EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018
|
|
|
- Gertrude Gilmore
- 5 years ago
- Views:
Transcription
1 1 EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
2 DISCLOSURES Institutional Research Support Medtronic Edwards Abbott 2
3 EVALUATION OF CHRONIC MITRAL REGURGITATION One of the most common valve lesions Published guidelines for the clinical and imaging evaluation and management of these patients are available This information has not penetrated in to day to day practice in many locations Many Barriers (Am Heart J 2016) Lack of auscultatory skills Echocardiographic quality / completeness Lack of knowledge of primary vs secondary MR and the differences in treatment approach Uncertainty as to appropriate timing of and treatment options available for treating MR Lack of local expertise in MV repair 3

4 4 RESOURCES / GUIDELINES
5 Survey of PCPs, General Cardiologists / Imaging Cardiologists, Interventional Cardiologists and Cardiac Surgeons Identified significant knowledge gaps in the management of MR (e.g. indications for / timing of interventions, appropriate interventions, knowledge of surgeons expertise / volume, understanding echo reports) PCPs reviewed the images or discussed the Echo report with the interpreting physician < 30% of the time What is on the report is taken as complete / factual Am Heart J 2016;172:70-79 Significant Gaps in the Quality / Completeness of Echo Performance Parameters and Reports 5
6 6 KNOWLEDGE GAPS IN THE ECHOCARDIOGRAPHIC ASSESSMENT OF MR: An Opportunity to Improve Patient Care What is missing from routine TTE Reports? Reports reviewed by non-echocardiographers < 2/3 of reports listed BP Quantitative measures (VC, ERO, RV, RF) in < 50% of studies. 10% stated quantitative data was never reported Interpreted / reported by Imagers BP reported in 82% VC (75%), ERO (64%), RV (45%), RF (39%) Imagers (vs non-imagers) who interpret Echo perform better What can / should be done For PCPs / Non imagers Review / ask questions of the interpreting physician For Echocardiographers Know when and how to quantitate MR (learn the techniques) Define the anatomy and mechanism of MR REPORT the findings Be open to reviewing the findings with other providers

7 Practice Gaps in MR Assessment: Recommended Interventions Am Heart J 2016 Sonographers: Incorporate quantification in education and implement in image acquisition Cardiologists: Systematic approach to implement an integrative assessment of MR Reporting: Standardize requirements for all reports when > mild MR is present: BP, MV anatomy / mechanism of MR, quantitative measures, prior study comparison CQI: Review image acquisition (sonographer) and interpretation / report (physicians). Correlation between TTE and TEE / intra-op findings 7
8 8 BRIDGING THE KNOWLEDGE GAP: IMPROVING THE ECHOCARDIOGRAPHIC ASSESSMENT OF MITRAL REGURGITATION
 TREATMENT: Intervention only indicated for severe (or moderate to severe)")
9 MANAGEMENT PATHWAY FOR MITRAL REGURGICATION IDENTIFY / STAGE: History, Clinical Exam, TTE. Stages A-D DEFINE: Mechanism / Classification SEVERITY: Quantification (more than an eyeball assessment of color Doppler jet) TREATMENT: Intervention only indicated for severe (or moderate to severe) MR. Options for clinical trials / best clinical (approved) therapies is determined by the mechanism of MR and confirmation of significant MR 9 JACC Nov 2017
10 OBJECTIVES Explain why it is important to classify the type of Mitral Regurgitation Define the Echocardiographic Methods used to classify Mitral Regurgitation Explain the importance of quantifying the severity of Mitral Regurgitation Review the Echocardiographic Methods used to assess the severity of Mitral Regurgitation 10
11 STAGES OF VALVULAR HEART DISEASE: MITRAL REGURGIATION Stage A: At risk (predisposition to develop VHD) Stage B: Progressive (mild to moderate disease, asymptomatic) Stage C: Asymptomatic Severe Disease (C1 without LV / RV dysfunction; C2 with LV / RV dysfunction) Stage D: Symptomatic Severe (symptoms due to VHD) 11

12 12 Stages of Primary MR (No changes from 2014 Guideline)
13 13 Stages of Secondary MR (Updated from 2014 Guideline) JACC 2017;70:252
14 Why is Defining Mechanism Important? Primary (Organic) and Secondary (Functional) MR are two different diseases Different natural history / prognosis Treatment recommendations and options are different Especially true for non-surgical therapies (e.g. MitraClip is approved for selected patients with Primary MR, not secondary MR) Surgical approaches (repair vs replacement) are different For Primary MR: Valve repair favored over replacement Best treatment for Secondary MR remains uncertain Reducing / eliminating MR is not curative MR is one piece of the problem (LV dysfunction, primary heart muscle disease, CAD etc.) No Class 1 indications for MV intervention 14
 MR A disease of the ventricle ( fixing the valve does not cure the underlying disease) Valve is usually structurally normal LV dysfunction (ICMP, NIMCP): LV dilates, papillary muscle")
15 15 Primary vs Secondary MR Primary (organic) MR A disease of the valve (fix the valve, potentially cure the disease) MVP / Barlow s FED Endocarditis CTD RHD Radiation Clefts / congenital Secondary (functional) MR A disease of the ventricle ( fixing the valve does not cure the underlying disease) Valve is usually structurally normal LV dysfunction (ICMP, NIMCP): LV dilates, papillary muscle displacement, leaflet tethering RWMA (esp inferolateral wall) Annular dilation (dilated LV, Afib)
 Secondary (functional) MR Valve anatomy is normal (impaired mobility) Only quantitative assessment of severity Primary anatomic / functional abnormalities of the LV")
16 Considerations in Staging of Primary vs Secondary MR Primary (organic) MR Emphasis is on valve anatomy Qualitative and quantitative assessment of severity Secondary effects on LA and LV Symptoms ascribed to the MR (CHF, etc) Secondary (functional) MR Valve anatomy is normal (impaired mobility) Only quantitative assessment of severity Primary anatomic / functional abnormalities of the LV Symptoms often due to underlying CAD or LV dysfunction 16
17 Indications for Surgery / Intervention Depend on Stage and Type of MR 17 PRIMARY MR Class I Stage D (EF > 30%) Stage C2 Repair > Replace Class IIa Stage C1 Stage B (with other surgery) Class IIb Stage D (EF <30%) TMV Repair (Stage D prohibitive surgical risk) Class III MV Replacement (unless repair unsuccessful) SECONDARY MR None Class I Class IIa Stage C/D (with other surgery) MV Replacement (Stage D ischemic MR)* Class IIb Stage D (repair or replace non ischemic)* Stage B (repair, with other surgery) * Symptoms despite GDMT for CHF
18 18 How Do I Define the Mechanism of MR?
19 Decision Tree for Defining The Mechanism of MR: Primary vs Secondary MR 19 JACC 2017:;70:2421
20 Steps in Defining The Mechanism of MR: Evaluate MV, LV and LA 20 Describe MV anatomy in detail Thickening, calcification, redundancy, flail, vegetations, perforations, chordal rupture Annulus Submitral apparatus LV findings Organic MR with normal LV / LA unlikely to be severe Normal MV anatomy suggests secondary MR Mechanism: LV dilation, RWMA, atrial enlargement JACC 2017:;70:2421
 Type II (Excessive Motion) Prolapse / flail (primary MR) Type IIIA (Motion restricted in systole / diastole) RHD, radiation, drugs, inflammatory disease (primary MR) Type IIIB (Motion")
21 Steps in Defining The Mechanism of MR: Define Leaflet Motion and Morphology 21 Carpentier Classification Type 1 (Normal Motion) Endocarditis, perforation, clefts (primary MR) Normal anatomy (atrial secondary MR) Type II (Excessive Motion) Prolapse / flail (primary MR) Type IIIA (Motion restricted in systole / diastole) RHD, radiation, drugs, inflammatory disease (primary MR) Type IIIB (Motion restricted in systole) Normal leaflets usually with ischemic / dilated CMP (secondary MR) Abnormal leaflets such as partial flail / torn chordae (mixed MR) JACC 2017:;70:2421
22 Steps in Defining The Mechanism of MR: Classify as Primary, Secondary or Mixed Primary MR Abnormal leaflets (Type I, II, IIIA) Secondary MR Normal leaflets (Type I or IIIB) Mixed MR Primary MR with secondary LV dilation / dysfunction (e.g. untreated chronic MR, intervening infarct with RWMA) Secondary MR with subsequent leaflet disruption (e.g. chordal / papillary muscle rupture) 22 JACC 2017:;70:2421
23 Common Pitfall / Misclassification Anterior leaflet override due to posterior leaflet restriction is pure secondary MR and NOT mixed etiology Consensus Statement (JACC 2017; 70: 2421) a severely restricted posterior leaflet due to ischemic wall motion abnormality may result in anterior leaflet override. In such cases, the anterior leaflet is not prolapsed and this does not represent a mixed etiology ASE Native Valve Regurgitation Guidelines (JASE 2017;30:303) 23
24 How Do I Define the Mechanism of MR? Other Clues Color Doppler jet direction Anteriorly directed jet Posterior leaflet prolapse / flail (common) or anterior leaflet restriction (not common) Posteriorly directed jet Anterior leaflet prolapse / flail or posterior leaflet restriction (common with functional MR) Central jet Common in secondary MR (dilated CMP), can be seen in primary MR PISA Hemispheric (primary) Not hemispheric (secondary) Continuous Wave Doppler May be mid-late systolic (primary MR in MVP) Holosystolic / uniform density (secondary MR with RWMA) Biphasic density with mid-systolic dropout ( dilated CMP with global dysfunction) 24

25 Primary vs Secondary MR 25 JASE 2017;30:303
26 ASSESSING SEVERITY QUANTIFICATION OF MITRAL VALVE REGURGITATION WHY, HOW and WHEN? WHY SHOULD I QUANTIFY VALVE REGURGITATION? WHY DON T WE QUANTIFY VALVE REGURGITATION? TOOLS TO QUANTIFY VALVE REGURGITATION (MR) WHAT IS QUANTIFICATION OF MR? WHEN SHOULD YOU QUANTIFY VALVE REGURGITATION? 26
27 Why is Echo Quantification of MR Important? Staging and subsequent treatment recommendations depend on an accurate assessment of the degree of MR Staging of both Primary and Secondary MR guided by quantitative measures Only quantitative methods are recommended for secondary MR Staging also involves an accurate evaluation of valve anatomy, hemodynamic consequences (LA, LV, PASP) and symptom assessment Color Flow Doppler (Qualitative) has many limitations Echocardiographic assessment has supplanted the invasive assessment of MR 27

28 PRIMARY MR EVALUATION QUANTITATIVE MEASURES DIFFERENTIATE STAGE B / C 28 Nishimura et al. ACC / AHA Valve Guidelines 2014
29 Stages of Secondary MR (Updated from 2014 Guideline) JACC 2017;70:252 ONLY QUANTITATIVE MEASURES ARE RECOMMENDED AND THESE PARAMETERS DIFFERENTIATE STAGE B / C 29 QUANTITATIVE MEASURES FOR ERO AND RV ARE NOW CONCORDANT WITH PRIMARY MR RECOMMENDATIONS
30 Should Quantitative Parameters Differ Between Primary and Secondary MR? In 2014 guidelines there were different (lower) quantitative cut-offs for secondary MR using PISA ERO and Regurgitant Volume Since LV is impaired in secondary MR, a smaller regurgitant volume or ERO may have greater (adverse) impact on outcome Severity may increase over time as LV continues to remodel / EF drops in secondary MR Doppler assessment (PISA ERO) may be less accurate in secondary MR 2017 Update made cut-offs concordant ERO > 0.2 cm 2 is more sensitive, an ERO > 0.4 cm 2 is more specific for severe secondary MR 30
31 Hemodynamic Considerations With Chronic MR MR can be dynamic Changes in loading conditions BP, effects of sedation / anesthesia, volume status, ischemia Severity can vary during systole (assuming constant flow or constant regurgitant orifice may overestimate MR severity) MVP (mid-late systole) Secondary MR (biphasic) SAM (HCMP, post MV repair) MR may change with volume status, LV contractility Rhythm and Pacing RV pacing can induce dyssynchrony (increases MR) Atrial fibrillation Variable MR depending on cycle length, changes in LV volume / contractility 31



32 QUANTIFICATION OF VALVE DISEASE ROUTINELY QUANTIFY VALVE STENOSIS AORTIC STENOSIS MEAN GRADIENT VALVE AREA WE DON T EYEBALL AS WHY NOT FOR VALVE INSUFFICIENCY? Why are we comfortable eyeballing MR?? 32
33 Why Do We Not Quantify MR? 33 Lack of training / knowledge Not thought to be important ( eyeball is good enough) We do not believe the Echo techniques Time Consuming Challenges in Grading the Severity of Valve Regurgitation What is the Gold Standard? Angiographic Grades vs Quantitative (invasive) grades compared to Echo / MRI Variability of severity depending on hemodynamics Time constraints and financial dis-incentives Severe MR gets paid the same as There is severe primary MR. The mitral valve is myxomatous with a flail P2 segment. The VC is 0.8 cm, the ERO is 0.45 cm 2 with a regurgitant volume of 63 cc. Compared to the last study, the P2 flail is new and the MR is now severe
 We do not believe the Echo techniques Time Consuming Challenges in Grading the Severity of Valve Regurgitation")
34 Why Do We Not Quantify MR? 34 Lack of training / knowledge Not thought to be important ( eyeball is good enough) We do not believe the Echo techniques Time Consuming Challenges in Grading the Severity of Valve Regurgitation What is the Gold Standard? Angiographic Grades vs Quantitative (invasive) grades compared to Echo / MRI Variability of severity depending on hemodynamics Time constraints and financial dis-incentives Severe MR gets paid the same as There is severe primary MR. The mitral valve is myxomatous with a flail P2 segment. The VC is 0.8 cm, the ERO is 0.45 cm 2 with a regurgitant volume of 63 cc. Compared to the last study, the P2 flail is new and the MR is now severe
35 ECHO ASSESSMENT OF MITRAL VALVE INSUFFICIENCY STRUCTURAL PARAMETERS VALVE ANATOMY (Classification of disease) ATRIAL / VENTRICULAR SIZE (consequences of disease, etiology of MR) DOPPLER PARAMETERS SPECTRAL DOPPLER TMF E WAVE PV DOPPLER PATTERN DENSITY / SHAPE OF MR JET COLOR DOPPLER JET AREA VENA CONTRACTA FLOW CONVERGENCE ZONE ERO (PISA) REGURGITANT VOLUME / FRACTION 35

36 ASE GUIDELINES FOR ASSESSING MR Advantages and Limitations 36 Zoghbi et al JASE 2003:16: 777
37 WHAT ECHOCARDIOGRAPHIC TOOLS ARE AVAILABLE TO ASSESS MR SEVERITY? QUALITATIVE SEMI-QUANTITATIVE QUANTITATIVE METHODS 37

38 WHAT QUALITATIVE TOOLS ARE AVAILABLE TO ASSESS MR? QUALITATIVE LA SIZE / LV SIZE DENSITY OF MR JET CONTOUR OF MR JET PV DOPPLER PATTERN E wave VELOCITY A WAVE DOMINANCE (severe MR unlikely) 38 Zoghbi et al JASE 2017;30:303 Fig 12

39 WHAT SEMI-QUANTITATIVE TOOLS ARE AVAILABLE TO ASSESS MR? SEMI-QUANTITATIVE COLOR JET AREA MULTIPLE LIMITATIONS VENA CONTRACTA FLOW CONVERGENCE (PISA) Zoghbi et al JASE 2003:16:
40 WHAT QUANTITATIVE TOOLS ARE AVAILABLE TO ASSESS MR? QUANTITATIVE MEASURES EROA (PISA and DOPPLER) REGURGITANT VOLUME PISA QUANTITATIVE ASSESSMENT OF STROKE VOLUME AND REGURGITANT VOLUME DOPPLER VOLUMES 2 / 3 D VOLUMES REGURGITANT FRACTION Zoghbi et al JASE 2003:16: Feigenbaum 6 th Ed, page 220
 Regurgitant jet area Vena Contracta Flow")
41 ASSESSMENT OF MR SEVERITY Color Flow Doppler Primary tool to screen for MR Absence of a color Doppler jet excludes MR Caveat: acoustic shadowing of the LA Three measurements (qualitative / semi-quantitative) Regurgitant jet area Vena Contracta Flow Convergence 41
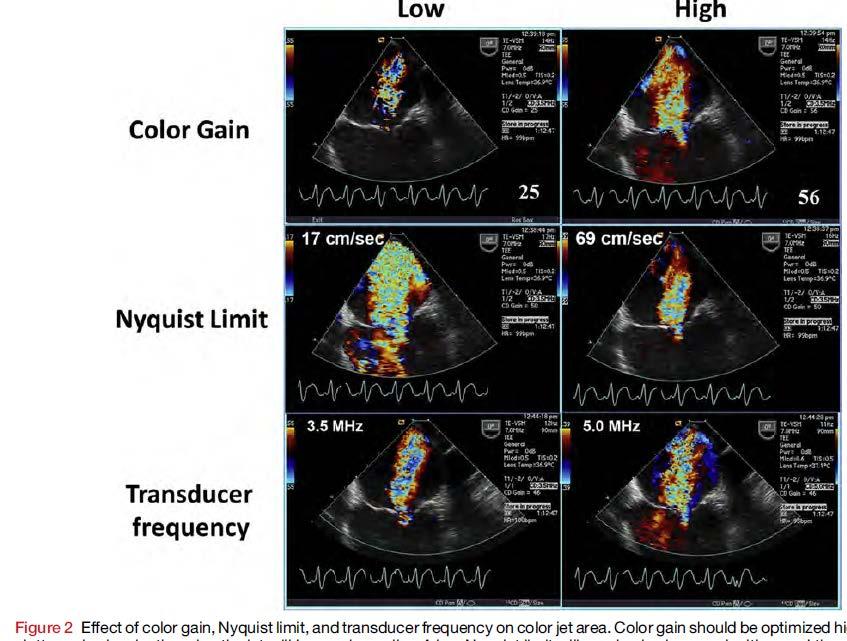
42 ASSESSMENT OF MR SEVERITY COLOR FLOW DOPPLER (Jet Area) Probably the most widely used measure Very qualitative Many limitations Affected by instrument settings Affected by hemodynamics For a given ERO, a high velocity jet will appear larger than a lower velocity jet A 6 m/s MR jet is 44% larger than a 5 m/s jet AS, uncontrolled hypertension will result in larger jets MR color jets in the setting of low driving pressure (e.g. severe LV dysfunction) often appear small and underestimate severity Eccentric jets appear smaller (Coanda effect) and underestimate severity 42
43 ASSESSMENT OF MR SEVERITY COLOR FLOW DOPPLER (Jet Area) Appearance can depend on mechanism Flail leaflet: eccentric jet (small, underestimates severity) Central slit like jets in secondary MR can overestimate severity Large in 2 chamber / commissural view Color Jet area alone (even indexed to LA) should NOT be used in isolation to assess MR severity Assess jet origin (VC / Flow convergence) A small non eccentric jet with a small VC and no flow convergence usually indicates mild MR A large jet with a wide VC, large flow convergence, that wraps around the LA and penetrates deep in to the PV is almost always severe MR 43

44 44 Zoghbi JASE 2017;30:303
45 ASSESSMENT OF MR SEVERITY COLOR FLOW DOPPLER (Vena Contracta) Semi-quantitative Independent of flow rate / driving pressure Estimation of the EROA (smaller than the ARO) Zoom of PLAX (A3ch is alternative) Measure narrowest diameter as jet emerges from orifice VC < 0.3 cm mild MR VC > 0.7 cm severe MR Intermediate values require further evaluation Not accurate with multiple jets / elliptical orifices / dynamic orifices 3 D VC area using MPRs and direct planimetry 45
46 ASSESSMENT OF MR SEVERITY COLOR FLOW DOPPLER (Flow Convergence or PISA) More accurate for central jets and circular orifices Challenging to determine exact location of orifice PISA can vary over the cardiac cycle Crescent shape orifice (often seen in functional MR) may result in underestimation of MR Lower cut-off values may be appropriate A small or non existent FC with a small jet is specific for mild MR A large FC that persists throughout systole is specific for severe MR FC data can be used to quantitate regurgitant flow 46

47 ASSESSMENT OF MR SEVERITY Continuous Wave Doppler as a Qualitative Measure Spectral density is proportionate to the # of rbc s reflecting the Doppler signal Timing / duration of jet reflects underlying hemodynamics Jets that are not holosystolic reflect less volume Predominate early systolic jets with CMP / dyssynchrony Mid-late systolic jets with MVP Non parabolic (early peaking or cutoff sign) suggests a large V wave Peak velocity does NOT reflect severity of MR May reflect hemodynamic consequences Low velocity (<4m/s) with low BP or high LAP 47 Zoghbi JASE 2017;30:303
 and E/A ratio suggest significant MR A wave predominance not consistent with severe MR Multiple limitations (presence of MS, DD,")

48 ASSESSMENT OF MR SEVERITY Pulsed Doppler as a Qualitative Measure TMF E and A velocity Increased Ev (>1.2m/s) and E/A ratio suggest significant MR A wave predominance not consistent with severe MR Multiple limitations (presence of MS, DD, MV ring, severe MAC) In secondary MR, confounded by influence of elevated filling pressures PV flow patterns As MR increases in severity, systolic flow is progressively blunted Systolic flow reversal is specific but not sensitive Confounded by effect of filling pressures Zoghbi JASE 2017;30:303 48
49 Doppler Quantitation of MR EROA PISA methodology Regurgitant volume Can be calculated using PISA combined with CW Doppler (ERO x VTI MR ) Can be calculated with Doppler assessment of forward stroke volume and total mitral valve stroke volume (or 2 D / 3 D derived volumes) Regurgitant Fraction Can be calculated with Doppler assessment of regurgitant volume and total stroke volume (or 2 D / 3 D derived volumes) 49
 Shape of PISA Shape of RO Eccentric jets (hard to align Doppler) Multiple")
50 Flow Convergence (PISA) Derived ERO Baseline shift in direction of flow Down on TTE Up on TEE Calculate the ERO as well as the Rvol Many limitations Timing of measurements Duration (if not holosystolic) Shape of PISA Shape of RO Eccentric jets (hard to align Doppler) Multiple jets 50
51 WHAT TOOLS ARE AVAILABLE TO ASSESS MR? QUANTITATIVE METHODS TO ASSESS VOLUMES Calculating Stroke Volume and Regurgitant Volume DOPPLER METHODS PW DOPPLER SV valve = πd 2 /4 x VTI valve REQUIRES ONE VALVE WITHOUT (SIGNIFICANT) REGURGITATION RV = SV REG VALVE - SV COMP VALVE 2D/3D METHODS TOTAL SV FROM LV ED VOL LV ES VOL RV = TOTAL SV - SV COMP VALVE EROA = Rvol / VTI mr jet 51
 2 * VTI LVOT = 58 cc SV MV = π(mvd/2) 2 * VTI MV inflow =183 cc RVol = 183-58=125 cc RF = 125/183 = 68 % 52")
52 DOPPLER CALCULATION OF SV, RV and RF for MR Measurement error in any one of these 4 parameters can occur Assumes a circular orifice Feigenbaum 6 th Ed, page 220 SV LVOT = π(lvotd/2) 2 * VTI LVOT = 58 cc SV MV = π(mvd/2) 2 * VTI MV inflow =183 cc RVol = =125 cc RF = 125/183 = 68 % 52
53 CALCULATION OF REGURGITANT FRACTION Mitral Regurgitant Fraction (Doppler) MV stroke volume - AV stroke volume MV stroke volume Mitral Regurgitant Fraction (2/3D volumes) LV stroke volume - AV stroke volume LV stroke volume 53

54 54 ASE GUIDELINES FOR ASSESSMENT OF MR Zoghbi et al JASE 2017;30:303
55 55 When Should I Quantitate MR?
56 When Should I (Perhaps) NOT Quantitate MR? INITIAL ASSESSMENT SUGGESTS MINIMAL / MILD MR SMALL COLOR JET AREA, VCW < 0.3 cm, NO FLOW CONVERGENCE, NORMAL LA / LV SIZE, PW AND CW DOPPLER (A wave predominance, soft or incomplete MR jet) INITIAL ASSESSMENT SUGGESTS SEVERE MR LARGE VCW > 0.7 cm, LARGE JET AREA, LARGE FLOW CONVERGENCE (radius > 1 cm), FLAIL LEAFLET / LACK OF LEAFLET COAPTATION, SPECTRAL DOPPLER E wave predominance, PV flow reversal, DILATED LV WITH NORMAL EF 56
57 WHEN SHOULD I QUANTIFY MR? WHEN CLINICAL DECISION MAKING HINGES ON AN ACCURATE ASSESSMENT OF MR SEVERITY ESPECIALLY IN THE ASYMPTOMATIC PATIENT IN 2-3+ MR PATIENTS INTERMEDIATE / MIXED QUALITATITVE / SEMIQUANTITATIVE FINDINGS CAN HELP TO DOWNGRADE or UPGRADE WHEN CLINICAL SYMPTOMS AND ECHO FINDINGS ARE DISCORDANT 57

58 58 When Should I Quantitate MR?






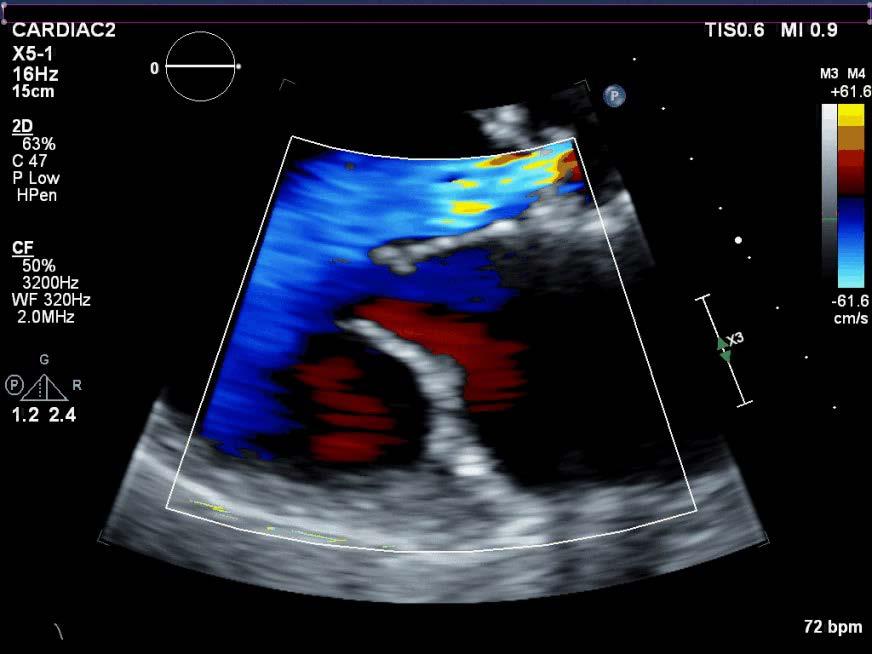
59 CHRONIC MR: A REAL CASE MILD, MODERATE OR SEVERE Primary, Secondary or Mixed? Mild, Moderate or Severe? ERO= 2π (0.5) 2 *39 = 0.13 cm


 2 *34 = 0.")
60 CHRONIC MR: ANOTHER REAL CASE MILD, MODERATE OR SEVERE Primary, Secondary or Mixed? Mild, Moderate or Severe? ERO= 2π (1.1) 2 *34 = 0.49 cm
61 HOW SHOULD I QUANTIFY MITRAL REGURGITATION? WHAT TOOLS ARE AVAILABLE? ECHOCARDIOGRAPHY INITIAL EVALUATION PRIMARY CLINICAL TOOL CARDIAC MRI IMPORTANT SECONDARY TOOL CATHETERIZATION / ANGIOGRAPHY LIMITED ROLE 61
62 Putting it All Together 62 Clinical scenario Symptoms Physical Exam Echocardiography Description of valve anatomy and mechanism (primary vs secondary) LA and LV assessment Assessment of Severity Qualitative measures Semi-quantitative measures Quantitative measures VC ERO (PISA) CALCULATE RV / RF Integrative approach All Echo methods / parameters have limitations Use all of the available tools
63 HELPFUL HINTS WITH PRIMARY MR Severe valve pathology (flail leaflet, ruptured papillary muscle, severe leaflet retraction or large perforation) is fairly specific for severe MR VCW > 0.7 cm and PV systolic flow reversal are specific for severe MR Lack of a FC zone or presence of A wave dominance are specific for nonsevere MR Assess MR duration and character of MR jet Late systolic MR rarely severe Spectral MR jet is not dense suggests nonsevere MR Normal LA volume usually precludes severe chronic MR as does normal PV flow 63
64 HELPFUL HINTS WITH SECONDARY MR Can be more challenging to grade LV forward SV is often low, therefore RV may be lower than in primary MR Regurgitant orifice is often not circular, therefore VCW and PISA assumptions may not apply (may underestimate severity) Blunted systolic PV flow may reflect elevated LV filling pressures and not significant MR More dynamic than primary MR 64

65 SENDING THE PATIENT TO US 65 JACC Nov 2017
66 Sending Us the Patient for Evaluation Having the imaging data prior to initial evaluation is helpful How to get us the information We often repeat evaluations (and may come up with different assessments) MR can be very dynamic Quantitative measures often override the qualitative assessment Many of our trials require quantitative information or specific information about the LA, MV and atrial septal anatomy 66
67 MITRAL REGURGITATION SUMMARY Defining the mechanism and type of MR is critical in the evaluation and management of the MR patient Assessment of the severity of MR requires an integrative approach and should incorporate qualitative, semi-quantitative and quantitative methods Color jet area alone should NOT be used Echo reports should provide a comprehensive evaluation of the MV anatomy and degree of MR 67 Clinical decision making requires a multi-disciplinary approach to management

68 ACCURATE ASSESSMENT OF THE MECHANISM AND SEVERITY OF MITRAL REGURGITATION IS ESSENTIAL IN DECISION MAKING 68 All Echo parameters have strengths and weaknesses No one parameter should be used An integrative approach is required USE ALL OF THE AVAILABLE DATA TO ASSESS MITRAL REGURGITATION
69 69 THANK YOU
MITRAL REGURGITATION ECHO PARAMETERS TOOL
 Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo
 Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo define the mechanism, quantify the regurgitation severity CP1293058-3
Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo define the mechanism, quantify the regurgitation severity CP1293058-3
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas
 Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Imaging MV. Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015
 Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
MR echo case. N.Koutsogiannis Department of Cardiology University Hospital Of Patras
 MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
What Degree of MR Deserves Surgical or Transcatheter Intervention, and How Should It Be Assessed?
 What Degree of MR Deserves Surgical or Transcatheter Intervention, and How Should It Be Assessed? Robert J. Siegel, M.D., FACC Nov. 14-15, 2017, Beverly Hills Director, Cardiac Non-Invasive Laboratory
What Degree of MR Deserves Surgical or Transcatheter Intervention, and How Should It Be Assessed? Robert J. Siegel, M.D., FACC Nov. 14-15, 2017, Beverly Hills Director, Cardiac Non-Invasive Laboratory
Regurgitant Lesions. Bicol Hospital, Legazpi City, Philippines July Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA
 Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
New 3D Quantification of Mitral Regurgitation Severity. Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA
 New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Prof. JL Zamorano Hospital Universitario Ramón y Cajal
 Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Blank DISCLOSURES 1/17/2017 COMPLEX VALVE CASES CHALLENGES IN EVALUATING AND MANAGING MULTIVALVULAR HEART DISEASE ECHO HAWAII 1/23/17 NONE
 Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens
 MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
Quantitation of Aortic Regurgitation ASCeXAM / ReASCE Review Course
 Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Management of TR in Patients Undergoing Mitral Interventions
 Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Valve Analysis and Pathoanatomy: THE MITRAL VALVE
 : THE MITRAL VALVE Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Washington University School of Medicine, St. Louis, MO Secretary, American Association for Thoracic Surgery
: THE MITRAL VALVE Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Washington University School of Medicine, St. Louis, MO Secretary, American Association for Thoracic Surgery
When should we intervene surgically in pediatric patient with MR?
 When should we intervene surgically in pediatric patient with MR? DR.SAUD A. BAHAIDARAH CONSULTANT, PEDIATRIC CARDIOLOGY ASSISTANT PROFESSOR OF PEDIATRICS HEAD OF CARDIOLOGY AND CARDIAC SURGERY UNIT KAUH
When should we intervene surgically in pediatric patient with MR? DR.SAUD A. BAHAIDARAH CONSULTANT, PEDIATRIC CARDIOLOGY ASSISTANT PROFESSOR OF PEDIATRICS HEAD OF CARDIOLOGY AND CARDIAC SURGERY UNIT KAUH
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Quantification of MR
 Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
PISA Evaluation of Mitral Regurgitation. Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011
 PISA Evaluation of Mitral Regurgitation Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011 Introduction Evaluation of MR. What is PISA? Physiologic basis Issues
PISA Evaluation of Mitral Regurgitation Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011 Introduction Evaluation of MR. What is PISA? Physiologic basis Issues
Guidelines in perspective?
 EuroValve 2016 Challenges in the management Secondary MR Guidelines in perspective? Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology, Liège, Belgium Heart Valve Clinic,
EuroValve 2016 Challenges in the management Secondary MR Guidelines in perspective? Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology, Liège, Belgium Heart Valve Clinic,
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The difficult patient with mitral regurgitation
 Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Mitral Regurgitation
 Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
Echo in Asymptomatic Mitral and Aortic Regurgitation
 2017 ASE Florida Orlando, FL October 9, 2017 10:40 11:00 PM 20 min Grand Harbor Ballroom South Echo in Asymptomatic Mitral and Aortic Regurgitation Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology
2017 ASE Florida Orlando, FL October 9, 2017 10:40 11:00 PM 20 min Grand Harbor Ballroom South Echo in Asymptomatic Mitral and Aortic Regurgitation Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Functional Mitral Regurgitation
 Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Index. B B-type natriuretic peptide (BNP), 76
, 76") Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Direct Planimetry of Mitral Valve Regurgitation Orifice Area by Real-time 3D Transesophageal Echocardiography
 Direct Planimetry of Mitral Valve Regurgitation Orifice Area by Real-time 3D Transesophageal Echocardiography Ertunc Altiok, Sandra Hamada, Silke van Hall, Mehtap Hanenberg, Eva Grabskaya, Michael Becker,
Direct Planimetry of Mitral Valve Regurgitation Orifice Area by Real-time 3D Transesophageal Echocardiography Ertunc Altiok, Sandra Hamada, Silke van Hall, Mehtap Hanenberg, Eva Grabskaya, Michael Becker,
Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας
 Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας Μυτάς Δημήτρης MD, PhD Επιμ Α ΕΣΥ Σισμανόγλειο Γενικό Νοσοκομείο Αττικής Δηλώνω υπεύθυνα ότι η παρούσα ομιλία δεν επιχορηγείται
Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας Μυτάς Δημήτρης MD, PhD Επιμ Α ΕΣΥ Σισμανόγλειο Γενικό Νοσοκομείο Αττικής Δηλώνω υπεύθυνα ότι η παρούσα ομιλία δεν επιχορηγείται
CHAPTER 4 AN EFFICACIOUS APPROACH FOR THE QUANTIFICATION OF MITRAL REGURGITATION USING IMAGE PROCESSING AND PROXIMAL FLOW CONVERGENCE METHOD
 CHAPTER 4 AN EFFICACIOUS APPROACH FOR THE QUANTIFICATION OF MITRAL REGURGITATION USING IMAGE PROCESSING AND PROXIMAL FLOW CONVERGENCE METHOD 4.1. Introduction Mitral Regurgitation also called Mitral Insufficiency
CHAPTER 4 AN EFFICACIOUS APPROACH FOR THE QUANTIFICATION OF MITRAL REGURGITATION USING IMAGE PROCESSING AND PROXIMAL FLOW CONVERGENCE METHOD 4.1. Introduction Mitral Regurgitation also called Mitral Insufficiency
NEW GUIDELINES. A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee
 NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
When Does 3D Echo Make A Difference?
 When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
Echocardiography. Guidelines for Valve and Chamber Quantification. In partnership with
 Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
School, The University of Texas Health Science Center at Houston, TX.
 Chapter 4: Basics of echocardiography for transcatheter interventions Adrian DaSilva-DeAbreu, MD 1, Catalin Loghin, MD 2 1 Resident, Department of Internal Medicine, McGovern Medical School, The University
Chapter 4: Basics of echocardiography for transcatheter interventions Adrian DaSilva-DeAbreu, MD 1, Catalin Loghin, MD 2 1 Resident, Department of Internal Medicine, McGovern Medical School, The University
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Back to Basics: Common Errors In Quantitation In Everyday Practice
 Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Titel Kardiologie-SG.ch hot topics in heart failure and mitral regurgitation
 Titel Kardiologie-SG.ch hot topics in heart failure and mitral regurgitation where and how to quantify mitral regurgitation: Echolab, Cathlab or MRI? Philipp K. Haager, St. Gallen Measuring mitral regurgitation?
Titel Kardiologie-SG.ch hot topics in heart failure and mitral regurgitation where and how to quantify mitral regurgitation: Echolab, Cathlab or MRI? Philipp K. Haager, St. Gallen Measuring mitral regurgitation?
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification. Rheumatic Mitral Stenosis 76yo male
 MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Secondary MR joint with the mitral academy. What is new in our understanding of this disease? Luc Pierard University Hospital, Liège
 Secondary MR joint with the mitral academy What is new in our understanding of this disease? Luc Pierard University Hospital, Liège Faculty disclosure Luc Pierard I have no financial relationships to disclose.
Secondary MR joint with the mitral academy What is new in our understanding of this disease? Luc Pierard University Hospital, Liège Faculty disclosure Luc Pierard I have no financial relationships to disclose.
Objectives. Considerations in management of multivalvular disease. Case Discussions. A Systematic Approach to Multivalve Disease.
 A Systematic Approach to Multivalve Disease James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
A Systematic Approach to Multivalve Disease James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Echocardiography: Guidelines for Valve Quantification
 Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Percutaneous Mitral Valve Repair
 Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Organic mitral regurgitation
 The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
PARAVALVULAR LEAK POST TAVR. Elements of Follow-up Post TAVR
 PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
ΓΙΩΡΓΟΣ ΜΑΚΑΒΟΣ, MD, PhD ΚΑΡΔΙΟΛΟΓΟΣ, ΕΠΙΜΕΛΗΤΗΣ Β Γ ΠΑΝΕΠΙΣΤΗΜΙΑΚΗ ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ Γ.Ν.Ν.Θ.Α. ΣΩΤΗΡΙΑ
 ΓΙΩΡΓΟΣ ΜΑΚΑΒΟΣ, MD, PhD ΚΑΡΔΙΟΛΟΓΟΣ, ΕΠΙΜΕΛΗΤΗΣ Β Γ ΠΑΝΕΠΙΣΤΗΜΙΑΚΗ ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ Γ.Ν.Ν.Θ.Α. ΣΩΤΗΡΙΑ Causes of TR Primary-Organic Secondary-Functional Rheumatic LV,valvular dysfunction I.Endocarditis
ΓΙΩΡΓΟΣ ΜΑΚΑΒΟΣ, MD, PhD ΚΑΡΔΙΟΛΟΓΟΣ, ΕΠΙΜΕΛΗΤΗΣ Β Γ ΠΑΝΕΠΙΣΤΗΜΙΑΚΗ ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ Γ.Ν.Ν.Θ.Α. ΣΩΤΗΡΙΑ Causes of TR Primary-Organic Secondary-Functional Rheumatic LV,valvular dysfunction I.Endocarditis
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας
 Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
Echocardiographic Evaluation of Mitral Valve Prostheses
 Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Disclosure Statement of Financial Interest Saibal Kar, MD, FACC
 MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
Aortic Regurgitation & Aorta Evaluation
 VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
Ischemic Mitral Regurgitation
 Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Diastolic Function: What the Sonographer Needs to Know. Echocardiographic Assessment of Diastolic Function: Basic Concepts 2/8/2012
 Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
GENERAL PRINCIPLES FOR ECHO ASSESSMENT OF DIASTOLIC FUNCTION (For full recommendation refer to the Left Ventricular Diastolic Function Guideline)
") 1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
Quantifying Aortic Regurgitation
 Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management
 Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
CHAPTER 5 EFFICIENT APPROACHES FOR QUANTIFICATION OF AORTIC REGURGITATION USING PROXIMAL ISOVELOCITY SURFACE AREA PROCESS
 CHAPTER 5 EFFICIENT APPROACHES FOR QUANTIFICATION OF AORTIC REGURGITATION USING PROXIMAL ISOVELOCITY SURFACE AREA PROCESS 5.1. Introduction Aortic Regurgitation is also known as Aortic Insufficiency (AI).
CHAPTER 5 EFFICIENT APPROACHES FOR QUANTIFICATION OF AORTIC REGURGITATION USING PROXIMAL ISOVELOCITY SURFACE AREA PROCESS 5.1. Introduction Aortic Regurgitation is also known as Aortic Insufficiency (AI).
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL
 PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis
 JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine
 Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the