Acute Respiratory Distress Syndrome
|
|
|
- Dustin Sharp
- 5 years ago
- Views:
Transcription
1 Acute Respiratory Distress Syndrome
2 ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications

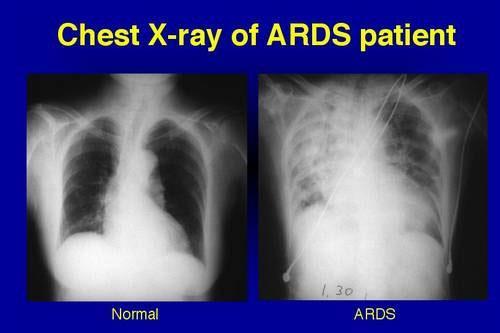
3 Clinical Manifestations Related to systemic inflammatory disease Bilateral pulmonary infiltration Increased pulmonary capillary permeability Decreased PaO2/FiO2 ratio
4 Severity Stages New classification system Better predictor of mortality Three classifications: Mild PaO2/FiO2 <300 mmhg Acute lung injury Moderate <200 mmhg Severe <100 mmhg 75% of cases are classified moderate or severe
5 Incidence 9% incidence of ARDS and ALL in the ICU United States: 64:100,000 Europe: :100,000 American Lung Association: cases/100,000 individuals 25-40% of cases end in death
6 Increasing Incidence of ARDS cases
7 Life Expectancy Dependent of cause of ARDS Patients with fewer chronic diseases have increased survival Sepsis induced ARDS has increased risk of mortality Pulmonary fibrosis is found to be a major factor 1988: 50-70% mortality 2008: 25-40% mortality Death typically results from MODS from a lack of oxygen rather than lung failure
8 Decreasing mortality risk for ARDS patients
9 Etiology Direct injury: Trauma Aspiration Inhaling Chemicals Obstructed airways Indirect injury Blood transfusion Sepsis Pneumonia
10 Signs and Symptoms Depending on the initial trauma specific S/S can occur Ex. Pneumonia cough Difficulty breathing Two-pillow orthopnea: support from pillows to in order to easy breathing that occurs from the recumbent position Rapid breathing Shortness of Breath Low blood oxygen level


11 S/S continued Trachea shift: trachea shifts from its normal position because of fluid accumulation in the pleural space Jugular distention: jugular veins bulge because of increased central venous pressure Bruit: noise unusual sound blood makes when passing an obstruction Medical professionals will look for bruit sounds to R/O other diseases
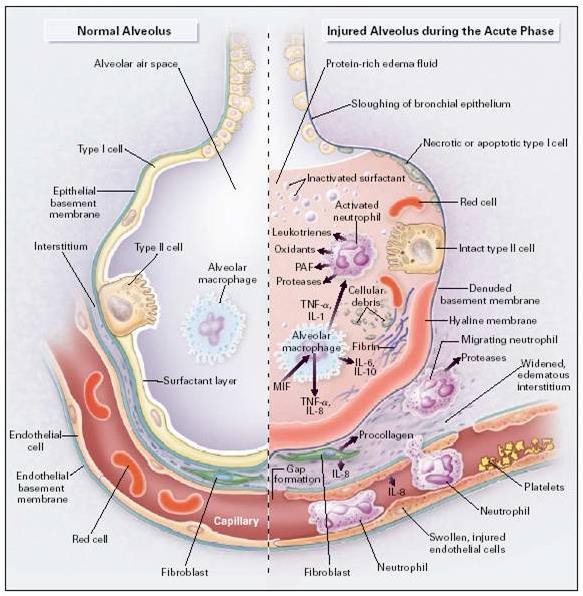
12 Pathophysiology Early phase: exudative (oozing) Occur as a result of direct or indirect lung insults Acute inflammatory stage with proinflammatory cytokines, neutrophils, and overall impaired endothelial cell barrier function Barrier between the capillaries and the alveoli allow water movement into the alveoli Most patients will survive this stage Later phase: fibroproliferative Alveolar damage Collagen deposition appears in 3 days; Fibrosis manifests within 3 weeks Pulmonary fibrosis resulting in 55% of ARDS deaths
13
14
15 Risk Factors Old age Shock Liver failure Patients with diabetes have half the risk for developing ARDS compared to patients without diabetes
16 Quality of Life Poor muscle function Pulmonary function returns to normal or near normal at approx. 6 months Decrease carbon monoxide diffusion capacity Memory loss: due to brain damage from lack of oxygen Fatigue Weakness Alopecia Pain from chest tubes Entrapment Neuropathy Heterotopic Ossification
17 Medical Therapy
18 Diagnosis Challenging because ARDS has nonspecific characteristics 48% of patients with autopsy-prove ARDS had ARDS diagnosis in their charts
19 Rule out other diseases Left heart failure Check left heart function Acute lung injury Less severe impairment of oxygen; PaO2/FiO2 <300 mmhg
20 Goals of Treatment Support breathing Treat underlying cause Medications to treat infections, reduce inflammation, and remove fluid from the lungs.

21 Health Impact 25-40% of cases are fatal By 7-10 days a patient has died or have been weaned off treatment

22 Collapsed Lung Pneumothorax Air escapes from the lung and fills the space outside the lung. Smokers, COPD, asthma, cystic fibrosis, tuberculosis
23 Collapsed Lung Increased Risk Smokers COPD Asthma Cystic fibrosis Tuberculosis Symptoms Sharp chest pain Shortness of breath Bluish color Easy fatigue Rapid heart rate
24 Treatment Small pneumothorax Can go away on its own Large Pneumothorax Chest tube Surgery Pleurodesis

25 Surgery Treat collapsed lung Stop fluid buildup
26 Pulmonary Fibrosis Scarring throughout the lungs

27 Prevention of ARDS No drug has proved beneficial in prevention
28 Corticosteroids High-dose corticosteroids Patients with ARDS persisting for at least 7 days had no benefit in 60 day mortality Patients treated 14 days after onset had worsened mortality with corticosteroid therapy Methylprednisone No survival advantage shown short-term clinical benefits included improved oxygenation and increased ventilator-free and shockfree days more likely to experience neuromuscular weakness, but the rate of infectious complications was not increased.
29 Corticosteroids Summary may be considered a form of rescue therapy may improve oxygenation and hemodynamics does not change mortality corticosteroids increase mortality in patients who have had ARDS for >14 d
30 Statins Somovstatin Preadmission use of statins was associated with a reduction in 30-day and 1-year mortality of a cohort of 12,483 critically ill patients. Patients under statin treatment developing MODS have a better outcome than age- and sex-matched MODS patients without statin therapy.
31
32 TNF and IL-1 Small sepsis trials suggest a potential role for antibody to tumor necrosis factor (TNF) and recombinant interleukin (IL)-1 receptor antagonist.
33 Prostacycline Prostacycline Inhaled prostacycline also has not been shown to improve survival.
34 Nitric Oxide Inhaled nitric oxide did not change mortality rates in adults with ARDS. Improves transient oxygenation
35 Side Effects Short-term Long-term Muscle wasting and weakness


36 Mechanical Ventilation
37
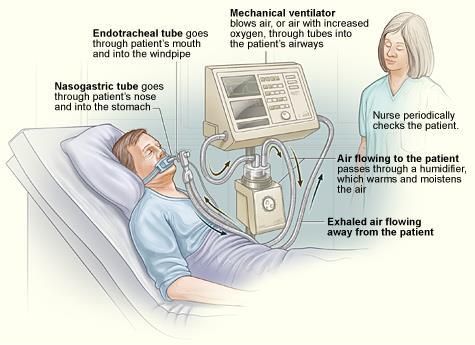
38 Ventilation A ventilator doesn t treat a disease or condition GOAL: provide breathing support, relieve respiratory muscles of their work
39 Ventilation Benefits Get oxygen into the lungs Help people breathe easier relieve respiratory muscles Provide breathing support
40 High vs. Low Tidal Volume High Tidal Volume Over-distend alveoli Worsen lung injury Inflammation Low Tidal Volume Decreased ventilatorassociated lung injury Increases survival rate Recommended to use Low Tidal Volume for ARDS
41 Positive End-Expiratory Pressure (PEEP) Airway pressure is maintained above atmospheric pressure at the end of exhalation Purpose: increase volume of gas remaining in the lungs at the end of expiration Decrease shunting of blood through lungs and improve gas exchange
")
42 Prone Positioning Supine: weight of heart and abdominal organs on lungs contribute to low compliancy Prone: improves oxygenation but does not improve survival Higher incidence of complications (i.e. pressure sores and obstruction of the endotracheal tube)
43 Weaning from Mechanical Ventilation Those who wean successfully have less morbidity and mortality Spontaneous breathing trials (SBTs) Progressive decreases in the level of pressure support during pressure support ventilation
44 The Cochrane Library 8.CD pub4/full Primary outcome Mortality Secondary Outcomes Development of multiple organ failure Duration of mechanical ventilation Stay in ICU Long term health related quality of life Long-term cognitive complications

45 Hemolung RAS CO2 removal and less invasive Similar to dialysis Uses less blood flow Smaller catheter One component system Active mixing Battery operated (patient can move around)
46 Hemolung RAS 2012 Successful pilot studies Arterial pco 2 levels reduced by 28% within 24 hours lessened dyspnea improved clinical status effective and stable CO 2 removal on the order of 50% of metabolic production No unexpected adverse events All patients were able to avoid intubation Still undergoing clinical trials
47 Medical Nutrition Therapy
48 Medical Nutrition Therapy Energy Needs: Calculate with indirect calorimetry (IC) Obese individuals : kcal/kg or 60%-70% of target value Why: High caloric intake increases levels of CO 2.
49 Medical Nutrition Therapy Carbohydrate: Been shown that concentrations of Carbohydrates not as important as calories provided Protein: g/kg Fat: Give enough to provide the right amount of calories
50 Medical Nutrition Therapy What to monitor and watch closely CO 2 Phosphate Vitamin A Vitamin C Vitamin E Meet requirements for Essential Fatty Acids
51 Medical Nutrition Therapy Enteral Nutrition Helps maintain GALT Less likely to overfeed Reduces ICU and hospital mortality Parental Nutrition More likely to overfeed Used for patients with: Shock, Nonfunctional Gut, and Peritonitis
52 Medical Nutrition Therapy Supplementation of Omega 3 over required amounts not effective. Do not use RQ for substrate mix Consider BMI
53 Case Study: DH Anthropometrics Age: 65 Male Married lives with wife (62) 4 children not living in the area Retired manager of local grocery chain Height: 5 4 Weight: 122 lbs BMI: 20.9 UBW: 135 lbs IBW: 130 lbs 8 lbs under
54 Case Study: DH Biochemical Hemoglobin 13.2 (14-17) Hematocrit 39 (40-54) ABG ph 7.2 ( ) ABG pco 2 65 (35-45) ABG CO 2 content 35 (25-30) ABG po 2 56 (>80) ABG HCO 3-38 (24-28) Clinical Extremities: cyanosis, 1+ pitting edema R femoral bruit present Pale skin Harsh inspiratory breath sounds noted over right chest absent sounds on left Use accessory muscles at rest
55 Case Study: DH Dietary General appetite: decreased over past several weeks Usual diet: B: Egg, hot cereal, bread or muffin, hot tea (with milk and sugar) L: soup, sandwich, hot tea (with milk and sugar) D: small amount of meat, rice, 2-3 kinds of vegetables, hot tea (with milk and sugar) History Diagnosed with emphysema more than 10 years ago Tobacco use: 2 PPD for 50 years Alcohol use: 1-2 drinks 1-2 x/week
56 PES Statement Inadequate caloric intake related to increased needs from history of COPD and Acute Respiratory Distress Syndrome as evidenced by decrease appetite and weight loss.

57 Oxepa Abbott Nutrition product for modulating Inflammation in Sepsis, ALI, and ARDS Benefits: Improves oxygenation Decrease time on ventilator Decreases length of stay in ICU For sole-source nutrition
58 Sample Diet Oxepa 25 kcal/kg for 24 hrs 55kg (122lbs) 1375 kcals Protein needs: minimum 82.5 g ( g/kg) Amount Calories (kcal) CHO 97 g Protein 57.3 g Fat 86 g Fluid 917 ml 0 0 Total Calories/24 hours 1412 % in total Calories
MEDICAL NUTRITION THERAPY
 MEDICAL NUTRITION THERAPY Goals of Nutritional Care Meet basic nutrient requirements Preserve LBM Restore respiratory muscle mass and strength Maintain fluid balance Improve resistance to infection Facilitate
MEDICAL NUTRITION THERAPY Goals of Nutritional Care Meet basic nutrient requirements Preserve LBM Restore respiratory muscle mass and strength Maintain fluid balance Improve resistance to infection Facilitate
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
INTRODUCTION. Acute respiratory distress syndrome (ARDS) is a common complication of critical illness
 is a common complication of critical illness") Breanna Keller NDFS 356 Acute Respiratory Distress Syndrome INTRODUCTION Acute respiratory distress syndrome (ARDS) is a common complication of critical illness and results in the sudden failure of the
Breanna Keller NDFS 356 Acute Respiratory Distress Syndrome INTRODUCTION Acute respiratory distress syndrome (ARDS) is a common complication of critical illness and results in the sudden failure of the
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chronic Obstructive Pulmonary. Disease (COPD) Natalie Mariscal Katy Veliz. Nicole Keally. Valerie Ward. Lily Che
 Natalie Mariscal Katy Veliz. Nicole Keally. Valerie Ward. Lily Che") Chronic Obstructive Pulmonary Disease (COPD) Lily Che Nicole Keally Natalie Mariscal Katy Veliz Valerie Ward Patient S.B. is a 62 YO female with Stage 1 COPD who has been admitted to the hospital on January
Chronic Obstructive Pulmonary Disease (COPD) Lily Che Nicole Keally Natalie Mariscal Katy Veliz Valerie Ward Patient S.B. is a 62 YO female with Stage 1 COPD who has been admitted to the hospital on January
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome. By Sydney Hunter. March 6, 2014 NDFS 356
 Acute Respiratory Distress Syndrome By Sydney Hunter March 6, 2014 NDFS 356 1 Introduction The onset of acute respiratory distress syndrome occurs as a result of previous trauma, stress, or shock. It can
Acute Respiratory Distress Syndrome By Sydney Hunter March 6, 2014 NDFS 356 1 Introduction The onset of acute respiratory distress syndrome occurs as a result of previous trauma, stress, or shock. It can
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Nutritional Assessment of the Critically Ill Patient Terry L. Forrette, M.H.S., RRT
 Nutritional Assessment of the Critically Ill Patient Sponsored by GE Healthcare Metabolic Rate How Much Fuel Does the Patient Need? Resting Energy Expenditure Basal Energy Expenditure REE or EE BEE Metabolic
Nutritional Assessment of the Critically Ill Patient Sponsored by GE Healthcare Metabolic Rate How Much Fuel Does the Patient Need? Resting Energy Expenditure Basal Energy Expenditure REE or EE BEE Metabolic
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
EVALUATE DATA IN THE PATIENT RECORD
 EVALUATE DATA IN THE PATIENT RECORD Shawna Strickland, PhD, RRT-NPS, AE-C, FAARC Objectives At the end of this module, the learner will be able to identify the pertinent data from the patient chart for
EVALUATE DATA IN THE PATIENT RECORD Shawna Strickland, PhD, RRT-NPS, AE-C, FAARC Objectives At the end of this module, the learner will be able to identify the pertinent data from the patient chart for
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Anatomy & Physiology 2 Canale. Respiratory System: Exchange of Gases
 Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Chapter 10. The Respiratory System Exchange of Gases. Copyright 2009 Pearson Education, Inc.
 Chapter 10 The Respiratory System Exchange of Gases http://www.encognitive.com/images/respiratory-system.jpg Human Respiratory System UPPER RESPIRATORY TRACT LOWER RESPIRATORY TRACT Nose Passageway for
Chapter 10 The Respiratory System Exchange of Gases http://www.encognitive.com/images/respiratory-system.jpg Human Respiratory System UPPER RESPIRATORY TRACT LOWER RESPIRATORY TRACT Nose Passageway for
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Mechanical ventilation in the emergency department
 Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory System. Chapter 9
 Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Author(s): Frank Madore (Hennepin County Medical Center), MD 2012
: Frank Madore (Hennepin County Medical Center), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Patient Management Code Blue in the CT Suite
 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Asthma Management Introduction, Anatomy and Physiology
 Asthma Management Introduction, Anatomy and Physiology University of Utah Center for Emergency Programs and The Utah Asthma Program Incidence, Impact and Goals of Asthma Management Prevalence, Morbidity
Asthma Management Introduction, Anatomy and Physiology University of Utah Center for Emergency Programs and The Utah Asthma Program Incidence, Impact and Goals of Asthma Management Prevalence, Morbidity
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine
 Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 These
Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 These
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
Indirect Calorimetry and the GE Engstrom Carestation. Jorge E. Rodriguez BSRC, RRT
 Jorge E. Rodriguez BSRC, RRT Indirect tcl Calorimetry and the GE To obtain the most accurate metabolic data from Indirect Calorimetry, one must: Evaluate the patient. Obtain consistent, Steady State data.
Jorge E. Rodriguez BSRC, RRT Indirect tcl Calorimetry and the GE To obtain the most accurate metabolic data from Indirect Calorimetry, one must: Evaluate the patient. Obtain consistent, Steady State data.
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Respiratory System. December 20, 2011
 Respiratory System December 20, 2011 Nasal Cavity: Contains cilia (hair cells) to prevent particles from entering the respiratory tract Mucus does the same, in addition to warming and moistening the air
Respiratory System December 20, 2011 Nasal Cavity: Contains cilia (hair cells) to prevent particles from entering the respiratory tract Mucus does the same, in addition to warming and moistening the air
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Respiratory Physiology Part II. Bio 219 Napa Valley College Dr. Adam Ross
 Respiratory Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Gas exchange Gas exchange in the lungs (to capillaries) occurs by diffusion across respiratory membrane due to differences in partial
Respiratory Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Gas exchange Gas exchange in the lungs (to capillaries) occurs by diffusion across respiratory membrane due to differences in partial
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM
 CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide
The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012
 Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY COMPLICATIONS AFTER SCI
 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Basics of NIV. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
EMS System for Metropolitan Oklahoma City and Tulsa 2017 Medical Control Board Treatment Protocols
 S O EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 3H WAVEFORM CAPNOGRAPHY ADULT & PEDIATRIC Indications: 1. Medical General Assessment/General Supportive Care. 2. Trauma General Assessment/Trauma & Hypovolemic
S O EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 3H WAVEFORM CAPNOGRAPHY ADULT & PEDIATRIC Indications: 1. Medical General Assessment/General Supportive Care. 2. Trauma General Assessment/Trauma & Hypovolemic
Respiratory Physiology
 Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
PULMONARY FUNCTION. VOLUMES AND CAPACITIES
 PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
ADVANCED ASSESSMENT Respiratory System
 ONTARIO BASE HOSPITAL GROUP QUIT ADVANCED ASSESSMENT Respiratory System 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Respiratory System AUTHOR(S) Mike Muir AEMCA, ACP, BHSc Paramedic Program Manager
ONTARIO BASE HOSPITAL GROUP QUIT ADVANCED ASSESSMENT Respiratory System 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Respiratory System AUTHOR(S) Mike Muir AEMCA, ACP, BHSc Paramedic Program Manager
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
June 2011 Bill Streett-Training Section Chief
 Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
Questions 1-3 refer to the following diagram. Indicate the plane labeled by the corresponding question number.
 Name: Grade: ANATOMY TEST Questions 1-3 refer to the following diagram. Indicate the plane labeled by the corresponding question number. 1. Plane #1 is the... 2. Plane #2 is the... 3. Plane #3 is the...
Name: Grade: ANATOMY TEST Questions 1-3 refer to the following diagram. Indicate the plane labeled by the corresponding question number. 1. Plane #1 is the... 2. Plane #2 is the... 3. Plane #3 is the...
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
A. Incorrect! The alveolus is where gas exchange takes place. B. Correct! Surfactant is the lipid-rich material that permits lung inflation.
 Toxicology - Problem Drill 13: Respiratory Toxicology No. 1 of 10 1. The lipid-rich material that decreases surface tension of the alveoli, allowing sacs to inflate properly and remain inflated during
Toxicology - Problem Drill 13: Respiratory Toxicology No. 1 of 10 1. The lipid-rich material that decreases surface tension of the alveoli, allowing sacs to inflate properly and remain inflated during
The Goal of the Respiratory Assessment. Two Parts of the Respiratory Assessment
 The Respiratory System Respiratory Assessment of the Adult Patient Mary Douglas, MSN, RN Nurse Educator Minneapolis VA Health Care System Respiratory system: moves oxygen into the body and carbon dioxide
The Respiratory System Respiratory Assessment of the Adult Patient Mary Douglas, MSN, RN Nurse Educator Minneapolis VA Health Care System Respiratory system: moves oxygen into the body and carbon dioxide
There are four general types of congenital lung disorders:
 Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Restrictive lung diseases
 Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
Chapter 16. Objectives. Objectives. Respiratory Emergencies
 Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key
Chapter 16 Respiratory Emergencies Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key