Aortic Regurgitation & Aorta Evaluation
|
|
|
- Prosper Tyrone Robertson
- 5 years ago
- Views:
Transcription


1


2 VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología Ignacio Chávez Mexico City. No disclosure.



3 Aortic Regurgitation Painting the history of cardiology: The clinical concept Murales del Instituto Nacional de Cardiología Ignacio Chávez Pintados por Diego Rivera.

4 Causes of Aortic Regurgitation
5 Stage of Chronic Aortic Regurgitation Stage Definition Valve Anatomy Valve Hemodynamics A At risk of AR Bicuspid aortic valve AR severity (or other congenital none or trace valve anomaly) Aortic valve sclerosis Diseases of the aortic sinuses or ascending aorta History of rheumatic fever or known rheumatic heart disease IE Hemodynamic Consequences None Symptoms None 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.

6 Pathophysiology of AR Volume overload compensatory mechanisms LV EDV increases without increase in diastolic presure (due to increased compliance) LV preload reserve is maintained initially Eccentric hypertrophy Increased afterload Increased chamber volume Increased systolic wall stress and afterload Concentric LVH Continued increase in chamber volume and afterload Descompensation Afterload mismatch (reversible) Impaired LV contractility (irreversible)
7 Stage of Chronic Aortic Regurgitation Stage Definition Valve Anatomy Valve Hemodynamics Hemodynamic Consequences B Progressive AR Mild-tomoderate calcification of a trileaflet valve bicuspid aortic valve (or other congenital valve anomaly) Dilated aortic sinuses Rheumatic valve changes Previous IE Mild AR: o Jet width <25% of LVOT o Vena contracta <0.3 cm o RVol <30 ml/beat o RF <30% o ERO <0.10 cm 2 o Angiography grade 1+ Moderate AR: o Jet width 25% 64% of LVOT o Vena contracta cm o RVol ml/beat o RF 30% 49% o ERO cm 2 o Angiography grade AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Normal LV systolic function Normal LV volume or mild LV dilation Symptoms None
8 Stage of Chronic Aortic Regurgitation Stage Definition Valve Anatomy Valve Hemodynamics Hemodynamic Consequences C Asymptomatic severe AR Calcific aortic valve disease Bicuspid valve (or other congenital abnormality) Dilated aortic sinuses or ascending aorta Rheumatic valve changes IE with abnormal leaflet closure or perforation Severe AR: o Jet width 65% of LVOT o Vena contracta >0.6 cm o Holodiastolic flow reversal in the proximal abdominal aorta o RVol 60 ml/beat o RF 50% o ERO 0.3 cm 2 o Angiography grade 3+ to 4+ o In addition, diagnosis of chronic severe AR requires evidence of LV dilation C1: Normal LVEF ( 50%) and mild-tomoderate LV dilation (LVESD 50 mm) C2: Abnormal LV systolic function with depressed LVEF (<50%) or severe LV dilatation (LVESD >50 mm or indexed LVESD >25 mm/m 2 ) Symptoms None; exercise testing is reasonable to confirm symptom status 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.
9 Stage of Chronic Aortic Regurgitation Stage Definition Valve Anatomy Valve Hemodynamics Hemodynamic Consequences D Symptomatic Calcific valve Severe AR: Symptomatic severe AR disease o Doppler jet width severe AR may Bicuspid valve 65% of LVOT; occur with normal (or other o Vena contracta >0.6 systolic function congenital cm, (LVEF 50%), abnormality) o Holodiastolic flow mild-to-moderate Dilated aortic reversal in the LV dysfunction sinuses or proximal abdominal (LVEF 40% to ascending aorta, 50%) or severe LV aorta o RVol 60 ml/beat; dysfunction (LVEF Rheumatic o RF 50%; <40%); valve changes o ERO 0.3 cm 2 ; Moderate-tosevere Previous IE o Angiography grade LV dilation with abnormal 3+ to 4+ is present. leaflet closure o In addition, diagnosis or perforation of chronic severe AR requires evidence of LV dilation Symptoms Exertional dyspnea or angina, or more severe HF symptoms 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.






10 AR Complete assessment Tubular Ascending Aorta Sinotubular Junction Sinuses of Valsalva Aortic Annulus 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.

11 Evaluation of Acute AR The sensivity and specifity of TTE for diagnosis of aortic dissection are only 60-80%, whereas TEE has a sensitivity of 98% to 100% and a specificity of 95% to 100%. CT imaging is very accurate, rapid approach to diagnosis at many centers. CMR imaging is rarely used in unstable patients with suspected disection. Angiography should be considered only when the diagnosis cannot be determined by noinvasive imaging and when patients have supected or known CAD, specially those with previous CABG

12 AR Diagnosis & follow up Recommendations COR LOE TTE is indicated in patients with signs or symptoms of AR (stages A to D) for accurate diagnosis of the cause of regurgitation, regurgitant severity, and LV size and systolic function, and for determining clinical outcome and timing of valve intervention I B TTE is indicated in patients with dilated aortic sinuses or ascending aorta or with a bicuspid aortic valve (stages A and B) to evaluate the presence and severity of AR I B 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.





13 AR, Echo evaluation. TTE is recommended as the first-line imaging modality in valvular regurgitation. TEE is advocated when TTE is of nondiagnostic value or when further diagnostic refinement is required. 3D TEE or TTE is reasonable to provide additional information in patients with complex valve lesion. TEE is not indicated in patients with a goodquality TTE except in the operating room when a valve surgery is performed.

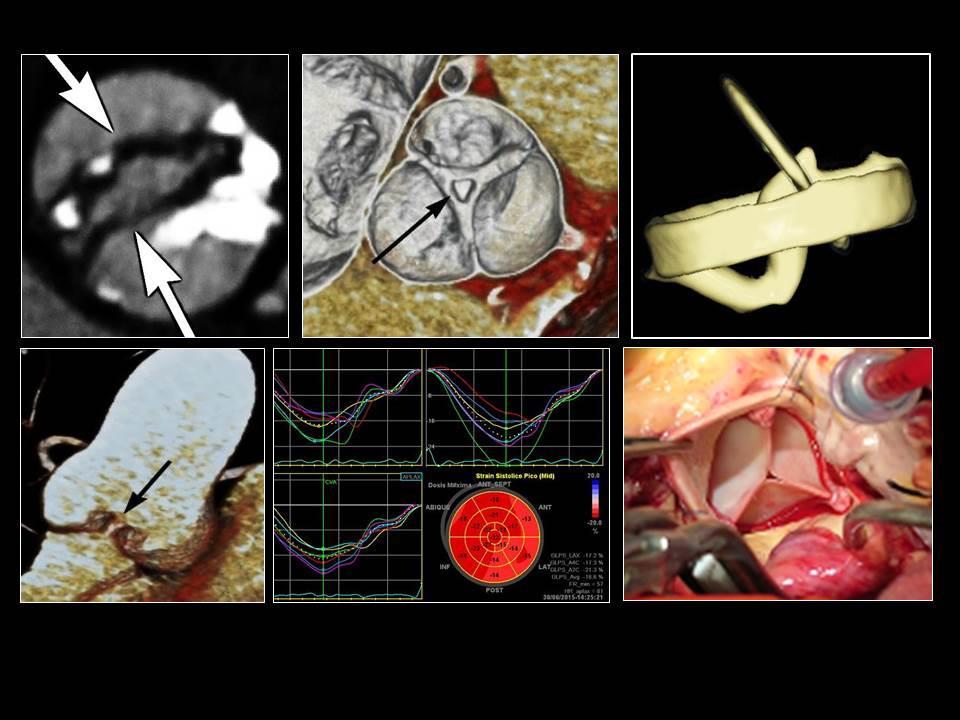
14 AR, Echocardiogram In patients with AR, careful aortic valve analysis is mandatory. The echo report should include information about the aetiology, the lesion process, and the type of dysfunction. Additional echo findings are used as complementary findings to assess the severity of AR. The assessment of the morphology and dimension of the aortic root is mandatory. Mechanisms of aortic regurgitation according to the Capentier functional classification. Type I, aortic annulus dilatation; Type IIa, prolapse of the left coronary cusp (arrow); Type III, rheumatic aortic valve disease with restricted cusp motion.
15 Chronic AR Diagnosis & follow up Recommendations COR LOE CMR is indicated in patients with moderate or severe AR (stages B, C, and D) and suboptimal echocardiographic images for the assessment of LV systolic function, systolic and diastolic volumes, and measurement of AR severity I B 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.



16 Aortic Regurgitation: CRM 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Heart 2014; 100: Dra. Gabriela Melèndez Resonancia Magnética. Instituto Nacional de Cardiología Ignacio Chàvez.
17 Evaluation of Coronary Anatomy Recommendations COR LOE Coronary angiography is indicated before valve intervention in patients with symptoms of angina, objective evidence of ischemia, decreased LV systolic function, history of CAD, or coronary risk factors (including men age >40 years and postmenopausal women) I C Coronary angiography should be performed as part of the evaluation of patients with chronic severe secondary MR I C
18 Biscuspid Aortic Valve & Aortopathy Recommendations Diagnosis & follow up COR LOE An initial TTE is indicated in patients with a known bicuspid aortic valve to evaluate valve morphology, to measure the severity of AS and AR, and to assess the of the aortic shape and diameter sinuses and ascending I B aorta for prediction of clinical outcome and to determine timing of intervention Aortic magnetic resonance angiography or CT angiography is indicated in patients with a bicuspid aortic valve when morphology of the aortic sinuses, sinotubular junction, or ascending aorta cannot be assessed accurately or fully by echocardiography I C 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.
19 Biscuspid Aortic Valve & Aortopathy Recommendations Diagnosis & follow up COR LOE Serial evaluation of the size and morphology of the aortic sinuses and ascending aorta by echocardiography, CMR, or CT angiography is recommended in patients with a bicuspid aortic valve and an aortic diameter greater than 4.0 cm, with the examination interval determined by the degree and rate of progression of aortic dilation and by family history. In patients with an aortic diameter greater than 4.5 cm, this evaluation should be performed annually I C 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.







20 Aorta Bivalva: Computed Tomography NO correlation between the degree of valvular dysfunction and degree of aortic dilatation. Different phenotypes different etiologies A genetic study is suggested J Am Coll Cardiol Img 2013:6:
21 Biscuspid Aortic Valve & Aortopathy Recommendations: Intervention COR LOE Operative intervention to repair the aortic sinuses or replace the ascending aorta is indicated in patients with a bicuspid aortic valve if the diameter of the aortic sinuses or ascending aorta is greater than 5.5 cm I B Operative intervention to repair the aortic sinuses or replace the ascending aorta is reasonable in patients with bicuspid aortic valves if the diameter of the aortic sinuses or ascending aorta is greater than 5.0 cm and a risk factor for dissection is present (family history of aortic dissection or if the rate of increase in diameter is 0.5 cm per year) IIa C 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.
 if the diameter of the ascending aorta is greater than 4.")
22 Biscuspid Aortic Valve & Aortopathy Recommendations: Intervention COR LOE Replacement of the ascending aorta is reasonable in patients with a bicuspid aortic valve who are undergoing aortic valve surgery because of severe AS or AR (Sections 3.4 and 4.4) if the diameter of the ascending aorta is greater than 4.5 cm IIa C 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.
23 CONCLUSIONS AR, is one of the clinical entities with more variety of clinical signs in physical examination. Evaluation of the aortic complex : Aortic valve, aorta and myocardial function. In patients with AR, careful aortic valve analysis by ECHO is mandatory. Valve analysis should integrate the assessment of the aetiology, the lesion process, and the type of dysfunction. It is a good guide to the timing of surgery. This should be considered when LV deterioration starts to occur. CMR is indicated in patients with moderate or severe AR and suboptimal echocardiographic images for the assessment of LV systolic function, systolic and diastolic volumes, and measurement of AR severity (Class I) CT is excellent option to evaluate bicuspid aortic valve and Aortopathy. There is not correlation between the degree of valvular dysfunction and degree of aortic dilatation.

24 Aortic Regurgitation Aorta Evaluation Thank you
Regurgitant Lesions. Bicol Hospital, Legazpi City, Philippines July Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA
 Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
NEW GUIDELINES. A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee
 NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
Quantitation of Aortic Regurgitation ASCeXAM / ReASCE Review Course
 Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient
 Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Regurgitation and Aortic Aneurysm - Epidemiology and Guidelines -
 Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Multi-imaging modality approach. Covadonga Fernández-Golfín Cardiac Imaging Unit. Cardiology Department. Ramón y Cajal Hospital.
 Multi-imaging modality approach Covadonga Fernández-Golfín Cardiac Imaging Unit. Cardiology Department. Ramón y Cajal Hospital.Madrid Faculty Disclosure Covadonga Fernández-Golfín I have no financial relationships
Multi-imaging modality approach Covadonga Fernández-Golfín Cardiac Imaging Unit. Cardiology Department. Ramón y Cajal Hospital.Madrid Faculty Disclosure Covadonga Fernández-Golfín I have no financial relationships
Which one of the following echocardiographic profiles most strongly indicates the need for aortic valve replacement? FS [
 Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Timing for surgery in asymptomatic aortic valvular diseases a matter of controversy
 Mædica - a Journal of Clinical Medicine STATE TE-OF OF-THE THE-AR ART Timing for surgery in asymptomatic aortic valvular diseases a matter of controversy Roxana Cristina SISU MD, Fellow in cardiology;
Mædica - a Journal of Clinical Medicine STATE TE-OF OF-THE THE-AR ART Timing for surgery in asymptomatic aortic valvular diseases a matter of controversy Roxana Cristina SISU MD, Fellow in cardiology;
Mixed aortic valve disease
 Mixed aortic valve disease IOANNIS NTALAS MD, PhD Cardiologist, Clinical Fellow in Cardiovascular Imaging & Non-Invasive Cardiology, St Thomas Hospital School of Biomedical Engineering & Imaging Sciences
Mixed aortic valve disease IOANNIS NTALAS MD, PhD Cardiologist, Clinical Fellow in Cardiovascular Imaging & Non-Invasive Cardiology, St Thomas Hospital School of Biomedical Engineering & Imaging Sciences
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Introduction RECOMMENDATIONS
 European Journal of Echocardiography (2010) 11, 223 244 doi:10.1093/ejechocard/jeq030 RECOMMENDATIONS European Association of Echocardiography recommendations for the assessment of valvular regurgitation.
European Journal of Echocardiography (2010) 11, 223 244 doi:10.1093/ejechocard/jeq030 RECOMMENDATIONS European Association of Echocardiography recommendations for the assessment of valvular regurgitation.
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Corrective Surgery in Severe Heart Failure. Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio
 Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
PARAVALVULAR LEAK POST TAVR. Elements of Follow-up Post TAVR
 PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
Unusual Causes of Aortic Regurgitation. Case 1
 Unusual Causes of Aortic Regurgitation Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA No Disclosures Case 1 54 year old female with h/o cerebral aneurysm and vascular malformation
Unusual Causes of Aortic Regurgitation Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA No Disclosures Case 1 54 year old female with h/o cerebral aneurysm and vascular malformation
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Aortic regurgitation. Physiopathology. Dr Pilar Tornos Hospital Vall d Hebron. Barcelona Eurovalve 2014
 Aortic regurgitation. Physiopathology Dr Pilar Tornos Hospital Vall d Hebron. Barcelona Eurovalve 2014 Faculty disclosure Pilar Tornos I have no financial relationships to disclose. Acute AR Etiology:
Aortic regurgitation. Physiopathology Dr Pilar Tornos Hospital Vall d Hebron. Barcelona Eurovalve 2014 Faculty disclosure Pilar Tornos I have no financial relationships to disclose. Acute AR Etiology:
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
Rotation: Echocardiography: Transthoracic Echocardiography (TTE)
") Rotation: Echocardiography: Transthoracic Echocardiography (TTE) Rotation Format and Responsibilities: Fellows rotate in the echocardiography laboratory in each clinical year. Rotations during the first
Rotation: Echocardiography: Transthoracic Echocardiography (TTE) Rotation Format and Responsibilities: Fellows rotate in the echocardiography laboratory in each clinical year. Rotations during the first
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo
 Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo define the mechanism, quantify the regurgitation severity CP1293058-3
Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo define the mechanism, quantify the regurgitation severity CP1293058-3
Original Date: October 2009 TRANSESOPHAGEAL (TEE) ECHO Page 1 of 6
 ECHO Page 1 of 6") National Imaging Associates, Inc. Clinical guideline Original Date: October 2009 TRANSESOPHAGEAL (TEE) ECHO Page 1 of 6 CPT codes: 93312, 93313, 93314, 93315, Last Review Date: September 2017 93316, 93317,
National Imaging Associates, Inc. Clinical guideline Original Date: October 2009 TRANSESOPHAGEAL (TEE) ECHO Page 1 of 6 CPT codes: 93312, 93313, 93314, 93315, Last Review Date: September 2017 93316, 93317,
Surgical indications in ascending aorta aneurysms: What do we know? Jean-Luc MONIN, MD, PhD. Institut Mutualiste Montsouris, Paris, FRANCE
 Surgical indications in ascending aorta aneurysms: What do we know? Jean-Luc MONIN, MD, PhD. Institut Mutualiste Montsouris, Paris, FRANCE Disclosures related to this talk : NONE 2 Clinical case A 40 year-old
Surgical indications in ascending aorta aneurysms: What do we know? Jean-Luc MONIN, MD, PhD. Institut Mutualiste Montsouris, Paris, FRANCE Disclosures related to this talk : NONE 2 Clinical case A 40 year-old
Learn and LiveSM. ACC/AHA Pocket Guideline. Based on the ACC/AHA 2006 Guideline Revision. Management of Patients With. Valvular Heart Disease
 Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2006 Guideline Revision Management of Patients With Valvular Heart Disease June 2006 Special thanks to Distributed through support from Medtronic
Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2006 Guideline Revision Management of Patients With Valvular Heart Disease June 2006 Special thanks to Distributed through support from Medtronic
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Comments restricted to Sapien and Corevalve 9/12/2016. Disclosures: Core Lab contracts with Edwards Lifesciences, Middlepeak, Medtronic
 Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Aortic valve disease. Acknowledgement for slides. Heart Valves 4/28/2018. Adopted from
 Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Transoesophageal echocardiography and decision making in valve surgery
 Transoesophageal echocardiography and decision making in valve surgery Intraoperative evaluation of the surgical results in aortic valve / root surgery Catherine Szymanski Disclosures None Sino-tubular
Transoesophageal echocardiography and decision making in valve surgery Intraoperative evaluation of the surgical results in aortic valve / root surgery Catherine Szymanski Disclosures None Sino-tubular
SURGICAL INTERVENTION IN AORTOPATHIES ZOHAIR ALHALEES, MD RIYADH, SAUDI ARABIA
 SURGICAL INTERVENTION IN AORTOPATHIES ZOHAIR ALHALEES, MD RIYADH, SAUDI ARABIA In patients born with CHD, dilatation of the aorta is a frequent feature at presentation and during follow up after surgical
SURGICAL INTERVENTION IN AORTOPATHIES ZOHAIR ALHALEES, MD RIYADH, SAUDI ARABIA In patients born with CHD, dilatation of the aorta is a frequent feature at presentation and during follow up after surgical
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
G. AORTIC STENOSIS (AS)
") G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Echo in Asymptomatic Mitral and Aortic Regurgitation
 2017 ASE Florida Orlando, FL October 9, 2017 10:40 11:00 PM 20 min Grand Harbor Ballroom South Echo in Asymptomatic Mitral and Aortic Regurgitation Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology
2017 ASE Florida Orlando, FL October 9, 2017 10:40 11:00 PM 20 min Grand Harbor Ballroom South Echo in Asymptomatic Mitral and Aortic Regurgitation Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Imaging MV. Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015
 Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences
 S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
What s New in Cardiac MRI
 What s New in Cardiac MRI Katie M. Hawthorne, MD Director, Cardiac MRI Main Line Health Philadelphia Cardiovascular Summit November 18, 2017 Cardiac MRI: Disclosure 2 Disclosures No financial disclosures
What s New in Cardiac MRI Katie M. Hawthorne, MD Director, Cardiac MRI Main Line Health Philadelphia Cardiovascular Summit November 18, 2017 Cardiac MRI: Disclosure 2 Disclosures No financial disclosures
Echo Assessment Pre-TAVI
 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
MITRAL REGURGITATION ECHO PARAMETERS TOOL
 Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Diseases of the Aorta
 Diseases of the Aorta ASE Review 2018 Susan E Wiegers, MD, FASE, FACC Professor of Medicine My great friend Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives Aneurysm Dissection
Diseases of the Aorta ASE Review 2018 Susan E Wiegers, MD, FASE, FACC Professor of Medicine My great friend Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives Aneurysm Dissection
New ASE Guidelines: What you must know
 New ASE Guidelines: What you must know Federico M Asch MD, FASE, FACC Chair, ASE Guidelines and Standards Committee Medstar Washington Hospital Center Medstar Health Research Institute Georgetown University
New ASE Guidelines: What you must know Federico M Asch MD, FASE, FACC Chair, ASE Guidelines and Standards Committee Medstar Washington Hospital Center Medstar Health Research Institute Georgetown University
Aortic root reconstructive surgery - new created technique for aortic stenosis
 Aortic root reconstructive surgery - new created technique for aortic stenosis Reconstructive surgery of the aortic root Academician d-r Zan Mitrev, T.Anguseva, E.Stoicovski, E Idoski Special hospital
Aortic root reconstructive surgery - new created technique for aortic stenosis Reconstructive surgery of the aortic root Academician d-r Zan Mitrev, T.Anguseva, E.Stoicovski, E Idoski Special hospital
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
MR echo case. N.Koutsogiannis Department of Cardiology University Hospital Of Patras
 MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
ASE 2011 Appropriate Use Criteria for Echocardiography
 ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
HIGHLIGHT SESSION. Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips
 Disclosures: Speaker Philips") Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Aortic regurgitation and aneurysm. epidemiology and guidelines
 Reconstruction of the Aortic Valve and Root A practical approach Aortic regurgitation and aneurysm epidemiology and guidelines Sebastian Ewen Klinik für Innere Medizin III Kardiologie, Angiologie und Internistische
Reconstruction of the Aortic Valve and Root A practical approach Aortic regurgitation and aneurysm epidemiology and guidelines Sebastian Ewen Klinik für Innere Medizin III Kardiologie, Angiologie und Internistische
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Cardiac catheterisation in AS
 AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Management of TR in Patients Undergoing Mitral Interventions
 Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
A Health Care Professional s Guide Aortic Stenosis in Seniors
 A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
Prof. JL Zamorano Hospital Universitario Ramón y Cajal
 Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Policy #: 222 Latest Review Date: March 2009
 Name of Policy: MRI Phase-Contrast Flow Measurement Policy #: 222 Latest Review Date: March 2009 Category: Radiology Policy Grade: Active Policy but no longer scheduled for regular literature reviews and
Name of Policy: MRI Phase-Contrast Flow Measurement Policy #: 222 Latest Review Date: March 2009 Category: Radiology Policy Grade: Active Policy but no longer scheduled for regular literature reviews and
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD. UCL -Cliniques Saint Luc
 New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
Disclosures Nothing to disclose
 Aortic Valve Disease Illustrative Cases December 8, 2009 David Stultz, MD, FACC Southwest Cardiology, Inc Handout available at http://www.drstultz.com Disclosures Nothing to disclose Objectives Understand
Aortic Valve Disease Illustrative Cases December 8, 2009 David Stultz, MD, FACC Southwest Cardiology, Inc Handout available at http://www.drstultz.com Disclosures Nothing to disclose Objectives Understand
ESC/EACTS Guidelines for the Management of Valvular Heart Disease
 ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
The Role of Imaging in Transcatheter Aortic Valve Implantation
 The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Transthoracic Echocardiography in Adults
 Medical Coverage Policy Effective Date...02/15/2018 Next Review Date...02/15/2019 Coverage Policy Number... 0510 Transthoracic Echocardiography in Adults Table of Contents Related Coverage Resources Coverage
Medical Coverage Policy Effective Date...02/15/2018 Next Review Date...02/15/2019 Coverage Policy Number... 0510 Transthoracic Echocardiography in Adults Table of Contents Related Coverage Resources Coverage
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine
 Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid