Lipid Update AHA/ACC 2013 Guidelines
|
|
|
- Jane Carroll
- 6 years ago
- Views:
Transcription
1 Lipid Update AHA/ACC 2013 Guidelines Jessica M. Fleagle (Bender) D.O. University of Missouri School of Medicine Assistant Professor of Clinical Medicine Associate Program Director of Medicine Residency January 31, 2015

2 Goals Overview Focus on ASCVD risk reduction: 4 statin benefit groups A new perspective on LDL-C and/or Non-HDL C treatment goals Global risk assessment for primary prevention: 10 year ASCVD risk Case applications Safety recommendations Role of Biomarkers and noninvasive tests
3 NHANES Top Sins for CVD mortality in Population-Attributable Fractions 1. BP (apaf of 39.2%) with or without treatment >120/80 Every 10% increase in hypertension treatment, an estimated deaths would be prevented annually 2. Current Smoking (14.3) Every 5% increase in smoking cessation would prevent 7000 deaths annually 3. Lack of healthy diet of < or =2 healthy diet score (13.2) 4. BMI >30 (11.3) 5. HbA1c >5.7 (8.2) 6. Cholesterol >240 (3.7)


4 NHANES <2% of Americans met 7 ideal measures Yang, et al. JAMA. 2012;307(12): doi: /jama NHANES 88-94, 99-04, 05-10
5
6 NHANES III Linked Mortality File cohort 14.5 years of follow-up, participants who met 6 or more vs 1 or fewer cardiovascular health metrics had: 51% lower risk of all-cause mortality 76% lower risk of CVD mortality 70% lower risk of IHD mortality.
7 Figure 1. Estimated effects of population-wide shifts in systolic BP distributions on mortality. Appel L J et al. Hypertension. 2006;47: Copyright American Heart Association, Inc. All rights reserved.

8 Why we care about lipids Figure 1 Estimate of number of events avoided for every 1.29 mmol/l reduction in cholesterol concentration in 1000 patients James Shepherd Resource management in prevention of coronary heart disease: optimising prescription of lipid-lowering drugs The Lancet, Volume 359, Issue 9325, 2002,
9 What s new in the 2013 AHA Lipid Guidelines Focus on ASCVD risk reduction: 4 statin benefit groups A new perspective on LDL-C and/or Non-HDL C treatment goals Not a SINGLE RTC to support treatments specific target, i.e. LDL <70, 100 NON statin therapy should NOT be used to reduce ASCVD risk, as the benefits are out weighed by risk and the superiority in statin performance Global risk assessment for primary prevention: 10 year ASCVD risk Safety recommendations Role of Biomarkers and noninvasive tests Future updates 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Stone, et al, Circulation, November 12, 2013

10 RISK RISK RISK RISK RISK RISK RISK RISK RISK
11 Resources to use Websites Apps ASCVD Risk estimator (a favorite at the UMHC) FREE in the app store Also gives summaries, lifestyle recommendations, how to initiate, safety recs and external links to guidelines Patient resources and links as well
12 Population group application Estimates of 10-year risk for ASCVD are applicable to: African-American men and women 40 through 79 years of age Non-Hispanic white men and women 40 through 79 years of age Other ethnic groups, it is recommended to use the equations for non- Hispanic whites, Though these estimates may Underestimate the risk for persons from some race/ethnic groups, especially American Indians, Some Asian Americans (e.g., of south Asian ancestry) Some Hispanics (e.g., Puerto Ricans) Overestimate the risk for others, including: Some Asian Americans (e.g., of east Asian ancestry) Some Hispanics (e.g., Mexican Americans)
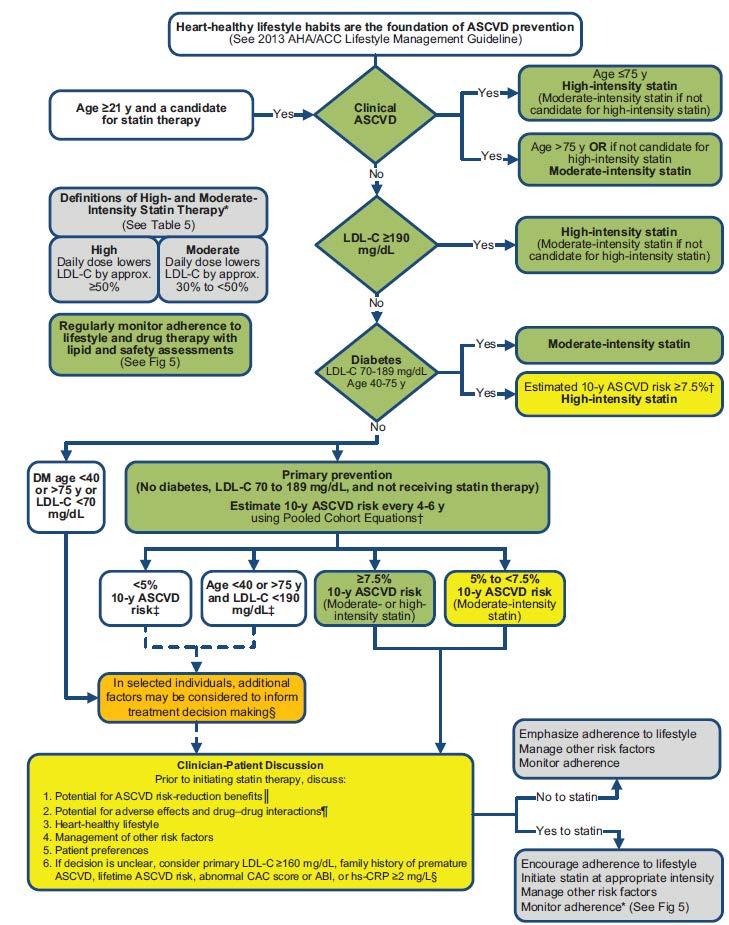
13 Targeted Treatment Groups 1. Clinical ASCVD (secondary). No need to risk assess this group Defined by: 1. ACS, 2. History of MI, 3. Stable or unstable angina, 4. Coronary or other arterial revascularization, 5. Stroke, or 6. Peripheral arterial disease presumed to be of atherosclerotic origin. 2. Primary elevations of LDL-C at or > 190 mg/dl 3. Diabetes aged with LDL-C mg/dl and without clinical ASCVD 4. Without clinical ASCVD or diabetes with LDL-C 70 to 189mg/dL AND estimated 10 yr ASCVD risk of 7.5% or higher

14 Patient perceptions: What my doctor wants, What I actually do
15
16
17 Why statins? Statins prevent both nonfatal and fatal ASCVD events (esp. strokes which women bear the brunt of disability in non-lethal strokes) STRONG evident to reduce mortality in patients with prior ASCVD Moderate evidence without known ASCVD to reduce total mortality with increased risk

18 How I feel about my patients
19 A new perspective on LDL-C and/or Non-HDL C treatment goals NO LONGER set targets just say no to <70 or <100! AIM-HIGH: the additional reduction in non-hdl-c in addition to apo- B, Lp(a) and TGs in addition to HDL-C increases with niacin did NOT reduce ASCVD when pts were treated to LDL-C mg/dl (!) ACCORD: futility in adding fenofibrate in patients with DM, BUT a subgroup showed in those with high TG and low HDL-C suggested that fenofibrate may reduce ASCVD in pts with DM
20 Statins in patients with known ASCVD All pts <75 yrs with known ASCVD If on a statin, go from low or moderate to high-intensity statin if possible High intensity is >50% reduction in LDL-C. Moderate is 30-50%, lower <30% reduction Atorvastatin 40-80mg (IDEAL trial only if not able to handle 80)reduced ASCVD risk more than moderate-intensity with atorvastatin 10, pravastatin 40 or simvastatin mg if >75 yrs of age no clear evidence of benefit of high dose statin Obvious benefit of moderate intensity.

21 Statin initiation in ASCVD
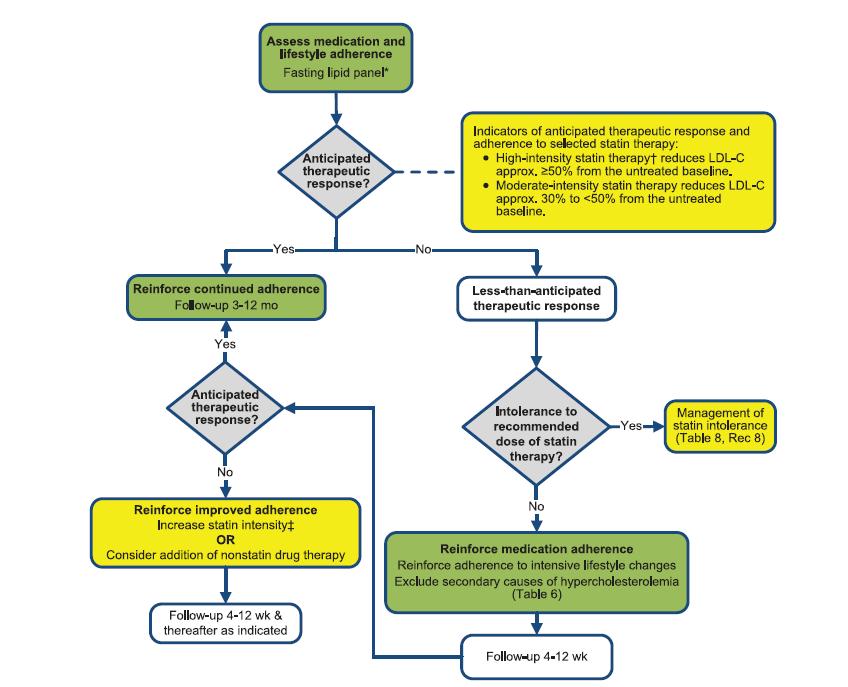
22 Statin Dosing AHA 2013/AHA Blood Cholesterol Update, Stone et al
23
24 Case 1. Kristoff A 63-year-old man is seen in the office 2 weeks after a ST-elevation myocardial infarction (MI). A former smoker with hypertension, he was discharged on atorvastatin 80mg daily, dual antiplatelet therapy, long-acting metoprolol, and an ACE inhibitor. One year before the acute MI, he was prescribed simvastatin 40 mg which was then increased to simvastatin 80 mg. He stopped the simavastatin 80 mg 2 weeks after developing muscle cramps in his legs. Although he has no muscle symptoms since he started the atorvastatin 80 mg, he is concerned about having had muscle cramps in the past on a statin and would like to decrease the atorvastatin to 20 mg daily. What is the best answer? 1. Randomized trials of high intensity statin therapy versus moderate intensity statin therapy have not shown a significant difference in outcomes. He should decrease the atorvastatin to 20 mg to minimize adverse effects. 2. Systematic meta-analyses of randomized clinical trials support using an intensive statin dose such as atorvastatin 80 mg/day over a moderate intensity statin. He should stay on atorvastatin 80 mg. 3. He should be followed with creatine kinase (CK) values when his lipids are checked at each visit for the first year. 4. Although his liver panel was normal in the hospital, he should have ALT done at each subsequent visit.
25 Other pearls from Kristoff CKs are not needed for screening CK obtain if muscle aches or consider in previous muscle aches If you have myalgias, do a stop statin and washout If after 2 weeks statin free and STILL with myalgic, go after NON-statin cause Try a dose reduction or a different statin, i.e. simvastatin to atorvastatin In Kristoff, a SLC01B1 deficiency may explain the simvastatin 80 and CCB leading to the muscle aches Simvastatin 80 not rec d any longer If your pt is on simvastatin 80 for 12 mo. or longer without muscle injury, that s ok, but don t initiate or up to that dose
26 Kristoff s back 3 yrs later He was on artovastatin 80mg for >2.5 yrs without muscle symptoms. He recently developed progressive myalgias and weakness over weeks. He can t do 3 squats and 6 mo. prior to was doing many at the local gym. He s been off statins for 2.5 weeks and still symptomatic. Which is the best answer? 1. He should be switched to red yeast rice 2. Stay off statin until he s eval d for other causes 3. Switch to rosuvastatin 40 mg and given CoQ10 4. He should be re-challenged with atorvastatin 80 If he s AA, CK levels are not useful in evaluating muscle symptoms
27 Myalgias are not always statin! Off >2 weeks, look elsewhere: PMR, etoh use, hypothyroidism, primary muscle disease CK, ESR, etc. In Kristoff, CK WNL ESR >100 Treated for PMR and then had statin re-instated Xuezhikang, red yeast rice extract










28 NO YES

29 Lifestyle Yes, I am serious You should be too Low fat vegetarian diet NO STATIN Meditation/Yoga Exercise Eating/ cooking Induction Less LDL decreased, but MORE reduction in atherosclerosis load and events just sayin >50-54% adherence
30
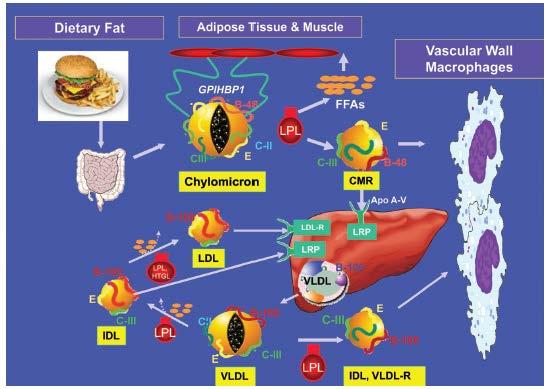
31 Lipid metabolism

 consider genetic.")
32 Triglycerides Clear increase risk of ASCVD with increased TG, female>men 25% undiagnosed DM Consider familial if > 95 th percentile >1000 FCHL FHTG, Apo C II def, Apo-A5, GP1HBP1 If high after diet, exercise, glucose control and removal of offending drugs, toxins (ETOH) consider genetic. See handout Lipodystrophy
33
 JELIS high risk group (TG >180 and HDL<40) statin and EPA had reduced 53%")
34 Triglycerides If statin candidate, statin first, then Fibrate, if primary and then 2-4 grams EPA (VA-HIT) Fibrate esp. if DM not at goal and TG> 204 and HDL low <34 (ACCORD) JELIS high risk group (TG >180 and HDL<40) statin and EPA had reduced 53% ASCVD risk
35 Case 2. Sven 48 yr man with FH and hx of CABG x3 7 years ago for statin intolerance. Max dose he tolerates is rosuvastatin 10 mg twice a week. If taken more than this, he has diffuse aching without weakness and a normal CK. Most recent FLP showed: LDL-C of 168, TG 138, and HDL-C of 46. Initial LDL-C was 240. Which is the best answer? 1. Ezetimibe has been shown to further reduced ASCVD events when added to statin therapy. Continue statin and add ezetimibe 10 mg 2. Gemfibrozil has been shown to reduce the ASCVD events when used as monotherapy in men with CAD. Continue statin, add gemfibrozil 3. Bile acid sequestrants have been shown to reduce ASCVD events when used as monotherapy in men with primary hypercholesterolemia. Continue statin, add cholestyramine 4 g packets BID 4. DC the rosuvastatin and begin the lovastatin 40 mg daily
36 Sven pearls Didn t get 50% reduction, but STAY on statin. Even the 72 decrease means 40% reduction in ASCVD risk for him If used as monotherapy, niacin and bile acid sequestrants reduce ASCVD events, but AIM-HIGH showed 0 benefit to adding either niacin or ezetimibe to statin. IMPROVE-IT showed ezetimibe with simvastatin with CKD reduced ASCVD events While gemfibrozil reduced ASCVD events in men with CAD, CAN T use with statin due to HIGH risk of myopathy and rhabdomyolysis. Consider if absolutely no statin possible. Rosuvastatin has the best LDL-C reduction for dose
37 Case 3. Elsa 26 yr woman with an LDL-C 260 mg/dl, TG 102, since her teens has tried lots of diets. Dad died of MI at 38, and dad s brother diet of stroke at 32. Both were smokers. She s on a second gen OCT and is wondering if she should get off. She wants to conceive. She social smokes. BP 110/60, BMI 24. Bl inferior pole cornea arcus, no xanthelasma, thickened Achilles tendon. CV exam WNL. Which is the best answer? 1. She s likely heterozygous for familial hypercholesterolemia and should start high-intensity statin 2. if her partner has normal cholesterol, the likelihood of her child having her genetic condition is an icy 1 in 4 3. Cigarette smoking should be stopped because of desired pregnancy Stop oct and start high dose statin Estimate 10 yr risk of ASCVD and then consider statin
38 Elsa She s heterozygous for FH HIGH statin BY THE AGE OF 21 Continue contraception while on statin. It s class X Once planned for pregnancy, stop 2-3 mo in advance, resume after lactation complete. Use non-estrogen. Autosomal Dominant, so 1:2 These folks should NEVER smoke Counsel other lifestyle

39 Primary prevention LDL-C >190 mg/dl Reduction in risk: diet, exercise, meditation, stress reduction, health awareness Look for secondary causes when LDL-C >190mg/dL and TG >500mg/dL if not clear to be FH If no secondary causes, screen for genetic source, then do family testing and counseling Screen for alt >3 times ULN
40 Secondary causes If TG non-fasting >500 get fasting, if >500 fasting, genetic testing (if not uncontrolled DM) Most common: Excess ETOH Uncontrolled DM Overt albuminuria Pregnancy and lactation Normal progressive rise of cholesterol and TG Contraindicated statins, ezetimibe, niacin

41 Starts before birth and in childhood.
42 Primary prevention For each 39 mg/dl reduction in LDL-C by statin, reduced ASCVD risk by about 20% AFCAPS-TEXCAPS and MEGA trials looked at target # goal, no benefit to LDL-C <100 vs % reduction If LDL-C >190 mg/dl, high dose statin regardless or 10 yr risk GOAL: at least 50% reduction in LDL-C If can t tolerate, highest dose tolerable May add other drugs to achieve greater reduction, but this is expert opinion However, add a drug when 50% reduction didn t occur
43
44
45 Case 4. Anna 60 yr AA female here to inquire about starting a statin, but worried about it causing DM. Her mom had DM and a stroke at 62. She s a nonsmoker, BP 142/88 on 2 BP meds and BMI is 31. FLP shows total cholesterol of 200, HDL-C 55, TG 100, LDL-C 125. fasting BG is 109 and HbA1C 5.9%. What s her 10 Yr ASCVD risk? Which is the best answer? 1. She should focus on lifestyle change to improve her risk because lifestyle has been show to reduce risk > than statins 2. Risk of progression to DM with a statin outweighs any ASCVD risk reduction from statins. No statin 3. She should start a moderate or high-intensity statin 4. A high-sensitivity CRP >2 would be needed to help decide to start a statin
46 Anna Risk >7.5% 10 yr moderate or high based on evidence (AFCAPS/TexCAPS, MEGA, JUPITER) AA women have higher risk that similarly aged non-hispanic white women She is not DM YET, LIFESTYLE CHANGE. MetS = metformin JUPITER showed women >60 with a CRP >2 had a reduction of ASCVD events with rosuvastatin 20 Moderate intensity statin results in 1 new DM, while preventing 5.4 ASCVD events per 1000 individuals/1 year High intensity statin resulted in 3 new DM while preventing 5.9 ASCVD events per 1000 individuals/ 1 year However this happened within the first 6 weeks, so may have been natural progression in metabolic syndrome Would only get hscrp if ASCVD risk <7.5% and considering statin
47 Case 5. Hans 35 yr man with a strong FMH of premature CAD with both dad and bro having MI <55. He s a nonsmoker, non-dm, exercising 150m minutes/week. He s gained 10 lbs since 18 yrs age. BP 140/90, wt 170 lb, ht 70 in, BMI FLP showed LDL-c 160mg/dL, HDL-C 45 mg/dl, TG 100. He also eats a heart healthy diet. His wife wants to discuss statin option given FMH. Which would be the most helpful in making a statin decision? 1. Strong FMH of premature ASCVD 2. CAC score of 300 units or more 3. hs- CRP > or equal to 2.0 mg/l 4. Lifetime risk of ASCVD 5. LDL-C at or > All of these can be considered
48 All things considered Primary LDL-C at or more than 160 mg/dl or other evidence or genetic hyperlipidemias FMH of premature ASCVD first degree relative <55 in male, <65 female in first degree female relative High CRP > or equal to 2 mg/dl CAC of at least 300 Agaston units or at or > 75 percentile for age, sex and ethnicity ABI <0.9 Elevated lifetime risk of ASCVD (5-7.5%), or still consider if have any above AND <5% 10 yr risk. For Hans, consider atorvastatin 10/day, simvastatin 20-40, or rosuvastatin 10. Reinforce good habits. Offer low fat vegetarian diet, exercise, meditation, stress reduction, and limit crap in diet. TALK. TALK.
49 Case 6. Olafa A 44 yr woman has a 10 year hx of type 2 DM. She is a nonsmoker with well-controlled DM and microalbuminuria. She is on dietary management, metformin, and takes one omega-3 fatty acid capsule with 840 mg EPA and DHA, lisinopril/hctz for BP. FMH of DM, but not premature ASCVD. She has BP of 134/78, BMI 36, FLP LDL-C 95, TG 350, and HDL-C 38, HbA1c 7.5%. What is the best answer? 1. Her LDL-C is under 100 so she at goal and doesn t require a statin 2. She should start simvastatin 20 mg and fenofibrate 160 mg a day 3. To reduce her risk of ASCVD event, the dose of omega-3 should be increased to 4 capsules daily to lower her TGs 4. If she does not want a statin, a bile acid Sequestrant is the next best choice for her 5. Her 10 yr ASCVD risk should be calculated to determine if she needs a high or moderate intensity statin
50
51

52 The real problem
53 Olafa Pearls She is DM, with and LDL = statin benefit CARDS trial showed women and men with DM, no ASCVD, had reduced ASCVD events with just moderate atorvastatin 10 mg a day JUPITER rosuvastatin 20 reduced ASCVD events If 10 yr ASCVD risk >7.5% HIGH intensity Don t need to know APO B or LDL particle number ACCORD showed no benefit adding fenofibrate to women with TG and love HDL-C. Statins help no matter the LDL # JELIS show 1800 mg EPA added to low dose statin in Japanese women, no primary benefit seen, EXCEPT 53% ASCVD risk reduction in high risk group Bile acid sequestrants can lower HbA1c, but elevate TG. Only start when TG < mg/dl LIFESTYLE: consider low fat vegetarian, low-fat vegan with supplements, Mediterranean diet, NO processed foods. Why? NO HDL-C increasing drugs are shown (YET) to reduce ASCVD events in statin tx d patients AHA recs 2-4 grams EPA and DHA daily for TG lowering, marine preferable (need RCT)
54

55 How times change
56 Practical application From the Canada Install a desktop calculator having characteristics congruent with your practice CCS algorithms using FRS might be most appropriate for Canada Quantification of dietary, exercise, and statin interventions are helpful Tool should include the following: real-time display of changes in risk factors and interventions that are turned on and off; graphics capability to display effects of risk factor changes on CVD risk; ability to generate cardiovascular age, which might improve patients understanding and decision support option for age thresholds, diabetes, and family history Use 10-y CVD risk as threshold for treatment in place of LDL level LDL levels are referenced only as extremes of the primary prevention spectrum and are no longer used as thresholds for intervention Abandon treatment goals In place of treatment goals...maximize change in dietary pattern with patient input; maximize exercise interventions with patient input; optimize exercise and assess myalgia before statin introduction; use statin therapy according to degree of FRS; and consider dispensing with LDL follow-up unless you think it will motivate the patient. This concept might have to be introduced gradually
57 Implementation take home Use statin dosing according to level of FRS and patient tolerance Abandon hscrp measurement as part of risk assessment Treat all patients with diabetes aged 40 to 75 y according to recommendations Treat all adults with LDL 5.0 mmol/l according to recommendations Make the patient part of the intervention decision Canadian Family Physician July 2014 vol. 60 no If intolerant, remember that a low-dose statin can give two-thirds of maximal lipid lowering High-risk patients require high-intensity dosing or maximally tolerated dosing Myalgia might respond to changes in dosing, timing, statin type, or dosing intensity No longer part of treatment decision Treat with moderate-intensity statin if no risk factors are present Treat with high-intensity statin if risk factors are present or the 10-y CVD risk is 7.5% Consider a secondary cause or familial hyperlipidemia Consider consultation A lifestyle commitment can modify risk and reduce need for drug use Patients understanding of absolute risk reduction using statins might influence treatment threshold A 10-y CVD risk treatment threshold of 7.5% is always negotiable


58 Questions?
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Dyslipidemia: What s New In The Guidelines?
 1 Dyslipidemia: What s New In The Guidelines? Rhonda Cooper-DeHoff, Pharm D, MS Associate Professor Colleges of Pharmacy and Medicine University of Florida Disclosures 2 No actual or perceived conflicts
1 Dyslipidemia: What s New In The Guidelines? Rhonda Cooper-DeHoff, Pharm D, MS Associate Professor Colleges of Pharmacy and Medicine University of Florida Disclosures 2 No actual or perceived conflicts
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Prevention Updates and Paradigm Shifts
 Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Primary Prevention Patients aged 85yrs and over
 Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
9/3/ AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis. Disclosure
 2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Disclosure. A New Partnership. Objectives 03/27/2014. What is the main way you have obtained information about the 2013 ACC/AHA Cholesterol Guideline?
 Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
NEW GUIDELINES FOR CHOLESTEROL
 NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary
 2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Treatment of Cholesterol in 2018: Time to Level Up. Most Important Slide. Three Things Learned that Will be Applied
 Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Inflammation and and Heart Heart Disease in Women Inflammation and Heart Disease
 Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Major recommendations for statin therapy for ASCVD prevention
 2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
CPE Session 7. Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction
 CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
APPENDIX 2F Management of Cholesterol
 Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Objec ves To discuss the process of formulation of guidelines and how this may differ among professional societies 5/14/15
 Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
Update on Hyperlipidemia Guidelines
 Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Update on Hyperlipidemia Guidelines Drew Keister MD Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow this and
Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Update on Hyperlipidemia Guidelines Drew Keister MD Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow this and
Cholesterol Medicines New & Old: What to Use When
 Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Pharmaceutical Help to Control Cholesterol
 Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Observations on US CVD Prevention Guidelines. Donald M. Lloyd-Jones, MD ScM FACC FAHA
 Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Pharmacology Challenges: Managing Statin Myalgia
 Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Reducing Cardiovascular Risk Through Non-Statins. Kim K. Birtcher, PharmD Joseph Saseen, PharmD
 Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Volume 2; Number 11 July 2008
 Volume 2; Number 11 July 2008 CONTENTS Page 1 NICE Clinical Guideline 67: Lipid Modification (May 2008) Page 7 NICE Technology Appraisal 132: Ezetimibe for the treatment of primary (heterozygous familial
Volume 2; Number 11 July 2008 CONTENTS Page 1 NICE Clinical Guideline 67: Lipid Modification (May 2008) Page 7 NICE Technology Appraisal 132: Ezetimibe for the treatment of primary (heterozygous familial
2/10/2016. Perspectives on the 2013 ACC/AHA Cholesterol Guidelines. Disclosures. ATP-III Update 2004
 Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures