral functions, lasting more than 24 hrs or leading to death,
Guidelines for management of stroke in childhood A clinical syndrome typified by rapidly developing signs of focal or global disturbance of cerebral functions, lasting more than 24 hrs or leading to death,
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
HYPERACUTE STROKE CASE STUDIES. By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH
 HYPERACUTE STROKE CASE STUDIES By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH MC Case study 82 years old, lady 9:30 well, in touch with her son 11:30 hairdresser came to her house and found her
HYPERACUTE STROKE CASE STUDIES By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH MC Case study 82 years old, lady 9:30 well, in touch with her son 11:30 hairdresser came to her house and found her
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
CT INTERPRETATION COURSE
 CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
CT INTERPRETATION COURSE Refresher Course ASTRACAT October 2012 Stroke is a Clinical Diagnosis A clinical syndrome characterised by rapidly developing clinical symptoms and/or signs of focal loss of cerebral
Patients presenting with acute stroke while on DOACs
 Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
About 700,000 Americans each year suffer a new or recurrent stroke. On average, a stroke occurs every 45 seconds
 UCLA Stroke Center Stroke Facts About 700,000 Americans each year suffer a new or recurrent stroke On average, a stroke occurs every 45 seconds Stroke kills more than 150,000 people a year (1 of every
UCLA Stroke Center Stroke Facts About 700,000 Americans each year suffer a new or recurrent stroke On average, a stroke occurs every 45 seconds Stroke kills more than 150,000 people a year (1 of every
Appendix A: Summary of evidence from surveillance
 Appendix A: Summary of evidence from surveillance 8-year surveillance (2016) stroke and transient ischaemic attack in over 16s (2008) NICE guideline CG68 Summary of new evidence from surveillance... 1
Appendix A: Summary of evidence from surveillance 8-year surveillance (2016) stroke and transient ischaemic attack in over 16s (2008) NICE guideline CG68 Summary of new evidence from surveillance... 1
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Acute Vestibular Syndrome (AVS) 12/5/2017
 12/5/2017") Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Stroke Workshop. Pre-Workshop Handout. With Walter Himmel, Meeta Patel & Anton Helman
 2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around
2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around
Successful Endovascular Revascularization of Acute Basilar Artery Occlusion Approached via an Aberrant Right Subclavian Artery
 Journal of Neuroendovascular Therapy 2017; 11: 416 420 Online April 27, 2017 DOI: 10.5797/jnet.cr.2016-0109 Successful Endovascular Revascularization of Acute Basilar Artery Occlusion Approached via an
Journal of Neuroendovascular Therapy 2017; 11: 416 420 Online April 27, 2017 DOI: 10.5797/jnet.cr.2016-0109 Successful Endovascular Revascularization of Acute Basilar Artery Occlusion Approached via an
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Stroke and TIA management in adults: guidelines for the first 72 hours of symptomonset Trust Ref: C23/2015
 Stroke and TIA management in adults: guidelines for the first 72 hours of symptomonset Trust Ref: C23/2015 1. Introduction Guidelines and principal related documents for the management of adults presenting
Stroke and TIA management in adults: guidelines for the first 72 hours of symptomonset Trust Ref: C23/2015 1. Introduction Guidelines and principal related documents for the management of adults presenting
Overview. Introduction. New Interventions for Acute Stroke. New Approaches to hemorrhagic Strokes
 Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Anticoagulants. Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT
 Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Sinus Venous Thrombosis
 Sinus Venous Thrombosis Joseph J Gemmete, MD FACR, FSIR, FAHA Professor Departments of Radiology and Neurosurgery University of Michigan Hospitals Ann Arbor, MI Outline Introduction Medical Treatment Options
Sinus Venous Thrombosis Joseph J Gemmete, MD FACR, FSIR, FAHA Professor Departments of Radiology and Neurosurgery University of Michigan Hospitals Ann Arbor, MI Outline Introduction Medical Treatment Options