Stroke and TIA. Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne
|
|
|
- Beverly Davidson
- 6 years ago
- Views:
Transcription
1


2 Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne
3 Global burden of stroke 20 million strokes each year 2 nd leading cause of death worldwide >50 million stroke/tia survivors alive 20% have further stroke <5 years Recent trials BP lowering therapy, statins, antiplatelet therapy, atrial fibrillation strategies, stents are changing practice
4 Case vignette 63 year old Mrs Faul with a past history of smoking and BP always elevated at medicals, thought to be white coat hypertension and untreated. Whilst attending national sales conference in Melbourne, giving a presentation, sudden onset of speech difficulties and right sided weakness, seems confused What should bystanders do?

5


6 Cincinnati Prehospital Stroke Scale Facial Droop: Have Patient Smile Image Source: NINDS


7 Arm Drift: Close Eyes & Hold Out Both Arms Image Source: NINDS
8 New definitions stroke and transient ischemic attack (TIA) Old definition 1960 s acute neurological deficit, vascular origin, >24 hour deficits New definitions Strokes can be silent Brief episodes < 24 hours but with brain injury = stroke, not TIA Brief neurological episodes (usually < 24 hours) without damage on imaging = TIA

9 Time is brain Rapid transport to a stroke centre Rapid ambulance transport Paramedical diagnostic stroke tools FAST,Cincinatti,LAPS Potential in future for ambulance-based therapy
10 Assessment in ED O/E (90 mins after onset of symptoms) alert, BP 170/100, irregular pulse expressive dysphasia, moderate right hemiparesis Appears frustrated What should be done next?
11 Emergency Department Code Stroke 1. Urgent triage and high priority for stroke patient 2. Mobilise the stroke team 3. IV - glucose, routine biochemistry, FBE 4. ECG 5. Accurate clinical diagnosis exclude mimics 6. Urgent CT
12 Conditions that mimic stroke Hand et al. Stroke 2006 Mimics presenting: Condition Total Number (%) Within 6 hrs After 6 hrs Seizure 23 (21.1%) 18 (29.0%) 5 (10.6%) Sepsis 14 (12.8%) 6 (9.7%) 8 (17.0%) Toxic / metabolic 12 (11.0%) 6 (9.7%) 6 (12.8%) Space occupying lesion 10 (9.2%) 3 (4.8%) 7 (14.9%) Syncope / presyncope 10 (9.2%) 9 (14.5%) 1 (2.1%) Acute confusional state 7 (6.4%) 3 (4.8%) 4 (8.5%) Vestibular dysfunction 7 (6.4%) 3 (4.8%) 4 (8.5%) Acute mononeuropathy 6 (5.5%) 4 (6.5%) 2 (4.3%) Functional/medically unexplained symptoms 6 (5.5%) 4 (6.5%) 2 (4.3%) Dementia 4 (3.7%) 2 (3.2%) 2 (4.3%) Migraine 3 (2.8%) 2 (3.2%) 2 (4.3%) Spinal cord lesion 3 (2.8%) - (0%) 3 (6.4%) Other? 3 (3.7%) 2 (3.2%) 1 (2.1%) Total 109 (100%) 62 (100%) 47 (100%)
13 Clinical features that distinguish between stroke & mimic (Hand et al 2006) Stroke predicted by exact time of onset patient could recall exactly what they were doing at symptom onset well in the last week definite focal symptoms or signs, worse NIHSS Mimic predicted if known cognitive impairment lost consciousness or seizure at onset patient could still walk no lateralising symptoms confusion, non-vascular or no neurological signs


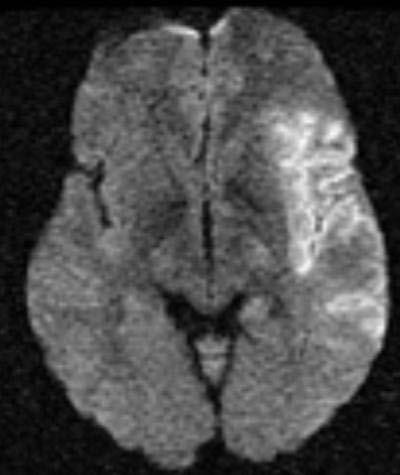



14 L MCA Infarct DWI lightbulb

15 R MCA Infarct 4.5 hours early ischemic changes on CT


16 Deep putaminal ICH
17 Major stroke types Ischemic stroke (cerebral infarction) Intracerebral hemorrhage (ICH) Subarachnoid hemorrhage (SAH)
18 Major stroke types Ischemic stroke 1. Large artery thromboembolism 2. Cardiogenic embolism 3. Small vessel (lacunar) infarction 4. Rarer causes 5. Unclassified or cryptogenic Intracerebral hemorrhage (ICH) 1. Deep hypertensive location 2. Lobar Subarachnoid hemorrhage (SAH) 1. Aneurysm 2. Arteriovenous malformation 3. Other
19 Ischemic Stroke Classification 1 Large artery thromboembolism Cortical infarction, >50% relevant large artery stenosis, absence of cardiac source Cardiogenic embolism Cortical infarction, cardiac source (most often Afib), absence of large artery disease Lacunar Infarction Subcortical infarction, absence of large artery or cardiac source, clinical syndromes
20 Ischemic Stroke Classification 2 Rare causes For example, arterial dissection, drugs, vasculitis, rarer arteriopathies such as Moyamoya disease Dual Pathology For example, cardiac + large artery source Unclassified Despite adequate investigation Inadequate investigation
21 Intracerebral Hemorrhage 15% stroke in NZ, 30% in Asia The most lethal stroke subtype Higher mortality (30-40%), worse functional outcome Stroke Unit Care effective BUT to date surgery and other therapies have shown NOT shown benefit in randomized clinical trials
22 Classification ICH Deep Lobar Putamen, thalamus, brainstem, cerebellum Usually due to hypertension and rupture of deep penetrating arteries Superficial Often secondary to amyloid angiopathy, tumour, arteriovenous malformation, aneurysm
23 Assessment in ED Mrs Faul has had an ischaemic stroke. What should be done next?
24 Why are early recognition and diagnosis time-critical? Both ischemic stroke and hemorrhagic stroke are dynamic, evolving conditions Stroke evolution results in increased lesion volume = worse outcome Therapies for both ischemic stroke and ICH are aimed at limiting stroke growth

25 Rescuing the penumbra: the aim of acute ischemic stroke treatment

26 Anterior Cerebral Artery collaterals Infarct Core Ischemic Penumbra Posterior Cerebral Artery collaterals
27 Time is brain Quantified Saver J. Stroke 2006;37: Every minute counts!

28 Thrombolysis Salvaging the Ischemic Penumbra Minutes Hours Time Days and weeks Dirnagl U. Trends Neursci. 1999;22:
29 How should she be treated? Mrs Faul was given IV tpa and admitted to the Stroke Unit. She had a good response to thrombolysis. An ECG confirms atrial fibrillation CTA (on admission) shows tight left ICA stenosis How should she be treated to prevent recurrent stroke?
30 Acute interventions based on level I evidence INTERVENTION INITIAL OR IMPORTANT RRR ARR NNT STUDY, YEAR (% ) Stroke unit Langhorne et al, tpa NINDS 1995;ECASS Aspirin IST, CAST Hemicraniectomy Vahedi K et al, GA Donnan, M Fisher, M Macleod SM Davis Lancet, 2008.

31
32 All trials strongly positive able 1: summary of recent endovascular trial results Trial Age (years) Baseline severity (NIHSS) IV rtpa Treatment Rate ENDOVASCULAR ONLY Artery opened Time to open artery ENDOVASCULAR VS CONTROL ARM 90 -DAY CLINICAL OUTCOMES Independent (%) Mortality (%) MR CLEAN % 59% 332 min 33% vs. 19% 21% vs 22% EXTEND-IA % 86% 248 min 71% vs 40% 9% vs 20% ESCAPE % 72% 241 min 53% vs 29% 10% vs 19% SWIFT PRIME % 88% 257 min 60% vs 36% 9% vs 12% REVASCAT % 66% 355 min 44% vs 28% 18% vs 16% Around double the rate of independent outcome Mortality reduction up to 50%
33 TIAs and ischemic strokes are high-risk patients 5-10% stroke at 1 week 10-20% stroke at 3 months Even higher recurrence rate if DWI performed Probably similar for ischemic stroke Patients with CVD are at high risk CHD and vascular death
34 Primary Prevention What are the risk factors? How can we reduce the risk?
35 Primary prevention - Risk factors for ischemic stroke Non-modifiable Modifiable risk factors risk factors Established Possible Age HT Physical inactivity Gender Diabetes Obesity Family history Smoking Dietary factors Ethnicity AF/heart disease Oral contraceptive use cholesterol Lack of HRT Alcohol consumption Infection Prothrombotic factors Stress Prior TIA Sleep apnea Prior stroke Socio economic
36 Primary Prevention Main modifiable risk factors are smoking, hypertension, diabetes and obesity Encourage smoking cessation, weight loss, increased physical activity and a healthy diet Antihypertensive drugs reduce the risk of primary stroke by up to 40% There is no clear indication for antiplatelet treatment in low risk, or intermediate risk (uncomplicated diabetes, hypertension or hypercholestrolaemia) of stroke In high risk of cardiovascular disease consider aspirin

37 What rhythm is this and why are we asking?
38 Atrial fibrillation (AF) AF is the most common heart rhythm disturbance 1 It is estimated 1 in 4 individuals aged 40 years will develop AF 1 In 2007, 6.3 million people in the US, Japan, Germany, Italy, Spain, France and UK were living with diagnosed AF 2 Due to the aging population, this number is expected to double within 30 years 3 1. Lloyd-Jones DM, et al. Circulation 2004;110: Decision Resources. Atrial Fibrillation Report. Dec Go AS, et al. JAMA 2001;285:


39 Stroke Risk in Atrial Fibrillation Control Groups in Randomized Trials Stroke Rate (% per year) Age (years) Atrial Fibrillation Investigators. Arch Intern Med 1994;154:1449.

40 Stroke severity in patients with AF Effect of first ischemic stroke in patients with AF (n=597) 1 60% 50% % of patients 40% 30% 20% 10% 0% Disabling Fatal 1. Gladstone DJ et al. Stroke. 2009; 40:
41 Warfarin in Atrial Fibrillation Stroke risk reduction Warfarin Better Control Better AFASAK SPAF BAATAF CAFA SPINAF EAFT Aggregate 100% 50% 0-50% -100% Hart RG et al. Ann Intern Med 1999; 131:492.
42 New Oral Anticoagulants (NOAC) Direct Thrombin Inhibitor Dabigatran (RE-LY study) Connolly SJ., et al. N Engl J Med 2009; 361: Factor Xa Inhibitors Rivaroxaban (ROCKET-AF study) Patel MR., et al. N Engl J Med 2011; 365: Apixaban (ARISTOTLE study) Granger CB., et al. N Engl J Med 2011; 365: Essentially, at least as effective and safe as warfarin in stroke prevention Registered and PBS subsidised for prevention of stroke (or systemic embolism) in non-valvular AF in a patient with one or more risk factors for developing stroke (see CHADS2)
43 Assessing stroke risk in non-valvular AF There needs to be consideration of benefit to risk. Oral anticoagulation carries a risk of haemorrhage at least 1-1.5% per annum, greater in over 80 years old. There are a number of published models for calculating risk and maybe used as an aid to balancing the risks Most widely used is the CHADS2 score
44 CHADS2 The CHADS2 scoring system (score 1 for each risk factor of heart failure, hypertension age >75, and diabetes, score 2 for previous stroke of TIA). If score zero, can undertake a more comprehensive risk assessment e.g. CHADSVASc CHADS2 score 1 recommends an oral anticoagulant Oral anticoagulants reduce the risk of stroke by about 60% in people with AF (aspirin RRR ~25%) CHADS2 score Annual risk (%)
45 Secondary Prevention Tailored to stroke pathogenesis in individual Recurrent stroke risk is 4% per annum Secondary prevention should start in hospital

46
47 ABCD 2 Score Generated from 2 derivation cohorts (California, Oxford, 1916 pts) and validated in 4 independent cohorts (2893 patients) Age >/= 60 1 BP SBP>/= 140 or DBP >/=90 1 Clinical Focal weakness 2 Speech imp w/o focal weakness 1 Duration >/=60min min 1 Diabetes 1 TOTAL _ / 7 Johnston SC, Rothwell PM, Nguyen-Huynj MN et al. Validation and refinement of scores to predict very early stroke risk after transient ischemic attack. Lancet 2007;369:283-92
48 Prevalence of stroke Risk group (ABCD2 score) Low (0-3) Moderate (4-5) High (6-7) Prevalence DAY 2 Prevalence DAY 7 1.0% 1.2% 3.1% 4.1% 5.9% 9.8% 8.1% 12% 18% Prevalence DAY 90
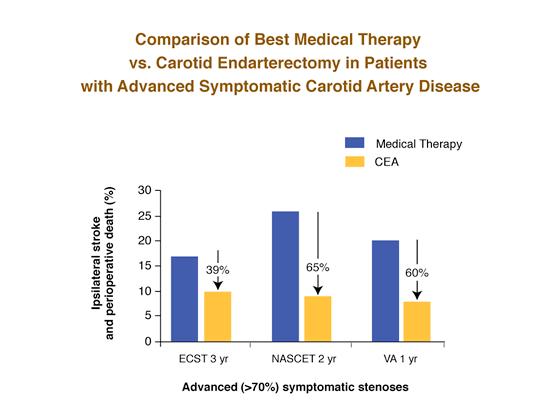
49 Overview of secondary prevention Blood pressure lowering Cholesterol and statins Antiplatelet therapy which strategy? Atrial fibrillation and anticoagulation Carotid revascularization endarterectomy and stenting
50 BP and recurrent stroke 2.00 Rodgers et al. BMJ mmhg: RR 28% SE Usual Systolic Blood Pressure (mm Hg)
51 SPARCL: Study design Stroke or TIA in 6 months, no known CHD, LDL-C mg/dl N = 4731 Atorvastatin 80 mg daily n = 2365 Randomized Double blind Placebo n = 2366 Primary end point: Fatal/nonfatal stroke Secondary end points: Major coronary or CV events Follow-up: ~5 years (until >540 primary end points) SPARCL Investigators. N Engl J Med. 2006;355:
52 SPARCL: Statin treatment reduces Primary outcome fatal/nonfatal stroke % RRR* HR 0.84 ( ) P = 0.03 Placebo NNT = 46 patients for 5 years Fatal/ nonfatal stroke (%) 8 4 Atorvastatin *Adjusted Time since randomization (years) SPARCL Investigators. N Engl J Med. 2006;355:
53 Paradigm shift in BP, cholesterol Lowering blood pressure and cholesterol at any level equally effective in secondary stroke prevention SPARCL results (atorvastatin post stroke) in 2005 Move away from concepts of normal vs high BP and cholesterol The polypill to reduce CVD by > 80% (Wald, Law BMJ 2003) Statin 3 BP drugs eg thiazide, beta blocker, ACE inhibitor Aspirin Folic acid
54 Antiplatelet Therapy Aspirin reduces the risk of subsequent stroke by approx. 13% and all vascular events by 20%1 Dipyridamole plus aspirin was marginally more effective than aspirin alone. Preferred if patient at moderate to severe absolute risk, or recurrent stroke. Side effect of headache common. 2 Clopidogrel is modestly more effective than aspirin in the prevention of serious high risk vascular events. 3 A+C may have a role in first 90 days after stroke, TIA 1. Algra,van Gijn JNNP Diener. Neurology CAPRIE Lancet 1996
55

56

57

58 Benefits of Endarterectomy are time-linked to last symptomatic event P M Rothwell, M Eliasziw, S A Gutnikov, C P Warlow, H J M Barnett, for the Carotid Endarterectomy Trialists Collaboration Lancet 2004; 363:

59 CEA Complications NASCET ECST Death or stroke 5.8% (6.7%) 7.1% Cranial nerve palsy 7.6 % 6.4% Wound complications 8.9 % 3.3% CVS complications 3.9 % 0.2% Other 0.3% Total complications 26.2 % 19.3%
60 How should Mrs Faul be treated? Lifestyle issues stop smoking Regular exercise Ideal weight Reduce BP to <120/80 Statin Carotid endarterectomy or stenting long-term anticoagulation with dabigatran or other new OAC
61 Conclusions Important to understand basic definition and classification of stroke This is vital because of the link to both acute treatment and secondary prevention Strokes evolve, providing an opportunity for treatments aimed at attenuation of growth of infarct and ICH Stroke is now regarded as a preventable and treatable disease
62 Secondary prevention summary High-risk patients benefit from BP, cholesterol lowering regardless of baseline Antiplatelet therapy routine if patient not anticoagulated Warfarin may be replaced for atrial fibrillation by new OAC Carotid endarterectomy proven therapy for carotid artery stenosis Carotid stenting may be equivalent for patients < 70 years
63 Copyright The University of Melbourne
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
La gestione dell ictus ischemico o emorragico nel paziente sotto NAO
 La gestione dell ictus ischemico o emorragico nel paziente sotto NAO Antonio Carolei e Cindy Tiseo Clinica Neurologica e Stroke Unit Avezzano - Sulmona Università degli Studi dell Aquila Abano Terme, 10
La gestione dell ictus ischemico o emorragico nel paziente sotto NAO Antonio Carolei e Cindy Tiseo Clinica Neurologica e Stroke Unit Avezzano - Sulmona Università degli Studi dell Aquila Abano Terme, 10
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Atrial Fibrillation & Acute Stroke
 Atrial Fibrillation & Acute Stroke Acute Stroke Stroke Facts Aetiology Thrombosis Classification outcomes Time is Brain Acute Stroke Over 5 million people die as a result of stroke and another 5 million
Atrial Fibrillation & Acute Stroke Acute Stroke Stroke Facts Aetiology Thrombosis Classification outcomes Time is Brain Acute Stroke Over 5 million people die as a result of stroke and another 5 million
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Patients presenting with acute stroke while on DOACs
 Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Disclosures. An Update on TIA and Minor Stroke. The Agenda PROGNOSIS PATHOPHYSIOLOGY GUIDELINES AND PROVEN MANAGEMENT STRATEGIES AGGRESSIVE TREATMENT
 Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Stroke secondary prevention. Gill Cluckie Stroke Nurse Consultant St. George s Hospital
 Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology
 Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
controversies in anticoagulation: optimizing outcome for atrial fibrillation
 controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care
 Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care 11 th and 25 th September 2014 3 KEY OBJECTIVES OF TALK 1.
Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care 11 th and 25 th September 2014 3 KEY OBJECTIVES OF TALK 1.
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Epidemiology and Prevention of Stroke
 Copyright Information Copyright protected material has been deleted from this presentation. References to the deleted material are provided for each slide. Epidemiology and Prevention of Stroke Larry B.
Copyright Information Copyright protected material has been deleted from this presentation. References to the deleted material are provided for each slide. Epidemiology and Prevention of Stroke Larry B.
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Modern management of atrial fibrillation, from blood pressure control to anticoagulation
 Modern management of atrial fibrillation, from blood pressure control to anticoagulation Adel Khalifa S. Hamad, BMS, MD, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist
Modern management of atrial fibrillation, from blood pressure control to anticoagulation Adel Khalifa S. Hamad, BMS, MD, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
OHSU. and Minor Stroke. Sierra Ford, DO
 TIA and Minor Stroke Sierra Ford, DO Disclosures No financial disclosures Objectives Introduction Epidemiology Assessment of possible stroke/tia History/Exam Testing Secondary stroke prevention treatments
TIA and Minor Stroke Sierra Ford, DO Disclosures No financial disclosures Objectives Introduction Epidemiology Assessment of possible stroke/tia History/Exam Testing Secondary stroke prevention treatments
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
TREATMENT OF STROKE PATIENTS THAT ARE TAKING NOVEL ANTICOAGULANTS. Jesse Weinberger, MD The Icahn School of Medicine at Mount Sinai
 TREATMENT OF STROKE PATIENTS THAT ARE TAKING NOVEL ANTICOAGULANTS Jesse Weinberger, MD The Icahn School of Medicine at Mount Sinai Acknowledgement Many of the slides for this presentation were obtained
TREATMENT OF STROKE PATIENTS THAT ARE TAKING NOVEL ANTICOAGULANTS Jesse Weinberger, MD The Icahn School of Medicine at Mount Sinai Acknowledgement Many of the slides for this presentation were obtained
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients. Giancarlo Agnelli
 NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Defining Sub-Clinical Atrial Fibrillation and its management
 Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Identifying Patients for Anticoagulation: While Many Patients Remain Untreated, Who Should NOT be Anticoagulated?
 Identifying Patients for Anticoagulation: While Many Patients Remain Untreated, Who Should NOT be Anticoagulated? Renato D. Lopes, MD MHS PhD Professor of Medicine Division of Cardiology Duke Clinical
Identifying Patients for Anticoagulation: While Many Patients Remain Untreated, Who Should NOT be Anticoagulated? Renato D. Lopes, MD MHS PhD Professor of Medicine Division of Cardiology Duke Clinical
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor
 Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
Recanalization Therapy & Secondary Prophylaxis in the Elderly
 Recanalization Therapy & Secondary Prophylaxis in the Elderly 21 st Annual Meeting of the Swiss Stroke Society Lausanne,11.01.2018 PD Dr. G. M. De Marchis, MD MSc Neurology & Stroke Center University Hospital
Recanalization Therapy & Secondary Prophylaxis in the Elderly 21 st Annual Meeting of the Swiss Stroke Society Lausanne,11.01.2018 PD Dr. G. M. De Marchis, MD MSc Neurology & Stroke Center University Hospital
Understanding transient ischaemic attack
 chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Ischemic stroke: management, prevention and follow up. Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute
 Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia
 Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia Charidimou et al, 2012 Pathogenesis of spontaneous and anticoagulationassociated
Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia Charidimou et al, 2012 Pathogenesis of spontaneous and anticoagulationassociated
IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS?
 IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS? J.Y. LE HEUZEY Georges Pompidou Hospital, René Descartes University, Paris H E G P Munich, August 27, 2012 Disclosure Consultant / Conferences / Advisory
IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS? J.Y. LE HEUZEY Georges Pompidou Hospital, René Descartes University, Paris H E G P Munich, August 27, 2012 Disclosure Consultant / Conferences / Advisory
Reversal Agents for NOACs (Novel Oral Anticoagulants)
") Reversal Agents for NOACs (Novel Oral Anticoagulants) Current status and future challenges Paul A Reilly, PhD Clinical Research, Boehringer Ingelheim, Inc CSRC Symposium Washington DC Oct 18, 2016 Atrial
Reversal Agents for NOACs (Novel Oral Anticoagulants) Current status and future challenges Paul A Reilly, PhD Clinical Research, Boehringer Ingelheim, Inc CSRC Symposium Washington DC Oct 18, 2016 Atrial
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
10/21/2014. Disclosures. Introduction. Reasons for the Decline in Stroke Mortality: Implications for Hypertension and Risk Factor Management
 Reasons for the Decline in Stroke Mortality: Implications for Hypertension and Risk Factor Management Daniel T Lackland Disclosures Member of NHLBI Risk Assessment Workgroup Member of 2014 Hypertension
Reasons for the Decline in Stroke Mortality: Implications for Hypertension and Risk Factor Management Daniel T Lackland Disclosures Member of NHLBI Risk Assessment Workgroup Member of 2014 Hypertension
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Results from RE-LY and RELY-ABLE
 Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Disclosures. Current Management of Acute Ischemic Stroke. Overview. Focal brain ischemia. Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015
 Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE
 Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Atrial Fibrillation. Alan Bell, MD, CCFP. Staff Physician, Humber River Regional Hospital. University of Toronto
 Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto