ΓΙΩΡΓΟΣ ΜΑΚΑΒΟΣ, MD, PhD ΚΑΡΔΙΟΛΟΓΟΣ, ΕΠΙΜΕΛΗΤΗΣ Β Γ ΠΑΝΕΠΙΣΤΗΜΙΑΚΗ ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ Γ.Ν.Ν.Θ.Α. ΣΩΤΗΡΙΑ
|
|
|
- Angel Green
- 5 years ago
- Views:
Transcription


1 ΓΙΩΡΓΟΣ ΜΑΚΑΒΟΣ, MD, PhD ΚΑΡΔΙΟΛΟΓΟΣ, ΕΠΙΜΕΛΗΤΗΣ Β Γ ΠΑΝΕΠΙΣΤΗΜΙΑΚΗ ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ Γ.Ν.Ν.Θ.Α. ΣΩΤΗΡΙΑ
2
3 Causes of TR Primary-Organic Secondary-Functional Rheumatic LV,valvular dysfunction I.Endocarditis Pulmonary hypertemdion Ebstein RV dysfunction Prolapse Carcinoid Congenital Papillary muscle dysfunction Connective tissue disease Τrauma Radiation Pacemaker/ICD
4
5

6
7
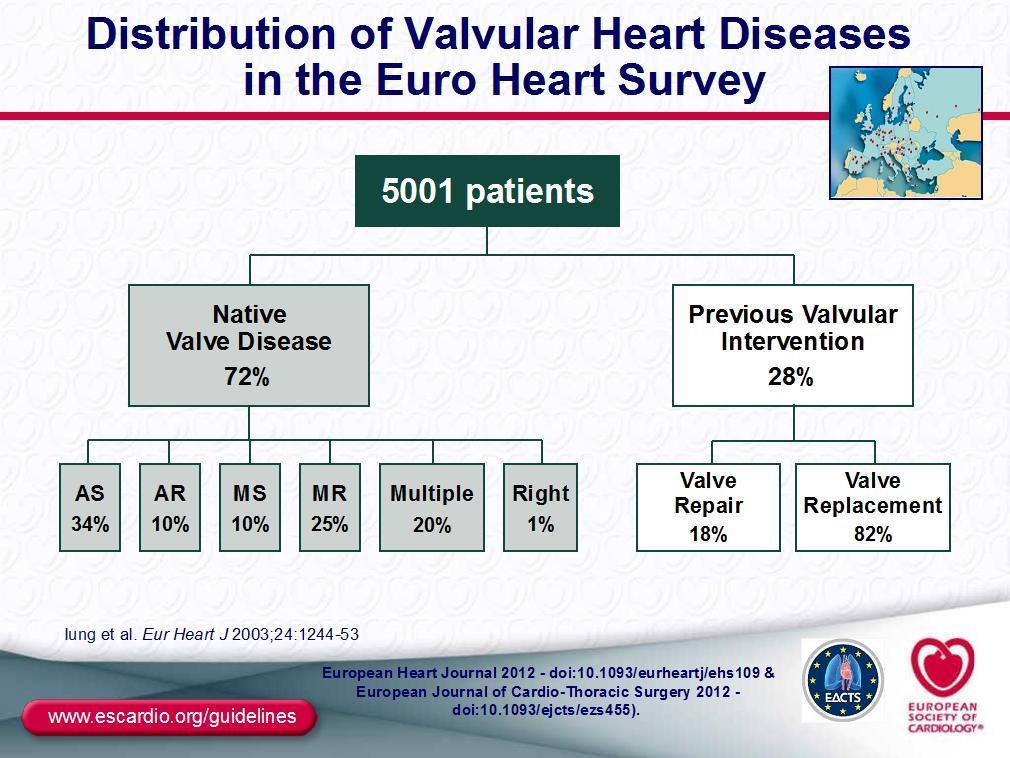
8 Tricuspid Valve Dysfunction Following Pacemaker or Cardioverter-Defibrillator Implantation In the USA, approximately 200,000 (600,000 worldwide) permanent pacemakers (PPMs) and 120,000 ICDs are implanted annually. The potential for cardiac implantable electronic device leads to interfere with TV function has gained increasing recognition as having hemodynamic and clinical consequences associated with incremental morbidity and death. The diagnosis and treatment of lead-related (as distinct from functional) tricuspid regurgitation pose unique challenges. A high level of clinical suspicion must be maintained to avoid overlooking the possibility that worsening heart failure is a consequence of mechanical interference with TV leaflet mobility or coaptation, as ICD recipients have, at baseline, LV systolic dysfunction and are thereby predisposed, independent of any effect of the device, to secondary or functional TR and right heart failure. Chang et al, J Am Coll Cardiol 2017;69:
9 Impact of Tricuspid Regurgitation on Long- Term Survival Increasing TR severity is associated with worse survival in regardless of LVEF or pulmonary artery pressure. Severe TR is associated with a poor prognosis, independent of age, biventricular systolic function, RV size, and dilation of the inferior vena cava. Nath et al. J Am Coll Cardiol 2004;43:405 9
10 TR and Mortality in Patients With Transvenous Pacemakers Among patients with a PPM lead, the presence of Severe TR was associated with increased mortality (adjusted hazard ratio 1.40) PPM leads are associated with higher risk of STR after adjustment for LV systolic/ diastolic function and PH; similarly to STR from other cardiac pathologies, PPM-related STR is associated with increased mortality. Delling et al. Am J Cardiol 2016;117:
 Or as left-sided heart failure when RV volume overload impairs LV filling by")
11 TR PATHOPHYSIOLOGY Tricuspid regurgitation RA pressure CVP RV volume overload Renal dyfunction Symptoms and signs of RV failure RV dysfunction Cardiac output TV dysfunction following CIED implantation can manifest clinically as rightsided heart failure secondary to TR (or less often to tricuspid stenosis) Or as left-sided heart failure when RV volume overload impairs LV filling by direct ventricular interaction through the interventricular septum
 Mechanical interference with normal leaflet mobility and coaptation (impingement) leaflet entrapment, subvalvular support structure entanglement, Endocarditis.")
12 MECHANISMS OF LEAD-RELATED TV DYSFUNCTION Structural consequences include: Valve leaflets, papillary muscles or chordae tendineae damage during lead placement or manipulation (perforation. laceration, avulsion) Mechanical interference with normal leaflet mobility and coaptation (impingement) leaflet entrapment, subvalvular support structure entanglement, Endocarditis. Damage to the TV can occur during extraction of infected or malfunctioning leads. Long-term interaction between endocardial leads and leaflet or chordal structures can result in inflammatory and fibrotic response, resulting in the encapsulation, ensheathment, or entrapment of the lead with subsequent loss of leaflet mobility or coaptation
, chordae tendineae, 2-3 papillary muscles (anterior and")

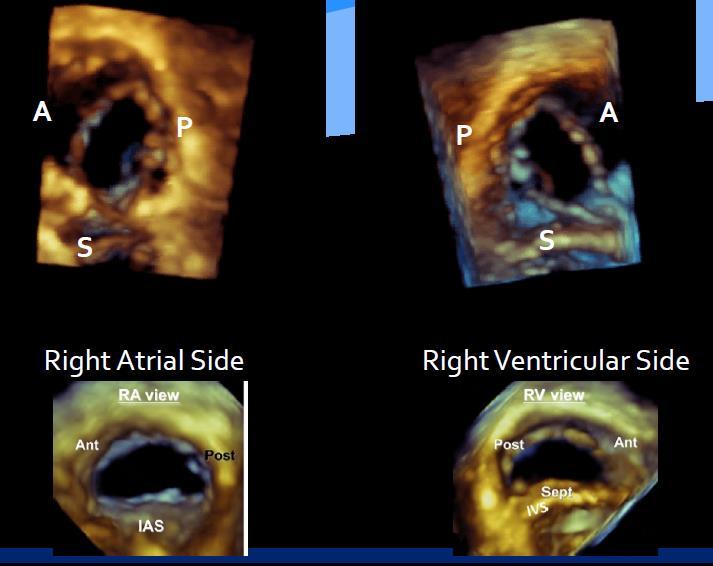
13 TV ANATOMY The tricuspid apparatus comprises a nonplanar elliptical annulus, 3 leaflets (anterior,posterior, and septal), chordae tendineae, 2-3 papillary muscles (anterior and posterior) carrying chordae to a single leaflet. Some of the TV chordae tendineae attach directly to the interventricular septum, RV free wall, or moderator band in the absence of an intervening papillary muscle


14 TRICUSPID VALVE ANATOMY AND PHYSIOLOGY The septal portion of the annulus subtends the right fibrous trigone and is supported by the cardiac skeleton the mural portion of the annulus subtends the RV free wall and is prone to elongate under a state of chronic pressure or volume overload, leading to annular dilation TR begetstr chronic volume overload, chamber and annular dilation, leaflet tethering, and loss of coaptation, which worsen the TR and create a vicious cycle. Particularly when left-sided cardiac dysfunction predisposing the patient to functional or secondary TR coexists, even a modest increment in TR associated with the presence of a CIED lead can, over time, result in severe TR and right-sided heart failure.

15 Tricuspid annular dialatation,papillary muscle tethering-pathophysiology Reverse remodelling of the RV may not occur. The flattening of the TV annulus may stretch papillary muscles When septum is hypokinetic, dyskinetic, or dilated, there can be a tethering effect on the TV through papillary muscles of the septal leaflet
16 Prevalence of PM-associated TR Estimates of the prevalence of significant TR (defined as 2/4) and incidence of TR worsening (by 1 or more grades) following CIED implantation vary from 10% to 39%, with most (but not all) studies attributing a higher incidence of worsening TR to ICD leads (implicating their greater thickness and stiffness) and with the presence of more than 1 RV leads Some 21.2% of patients with baseline mild TR or less developed abnormal TR (3.4% mild-moderate, 12.8% moderate, 1.1% moderate-severe, 3.9% severe) after implant. TR worsened by 1 grade or more after implant in 24.2% TR worsening was more common with ICDs than PPMs in patients with baseline mild TR or less. (32.4% vs. 20.1%; P <.05). Kim et al.j Am Soc Echocardiogr 2008;21: Chang et al, J Am Coll Cardiol 2017;69:
17 Prevalence of TR PM-associated Lin et al. J Am Coll Cardiol 2005;45: In a series of 41 patients undergoing TV surgery for severe TR believed to be caused by a CIED lead, leaflet perforation in 7 patients, leaflet entanglement in 4, leaflet impingement in 16, leaflet adherence in 14. The septal leaflet was most often (6 of 7 patients) perforated Postmortem analyses have also shown that TV lacerations are more common on the posterior leaflet
18 Lead related and TV endocarditis PM/ICD infection almost always necessitates lead extraction. Morbidity and mortality rates related to CIED infection increase significantly when the TV is involved compared with when evidence of TV endocarditis is absent. Patients undergoing removal of an infected device during hospitalization are one-half as likely to die (19.9%) at 1 year as patients who do not undergo device removal (38.2%) TV dysfunction in the setting of lead-related endocarditis can occur as a result of leaflet destruction by the infectious process itself or during lead extraction Predictors of TR worsening after TLE include removal of more than 1 lead, advanced age, and endocarditis involving the TV as the indication for device explantation Athan et al. JAMA 2012;307: Coffey et al. Pacing Clin Electrophysiol 2014;37:19 24.

19 Pacemaker extraction Post endocarditis pre post


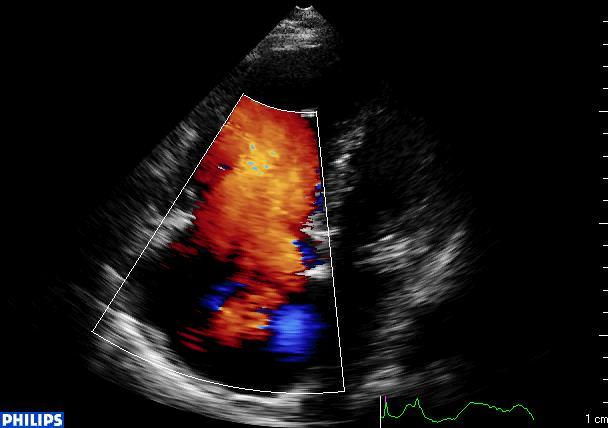
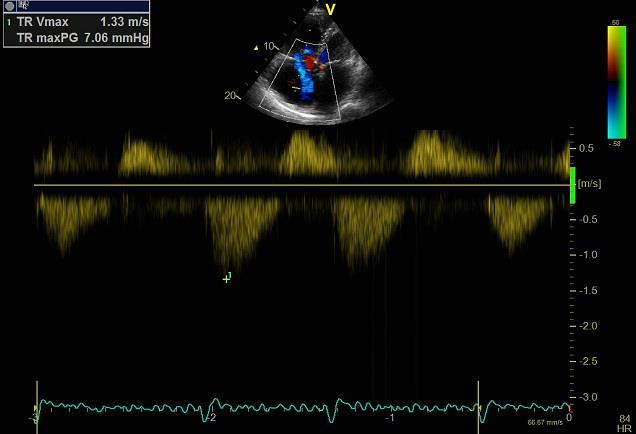
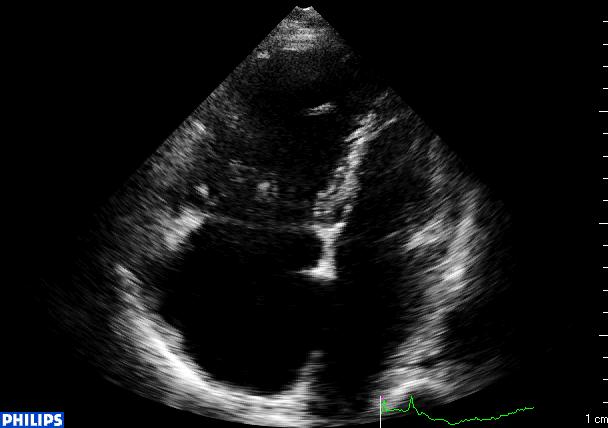
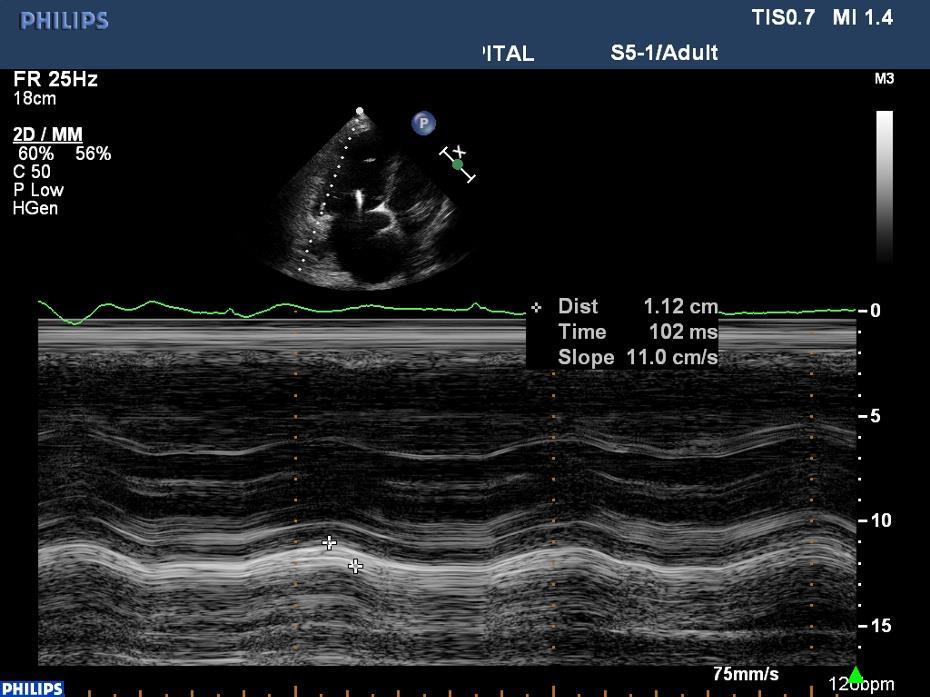
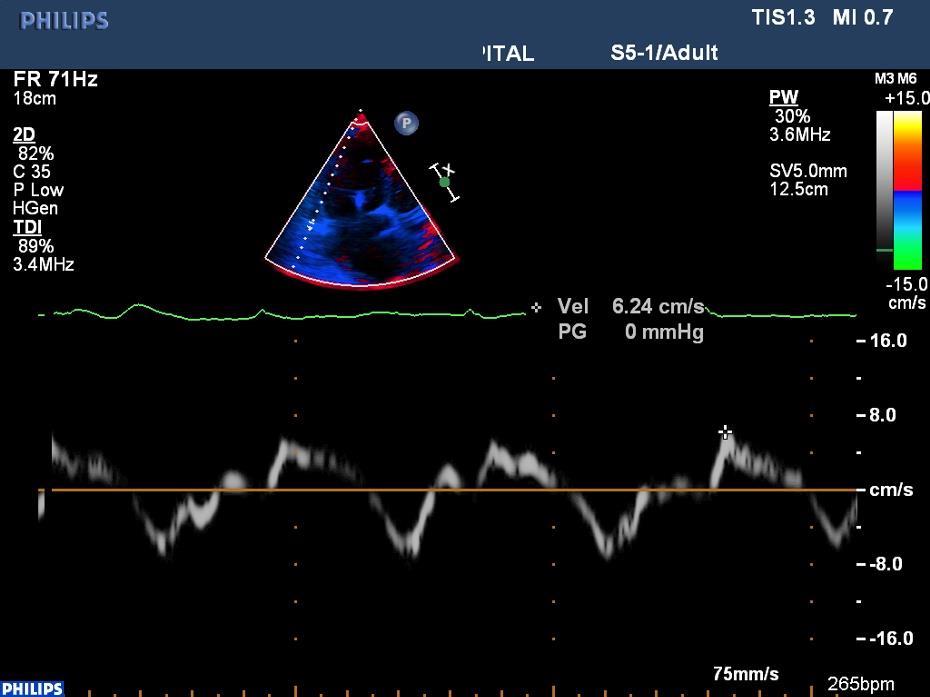
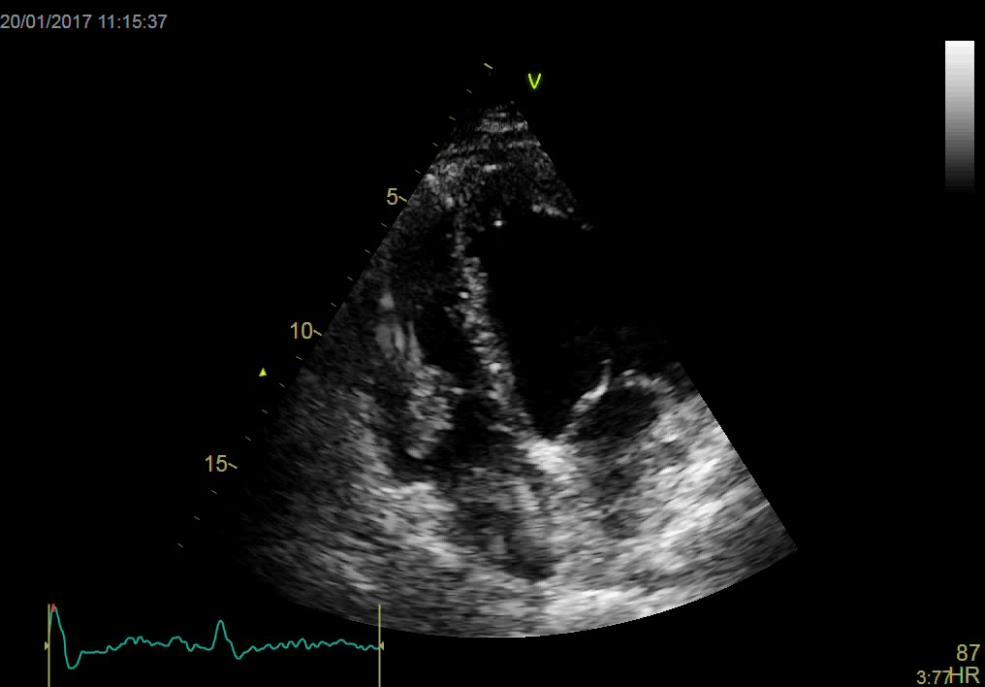
20 DIAGNOSIS OF TV DYSFUNCTION ASSOCIATED WITH PM/ICD LEADS 2D, 3D, and Doppler echocardiographic examinations are the mainstays for the diagnosis of TV dysfunction associated with CIED leads. The echocardiographic diagnosis of TR in patients with CIEDs is similar to that in patients without endocardial leads. ESC guidelines VHD 2017
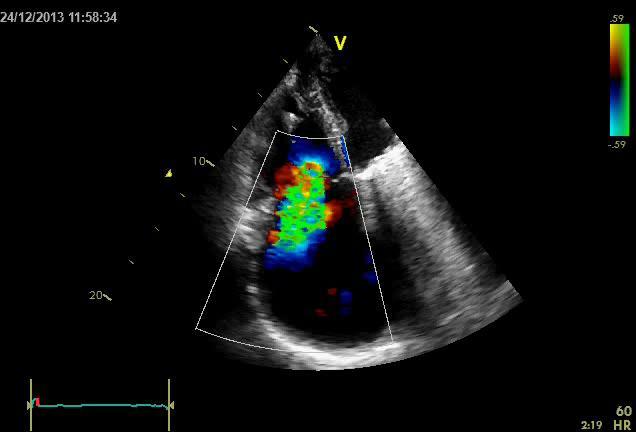

21 PISA

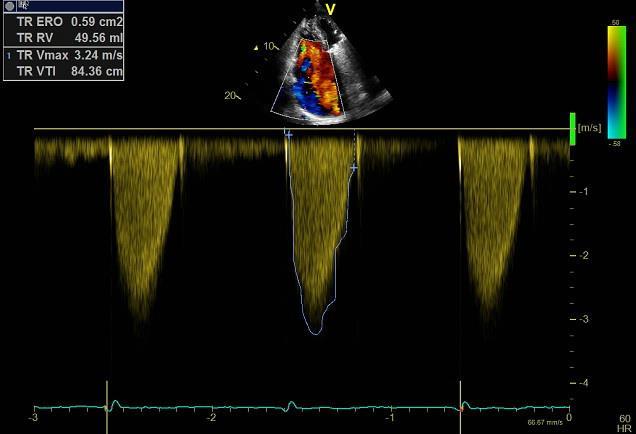
22 Vena contracta
23 DIAGNOSIS OF TV DYSFUNCTION ASSOCIATED WITH CIED LEADS PM/ICD leads cause echocardiographic imaging artifacts and signal attenuation because of their high acoustic reflectivity, with underestimation of TR by Doppler color When TR is caused by an asymmetrical alteration in leaflet mobility, the regurgitant jet tends to assume an eccentric (wall-hugging), rather than a central, trajectory, resulting in loss of Doppler color flow signal (Coanda effect) and hence underestimation of regurgitation. In patients eventually found to have severe TR resulting from CIED leads, only 63% had a correct diagnosis by TTE during the preoperative study


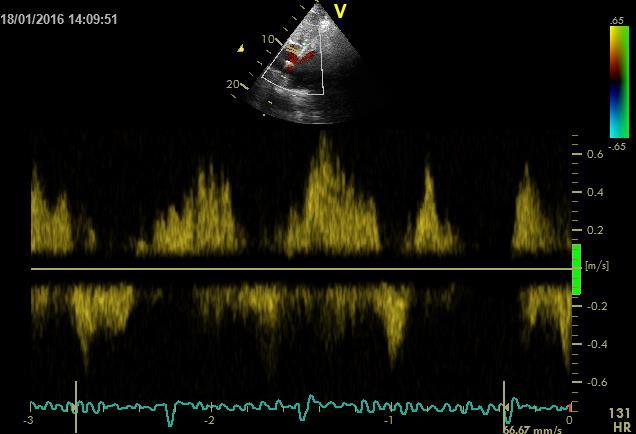
24 DIAGNOSIS OF TV DYSFUNCTION ASSOCIATED WITH CIED LEADS Pattern of hepatic vein flow not affected by leadinduced acoustic artifacts. Holosystolic hepatic vein flow reversal is diagnostic of severe TR, although if the right atrium is severely dilated, the negative predictive value of hepatic vein systolic flow reversal may be reduced.

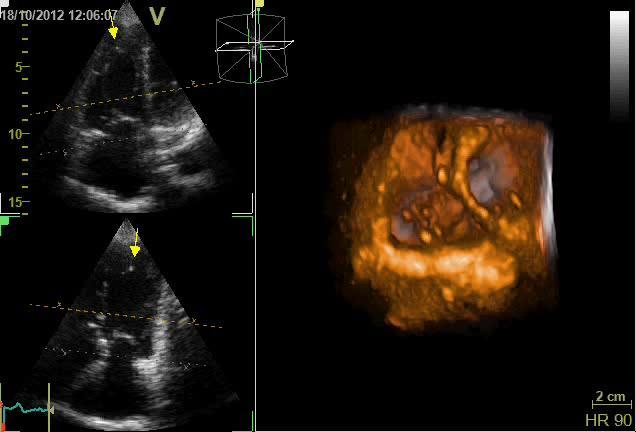
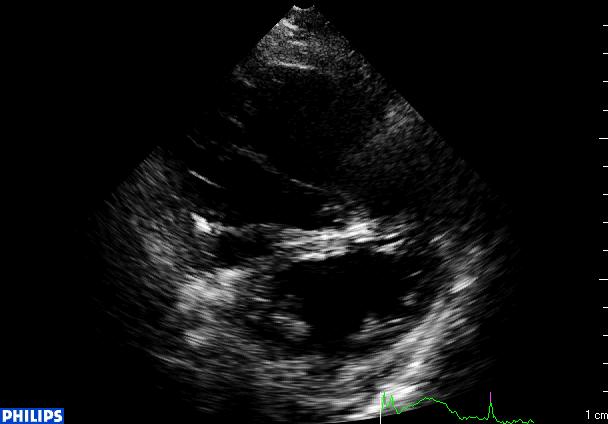
25 3D ECHO TV
26 Cheng et al. Echocardiography.2016;33: Seo et al. Circ J 2008;72: DIAGNOSIS OF TV DYSFUNCTION ASSOCIATED WITH CIED LEADS Sensitivity of 2D TTE for identification of a CIED lead as the primary cause of TV dysfunction is low (12% to 17%) 3D echocardiography offers improved spatial definition of the interaction between lead and valve or subvalvular apparatus 3D TTE was able to delineate the course and position of leads in 153 of 207 (74%) patients, with a clear association between lead impingement and worsening TR after lead placement In a comparison of 2D and 3D TTE for the diagnosis of lead-related TR in 87 patients with CIEDs, it was found that 2D TTE satisfactorily delineated the spatial relationship between lead and valve in only 17.2% of patients, whereas 3D TTE did so in 94.2%


27 3D Echo Location of Implantable Device Leads and Mechanism of Associated TR 3D TTE clearly depicted lead position in 90% of patients. Leads interfering with normal leaflet mobility were associated with more TR than nonimpinging leads (vena contracta: median 0.62 cm [1st and 3rd quartiles: 0.51, 0.84 cm] vs cm [1st and 3rd quartiles: 0.00, 0.48 cm]; p < 0.001). MedirattaJ Am Coll Cardiol Img 2014;7:337 47



28 3D Echocardiographic Location of Implantable Device Leads and Mechanism of Associated TR An intercommissural or middle-of-the-annulus position is desired to minimize device-related TR post implantation 3D TTE showed a clear association between device lead position and TR. To minimize TR induced by device-leads, 3D TTE guidance should be considered for placement in a commissural position. MedirattaJ Am Coll Cardiol Img 2014;7:337 47

29 Impinging septal leaflet causing TR Non impinging
30 Impinging posterior leaflet

31 TREATMENT OF TV DYSFUNCTION ASSOCIATED WITH PM LEADS Valve repair: Suture (DeVega) annuloplasty, Ring annuloplasty Damage to the leaflets: suture or patch repair. The lead can be repositioned to prevent leaflet impingement by securing it in a location abutting the tricuspid annulus in a cleft created by suture bicuspidization of the valve. Valve replacement with or without lead retention. Lead extraction without valve repair or replacement, adequate to ameliorate lead related TR usually cannot be determined and depends on severity of RV and tricuspid annular dilation, the degree of leaflet tethering, and the extent of leaflet damage or distortion. If the lead is relatively new, with minimal leaflet damage or distortion, a surgical procedure may be avoided. Because further damage may ensue, a valve replacement or repair strategy must be in place before TLE. Nazmul et al. Europace 2013;15: Chang et al. J Am Coll Cardiol 2017;69:
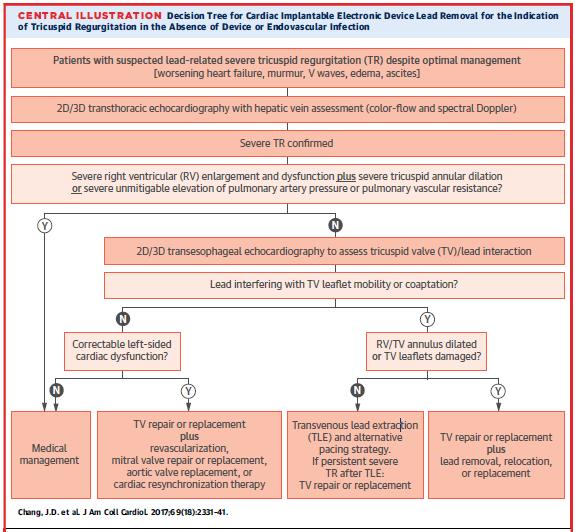
32 INDICATIONS FOR REMOVAL OF LEADS TO TREAT TR TV repair or replacement for lead-related: no prospective data to support TR in the absence of device or endovascular infection as an indication for TLE Risk-benefit ratio incremental morbidity and mortality independently attributable to severe TR against those associated with lead removal with or without TV repair or replacement. The excess mortality rates associated with severe TR have been estimated to be 31% in the general population and 40% to 75% in patients with PM/ICDs.when operative risk is low, patients with leadrelated severe TR would be expected to benefit from corrective intervention. Patients with symptomatic severe TR and with compelling 3D echocardiographic evidence that valve function has been compromised primarily by the lead Likelihood of successful treatment by lead extraction and valve repair or replacement decreases with increasing duration of TR when the tricuspid annulus and RV are dilated that leaflet coaptation would not be possible even in the absence of the lead. Strategies to pace the heart without crossing the TV, and thus not interfering with its closing mechanism, include placement of a coronary sinus pacing lead, surgical epicardial placement of leads, and leadless pacing systems. Chang et al. J Am Coll Cardiol 2017;69:
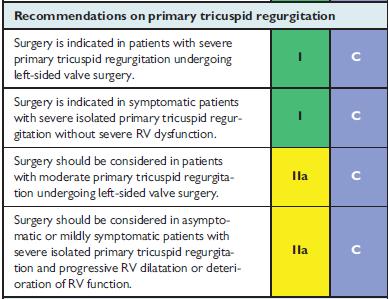
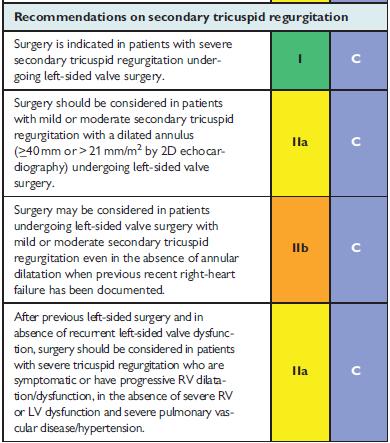
33 ESC guidelines VHD 2017
34

35 CONCLUSIONS Although the putative contribution of PM/ICD leads to TV dysfunction has gained increasing recognition as having hemodynamic and clinical consequences associated with incremental morbidity and death, all evidence are from retrospective analyses. A higher level of clinical suspicion with 3D echocardiography, may alert the clinician to the possibility that worsening heart failure is consequence of mechanical interference with TV leaflet mobility or coaptation and is amenable to lead extraction or valve repair or replacement. When clinical, hemodynamic, and echo assessment provides compelling evidence of lead related severe TR, corrective intervention should be provided in a timely fashion, before the onset of severe annular and chamber dilation and severe RV dysfunction The future in which endocardial leads are absent or nontransvalvular is likely to be associated with a reduction in lead-related cardiac dysfunction.
36 Thank you
37
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis
 JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
Imaging MV. Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015
 Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
MITRAL REGURGITATION ECHO PARAMETERS TOOL
 Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Management of TR in Patients Undergoing Mitral Interventions
 Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
MITRAL VALVE PATHOLOGY WITH TRICUSPID REGURGITATION (AND PHT)
") UNIVERSITY OF PADUA, SCHOOL OF MEDICINE Department of Cardiac,Thoracic and Vascular Sciences Padua, Italy MITRAL VALVE PATHOLOGY WITH TRICUSPID REGURGITATION (AND PHT) Luigi P. Badano**, MD, PhD, FESC,
UNIVERSITY OF PADUA, SCHOOL OF MEDICINE Department of Cardiac,Thoracic and Vascular Sciences Padua, Italy MITRAL VALVE PATHOLOGY WITH TRICUSPID REGURGITATION (AND PHT) Luigi P. Badano**, MD, PhD, FESC,
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Index. B B-type natriuretic peptide (BNP), 76
, 76") Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
3D Echo for Evaluation of Tricuspid Regurgitation Jong-Min Song, MD, PhD
 3D Echo for Evaluation of Tricuspid Regurgitation Jong-Min Song, MD, PhD Asan Medical Center University of Ulsan College of Medicine Seoul, Korea Causes of TR Primary causes (25%) Rheumatic Myxomatous
3D Echo for Evaluation of Tricuspid Regurgitation Jong-Min Song, MD, PhD Asan Medical Center University of Ulsan College of Medicine Seoul, Korea Causes of TR Primary causes (25%) Rheumatic Myxomatous
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Organic mitral regurgitation
 The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
When Does 3D Echo Make A Difference?
 When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Atrioventricular valve repair: The limits of operability
 Atrioventricular valve repair: The limits of operability Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart
Atrioventricular valve repair: The limits of operability Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Ο ΡΟΛΟΣ ΤΩΝ ΚΟΛΠΩΝ ΣΤΗ ΛΕΙΤΟΥΡΓΙΚΗ ΑΝΕΠΑΡΚΕΙΑ ΤΩΝ ΚΟΛΠΟΚΟΙΛΙΑΚΩΝ ΒΑΛΒΙΔΩΝ
 Ο ΡΟΛΟΣ ΤΩΝ ΚΟΛΠΩΝ ΣΤΗ ΛΕΙΤΟΥΡΓΙΚΗ ΑΝΕΠΑΡΚΕΙΑ ΤΩΝ ΚΟΛΠΟΚΟΙΛΙΑΚΩΝ ΒΑΛΒΙΔΩΝ Ανδρέας Κατσαρός Καρδιολόγος Επιµ. Α Καρδιοχειρ/κών Τµηµάτων Γ.Ν.Α. Ιπποκράτειο ΚΑΜΙΑ ΣΥΓΚΡΟΥΣΗ ΣΥΜΦΕΡΟΝΤΩΝ ΑΝΑΦΟΡΙΚΑ ΜΕ ΤΗΝ ΠΑΡΟΥΣΙΑΣΗ
Ο ΡΟΛΟΣ ΤΩΝ ΚΟΛΠΩΝ ΣΤΗ ΛΕΙΤΟΥΡΓΙΚΗ ΑΝΕΠΑΡΚΕΙΑ ΤΩΝ ΚΟΛΠΟΚΟΙΛΙΑΚΩΝ ΒΑΛΒΙΔΩΝ Ανδρέας Κατσαρός Καρδιολόγος Επιµ. Α Καρδιοχειρ/κών Τµηµάτων Γ.Ν.Α. Ιπποκράτειο ΚΑΜΙΑ ΣΥΓΚΡΟΥΣΗ ΣΥΜΦΕΡΟΝΤΩΝ ΑΝΑΦΟΡΙΚΑ ΜΕ ΤΗΝ ΠΑΡΟΥΣΙΑΣΗ
Ischemic Mitral Regurgitation
 Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
PRINCIPLES OF ENDOCARDITIS
 015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
Assessing the Impact on the Right Ventricle
 Advances in Tricuspid Regurgitation Congress of the European Society of Cardiology (ESC) Munich, August 25-29, 2012 Assessing the Impact on the Right Ventricle Stephan Rosenkranz, MD Clinic III for Internal
Advances in Tricuspid Regurgitation Congress of the European Society of Cardiology (ESC) Munich, August 25-29, 2012 Assessing the Impact on the Right Ventricle Stephan Rosenkranz, MD Clinic III for Internal
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
MR echo case. N.Koutsogiannis Department of Cardiology University Hospital Of Patras
 MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
Imaging to select patients for Transcatheter TV
 Imaging to select patients for Transcatheter TV Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands San Diego, february 2018 Research grants: Medtronic, Biotronik, Boston Scientific,
Imaging to select patients for Transcatheter TV Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands San Diego, february 2018 Research grants: Medtronic, Biotronik, Boston Scientific,
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Surgery For Ebstein Anomaly
 Surgery For Ebstein Anomaly Christian Pizarro, MD Chief, Pediatric Cardiothoracic Surgery Director, Nemours Cardiac Center Alfred I. dupont Hospital for Children Professor of Surgery and Pediatrics Sidney
Surgery For Ebstein Anomaly Christian Pizarro, MD Chief, Pediatric Cardiothoracic Surgery Director, Nemours Cardiac Center Alfred I. dupont Hospital for Children Professor of Surgery and Pediatrics Sidney
When should we intervene surgically in pediatric patient with MR?
 When should we intervene surgically in pediatric patient with MR? DR.SAUD A. BAHAIDARAH CONSULTANT, PEDIATRIC CARDIOLOGY ASSISTANT PROFESSOR OF PEDIATRICS HEAD OF CARDIOLOGY AND CARDIAC SURGERY UNIT KAUH
When should we intervene surgically in pediatric patient with MR? DR.SAUD A. BAHAIDARAH CONSULTANT, PEDIATRIC CARDIOLOGY ASSISTANT PROFESSOR OF PEDIATRICS HEAD OF CARDIOLOGY AND CARDIAC SURGERY UNIT KAUH
MATRIX VHD FORM. State the name of the patient ( Product Recipient ) for whom you are providing the information contained in this form.
 for whom you are providing the information contained in this form.") MATRIX VHD FORM A. Patient Information State the name of the patient ( Product Recipient ) for whom you are providing the information contained in this form. (First Name) (Middle Initial) (Last Name) (Date
MATRIX VHD FORM A. Patient Information State the name of the patient ( Product Recipient ) for whom you are providing the information contained in this form. (First Name) (Middle Initial) (Last Name) (Date
Percutaneous Mitral Valve Repair
 Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Management of Tricuspid Regurgitation
 Management of Tricuspid Regurgitation Antonis A. Pitsis, FETCS, FESC Thessaloniki Heart Institute, St. Luke s Hospital, Thessaloniki, GREECE HEART FAILURE 2012 BELGRADE SERBIA Does Tricuspid Regurgitation
Management of Tricuspid Regurgitation Antonis A. Pitsis, FETCS, FESC Thessaloniki Heart Institute, St. Luke s Hospital, Thessaloniki, GREECE HEART FAILURE 2012 BELGRADE SERBIA Does Tricuspid Regurgitation
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Tricuspid leaflet repair: innovative solutions
 Perspective Tricuspid leaflet repair: innovative solutions Jack H. Boyd 1, J. James B. Edelman 2, David H. Scoville 1, Y. Joseph Woo 1 1 Department of Cardiothoracic Surgery, Stanford University School
Perspective Tricuspid leaflet repair: innovative solutions Jack H. Boyd 1, J. James B. Edelman 2, David H. Scoville 1, Y. Joseph Woo 1 1 Department of Cardiothoracic Surgery, Stanford University School
CASE REPORT: DOUBLE ORIFICE MITRAL VALVE WITH CLEFT IN ANTERIOR LEAFLET OF DOMINANT VALVE IN AN AFRO-CARIBBEAN
 CASE REPORT: DOUBLE ORIFICE MITL VAE WITH CLEFT IN ANTERIOR LEAFLET OF DOMINANT VAE IN AN AFRO-CARIBBEAN Disclosure: No potential conflict of interest. Received: 27.08.13 Accepted: 23.06.14 Citation: EMJ
CASE REPORT: DOUBLE ORIFICE MITL VAE WITH CLEFT IN ANTERIOR LEAFLET OF DOMINANT VAE IN AN AFRO-CARIBBEAN Disclosure: No potential conflict of interest. Received: 27.08.13 Accepted: 23.06.14 Citation: EMJ
Regurgitant Lesions. Bicol Hospital, Legazpi City, Philippines July Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA
 Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Introduction. Aortic Valve. Outflow Tract and Aortic Valve Annulus
 Chapter 1: Surgical anatomy of the aortic and mitral valves Jordan RH Hoffman MD, David A. Fullerton MD, FACC University of Colorado School of Medicine, Department of Surgery, Division of Cardiothoracic
Chapter 1: Surgical anatomy of the aortic and mitral valves Jordan RH Hoffman MD, David A. Fullerton MD, FACC University of Colorado School of Medicine, Department of Surgery, Division of Cardiothoracic
Pacing in patients with congenital heart disease: part 1
 Pacing in patients with congenital heart disease: part 1 September 2013 Br J Cardiol 2013;20:117 20 doi: 10.5837/bjc/2013.028 Authors: Khaled Albouaini, Archana Rao, David Ramsdale View details Only a
Pacing in patients with congenital heart disease: part 1 September 2013 Br J Cardiol 2013;20:117 20 doi: 10.5837/bjc/2013.028 Authors: Khaled Albouaini, Archana Rao, David Ramsdale View details Only a
Prof. JL Zamorano Hospital Universitario Ramón y Cajal
 Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας
 Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Trans-catheter TV repair Leaflet or Annuloplasty Techniques
 EuroValve 2018 Palermo, Italy Trans-catheter TV repair Leaflet or Annuloplasty Techniques Corrado Tamburino, MD, PhD Full Professor, University of Catania University Policlinic, Catania FACTS ON TRICUSPID
EuroValve 2018 Palermo, Italy Trans-catheter TV repair Leaflet or Annuloplasty Techniques Corrado Tamburino, MD, PhD Full Professor, University of Catania University Policlinic, Catania FACTS ON TRICUSPID
What is Ebstein Anomaly?
 Echocardiograpnhic Evaluation of : Definition, Detection and Determinants of Outcome P. W. O Leary, M.D. Division of Pediatric Cardiology Mayo Clinic No Conflicts to Disclose What is? Failure of the TV
Echocardiograpnhic Evaluation of : Definition, Detection and Determinants of Outcome P. W. O Leary, M.D. Division of Pediatric Cardiology Mayo Clinic No Conflicts to Disclose What is? Failure of the TV
Cardiac ultrasound protocols
 Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Effects of pacemaker and implantable cardioverter defibrillator electrodes on tricuspid regurgitation and right sided heart functions
 ORIGINAL ARTICLE Cardiology Journal 2015, Vol. 22, No. 6, 637 644 DOI: 10.5603/CJ.a2015.0060 Copyright 2015 Via Medica ISSN 1897 5593 Effects of pacemaker and implantable cardioverter defibrillator electrodes
ORIGINAL ARTICLE Cardiology Journal 2015, Vol. 22, No. 6, 637 644 DOI: 10.5603/CJ.a2015.0060 Copyright 2015 Via Medica ISSN 1897 5593 Effects of pacemaker and implantable cardioverter defibrillator electrodes
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018
 1 EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018 David A. Orsinelli, MD, FACC, FASE Professor, Internal
1 EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018 David A. Orsinelli, MD, FACC, FASE Professor, Internal
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine
 Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Pericardial Diseases. Smonporn Boonyaratavej, MD. Division of Cardiology, Department of Medicine Chulalongkorn University
 Pericardial Diseases Smonporn Boonyaratavej, MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital 21 AUGUST 2016 Pericardial
Pericardial Diseases Smonporn Boonyaratavej, MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital 21 AUGUST 2016 Pericardial
The Edge-to-Edge Technique f For Barlow's Disease
 The Edge-to-Edge Technique f For Barlow's Disease Ottavio Alfieri, Michele De Bonis, Elisabetta Lapenna, Francesco Maisano, Lucia Torracca, Giovanni La Canna. Department of Cardiac Surgery, San Raffaele
The Edge-to-Edge Technique f For Barlow's Disease Ottavio Alfieri, Michele De Bonis, Elisabetta Lapenna, Francesco Maisano, Lucia Torracca, Giovanni La Canna. Department of Cardiac Surgery, San Raffaele
Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας
 Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας Μυτάς Δημήτρης MD, PhD Επιμ Α ΕΣΥ Σισμανόγλειο Γενικό Νοσοκομείο Αττικής Δηλώνω υπεύθυνα ότι η παρούσα ομιλία δεν επιχορηγείται
Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας Μυτάς Δημήτρης MD, PhD Επιμ Α ΕΣΥ Σισμανόγλειο Γενικό Νοσοκομείο Αττικής Δηλώνω υπεύθυνα ότι η παρούσα ομιλία δεν επιχορηγείται
Functional Mitral Regurgitation
 Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
April 16, 09:00-09:15 중앙대학교 윤신원
 April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
Valve Analysis and Pathoanatomy: THE MITRAL VALVE
 : THE MITRAL VALVE Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Washington University School of Medicine, St. Louis, MO Secretary, American Association for Thoracic Surgery
: THE MITRAL VALVE Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Washington University School of Medicine, St. Louis, MO Secretary, American Association for Thoracic Surgery
Aortic Regurgitation & Aorta Evaluation
 VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
Ischemic Mitral Regurgitation
 Ischemic Mitral Regurgitation 1 / 6 2 / 6 3 / 6 Ischemic Mitral Regurgitation Background Myocardial infarction (MI) can directly cause (IMR), which has been touted as an indicator of poor prognosis in
Ischemic Mitral Regurgitation 1 / 6 2 / 6 3 / 6 Ischemic Mitral Regurgitation Background Myocardial infarction (MI) can directly cause (IMR), which has been touted as an indicator of poor prognosis in
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Upgrade to Resynchronization Therapy. Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic May 2016
 Upgrade to Resynchronization Therapy Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic May 2016 Event Free Survival (%) CRT Cardiac resynchronization therapy (CRT)
Upgrade to Resynchronization Therapy Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic May 2016 Event Free Survival (%) CRT Cardiac resynchronization therapy (CRT)
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
pulmonary valve on, 107 pulmonary valve vegetations on, 113
 INDEX Adriamycin-induced cardiomyopathy, 176 Amyloidosis, 160-161 echocardiographic abnormalities in, 160 intra-mural tumors similar to, 294 myocardial involvement in, 160-161 two-dimensional echocardiography
INDEX Adriamycin-induced cardiomyopathy, 176 Amyloidosis, 160-161 echocardiographic abnormalities in, 160 intra-mural tumors similar to, 294 myocardial involvement in, 160-161 two-dimensional echocardiography
Ιπποκράτειες μέρες καρδιολογίας Θεσσαλονίκη, 9-10 Μαρτίου Φωτεινή Α. Λαζαρίδου Επιμελήτρια Α Γενικό Νοσοκομείο Αγιος Παύλος, Θεσσαλονίκη
 Ιπποκράτειες μέρες καρδιολογίας Θεσσαλονίκη, 9-10 Μαρτίου 2018 Φωτεινή Α. Λαζαρίδου Επιμελήτρια Α Γενικό Νοσοκομείο Αγιος Παύλος, Θεσσαλονίκη RV shape Triangular shape in frontal plane crescent shape in
Ιπποκράτειες μέρες καρδιολογίας Θεσσαλονίκη, 9-10 Μαρτίου 2018 Φωτεινή Α. Λαζαρίδου Επιμελήτρια Α Γενικό Νοσοκομείο Αγιος Παύλος, Θεσσαλονίκη RV shape Triangular shape in frontal plane crescent shape in
Despite advances in our understanding of the pathophysiology
 Suture Relocation of the Posterior Papillary Muscle in Ischemic Mitral Regurgitation Benjamin B. Peeler MD,* and Irving L. Kron MD,*, *Department of Cardiovascular Surgery, University of Virginia, Charlottesville,
Suture Relocation of the Posterior Papillary Muscle in Ischemic Mitral Regurgitation Benjamin B. Peeler MD,* and Irving L. Kron MD,*, *Department of Cardiovascular Surgery, University of Virginia, Charlottesville,
Assessment of Tricuspid and Pulmonic Valve Disease: Importance of 3D
 ssessment of Tricuspid and ulmonic Valve Disease: Importance of 3D Roberto M Lang, MD nterior eptal M-mode 2D Echocardiography osterior eptal nterior eptal 1 THE TV ON 3D ECHO RV perspective R perspective
ssessment of Tricuspid and ulmonic Valve Disease: Importance of 3D Roberto M Lang, MD nterior eptal M-mode 2D Echocardiography osterior eptal nterior eptal 1 THE TV ON 3D ECHO RV perspective R perspective
Μαρία Δρακοπούλου, Σοφία Βαïνά
 Μαρία Δρακοπούλου, Σοφία Βαïνά Α Πανεπιστημιακή Καρδιολογική Κλινική Ιπποκράτειο Νοσοκομείο Spectrum of mitral regurgitation German Heart Report 2017 MitraClip implantations have numerically outperformed
Μαρία Δρακοπούλου, Σοφία Βαïνά Α Πανεπιστημιακή Καρδιολογική Κλινική Ιπποκράτειο Νοσοκομείο Spectrum of mitral regurgitation German Heart Report 2017 MitraClip implantations have numerically outperformed
The Heart. Happy Friday! #takeoutyournotes #testnotgradedyet
 The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
Tricuspid and Pulmonic Valve Disease
 Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
MitraClip in the ICCU: Which Patient will Benefit?
 MitraClip in the ICCU: Which Patient will Benefit? DAVID MEERKIN STRUCTURAL A ND CONGENITAL HEART DISEASE UNIT SHAARE ZEDEK MEDICAL CENTER JERUSALEM Conflict of Interest No relevant disclosures Complex
MitraClip in the ICCU: Which Patient will Benefit? DAVID MEERKIN STRUCTURAL A ND CONGENITAL HEART DISEASE UNIT SHAARE ZEDEK MEDICAL CENTER JERUSALEM Conflict of Interest No relevant disclosures Complex
Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens
 MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
Ανεπάρκεια Τριγλώχινας Επιλογή Επεμβατικής Θεραπείας. Μ. Χρυσοχέρης Τμήμα Διαδερμικών Βαλβίδων ΔΘΚΑ ΥΓΕΙΑ
 Ανεπάρκεια Τριγλώχινας Επιλογή Επεμβατικής Θεραπείας Μ. Χρυσοχέρης Τμήμα Διαδερμικών Βαλβίδων ΔΘΚΑ ΥΓΕΙΑ Disclosures - Proctoring activities for Abbott Vascular, Edwards Lifesciences I and the HYGEIA Hospital
Ανεπάρκεια Τριγλώχινας Επιλογή Επεμβατικής Θεραπείας Μ. Χρυσοχέρης Τμήμα Διαδερμικών Βαλβίδων ΔΘΚΑ ΥΓΕΙΑ Disclosures - Proctoring activities for Abbott Vascular, Edwards Lifesciences I and the HYGEIA Hospital
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Advanced imaging of the left atrium - strain, CT, 3D, MRI -
 Advanced imaging of the left atrium - strain, CT, 3D, MRI - Monica Rosca, MD Carol Davila University of Medicine and Pharmacy, Bucharest, Romania Declaration of interest: I have nothing to declare Case
Advanced imaging of the left atrium - strain, CT, 3D, MRI - Monica Rosca, MD Carol Davila University of Medicine and Pharmacy, Bucharest, Romania Declaration of interest: I have nothing to declare Case
Questions on Chamber Quantitation
 Questions on Chamber Quantitation @RobertoMLang Which of the following statements is true? 1. The aortic annulus should be measured in midsystole. 2. The aortic annulus should be measured in enddiastole.
Questions on Chamber Quantitation @RobertoMLang Which of the following statements is true? 1. The aortic annulus should be measured in midsystole. 2. The aortic annulus should be measured in enddiastole.
Tricuspid Valve Stenosis Related to Subvalvular Adhesion of Pacemaker Lead: A Case Report
 J Cardiol 2006 Jun; 47 6 : 301 306 Tricuspid Valve Stenosis Related to Subvalvular Adhesion of Pacemaker Lead: A Case Report Kayano Asumi Akihisa Tatsuya Atsuhiro Kouichi TAIRA, MD SUZUKI, MD FUJINO, MD
J Cardiol 2006 Jun; 47 6 : 301 306 Tricuspid Valve Stenosis Related to Subvalvular Adhesion of Pacemaker Lead: A Case Report Kayano Asumi Akihisa Tatsuya Atsuhiro Kouichi TAIRA, MD SUZUKI, MD FUJINO, MD
Although most patients with Ebstein s anomaly live
 Management of Neonatal Ebstein s Anomaly Christopher J. Knott-Craig, MD, FACS Although most patients with Ebstein s anomaly live through infancy, those who present clinically as neonates are a distinct
Management of Neonatal Ebstein s Anomaly Christopher J. Knott-Craig, MD, FACS Although most patients with Ebstein s anomaly live through infancy, those who present clinically as neonates are a distinct
How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto
 How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto Introduction Hypertrophic cardiomyopathy is the most common genetic cardiomyopathy,
How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto Introduction Hypertrophic cardiomyopathy is the most common genetic cardiomyopathy,
THE HEART. A. The Pericardium - a double sac of serous membrane surrounding the heart
 THE HEART I. Size and Location: A. Fist-size weighing less than a pound (250 to 350 grams). B. Located in the mediastinum between the 2 nd rib and the 5 th intercostal space. 1. Tipped to the left, resting
THE HEART I. Size and Location: A. Fist-size weighing less than a pound (250 to 350 grams). B. Located in the mediastinum between the 2 nd rib and the 5 th intercostal space. 1. Tipped to the left, resting
ΔΙΑΔΕΡΜΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΔΟΜΙΚΩΝ ΠΑΘΗΣΕΩΝ: Ο ΡΟΛΟΣ ΤΗΣ ΑΠΕΙΚΟΝΙΣΗΣ ΣΤΟ ΑΙΜΟΔΥΝΑΜΙΚΟ ΕΡΓΑΣΤΗΡΙΟ ΣΤΗΝ ΤΟΠΟΘΕΤΗΣΗ MITRACLIP
 ΔΙΑΔΕΡΜΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΔΟΜΙΚΩΝ ΠΑΘΗΣΕΩΝ: Ο ΡΟΛΟΣ ΤΗΣ ΑΠΕΙΚΟΝΙΣΗΣ ΣΤΟ ΑΙΜΟΔΥΝΑΜΙΚΟ ΕΡΓΑΣΤΗΡΙΟ ΣΤΗΝ ΤΟΠΟΘΕΤΗΣΗ MITRACLIP ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ ΘΕΣΣΑΛΟΝΙΚΗ CONFLICT OF INTEREST PROCTOR
ΔΙΑΔΕΡΜΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΔΟΜΙΚΩΝ ΠΑΘΗΣΕΩΝ: Ο ΡΟΛΟΣ ΤΗΣ ΑΠΕΙΚΟΝΙΣΗΣ ΣΤΟ ΑΙΜΟΔΥΝΑΜΙΚΟ ΕΡΓΑΣΤΗΡΙΟ ΣΤΗΝ ΤΟΠΟΘΕΤΗΣΗ MITRACLIP ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ ΘΕΣΣΑΛΟΝΙΚΗ CONFLICT OF INTEREST PROCTOR
Revealing new insights. irotate electronic rotation and xplane adjustable biplane imaging. Ultrasound cardiology. irotate and xplane
 Ultrasound cardiology irotate and xplane Revealing new insights irotate electronic rotation and xplane adjustable biplane imaging Annemien van den Bosch and Jackie McGhie Department of Cardiology, Erasmus
Ultrasound cardiology irotate and xplane Revealing new insights irotate electronic rotation and xplane adjustable biplane imaging Annemien van den Bosch and Jackie McGhie Department of Cardiology, Erasmus
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT
 FOR REPAIRED TETRALOGY OF FALLOT") MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
the Cardiovascular System I
 the Cardiovascular System I By: Dr. Nabil A Khouri MD, MsC, Ph.D MEDIASTINUM 1. Superior Mediastinum 2. inferior Mediastinum Anterior mediastinum. Middle mediastinum. Posterior mediastinum Anatomy of
the Cardiovascular System I By: Dr. Nabil A Khouri MD, MsC, Ph.D MEDIASTINUM 1. Superior Mediastinum 2. inferior Mediastinum Anterior mediastinum. Middle mediastinum. Posterior mediastinum Anatomy of
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ
 ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ European Accreditation in TTE, TEE and CHD Echocardiography NOTHING TO DECLARE ATRIAL SEPTAL DEFECT TYPES SECUNDUM
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ European Accreditation in TTE, TEE and CHD Echocardiography NOTHING TO DECLARE ATRIAL SEPTAL DEFECT TYPES SECUNDUM
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Late secondary TR after left sided heart disease correction: is it predictibale and preventable
 Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Disclosure Statement of Financial Interest Saibal Kar, MD, FACC
 MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
Girish M Nair, Seeger Shen, Pablo B Nery, Calum J Redpath, David H Birnie
 268 Case Report Cardiac Resynchronization Therapy in a Patient with Persistent Left Superior Vena Cava Draining into the Coronary Sinus and Absent Innominate Vein: A Case Report and Review of Literature
268 Case Report Cardiac Resynchronization Therapy in a Patient with Persistent Left Superior Vena Cava Draining into the Coronary Sinus and Absent Innominate Vein: A Case Report and Review of Literature
Ebstein s anomaly is defined by a downward displacement
 Repair of Ebstein s Anomaly Sylvain Chauvaud, MD Ebstein s anomaly is a tricuspid valve anomaly associated with poor right ventricular contractility in severe cases. Surgery is indicated in all symptomatic
Repair of Ebstein s Anomaly Sylvain Chauvaud, MD Ebstein s anomaly is a tricuspid valve anomaly associated with poor right ventricular contractility in severe cases. Surgery is indicated in all symptomatic
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
By the end of this session, the student should be able to:
 Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired