Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along?
|
|
|
- Garry Clark
- 5 years ago
- Views:
Transcription


1


2 Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along?
3 Disclosure Statement Faculty/Presenters/Authors/Content Reviewers/Planners disclose no conflict of interest relative to this educational activity.
4 Presented by : Elizabeth Seislove, MSN, RN Past President, STN Director, Trauma Program Lehigh Valley Health Network Allentown, PA Oszkar Szentirmai, MD, FACS Assistant Professor, Department of Neurosurgery, University of South Florida (USF) Chief of Neurosurgery, Lawnwood Regional Medical Center
5 Presented by : Stanley Kurek DO, FACS President, Eastern Association for the Surgery of Trauma Professor of Surgery, University of South Florida Morsani College of Medicine, USF-HCA Trauma Care Network Professor of Surgery, Florida State University College of Medicine Medical Director Trauma, Acute Care Surgery and Surgical Critical Care, Lawnwood Regional Medical Center, Ft. Pierce, FL

6 Learning Objectives To identify the various treatment options for traumatic brain injury
7 Overview: Over 1.4 million people in the US sustain traumatic brain injury (TBI) annually Approximately 250,000 hospitalized and 50,000 die Severe TBI: defined by a GCS of 8 or less is a major cause of this morbidity and mortality Significant functional, social and economic sequelae Langlois, 2007
8 Overview: 2 mechanisms of brain injury: Primary insult: Due to the trauma, irreversible Prevent the accident Secondary insult: May result from Intracranial causes (mass lesions, focal/diffuse brain swelling, ICH, vasospasm and ischemia. Extracranial causes: hypotension, hypoxia, and coagulopathy Management of patients with severe TBI focuses on the prevention and treatment of secondary brain injury
9 Treatment strategies: CPP and volume targeted management strategies Osmotherapy: Mannitol and/or Hypertonic Saline (HTS) CSF Drainage Barbituates Decompressive Craniectomy Therapeutic hypothermia Prevention of seizures Normobaric Hyperoxia
10 Traumatic Brain Injury Guidelines Developed by AANS/Joint Section on Neurotrauma & Critical Care and Brain Trauma Foundation Evidenced based guidelines - Meticulous process of scientific evidence rather than expert opinion to guide clinical practice 14 practice guideline statements Published 1995
11 Guidelines for Managing Severe TBI BTF Guidelines 1995, 2000, Update JOURNAL OF NEUROTRAUMA Volume 24, Supplement 1, 2007 Brain Trauma Foundation DOI: /neu
12 BTF 2007 Severe TBI Guidelines BP & Oxygenation Hyperosmolar Tx Prophylactic Hypothermia DVT Prophylaxis Indications for ICP Monitoring ICP Monitoring Technology ICP Thresholds CPP Thresholds Brain Oxygen Monitoring &Thresholds Anesthetics, Analgesics, & Sedatives Nutrition Anti-Seizure Hyperventilation Steroids
13
14
15
16
17
18
19
20
21
22 Audience Poll
23 Do you believe your institution follows the BTF guidelines closely Text. For yes Text for no
24 Do you have more difficulty with the Neurosurgeons or Trauma/ Critical Care surgeons being non compliant? Text. For NS Text..For Trauma Surgeons
25 Survey of TBI Management Hesdorffer D, Ghajar J, Iacono L. Predictors of compliance with the evidence-based guidelines for traumatic brain injury care: A survey of United States trauma centers. J of Trauma 2002: 52 (6): % full compliance in 433 active centers Compliance with ICP monitoring was 33% Protocols improved compliance from 7% to 26%
26 2015 Treatment Strategies
27 Treatment strategies: CPP and volume targeted management strategies Osmotherapy: Mannitol and/or Hypertonic Saline (HTS) CSF Drainage Barbituates Decompressive Craniectomy Therapeutic hypothermia Prevention of seizures Normobaric Hyperoxia
28 CPP and volume targeted management strategies Monro-Kellie doctorine In 1783 Alexander Monro deduced that the cranium was a "rigid box" filled with a "nearly incompressible brain" and that its total volume tends to remain constant. The doctrine states that any increase in the volume of the cranial contents (e.g. brain, blood or cerebrospinal fluid), will elevate intracranial pressure. Further, if one of these three elements increase in volume, it must occur at the expense of volume of the other two elements. In 1824 George Kellie confirmed many of Monro's early observations
29 Pathophysiology: Intracranial Pressure Theories on Brain Compartment 80% brain 10% blood 10% CSF If one increases the other two decrease Compensatory mechanisms 80% Brain moves over 1 0 % SDH Venous blood to heart 1 0 % CSF shunts to spine SAS
30 Cerebral Blood Flow CBF = CPP CVR CPP = MAP - ICP Injured Brain optimize CPP Normal CPP does not ensure CBF is adequate to meet the needs of the injured brain
31 In the presence of intact cerebral autoregulation CBF remains relatively constant within a wide range of perfusion pressures This occurs by vasoconstrictive responses to increased CPP and vasodilatory responses to decreased CPP When CPP is outside the breakpoints of pressure auto-regulation (50 and 150 mmhg) CBF becomes directly dependent on CPP
32 Currently there is controversy concerning the optimal CPP thresholds after TBI 2 groups of thought on the best approach for optimizing cerebrovascular dynamics CPP-targeted group Volume targeted group
33 CPP targeted approach Based on vasodilatory cascade Decreased CPP stimulates vasodilation, increases CBF and ICP Supported by BTF Some studies show a benefit while others cannot demonstrate any difference in outcome
34 Volume-targeted therapy Based on Starling forces of capillary flow Aim is to reduce intracranial volume and to improve the microcirculation by preserving colloid osmotic pressure using albumin and prbc s, reducing capillary hydrostatic pressure using metoprolol and clonidine, and reducing cerebral blood flow using thiopental Several centers in Europe Mixed results
35 Osmotherapy: Mannitol or Hypertonic Saline
36 Background The ICP reducing effects of Mannitol: Osmotic diuretic Reduces blood viscosity by decreasing HCT and by decreasing the volume, rigidity and cohesiveness of red blood cells Reduced Cerebrovascular resistance and Increaed CBF, causing auto-regulatory decrease CBF and ICP May cause Hypotension in under resuscitated patients
37 Background Hypertonic Saline (HTS) mechanism similar to Mannitol Unlike Mannitol though HTS less likely to cross BBB and therefore less likely to cause rebound cerebral edema.
38 Mannitol versus HTS Vialet, et al, Crit Care Med 2003: Small randomized trial involving 20 pts Isovolume infusions of 7.5% HTS or 20% Mannitol Mannitol group had more episodes of elevated ICP and the daily total time was longer Treatment failure higher in Mannitol Group Outcomes not measured
39 Mannitol versus HTS Class 1 studies are lacking but Class 2 an 3 studies show both may be effective
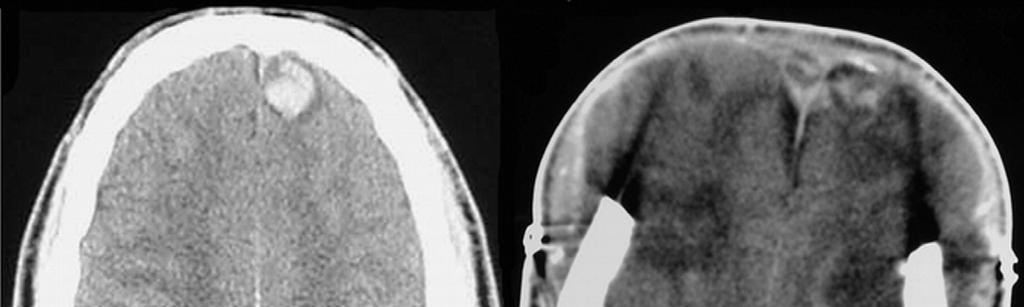
40 Case #1 26 YO male MCC high rate of speed Positive for cocaine and alcohol, father was following in his car and witnessed event GCS 3T at scene-intubated by EMS GCS 6-7T trauma bay

41 Case #1 CT head: Diffuse b/l SAH DAI small SDH B/L frontoparietal hemorrhage Intraventricular hemorrhage
42 Case # 1 Management: Ventriculostomy not inserted Would you start treatment with Hypertonic Saline Text >>>> yes Text >>>>No
43 Case # 1 3% NS started-na 145 NA to mid for several days 3% NS tapered down d/c d

44 Repeat Head CT PTD #1 Significant worsening of SAH, DAI, frontoparietal bleeding Hypertonic Saline continued

45 Repeat Head CT PTD#2 Increased cerebral edema effacement of cistern, beginning herniation Na 155 Hypertonic Saline off ICP s 20, CPP s 60 s

46 Repeat Head CT PTD#3 Sinus bradycardia 30-50/min-atropine GCS 4 T Family discussion X2 No DNR Following morning patient coded
47 Opportunities Early ventriculostomy placement HTS versus Mannitol
48 CSF Drainage
49 CSF Drainage Current BTF guidelines recommend that ICP should be monitored in all comatose patients with GCS </=8 with either an abnormal CT or 2 or more of the following: >40 years old, posturing and SBP <90 Intraventricular catheter connected to an extracranial ventricular drain and a pressure transducer is most accurate With the ability drain CSF why use anything else?
50 Poll In your institution what is the most commonly inserted monitoring device Text. ICP bolt Text.Ventriculostomy Text Neither
51 Barbiturates
52 Barbituates Known as early as the 1930 s that high does barbituates are effective in reducing ICP Shapiro, Br J Anesaesth, 1985 Cause a dose dependent reversible depression of neuronal activity with reduction of the cerebral metabolic rate, CBF and ICP Kassel, NE, Neurosurgery 1980
53 Barbituates Complications include: Hypotension from myocardial depression and decreased SVR Increased infections, usually pulmonary Schwartz, et al 1984 Can J Neurol Sci: Compared Barb s with mannitol as initial treatment in 59 pts. Randomized. Mannitol more effective in lowering ICP s No difference in mortality but patients with DAI had worse outcomes with Barb s
54 Barbituates Are effective when used to control refractory intracranial hypertension but still few evidence exists of an outcome benefit.
55 Decompressive Craniectomy
56 Decompressive Craniectomy Numerous publications over the last 20 years with variable results. Difficulty with making conclusions: Different operative techniques, b/l, one sided, size of flap, etc. Outcome variables different Variability of injuries Variability of presenting GCS Timing of procedure
57 Case #2 55 year old (+) ETOH abuser fell down 12 steps (+) LOC Reported falling about an hour or so before pre-hospital arrival GCS = 9 Collared/boarded and loaded into the ambulance
58 Arrival at Level I Trauma Center 132/70, 102, 18, 84%, T = 95.5, GCS = 10 Sent to CT Scan within 20 minutes of arrival ETOH level = 338 Pupils unequal Agitated GCS = 11 Consulted Neurosurgery

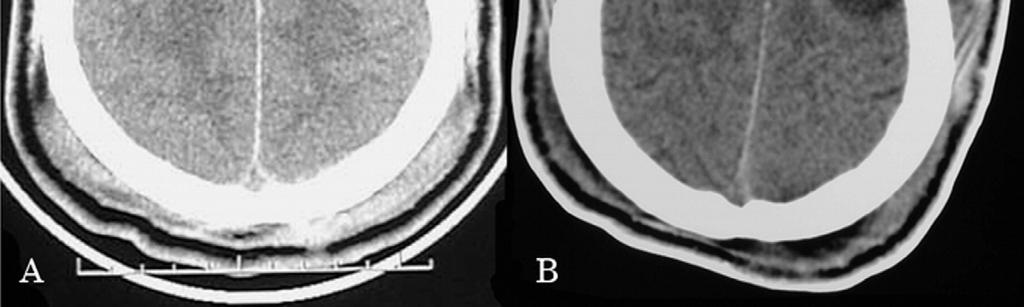
59 CT Results Acute subdural hemorrhage along the right cerebral convexity Subdural hemorrhage along the right tentorium. Associated mass effect an approximately 4 mm leftward midline shift. Patchy parenchymal contusions in the inferior left temporal and frontal lobes. Fractures of the right temporal bone involving the squamous and mastoid portions.
60 What is your immediate next step? 1. Intubate? 2. Go directly to the OR for craniectomy or craniotomy? 3. Start 3% Saline? 4. Give Mannitol? 5. Start Keppra? 6. Observe? 7. All of the above 8. None of the above

61 Observation with a CT in 4 hours 4 hour later CT scan Chose to continue to watch GCS = 14 Admitted to the ICU Started to become very agitated

62 Morning CT of the Head Slight increase in the bleed along the right convexity and a new subfalcine herniation on the left
63 Now what do you want to do? Intubate? Go directly to the OR for craniectomy? Start 3% Saline? Give Mannitol? Start Keppra? All of the above None of the above

64 We went to the OR for a Craniotomy
65 Post-op Course POD#1 Extubated CIWA score demonstrating potential ETOH withdrawal. Score 16 POD#2 Valium given along with Haldol for extreme agitation Obtunded 3% Saline started Re-intubated Agitated, CIWA s in the high teens
 Propofol gtt.")
66 POD #3 Ventriculostomy placed: ICP s = 39 (ordered at 10 and remain open) Propofol gtt. started 3% Maintained

67 Post Craniectomy POD #4 Returned to the OR for craniectomy Keppra started Temps = 103 s GCS = 4T

68 POD #8 Palliative Care consult POD #10 Patient made comfort care Expired
69 Let s Discuss our opportunities and Neurosurgeon Colleague Input Nursing Input Trauma Surgeon Input
70 Hypothermia for TBI and SCI
71 Hypothermia for neuroprotection National Acute Brain Injury Study: Hypothermia Large muti-center randomized controlled trial 48 hrs of moderate hypothermia (33 o C) reached within 8 hrs of injury Terminated after enrollment of 392 of a planned 500 patients Results: No difference in outcome at 6 months
72 Hypothermia for ICP control Multiple studies demonstrate that mild hypothermia (34 o C) reduces ICP in severe TBI but in contrast many also showed no difference in outcome and increased complication rates. Several recent studies have shown that maintaining normothermia may be beneficial
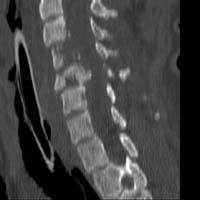
73 Case SCI 24 yo male jumps from boat into water Immediately no sensation from neck down Immobilized and transported
74 Case SCI When Paramedics arrived at shoreline, iced bags of NS were placed around the patients neck and he was given 2 L ice cold NS en route to the trauma center. Do you think these measures will help or hurt the patient? Text >>> Definitely wil help patient Text.. May help patient Text.. May hurt patient
75 Case SCI Upon arrival to the trauma center the patients undergoes resuscitation, started on Neosynephrine for spinal shock and undergoes CT of head and C-spine
76 SCI




77
78 Operative Treatment Reduction and Stabilization while cold Rewarming: Automatic 0.5*C per hour 37*

79 SCI
80 Neurotherapeutics Apr; 8(2): Hypothermic Treatment for Acute Spinal Cord Injury W. Dalton Dietrich, 1,2 Allan D. Levi, 1,2 Michael Wang, 1,2 and Barth A. Green 1,2
81 Selection of patients Age years ASIA Injury Score A Non penetrating injury Lower temperature to 33*c Maintained for 48 hours Patients taken to the OR for surgical reduction may be included Slow re-warming
82 Selection of Patients - Contraindications Age >65 years ASIA score B C D Hyperthermia on admission (>38.5) Severe systemic injury Severe bleeding Pregnancy Coagulopathy Thrombocytopenia Known cardiac history Blood dyscrasia Pancreatitis Reynauds syndrome Spinal cord transaction Patients intubated and sedated prior to initial exam by the trauma surgeon and neurosurgeon
83 Initial Study Showed N=14 6 improved 3 from A to B 2 from A to C 1 from A to D 42.8% improvement Control group without hypothermia showed 12.5% improvement
84 Complications Respiratory, predominantly atelectasis No problems with Coagulopathy, DVT PE Prevents hyperthermic damage to cells!
85 Prevention of Seizures
86 Evidence Level 1: Phenytoin is effective in decreasing the risk of early PTS prophylaxis Valproate should not be used for prophylaxis Phenytoin, carbamazepine, and valproate are ineffective in decreasing the risk of late PTS Insufficient data to recommend routine PTS prophylaxis in patients with mild or moderate TBI Cheatham, 2012
87 Evidence Level 2: Levetiracetam is an effective and safe alternative to phenytoin for early PTS prophylaxis Routine prophylaxis of late PTS is not recommended Level 3: Levetiracetam should not replace phenytoin as a first line agent for PTS prophylaxis Higher seizure potential Cheatham, 2012
88 Normobaric Hyperoxia
89 Results of Changing Practice: TBI Guidelines/Oxygen Monitoring Pre PbtO2 23 Patients GOS % GOS 1 41% Post PbtO2 24 Patients GOS % GOS 1 25% Management and therapy aimed at preventing cerebral hypoxia and maintaining brain tissue oxygen is successful in reducing mortality in traumatic brain injury. Steifel et al (Le Roux), U of Pennsylvania experience (J of Neurosurgery 2005)


90
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY. Dr Nick Taylor MBBS FACEM
 PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Severe Traumatic Brain Injury Protocol
 Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
ICP. A Stepwise Protocol
 ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Conflict of Interest Disclosure J. Claude Hemphill III, MD,MAS. Difficult Diagnosis and Treatment: New Onset Obtundation
 Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Measuring severity of TBI. Traumatic Brain injury: TBI. Glasgow Coma Scale & score. Glasgow coma scale/score. Glasgow coma scale with score (GCS)
") Measuring severity of TBI Glasgow coma scale with score (GCS) ก กก functional outcome Post traumatic Amnesia (PTA) cognitive & functional deficit Assist. Prof.Savai Norasan First National Neuroscience
Measuring severity of TBI Glasgow coma scale with score (GCS) ก กก functional outcome Post traumatic Amnesia (PTA) cognitive & functional deficit Assist. Prof.Savai Norasan First National Neuroscience
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
12/1/2017. Disclosure. When I was invited to give a talk in Tokyo 2011 at the 4 th International. Hypothermia Symposium
 Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
UAMS MEDICAL CENTER TRAUMA and CRITICAL CARE SERVICES MANUAL. SUPERSEDES: New PAGE: 1 of 5. RECOMMENDATION(S): Drs. Bill Beck/J.R.
: Drs. Bill Beck/J.R.") SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Blood Brain Barrier (BBB)
") Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Traumatic Brain Injury
 General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Guidelines and Beyond: Traumatic Brain Injury
 Guidelines and Beyond: Traumatic Brain Injury Aimee Gowler, PharmD, BCCCP, BCPS Neuromedicine Critical Care Clinical Pharmacy Specialist UF Health Shands Disclosures I have no financial interests to disclose.
Guidelines and Beyond: Traumatic Brain Injury Aimee Gowler, PharmD, BCCCP, BCPS Neuromedicine Critical Care Clinical Pharmacy Specialist UF Health Shands Disclosures I have no financial interests to disclose.
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Therapeutic Hypothermia
 Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Neurotrauma: The Place for Cooling
 Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Management of head injury in the intensive-care unit
 Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Pediatric Trauma Initial Evaluation and management
 Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
INDUCED HYPOTHERMIA. F. Ben Housel, M.D.
 INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Positron Emission Tomography Imaging in Brain Injured Patients
 Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Head Trauma Protocol
 Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury
 Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED
 ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury
 Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Objectives. Trends in Resuscitation POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE?
 POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Management of Traumatic Brain Injury. Olaide O. Ajayi, MD
 Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Paediatric Neurosurgical Emergencies. Kate Parkins Consultant Paediatric Intensivist Alder Hey
 Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Early Treatment of TBI A Prospective Study from Austria
 Early Treatment of TBI A Prospective Study from Austria Walter Mauritz MD, PhD Dept. of Anaesthesiology & Critical Care Trauma Hospital XX, 1200 Vienna, Austria International Neurotrauma Research Organisation,
Early Treatment of TBI A Prospective Study from Austria Walter Mauritz MD, PhD Dept. of Anaesthesiology & Critical Care Trauma Hospital XX, 1200 Vienna, Austria International Neurotrauma Research Organisation,
PROTECT - ION 11/26/2014. Traumatic Brain Injury. Pathophysiology and Management. Disclosures. Neuro PROTECTion in Severe Traumatic Brain Injury
 Disclosures Neuro PROTECTion in Severe Traumatic Brain Injury Presented by: Mary Kay Bader RN, MSN CCNS, CNRN, CCRN, SCRN, FAHA, FNCS Neuro/Critical Care CNS Mission Hospital Badermk@aol.com Bader Honorarium
Disclosures Neuro PROTECTion in Severe Traumatic Brain Injury Presented by: Mary Kay Bader RN, MSN CCNS, CNRN, CCRN, SCRN, FAHA, FNCS Neuro/Critical Care CNS Mission Hospital Badermk@aol.com Bader Honorarium
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Medicines Protocol HYPERTONIC SALINE 5%
 Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Therapeutic Hypothermia ANZCA 2013
 Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Patient Case. Post cardiac arrest pathophysiology 10/19/2017. Disclosure. Objectives. Patient Case-TM
 Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
9/16/2018. Recognizing & Managing Seizures in Pediatric TBI. Objectives. Definitions and Epidemiology
 Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Severe Head dinjury Management and Recent Advances
 Severe Head dinjury ent and Recent Advances Presenter Dr Shejoy P Joshua Moderator Dr AK Mahapatra Dr Deepak Kumar Gupta 1 KEY Epidemiology Resuscitation Primary survey Secondary survey Neurological evaluation
Severe Head dinjury ent and Recent Advances Presenter Dr Shejoy P Joshua Moderator Dr AK Mahapatra Dr Deepak Kumar Gupta 1 KEY Epidemiology Resuscitation Primary survey Secondary survey Neurological evaluation