Imitrex Speaker Training
|
|
|
- Albert Pearson
- 5 years ago
- Views:
Transcription


1 Neuro- Ophthalmology and the Healthcare Team Aljoeson Walker,MD Neuro-Ophthalmology Director, General Neurology Division Department of Neurology and Storm Eye Institute Medical University of South Carolina Charleston, South Carolina Vision loss- acute and chronic Corneal defects Retinal changes Lens displacement or related changes Check vision Eye chart The EYE Examination Distance vision Near vision Presbyopia check age + lens Vision A subjective disorders with objective findings. The presence of the rapd Changes in the back of the eye Pallor Edema inflammation 1






2 Tools for vision testing Direct light Vision cover/uncover Eye/vision chart Color vision Visual field testing- confrontational, automated MRI/MRA/CT 2

3 Retinal Physiology Cones Rods Swinging light test First have the patient look into the distance Next determine the reactivity of the pupils Next shine the light into the eyes, right no more than 3 seconds then the contra lateral eye. Normal is no change in the contra lateral pupil initially when contacted by the light. Abnormal is the dilation of the contra lateral pupil when contacted by the light. Direct Standard Pan optic Fundus Examination Both to review the vascular changes Both to review the optic nerve Slit Lamp Ophthalmologist/optometrist 3


4 Confrontational Operator/examiner Automated Humphrey Goldmann Visual fields Visual Field/Ophthalmic Terms Arcuate Monocular Binocular Chiasmal Postchiasmal Bitemporal hemianopia Congruous Incongruous Field/Ophthalmic Terminology Scotoma-depression of sensitivity to surroundings Central Paracentral cecocentral 4



5 Patient #1 56 year old Presents with sudden vision loss in the left eye There is pain No pain on eye movement Examination Noted rapd Pattern of loss on confrontation FUNDUS- swollen nerve- optic #1 Labs Sedimentation- rate normal?? MRI? Vitals Blood pressure? Anterior Ischemic Optic Neuropathy Loss of peripheral and/ or central vision Optic disc swelling Peripapillary swelling Common disorder Usually are Inferior hemifield most common affected NAION Pallor 5
6 Cont. Risk factors: small cup-to-disc Diabetes or hypertension Patient #2 72 year old Presents with sudden vision loss in the left eye There is pain No pain on eye movement Examination Noted rapd Pattern of loss on confrontation FUNDUS- swollen nerve- optic #2 Labs Sedimentation- rate elevated?? Evaluation continued: Consider Bx?? Bilateral or single If negative Then what-- MRI? Vitals Blood pressure? Arteritic AION Age onset s Vision loss seems more severe as a general rule Jaw claudication,temporal headache,weight loss,fatigue and joint pain. Lupus, polyarteritis nodosa, syphilis, and radiation necrosis Cont... ESR C - reactive protein TA bx- suggest at least a one inch sample 6



7 Patient #3 36 year old Presents with sudden vision loss -OU There is pain No pain on eye movement Examination Noted no - rapd Pattern of loss on confrontation FUNDUS- swollen nerve- optic IIH/PTCs Child bearing age Bilateral Nerve swelling, maybe edema(papilledema) Family Hx Medication effect treatments #3 Labs Sedimentation- rate normal?? MRI? Vitals Blood pressure? 7
8 Fundus- Nerves abnormal Patient #3 small- cup to disc ratio Asymmetric Why elevated pressure - new meds, trauma, non- compliance etc. Patient #4 28 year old Presents with sudden vision loss There is pain pain on eye movement Examination Noted rapd Pattern of loss on confrontation FUNDUS- no swollen nerve- optic #4 Labs Sedimentation- rate normal??? MRI? Vitals Blood pressure? Vision loss- acute and chronic Acute vision loss Optic neuritis MS Neuro-sarcoidosis cancer Ischemic/compressive/inflammatory Optic Neuritis 8


9 Vision-Most common complaint- sensory modality Classic pain on eye movement Optic nerve elevation Second event MS Diagnosis Signs of Multiple Sclerosis History Neurologic MRI CSF Spasticity Hyperreflexia Babinski s Dysmetria or tremor Nystagmus and diplopia Impaired vibratory Facial weakness Impaired pain/touch Impaired temperature Changes in intellectual function Diplopia. 9
10 Diplopia Double vision Definitions: Monocular or Binocular? Horizontal or vertical or oblique Constant or intermittent Presentation Sudden or chronic Associated events or conditions Terms related- maybe Visual Blurred vision Not clear Things look off I can not read I can not drive The examination Ductions Versions Monocular Diplopia Keratoconus Lens opacities Retinal pathology Macular pathology Deviation Old 6 th Divergence Insufficiency Bilateral 6 th 10
11 Incomitant Deviations Fusional amplitudes about 2 diopters vertical about diopters horizontal Retrictive Misalignment Thyroid- orbitopathy Post traumatic Orbital myositis Neoplasm Congenital Thyroid - Orbitopaty Most common Inferior and medial rectus most common Proptosis, chemosis, lid retraction and lid lag Evaluation- forced ductions, MRI- should reflect muscle change, but no tendon change Trauma If at the most posterior aspects of the orbital regionnear the cone- narrow region Blowout fractures Inferior orbital floor-entrapment- inferior rectus Medial rectus less likely Orbital myositis Ophthalmoplegia and pain Conjunctival hyperemia, chemosis, maybe proptosis Meningiomas Mets Neoplasms Usually found on MRI - NOTED tendon and muscle enlargement Maybe related to lupus, sarcoidosis or Wegener's granulomatosis 11
12 Congenital Brown syndrome Limited upgaze, when eye is adducted Short superior oblique tendon Fibrosis syndrome Agenesis ocular motoneurons in brain stem(superior division, 3 rd cranial nerve- atrophy superior rectus and lavator palpebrae muscles CFEOM- congenital fibrosis of the extraocular muscles- Autosomal dominate - bilateral ptosis and external Ophthalmoplegia Congenital cont-- Mobius syndrome Agenesis 6 th nerve nuclei and 7 th nerve nuclei Facial diplegia and ophthalmoplegia. May also have scoliosis and atrophy of the tongue Duane Retraction Syndrome Failure formation of the 6 th nerve nucleus Abducens paresis Aberrant co- contraction of the horizontal rectus muscle Anomalous branch of the 3 rd nerve w/n the orbit So, attempted adduction of the eye will trigger -retraction of the eye- narrowing of the lid fissures -- can be bilateral. Do not report diplopia Internuclear INO Medial longitudinal Fasciculus (MLF)- connecting the 6 th nerve nucleus on one side medial rectus subnucleus(3 rd ) on the contralateral side Slowed adducting saccadic velocity- nystagmus of the abducting eye. May have limited movement of the adducting eye. May have a skew deviation- ipsilateral to the lesion ( stroke- demyelination) One-and-a-half syndrome Pontine lesion big enough to affect the MLF and the PPRF or 6 th nerve nucleus on the same side Move only abduction of the contralateral eye ( stroke) Bilateral INO MLF dual lesion, but also have gaze evoked nystagmusnotes in upgaze- vertical vestibular nuclei. (stroke) Nuclear Fascicular Subarachnoid Divisional Aberrant 3 rd nerve Nuclear 3 rd Damage to one 3 rd nerve nucleus bilateral ptosis, bilateral dysfunction of both superior recti muscles and the usual- pupillary issues and eye movement abnormalities. Single (central caudal nucleus) and axons decussate just after they leave subnuclei- therefore lesion in the mid line region can affect both Fascicular 3 rd Cranial nerve injury beyond nucleus, but still in brainstem Weber syndrome Damage ventral midbrain/cerebral peduncle- contralateral hemiparesis Benedikt syndrome Damage red nucleus, substantia nigra- contralateral ataxia/tremor Claude syndrome Damage dorsal midbrain, superior cerebellar peduncle- contralateral ataxia Nothnagel syndrome Damage dorsal lesion- plus 3 rd nerve lesion- supranuclear eye dysfunction and ataxia 12
13 Subarachnoid Brainstem to the cavernous sinus Cause is usually microvascular injury to the nerve Risk factors DM, HTN, lipids 3 rd nerve palsy- complete Ptosis, downward, outward deficit and pupil dilated microvascular injuries, compression, infiltrative disorders, increased intracranial pressure Pupil- involving 3 rd nerve palsy If incomplete concern for compression Aneurysms Post. Communicating/internal carotid Pupil- sparing 3 rd nerve palsy Complete loss of lid function and movement from the 3 rd nerve microvascular Usually DM MRA/CTA to evaluate Pupillary Dysfunction Normal lid and extraocular movements Usually benign Adie tonic Pharmacologic Divisional 3rd Two divisions in the cavernous sinus Superior Inferior Usually other cranial nerves are involved rare in isolation 13



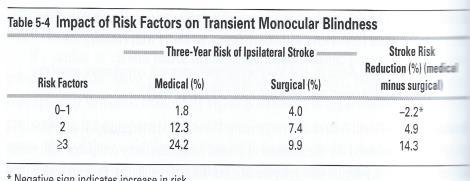
14 4 th nerve Worse in down gaze and head tilt Transient vision loss 83 The approach to this clinical situation- WHAT ARE THE QUESTION- -is the vision loss monocular or binocular Carotid artery or retinal circulation or optic nerve Posterior circulation or migraine- visual cortex Younger than 50 - migraine, vasospasm - Pregnant- eclampsia Shade coming down TIA uhthoff syndrome How old is the patient Older than 50 - consider TIA, GCA If vascular 15 minutes or less/more vasospasm/migraine What was the duration of the visual loss What was the pattern of visual loss and recovery Monocular loss 1-10 minutes 70-90% ipsilateral carotid Vision loss lasing seconds- optic disc drusen,papilledema 84 fortification spectra's optic neuroticism 85 14
15 Determine the status of the afferent visual axis Best corrected vision Visual fields Afferent pupillary defects Fundus exam What to look at atrophy, vascular abnormalities or orbital disease blepharospasm Cannot keep the eyes open -irregularity of the corneal tear film Testing- slit lamp reveal abnormal-apperaing film and cornea. Rapiid tearfilm break down and punctal keratopathy - schirmers Ocular continued Hyphema UGH Large PVD Angle-closure glaucoma Macular degeneration- delayed vision recovery exposed to light Deatachment Orbital Hemangioma Meningioma -intraconal mass Positional maybe with looking down Papilledema- grayouts Disc anomalies- drusen, high myopia and colobomas Systemic Retinovascular Embolic Retinal circulation- Cardiovascular - painless vision loss - amaurosis fugax -lasting 2-30 minutes Sudden painless Three types Lasting 2-30 minutes -cholesterol -platelet-fibrin 90 -calcium 91 15

16 Other cause- Hypercoable states, mitral valve prolapse, cardiac arrhythmias, GCA, vasospasms-migraine, HTN, DM, CADASIL Laboratory evaluation- Angiogram >1% with experience MRA - carotid dissection Echocardiogram -valves Risk for vision loss Vasculitis Usuaslly over 50 years old -sed rate C-reactive proein hypoperfusion 94 Ocular ischemic syndrome- 95 Migraine Transient Binocular vision Loss Most common cause Occipital mass/lesion Fixed defficit unlateral or central


17
Neuro-Ocular Grand Rounds
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-ophthalmologyophthalmology. Marek Michalec, MD.
 Neuro-ophthalmologyophthalmology Marek Michalec, MD. Neuro-ophthalmology Study integrating ophthalmology and neurology Disorders affecting parts of CNS devoted to vision or eye: Afferent system (visual
Neuro-ophthalmologyophthalmology Marek Michalec, MD. Neuro-ophthalmology Study integrating ophthalmology and neurology Disorders affecting parts of CNS devoted to vision or eye: Afferent system (visual
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Alan G. Kabat, OD, FAAO (901)
") THE SWOLLEN OPTIC DISC: EMERGENCY OR ANOMALY? Alan G. Kabat, OD, FAAO (901) 252-3691 Memphis, Tennessee alan.kabat@alankabat.com Course description: The swollen disc presents a diagnostic dilemma. While
THE SWOLLEN OPTIC DISC: EMERGENCY OR ANOMALY? Alan G. Kabat, OD, FAAO (901) 252-3691 Memphis, Tennessee alan.kabat@alankabat.com Course description: The swollen disc presents a diagnostic dilemma. While
3/16/2018. Optic Nerve Examination. Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital
 Air Force Hospital") Optic Nerve Examination Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital 1 Examination Structure ( optic disc) Function Examination of the optic disc The only cranial nerve (brain tract) which
Optic Nerve Examination Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital 1 Examination Structure ( optic disc) Function Examination of the optic disc The only cranial nerve (brain tract) which
OCT : retinal layers. Extraocular muscles. History. Central vs Peripheral vision. History: Temporal course. Optical Coherence Tomography (OCT)
") Optical Coherence Tomography (OCT) OCT : retinal layers 7 Central vs Peripheral vision Extraocular muscles RPE E Peripheral Vision: Rods (95 million) 30% Ganglion cells Central Vision: Cones (5 million)
Optical Coherence Tomography (OCT) OCT : retinal layers 7 Central vs Peripheral vision Extraocular muscles RPE E Peripheral Vision: Rods (95 million) 30% Ganglion cells Central Vision: Cones (5 million)
Learn Connect Succeed. JCAHPO Regional Meetings 2017
 Learn Connect Succeed JCAHPO Regional Meetings 2017 NO FINANCIAL DISCLOSURES Technician s Role in Neuro-Ophthalmology Workup Beth Koch COT, ROUB Cleveland 9/16/2017 What Tests Are You Expected To Perform?
Learn Connect Succeed JCAHPO Regional Meetings 2017 NO FINANCIAL DISCLOSURES Technician s Role in Neuro-Ophthalmology Workup Beth Koch COT, ROUB Cleveland 9/16/2017 What Tests Are You Expected To Perform?
Lecture Content. Disorders of optic nerve and retina Chiasmal and retrochiasmal disorders Pupil disorders Motility disorders
 Neuro-Ophthalmology Celia H. Chang MD Department of Neurology MIND Institute University of California, Davis, Health System celia.chang@ucdmc.ucdavis.edu Lecture Content Disorders of optic nerve and retina
Neuro-Ophthalmology Celia H. Chang MD Department of Neurology MIND Institute University of California, Davis, Health System celia.chang@ucdmc.ucdavis.edu Lecture Content Disorders of optic nerve and retina
BRAINSTEM SYNDROMES OF NEURO-OPHTHALMOLOGICAL INTEREST
 BRAINSTEM SYNDROMES OF NEURO-OPHTHALMOLOGICAL INTEREST Steven L. Galetta, MD NYU Langone Medical Center New York, NY I. Anatomical Considerations The brain stem is about the size of a fat forefinger and
BRAINSTEM SYNDROMES OF NEURO-OPHTHALMOLOGICAL INTEREST Steven L. Galetta, MD NYU Langone Medical Center New York, NY I. Anatomical Considerations The brain stem is about the size of a fat forefinger and
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
Optic Nerve Disorders: Structure and Function and Causes
 Optic Nerve Disorders: Structure and Function and Causes Using Visual Fields, OCT and B-scan Ultrasound to Diagnose and Follow Optic Nerve Visual Losses Ohio Ophthalmological Society and Ophthalmic Tech
Optic Nerve Disorders: Structure and Function and Causes Using Visual Fields, OCT and B-scan Ultrasound to Diagnose and Follow Optic Nerve Visual Losses Ohio Ophthalmological Society and Ophthalmic Tech
Re-Double. Ron Teed, M.D. 12 January 2007 Vanderbilt Eye Institute. Alfred Bielschowsky
 Re-Double Ron Teed, M.D. 12 January 2007 Vanderbilt Eye Institute Alfred Bielschowsky Patient History I cc: vertical binocular diplopia 63 yo male with 4 week history of diplopia; first intermittent, then
Re-Double Ron Teed, M.D. 12 January 2007 Vanderbilt Eye Institute Alfred Bielschowsky Patient History I cc: vertical binocular diplopia 63 yo male with 4 week history of diplopia; first intermittent, then
Jacqueline Theis, O.D., F.A.A.O.
 Neuro-Ophthalmological Emergencies Presenting in Primary Care Optometry Describes the symptoms, signs, and management of neuro-ophthalmological emergencies. Signs/Symptoms to be Concerned about (especially
Neuro-Ophthalmological Emergencies Presenting in Primary Care Optometry Describes the symptoms, signs, and management of neuro-ophthalmological emergencies. Signs/Symptoms to be Concerned about (especially
Learn Connect Succeed. JCAHPO Regional Meetings 2015
 Learn Connect Succeed JCAHPO Regional Meetings 2015 OPTIC NEUROPATHY AS EASY AS 1,2,3,4 OPTIC NERVE ANATOMY M. Tariq Bhatti, MD Departments of Ophthalmology and Neurology Duke Eye Center and Duke University
Learn Connect Succeed JCAHPO Regional Meetings 2015 OPTIC NEUROPATHY AS EASY AS 1,2,3,4 OPTIC NERVE ANATOMY M. Tariq Bhatti, MD Departments of Ophthalmology and Neurology Duke Eye Center and Duke University
NEURO 101 NEURO SYMPTOMS NEURO SIGNS. Transient Visual Obscurations AMAUROSIS FUGAX WORK-UP FOR AMAUROSIS
 NEURO 101 Jill Autry, O.D., R.Ph. Eye Center of Texas, Houston drjillautry@tropicalce.com NEURO SYMPTOMS Sudden or gradual vision loss/visual field loss AION, optic neuritis, compressive lesion Transient
NEURO 101 Jill Autry, O.D., R.Ph. Eye Center of Texas, Houston drjillautry@tropicalce.com NEURO SYMPTOMS Sudden or gradual vision loss/visual field loss AION, optic neuritis, compressive lesion Transient
Pupil Exams and Visual Fields
 Pupil Exams and Visual Fields A Closer Look at Cranial Nerves No Financial Interests Amy Jost does not have any financial interests related to this presentation AMY JOST, BS, COMT, CCRC, OSC CINCINNATI
Pupil Exams and Visual Fields A Closer Look at Cranial Nerves No Financial Interests Amy Jost does not have any financial interests related to this presentation AMY JOST, BS, COMT, CCRC, OSC CINCINNATI
THE BRAINSTEM. Raymond S. Price, MD University of Pennsylvania
 THE BRAINSTEM Raymond S. Price, MD University of Pennsylvania Overview of Brainstem Functions The brainstem serves numerous crucial neurologic functions. The most clinically relevant functions include:
THE BRAINSTEM Raymond S. Price, MD University of Pennsylvania Overview of Brainstem Functions The brainstem serves numerous crucial neurologic functions. The most clinically relevant functions include:
Carotid Cavernous Fistula
 Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Picture of patient with apparent lid retraction and poor elevation. Shows you Orbital CT-Scan with muscle involvement including IR and asks is this
 NEUROLOGY Q: MENINGIOMAS AND SKULL (*2) Real skull is given, and you are asked to point to tuberculum sella What kind of meningioma occurs at this location? Where is the anterior clinoid process? Where
NEUROLOGY Q: MENINGIOMAS AND SKULL (*2) Real skull is given, and you are asked to point to tuberculum sella What kind of meningioma occurs at this location? Where is the anterior clinoid process? Where
Faculty Financial Disclosure. Learning Objectives: Office Ophthalmology. Basic Eye Exam: What s in your pocket/office? Office Ophthalmology
 Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Neuro Ocular Grand Rounds Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD
 Neuro Ocular Grand Rounds Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD 58 YOWM! C/O I think there is something wrong with my vision, but I m not sure what it is.! +PMH for HTN, atrial fibrillation,
Neuro Ocular Grand Rounds Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD 58 YOWM! C/O I think there is something wrong with my vision, but I m not sure what it is.! +PMH for HTN, atrial fibrillation,
NEURO-OPHTHALMIC ASSESSMENT DR. B. C. UGWU
 CLINICAL VIGNETTE 2019; 5:1 NEURO-OPHTHALMIC ASSESSMENT DR. B. C. UGWU Editor-in-Chief: Prof Olufemi Idowu Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright-
CLINICAL VIGNETTE 2019; 5:1 NEURO-OPHTHALMIC ASSESSMENT DR. B. C. UGWU Editor-in-Chief: Prof Olufemi Idowu Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright-
Management of Diplopia Indiana Optometric Association Annual Convention April 2018 Kristine B. Hopkins, OD, MSPH, FAAO
 Management of Diplopia Indiana Optometric Association Annual Convention April 2018 Kristine B. Hopkins, OD, MSPH, FAAO For patients with diplopia, the clinician must differentiate monocular from binocular
Management of Diplopia Indiana Optometric Association Annual Convention April 2018 Kristine B. Hopkins, OD, MSPH, FAAO For patients with diplopia, the clinician must differentiate monocular from binocular
Objectives. Unexplained Vision Loss: Where Do I Go From Here. History. History. Drug Induced Vision Loss
 Objectives Unexplained Vision Loss: Where Do I Go From Here Denise Goodwin, OD, FAAO Coordinator, Neuro-ophthalmic Disease Clinic Pacific University College of Optometry goodwin@pacificu.edu Know the importance
Objectives Unexplained Vision Loss: Where Do I Go From Here Denise Goodwin, OD, FAAO Coordinator, Neuro-ophthalmic Disease Clinic Pacific University College of Optometry goodwin@pacificu.edu Know the importance
The Eye in Neurology: Evaluation of Sudden Visual Loss and Diplopia Diagnostic Pointers and Pitfalls
 143 The Eye in Neurology: Evaluation of Sudden Visual Loss and Diplopia Diagnostic Pointers and Pitfalls S C Loong,*FAMS, MBBS, FRACP Abstract The evaluation of sudden visual loss should begin with the
143 The Eye in Neurology: Evaluation of Sudden Visual Loss and Diplopia Diagnostic Pointers and Pitfalls S C Loong,*FAMS, MBBS, FRACP Abstract The evaluation of sudden visual loss should begin with the
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetazolamide, in idiopathic intracranial hypertension, 49 52, 60 Angiography, computed tomography, in cranial nerve palsy, 103 107 digital
Index Note: Page numbers of article titles are in boldface type. A Acetazolamide, in idiopathic intracranial hypertension, 49 52, 60 Angiography, computed tomography, in cranial nerve palsy, 103 107 digital
Vertical Muscles Transposition with Medical Rectus Botulinum Toxin Injection for Abducens Nerve Palsy
 JKAU: Med. Sci., Vol. 16 No. 2, pp: 43-49 (2009 A.D. / 1430 A.H.) DOI: 10.4197/Med. 16-2.4 Vertical Muscles Transposition with Medical Rectus Botulinum Toxin Injection for Abducens Nerve Palsy Nizar M.
JKAU: Med. Sci., Vol. 16 No. 2, pp: 43-49 (2009 A.D. / 1430 A.H.) DOI: 10.4197/Med. 16-2.4 Vertical Muscles Transposition with Medical Rectus Botulinum Toxin Injection for Abducens Nerve Palsy Nizar M.
Professor Helen Danesh-Meyer. Eye Institute Auckland
 Professor Helen Danesh-Meyer Eye Institute Auckland Bitten by Ophthalmology Emergencies Helen Danesh-Meyer, MBChB, MD, FRANZCO Sir William and Lady Stevenson Professor of Ophthalmology Head of Glaucoma
Professor Helen Danesh-Meyer Eye Institute Auckland Bitten by Ophthalmology Emergencies Helen Danesh-Meyer, MBChB, MD, FRANZCO Sir William and Lady Stevenson Professor of Ophthalmology Head of Glaucoma
Arielle Bokhour, class of 2017
 Arielle Bokhour, class of 2017 Objectives 1. Understand the actions and innervation of the extrinsic and intrinsic eye muscles 2. Describe the pathways for pupillary constriction and dilation 3. Understand
Arielle Bokhour, class of 2017 Objectives 1. Understand the actions and innervation of the extrinsic and intrinsic eye muscles 2. Describe the pathways for pupillary constriction and dilation 3. Understand
Learn Connect Succeed. JCAHPO Regional Meetings 2015
 Learn Connect Succeed JCAHPO Regional Meetings 2015 VISUAL FIELDS No financial conflicks Florida Society of Ophthalmology 2015 Gary Schemmer, MD Definition of Visual Field The area in space perceived by
Learn Connect Succeed JCAHPO Regional Meetings 2015 VISUAL FIELDS No financial conflicks Florida Society of Ophthalmology 2015 Gary Schemmer, MD Definition of Visual Field The area in space perceived by
C19. Pediatric Neuro-ophthalmology: Dilemmas in clinical practice. 12 June, :15 15:45. Room 115 HAND-OUTS
 C19 Pediatric Neuro-ophthalmology: Dilemmas in clinical practice 12 June, 2017 14:15 15:45 Room 115 HAND-OUTS Is this strabismus really harmful? Karl Golnik, MD, MEd University of Cincinnati, USA Childhood
C19 Pediatric Neuro-ophthalmology: Dilemmas in clinical practice 12 June, 2017 14:15 15:45 Room 115 HAND-OUTS Is this strabismus really harmful? Karl Golnik, MD, MEd University of Cincinnati, USA Childhood
Strabismus. A.Medghalchi,M.D Assistant professor of ophthalmology Gilan medical science university
 Strabismus A.Medghalchi,M.D Assistant professor of ophthalmology Gilan medical science university ۳ Anatomy Of The EOM s Six Extraocular muscles surround eye: Medial Rectus Lateral Rectus Superior Rectus
Strabismus A.Medghalchi,M.D Assistant professor of ophthalmology Gilan medical science university ۳ Anatomy Of The EOM s Six Extraocular muscles surround eye: Medial Rectus Lateral Rectus Superior Rectus
LECTURE # 7 EYECARE REVIEW: PART III
 LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
GNK485 The eye and related structures. Prof MC Bosman 2012
 GNK485 The eye and related structures Prof MC Bosman 2012 Surface anatomy Bony orbit Eyeball and Lacrimal apparatus Extra-ocular muscles Movements of the eye Innervation Arterial supply and venous drainage
GNK485 The eye and related structures Prof MC Bosman 2012 Surface anatomy Bony orbit Eyeball and Lacrimal apparatus Extra-ocular muscles Movements of the eye Innervation Arterial supply and venous drainage
Neurology Case Presentation. Rawan Albadareen, MD 12/20/13
 Neurology Case Presentation Rawan Albadareen, MD 12/20/13 Case presentation A 49 y.o. female presented to the ED after an episode of zigzagging w a jagged bright light crossing through her Rt visual field
Neurology Case Presentation Rawan Albadareen, MD 12/20/13 Case presentation A 49 y.o. female presented to the ED after an episode of zigzagging w a jagged bright light crossing through her Rt visual field
Case Follow Up. Sepi Jooniani PGY-1
 Case Follow Up Sepi Jooniani PGY-1 Triage 54 year old M Pt presents to prelim states noticed today he had reddness to eyes, states worse in R eye. Pt denies any pain or itching. No further complaints.
Case Follow Up Sepi Jooniani PGY-1 Triage 54 year old M Pt presents to prelim states noticed today he had reddness to eyes, states worse in R eye. Pt denies any pain or itching. No further complaints.
LOCALIZATION NEUROLOGY EPISODE IV EYE MOVEMENT AND FOOT DROP
 LOCALIZATION NEUROLOGY EPISODE IV EYE MOVEMENT AND FOOT DROP 1 EPISODE IV2012 EYE MOVEMENT LOCALIZATION NEUROLOGY DEPARTMENT of MEDICINE MAHARAT NAKORNRAJSIMA HOSPITAL PAWUT MEKAWICHAI MD 2 ABNORMAL EYE
LOCALIZATION NEUROLOGY EPISODE IV EYE MOVEMENT AND FOOT DROP 1 EPISODE IV2012 EYE MOVEMENT LOCALIZATION NEUROLOGY DEPARTMENT of MEDICINE MAHARAT NAKORNRAJSIMA HOSPITAL PAWUT MEKAWICHAI MD 2 ABNORMAL EYE
! Women greater than men (4:1)» Typical of other autoimmune diseases
» Typical of other autoimmune diseases") 1 2 3 4 : Overview and Diagnosis Suzanne K. Freitag, M.D. Director, Ophthalmic Plastic Surgery Massachusetts Eye and Ear Infirmary Harvard Medical School! I have no financial disclosures. Learning Objectives!
1 2 3 4 : Overview and Diagnosis Suzanne K. Freitag, M.D. Director, Ophthalmic Plastic Surgery Massachusetts Eye and Ear Infirmary Harvard Medical School! I have no financial disclosures. Learning Objectives!
University Journal of Surgery and Surgical Specialities
 University Journal of Surgery and Surgical Specialities Volume 1 Issue 1 2015 PARINAUD'S SYNDROME A CASE REPORT Basker K Shubha Raguram K Stanley Medical College Introduction: Gaze palsies are a group
University Journal of Surgery and Surgical Specialities Volume 1 Issue 1 2015 PARINAUD'S SYNDROME A CASE REPORT Basker K Shubha Raguram K Stanley Medical College Introduction: Gaze palsies are a group
Diagnosis and Management of Neuroophthalmic Disease: Rules, Exceptions to the Rules, and Exceptions to Exceptions to the Rules
 1 Diagnosis and Management of Neuroophthalmic Disease: Rules, Exceptions to the Rules, and Exceptions to Exceptions to the Rules Joseph W. Sowka, OD, FAAO, Diplomate Professor of Optometry Nova Southeastern
1 Diagnosis and Management of Neuroophthalmic Disease: Rules, Exceptions to the Rules, and Exceptions to Exceptions to the Rules Joseph W. Sowka, OD, FAAO, Diplomate Professor of Optometry Nova Southeastern
13/02/1440 بسم ا هلل ا لرحمن ا لر حيم
 بسم ا هلل ا لرحمن ا لر حيم 1 Slowly progressive versus rapidly progressive proptosis by Ali M ISMAIL professor of ophthalmology @SOHAG U H Occuloplastic fellow @NNUH Occuloplastic fellow @Cambridge UH
بسم ا هلل ا لرحمن ا لر حيم 1 Slowly progressive versus rapidly progressive proptosis by Ali M ISMAIL professor of ophthalmology @SOHAG U H Occuloplastic fellow @NNUH Occuloplastic fellow @Cambridge UH
Non-arteritic anterior ischemic optic neuropathy (NAION) with segmental optic disc edema. Jonathan A. Micieli, MD Valérie Biousse, MD
 with segmental optic disc edema. Jonathan A. Micieli, MD Valérie Biousse, MD") Non-arteritic anterior ischemic optic neuropathy (NAION) with segmental optic disc edema Jonathan A. Micieli, MD Valérie Biousse, MD A 75 year old white woman lost vision in the inferior part of her visual
Non-arteritic anterior ischemic optic neuropathy (NAION) with segmental optic disc edema Jonathan A. Micieli, MD Valérie Biousse, MD A 75 year old white woman lost vision in the inferior part of her visual
Help! My Baby s Eyes Are Crossed (or Something!)
") Help! My Baby s Eyes Are Crossed (or Something!) Madhuri Chilakapati, MD Ophthalmology Chief Complaint My baby has a lazy eye The eyes move funny The eyes don t move together The eyes get stuck The eyes
Help! My Baby s Eyes Are Crossed (or Something!) Madhuri Chilakapati, MD Ophthalmology Chief Complaint My baby has a lazy eye The eyes move funny The eyes don t move together The eyes get stuck The eyes
Course # Flashes and Floaters and Curtains, Oh My!
 Course # 132 Flashes and Floaters and Curtains, Oh My! FLASHES and FLOATERS and CURTAINS, OH MY!!! FLASHES OF LIGHT Vitreous is the villain Retinal traction Retinal hole Retinal tear Migraine Classic migraine
Course # 132 Flashes and Floaters and Curtains, Oh My! FLASHES and FLOATERS and CURTAINS, OH MY!!! FLASHES OF LIGHT Vitreous is the villain Retinal traction Retinal hole Retinal tear Migraine Classic migraine
Course # Flashes and Floaters and Curtains, Oh My!
 Course # 132 Flashes and Floaters and Curtains, Oh My! FLASHES and FLOATERS and CURTAINS, OH MY!!! FLASHES OF LIGHT Vitreous is the villain Retinal traction Retinal hole Retinal tear Migraine Classic migraine
Course # 132 Flashes and Floaters and Curtains, Oh My! FLASHES and FLOATERS and CURTAINS, OH MY!!! FLASHES OF LIGHT Vitreous is the villain Retinal traction Retinal hole Retinal tear Migraine Classic migraine
Imaging Orbit/Periorbital Injury
 Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Differential diagnosis and management of acquired sixth cranial nerve palsy
 Optometry (2006) 77, 534-539 Differential diagnosis and management of acquired sixth cranial nerve palsy Denise Goodwin, O.D. Pacific University College of Optometry, Forest Grove, Oregon. KEYWORDS Sixth
Optometry (2006) 77, 534-539 Differential diagnosis and management of acquired sixth cranial nerve palsy Denise Goodwin, O.D. Pacific University College of Optometry, Forest Grove, Oregon. KEYWORDS Sixth
Extraocular Muscles and Ocular Motor Control of Eye Movements
 Extraocular Muscles and Ocular Motor Control of Eye Movements Linda K. McLoon PhD mcloo001@umn.edu Department of Ophthalmology and Visual Neurosciences Your Eyes Are Constantly Moving. Yarbus, 1967 Eye
Extraocular Muscles and Ocular Motor Control of Eye Movements Linda K. McLoon PhD mcloo001@umn.edu Department of Ophthalmology and Visual Neurosciences Your Eyes Are Constantly Moving. Yarbus, 1967 Eye
Ocular Motility in Health and Disease
 Ocular Motility in Health and Disease Contents: Extraocular Muscles Eye Movements Single Binocular Vision Strabismus Amblyopia Objectives: By the end of this course the undergraduate student should be
Ocular Motility in Health and Disease Contents: Extraocular Muscles Eye Movements Single Binocular Vision Strabismus Amblyopia Objectives: By the end of this course the undergraduate student should be
OCULAR MOTILITY DISORDERS DUE TO BRAINSTEM DISEASE
 OCULAR MOTILITY DISORDERS DUE TO BRAINSTEM DISEASE Eric R. Eggenberger, DO, MSEpi Michigan State University Lansing, MI LEARNING OBJECTIVE 1. Review brainstem anatomy and its relevance to clinical presentations
OCULAR MOTILITY DISORDERS DUE TO BRAINSTEM DISEASE Eric R. Eggenberger, DO, MSEpi Michigan State University Lansing, MI LEARNING OBJECTIVE 1. Review brainstem anatomy and its relevance to clinical presentations
Ophthalmic Trauma Update
 Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
ASSESSING THE EYES. Structures. Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris.
 ASSESSING THE EYES Structures External Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris 1 2 Structures Internal Optic disc Physiological cup Retinal
ASSESSING THE EYES Structures External Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris 1 2 Structures Internal Optic disc Physiological cup Retinal
Pathologies of postchiasmatic visual pathways and visual cortex
 Pathologies of postchiasmatic visual pathways and visual cortex Optic radiation: anatomy Pathologies of the postchiamsatic visual pathways and visual cortex Characterized by homonymous hemianopsia. This
Pathologies of postchiasmatic visual pathways and visual cortex Optic radiation: anatomy Pathologies of the postchiamsatic visual pathways and visual cortex Characterized by homonymous hemianopsia. This
Strabismus. Nathalie Azar, MD Pediatric Ophthalmology for the Non-Ophthalmologist April 7, 2018 TERMINOLOGY:
 Strabismus Nathalie Azar, MD Pediatric Ophthalmology for the Non-Ophthalmologist April 7, 2018 TERMINOLOGY: Strabismus comes from the Greek word Strabismos which means to squint. For accuracy when describing
Strabismus Nathalie Azar, MD Pediatric Ophthalmology for the Non-Ophthalmologist April 7, 2018 TERMINOLOGY: Strabismus comes from the Greek word Strabismos which means to squint. For accuracy when describing
Rafik Girgis. Consultant Ophthalmic Surgeon ( Cataract & Primary Care)
") Rafik Girgis Consultant Ophthalmic Surgeon ( Cataract & Primary Care) Blepharitis Is a very common condition which usually bilateral & symmetrical. The main types are: Anterior, posterior or mixed Complications:
Rafik Girgis Consultant Ophthalmic Surgeon ( Cataract & Primary Care) Blepharitis Is a very common condition which usually bilateral & symmetrical. The main types are: Anterior, posterior or mixed Complications:
Unexplained visual loss in seven easy steps
 Unexplained visual loss in seven easy steps Andrew G. Lee, MD Chair Ophthalmology, Houston Methodist Hospital, Professor, Weill Cornell MC; Adjunct Professor, Baylor COM, U Iowa, UTMB Galveston, UT MD
Unexplained visual loss in seven easy steps Andrew G. Lee, MD Chair Ophthalmology, Houston Methodist Hospital, Professor, Weill Cornell MC; Adjunct Professor, Baylor COM, U Iowa, UTMB Galveston, UT MD
Midbrain Infarction Causing Diplopia and Atypical Neurological Symptoms: An Abducens Palsy Review
 Midbrain Infarction Causing Diplopia and Atypical Neurological Symptoms: An Abducens Palsy Review A 68 year old white male reports distance horizontal diplopia immediately following a cerebrovascular accident.
Midbrain Infarction Causing Diplopia and Atypical Neurological Symptoms: An Abducens Palsy Review A 68 year old white male reports distance horizontal diplopia immediately following a cerebrovascular accident.
Neuro Op Grand Rounds: Fields and Diplopia Utah Optometric Association June 2018
 Disclosures Neuro Op Grand Rounds: Fields and Diplopia Utah Optometric Association June 2018 I have received honorarium from the following: Glaukos CE in Italy Heidelberg Engineering Review of Optometry
Disclosures Neuro Op Grand Rounds: Fields and Diplopia Utah Optometric Association June 2018 I have received honorarium from the following: Glaukos CE in Italy Heidelberg Engineering Review of Optometry
Rapid Visual Loss. Dr Michael Johnson PhD FCOptom DipOrth DipGlauc DipTp(IP) Independent Prescribing Optometrist
 Independent Prescribing Optometrist") Rapid Visual Loss Dr Michael Johnson PhD FCOptom DipOrth DipGlauc DipTp(IP) Independent Prescribing Optometrist Outline Pathophysiology Differential diagnosis. Patient scenarios in community practice:
Rapid Visual Loss Dr Michael Johnson PhD FCOptom DipOrth DipGlauc DipTp(IP) Independent Prescribing Optometrist Outline Pathophysiology Differential diagnosis. Patient scenarios in community practice:
No Financial Interest
 Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Neuroradiology in the Ocular Motility Disorders :
 Neuroradiology in the Ocular Motility Disorders : I. Supranuclear Pathway 1 H y u ng-jin Kim, M.D. 1, 2, Byung Hoon Lim, M.D. 3, Jae Bum Na, M.D. Jae Hyoung Kim, M.D., Sung Hoon Chung, M.D. The supranuclear
Neuroradiology in the Ocular Motility Disorders : I. Supranuclear Pathway 1 H y u ng-jin Kim, M.D. 1, 2, Byung Hoon Lim, M.D. 3, Jae Bum Na, M.D. Jae Hyoung Kim, M.D., Sung Hoon Chung, M.D. The supranuclear
The science and art of handball : when have to do it fast, when you can do it slow
 AVC 2017 A primer on palsies aka The science and art of handball : when have to do it fast, when you can do it slow LIONEL KOWAL MELBOURNE MAGPIE A PRIMER ON PALSIES This is a Very difficult area A condition
AVC 2017 A primer on palsies aka The science and art of handball : when have to do it fast, when you can do it slow LIONEL KOWAL MELBOURNE MAGPIE A PRIMER ON PALSIES This is a Very difficult area A condition
Acute Visual Loss and Other Neuro- Ophthalmologic Emergencies: Management
 Acute Visual Loss and Other Neuro- Ophthalmologic Emergencies: Management Jennifer S. Graves, MD, PhD a,b, *, Steven L. Galetta, MD b,c KEYWORDS Vision loss Double vision Papilledema Optic neuropathy Neuro-ophthalmologic
Acute Visual Loss and Other Neuro- Ophthalmologic Emergencies: Management Jennifer S. Graves, MD, PhD a,b, *, Steven L. Galetta, MD b,c KEYWORDS Vision loss Double vision Papilledema Optic neuropathy Neuro-ophthalmologic
Dr Jo-Anne Pon. Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch
 Dr Jo-Anne Pon Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch 12:15-12:30 Visual Migraines to be Worried About Visual Migraines To Be Worried About Jo-Anne Pon
Dr Jo-Anne Pon Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch 12:15-12:30 Visual Migraines to be Worried About Visual Migraines To Be Worried About Jo-Anne Pon
Pearls, Pitfalls and Advances in Neuro-Ophthalmology
 Pearls, Pitfalls and Advances in Neuro-Ophthalmology Nancy J. Newman, MD Emory University Atlanta, GA Consultant for Gensight Biologics, Santhera Data Safety Monitoring Board for Quark AION Study Medical-legal
Pearls, Pitfalls and Advances in Neuro-Ophthalmology Nancy J. Newman, MD Emory University Atlanta, GA Consultant for Gensight Biologics, Santhera Data Safety Monitoring Board for Quark AION Study Medical-legal
DIAGNOSIS? CASE NUMBER ONE CONVERGENCE DIFFICIENCIES. Children vs. Adults. Insufficiency vs. Paralysis CONVERGENCE INSUFFICIENCY
 CONVERGENCE DIFFICIENCIES Children vs. Adults Insufficiency vs. Paralysis CASE NUMBER ONE DIAGNOSIS? 8 year boy referred from school- headaches, reading difficulties and blurred vision MY EXAMINATION 20/20-
CONVERGENCE DIFFICIENCIES Children vs. Adults Insufficiency vs. Paralysis CASE NUMBER ONE DIAGNOSIS? 8 year boy referred from school- headaches, reading difficulties and blurred vision MY EXAMINATION 20/20-
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA
 OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
Neuro-imaging for the Ophthalmologist. Karl C. Golnik, MD, MEd University of Cincinnati & The Cincinnati Eye Institute
 Neuro-imaging for the Ophthalmologist Karl C. Golnik, MD, MEd University of Cincinnati & The Cincinnati Eye Institute Neuro-ophthalmology is that subspecialty where the diagnosis is made upon reinterpretation
Neuro-imaging for the Ophthalmologist Karl C. Golnik, MD, MEd University of Cincinnati & The Cincinnati Eye Institute Neuro-ophthalmology is that subspecialty where the diagnosis is made upon reinterpretation
Oculomotor System George R. Leichnetz, Ph.D.
 Oculomotor System George R. Leichnetz, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be able to: 1. Define different types of eye movement and their underlying neural
Oculomotor System George R. Leichnetz, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be able to: 1. Define different types of eye movement and their underlying neural
Dr/ Marwa Abdellah EOS /16/2018. Dr/ Marwa Abdellah EOS When do you ask Fluorescein angiography for optic disc diseases???
 When do you ask Fluorescein angiography for optic disc diseases??? 1 NORMAL OPTIC DISC The normal optic disc on fluorescein angiography is fluorescent due to filling of vessels arising from the posterior
When do you ask Fluorescein angiography for optic disc diseases??? 1 NORMAL OPTIC DISC The normal optic disc on fluorescein angiography is fluorescent due to filling of vessels arising from the posterior
Pearls in PACES (Eye- General) Adel Hasanin EYE - GENERAL CLINICAL MARK SHEET
 Adel Hasanin EYE - GENERAL CLINICAL MARK SHEET") EYE - GENERAL CLINICAL MARK SHEET Examiners are required to make a judgement of the candidate's performance in each of the following sections by filling in the appropriate box then record the overall judgement
EYE - GENERAL CLINICAL MARK SHEET Examiners are required to make a judgement of the candidate's performance in each of the following sections by filling in the appropriate box then record the overall judgement
Anatomy: There are 6 muscles that move your eye.
 Thyroid Eye Disease Your doctor thinks you have thyroid orbitopathy. This is an autoimmune condition where your body's immune system is producing factors that stimulate enlargement of the muscles that
Thyroid Eye Disease Your doctor thinks you have thyroid orbitopathy. This is an autoimmune condition where your body's immune system is producing factors that stimulate enlargement of the muscles that
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7. Some PGY1
 Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
Open Access Journal of Ophthalmology
 Esotropia Anurag Narula 1 * and Shilpa Singh 2 1Safdarjung Hospital, VMMC, India 2Visitech Eye Centre, India *Corresponding author: Anurag Narula, Consultant, Safdarjung Hospital, Vardhman Short Communication
Esotropia Anurag Narula 1 * and Shilpa Singh 2 1Safdarjung Hospital, VMMC, India 2Visitech Eye Centre, India *Corresponding author: Anurag Narula, Consultant, Safdarjung Hospital, Vardhman Short Communication
I have nothing to disclose but I
 OPTIC NEUROPATHIES Robert L. Tomsak MD PhD Professor of Ophthalmology and Neurology Wayne State t University it Sh School of Mdii Medicine I have nothing to disclose but I wish I did. dd Road map for this
OPTIC NEUROPATHIES Robert L. Tomsak MD PhD Professor of Ophthalmology and Neurology Wayne State t University it Sh School of Mdii Medicine I have nothing to disclose but I wish I did. dd Road map for this
Neuro-ophthalmology. MBBS, MMed (Ophth), FRCSEd (Ophth) Registrar, Ophthalmology & Visual Sciences
, FRCSEd (Ophth) Registrar, Ophthalmology & Visual Sciences") Neuro-ophthalmology Sangtam Tiakumzuk MBBS, MMed (Ophth), FRCSEd (Ophth) Registrar, Ophthalmology & Visual Sciences Blurring of Vision: A Practical Approach to Common Case Scenarios 13 February 2016 http://www.deviatingeye.com/graphics/textbook-illustrations/visual-pathway-fromthe.html
Neuro-ophthalmology Sangtam Tiakumzuk MBBS, MMed (Ophth), FRCSEd (Ophth) Registrar, Ophthalmology & Visual Sciences Blurring of Vision: A Practical Approach to Common Case Scenarios 13 February 2016 http://www.deviatingeye.com/graphics/textbook-illustrations/visual-pathway-fromthe.html
MRI masterfile Part 5 WM Heme Strokes.ppt 1
 Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Anterior Ischemic Optic Neuropathy (AION)
") Anterior Ischemic Optic Neuropathy (AION) Your doctor thinks you have suffered an episode of anterior ischemic optic neuropathy (AION). This is the most common cause of sudden decreased vision in patients
Anterior Ischemic Optic Neuropathy (AION) Your doctor thinks you have suffered an episode of anterior ischemic optic neuropathy (AION). This is the most common cause of sudden decreased vision in patients
UC SF. g h. Eye Trauma. Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California
 UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
Identify the choice that best completes the statement or answers the question.
 Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
IMAGE OF THE MOMENT PRACTICAL NEUROLOGY
 178 PRACTICAL NEUROLOGY IMAGE OF THE MOMENT Gawn G. McIlwaine*, James H. Vallance* and Christian J. Lueck *Princess Alexandra Eye Pavilion, Chalmers Street, Edinburgh UK; The Canberra Hospital, P.O. Box
178 PRACTICAL NEUROLOGY IMAGE OF THE MOMENT Gawn G. McIlwaine*, James H. Vallance* and Christian J. Lueck *Princess Alexandra Eye Pavilion, Chalmers Street, Edinburgh UK; The Canberra Hospital, P.O. Box
Management of diplopia
 Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:166-170 REVIEW Management of diplopia Iliescu Daniela Adriana, Timaru Cristina Mihaela, Alexe Nicolae, Gosav Elena, De Simone
Romanian Journal of Ophthalmology, Volume 61, Issue 3, July-September 2017. pp:166-170 REVIEW Management of diplopia Iliescu Daniela Adriana, Timaru Cristina Mihaela, Alexe Nicolae, Gosav Elena, De Simone
Ophthalmoplegia in carotid cavernous sinus fistula
 British Journal of Ophthalmology, 1984, 68, 128-134 Ophthalmoplegia in carotid cavernous sinus fistula T. J. K. LEONARD, I. F. MOSELEY, AND M. D. SANDERS From the Departments ofneuro-ophthalmology and
British Journal of Ophthalmology, 1984, 68, 128-134 Ophthalmoplegia in carotid cavernous sinus fistula T. J. K. LEONARD, I. F. MOSELEY, AND M. D. SANDERS From the Departments ofneuro-ophthalmology and
3/16/2018. Optic nerve axons of retinal ganglion cells. 1.2 million nerve fibers. ON sheath: continuous with the meninges dura arachnoid and pia mater
 Optic nerve axons of retinal ganglion cells 1.2 million nerve fibers. ON sheath: continuous with the meninges dura arachnoid and pia mater 1 1.Visual Acuity 2.Color Vision 3.Pupil 4.Contrast sensitivity
Optic nerve axons of retinal ganglion cells 1.2 million nerve fibers. ON sheath: continuous with the meninges dura arachnoid and pia mater 1 1.Visual Acuity 2.Color Vision 3.Pupil 4.Contrast sensitivity
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuro-Ophthalmic Masqueraders
 Neuro-Ophthalmic Masqueraders Leonid Skorin, Jr., OD, DO, MS, FAAO, FAOCO Mayo Clinic Health System in Albert Lea Denise Goodwin, OD, FAAO Pacific University College of Optometry Please silence all mobile
Neuro-Ophthalmic Masqueraders Leonid Skorin, Jr., OD, DO, MS, FAAO, FAOCO Mayo Clinic Health System in Albert Lea Denise Goodwin, OD, FAAO Pacific University College of Optometry Please silence all mobile
Speaker Disclosure Statement. " Dr. Tim Maillet and Dr. Vladimir Kozousek have no conflicts of interest to disclose.
 Speaker Disclosure Statement Dr. Tim Maillet and Dr. Vladimir Kozousek have no conflicts of interest to disclose. Diabetes Morbidity Diabetes doubles the risk of stroke. Diabetes quadruples the risk of
Speaker Disclosure Statement Dr. Tim Maillet and Dr. Vladimir Kozousek have no conflicts of interest to disclose. Diabetes Morbidity Diabetes doubles the risk of stroke. Diabetes quadruples the risk of
Shared embryology Eye and brain develop from neuro-ectoderm
 The Patient with Visual Loss: Localization of Neuropathologic Disease and Select Diseases of Neuropathologic Interest Steven A. Kane, M.D., Ph.D. The Edward S. Harkness Eye Institute Shared embryology
The Patient with Visual Loss: Localization of Neuropathologic Disease and Select Diseases of Neuropathologic Interest Steven A. Kane, M.D., Ph.D. The Edward S. Harkness Eye Institute Shared embryology
American Board of Optometry Board Certification Examination DETAILED OUTLINE
 American Board of Optometry Board Certification Examination DETAILED OUTLINE General Practice (160 items) The core of the examination is based in the following ten areas of general practice. 1. Ametropia/Ophthalmic
American Board of Optometry Board Certification Examination DETAILED OUTLINE General Practice (160 items) The core of the examination is based in the following ten areas of general practice. 1. Ametropia/Ophthalmic
LISC-322 Neuroscience. Visual Field Representation. Visual Field Representation. Visual Field Representation. Visual Field Representation
 LISC-3 Neuroscience THE VISUAL SYSTEM Central Visual Pathways Each eye sees a part of the visual space that defines its visual field. The s of both eyes overlap extensively to create a binocular. eye both
LISC-3 Neuroscience THE VISUAL SYSTEM Central Visual Pathways Each eye sees a part of the visual space that defines its visual field. The s of both eyes overlap extensively to create a binocular. eye both
Band atrophy of the optic nerve: A report on different anatomical locations in three patients
 Saudi Journal of Ophthalmology (2013) 27, 65 69 Case Report Band atrophy of the optic nerve: A report on different anatomical locations in three patients Alberto Gálvez-Ruiz, MD a,b, ; Nawal Arishi, MD
Saudi Journal of Ophthalmology (2013) 27, 65 69 Case Report Band atrophy of the optic nerve: A report on different anatomical locations in three patients Alberto Gálvez-Ruiz, MD a,b, ; Nawal Arishi, MD
INTRAOCULAR INNERVATION. Oculomotor Nerve Palsy (CN 3) Signs and Symptoms. Pathophysiology. CN Palsy Update for the Primary Care OD 2018
 Signs and Symptoms. Pathophysiology. CN Palsy Update for the Primary Care OD 2018") Christopher Wolfe, OD, FAAO, Dipl. ABO Oculomotor Nerve Palsy (CN 3) Signs and Symptoms The primary symptom is diplopia caused by misalignment of the visual axes, the pattern of image separation (horizontal,
Christopher Wolfe, OD, FAAO, Dipl. ABO Oculomotor Nerve Palsy (CN 3) Signs and Symptoms The primary symptom is diplopia caused by misalignment of the visual axes, the pattern of image separation (horizontal,
Patient Symptoms- What They Might Mean. Sarah Dougherty Wood, OD, MS, FAAO Heart of America, February 2011 Paraoptometric Lecture
 Patient Symptoms- What They Might Mean Sarah Dougherty Wood, OD, MS, FAAO Heart of America, February 2011 Paraoptometric Lecture Basic ocular anatomy and physiology Movie projector analogy Blur at near/eye
Patient Symptoms- What They Might Mean Sarah Dougherty Wood, OD, MS, FAAO Heart of America, February 2011 Paraoptometric Lecture Basic ocular anatomy and physiology Movie projector analogy Blur at near/eye
CNS 2 Physiology lab
 It should be noted that the doctor emphasized that this material is also considered as continuation of the theory material and is INCLUDED IN THE THEORY EXAM. Presbiopia: is decrease in accommodation of
It should be noted that the doctor emphasized that this material is also considered as continuation of the theory material and is INCLUDED IN THE THEORY EXAM. Presbiopia: is decrease in accommodation of
Evaluation of ONH Pallor in Glaucoma Patients and Suspects. Leticia Rousso, O.D. Joseph Sowka, O.D
 Evaluation of ONH Pallor in Glaucoma Patients and Suspects Leticia Rousso, O.D Joseph Sowka, O.D I. Abstract This case report will evaluate a young glaucoma suspect with unilateral sectoral optic nerve
Evaluation of ONH Pallor in Glaucoma Patients and Suspects Leticia Rousso, O.D Joseph Sowka, O.D I. Abstract This case report will evaluate a young glaucoma suspect with unilateral sectoral optic nerve
Ocular Manifestations of Intracranial Space Occupying Lesions A Clinical Study
 248 Kerala Journal of Ophthalmology Vol. XXI, No. 3 ORIGINAL ARTICLE Ocular Manifestations of Intracranial Space Occupying Lesions A Clinical Study Dr.Sandhya somasundaran.ms, Dr. K.V.Raju.MS Abstract
248 Kerala Journal of Ophthalmology Vol. XXI, No. 3 ORIGINAL ARTICLE Ocular Manifestations of Intracranial Space Occupying Lesions A Clinical Study Dr.Sandhya somasundaran.ms, Dr. K.V.Raju.MS Abstract
Lecture 10 Orbit and control of eye movements
 Lecture 10 Orbit and control of eye movements Overview of structures in the orbit (Moore pp 899, Netter Plate 1) The orbit contains the eye, from which the optic nerve exits into the cranial cavity optic
Lecture 10 Orbit and control of eye movements Overview of structures in the orbit (Moore pp 899, Netter Plate 1) The orbit contains the eye, from which the optic nerve exits into the cranial cavity optic
Examination and Diseases of Cranial Nerves
 Cranial nerve evaluation is an important part of a neurologic exam. There are some differences in the assessment of cranial nerves with different species but the general principles are the same. Going
Cranial nerve evaluation is an important part of a neurologic exam. There are some differences in the assessment of cranial nerves with different species but the general principles are the same. Going
Incomitancy in Practice. Niall Strang. ANATOMICAL CONSIDERATIONS. Medial Rectus. Lateral Rectus : abduction Superior Rectus
 Incomitancy in Practice Niall Strang n.strang@gcu.ac.uk ANATOMICAL CONSIDERATIONS Medial Rectus There are 6 extraocular muscles 4 rectus muscles, 2 oblique muscles Length of each 40 mm, the inferior oblique
Incomitancy in Practice Niall Strang n.strang@gcu.ac.uk ANATOMICAL CONSIDERATIONS Medial Rectus There are 6 extraocular muscles 4 rectus muscles, 2 oblique muscles Length of each 40 mm, the inferior oblique
Retro-bulbar visual anatomy Optic nerves carry. Normal left ocular fundus. Retinal nerve fiber layer anatomy
 The Patient with Visual Loss: Localization of Neuropathologic Disease and Select Diseases of Neuropathologic Interest Steven A. Kane, M.D., Ph.D. The Edward S. Harkness Eye Institute Shared embryology
The Patient with Visual Loss: Localization of Neuropathologic Disease and Select Diseases of Neuropathologic Interest Steven A. Kane, M.D., Ph.D. The Edward S. Harkness Eye Institute Shared embryology